Distribution of the Mr 52,000 Estrogen-regulated Protein in Benign ... · (ovary, placenta,...
5
[CANCER RESEARCH 46, 3734-3738, July 1986] Distribution of the Mr 52,000 Estrogen-regulated Protein in Benign Breast Diseases and Other Tissues by Immunohistochemistry1 Marcel Garcia, Guillermo Salazar-Retana, AndréPages, Gilbert Richer, J. Domergue, Anne Marie Pages, Ghislaine Cavalle, Jean Michel Martin, Jean-Louis Lamarque, Bernard Pau, Henri Pujol, and Henri Rochefort Unité d'Endocrinologie Cellulaire el Moléculaire,V 148, Institut National de la Santéet de la Recherche Médicale, 60, Rue de Navacelles, 34100 Montpellier [M. G., G. S-R., G. C., H. R.J; Laboratoire d'Anatomie Pathologique, Centre Médico-ChirurgicalGui-de-Chauliac, HôpitalSaint-Eloi, 2, Avenue Bertin Sans, 34059 Montpellier Cedex {A. P., A. M. P.]; Centre de Recherche Clin-Midy/Sanofi. Immunologie, Rue du Professeur Joseph Blayac, 34082 Montpellier Cedex [G. R., B. P.]; Centre Paul Lamarque, 2, Avenue BéninSans—HP5054, 34033 Montpellier Cedex [J. D., H. P.]; Départementd'imagerie Médicale, Hôpital Lapeyronie, 555, Route de Ganges, 34059 Montpellier Cedex [J. M. M., J-L. L.J; and Laboratoire de Biochimie Cellulaire, Facultéde Médecine, 2, Rue de l'Ecole de Médecine, 34060 Montpellier Cedex [G. C., H. R.l, France ABSTRACT A secreted glycoprotein with a molecular weight of 52,000 is induced by estrogen in breast cancer cells and has been purified to prepare monoclonal antibodies. The protein has been detected in some breast cancers but not in normal breast and uterus. In order to study its potential value as a marker, we have tested by immunohistochemistry frozen sections of several normal and malignant tissues and of benign mastopa- thies. Among different tissues tested, the M, 52,000 protein was detected only in liver, sweat glands, and some sebaceous glands, and in malignant melanomas and some breast tumors. Other estrogen-responsive tissues (ovary, placenta, endometrium, etc.) gave negative results. Immunoradiometric assay of the M, 52,000 protein in biological fluid revealed an elevated concentration in cyst fluid (0.5 to 7.4 nu/ml). pleural effusions of certain metastatic breast cancer, and sweat. By immunohistochemistry, the \1, 52,000 antigen was also detected in 42% of 129 benign mastopathies. Gynecomastia, fibrous disease, fibro adenoma, and adenosis were mainly negative, whereas ductal hyperplasia and cysts were positive. The M, 52,000 protein was found mostly in proliferative ducts and in cysts but not in lobular hyperplasia and non- proliferative lesions without cyst. More M, 52,000 protein was found in postmenopausal patients than in premenopausal patients. We conclude that the M, 52,000 protein is a marker associated with mammary cysts and proliferative ducts. On the basis of the increased risk of breast cancer in proliferative mastopathies, we suggest that the M, 52,000 protein is useful for predicting high-risk mastopathies acting as a marker associated with the proliferation of ductal tissue. INTRODUCTION An increasing number of monoclonal antibodies to mammary cancer antigens or purified proteins are available (1-7). These antibodies are used as markers of mammary tissue, as cancer associated markers, or as markers of hormone dependency in breast cancer; however, few markers if any (8) are available for detecting the early steps of cancerogenesis and for discrimina ting high-risk mastopathies (9, 10) from benign mastopathies, which have been defined as non-disease entities (11). Recently, Dupont and Page (12) have indicated that proliferative lesions are more exposed to breast cancer risk and some can be consid ered to be precancerous lesions, whereas the majority of these mastopathies (70%) are nonproliferative and not exposed to breast cancer risk. Since the current pathological grading of benign lesions is time consuming and may be subjective, bio chemical markers would be more useful in helping pathologists to define these high-risk mastopathies. We have developed several monoclonal antibodies (13) to an estrogen-regulated protein secreted by metastatic breast cancer Received 12/4/85; revised 3/13/86; accepted 3/17/86. