Dizziness: Differential Diagnosis Mark Klafter,...
41
Dizziness: Differential Dizziness: Differential Diagnosis Diagnosis Mark Klafter, D.O. Mark Klafter, D.O. Teaching Attending, Orlando Regional Teaching Attending, Orlando Regional Healthcare System Healthcare System
Transcript of Dizziness: Differential Diagnosis Mark Klafter,...
Dizziness: Differential Dizziness: Differential DiagnosisDiagnosisMark Klafter, D.O.Mark Klafter, D.O.
Teaching Attending, Orlando Regional Teaching Attending, Orlando Regional Healthcare SystemHealthcare System

““Is it in your feet or your head?Is it in your feet or your head?””
Imbalance: Perceived as Imbalance: Perceived as ““dizzinessdizziness”” to some to some people, but no lightheadedness or vertigopeople, but no lightheadedness or vertigoRemember that blurred vision is often perceived Remember that blurred vision is often perceived as as ““dizzinessdizziness””If not If not ““imbalance in the feet onlyimbalance in the feet only””, or blurring , or blurring of vision, differentiate between vertigo and of vision, differentiate between vertigo and lightheadedlightheaded--type dizzinesstype dizziness
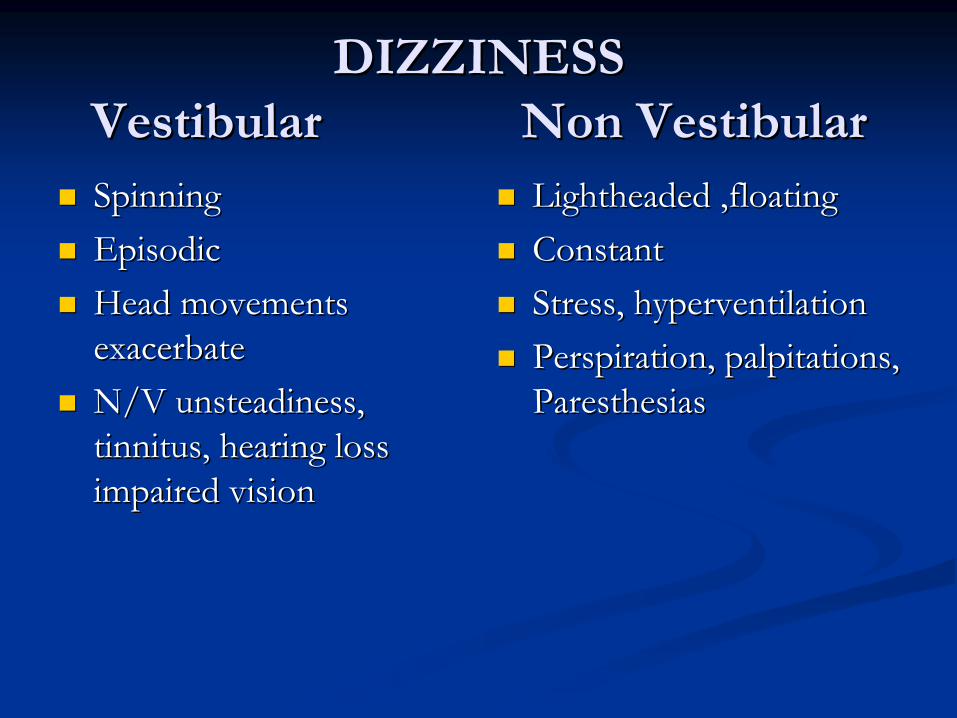
DIZZINESSDIZZINESS Vestibular Non VestibularVestibular Non Vestibular
SpinningSpinningEpisodicEpisodicHead movements Head movements exacerbateexacerbateN/V unsteadiness, N/V unsteadiness, tinnitus, hearing loss tinnitus, hearing loss impaired visionimpaired vision
Lightheaded ,floatingLightheaded ,floatingConstant Constant Stress, hyperventilationStress, hyperventilationPerspiration, palpitations, Perspiration, palpitations, ParesthesiasParesthesias
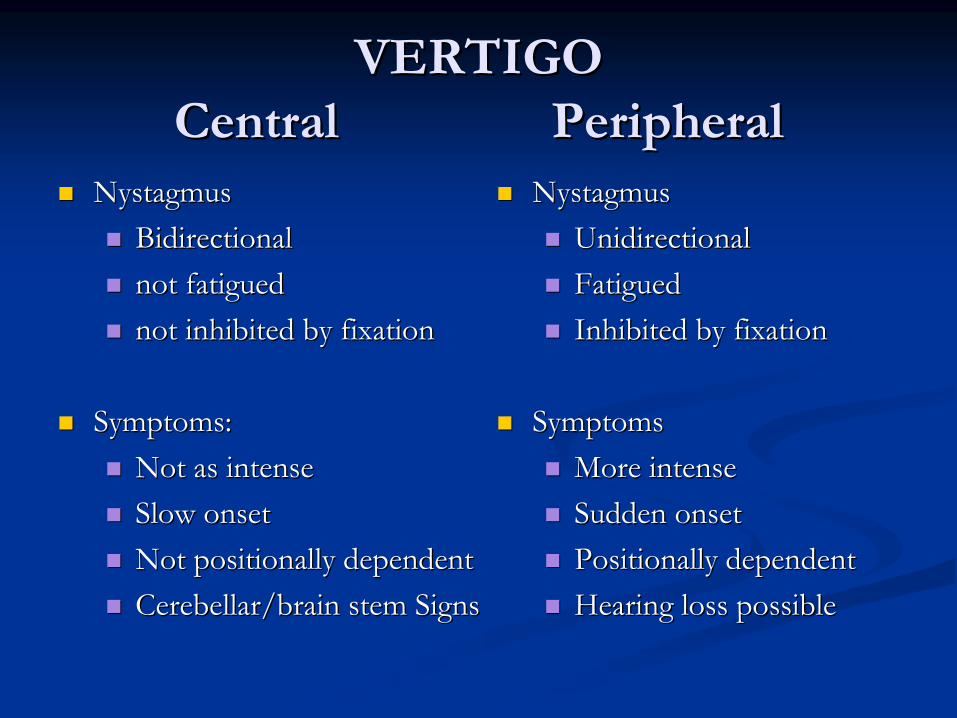
VERTIGOVERTIGO Central PeripheralCentral Peripheral
NystagmusNystagmusBidirectionalBidirectionalnot fatiguednot fatiguednot inhibited by fixationnot inhibited by fixation
Symptoms: Symptoms: Not as intenseNot as intenseSlow onsetSlow onsetNot positionally dependentNot positionally dependentCerebellar/brain stem SignsCerebellar/brain stem Signs
NystagmusNystagmusUnidirectionalUnidirectionalFatiguedFatiguedInhibited by fixationInhibited by fixation
SymptomsSymptomsMore intenseMore intenseSudden onsetSudden onsetPositionally dependentPositionally dependentHearing loss possibleHearing loss possible

