Head Trauma 181 st INF BDE Combat Lifesaver Plus 181 st INF BDE Combat Lifesaver Plus.
Upload
gbarefoot123Category
view
83download
2Combat Trauma Medicine (CTM)
Student Reference Manual
Deployment Medicine International 2
"These materials may be used only for Educational and Training Purposes. They include extracts of copyright works copied under copyright licenses. You may not copy or distribute any part of this material to any other person. Where the material is provided to you in electronic format you may download or print from it for your own use. You may not download or make a further copy for any other purpose. Failure to comply with the terms of this warning may expose you to legal action for copyright infringement."
Deployment Medicine International 3
THIS PAGE LEFT INTENTIONALLY BLANK
Deployment Medicine International 4
COURSE INTENT Combat Trauma Medicine (CTM)
1. We are medical trainers; we do not establish policy or protocol. We contribute to these processes through our individual and collective experience on the field of battle. We are educators and trainers devoted to the transformation of warriors into warrior healers; the ultimate Warfighter trained to save lives as well as take them.
2. This course of instruction is designed to address the medical theory and
science behind the special needs of providers in a theatre of war. Our goal is to augment the skills already given you through your service schools and other trainingto present you with innovative lessons learned from the battlefieldto give you additional confidence and knowledge. Our mission it to train you to be your best when youre best is needed in combat. Our mission is to train you to save the life of the operator sitting next to you.
3. The DMI CTM (with Live Tissue Training) course addresses the mission of the operational emergency medical care, remote medical care, prolonged transport times, unique military wounding and the pre-hospital environment. In this course we stress both the How and Why of every combat trauma medical task.
4. We provide a course based on current science and actual experience
specific to the unique environments and resources of operational units to build on previous non-medical training to specify and train to the treatment options available to you, the Warfighter, in the combat environment based on the best academic medical consensus (as a minimum, Tactical Combat Casualty Care; Basic and Advanced Pre-hospital Trauma Life SupportCurrent Version), real casualty data, and actual combat experience to include (as a minimum):
Managing Blood Loss Airway Management (Non Surgical) Respiratory Injury Management Circulation Shock Management Head Injury and Hypothermia
Deployment Medicine International 5
Casualty Assessment Medical Ramifications of Blast Injury Operational Burn Injury Management Prolonged Care Advanced Wound Care Management Pain Management Maximizing Operational Performance Field Exercises and Tactically Relevant Scenarios
M A R C H
Deployment Medicine International 6
5. Training for todays warrior healer (Warfighter) has changed tremendously in the past decade. Lessons learned in previous conflicts and requirements for military transformation have been incorporated into this training. The warrior healer of today is the most technically advanced, highest trained, and best equipped ever produced by the United States Militaryour mission is to take your training to the next level.
6. We account for every minute of your training time to maximize your training
experience.
7. Your missions ask questions, contribute, and remain present and
focused. Everything you learn over the next several days will save your life, or the lives of your comrades should you have to apply what is taught in this course pay attention.
8. We believe that proper, detailed, and current medical science taught in the
classroom, and reinforced in the Live Tissue Training will bring together the students performance, knowledge and skills. Therefore, we stress critical points of operational medicine and lessons learned through case studies and experience in austere operational environments. We are dedicated to giving our students the time, training, and experience necessary for them to remain this Nations vanguard.
9. Classroom didactic lecture, simulator training, and practical exercise (mini
labs) will incorporate the following (as a minimum) course criteria DMI will add to this the curriculum and include a much broader spectrum to training for the non-medical operator or combat lifesaver.
Deployment Medicine International 7
COURSE METHOD
The Hybrid Training Model
1. Although not new to the military training regime, performance oriented
training (Task, Condition & Standard) developed in the 1970s and 1980s was adopted years ago as the teaching mechanism of choice by Deployment Medicine International (DMI). DMI accepts performance-oriented training as the baseline standard for all of its training programs. However, training has evolved in the decades following the inception of service wide performance oriented training programsespecially in the field of operational medicine. Therefore, DMI has adopted a four-phased hybrid-training model, which expands the students learning experience in two functional areas (performance and retention). We do this to ensure a definitive result where it is needed mostin battle.
2. The four-phases of the hybrid-training model are:
a. The Classroom Didactic. This will be the lecture portion of your
class, each day, wherein the theory, science, and case studies of each learning objective are discussed.
b. Practical Exercise, Lab and Simulator training (mannequin,
FAST-1, others). This portion of the training model involves the (in class) use of simulators, practical demonstrations, videos, hands on applications and practice using mannequins and other simulators, as well as the experience of performing (permitted) medical procedures on each other and on harvested animal tissues (swine tracheas and ears).
c. Live Tissue Procedures (a half day of medical procedures on
anesthetized animals). The field training exercise training is divided into two-phases (procedures and scenarios). Phase 1 of the live tissue portion of your training involves the intensive focus of performing life-saving battlefield trauma procedures on fully anesthetized animals. DMI instructors monitor and train you
Deployment Medicine International 8
walking you through each procedure, demonstrating, and then allowing you and your team to perform the procedure under their tutelage. DMIs veterinary staff and instructors constantly monitor your patients (anesthetized swine). Students will assist in this attention.
d. Live Tissue Scenarios (a half day of hyper-realistic, tactically
relevant scenario based training using anesthetized animals). The term tactically relevant in Phase II of live tissue training is critical. You are expected to respond to scenarios that template OIF/OEF battlefield conditions, and you will be likely to provide care to the wounded in all three phases of Tactical Combat Casualty Care, (1) Care Under Fire, (2) Tactical Field Care, and (3) Prolonged Field Care conditions.
3. Why do we employ the hybrid-training model; why not just teach medicine?
This is a very good question; however, the training mission of DMI is not only to teach medicine, it is to teach medicine employed in high-threat environments. This is medicine to save life while all around you; the enemy will be trying to take your life. To function in this environment requires the convergence of two elements of the human performance model: the performance curve, and the retention curve.
4. The performance curve defines your ability to do just that, perform, to see
the patient, access the patient, decide the optimum course of action to
treat the patient and then treatsave life. Many of your
colleagues/operators have adopted the adage, Minutes equal blood, and
blood equals life. The performance curve must peak at the point of
wounding, often under fire (care under fire) or facing imminent danger as
you treat (tactical field care), or during prolonged field care. History
demonstrates that performance curves are high in low stress environments
and markedly low in high stress environments. Therefore, how do you
ensure that your performance curve peaks at the point of wounding? In
addition, what other mechanisms drive this peak performance?
Deployment Medicine International 9
5. The other element of measurement in training is the retention curvethe
ability to recall all of the decision variables related to a life saving task at
the speed of thought, during the worst of circumstancesat the point of
wounding. The classroom didactic, the practical labs and Phase I of the
live tissue training are all designed to build muscle memory, to reinforce
analysis, decision, and right action. Through decades of educational
science, it has been determined that the retention curve is affected
differently than the performance curve in high stress learning
environments. In this instance, the stressors of the classroom environment
build and embed neural patterns affecting muscle memory. These
patterns are called upon in battle; what you know must coalesce at
precisely the right moment as action (performance) if you are to be
effective in battle.
Deployment Medicine International 10
The illustration above (first figure) shows the retention curve and performance curve coming together past the point of woundingthis equates to lives lost. The illustration below (second figure) demonstrates the desired outcome of the emergence of the performance and retention curves at the point of woundinga condition of training via the hybrid model.
6. To summarize, in education and training we are dealing with two curves: performance and retention. In high stress learning environments, the performance curve decreases; you do not perform at your highest state when learning complex tasks under high stress conditions. Conversely, when learning complex tasks under low stress conditions, you perform at a
Deployment Medicine International 11
higher level; however, you retain less. This is the educators dilemma, especially when training Warfighters to be their best when their best is needed.
7. The objective is to bring both the retention curve and the performance
curve together, at their peak state, and most critically at the point of wounding. To do so, requires a hybrid-training model. This is why, we do not simply teach medicine from a classroom didactic perspective, nor do we limit your experience to practical exercise, labs and simulatorsto do so would not provide the level of stress necessary to influence both learning curves optimally. To achieve the necessary impact, we involve live tissue in two phases; gradually increasing the environmental training stressors to a level that increases retention, and to a degree decreases performance (in the moment). Instructors focus on reinforcing performance, and retrain where required in the high stress environmenthere is where optimal learning occurs.
8. The objective and evidence of this hybrid-training model is increased
performance and situational awareness through rapid recall of all the steps necessary to perform any given medical task, no matter the complexity. The hybrid-training model trains our medical personnel at all levels to spin the decision cycle faster. Medical personnel are trained to see, access, decide and react under even the most incomprehensible battlefield environments. Remember, Minutes equal blood, and blood equals life. If the sights, sounds, tastes, smells and textures of the battlefield are not unfamiliar to you; if you have to a degree experienced these factorsyou will perform at a higher ratethis is the objective of this course of study and practical exercise.