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1Preliminary results have been reported at the International Congress of Gynecology and Obstetrics (Berlin. Germany, September 15-20, 1985), at the International Symposium on Monoclonal Antibodies (Florence. Italy, October 2-4, 1985), and in Ref. I. This work was supported by INSERM-SANOFI Contract 81039, the Facultéde MédecineMontpellier, and the Ligne Nationale de Lutte contre le Cancer. cells in culture and defined by its molecular weight of 52,000 in sodium dodecyl sulfate-polyacrylamide gel electrophoresis (14-16). Using immunoperoxidase staining of frozen sections of tissue biopsies in a preliminary study, we have detected this protein (or an immunologically related protein) in 75% of the breast cancers analyzed but not in endometrium or norma' resting mammary glands (17). In order to specify the clinical potential of this protein as a marker, we have studied its distribution in several normal and tumoral tissues and in 129 benign mastopathies of different histológica! types. MATERIALS AND METHODS Breast Biopsies. Breast biopsies were performed for diagnostic pur poses in patients undergoing surgery for lumps. Most of the tissues were sent to pathologists for routine analysis and the remaining por tions were immediately frozen in liquid nitrogen. Serial frozen sections were made from a tissue block, and one of 3 adjacent sections containing epithelial structures was analyzed for histológica! grading by a pathol ogist while the others were processed independently for immunodetec- tion of the M, 52,000 protein and reviewed by two different observers. Thirteen samples were subsquently excluded because they were found to be invasive or in situ mammary cancers or they lacked breast epithelial cells; 129 samples remained for analysis. Immunohistochemical Staining of the M, 52,000 Protein. Eight-mm thick frozen sections, quickly fixed by cold acetone, were stained by the Sternberger (18) peroxidase-antiperoxidase method as previously de scribed (17), using the D7E3 or M1G8 antibody (5 ng/ml) in some cases. Each staining series was associated with a positive control per formed with a positive breast cancer tissue and a negative control performed with an irrelevant monoclonal antibody (IgGl; MOPC21, Bionetics) of the same subclass. In 30 cases duplicate experiments on serial sections from the same tissue block gave similar results. The staining was quantified according to the estimated percentage of posi tive epithelial cells in the total of 2,000 to 50,000 cells examined and was graded from 0 (no positive cells) to + (1 to 5% positive epithelial cells) and to ++ (>5% positive epithelial cells). In positive benign mastopathies, the staining intensity was not taken into consideration since it was high in the majority of cases. Each section was graded for staining independently by two observers. In case of a discrepancy, a consensus was reached by the two observers or additional sections were analyzed. Pathological Examination. This was performed after fixation and staining by hematoxylin and eosin. Each biopsy was classified according to the methods of Azzopardi (9) and Haagensen et al. (10) on the basis of cystic or noncystic lesions, and according to the criteria of Page et al. (19) on the basis of proliferative or nonproliferative lesions. The clinical history of each patient, hormonal status, age, and treatment were recorded. Immunoradiometric Assay of the M, 52,000 Protein in Fluids. This was performed by a two-site solid phase assay as previously described (13). An adaptation of this assay to biological fluids was performed after validation of the assay by recovery experiments. Data were ex pressed as M, 52,000 protein, ng per ml, according to a standard curve assayed in parallel using the secreted M, 52,000 protein purified from human breast cancer (MCF7) and quantified by silver-stained sodium 3734
Transcript of Distribution of the Mr 52,000 Estrogen-regulated Protein in Benign ... · (ovary, placenta,...