CENTRAL VERTIGOCENTRAL VERTIGO CausesCauses
Stroke and TIAStroke and TIACerebellumCerebellumAICA distributionAICA distributionPICA distributionPICA distributionVertebrobasilar migraine Vertebrobasilar migraine
Adult formAdult formChildhood variant (benign Childhood variant (benign paroxysmal vertigo of paroxysmal vertigo of childhood)childhood)Seizure (temporal lobe)Seizure (temporal lobe)Multiple sclerosis, Multiple sclerosis, Post infectious demyelinationPost infectious demyelination
Tumors of eight nerve, brain Tumors of eight nerve, brain stem, or cerebellumstem, or cerebellumParaneoplastic Paraneoplastic Cerebellar degenerationCerebellar degenerationWernicke's syndromeWernicke's syndromeTIA, transient ischemic attack;TIA, transient ischemic attack;AICA, anterior inferior cerebellar AICA, anterior inferior cerebellar artery; PICA, posterior inferior artery; PICA, posterior inferior cerebellar artery.cerebellar artery.ArnoldArnold--Chiari malformationChiari malformation
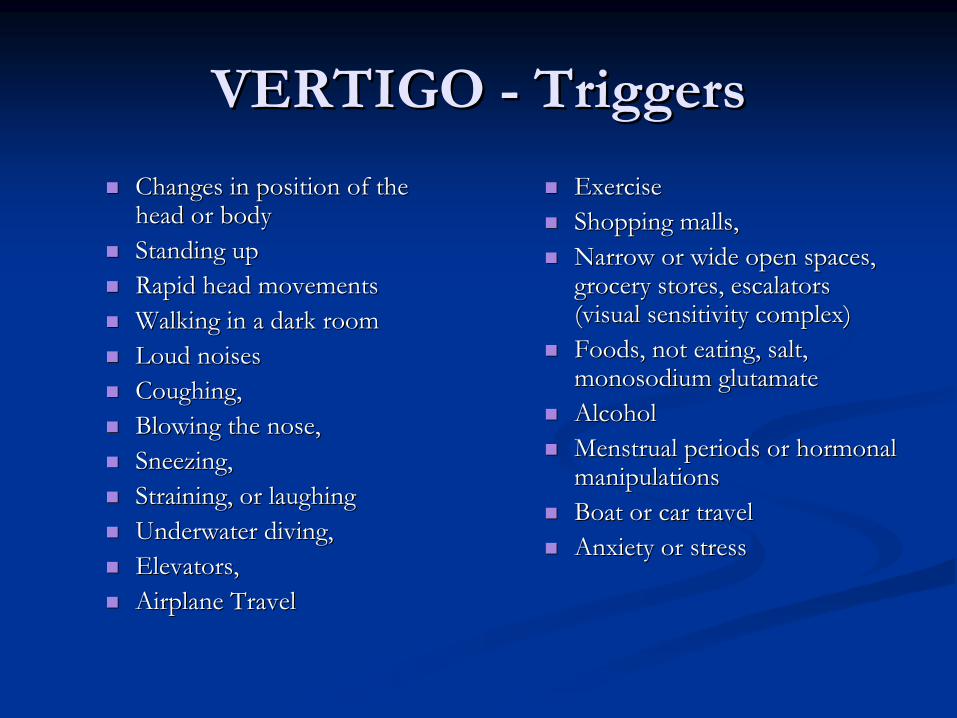
VERTIGO VERTIGO --
TriggersTriggers
Changes in position of the Changes in position of the head or bodyhead or bodyStanding upStanding upRapid head movementsRapid head movementsWalking in a dark roomWalking in a dark roomLoud noisesLoud noisesCoughing, Coughing, Blowing the nose, Blowing the nose, Sneezing, Sneezing, Straining, or laughingStraining, or laughingUnderwater diving, Underwater diving, Elevators,Elevators,Airplane TravelAirplane Travel
ExerciseExerciseShopping malls,Shopping malls,Narrow or wide open spaces, Narrow or wide open spaces, grocery stores, escalators grocery stores, escalators (visual sensitivity complex)(visual sensitivity complex)Foods, not eating, salt, Foods, not eating, salt, monosodium glutamatemonosodium glutamateAlcoholAlcoholMenstrual periods or hormonal Menstrual periods or hormonal manipulationsmanipulationsBoat or car travelBoat or car travelAnxiety or stressAnxiety or stress
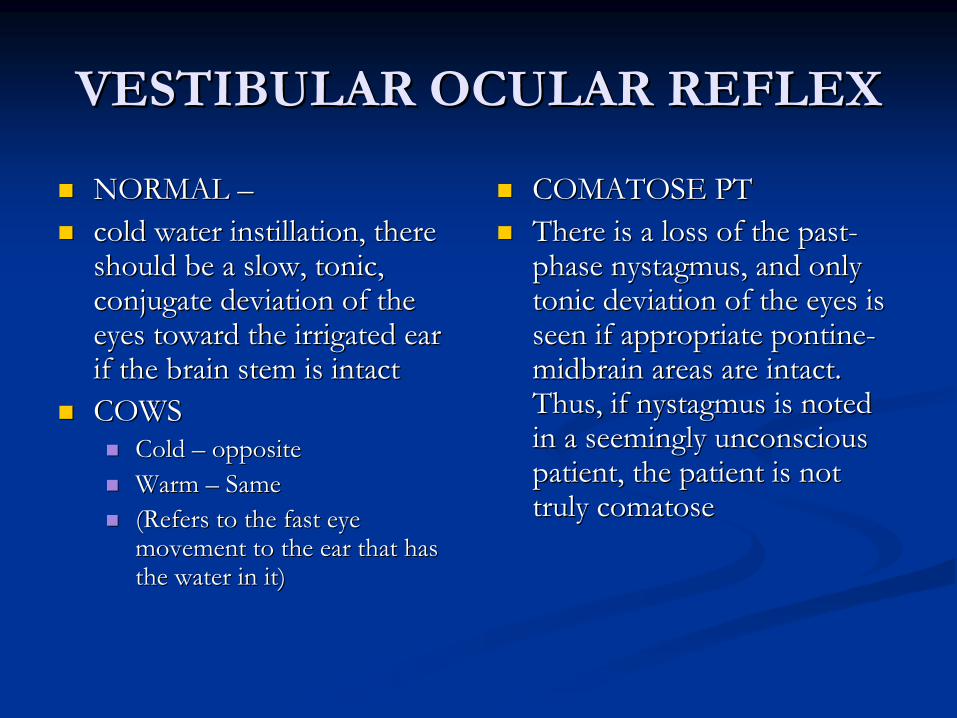
VESTIBULAR OCULAR REFLEXVESTIBULAR OCULAR REFLEX
NORMAL NORMAL ––cold water instillation, there cold water instillation, there should be a slow, tonic, should be a slow, tonic, conjugate deviation of the conjugate deviation of the eyes toward the irrigated ear eyes toward the irrigated ear if the brain stem is intact if the brain stem is intact COWSCOWS
Cold Cold –– oppositeoppositeWarm Warm –– Same Same (Refers to the fast eye (Refers to the fast eye movement to the ear that has movement to the ear that has the water in it)the water in it)
COMATOSE PTCOMATOSE PTThere is a loss of the pastThere is a loss of the past--phase nystagmus, and only phase nystagmus, and only tonic deviation of the eyes is tonic deviation of the eyes is seen if appropriate pontineseen if appropriate pontine--midbrain areas are intact. midbrain areas are intact. Thus, if nystagmus is noted Thus, if nystagmus is noted in a seemingly unconscious in a seemingly unconscious patient, the patient is not patient, the patient is not truly comatose truly comatose
VERTIGO VERTIGO TESTINGTESTING
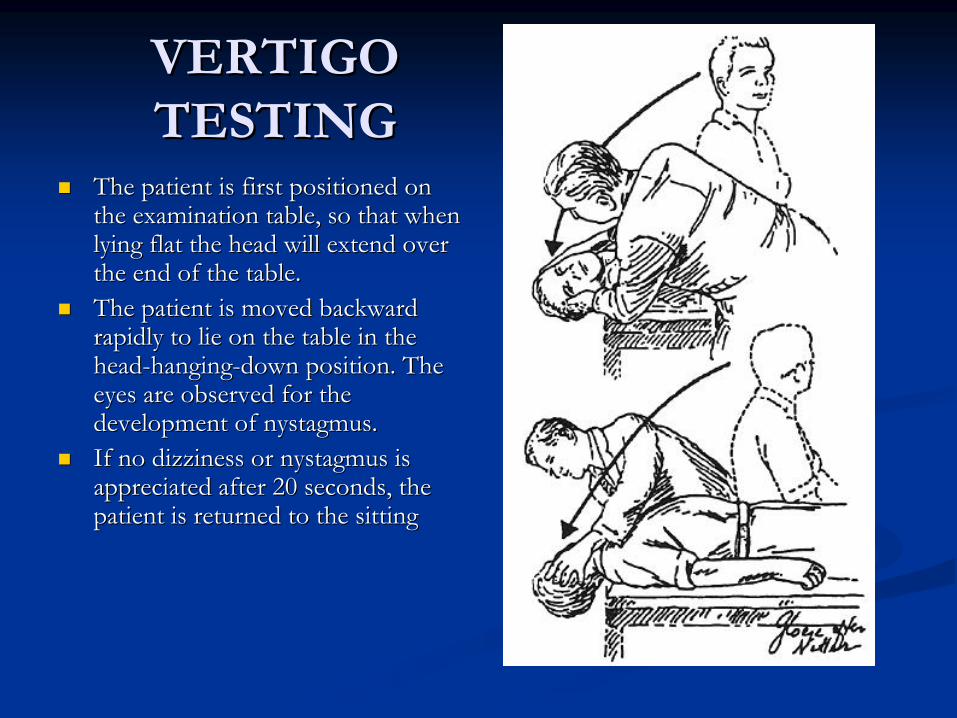
The patient is first positioned on The patient is first positioned on the examination table, so that when the examination table, so that when lying flat the head will extend over lying flat the head will extend over the end of the table. the end of the table. The patient is moved backward The patient is moved backward rapidly to lie on the table in the rapidly to lie on the table in the headhead--hanginghanging--down position. The down position. The eyes are observed for the eyes are observed for the development of nystagmus. development of nystagmus. If no dizziness or nystagmus is If no dizziness or nystagmus is appreciated after 20 seconds, the appreciated after 20 seconds, the patient is returned to the sitting patient is returned to the sitting