9. DMI employs educational scientists who continually review the manner in
which we present information to our studentsensuring we explore mechanisms involved in the development of battlefield injury, review human and animal studies, and conduct constant research on and off the battlefield. We commit to being hyper-vigilant; collecting and teaching current information as it pertains to the development of injury and treatment on the battlefield. While teaching the science and mechanism of battlefield trauma now, we also pledge our continued focus to the future of battlefield medicine.
10. This Student Manual is designed to serve you in several ways: a
guide for your classroom didactic portion (lecture), a guide for your practical exercises in class using simulators and during practical labs. This manual is not meant to be an exhaustive review, or finite reference; rather
Deployment Medicine International 12
it is an introduction to key principals of the field of combat trauma medicine. It is meant to be a concise manual for those of you preparing to enter the global war on terror as medical providers across the spectrum, from physician to corpsman. The aim of this course is to inspire you with the theory, the science, and the practical What do I do now? level of information. You will be inundated with a great deal of information; this reference manual will serve as a historical source document for your use, to reflect back on this experience; to use as an azimuth check during your experience in operational medicine.
11. Do not hesitate to ask the faculty for clarification on any training
objective, or to ask for further reference if it is not contained in the master reference list provided.
12. As the field of operational medicine progresses, so shall this
reference manual. We attempt to update as necessary.
Deployment Medicine International 13
WHY THIS COURSE?
Deployment Medicine International Mission Statement: - A team of professionals committed to providing unsurpassed operational medical training complemented by unmatched direct deployed medical support and mission oriented research. We (DMI) believe that proper, detailed, and current medical science taught in the classroom, and reinforced in the field exercises will bring together the students performance and retention curves at the point of wounding. Therefore, we stress critical points of operational medicine and lessons learned through case studies and experience in austere environments. DMI has been training physicians, combat medics, Special Forces soldiers, conventional war-fighters, and personal protection details including White House, and law enforcement in operational medicine for over 15 years. DMI is unique because it is focused on operational medicine. There is no greater reward for our instructors than to know they made a difference through the passing of knowledge and thereby saved a life.
Deployment Medicine International 14
COURSE PREREQUISITES
1. Originally, the intended audience for the various DMI training courses was the Special Operations Forces (SOF) medic, (US Army 18D, US Air Force Para Rescue, US Air Force Special Operations Medics, US Marine Corps RECON Corpsmanor equivalent) and key personnel (Physicians, Physician Assistants, Registered Nurses and Emergency Medical TechnicianParamedics, Intermediate and Basic, Independent Duty Corpsman) associated with suchor equivalent.
2. These mission requirements to support the national forces operational
tempo have shifted the prerequisite skill levels necessary to attend CTM to include basic graduates of the Field Medical Training Battalion corpsman training (and equivalent), as well as, members of the Local, State and Federal Law Enforcement Agencies, as well as other Federal Agencies.
3. Essentially, if you have any medical training at all, you will benefit from the
training offered in this course. Even individuals without medical training have attended this course (non-military) and have expressed a relative degree of comfort with the material (due primarily to the manner and mechanism of instruction) and have stated and demonstrated increased confidence and competence in providing medical aid in emergency trauma situations.
4. It is entirely the decision of the operational commander to challenge the
student to meet or exceed the commanders training expectations. DMI will meet the expectations of any operational commander to train their troops, to augment their skills, improve their confidence and competence to sustain life at the point of wounding on the battlefield.
5. DMI conducts all training in accordance with the applicable guidelines
established by the Committee on Tactical Combat Casualty Care (CoTCCC), and Pre-Hospital Trauma Life Support PHTLS (Current Version) and other policy guidance for Combat Trauma Training (CTT) that includes Live Tissue Training (LTT). This includes ATTP 4-02, OCT 2011, table 2-2, page 2-3 or other appropriate and current US Army Doctrine.
Deployment Medicine International 15
COURSE COMPLIANCE
Information concerning this training is considered to be of a sensitive nature. Therefore, the release of any information pertaining to this course is prohibited without the express written consent of the Medical Director for Deployment Medicine International (DMI).
TACTICAL COMBAT CASUALTY CARE (TCCC) SKILL SETS
Course content is based on skill level. Course material in this manual is limited to skill sets for deploying combatants as listed in the tables below. Supplements to this manual are provided for combat lifesaver, corpsmen, medics and PJs. PHTLS FIGURE 24-1 PHTLS 7TH EDITION, PAGE 595
Deployment Medicine International 16
FIGURE 24-1 TACTICAL COMBAT CASUALTY CARE (TCCC) SKILL SETS
ALL DEPLOYING COMBATANTS SKILL HEMOSTASIS APPLY TOURNIQUET APPLY DIRECT PRESSURE APPLY BANDAGE APPLY COMBAT GAUZE APPLY PRESSURE DRESSING CASUALTY MOVEMENT TECHNIQUES AIRWAY CHIN LIFT/JAW THRUST MANEUVER NASOPHARYNGEAL AIRWAY RESCUE BREATHING PATTERN SIT UP/LEAN FORWARD AIRWAY POSITION BREATHING TREAT SUCKING CHEST WOUND INTRAVENEOUS ACCESS AND IV THERAPY ASSESS FOR SHOCK PREVENT HYPOTHERMIA ORAL AND INTRAMUSCULAR THERAPY ORAL ANTIBIOTIC ORAL ANALGESIA FRACTURE MANAGEMENT SPLINTING
Deployment Medicine International 17
FIGURE 24-1 TACTICAL COMBAT CASUALTY CARE (TCCC) SKILL SETS
COMBAT LIFESAVER SKILL HEMOSTASIS APPLY TOURNIQUET APPLY DIRECT PRESSURE APPLY BANDAGE APPLY COMBAT GAUZE APPLY PRESSURE DRESSING CASUALTY MOVEMENT TECHNIQUES AIRWAY CHIN LIFT/JAW THRUST MANEUVER NASOPHARYNGEAL AIRWAY RESCUE BREATHING PATTERN SIT UP/LEAN FORWARD AIRWAY POSITION BREATHING TREAT SUCKING CHEST WOUND NEEDLE THORACOSTOMY INTRAVENEOUS ACCESS AND IV THERAPY ASSESS FOR SHOCK PREVENT HYPOTHERMIA ORAL AND INTRAMUSCULAR THERAPY ORAL ANTIBIOTIC ORAL ANALGESIA IM MORPHINE FRACTURE MANAGEMENT SPLINTING TRACTION SPLINTING
Deployment Medicine International 18
FIGURE 24-1 TACTICAL COMBAT CASUALTY CARE (TCCC) SKILL SETS
CORPSMAN/MEDIC/PJ SKILL HEMOSTASIS APPLY TOURNIQUET APPLY DIRECT PRESSURE APPLY BANDAGE APPLY COMBAT GAUZE APPLY PRESSURE DRESSING CASUALTY MOVEMENT TECHNIQUES AIRWAY CHIN LIFT/JAW THRUST MANEUVER NASOPHARYNGEAL AIRWAY RESCUE BREATHING PATTERN SIT UP/LEAN FORWARD AIRWAY POSITION LARYNGEAL MASK AIRWAY (LMA) SURGICAL AIRWAY ENDOTRACHEAL INTUBATION COMBITUBE BREATHING TREAT SUCKING CHEST WOUND NEEDLE THORACOSTOMY CHEST TUBE ADMINISTER OXYGEN INTRAVENEOUS ACCESS AND IV THERAPY ASSESS FOR SHOCK START IV LINE/SALINE LOCK OBTAIN INTRAOSSEOUS ACCESS IV FLUID RESUSCITATION IV ANALGESIA IV ANTIBIOTICS
Deployment Medicine International 19
ADMINISTER PACKED RED BLOOD CELLS PREVENT HYPOTHERMIA ORAL AND INTRAMUSCULAR THERAPY ORAL ANTIBIOTIC ORAL ANALGESIA IM MORPHINE FRACTURE MANAGEMENT SPLINTING TRACTION SPLINTING ELECTRONIC MONITORING
Deployment Medicine International 20
INTRODUCTION TO OPERATIONAL MEDICINE
A combination of battlefield tactics and immediate casualty care are essential to mission success and Warfighter survival. This type of combat casualty care is defined as Operational Medicine. TRAINING OBJECTIVES:
1. Explain the role of the non-medical Warfighter in combat casualty care.
2. Explain the combat casualty mortality curve.
3. Identify the Warfighters role in participating in a 3-phase approach to tactical
trauma care.
a. Care Under Fire
b. Tactical Field Care
c. Tactical Evacuation Care
d. ADVANCED: Prolonged Field Care
4. Explain the difference between civilian and combat medicine.
5. Explain the M. A. R. C. H. algorithm approach to combat casualty care:
1. Massive Bleeding 2. Airway 3. Respiration 4. Circulation 5. Head injury & Hypothermia
6. Answer all remaining questions regarding the science of combat casualty care.
Deployment Medicine International 21
The focus of this course is on casualty care and how the non-medical Warfighter must participate in an active role to ensure tactical and medical objectives are achieved. Mission success is no longer defined as just achieving the mission objective but now requires team survival with minimal casualties.