[CANCER RESEARCH 46, 3734-3738, July 1986]
Distribution of the Mr 52,000 Estrogen-regulated Protein in Benign Breast Diseasesand Other Tissues by Immunohistochemistry1
Marcel Garcia, Guillermo Salazar-Retana, AndréPages, Gilbert Richer, J. Domergue, Anne Marie Pages,Ghislaine Cavalle, Jean Michel Martin, Jean-Louis Lamarque, Bernard Pau, Henri Pujol, and Henri RochefortUnitéd'Endocrinologie Cellulaire el Moléculaire,V 148, Institut National de la Santéet de la Recherche Médicale,60, Rue de Navacelles, 34100 Montpellier [M. G.,G. S-R., G. C., H. R.J; Laboratoire d'Anatomie Pathologique, Centre Médico-ChirurgicalGui-de-Chauliac, HôpitalSaint-Eloi, 2, Avenue Bertin Sans, 34059 MontpellierCedex {A. P., A. M. P.]; Centre de Recherche Clin-Midy/Sanofi. Immunologie, Rue du Professeur Joseph Blayac, 34082 Montpellier Cedex [G. R., B. P.]; Centre PaulLamarque, 2, Avenue BéninSans—HP5054, 34033 Montpellier Cedex [J. D., H. P.]; Départementd'imagerie Médicale,Hôpital Lapeyronie, 555, Route de Ganges,34059 Montpellier Cedex [J. M. M., J-L. L.J; and Laboratoire de Biochimie Cellulaire, Facultéde Médecine,2, Rue de l'Ecole de Médecine,34060 Montpellier Cedex
[G. C., H. R.l, France
ABSTRACT
A secreted glycoprotein with a molecular weight of 52,000 is inducedby estrogen in breast cancer cells and has been purified to preparemonoclonal antibodies. The protein has been detected in some breastcancers but not in normal breast and uterus. In order to study its potentialvalue as a marker, we have tested by immunohistochemistry frozensections of several normal and malignant tissues and of benign mastopa-thies. Among different tissues tested, the M, 52,000 protein was detectedonly in liver, sweat glands, and some sebaceous glands, and in malignantmelanomas and some breast tumors. Other estrogen-responsive tissues(ovary, placenta, endometrium, etc.) gave negative results.
Immunoradiometric assay of the M, 52,000 protein in biological fluidrevealed an elevated concentration in cyst fluid (0.5 to 7.4 nu/ml). pleuraleffusions of certain metastatic breast cancer, and sweat.
By immunohistochemistry, the \1, 52,000 antigen was also detected in42% of 129 benign mastopathies. Gynecomastia, fibrous disease, fibroadenoma, and adenosis were mainly negative, whereas ductal hyperplasiaand cysts were positive. The M, 52,000 protein was found mostly inproliferative ducts and in cysts but not in lobular hyperplasia and non-proliferative lesions without cyst. More M, 52,000 protein was found inpostmenopausal patients than in premenopausal patients.
We conclude that the M, 52,000 protein is a marker associated withmammary cysts and proliferative ducts. On the basis of the increasedrisk of breast cancer in proliferative mastopathies, we suggest that theM, 52,000 protein is useful for predicting high-risk mastopathies actingas a marker associated with the proliferation of ductal tissue.
INTRODUCTIONAn increasing number of monoclonal antibodies to mammary
cancer antigens or purified proteins are available (1-7). Theseantibodies are used as markers of mammary tissue, as cancerassociated markers, or as markers of hormone dependency inbreast cancer; however, few markers if any (8) are available fordetecting the early steps of cancerogenesis and for discriminating high-risk mastopathies (9, 10) from benign mastopathies,which have been defined as non-disease entities (11). Recently,Dupont and Page (12) have indicated that proliferative lesionsare more exposed to breast cancer risk and some can be considered to be precancerous lesions, whereas the majority of thesemastopathies (70%) are nonproliferative and not exposed tobreast cancer risk. Since the current pathological grading ofbenign lesions is time consuming and may be subjective, biochemical markers would be more useful in helping pathologiststo define these high-risk mastopathies.
We have developed several monoclonal antibodies (13) to anestrogen-regulated protein secreted by metastatic breast cancer
Received 12/4/85; revised 3/13/86; accepted 3/17/86.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Preliminary results have been reported at the International Congress ofGynecology and Obstetrics (Berlin. Germany, September 15-20, 1985), at theInternational Symposium on Monoclonal Antibodies (Florence. Italy, October2-4, 1985), and in Ref. I. This work was supported by INSERM-SANOFIContract 81039, the Facultéde MédecineMontpellier, and the Ligne Nationalede Lutte contre le Cancer.
cells in culture and defined by its molecular weight of 52,000in sodium dodecyl sulfate-polyacrylamide gel electrophoresis(14-16). Using immunoperoxidase staining of frozen sectionsof tissue biopsies in a preliminary study, we have detected thisprotein (or an immunologically related protein) in 75% of thebreast cancers analyzed but not in endometrium or norma'resting mammary glands (17).