VESTIBULAR NEURONITIS VESTIBULAR NEURONITIS
DEF: DEF: Sudden spontaneous unilateral loss of vestibular Sudden spontaneous unilateral loss of vestibular functionfunctionAcute unilateral peripheral vestibulopathy, Acute unilateral peripheral vestibulopathy, Preserved hearingPreserved hearingNo other symptoms or signs of brainstem No other symptoms or signs of brainstem dysfunction, dysfunction,
Etiol:Etiol:-- Thought to be viral (HSV I)Thought to be viral (HSV I)Treatment Treatment –– Symptomatic Symptomatic
Benign Positional VertigoBenign Positional VertigoEtiol Etiol --
FreeFree--floating calcium carbonate crystals (normally attached to the floating calcium carbonate crystals (normally attached to the utricular macule) that inadvertently enter the long arm of the utricular macule) that inadvertently enter the long arm of the posterior semicircular canal. posterior semicircular canal.
Sx: Sx: Fatigable paroxysmal positional nystagmus after a rapid change fFatigable paroxysmal positional nystagmus after a rapid change from rom the sitting to the headthe sitting to the head--hanging position. No spontaneous nystagmus hanging position. No spontaneous nystagmus or hearing loss/tinnitus. Motion will worsen symptomsor hearing loss/tinnitus. Motion will worsen symptomsVery common in elderlyVery common in elderly
Tx: Tx: Remove crystals, or surgery to remove ampullary nerve Remove crystals, or surgery to remove ampullary nerve Must be distinguished from other causes of positional vertigo thMust be distinguished from other causes of positional vertigo that at may occur with tumors or infarcts of the posterior fossa if the may occur with tumors or infarcts of the posterior fossa if the Sx or Sx or treatment resolution is atypicaltreatment resolution is atypical
BENIGN POSITIONAL VERTIGOBENIGN POSITIONAL VERTIGO TreatmentTreatment
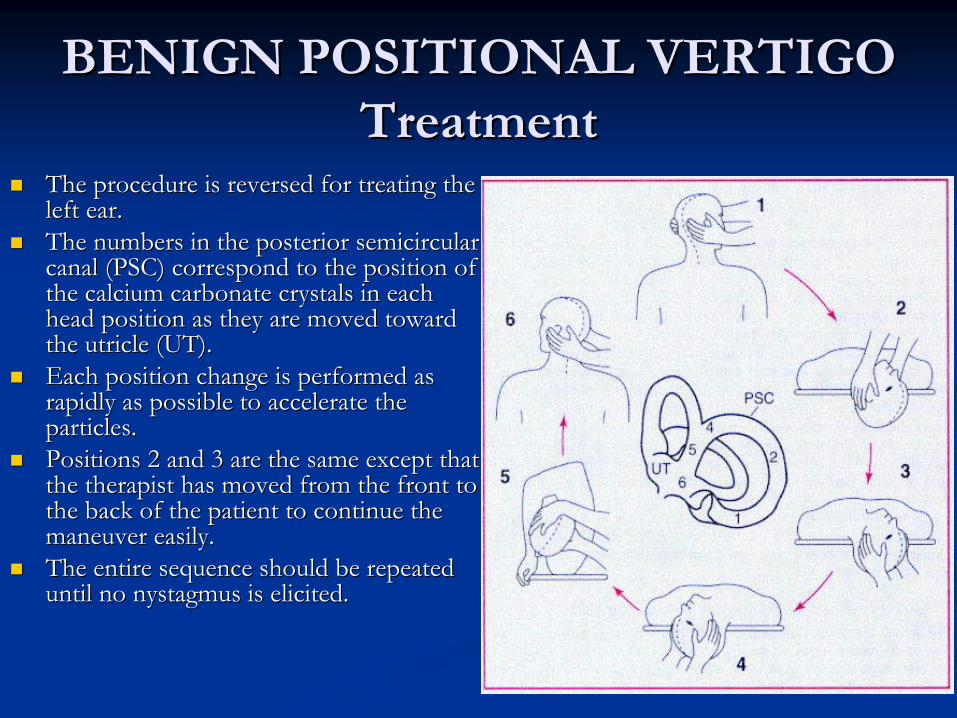
The procedure is reversed for treating the The procedure is reversed for treating the left ear. left ear. The numbers in the posterior semicircular The numbers in the posterior semicircular canal (PSC) correspond to the position of canal (PSC) correspond to the position of the calcium carbonate crystals in each the calcium carbonate crystals in each head position as they are moved toward head position as they are moved toward the utricle (UT). the utricle (UT). Each position change is performed as Each position change is performed as rapidly as possible to accelerate the rapidly as possible to accelerate the particles.particles.Positions 2 and 3 are the same except that Positions 2 and 3 are the same except that the therapist has moved from the front to the therapist has moved from the front to the back of the patient to continue the the back of the patient to continue the maneuver easily. maneuver easily. The entire sequence should be repeated The entire sequence should be repeated until no nystagmus is elicited. until no nystagmus is elicited.

