DM Chapter7

of 14
-
Upload
saymynames -
Category
Documents
-
view
260 -
download
0
Transcript of DM Chapter7
-
7/31/2019 DM Chapter7
1/14
Chapter7Diabetes andStroke
7.151
Diabetes in Ontario Practice Atlas
Authors: Moira K. Kapral, Deanna M. Rothwell, Kinwah Fung,Mei Tang, Gillian L. Booth and Andreas Laupacis
-
7/31/2019 DM Chapter7
2/14
BackgroundStroke is a leading cause of death and disability in Canada.1 Diabetes
mellitus (DM) increases the risk of stroke, and is a particularly
potent stroke risk factor in younger individuals, with previous
studies suggesting an increase in stroke risk of as much as 10-fold
in some younger subgroups.2,3,4 DM is associated with a higher
prevalence of other stroke risk factors, including high bloodpressure and high cholesterol,5 and may increase the risk of stroke
recurrence and mortality.6,7 Despite the association between DM
and stroke, the available data from clinical trials do not support the
hypothesis that better blood sugar control decreases stroke risk.6,8
Carotid endarterectomy is a surgical procedure to remove athero-
sclerotic plaque from the carotid artery. Clinical trials have found
that in appropriately selected individuals with previous stroke or
transient ischemic attack (TIA), carotid endarterectomy substantially
lowers the risk of future stroke or death compared to medical
therapy.9-11 It is not known whether carotid endarterectomy rates
are different in those with and without DM. Perioperativecomplications may be more frequent in those with DM.12
This chapter will present analyses of stroke-related hospitalizations,
outcomes (death, length of stay and discharge to complex continuing
care institutions) and procedures (carotid endarterectomy) in Ontario,
in people with and without DM, with stratification by age, sex,
socioeconomic status and geographic region.
Data SourcesThe Registered Persons Database (RPDB) was used to identify all
individuals between the ages of 20 and 105 who were eligible for
coverage under the Ontario Health Insurance Plan (OHIP) during the
fiscal years 1995 to 1999. Persons with DM were identified using the
Ontario Diabetes Database (ODD), which is described in detail in the
Chapter 1 Technical Appendix TA1.A. Individuals in the RPDB who were
not present in the ODD served as a non-diabetic comparison group.
Creation of this cohort is described in Chapter 5 Technical Appendix
TA5.A. Records of hospitalizations for stroke and carotid endart-
erectomy procedures were obtained from the Canadian Institute for
Health Information (CIHI) discharge abstract database. Census data from
Statistics Canada were used to obtain information on the socio-
economic status of residential neighbourhoods. These data were linkedto other sources using postal code of residence as a common variable.
How the analysiswas doneAnnual stroke hospitalization rates were calculated from fiscal 1995
(April 1, 1994 to March 31, 1995) through fiscal 1999. The total
number of persons with DM who were admitted with a stroke in
a given year defined the numerator, while the denominator was the
total number of persons with DM during the same time period.
7.152
Diabetes in Ontario
Key Messages
Stroke risk is markedly increased in thepresence of diabetes mellitus (DM), even in
younger individuals. Health care professionals
and patients should be aware of these risks,
and should be attentive to the appropriate
management of associated stroke risk factors.
Stroke hospitalization rates in those with DMare declining over time. Further research is
needed to determine whether this is due to
changes in stroke incidence or stroke admission
thresholds.
Diabetes and Stroke
-
7/31/2019 DM Chapter7
3/14
Records of admissions to acute care hospitals with a diagnosis of
stroke were obtained from the CIHI discharge abstract database
using ICD-9 codes 431, 434 and 436. Previous studies using these
codes have established an accuracy rate of over 90% for the
diagnosis of stroke.13 Persons transferred from other facilities and
those with stroke as an in-hospital complication
were excluded from the analyses. For those
persons with more than one stroke admission
during the study time frame, only the first
stroke admission was included in the analyses.
Annual stroke hospitalization rates were
calculated for persons with and without DM, and
were categorized by age, sex, socioeconomic
status, and geographic region (county). In
Ontario, personal income is not available
in administrative data sources. Therefore,
neighbourhood median household income
was attributed to the individuals studied.