In order to specify the clinical potential of this protein as amarker, we have studied its distribution in several normal andtumoral tissues and in 129 benign mastopathies of differenthistológica! types.
MATERIALS AND METHODS
Breast Biopsies. Breast biopsies were performed for diagnostic purposes in patients undergoing surgery for lumps. Most of the tissueswere sent to pathologists for routine analysis and the remaining portions were immediately frozen in liquid nitrogen. Serial frozen sectionswere made from a tissue block, and one of 3 adjacent sections containingepithelial structures was analyzed for histológica!grading by a pathologist while the others were processed independently for immunodetec-tion of the M, 52,000 protein and reviewed by two different observers.
Thirteen samples were subsquently excluded because they were foundto be invasive or in situ mammary cancers or they lacked breastepithelial cells; 129 samples remained for analysis.
Immunohistochemical Staining of the M, 52,000 Protein. Eight-mmthick frozen sections, quickly fixed by cold acetone, were stained by theSternberger (18) peroxidase-antiperoxidase method as previously described (17), using the D7E3 or M1G8 antibody (5 ng/ml) in somecases. Each staining series was associated with a positive control performed with a positive breast cancer tissue and a negative controlperformed with an irrelevant monoclonal antibody (IgGl; MOPC21,Bionetics) of the same subclass. In 30 cases duplicate experiments onserial sections from the same tissue block gave similar results. Thestaining was quantified according to the estimated percentage of positive epithelial cells in the total of 2,000 to 50,000 cells examined andwas graded from 0 (no positive cells) to + (1 to 5% positive epithelialcells) and to ++ (>5% positive epithelial cells). In positive benignmastopathies, the staining intensity was not taken into considerationsince it was high in the majority of cases.
Each section was graded for staining independently by two observers.In case of a discrepancy, a consensus was reached by the two observersor additional sections were analyzed.
Pathological Examination. This was performed after fixation andstaining by hematoxylin and eosin. Each biopsy was classified accordingto the methods of Azzopardi (9) and Haagensen et al. (10) on the basisof cystic or noncystic lesions, and according to the criteria of Page etal. (19) on the basis of proliferative or nonproliferative lesions. Theclinical history of each patient, hormonal status, age, and treatmentwere recorded.
Immunoradiometric Assay of the M, 52,000 Protein in Fluids. Thiswas performed by a two-site solid phase assay as previously described(13). An adaptation of this assay to biological fluids was performedafter validation of the assay by recovery experiments. Data were expressed as M, 52,000 protein, ng per ml, according to a standard curveassayed in parallel using the secreted M, 52,000 protein purified fromhuman breast cancer (MCF7) and quantified by silver-stained sodium
3734

M, 52,000 ESTROGEN-REGULATED PROTEIN IN BENIGN BREAST DISEASE
Table 1 Immunoperoxidase staining ofM, 52,000 protein in human tissuesThe binding of the monoclonal antibody D7E3 was detected in frozen tissue sections by an indirect immunoperoxidase technique described in "Materials and
Methods." Tissues were classified as positive when at least 1% of one cell type population was specifically stained.
NormaltissueNegative
PositiveBreast(8)° Liver(9)Endometrium
(9) Sweat glands(4)Ovary(4) Sebaceous glands(4)Kidney
(3)Lung(l)Thymus
(4)Placenta(3)Brain(1)Prostate(1)Parotid(2)Appendix(1)Amygdala(1)Spleen(2)Striated
muscle(3)Lymphnodes(3)Epidermis
(10)Dermis(10)Hair
follicle(10)Sebaceousglands (3)CancerNegative
PositiveBreast
(8) Breast(24)Melanoma(3) Melanoma(5)Uterus
(3)Ovary(1)Colon(1)Lung(4)Osteosarcoma
(1)Sarcoma(1)Lymphoma(l)Bladder
(1)Benign
tumorsNegative
PositiveMastopathies
(71) Mastopathies(54)Gynecomastia(4)Naevi
(6)•
Numbers in parentheses, number of different patients.
dodecyl sulfate-gels.2
Statistics. Statistical significance of the difference between twogroups was determined by the x2 test.