Operational Medicine-Combat Casualty Care
1. Emergency medical care provided in austere and/or remote locations.
2. Casualty care is often secondary to completing the mission.
3. Injuries are primarily penetrating trauma from either fragmentation or gunshot
wounds (GSW).
4. Injuries often occur in a resource-limited environment, where medical supplies
are limited to a Warfighters individual medical kit or a medical providers rucksack.
5. Evacuation of casualties is often measured in hours requiring strategic planning
of evacuation assets.
6. Casualty care is usually initiated by non-medic Warfighters and continued by
medical providers.
7. Resources and personnel are often overwhelmed with multiple casualties and
limited number of medically trained personnel.
Changing tactics is not a consideration in operational medical care!
Deployment Medicine International 22
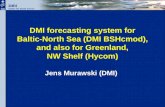
THE COMBAT MORTALITY CURVE
1. Following trauma, the chances of a casualty surviving are dependent upon
numerous variables, including the speed at which appropriate medical treatment
is administered. During this session, we will look at the factors that can affect the
chances of a casualty surviving as injuries develop from initial trauma, through
hemorrhage and/or respiration compromise, as well as shock and infection.
2. The Combat Mortality Curve is based on battlefield penetrating trauma (gunshot
wounds, fragmentation). It was derived from research the lethality of weapons
during the Vietnam conflict. This research provides an understanding of the
survivability of combat casualties over an extended timeline of 72 hours. The
Combat Casualty Mortality Curve also provides a comparison between the
survivability of casualties that receive no medical care and those that do.
%
TIME
Deployment Medicine International 23
COMBAT MORTALITY CURVE DATA
Combat Mortality Curve 100%
90%
70%
60%
50%
80%
6 min 1 hr 6 hr 24 hr 72 hr
-Massive Bleeding
-Respiratory
-Head Injury
-Hypothermia -Wounds (Infection)
-Self Aid & Buddy Aid
-Advanced Life Support (Medic) -Surgery &
Antibiotics
-Airway
-Circulation (Shock)
Deployment Medicine International 24
Time Line 1. 0-6 Minutes:
a. Historically 20% of injuries produce an Inevitable Death Rate (IDR) no matter what medical care they receive. These would include casualties with major system trauma (heart, brain or spinal). The IDR has changed very little during the last 200 years. The use of modern Personal Protective Equipment (PPE) has reduced the rate from 25% to 20%. There are documented cases of casualties with non-survivable injuries surviving for up to six minutes. Therefore, after six minutes, about 80% of the casualties will be alive. Currently reports show an 18% instantaneous death rate.
2. 6 Minutes-1 Hour a. By the end of the first hour, another 10% will die from
exsanguinating hemorrhage (large vessels of the extremities and neck) or from obstruction of the airway (choking) displaced facial tissue and/or swelling occluding the airway. If a casualty can survive the first hour, it is highly probable they will make it to the third hour. Therefore, after 60 minutes, about 70% will survive.
3. 1 Hour-6 Hours a. By six hours, another 10% will succumb to breathing complications.
Some casualties will show the first signs of shock caused by the body running on less blood than normal. Although at this stage, they are unlikely to die from shock alone. After six hours, about 60% will survive.
4. 6 Hours-24 Hours a. Between six and 24 hours, deaths occur from shock early on, but
after this condition, they remain relatively stable although dirty wounds will continue to become more and more infected. After six
Deployment Medicine International 25
hours, the curve is relatively unchanged, about 60% will be alive.
5. 24 Hours-72 Hours a. Between 24 and 72 hours around 10% of the remaining casualties
are lost due to infection or the lack of surgical intervention.
6. 72 Hours a. By 72 hours, deaths occur mostly from wound infections. At 72
hours approximately 50% will survive.
Combat Mortality Curve Timeline
Mitigating Factors:
1. Zero to six minutesPrevent injuries. Personal Protective Equipment (PPE) and good tactics.
2. Six to sixty minutesSelf Aid & Buddy Aid. Stop the bleeding and open the
airway.
3. One to six hoursSkilled Warfighter and Advanced Life Saving (ALS) level
skills to include decompression of tension pneumothorax, chest tubes, oxygen therapy, IV access / fluid resuscitation, antibiotics and advanced airway management.
4. Six hours or moresurgical intervention and additional infection control are
required to show any marked improvements in survival rates beyond the 6-hour mark.
Deployment Medicine International 26
NOTES:
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Deployment Medicine International 27
WAR CASUALTY STATISTICS
In World War II, 30 percent of the Americans injured in combat died. In Vietnam, 24 percent of Americans injured in combat died. In the war in Iraq and Afghanistan, about 10 percent of those injured
have died. Half of battlefield deaths occur within 30 minutes of wounding, largely
on account of blood loss. US forces in OIF/OEF are primarily engaged in counterinsurgency
operations within irregular war, in which enemy tactics are primarily based on terrorism, insurgency and guerilla warfare.
There is no uniformed enemy, no defined front lines or order of battle, and allegiances can be fluid. As a result, most combat casualties occur due to ambush or increasingly from the use of improvised explosive devices (IEDs). IEDs are destructive devices constructed from homemade, commercial, or military explosive material that are deployed in ways other than conventional military means. IEDs are designed to destroy, disfigure, or otherwise interdict military assets in the field and include buried artillery rounds, antipersonnel mines and car bombs.
The number of casualties due to explosives has increased relative to those caused by gunshot.
An analysis of the epidemiology of injuries in OIF/OEF documented that 81% of all injuries were due to explosions. (Reference: LTC Philip et al. Epidemiology of Combat Wounds in Operation Iraqi Freedom and Operation Enduring Freedom: Orthopedic Burden of Disease. Journal of Surgical Orthopedic Advances. 2010 Vol 19:1 pg. 2-7)
The use of body armor by US soldiers provides increased protection to the thorax and to a lesser extent the abdomen and pelvis, and its effects were first observed in Operation Desert Storm, which saw a decline in thoracic injuries to 5% compared to 13% seen in Vietnam. (Reference: Belmont, P.J et al. Incidence and Epidemiology of Combat Injuries Sustained During The Surge Portion of Operation Iraqi Freedom by a U.S.Army Brigade Combat Team. J. Trauma. 2010; 68 p.204-210)
Deployment Medicine International 28
WAR CASUALTY STATISTICS
Current Literature: A study from 2011 looking at 2001-2009 combat statistics shows that 48.6% of mortality secondary to combat wounds was considered
non-survivable. 51.4% of mortality secondary to combat wounds is considered
survivable. 80% of the potentially survivable combat mortalities were
secondary to hemorrhage. Of the hemorrhage related mortalities the major regions affected
were: Torso 48% Extremity 31% Junctional region; neck, armpit and groin. 21%
Total 100%
Non Survivable cases: TBI, 83% Hemorrhage 16% Other causes 1%
Total 100%
(Reference: Eastridge B.J. et al. Died of wounds on the battlefield: causation and implications for improving combat casualty care. J. Trauma 2011;71:S4-S8) See Table 4 and 5 below.
Deployment Medicine International 29
US Military Casualties Data taken from: Defense Casualty Analysis System Website: www.dmdc.osd.mil; access date: 8/1/12
Deployment Medicine International 30
Deployment Medicine International 31
Deployment Medicine International 32
Deployment Medicine International 33
Time Line: Operation Iraqi Freedom, Operation New Dawn and Operation Enduring Freedom
Deployment Medicine International 34
What we have seen is the [Interceptor] Body Armor; particularly
what are called the SAPI plates (small arms protective inserts), the
ceramic material plates that go inside the flack (Kevlar) vest that Marines
wear in the field. It's the standard body armor that is now distributed to
everybody; that plus the Kevlar helmets that everyone wears. The result
has been that there has been a decrease in the number of Marines
wounded in the thorax, in the chest and the abdomen-fewer trunk wounds
because of the protective effects of that body armor. And therefore what
wounds that might previously have penetrated the chest or abdomen and
caused fatal or serious injury is not occurring. And that's led to a shift in
the proportion of casualties that we're seeing with extremity injuries and
with head and face and neck injuries.
Capt. Gerard Cox, MC, USN, Director of Medical Programs
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Deployment Medicine International 35
INTRODUCTION TO COMBAT CASUALTY CARE
These medical concepts are specific to battlefield casualty care:
1. Not civilian (EMS) ambulance or hospital care.
2. Involves a combat situation with the possibility of limited available medical
resources or lengthy evacuation times.
3. Concepts in this environment need to remain simple and oriented toward good
tactics.
4. Process begins with the involvement of the Warfighter.
5. If the process doesnt begin or is delayed, more casualties will die.
The Phases of Combat Casualty Care:
1. Consider the management of casualties that occur during combat missions as being divided into three distinct phases:
2. This approach recognizes a particularly important principle: Perform the
correct intervention at the correct point on the timeline of care.