MeniereMeniere’’s Diseases Disease
Classic Meniere's disease presents as a quadrad of paroxysmal Classic Meniere's disease presents as a quadrad of paroxysmal symptoms, includingsymptoms, including
1. Tinnitus, 1. Tinnitus, ringing noise between attacks ringing noise between attacks -- becomes a multifrequency noise such as a becomes a multifrequency noise such as a roar, hiss, or buzz. roar, hiss, or buzz. monaural fullness, a sensation as if the ear were full of water,monaural fullness, a sensation as if the ear were full of water, beginning a day beginning a day or two before an attackor two before an attackHearing is normal at the onset of the condition, but with each aHearing is normal at the onset of the condition, but with each attack a lowttack a low--frequency sensorineural reduction in hearing appears and it resofrequency sensorineural reduction in hearing appears and it resolves in 24 lves in 24 ––48 hrs. After many attacks, hearing will decline and involve the48 hrs. After many attacks, hearing will decline and involve the high high frequencies. Permanent sensorineuronal deafness appearsfrequencies. Permanent sensorineuronal deafness appears
2. Monaural fullness, 2. Monaural fullness, 3. Fluctuating hearing, 3. Fluctuating hearing, 4. Episodic vertigo. 4. Episodic vertigo.
MENIEREMENIERE’’S DISEASES DISEASE
This clinical picture is sometimes called the "hydrops" This clinical picture is sometimes called the "hydrops" symptom complex, inferring that the mechanism is symptom complex, inferring that the mechanism is related to dilation and rupture of the endolymphatic related to dilation and rupture of the endolymphatic compartment of the inner ear.compartment of the inner ear.TREATMENT:TREATMENT:
Meds: Antivert, Lorazepam, Scopolamine patch , Valium Meds: Antivert, Lorazepam, Scopolamine patch , Valium Some advocate diureticsSome advocate diureticsSURG: SURG: -- Destroy vestibular function. Destroy vestibular function. -- [a] labyrinthectomy, [a] labyrinthectomy, [b] selective vestibular nerve section, and [c] transtympanic. [b] selective vestibular nerve section, and [c] transtympanic. Gentamycin treatment is presently growing rapidly in Gentamycin treatment is presently growing rapidly in popularity. popularity.

ALCOHOL USE AND ABUSEALCOHOL USE AND ABUSE
Major DepressionMajor DepressionAnxiety DisordersAnxiety DisordersPsychosisPsychosis
***alcohol affects the viscosity of ***alcohol affects the viscosity of perilymphaticperilymphatic(inner ear) fluid, inducing vertiginous(inner ear) fluid, inducing vertiginous--type dizziness type dizziness ((““the room is spinningthe room is spinning””))
MIGRAINE MIGRAINE HEADACHESHEADACHES
Specifically Specifically ““basilarbasilar”” migrainesmigraines

MIGRAINE HEADACHEMIGRAINE HEADACHE
DIAGNOSIS DIAGNOSIS Five attacks with headache lasting 4 Five attacks with headache lasting 4 -- 72 hrs72 hrs
Headache with TWO of the followingHeadache with TWO of the followingUnilateral locationUnilateral location Pulsating quality Pulsating quality Intensity mod/severeIntensity mod/severe Exacerbated by routine activityExacerbated by routine activity
PLUS ONE OF THE FOLLOWINGPLUS ONE OF THE FOLLOWINGnauseanausea vomitingvomitingphotophobiaphotophobia phonophobiaphonophobia
PLUSPLUS
Hx / PE / Neuro Exam not suggestive of any other Hx / PE / Neuro Exam not suggestive of any other diseasedisease