Neighbourhoood level income quintiles were
obtained from 1996 census data at the level of
the enumeration area.14 This method defines
quintiles separately for census metropolitan
areas (CMA) or census agglomerations (CA)
and areas not in any CMA or CA, so that the
measure is relative to the larger area in which
a person resides.
Among stroke patients, median length of stay
and rates of discharge to complex continuing care
institutions were compared in persons with and
Practice Atlas
7.153
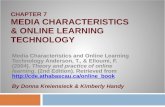
Stroke hospitalization rates are almost three-fold higher in individuals with DM compared to those without DM, and therelative increase in stroke risk is particularly marked in the younger age groups.
1995 DM 147.8 575.8 1,427.5 2,846.8 177.3
1996
DiabeticStatus
Women by Age Group
DM 109.9
738.0 1,661.5
541.9 1,323.7
3,290.8
2,800.1
Men by Age Group
177.2 743.3 1,700.7 3,077.3
136.2 691.4 1,639.9 3,073.2
14.4 156.0 574.0 1,585.8
14.4 147.0 590.0 1,639.9
1997 DM 116.4 579.6 1,303.9 2,706.4
No DM 12.6 86.9 372.1 1,334.3
No DM 11.6 94.6 373.9 1,344.5
Source: Ontario Diabetes Database (ODD). *Odds Ratios (95% CI) are only for 1999. Note: Fiscal year 1995 = April 1, 1994 to March 31, 1995. Adjusted for age and
Exhibit 7.1 Overall and Age-/Sex-specific Stroke Hospitalization Rates per 100,000 Ontarians with/without DM19951999
4,526
4,792
5,071
12,078
11,972
No DM 11.1 88.8 395.6 1,374.712,131 14.1 154.5 639.1 1,691.7
1,214
Overall Men &Women
1,177
158
1,151
154
154
5,125
11,906
152.3 605.0 1,526.9 2,883.8
15.2 142.2 548.7 1,527.3
1998 DM 135.3 513.6 1,243.3 2,509.01,074
150No DM 11.9 80.6 347.2 1,334.5
5,222
11,356
164.4 594.8 1,405.3 2,688.7
14.0 132.2 514.4 1,435.6
1999 DM 82.5 467.4 1,130.9 2,487.51,015
141No DM 10.5 79.3 349.1 1,218.6
1,203
1,145
156
1,134
154
155
1,059
151
999
142
1,225
1,207
1,167
153
154
160
1,088
148
1,029
139
OverallnFiscal Year 2049 5064 6574 75+ Overa2049 5064 6574 75+Rate
7.
(7.167.
11.74
(9.4014.65)
4.52
(4.085.01)
2.76
(2.542.99)
1.90
(1.772.04)7.28 (7.057.53)
Odds RatioCrude*
7.08
(6.757.42)
7.87
(5.7810.72)
5.92
(5.196.75)
3.27
(2.983.5)
2.07
(1.942.20)
2.
(2.542.2.67 (2.582.76)
Odds RatioAdjusted*
2.67
(2.552.81)
Exhibit 7.2 Age-/Sex-specific Hospitalization Rates for Stroke per
100,000 Ontarians with/without DM Aged 20 Years and Over, 1995199
There was a decline in stroke hospitalization rates over the study periodin persons with and without DM.
Source: Ontario Diabetes Database (ODD). Note: Fiscal year 1995 = April 1, 1994 to March 31, 199
-
7/31/2019 DM Chapter7
4/14
without DM, with stratification by stroke type (hemorrhagic and
ischemic). Mortality rates following hospitalization for stroke were
calculated at 30 days and one year after the index admission.
Deaths were ascertained from the Registered Persons Data Base
(RPDB) and CIHI discharge abstracts. Mortality rates after stroke
were adjusted for age, sex, stroke type and
comorbidity based on the Charlson-Deyo score,
a commonly used method that uses indicators of
major disease groups within hospital diagnostic
codes to assign a level of comorbidity.15
Admissions for carotid endarterectomy pro-
cedures within a year after the index admission
were identified from CIHI records in which the
Canadian Classification of Procedures (CCP) code
was 50.12. Carotid endarterectomy rates per
100 patients with stroke were calculated for
persons with and without DM, categorized by
age and sex. Waiting times for carotid surgery
were calculated using the time from stroke
admission to the date of surgery.