3. A medically correct intervention at the wrong time in combat may lead to further
casualties, which may be going against good tactics. Remember, the tactical situation always take precedence over the medical situation.
Care Under Fire Tactical Field Care Tactical Evacuation
Deployment Medicine International 36
CARE UNDER FIRE PHASE
1. Care Under Fire is the care rendered by the first responder at the scene of the injury while he and the casualty are still under effective hostile fire. Available medical equipment is limited to that carried by the Warfighter. Typically, equipment is made available in personal cargo pouches or provided to individuals in personal first aid kits.
2. The risk of injury to other personnel and additional injury to the wounded will be
reduced if immediate attention is directed to the suppression of hostile fire.
3. As soon as the Warfighter is able to, keeping the casualty from sustaining
additional injuries is the first major medical objective.
4. Wounded Warfighters who are unable to participate further in the engagement
should lie flat and still if no ground cover is available, or move as quickly as possible if nearby cover is available. If there is no cover and the casualty is unable to move himself to find cover, he should remain motionless on the ground so as not to draw additional fire. A tourniquet that can be applied by the casualty himself is the most reasonable initial choice to stop major bleeding.
Deployment Medicine International 37
Basic Management Plan for Care Under Fire
1. Return fire and take cover. 2. Direct or expect casualty to remain engaged as a
combatant if appropriate. 3. Direct casualty to move to cover and start self-aid if
able. 4. Try to keep the casualty from sustaining additional
wounds. 5. Casualties should be extricated from burning
vehicles or buildings and moved to places of relative safety. Do what is necessary to stop the burning process.
6. Airway management is generally best deferred until the Tactical Field Care phase.
7. Stop life-threatening external hemorrhage if tactically feasible: Direct casualty to control hemorrhage by self-aid
if able. Use of CoTCCC recommended tourniquet for
hemorrhage that is anatomically amenable to tourniquet application.
Apply the tourniquet proximal to the bleeding site, over the uniform, tighten, and move the casualty to cover.
PHTLS Military Manual Version Seven, Figure 25-1, Page 600
Deployment Medicine International 38
CASUALTY MOBILITY
Casualty mobility is of the utmost importance in the Care Under Fire phase of care. Casualty drag maneuvers, hasty litters, and drag straps should be used, when needed to rapidly and safely move a casualty to cover and concealment. It is imperative that deploying units integrate casualty mobility exercises into their pre-deployment training. Consider the benefits and limitations of rigid litters during this phase of casualty care.
Casualty Movement Methods
1. Immobilize casualty a. Default Drag: Grab any available equipment point b. Wheelbarrow Drag: Grab both feet facing away from casualty c. Two Person Drag: Each individual grabs a shoulder strap d. Drag Strap: Attach a tubular nylon strap to the casualty with a D-ring e. Multiple Rescuer Carry: Requires minimum of three persons to pick up
casualty at waist 2. Semi-Mobile Casualty
a. Assisted walk: Place the casualty over shoulder and bear the weight of the injured casualty while moving
b. Firemans Carry: Pick up casualty and carry over shoulder (REQUIRES CASUALTY TO ASSIST)
Deployment Medicine International 39
CONSIDERATIONS:
1. Understand that various situations will call for different movement techniques.
2. Casualty condition, terrain, available equipment and combat situation will all
play a part in which casualty movement method is used
3. Train on all movement techniques prior to deployment
4. Casualty movement SOPs should focus on simple and reproducible methods
that requires a minimal amount of specialty equipment.
NOTES:
Deployment Medicine International 40
CASUALTY MOBILITY DEVICES: TALON II LITTER
FOXTROT LITTER
Deployment Medicine International 41
TACTICAL FIELD CARE PHASE
1. Tactical Field Care is the care rendered by the first responder or medic once he
and the casualty are no longer under effective hostile fire. It also applies to
situations in which an injury has occurred, but there has been no hostility.
Available medical equipment is limited to that carried into the field by the team.
Timeline during this phase may vary from a few moments to many hours.
2. This period may consist of only a short opportunity to assess and treat life-
threatening problems due to the need to re-engage threat or it may allow for long
period of casualty management.
3. Tactics, situation and evacuation time will determine the available timeframe.
Deployment Medicine International 42
a. With casualty behind cover/concealment perform an examination of the
casualty and determine the severity of the injuries (See Casualty
Assessment M.A.R.C.H.)
b. Apply the interventions you have been taught and do so knowing that
your situation can quickly change back to Care Under Fire.
c. Be prepared to move and continually communicate with your team.
d. Be aware of your tactical situation.
e. Use your skill and know your time limitations.
f. Get some help!
g. Initiate a TACEVAC request as soon as possible.
4. Take care to reassess earlier interventions:
a. After major movements
b. After re-engaging a threat
c. As soon and as often as the situation allows
d. Go back and look at the interventions you performed while you were under
fire. These actions were performed quickly and may not have been
effective or will not remain effective.
5. Assess the casualty in M.A.R.C.H. order:
Deployment Medicine International 43
a. It is essential to maintain strict adherence to the M.A.R.C.H. algorithm in
this phase of care.
b. As listed above, this phase of care may be short or long in duration. If
wounds are treated out of sequence, life-threatening wounds may remain
untreated prior to TACEVAC.
6. Packaging the casualty for movement or evacuation:
a. The casualty will need to be packaged for protection and evacuation.
Special care will be required when dealing with casualties that are no
longer awake or might lose consciousness during transport or evacuation.
b. Dust and debris during helicopter transport is expected.
c. Casualties that have lost a lot of blood are at risk for hypothermia.
d. Ensure they are covered and kept war.
e. If you are wearing ear protection then you should provide it for your
casualty.
f. Secure arms and legs as necessary-they tend to fall off stretchers during
movement and get banged up during loading casualties on helicopters
and in vehicles.
g. Do not cause further injury!
Deployment Medicine International 44
7. Document the casualtys condition and treatments: Fill out the TCCC
(recommended) Casualty Card (DA Form 7656), or assign a person to do
it for you.
8. PHTLS 7th edition Figure 26-17 pg 633
Deployment Medicine International 45
9. Prepare for casualty turnover.
a. Complete an A.T.M.I.S.T. report
i. The A.T.M.I.S.T report is an organized method of turning over
essential casualty information to receiving TACEVAC personnel
and receiving treatment facility.
b. The goal of the A.T.M.I.S.T report is to be organized and concise. This is
essential when turning over casualties to TACEVAC personnel in the
noisy environment of a Landing Zone.
c. Many units also use the A.T.M.I.S.T approach when passing casualty
information over the radio.
10. The A.T.M.I.S.T. report:
Deployment Medicine International 46
A Age
T Time of Injury
M Mechanism of Injury Examples: Gunshot wound, Blast, Motor Vehicle acciden, blunt trauma, fall
I Injuries Sustained
S Signs and Symptoms Respiratory rate, pulse rate, casualty feedback
T Treatments Describe what you have done and what time the procedure was done
Organize to M.A.R.C.H or head to toe
Deployment Medicine International 47
Basic Management Plan for Tactical Field Care 1. Casualties with an altered mental status should be
disarmed immediately. 2. Airway Management
a. Unconscious casualty without airway obstruction: Chin lift or jaw thrust maneuver Nasopharyngeal airway Place casualty in recovery position
b. Casualty with airway obstruction or impending airway obstruction: Chin lift or jaw thrust maneuver Nasopharyngeal airway Allow casualty to assume any position that
best protects the airway, to include sitting up.
Place unconscious casualty in the recovery position.
If previous measures unsuccessful: Surgical Cricothyroidotomy (with
lidocaine if conscious) 3. Breathing
a. In a casualty with progressive respiratory distress and known or suspected torso trauma, consider a tension pneumothorax and decompress the chest on the side of the injury with a 14-gauge, 3.25 inch needle/catheter unit inserted in the second intercostal space at the midclavicular line. Ensure that the needle entry into the chest is not medial to the nipple line and is not directed towards the heart.
b. All open and/or sucking chest wounds should be treated by immediately applying an occlusive material to cover the defect and securing it in place. Monitor the casualty for the potential development of a subsequent tension pneumothorax.
4. Bleeding a. Assess for unrecognized hemorrhage and
control all sources of bleeding. If not already done, use a CoTCCC-recommended tourniquet application or for any traumatic amputation. Apply directly to the skin 2-3 inches above wound.
b. For compressible hemorrhage not amenable to tourniquet use or as an adjunct to tourniquet removal (if evacuation time is anticipated to be longer than 2 hours), use Combat Gauze as the hemostatic agent of choice. Combat Gauze should be applied with at least 3 minutes of direct pressure. Before releasing any tourniquet on a casualty who has been resuscitated for hemorrhagic shock, ensure a positive response to resuscitation efforts (i.e., a peripheral pulse normal in character and normal mentation of there is no traumatic brain injury (TBI).
c. Reassess prior tourniquet application. Expose
wound and determine if tourniquet is needed. If so, move tourniquet from over uniform and apply directly to skin 2-3 inches above wound. If tourniquet is not needed, use other techniques to control bleeding.
d. When time and the tactical situation permit, a distal pulse check should be accomplished. If a distal pulse is still present, consider additional tightening of the tourniquet or the use of a second tourniquet, side-by-side and proximal to the first, to eliminate the distal pulse.
e. Expose and clearly mark all tourniquet sites with the time of tourniquet application. Use an indelible marker.