MIGRAINE HEADACHEMIGRAINE HEADACHE TreatmentTreatment
Prophylaxis Prophylaxis -- when 3 when 3 -- 4 attacks / month occur4 attacks / month occurUSEFUL AGENTS FOR MIGRAINEUSEFUL AGENTS FOR MIGRAINE--RELATED RELATED DIZZINESSDIZZINESS
Ca Channel blockersCa Channel blockers(especially (especially VerapamilVerapamil
SR)SR)
AntiAnti--epileptic drugsepileptic drugs((TopamaxTopamax
and and DepakoteDepakote))
Seizure DISORDERSSeizure DISORDERS
Seizures Seizures ClassificationsClassifications
Partial SeizuresPartial SeizuresSimple Partial Seizures Simple Partial Seizures
Consciousness is preservedConsciousness is preservedClinical manifestations are relatively simpleClinical manifestations are relatively simpleMotor, sensory, autonomic or psychic Motor, sensory, autonomic or psychic SxSx, and yes, , and yes, even dizziness!even dizziness!Jacksonian March not unusualJacksonian March not unusualTodds ParalysisTodds ParalysisMay last days May last days -- Epilepsia partialis continuaEpilepsia partialis continuaAura may also occurAura may also occur
Seizures Seizures ClassificationsClassifications
Partial SeizuresPartial SeizuresComplex Partial SeizuresComplex Partial Seizures
Focal partial seizures Focal partial seizures Transient impairment of pt to deal with Transient impairment of pt to deal with
environmentenvironmentAura usually presentAura usually presentStart of ictal phase starts amnestic responseStart of ictal phase starts amnestic responseAutomatism presentAutomatism presentEEG EEG -- epileptiform spikesepileptiform spikes

SEIZURE MEDICAL SEIZURE MEDICAL THERAPY THERAPY
Selection of Antiepileptic DrugsSelection of Antiepileptic DrugsFIRST LINE THERAPYFIRST LINE THERAPY
Primary Generalized Tonic Clonic SeizurePrimary Generalized Tonic Clonic SeizureValproic AcidValproic Acid LamotrigineLamotrigine
Partial Partial CarbamazepineCarbamazepine DilantinDilantinValproic AcidValproic Acid LamotrigineLamotrigine
AbsenceAbsenceEthosuximideEthosuximide Valproic Acid Valproic Acid
Atypical Absence, Myoclonic, AtonicAtypical Absence, Myoclonic, AtonicValproic Acid Valproic Acid
BELLS PALSYBELLS PALSYDEF: 7DEF: 7thth Nerve paralysis Nerve paralysis –– peripheral (will include forehead)peripheral (will include forehead)ETIOL herpes simplex infection. ETIOL herpes simplex infection. CLIN SX CLIN SX
Peripheral CN VII dysfunction involving all distal branches;Peripheral CN VII dysfunction involving all distal branches;Sudden onset with maximal facial weakness usually reached withinSudden onset with maximal facial weakness usually reached within several several days; days; Impaired result on acoustic reflex test in 90 percent; Impaired result on acoustic reflex test in 90 percent; Viral prodrome in 60 percent; Viral prodrome in 60 percent; Numbness or pain of the ear, tongue, or face in 50 percent; Numbness or pain of the ear, tongue, or face in 50 percent; chorda tympani nerve appears red in 40 percent; chorda tympani nerve appears red in 40 percent; Reduction in ipsilateral tearing or salivary flow in 10 percentReduction in ipsilateral tearing or salivary flow in 10 percentSpontaneous improvement within 6 months.[Spontaneous improvement within 6 months.[33] ] REM: Central lesions spare the frontalis muscleREM: Central lesions spare the frontalis muscle
TREATMENT: Acyclovir and steroids,(hasten the recovery and TREATMENT: Acyclovir and steroids,(hasten the recovery and to lessen the ultimate degree of dysfunction)to lessen the ultimate degree of dysfunction)