Multivariate techniques (Cox proportional
hazards models) were used to identify risk
factors for suffering a stroke during the five-
year observation period. Factors that were
tested included age, sex, socioeconomic status
(SES), presence of other medical conditions
(comorbidity), type of residential area (urban
versus rural), geographic region of the province,
and use of outpatient services. Individuals were
categorized as having a regular provider of care
Diabetes in Ontario
7.154
Source: Ontario Diabetes Database (ODD)
Diabetes and Stroke
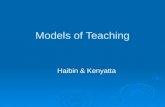
Stroke hospitalization rates in both those with and without DM were inversely related to socioeconomic status, with modestlyincreased stroke hospitalization rates seen in the lowest income quintiles.
Exhibit 7.3 Overall and Five-year Average Age-/Sex-specific Stroke Hospitalization Rates per 100,000Ontarians with/without DM by DM Status and Residence Area Income Quintile, 19951999
1,141Q1 (low) DM 145.9 636.4 1,405.8 2,586.81,215
1,078
1,194164.9
1,111Q2
Diabetic
Status
Women by Age Group
DM 124.9
779.1 1,736.7
521.4
938
2,275
2,472
176
1,304.0
No DM 13.0
3,131.8
118.3
2,703.5 1,172
Men by Age Group
150.7 706.9
431.5 1,384.32,678
1,638.4
1,134
16.3
3,018.0
149
155.2 682.0 1,487.9 3,078.9
159
15.8 145.1 566.2 1,517.6
164
14.7 168.6 606.0 1,588.4
196.3 679.6 1,753.7
1,166
Overall Men &
Women
1,045Q3 DM 91.8 501.9 1,179.4 2,679.3
1,143
170
1,092
148
159
147No DM 11.7 92.9 360.9 1,304.9
804
1,967
1,085179.1 609.3
159No DM 12.5 85.7 380.2 1,355.0
1,572.2 2,965.0
13313.5 124.9 528.3 1,509.2
1,056Q4 DM 101.6 489.4 1,198.6 2,860.01,072
130 127No DM 11.1 77.1 343.0 1,309.7
707
2,029
1,053153.8 564.3 1,419.1 2,807.8
13811.4 110.6 478.5 1,503.4
1,035Q5 (high) DM 98.5 426.8 1,198.4 2,611.01,045
131 126No DM 9.2 62.1 303.5 1,241.1
OverallnIncomeQuintile
2049 5064 6574 75+ Overall2049 5064 6574 75+Rate
Exhibit 7.4 Five-year Average Stroke Hospitalization Ratesper 100,000 Ontarians with DM Aged 20 Years and Over by
Residence Area Income Quintile, 19951999Stroke hospitalization rates in both persons with/without DM wereinversely related to socioeconomic status.
Source: Ontario Diabetes Database (ODD)
-
7/31/2019 DM Chapter7
5/14
if at least 50% of their primary care visits were to a single provider.
Adjustment for the presence of other medical conditions that
might affect outcomes was performed using the John Hopkins
Ambulatory Care Groups (ACG) assignment software.16.17 Region
of residence was based on the Ontario Ministry of Health and Long-
Term Care (MOHLTC) planning regions. There was no significant
colinearity between any of the variables included in the model.
Small area rate variation (SARV) analysis compared hospitalization
and procedure rates across regions of the province (a review of
SARV statistics appears in Chapter 2 Technical Appendix TA2.1).
Interpretive CautionsThe analyses rely on administrative data, which lack information
on important prognostic factors such as stroke subtype and severity.
In addition, comorbid conditions may be miscoded. The analyses
use neighbourhood income quintile as a marker of socioeconomic
status, rather than individual level data, which may lead to
misclassification of individual socioeconomic status. The CIHIdatabase only captures hospital admissions, which would lead to
under-reporting of stroke rates since it does not include patients
with stroke or transient ischemic attack who were never admitted
to hospital. It is not known whether any of these factors would
lead to systematic bias in comparisons between individuals with
and without DM. However, it is conceivable that a person with DM
and minor stroke or TIA is more likely to be admitted to hospital
than a person without DM with a similar stroke presentation. This
could lead to higher stroke admission rates (and decreased stroke
severity among admitted patients) in persons with DM relative to
those without.