5. Intravenous (IV) access Start an 18-gauge IV or saline lock if
indicated. If resuscitation is required and IV access is
not obtainable, use the Intraosseous (IO) route.
6. Fluid resuscitation Assess for hemorrhagic shock. Altered mental status (in the absence of head injury) and weak or absent peripheral pulses are the best field indicators of shock. a. If not in shock:
NO IV fluids necessary PO fluids permissible if casualty is
conscious and can swallow b. If in shock:
Hextend, 500-ml IV bolus Repeat once after 30 minutes if still in
shock. No more than 1000 ml of Hextend
c. Continued efforts to resuscitate must be weighed against logistical and tactical considerations and the risk of incurring further casualties.
d. If a casualty with TBI is unconscious and has no peripheral pulse, resuscitate to restore the radial pulse.
7. Prevention of hypothermia a. Minimize casualtys exposure to the elements.
Keep protective gear on or with the casualty if feasible.
b. Replace wet clothing with dry if possible. c. Apply Ready-Heat blanket to torso. d. Wrap in Blizzard survival blanket. e. Put Thermo-Lite Hypothermia Prevention
System cap on the casualtys head, under the helmet.
f. Apply additional interventions as needed and available.
g. If mentioned gear is not available, use dry blankets, poncho liners, sleeping bags, body bags, or anything that will retain heat and keep the casualty dry.
Deployment Medicine International 48
Basic Management Plan for Tactical Field Care (Cont) 8. Penetrating Eye Trauma
If a penetrating eye injury is noted or suspected: a. Perform a rapid field test of visual acuity. b. Cover the eye with a rigid eye shield (NOT a
pressure patch). c. Ensure that the 400 mg moxifloxacin tablet in
the combat pill pack is taken, if possible, or that IV/IM antibiotics are given as outlined below if oral moxifloxacin cannot be taken.
9. Monitoring Pulse oximetry should be available as an adjunct to clinical monitoring. Note: Readings may be misleading in the settings of shock or marked hypothermia.
10. Inspect and dress known wounds. 11. Check for additional wounds. 12. Provide analgesia as necessary.
a. Able to fight: Note: These medications should be carried by the combatant and self-administered as soon as possible after the wound is sustained. Mobic, 15 mg PO once a day Tylenol, 650-mg bilayer caplet, 2 PO every
8 hours b. Unable to fight:
Note: Have naloxone readily available whenever administering opiates. Does not otherwise require IV/IO access:
Oral transmucosal fentanyl citrate (OTFC), 800 mcg transbuccally (a) Recommend taping lozenge-on-a-
stick to casualtys finger as an added safety measure
(b) Reassess in 15 minutes (c) Add second lozenge, in other
cheek, as necessary to control sever pain.
(d) Monitor for respiratory depression. IV or IO access obtained:
Morphine sulfate, 5 mg IV/IO Reassess in 10 minutes. Repeat dose every 10 minutes as
necessary to control severe pain. Monitor for respiratory depression Promethazine, 25 mg IV/IM/IO every 6
hours as needed for nausea or for synergistic analgesic effect
13. Splint fractures and recheck pulses. 14. Antibiotics (recommended for all open combat
wounds): a. If able to take PO:
Moxifloxacin, 400 mg PO once a day b. If unable to take PO (shock, unconsciousness):
Cefotetan, 2 g IV (slow push over 3-5 minutes) or IM every 12 hours, or
Ertapenem, 1 g IV/IM once a day
15. Burns*
a. Facial burns, especially those that occur in closed spaces, may be associated with inhalation injury. Aggressively monitor airway status and oxygen saturation is such patients and consider early surgical airway for respiratory distress or oxygen desaturation.
b. Estimate total body surface area (TBSA) burned to the nearest 10% using the Rule of Nines.
c. Cover the burn area with dry, sterile dressings. For extensive burns (>20%), consider placing the casualty in the Blizzard survival blanket in the hypothermia prevention kit in order to both cover the burned areas and prevent hypothermia.
d. Fluid resuscitation (USAISR Rule of Ten): If burns are greater than 20% of Total body
Surface Area, fluid resuscitation should be initiated as soon as IV/IO access is established. Resuscitation should be initiated with Lactated Ringers, normal saline, or Hextend. If Hextend is used, no more than 1000 ml should be given, followed by Lactated Ringers or normal saline as needed.
Initial IV/IO fluid rate is calculated as %TBSA x 10 ml/hour for adults weighing 40-80 kg, increase initial rate by 100 ml/hour.
If hemorrhagic shock is also present, resuscitation for hemorrhagic shock takes precedence over resuscitation for burn shock. Administer IV/IO fluids per the TCCC Guidelines in Section 6.
e. Analgesia is accordance with TCCC Guidelines in Section 12 may be administered to treat burn pain.
f. Pre-hospital antibiotic therapy is not indicated solely for burns, but antibiotics should be given per TCCC guidelines in Section 14 if indicated to prevent infection in penetrating wounds.
g. All TCCC interventions can be performed on or through burned skin in a burn casualty.
16. Communicate with the casualty if possible. Encourage: reassure Explain care
17. Cardiopulmonary resuscitation (CPR) Resuscitation on the battlefield for victims of blast or penetrating trauma who have no pulse, no ventilations, and no other signs of life will be successful and should not be attempted.
18. Documentation of Care Document clinical assessments, treatments rendered, and changes in the casualtys status on a TCCC Casualty Card. Forward this information with the casualty to the next level of care.
PHTLS Military Manual Version Seven, Figure 26-1, Page 613-614
Deployment Medicine International 49
TACTICAL FIELD CARE
REASSESS
After major movements
As often as possible
After engaging any
threats
Any interventions performed under =ire
Deployment Medicine International 50
TACTICAL EVACUATION CARE
TRAINING OBJECTIVE:
1. Define the Warfighters role in the casualty evacuation phase of combat casualty
care.
2. Explain the importance of initiating a 9-Line.
3. Explain the importance of communication in combat casualty care.
4. Define what information is essential to CASEVAC/MEDEVAC initiation.
5. Explain the principles of managing a casualty collection point.
6. Define triage in modern combat casualty care.
7. Explain considerations unique to CASEVAC/MEDEVAC.
8. Explain proper casualty movement procedures.
9. Explain the considerations associated with the various platforms used in casualty
evacuation.
10. Answer all remaining questions regarding casualty evacuation in combat casualty
care
Deployment Medicine International 51
TACTICAL EVACUATION CARE
1. Combat Tactical Evacuation Care is the care rendered once an aircraft, vehicle
or boat has picked up the casualty.
2. Additional medical personnel and equipment may be available at this stage of
care, which may allow more advanced medical procedures to be performed.
3. Initiate TACEVAC early and with good information.
4. You are responsible for your casualty until you are not.
5. It is also always a good idea to preposition medical supplies if possible. You can
store them in vehicles or other strategic places in case you need them later. This
Deployment Medicine International 52
will allow you to have a cache of medical supplies that are too bulky or heavy for
individuals to be carrying, but are nearby if and when you need them.
CONSIDERATIONS:
1. Standard litters for patient evacuation may not be available for movement of
casualties in the care under fire phase. Consider alternate methods of patient
movement (e.g. dragging the casualty by the web gear or using ponchos, etc.).
2. Keep in mind that if you and the receiving aircraft or vehicle doesnt have the
necessary litters for all of your patients, you can floor load the patients and
secure them with cargo straps. Always defer to the direction of the flight crews
who will guide you in all patients loading and unloading.
3. Consider the use of obscurants (such as smoke) to assist in casualty movement.
4. Vehicles can also be used as shields during evacuation attempts.
5. Once the patient has been transported to the site where evacuation is
anticipated, consider loosening or removing tourniquets and using direct
pressure or direct pressure with hemostatic agents to control bleeding if the
tactical situation allows.
6. Vehicles (ground and air) present unique difficulties with ongoing patient
assessment. In the back of a noisy, dark, turbulent, and windy helicopter, it can
be impossible to perform a basic assessment (e.g. you can only feel for
respirations with a hand on the chest.
7. A patient with a wound that is not properly controlled can bleed in the back of a
Deployment Medicine International 53
dark vehicle without the medical providers knowledge. It is imperative that all
bleeding is absolutely controlled prior to transport.
8. Another consideration of vehicle transport is the threat of hypothermia. In rotary
winged assets you must deal with colder temperatures and high winds
associated with these assets. You must take great care to ensure your patients
are packaged warmly and appropriately.