HEARING LOSS HEARING LOSS ––
88thth
NerveNerve
Etiol: Etiol: Mass Lesions : Mass Lesions :
Acoustic SchannomaAcoustic SchannomaCerebellopontine angle tumor (CPA)Cerebellopontine angle tumor (CPA)
SYMPTOMSSYMPTOMSVertigo, Hearing loss, AtaxiaVertigo, Hearing loss, Ataxia
TREATMENTTREATMENTTreat underlying cause Treat underlying cause SurgerySurgery
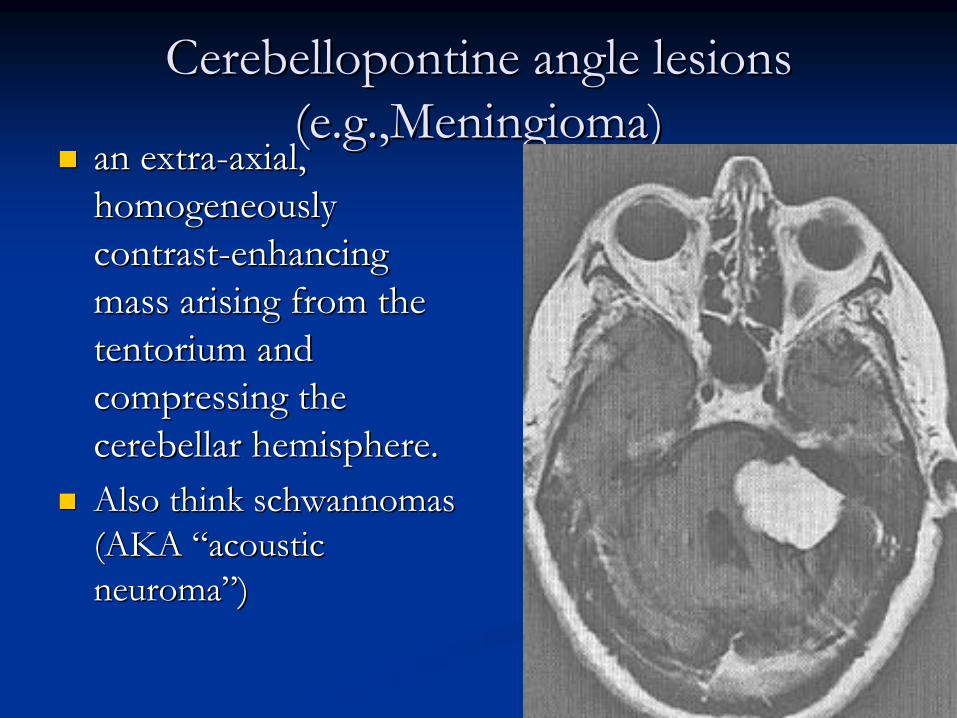
CerebellopontineCerebellopontine
angle lesions angle lesions ((e.g.,Meningiomae.g.,Meningioma))
an extraan extra--axial, axial, homogeneously homogeneously contrastcontrast--enhancing enhancing mass arising from the mass arising from the tentoriumtentorium and and compressing the compressing the cerebellar hemisphere.cerebellar hemisphere.Also think Also think schwannomasschwannomas(AKA (AKA ““acoustic acoustic neuromaneuroma””))
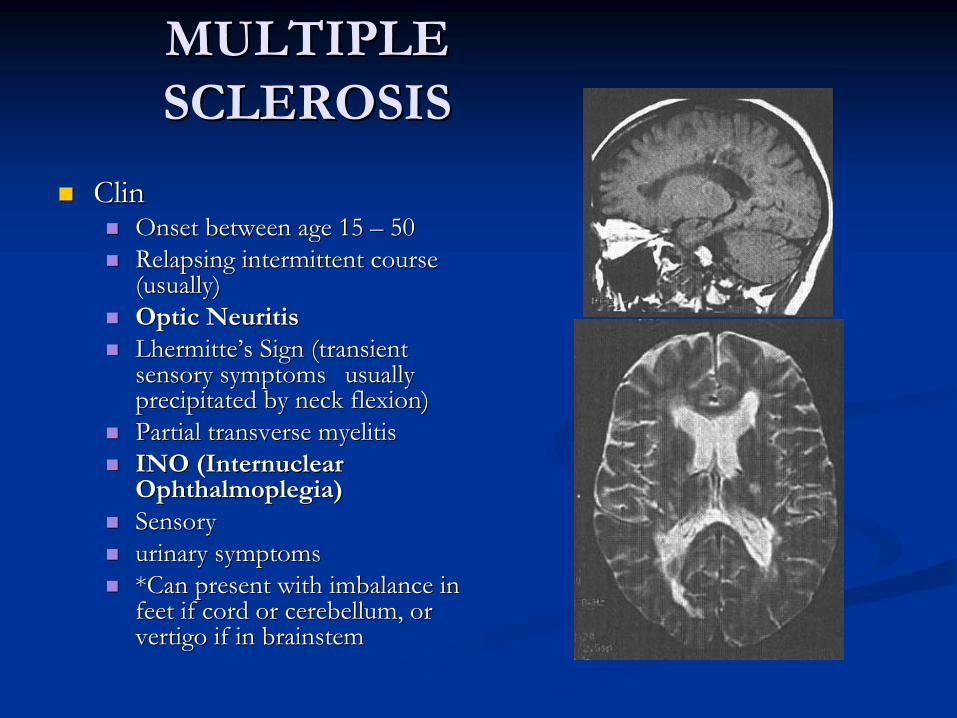
MULTIPLE MULTIPLE SCLEROSISSCLEROSIS
ClinClinOnset between age 15 Onset between age 15 –– 5050Relapsing intermittent course Relapsing intermittent course (usually)(usually)Optic NeuritisOptic NeuritisLhermitteLhermitte’’s Sign (transient s Sign (transient sensory symptoms sensory symptoms usually usually precipitated by neck flexion)precipitated by neck flexion)Partial transverse myelitis Partial transverse myelitis INO (Internuclear INO (Internuclear Ophthalmoplegia)Ophthalmoplegia)Sensory Sensory urinary symptomsurinary symptoms*Can present with imbalance in *Can present with imbalance in feet if cord or cerebellum, or feet if cord or cerebellum, or vertigo if in brainstem vertigo if in brainstem
STROKESTROKE
TYPES OF STROKESTYPES OF STROKES RISK FACTORSRISK FACTORSEmbolic Embolic --
RF RF -- Afib, Mitral Stenosis, Endocarditis, Prosthesis, MIAfib, Mitral Stenosis, Endocarditis, Prosthesis, MI
HemorrhagicHemorrhagic--RF RF -- AV malf, Aorta coarctation, Polycystic disease, HBPAV malf, Aorta coarctation, Polycystic disease, HBP
Ischemic Ischemic ––RF:DM, Tobacco, HBP, Card Disease (BCP females)RF:DM, Tobacco, HBP, Card Disease (BCP females)
TRANSIENT ISCHEMIC TRANSIENT ISCHEMIC ATTACKATTACK
TIA TIA --DEF: DEF: --Neuro deficit that resolves within 24 hrs Neuro deficit that resolves within 24 hrs (most do in < 1 hr)(most do in < 1 hr)Harbinger of stroke in < 5 yrs Harbinger of stroke in < 5 yrs –– 25% 25% Tx: Low dose Aspirin / Platelet inhibitorsTx: Low dose Aspirin / Platelet inhibitors