RESULTS
Tissue Distribution of the M, 52,000 Protein. Preliminarystudies indicated that the M, 52,000 protein was not an estrogen-regulated marker like the progesterone receptor or the M,24,000 protein (4), since it was absent from endometrium (17).We completed the tissue distribution analysis of the M, 52,000protein by studying different normal and tumoral tissues (Table1). The protein, which was initially detected in some prolifera-tive mammary cancer cells, was not detected in other endocrine-related tissues (endometrium, placenta, ovary, prostate) andother tissues. The only other positive tissues were liver andskin. In liver, the staining was homogeneous throughout thetissue with a relatively high nonspecific background. In skin,the only positivity was seen in some sebaceous and in sweatglands. This last staining is in agreement with the high content(2 Mg/ml) of an immunologically related M, 52,000 protein insweat, as assayed by immunoradiometric assay (as shown later).Among other cancers, five malignant melanomas of eight werefound to be positive, whereas nevocellular nevi were all negative.In two cases, progressive invasion of lymph nodes by stainedmetastatic melanoma cells were evidenced. This marker maytherefore be very useful for detecting malignant melanomas andtheir metastasis. By contrast, the three endometrial cancerswere not stained. The M, 52,000 protein is therefore not ageneral marker of estrogen-responsive tumors, as is the progesterone receptor. It may, however, be related to the high metastatic potential of cancers such as breast cancer and malignantmelanoma.
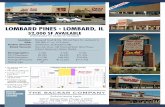
Distribution of the M, 52,000 Protein in Benign Breast Diseases. No staining was observed in 8 resting mammary glandscollected during reduction mammoplasties, as previously described (17), but we detected the M, 52,000 protein antigen in43.2% of the benign mastopathies which were biopsied. Fig. 1shows typical positive sections obtained in a ductal hyperplasia(Fig. la) and a cyst (Fig. \t>)without counterstaining the nuclei.The brown staining is mostly cytoplasmic. Contrary to breastcancer tissue, where staining was most often heterogeneous,
: M. Garcia et al., submitted for publication.
with a majority of negative cancer cells, the staining in positivebenign mastopathies was more intense and homogeneous, involving as much as 100% of the mammary epithelial cells.Connective tissue was not stained. All cysts with a diameter ofmore than 3 mm were positive in the epithelial cells borderingthe lumen (Fig. 1Z>),and had apocrine cells. In 5 of 54 positivecases, the staining was also observed in nonepithelial cells(probably macrophages) surrounding positive ductal hyperpla-sias. Lobuloalveolar structures (Fig. \c) were mostly negativewhether the lesions were associated with a risk factor (atypicallobular hyperplasia) or not (adenosis or sclerosing adenosis);thus, of the proliferative lesions, only ductal hyperplasias werepositive for the M, 52,000 protein. The overall distribution ofthe M, 52,000 protein in the different histological types issummarized in Table 2. All gynecomastias were negative; fibroadenoma (Fig. li/) and fibrous mastopathies were most oftennegative. When the different histological types were pooled intoproliferative (high risk) and nonproliferative (low risk) lesions,there was a clear correlation between proliferation (Table 3)and risk of developing breast cancer (Fig. 2) on one hand andpositivity for the M, 52,000 protein on the other hand. Amongthe 23% proliferative lesions, 79.3% were positive for the M,52,000 protein. The negative cases were all lobular hyperplasias.Thirty-two % of the nonproliferative lesions were positive forthe Mr 52,000 protein (Table 3). This positivity was due mostlyto the presence of cysts. The value of the M, 52,000 proteinstaining in predicting high-risk mastopathies is therefore relatively high but may vary according to the histological type ofthe lesion. The M, 52,000 negative lesions have a 91.5% chanceof being nonproliferative. The only proliferative lesions thatwere not detected by this immunostaining were simple lobularhyperplasia (sclerosing adenosis) or lobular hyperplasia withatypia. In case of M, 52,000 protein-positive lesions, the predictive value is not good; however, by excluding nonproliferativecysts, a positive M, 52,000 protein staining indicates a 60.5%chance of proliferative disease and a 39.5% chance of nonproliferative lesion. We conclude that the M, 52,000 protein isassociated with the proliferation of ductal mammary cells andin the presence of cyst(s) 2 pathological criteria that are knownto increase breast cancer risk.