9. Lastly, remember that more than likely there will be a limited number of medical
providers in any one particular vehicle or asset. You should ensure that as much
medical gear as possible has been given prior to transport. For instance, if there
is one medical provider in the back of a helicopter and he must provide
ventilations for one of the patients, it will be impossible for him to care for and
assess the other patients that are on board. The non-medic may need to
accompany the patient(s) so the medical provider can care for all of the patients.
10. The final phase of casualty care can be the most problematic. Casualties require
a lot of effort to prepare for transport. Insurgent attacks on advanced medical
providers and the vehicles that are utilized are common. If your casualties
require transport by helicopter you must consider the likelihood of an attack
during evacuation. Prior to evacuating your patients, secure a safe landing zone
or extraction point. Establish good communications with the incoming unit(s) and
update them if and when the situation changes.
Deployment Medicine International 54
INITIATING CASUALTY EVACUATION: .
1. Initiate early. Per the usual operational SOP, only the first three lines of the 9-line
are required to initiate TACEVAC/CASEVAC. Ensure that this information is available as early as possible.
2. Update the evacuation asset and Command & Control (C2) as the injuries and
situation are better understood or change.
3. Carry a 9-Line request card on your person.
4. Relay: Who, What, When, Where, Why and How many
ACTIONS REQUIRED PRIOR TO CASUALTY EVACUATION:
1. Control bleeding (Have a plan to do so throughout transport).
2. Airway Management (Have a plan for managing the casualtys airway throughout
transport).
3. Ensure respiration assessment is conducted for presence of tension
pneumothorax (See Respiration section).
4. Reassess M.A.R.C.H.
5. Prepare A.T.M.I.S.T. report for each casualty
Age
Time of injury
Mechanism of Injury
Injuries
Signs & Symptoms
Treatments
Deployment Medicine International 55
6. Reassess earlier interventions
7. Casualty eye/ear protection
8. Cross-load mission essential gear
9. Treat for hypothermia
10. Provide pain management as necessary (see page 111 for TCCC update)
ADDITIONAL CONSIDERATIONS:
1. Store bulky or heavy equipment and supplies in vehicles and evacuation assets.
These items may include:
Oxygen
Mass casualty kits
High angle rescue equipment
Vehicle extrication equipment
M.A.S.T. pants
Femur traction splint
Ice packs
Cervical collars
Hypothermia Prevention and Burn blankets
Deployment Medicine International 56
EVACUATION PLATFORM CONSIDERATIONS:
1. Ground or Air
2. Number of casualties/condition asset that evacuation assets/s can be taken.
3. Know the medical plan for turning casualties over.
4. Space Available.
5. Different platforms have different passenger ingress routes.
6. Always follow crew chief or flight medics instructions for loading the aircraft.
7. Situational awareness, i.e. landing zone selection, safety, etc.
ENROUTE TREATMENT CONSIDERATIONS:
1. Consider the use of NVG (Night Vision Goggle) compatible lights.
2. Senses may be impaired (wind, turbulent, darkness, etc.) Learn to use feel
instead of listen techniques
3. Not all platforms have a dedicated TACEVAC/CASEVAC medic; you may
become the TACEVAC/CASEVAC medical provider needed to assist.
4. Have all the kit you will need for the flight (plan ahead in case of flight delays).
Deployment Medicine International 57
COMBAT CASUALTY TRIAGE
1. The following is one of many triage systems.
2. Your medical control and casualty evacuation system must support this
system prior to using it.
TRIAGE PRINCIPLES:
1. Do the greatest good for the greatest number of casualties.
2. Employ the available resources in the most efficient way.
3. Triage does not stop, it only repeats.
1. 4. Current triage concepts focus on establishing casualty treatment and
evacuation priority.
4. Focus on updating the Command & Control (C2) element in real time.
5. Plan, prepare and train for triage situations.
TRIAGE CONSIDERATIONS:
1. 1.Triage should: a. Be used when the number of casualties overwhelms the
medical treatment capabilities, not when medical treatment providers are not comfortable with the number of casualties.
b. Casualties may be neglected in mass casualty situations.
2. All the casualties will be treated. Triage is focused on the order and priority of
treatment, not which casualties will receive treatment. The exception is casualties with wounds incompatible with life and those showing no signs of life.
3. Utilize ALL available personnel not currently involved in security operations or
Command & control (C2) efforts.
Deployment Medicine International 58
4. Take into account resupply assets when making decisions regarding how many
medical supplies to use.
TRIAGE CATEGORIES:
1. Immediate: Casualties with high chances of survival who require life-saving surgical procedures or medical care.
2. Delayed: Casualties who require surgery or medical care, but whose general
condition permits a delay in treatment without unduly endangering the casualty.
3. Minimal: Casualties who have relatively minor injuries or illnesses and can
effectively care for themselves or be helped by non-medical personnel.
4. Expectant: Casualties with wounds so extensive that even with the benefit of
optimal medical resource application, their survival is unlikely.
CASUALTY COLLECTION POINT OPERATIONS
1. Ensure area is secure.
2. Place all casualties in a manageable configuration. See the Tactical Field Care
section for diagram.
3. Consolidate medical supplies.
4. Triage; Number, Severity, Supplies
5. Ensure Command and control (C2) group is given current reports of casualty
conditions and triage status.
6. Your entire team must understand the principles of CCP operations and the
correct configuration of casualties and resources.
Deployment Medicine International 59
NOTES:
Deployment Medicine International 60
CASUALTY COLLECTION POINT CONFIGURATIONS:
1. TRIANGLE CONFIGURATION a. Beneficial to distribution of medical supplies and information. b. Arguable more tactically sound than other methods c. Casualties should be placed with their heads pointed to the center of the
triangle for easy assessment of their airways.
Deployment Medicine International 61
2. LINEAR CONFIGURATION a. Easy to organize b. Allows for easiest priority of movement to TACEVAC/CASEVAC
Deployment Medicine International 62
HEMORRHAGE CONTROL
TRAINING OBJECTIVES:
1. Explain the importance of hemorrhage control in combat casualty care.
2. Define the Warfighters role in hemorrhage control.
3. Describe hemorrhage control concepts.
4. Describe and demonstrate proper direct pressure application.
5. Explain current tourniquet application concepts.
6. Demonstrate the application of tourniquets in DOD circulation.
7. Perform tourniquet practical application lab.
8. Explain correct application of gauze in combat wounds.
9. Demonstrate the application of pressure dressings in DOD circulation.
Deployment Medicine International 63
10. Perform pressure dressing practical application lab.
11. Define hemostatic agent application criteria.
12. Explain the process of applying hemostatic agents.
13. Define hemostatic agent re-application criteria.
14. Explain post application management of wounds treated with hemostatic
agents.
15. Answer all remaining questions regarding hemorrhage control in combat
casualty care.
Deployment Medicine International 64
HEMORRHAGE CONTROL METHODS
PRIMARY METHODS:
1. Direct Pressure
2. Tourniquets
3. Wound Packing
4. Hemostatic Agent
5. Pressure Dressing
ADJUNCT METHODS: (Not definitive, makes your primary interventions more effective).
1. Indirect pressure
a. Leg pressure points.
b. Arm pressure points.
2. Elevation
3. Anatomical/Rigid Splinting
NOTES:
Deployment Medicine International 65
DIRECT PRESSURE
THE GOAL OF DIRECT PRESSURE TO COMPRESS THE BLEEDING VESSEL
AGAINST THE BONE
CONSIDERATIONS FOR DIRECT PRESSURE:
1. Direct pressure is the usual initial control measure for hemorrhage. Your first response in most settings is direct pressure. While the tourniquet is being retrieved from its storage location-apply direct pressure to the wound to control the bleeding. Use gauze, a blouse or anything that will assist you in applying direct pressure. If the wound requires the application of a hemostatic agent, apply direct pressure while you locate the agent and prepare to apply it. Time is critical and the tactical situation always takes precedence over the medical situation. Apply direct pressure while assessing the situation and decide the correct course of action.
2. Palm pressure as opposed to Finger Tip pressure:
a. Diffuse pressure is key, no artery hunting with fingertips.
b. More effective due to the surface area covered.
c. Allows for greater pressure to be applied.
d. Can be maintained for long periods.
e. Fingertip pressure does not provide full contact with wound.
3. Body position is important
a. Arms are straight to reduce fatigue.
b. Shoulders are directly over the wound.
Deployment Medicine International 66
c. Full body weight is required to compress an arterial injury.
4. Packing material is packed into the wound to assist direct pressure.
a. Packing material means gauze, other bandage material or clothing in a
resource limited environment.
b. Packing material allows for more pressure into the wound.
c. Packing material must be in full contact with the wound site to be effective.
5. Hemostatic agents increase the effectiveness of direct pressure, but direct pressure is critical for the success of hemostatic agents.
6. Direct pressure requires the ground or another hard surface under the casualty
for counter pressure
7. Direct pressure must be dedicated.
a. Do not remove direct pressure to assess the wound. This will invite re-
bleeding. Re-bleeding can be fatal.
b. When transitioning to a pressure bandage, do not release pressure from
the wound.