BLOOD BLOOD FLOW FLOW
Vessels forming the circle of Willis Vessels forming the circle of Willis are highlighted in dark red. are highlighted in dark red. Abbreviations for intracranial and Abbreviations for intracranial and extracranial arteries are as follows: extracranial arteries are as follows: ACA = anterior cerebral artery; ACA = anterior cerebral artery; MCA = middle cerebral artery; MCA = middle cerebral artery; PCA = posterior cerebral artery; PCA = posterior cerebral artery; EE--I anast = extralI anast = extral--intracranial intracranial anastomosisanastomosisICA = internal carotid artery; ICA = internal carotid artery; ECA = external carotid artery; ECA = external carotid artery; CCA = common carotid artery;CCA = common carotid artery;Ant. Comm. = anterior Ant. Comm. = anterior communicating artery;communicating artery;Post. Comm. = posterior Post. Comm. = posterior communicating artery;communicating artery;SCA = superior cerebellar artery; SCA = superior cerebellar artery; AICA = anterior inferior cerebellar AICA = anterior inferior cerebellar artery; artery; PICA = posterior inferior cerebellar PICA = posterior inferior cerebellar artery. artery. .).)
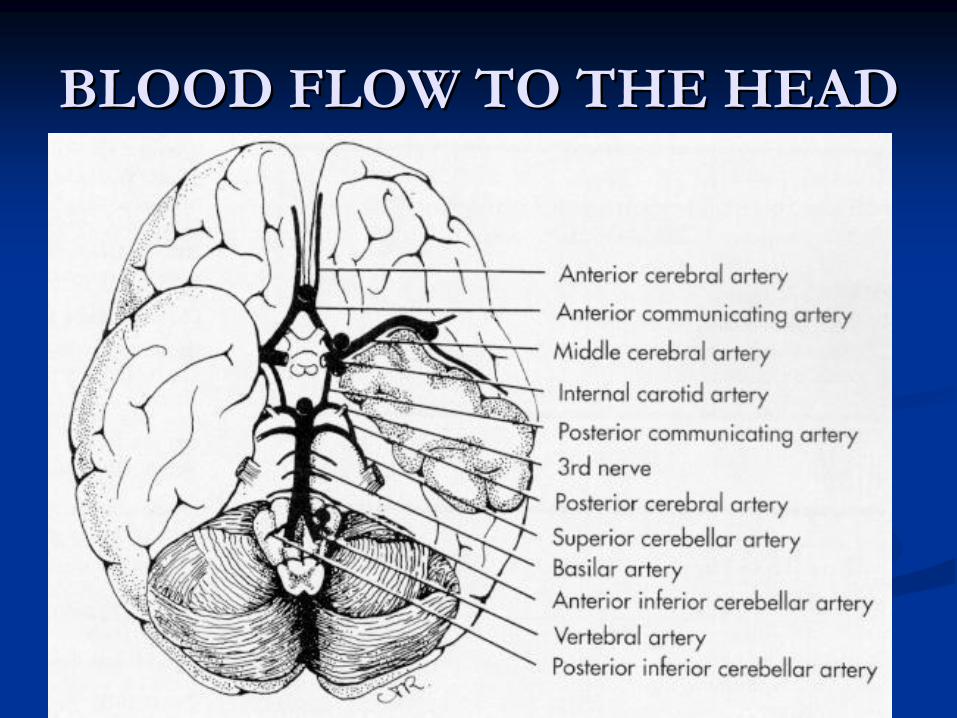
BLOOD FLOW TO THE HEADBLOOD FLOW TO THE HEAD
BASILAR ATERYBASILAR ATERYANATOMY; The ANATOMY; The basilarbasilar
arteryartery
gives rise to gives rise to
perforating branches as it spans the ventral perforating branches as it spans the ventral midline midline ponspons
and midbrain These short and midbrain These short
perpendicular branches distribute blood to the perpendicular branches distribute blood to the paramedianparamedian
structures, including the structures, including the
corticospinal tracts, the corticospinal tracts, the pontinepontine
reticular nuclei, reticular nuclei, the medial the medial lemniscilemnisci, the medial longitudinal , the medial longitudinal fasciculifasciculi, and the , and the pontinepontine
reticular nucleireticular nuclei
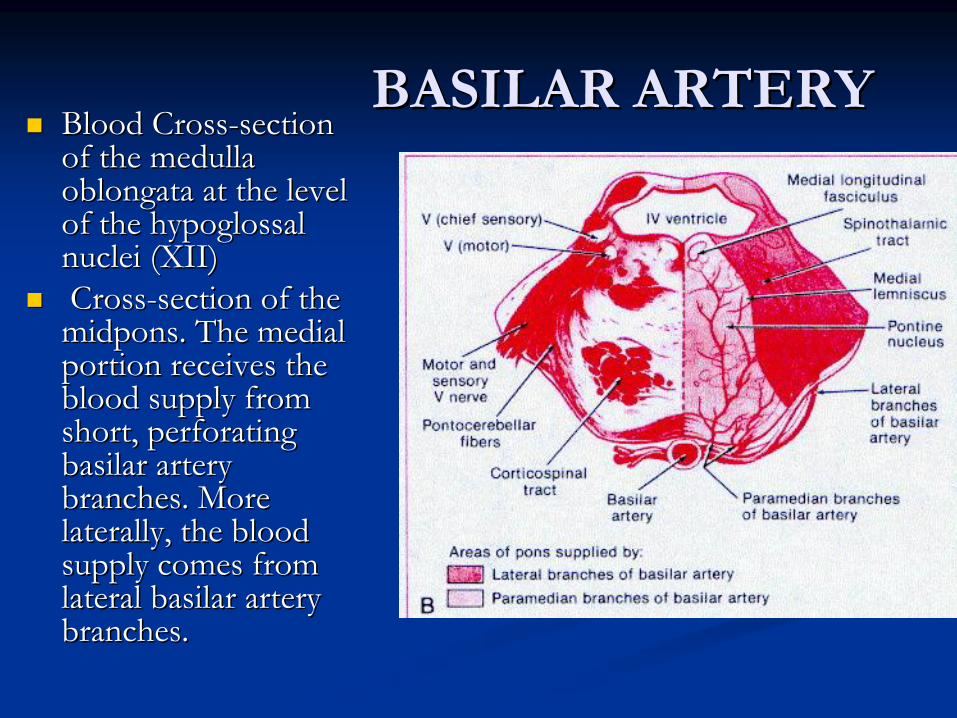
BASILAR ARTERYBASILAR ARTERYBlood CrossBlood Cross--section section of the medulla of the medulla oblongata at the level oblongata at the level of the hypoglossal of the hypoglossal nuclei (XII)nuclei (XII)CrossCross--section of the section of the
midponsmidpons. The medial . The medial portion receives the portion receives the blood supply from blood supply from short, perforating short, perforating basilar artery basilar artery branches. More branches. More laterally, the blood laterally, the blood supply comes from supply comes from lateral basilar artery lateral basilar artery branches.branches.
SUPERIOR CEREBELLAR SUPERIOR CEREBELLAR ARTERYARTERY
Supplies: most of the cerebellar cortex. Supplies: most of the cerebellar cortex. Occlusion of this vessel is the most common cause of Occlusion of this vessel is the most common cause of cerebellar cerebellar infarction,infarction,CLIN: CLIN:
gait ataxia, gait ataxia, headache, headache, nausea, vomiting, nausea, vomiting, dizziness, dizziness, ipsilateral clumsiness, ipsilateral clumsiness, dysarthria. dysarthria. ipsilateral gaze paresis and/or nystagmus toward the side of theipsilateral gaze paresis and/or nystagmus toward the side of theinfarction; infarction; Cerebellar edema formation can obstruct the fourth ventricle, prCerebellar edema formation can obstruct the fourth ventricle, producing oducing hydrocephalus, and can result in herniation of the cerebellum eihydrocephalus, and can result in herniation of the cerebellum either ther upward across the tentorium or downward through the foramen upward across the tentorium or downward through the foramen magnum. magnum. *also think anterior inferior *also think anterior inferior cerebellarcerebellar artery (AICA) and posterior artery (AICA) and posterior inferior inferior cerebellarcerebellar artery (PICA)artery (PICA)