Clinical Parameters and the if, 52,000 Protein in BenignMastopathies. The clinical follow-up of the patients has beentoo short to allow a general conclusion about the actual prog-
3735

M, 52,000 ESTROGEN-REGULATED PROTEIN IN BENIGN BREAST DISEASE
»"•A
Fig. 1. Immunoperoxidase staining with a monoclonal antibody to M, 52,000 protein on cryosections from benign mastopathies. All sections were immunostainedwith the monoclonal antibody D7E3 and a peroxidase-antiperoxidase technique (see "Materials and Methods"). Controls for nonspecific binding in serial sections
(not shown) were negative. The sections were not counterstained. a, ductal hyperplasia. The epithelial cell layer had to be at least 3 cells thick to be accepted forinclusion in this group (19). Strong staining was restricted to the cytoplasm of epithelial cells and contrasted with the unstained pale ovoid nuclei. No reaction can beseen in the stroma. X 330. b. cystic lesion with papillary apocrine change. The cytoplasms of epithelial cells lining the cysts or forming papillary projections in thelumen were strongly stained, x 82. c, moderate adenosis. Lobular cells were not stained with the antibody, in contrast with a portion of microcyst seen on the right.X 165. d, fibroadenoma. Nonproliferative ductal cells and si rumai cells were negative, x 320.
nostic value of M, 52,000 protein detection in mammary biopsies. Since the protein is regulated by estrogen in breast cancercell lines, we anticipated variations in the M, 52,000 proteincontent as a function of the hormonal status of the patients atthe time of biopsy. No significant difference was found betweenthe follicular (18 cases) and luteal (17 cases) phases of themenstrual cycle.
By contrast, the percentage of tumors positive for the M,52,000 protein was higher in postmenopausal (73%, 15 cases;P < 0.02) than in premenopausal patients (39.5% positive, 76cases) and in patients over 45 yr of age (56%) compared toyounger patients (37% positive, 73 cases; P < 0.01). The increase in the Mr 52,000 protein with age may be due to a lowerlevel of progesterone and an unopposed estrogen effect (20) ormay be associated with the higher risk of benign breast diseaseobserved after the age of 45. In the 18 cases of 70 that had afamily history of breast cancer (in the mother, grandmother,sister, or aunt), there was no increase in the percentage of the
A/r 52,000 protein, suggesting that the protein is a parameterindependent of family history. A more complete study and aprolonged follow-up of the patients are required before a definitive conclusion can be reached concerning the clinical significance of this marker.
Assay of the M, 52,000 Protein in Mammary Cyst Fluid andOther Biological Fluids. In 38 patients, tissue biopsies were nottaken but fluid was aspirated by needle puncture from grossmammary cysts. The M, 52,000 protein content was measuredby immunoradiometric assay and found to vary from 0.5 to 7.4Mg/ml depending on the patient, with a mean value of 3 ftg/mi.This value is much higher than the basal level detected in plasmabut similar to the M, 52,000 protein concentration in sweat.These results were consistent with positive immunoperoxidasestaining of mammary cysts and indicated that the M, 52,000protein is always highly concentrated in cyst fluid. The significance of the variable level is not yet known. There was nosignificant correlation with the menstrual cycle phase at collec-
3736


M, 52,000 ESTROGEN-REGULATED PROTEIN IN BENIGN BREAST DISEASE
protein in cyst fluid is useful for discriminating between high-and low-risk cysts. We propose that the immunohistochemicaldetection of the M, 52,000 protein along with the pathologicalexamination of tissue sections and the presence of a familyhistory of breast cancer may be an additional high-risk factorto take into account when defining the treatment of these benignbreast diseases. By improving the prediction of high-risk mas-topathies, it might also help to improve the prevention of breastcancer. More extensive studies with a clinical follow-up of thesepatients will demonstrate whether or not the M, 52,000 proteinis a precancerous marker of ductal lesions in mammary tissue.