8. Kneeling on wound site in extreme situations.
a. A knee may be effective if gauze allows transmission of pressure to wound.
Deployment Medicine International 67
NOTES:
Deployment Medicine International 68
TOURNIQUETS
Extremity Bleeding
1. One of the first considerations for bleeding control
a. The amount of blood loss is an important factor in patients survival, in the
absence of unlimited medical resources (blood, I.V. Fluids, etc.) and the length of time before the patient will receive definitive treatment
b. The first choice during CARE UNDER FIRE PHASE
c. A bleeding wound requires pressure enough to block the arteries.
d. Tactical situation requires immediate management of blood loss to ensure
the best outcome for the casualty.
2. Lessons from OEF/OIF indicate the use of tourniquets provides better outcome
for casualties.
a. Quickest and easiest way to control extremity hemorrhage
b. Should be used on bleeding extremities initially
NOTES:
Deployment Medicine International 69
Figure 26-4 PHTLS Manual 7th Edition pg. 619
FIGURE 26-4 Tourniquet Tips POINTS TO REMEMBER
Damage to the arm or leg is rare if the tourniquet is left on less than 2 hours
Tourniquets are often left in place for several hours during surgical procedures
In the face of massive extremity hemorrhage, it is better to accept the small risk of damage to the limb than to allow a casualty to bleed to death.
SIX MAJOR TOURNIQUET MISTAKES 1. Not using the tourniquet when it should be used 2. Using a tourniquet when it should not be used 3. Putting the tourniquet on too proximally 4. Not tightening the tourniquet well enough 5. Not taking the tourniquet off when possible 6. Periodically loosening the tourniquet to allow intermittent
blood flow DEATH FROM EXANGUINATION How long does it take to bleed to death from a complete femoral artery and vein disruption? Casualties with such an injury are likely to die in about 10 minutes, but some will bleed to death in as little as 3 minutes. TOURNIQUET APPLICATION
1. Apply without delay for life-threatening bleeding in the Care under Fire phase
Both the casualty and the corpsmen/medic are in serious danger while a tourniquet is being applied in this phase
The decision regarding the relative risk of further injury versus that of bleeding to death must be made by the person rendering care
NOTE: The life-saving benefit of a tourniquet is far more pronounced when the tourniquet is applied BEFORE the casualty
Deployment Medicine International 70
has gone into shock from his wound. 2. Non-life-threatening bleeding should be ignored until the
Tactical Field Care phase 3. Apply proximal to the site of hemorrhage over the uniform
during Care Under Fire 4. Tighten the tourniquet until bleeding stops 5. During Tactical Field Care, expose the wound and reapply the
tourniquet directly to the skin 2-3 inches above the bleeding site
6. Check for distal pulse 7. Tighten the tourniquet or apply a second tourniquet side-by-
side and just proximal to the first as needed to eliminate the distal pulse
8. Note the time of tourniquet application REMOVING THE TOURNIQUET
Remove as soon as direct pressure or hemostatic dressings become feasible and effective, unless the casualty is in shock or the tourniquet has been on for more than 6 hours
Only a combat medic, or physicians assistant, or a physician should remove the tourniquets
Do not remove tourniquet if the distal extremity is gone Do not attempt to remove the tourniquet if the casualty will
arrive at a hospital in 2 hours or less after application TECHNIQUE FOR REMOVAL
1. Apply Combat Gauze as per instructions 2. Loosen the tourniquet 3. Apply direct pressure for 3 minutes 4. Check for bleeding 5. If no bleeding, apply pressure dressing over the Combat
Gauze 6. Leave tourniquet in place but loose 7. Monitor for bleeding from underneath the pressure dressings 8. If bleeding does not remain controlled, retighten tourniquet,
remove dressings, and expedite evacuation
Deployment Medicine International 71
TOURNIQUET APPLICATION:
1. Ensure tourniquet is as tight as possible prior to engaging the windlass or other
mechanical system.
2. The common problem with tourniquet application is OIF/OEF is that they are not
tight enough.
3. Ensure the tourniquet is secured after it is tightened.
4. The tourniquet should ideally be applied directly to the skin. Remove the uniform
if possible.
5. Use two if necessary:
a. The second tourniquet should ideally be applied above the first if possible.
6. Mark the tourniquet (Time of placement)
NOTES:
Deployment Medicine International 72
STATISTICS ON TOURNIQUET USE Kragh 2009
91% of tourniquet use in Baghdad was 2 hours or less with low risk of
complications.
Kragh 2008 Baghdad Combat Support hospital)
85% of battle casualties with (one or more) tourniquets had the device applied
before arrival to a facility (prehospital tourniquet)
15% had their first tourniquet applied in the hospital.
Kragh 2009
232 patients; 428 tourniquets were used on 300 limbs
31 of these died due to primary injury; secondary was hemorrhage with no
deaths attributed to tourniquet use
10 patients had tourniquet use AFTER shock and 9 died
222 patients had tourniquets used BEFORE shock and 22 died
No amputations were solely due to tourniquet use
40% of Tourniquets placed pre-hospital are NOT MARKED
Kragh 2011
The pressure in or under the tourniquet is not the key to optimal use.
The key to effectiveness is the occluding the artery,
Users often assume that optimal use requires more force, but optimal use is not
synonymous with effective use; optimal use must include safe use.
More force was associated with misuse.
Deployment Medicine International 73
IDEAL EMERGENCY TOURNIQUET TRAITS TRAIT IDEAL Effective Stops distal pulse Use width Wide compression Length Fits casualty Use ease Simple to apply Weight Low carry weight Tactical use Care under fire Cost Inexpensive Torque control User can limit force Size small volume Application speed don quickly Self-application casualty dons on and off Open-ended design can route proximal Don single handedly single-handed Toughness wears little in use Doff emergently rapid removal Stable stays effective Mechanics internal capacity Power twist or pump Placement stays put Multisetting field to hospital Replacement can don again Repair ease few repairs needed Cleaning ease washes quickly Storage cube stores densely Storage life shelf life>10 years Safety safe use limit Safe pressure manometer Monitors pressure, timer Conformity kept maintains shape Rugged materials field ready User expectations preconceptions met Abridged from Kragh JF. The military emergency tourniquet program's lessons learned with devices and designs. Mil Med 176:1144 (2011) Table III. Ideal Emergency Tourniquet Traits
Deployment Medicine International 74
TOURNIQUET REASSESSMENT:
1. Tourniquets applied in the combat environment may become ineffective after the
initial success due to:
a. Casualty movement
b. Shifting of the tourniquet due to placement over uniform
c. Anatomical changes in the shape of the extremity due to movement
d. Physiological changes in the casualty as a result of I.V. fluid treatments
e. Removal or loosening of the tourniquet by the casualty due to pain
2. Reassess the wound for re-bleeding:
a. After making movement
b. After rolling the casualty
c. After engaging an enemy threat
d. After augmenting the casualtys circulatory volume
e. As often as possible
Deployment Medicine International 75
PAIN CONSIDERATIONS:
1. Tourniquets are painful when applied
a. When properly applied, a tourniquet can cause more pain than the wound.
b. Casualties with tourniquets applied may beg for the tourniquet to be
removed or attempt to remove it themselves.
c. Tourniquets become more painful over time (ischemia sets in
approximately 20 minutes after application). Pain management considerations should take into account this anticipated tourniquet pain.
d. Reassurance and pain management is important.
NOTES:
Deployment Medicine International 76
TOURNIQUET REMOVAL The decision to remove a tourniquet should be made by a medical provider PICKING THE RIGHT TOURNIQUET:
1. Types of Tourniquets:
a. Mechanical
b. Windlass
c. Pneumatic
d. Other
2. Combat Effective Tourniquet Criteria:
a. Must STOP arterial blood flow in the lower extremities.
b. You must be able to self-apply the tourniquet.
c. Incremental (ratcheting) adjustment to increase pressure or decrease
pressure.