Trends in the control of risk factors, especially hypertension, are likely
to be important determinants of stroke rates over time, and these
were not evaluated in the current analyses. For the analyses of
carotid endarterectomy rates, administrative data do not have
information on the prevalence or degree of carotid stenosis or the
indications for surgery, so one cannot comment on the
appropriateness of the observed rates of surgery in this study
population. In addition, waiting times for carotid endarterectomy
are estimated based on the time between the index stroke
admission and the date of surgery, and may not be an accurate
reflection of the time interval from diagnosis or referral to surgery.
Findings and DiscussionEven after adjustment for age and sex, stroke risk was greatly
increased in those with DM, with stroke hospitalization rates
almost three-fold higher in individuals with DM than in those
without (Exhibit 7.1). The diabetes-related stroke risk was particularly
marked in the younger age groups, such that their stroke risk was
similar to what would be expected in an older non-diabetic
population. For example, the risk of stroke in a 20 to 49-year-old
person with DM was greater than that of a 50 to 64-year-old
Practice Atlas
7.155
Key Research Findings
Stroke hospitalization rates are approximatelythree-fold higher in those with diabetes
mellitus (DM) compared to those without,and are even more markedly increased in
younger age groups.
Stroke hospitalization rates are decreasingover time.
There are only minor regional variations instroke hospitalization rates across Ontario.
Older age, male sex, lower neighbourhoodincome quintile, previous myocardial
infarction and comorbid illness are allassociated with increased stroke admission
rates; conversely, the presence of a regular
source of care and the number of ambulatory
care visits do not appear to affect stroke
admission rates.
After stroke admission, those with DM areat increased risk of death within 30 days or
discharge to chronic care compared to
those without DM.
Men are more likely than women to undergocarotid endarterectomy after stroke.
-
7/31/2019 DM Chapter7
6/14
Diabetes in Ontario Diabetes and Stroke
7.156
Exhibit 7.5a Five-year Averaged Crude and Age-/Sex-adjusted Stroke Hospitalization Rates per 100,000Ontarians with DM Aged 20 Years and Over by County, 19951999
Regional differences in hospitalization rates for stroke were not statistically significant in individuals with DM.
Source: Ontario Diabetes Database (ODD)
-
7/31/2019 DM Chapter7
7/14
-
7/31/2019 DM Chapter7
8/14
Diabetes in Ontario Diabetes and Stroke
7.158
Sources:Can
adianInstituteforHealthInformation(CIHI),
OntarioDiabetesDatabase(ODD)
Exhibit7.6a
Age-/Sex-adjustedStrokeHospitalizationRatespe
r100,000OntarianswithDM,Age
d20YearsandOver,byCounty,N
orthernOntario,
19951999
Note:
See
Exhibit7.6
b
forLegend.
-
7/31/2019 DM Chapter7
9/14
Practice Atlas
7.159
Exhibit7.6b
Age-/Sex-adjust
edStrokeHospitalizationRatespe
r100,000OntarianswithDM,Age
d20YearsandOver,byCounty,S
outhernOntario,
19951999
Peterborough
-
7/31/2019 DM Chapter7
10/14
Diabetes in Ontario Diabetes and Stroke
Exhibit 7.7 Characteristics of Stroke Patients by DM Status in Ontario, 19951999
There were significant differences in
stroke type in persons with/without DM,
with a higher proportion of ischemic
stroke among those with diabetes.
Source: Ontario Diabetes Database (ODD)
7.160
Exhibit 7.8 Age-adjusted Rates of Discharge to Complex Continuing Care Institution or Death within
30 Days after Stroke per 100 Ontarians with Stroke by DM Status, Stroke Type, and Gender, 19951999
After admission to hospital for either ischemic or hemorrhagic stroke, mortality within 30 days or discharge to chronic carewas higher in those with DM.
Mean ageyears
Q1 (low) 4,952 (24%)
72.92
Malen (%) 11,450 (53%)
12,243 (23%)
73.81
27,335 (48%)
N 21,774 56,759
11,308 (21%)
Income quintile n (%)
Q2
9,337 (18%)
4,583 (23%)
9,517 (18%)
10,571 (20%)
-
7/31/2019 DM Chapter7
11/147.161
Practice Atlas
Exhibit 7.9 Thirty-day and One-year Mortality Rates per 100 Persons with Stroke by DM Status andGender in Ontario, 19951999
After adjusting for age, sex, comorbid conditions and stroke type, there were no large differences in all-cause mortality at30 days or one year in those with or without DM.