MAJOR DEPRESSIONMAJOR DEPRESSIONDIFFERENTIAL DX DIFFERENTIAL DX
BereavementBereavementAdjustment Disorder with depressed mood Adjustment Disorder with depressed mood Alcohol DependenceAlcohol DependenceCocaine / Amphetamine DependenceCocaine / Amphetamine DependencePersonality DisorderPersonality DisorderSomatization DisorderSomatization DisorderObsessive Compulsive Disorder (OCD)Obsessive Compulsive Disorder (OCD)Panic DisorderPanic Disorder
TREATMENT TREATMENT Regardless of the cause (or the explainability) patients who Regardless of the cause (or the explainability) patients who meet criteria for a major depressive episode should receive meet criteria for a major depressive episode should receive antidepressant therapyantidepressant therapy
PANIC DISORDERPANIC DISORDER
Disorder consists of recurrent panic attacksDisorder consists of recurrent panic attacksCan be associated with agoraphobiaCan be associated with agoraphobiaDiagnostic CriteriaDiagnostic Criteria
Recurrent unexpected panic attacksRecurrent unexpected panic attacks

PANIC DISORDERPANIC DISORDER
6. OCD6. OCD7. Post traumatic stress 7. Post traumatic stress Disorder (PTSD)Disorder (PTSD)8. Separation Anxiety 8. Separation Anxiety Disorder (SAD)Disorder (SAD)9. Hyperthyroidism9. Hyperthyroidism10. Hypoglycemia10. Hypoglycemia11. Hypoxia11. Hypoxia12. Medication/substance 12. Medication/substance induced (e.g. caffeine, induced (e.g. caffeine, 13. Myocardial ischemia13. Myocardial ischemia
Age of onsetAge of onsetFrom the late adolescence From the late adolescence through the mid 30through the mid 30’’ssPrevalence Prevalence
3 3 -- 5 % lifetime prevalence5 % lifetime prevalenceWomen are 2 Women are 2 -- 3 x more 3 x more likely to be affected than likely to be affected than menmen
Natural history Natural history -- chronic illness chronic illness that waxes and wanesthat waxes and wanes
Other psychiatric DisturbancesOther psychiatric Disturbances1. Major Depression1. Major Depression2. Substance Dependence2. Substance Dependence3. Substance withdrawal 3. Substance withdrawal (Alcohol, Benzodiazepines)(Alcohol, Benzodiazepines)4. Social phobia4. Social phobia5. Generalized anxiety disorder5. Generalized anxiety disorder

OBSESSIVE COMPULSIVE OBSESSIVE COMPULSIVE DISORDER (OCD)DISORDER (OCD)
Age of onsetAge of onsetUsually in adolescence or early adulthoodUsually in adolescence or early adulthood
May begin in childhoodMay begin in childhoodEarlier in males than in femalesEarlier in males than in females
PrevalencePrevalence2.5% (lifetime) but his might be substantially higher than reali2.5% (lifetime) but his might be substantially higher than reality ty because of poor validitybecause of poor validity
Natural HxNatural HxTypically , onset is gradual but acute onset has been noted i soTypically , onset is gradual but acute onset has been noted i some me casescasesThe majority of individuals have a chronic waxing and waning couThe majority of individuals have a chronic waxing and waning course rse with exacerbation of symptoms that may be related to stresswith exacerbation of symptoms that may be related to stress
OBSESSIVE COMPULSIVE OBSESSIVE COMPULSIVE DISORDER DISORDER --
DIFF Dx DIFF Dx
Bilateral Bilateral GlobusGlobusPallidusPallidus lesionslesionsCarbon Monoxide Carbon Monoxide PoisoningPoisoningManganese PoisoningManganese PoisoningEncephalitis Encephalitis lethargicalethargica
SydenhamSydenham’’ss ChoreaChorea
Major DepressionMajor Depression
Panic DisorderPanic DisorderGeneralized Anxiety Generalized Anxiety DisorderDisorderTrichotillomaniaTrichotillomaniaAnorexia NervosaAnorexia Nervosa
Impulse Control Impulse Control DisorderDisorderTouretteTourette’’s Disorders Disorder

NORMAL PRESSURE NORMAL PRESSURE HYDROCELPHALUS (NPH)HYDROCELPHALUS (NPH)
Clinical Triad Clinical Triad Wide gait disturbance (ataxia)Wide gait disturbance (ataxia)DementiaDementiaUrinary IncontinenceUrinary Incontinence
LABS: LABS: Dilated ventricles on CTDilated ventricles on CTLP has high opening pressureLP has high opening pressureNo Cortical atrophyNo Cortical atrophy
Brain : Communicating hydrocephalus and patent Aqueduct of Brain : Communicating hydrocephalus and patent Aqueduct of SylviusSylviusTREATMENT: Shunt placement TREATMENT: Shunt placement
Gait may improve more than memoryGait may improve more than memory
NeuropathiesNeuropathies
““dizzinessdizziness””
is actually imbalanceis actually imbalance
*diabetes and *diabetes and etohetoh
account for about 90% of account for about 90% of chronic neuropathies in North Americachronic neuropathies in North America
*also think B12 deficiency and tertiary *also think B12 deficiency and tertiary syphillissyphillis

GUILLIANGUILLIAN--BARRE (GB) BARRE (GB) SYNDROMESYNDROME
General General Acute, severe, progressive, fulminant polyradiculopathy Acute, severe, progressive, fulminant polyradiculopathy Autoimmune Autoimmune –– results from immune responses against results from immune responses against various various componenetscomponenets of peripheral nerve fibers of peripheral nerve fibers Demyelinating disease causes conduction block of Demyelinating disease causes conduction block of nerves nerves

summarysummaryDifferentiate between head and feet, then Differentiate between head and feet, then lightheadedness vs. vertigo (versus simple visual lightheadedness vs. vertigo (versus simple visual blurring)blurring)Keep a wide differential diagnosisKeep a wide differential diagnosisTreat causes that can be treatedTreat causes that can be treated