3. Should be tested and approved by medical control.
NOTES:
Deployment Medicine International 77
TOURNIQUETS
CoTCCC Approved
1. Combat Application Tourniquet (C-A-T): wide strap with Velcro and stick for windlass
C-A-T Generation 6
Emergency Tourniquet Program
example, the inner strap folds went clockwise or counterclock-wise depending on the direction of hand twisting of the wind-lass (plastic rod of glass-reinforced nylon with a chamferedslot passing the inner strap). More importantly, when the CATwas applied loosely (not enough slack was taken out) beforewindlass twisting began, too many twists of the windlass wereneeded (>540, one twist was 180) to take in the slack beforecompressing the limb. Such loosely applied devices had to beovertwisted since hemorrhage was not controlled with fewertwists and the device rolled in the direction of twisting (Fig, 2),As roll progressed, the windlass and its slot became perpen-dicular to the pull of the inner strap instead of being parallel asit was before twisting. Roll then put the windlass at a structuraland mechanical disadvantage as less than half of the windlassdiameter resisted torque instead of the whole. This phenom-enon was observed in care, and direct feedback for complyingwith the instructions to remove slack before twisting the wind-lass minimized roll and improved results. Noncompliance ledto device deformation, breakage, and ineffectiveness. Most(63%, 61/97) CAT windlass rods had a craze, a fine crack,at the chamfered slot; and this undisplaced crack occurredonly at one spot,
Deployment Medicine International 78
C-A-T before (LEFT) and after (RIGHT) twisting
C-A-T after use and windless pieces after breakage
2. SOF-T Tourniquet: No Velcro, Strap with screw to prevent release and aluminum bar for windlass.
Emergency Tourniquet Program
example, the inner strap folds went clockwise or counterclock-wise depending on the direction of hand twisting of the wind-lass (plastic rod of glass-reinforced nylon with a chamferedslot passing the inner strap). More importantly, when the CATwas applied loosely (not enough slack was taken out) beforewindlass twisting began, too many twists of the windlass wereneeded (>540, one twist was 180) to take in the slack beforecompressing the limb. Such loosely applied devices had to beovertwisted since hemorrhage was not controlled with fewertwists and the device rolled in the direction of twisting (Fig, 2),As roll progressed, the windlass and its slot became perpen-dicular to the pull of the inner strap instead of being parallel asit was before twisting. Roll then put the windlass at a structuraland mechanical disadvantage as less than half of the windlassdiameter resisted torque instead of the whole. This phenom-enon was observed in care, and direct feedback for complyingwith the instructions to remove slack before twisting the wind-lass minimized roll and improved results. Noncompliance ledto device deformation, breakage, and ineffectiveness. Most(63%, 61/97) CAT windlass rods had a craze, a fine crack,at the chamfered slot; and this undisplaced crack occurredonly at one spot,
Deployment Medicine International 79
TOURNIQUETS SUMMARY:
1. In Care Under Fire apply tourniquet on extremity as close to torso as possible
2. Apply it tight
3. Reassess often
4. Ensure that any tourniquet that you or your team carries is approved by your
medical control.
5. Learn how it is used-train frequently.
a. Train your team: Ensure everyone you deploy with or work with knows
how to use your type of tourniquet and you know how to use his or hers.
b. Practice using it
1. -One hand application 2. -Two hand application 3. -Upper extremity 4. -Lower extremity 5. -Under light conditions 6. -Under no-light conditions.
ii. Know how to use it----absolutely.
6. Carry it with you-all the time-and carry more than one.
2. 7. C-A-T shown to be the safest and most effective tourniquet and requires
30% less pressure to achieve successful occlusion of the blood flow, which means that the C-A-T is not only more effective, but also less likely to cause permanent nerve damage, faciotomies, an amputation or blood clots. (Kragh JF. The military emergency tourniquet program's lessons learned with devices and designs. Mil Med 176:1144 (2011). C-A-T has been recommended as the
Deployment Medicine International 80
primary battlefield tourniquet by US Army Institute of Surgical Research (USAISR) and TCCC Committee
NOTES:
Deployment Medicine International 81
WOUND PACKING THE GOAL OF WOUND PACKING:
1. Wound packing transmits pressure to the source of the bleeding.
2. Maintain the pressure that wound packing provides.
a. Maintaining pressure on the source of bleeding while packing the wound is
of critical importance.
b. This is accomplished by performing a one for one placement of pressure
while packing. This means that prior to removing pressure from one hand,
there must be pressure in place from the opposite hand
3. Pack out the entire wound.
a. Emphasis should be placed on directing pressure to the source of
bleeding and then to the sides of the wound.
4. Pack to the bone:
a. In many cases, it is very difficult to find the source of the bleeding.
b. Default to packing to the bone.
c. Large arteries lay close to large bone structures.
Deployment Medicine International 82
FEMORAL INJURY
Deployment Medicine International 83
WOUND PACKING MATERIAL:
1. Gauze: a. Gauze is used as the primary packing material because of its surface area
and ability to conform to wound created by high velocity weapons.
b. By filling and conforming to the wound, gauze allows for better application
of pressure to the source of bleeding.
c. Applying gauze to a wound without a source of pressure is nothing more
than wound decoration and will not result in hemorrhage control.
2. Tampons: a. A tampon will not conform to the inner surface of a ballistic wound.
3. Miscellaneous Material:
a. If no gauze is available, other material may be used to include uniforms and elastic bandaging material.
Deployment Medicine International 84
PRESSURE DRESSINGS
1. Definition of Dressings
a. Gauze with a means to hold itself in place. b. Dressings are more absorbent and provide better protection to wounds
than just gauze. c. Reasonable answer as the only intervention for minor wounds left over
after addressing massive bleeding.
2. Definition of Pressure Dressings:
a. Includes elastic material, which allows the dressing to hold a pressure
load. b. Allows for application of increased pressure to the wound site. c. Maintains long-term direct pressure at the wound site in absence of palm
pressure. d. Allows for responder to move on to next wound. e. The effective use of elastic wrap and gauze together has spawned new
dressings.
Notes:
Deployment Medicine International 85
PRESSURE DRESSING APPLICATION:
1. Long-term combination of pressure and gauze.
2. Allows for application of increased pressure to the wound site providing better
management of blood loss.
3. Pressure at wound site must be greater than or equal to pressure of blood exiting
wound.
4. Application Principles:
a. Keep dressing flat b. Anchor dressing/ make sure it will not shift c. Multiple wraps are what increase pressure/effectiveness. d. Wrap above and below the wound to account for wound tracks
Notes:
Deployment Medicine International 86
TYPES OF PRESSURE DRESSINGS: 1. Israeli (Emergency Bandage) Dressing
2. Cinch Tight Dressing
3. Elastic Bandage
Deployment Medicine International 87
HEMOSTATIC AGENTS
Training Objectives:
1. Provide an answer to injuries that are not manageable through other techniques due to their severity and location on the body.
2. Application Locations:
a. Axilla (Shoulder)
b. Inguinal Crease (Groin)
3. Application Criteria:
a. Arterial Bleeding
b. High Pressure
c. High volume
d. Non-compressible
e. Not able to be controlled with a tourniquet.
4. Hemostatic agents come at a cost:
a. Complexity of application
b. Time required to apply.
c. Requires special packaging and handling of casualty.
d. High potential of re-bleeding.
5. Not currently designed to deal with:
Deployment Medicine International 88
a. Abdominal injury (belly wounds).
b. Intra-thoracic injury (chest wounds).
6. Hemostatic agents are used where other less costly techniques are not
successful or applicable.
7. The use of a hemostatic agent is aimed at solving one problemthe occlusion or
partial reduction of an arterial insult that is unable to be controlled by lesser methods.
8. Hemostatic agent application is a complex process that requires a systematic
approach to ensure application success on the battlefield.
Deployment Medicine International 89
HEMOSTATIC AGENTS
PURPOSE:
1. Provide an answer to injuries that are not manageable through other
techniques due to their severity and location on the body.
2. Facilitate clot formation on high limb (torso-extremity junction) arterial I
njury.
3. The use of a hemostatic agent is aimed at solving one problem-the
occlusion or partial reduction of an arterial insult that is unable to be
controlled by lesser methods.
4. Currently designed for a free-flowing bleeding wound accessible from the
surface.
Deployment Medicine International 90
APPLICATION:
1. Application Locations (Edge of Armor Injuries):
a. Axilla (Shoulder)
b. Inguinal Crease (Groin)
c. Neck
2. Primary Application Criteria:
a. Arterial Bleeding
b. High Pressure
c. High Volume
d. Not able to be controlled with a tourniquet
e. Not able to be controlled with a pressure dressing
3. Secondary Application Criteria (Gauze based agents): Extremity wound in
conjunction to pressure dressing to reduce tourniquet.
4. Not currently designed to deal with:
a. Abdominal injury (belly wounds).
b. Intra-thoracic injury (chest wound).
c. NEVER place inside a body cavity (chest, abdomen, skull or pelvis).
Deployment Medicine International 91
PRIMARY HEMOSTATIC AGENT APPLICATION LOCATIONS: (CIRCLE AREAS)
Deployment Medicine International 92
CONSIDERATIONS:
1. Hemostatic agents are not magic:
a. A hemostatic agent is an augmentation to pressure, not a replacement
for pressure
2. Hemostatic agent management:
a. Cover agent with gauze and a firm pressure dressing after successful
application to maintain control of bleeding
b. Re-examine wound for signs of additional blood loss or clot breakage.
c. If clot breaks apply direct pressure and reapply with more hemostatic
agent or gauze
d. Apply anatomical and rigid splinting techniques to avoid excessive
movement of injured area
3. Hemostatic agent applications require gauze reinforcement and a pressure dressing
4. Problems with use of hemostatic agents:
a. Reliance on hemostatic agents as the only method of controlling
junctional bleeding
b. Not applying the agent to the source(s) of the bleeding
c. Allowing the agent to shift away from the source of the bleeding
d. Removing pressure from the wound
e. Not reinforcin