Source: Ontario Diabetes Database (ODD). Note: Fiscal year 1995 = April 1, 1994 to March 31, 1995.
Exhibit 7.10 Sex-specific Post-stroke Carotid Endarterectomy Rates per 100 Ontarians with Stroke andWaiting Times by DM Status, 19951999
Overall rates of carotid endarterectomy after stroke were similar in those with and without DM.
1-year Mortality
Number of Cases Risk-adjusted Rate*
30-day Mortality
Gender/DM Status Number of Cases Risk-adjusted Rate*
13,131Overall
4,024 34.40 (95%CI; 33.59-35.21)
9,107 35.37 (95%CI; 34.82-35.93)
7,728
DM 2,295 20.63 (95%CI;19.90-21.36)
5,433 20.82 (95%CI;20.35-21.30)
Men
No DM
14,411Overall
3,725 33.58 (95%CI; 32.76-34.41)
10,686 35.62 (95%CI; 35.11-36.13)
8,580
DM 2,170 20.36 (95%CI;19.61-21.10)
6,410 21.91 (95%CI;20.47-21.34)
Women
No DM
Source: Ontario Diabetes Database (ODD). *Adjusted for age, sex, Charlson comorbidity and stroke type.
27,542Overall
7,749 34.00 (95%CI; 34.42-34.58)
19,793 35.51 (95%CI; 35.13-35.88)
16,308
DM 4,465 20.50 (95%CI;19.98-21.02)
11,843 20.87 (95%CI;20.55-21.19)
All Patients
No DM
1995 DM 51 1.9 2.477
711996
DMStatus
Median Waiting
Time (days)
DM 74
Men
Overall
Women
Overall
1.0
59
143
144
2.6
No DM 41 1.0 2.2150
2.2
OverallMen & Women
1997 DM 82 1.1 1.8
1.9
1.6
1.5
1.5
1.5
No DM 55 0.8 2.2
75
144
No DM 63 0.9 2.2
1998 DM 62 1.1 2.41.8
1.5No DM 70 1.0 2.2
70
141
1999 DM 74 1.3 2.01.7
1.6No DM
55 1.2 2.0
nFiscal Year Rate RateRate
1.07 (0.801.42)Odds Ratio Crude*(95% CI)
1.14 (0.711.82) 0.99 (0.691.43)
0.95 (0.711.27)Odds Ratio Adjusted*(95% CI)
1.00 (0.621.60) 0.99 (0.691.43)
-
7/31/2019 DM Chapter7
12/14
Diabetes and Stroke
7.162
Diabetes in Ontario
infarction and comorbid illness. Rural residence, region of
residence, number of ambulatory care visits and having a regular
source of care were not significant predictors of subsequent
stroke admission.
Among hospitalized stroke patients, the characteristics of those
with and without DM were similar. Those with DM were
slightly younger and were more likely to be male, but the
differences were small (Exhibit 7.7). There were significant
differences in stroke type in those with and without DM, with
a higher proportion of ischemic stroke among those with DM
(94% vs. 89%, P
-
7/31/2019 DM Chapter7
13/14
References1. Heart and Stroke Foundation of Canada. Statistics Canada, He
Canada, and Heart and Stroke Foundation of Canada, editors. H
disease and stroke in Canada, 1997.
2. Jamrozik K, Broadhurst RJ, Forbes S, Hankey GJ, Anderson CS. Predic
of death and vascular events in the elderly. The Perth CommuStroke Study. Stroke 2000; 31:863868.
3. Kuusisto J, Mykkanen L, Pyorala K, Laakso M. Non-insulin-depend
diabetes and its metabolic control are important predictors of strok
elderly subjects. Stroke 1994; 25:11571164.
4. Jorgensen H, Nakayama H, Raaschou HO, Olsen TS. Stroke in patiwith diabetes: the Copenhagen Stroke Study. Stroke 1994; 25:197719
5. Benson RT, Sacco RL. Stroke prevention: hypertension, diabetes, toba
and lipids. Neurol Clin 2000; 18:309319.
6. UK Prospective Diabetes Study Group. Intensive blood-glucose con
with sulphonylureas or insulin compared with conventional treatm
and risk of complications in patients with type 2 diabetes (UKPDS
Lancet1998; 352:837853.
7. Tuomilehto J, Rastenyte D, Jousilahti P, et al. Diabetes mellitus as a
factor for death from stroke. Prospective study of a middle a
Finnish population. Stroke 1996; 27:202205.
8. Hankey GJ, Jamrozik K, Broadhurst RJ, Forbes S, Burvill PW, AndeCS, Stewart-Wynne EG. Long-term risk of first recurrent stroke in
Perth Community Stroke Study. Stroke 1998; 29:24912500.
9. North American Symptomatic Carotid Endarterectomy T
Collaborators. Beneficial effect of carotid endarterectomysymptomatic patients with high-grade carotid stenosis. N Engl J M1991; 325:445453.
10. European Carotid Surgery Trialists Collaborative Group. MRC Europ
Carotid Surgery Trial: interim results for symptomatic patients w
severe (7099%) or with mild (029%) carotid stenosis. Lancet 19337:12351243.
11. Barnett HJM, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes
Rankin RN, Clagett GP, Hachinski VC, Sackett DL, et al. Benefi
carotid endarterectomy in patients with symptomatic moderatesevere stenosis. N Engl J Med1998; 339: 14151425.
12. Fabris F, Zanocchi M, Bo M, et al. Carotid plaque, aging and
factors. A study of 457 subjects. Stroke 1994; 25:11331140.
13. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity in
for use with ICD-9-CM administrative databases. J Clin Epi1992; 45613619.
14. Weiner JP, Starfield BH, Steinwachs DM, Mumford LM. Developm
and application of a population-oriented measure of ambulatory ccase-mix. Medical Care 1991; 29:452472.
15. Reid RJ, MacWilliam L, Verhulst L, Roos N, Atkinson M. Performance of
ACG Case-Mix system in two Canadian Provinces. Medical Care 239:3699.
16. Barrett-Connor E, Khaw K: Diabetes mellitus: An independent
factor for stroke. Am J Epidemiol1988; 128:116124.
very little difference in 30-day and one-year all-cause mortality
in those with and without DM (Exhibit 7.9).
Overall rates of carotid endarterectomy after stroke were low,
but similar in those with and without DM (Exhibits 7.10 and
7.11). The most significant finding was that rates of surgery
were about twice as high for men than for women regardless
of DM status.
ConclusionsDiabetes is an extremely powerful risk factor for stroke (it
increases the risk of stroke almost three-fold), in both men and
women and in every age group. Between 1995 and 1999, there
was a gradual decline in the risk of stroke hospitalization in
those with and without DM. This could be related to a decrease
in the incidence of stroke due to improved blood glucose
control, use of antithrombotic agents, or modification of other
stroke risk factors such as hypertension and hyperlipidemia.
Of note, there was an increase in the use of antihypertensive
and lipid lowering medications during the study time frame
(See Chapter 3: Drug Use in Older People with Diabetes).
However, it is difficult to draw firm conclusions given the
multifactorial etiology of stroke and the relatively short time
interval studied. Other potential explanations for the observed
decline in stroke hospitalization rates include changes in
admission thresholds for those with less severe strokes.
These analyses do not provide direct information on the
influence of diabetes on stroke severity. Persons with DM had
a slightly longer length of stay, and were more likely to be
either discharged to complex continuing care facility or die
within 30 days of stroke, regardless of stroke type. While this
could indicate greater stroke severity in those with DM, other
explanations include a greater frequency of post-stroke
complications or other comorbid illness. The finding that
adjusted 30-day and 1-year all cause mortality after stroke
were not increased in those with DM argues against major
differences in stroke severity based on DM status.
Post-stroke carotid endarterectomy rates were similar in those
with and without DM. It is surprising that women were only
half as likely as men to undergo carotid endarterectomy, even
in the presence of DM where stroke risks are similar in women
and men. Data sources with more detailed clinical information
are needed to determine the prevalence of moderate to severe
carotid stenosis in men and women with and without DM and
the appropriate rates of carotid endarterectomy in these
populations.
Overall, these analyses confirm that stroke is a common and
serious complication of DM. Further study is needed to determine
whether local initiatives to improve DM care will result in
significant reductions in stroke risks or improved stroke outcomes.
Practice Atlas
7.163
-
7/31/2019 DM Chapter7
14/14
Diabetes in Ontario Diabetes and Stroke