The M, 52,000 protein is secreted in metastatic breast cancercells under estrogen stimulation, and the hormonal regulationof this protein in the normal mammary gland (21) and in benignmastopathies is possible. Benign mastopathies contain receptors for estrogen and progesterone (22, 23); moreover, theproliferative lesions appear to contain higher receptor concentration (24, 25)4 and it is likely that these tissues are hormone
responsive. Monoclonal antibodies to the estrogen receptor andto the M, 52,000 protein are two useful probes for detectingthese proteins in biopsied benign mammary lumps. The factthat the M, 52,000 protein is found mostly in proliferativeductal lesions is also in agreement with the recent finding thatthe purified M, 52,000 protein can stimulate the growth ofbreast cancer cells in vitro (15, 26). It also suggests that anincreased production of the protein may be associated withearly stages of mammary cancerogenesis. The present immunohistochemical study also confirms the cellular heterogeneityof benign mastopathies, as already shown with other markers.
Negative staining may not always mean that the tissue contains no antigenically related M, 52,000 protein. Using a moresensitive two-site immunometric assay of cell extracts, we havein fact found that normal resting mammary cells contain smallamounts of the M, 52,000 protein.5 Comparative studies ofcancer cell lines using immunoperoxidase staining and ¡mimi-noradiometric assay indicate that the threshold between histo-chemically positive and negative cells is approximately 30 ng//¿gDNA.6 This sensitivity is low enough to discriminate be
tween a high and low cellular content of the protein. Falsenegative staining may also be found when positive proliferativecells are absent in the tissue sections examined but present inanother region of the mastopathy.
This is the first study showing that the A/r 52,000 protein isa potential tissue marker for distinguishing high- (proliferative)from low-risk (nonproliferative) benign breast diseasee. Moreextensive studies are obviously needed in order to confirm andextend this assumption, including a clinical follow-up of thesepatients. Other growth-associated proteins may also be usefulin studying high-risk proliferative mastopathies (27-29). Theadvantages of the M, 52,000 protein is its relative tissue specificity and its mitogenic activity (26), which may also facilitateits use in other diagnostic and therapeutic applications.
REFERENCES
1. Dao, T., Brodie, A., and Ip, C. (eds.). Tumor markers and their significancein the management of breast cancer. Prog. Clin. Biol. Res., 204: 1986.
2. Schlom, J., Greiner, J., Horan Hand, P., Colcher, D., Inghirami, G., Weeks,M., Pestka, S., Fisher, P. B., Noguchi, P., and Kufe, D. Monoclonal antibodies to breast cancer-associated antigens as potential reagents in themanagement of breast cancer. Cancer (Phila.), 54: 2777-2794, 1984.
3. Ceriani, R. L., Sasaki, M., Sussman, H., Wara, W. M., and Blank, E. W.Circulating human mammary epithelial antigens in breast cancer. Proc. Nati.
4J. Toth and E. De Sombre, personal communication.*G. Cavalle, unpublished experiments.' M. Garcia et al., unpublished observations.
Acad. Sci. USA, 79: 5420-5424. 1982.4. Ciocca, D. R., Adams, D. J., Edwards, D. P., Bjerke, R. J., and McGuire,
W. L. Distribution of an estrogen-induced protein with a molecular weightof 24,000 in normal and malignant tissue and cells. Cancer Res., 43: 1204-1210, 1983.
5. Taylor-Papadimitriou, J., Peterson, J. A., Arklie, J., Burchell, J., Ceriani, R.L., and Bodmer, W. F. Monoclonal antibodies to epithelium specific components of the human milk fat globule membrane: production and reactionwith cells in culture. Int. J. Cancer, 28:17-21, 1981.
6. Greene, G. L., Nolan, C., Engler, J. P., and Jensen, E. V. Monoclonalantibodies to human estrogen receptor. Proc. Nati. Acad. Sci. USA, 77:5115-5119, 1980.
7. Menard, S., Tagliabue, E., Canevari, S., Fossati, G., and Colnaghi, M. I.Generation of monoclonal antibodies reacting with normal and cancer cellsof human breast. Cancer Res., 43: 1295-1300, 1983.
8. McGuire, W. L., Ceriani, R. L., Schlom, J., and Frankel, A. E. Monoclonalantibodies, benign breast disease, and breast cancer. Breast Cancer Res.Treat., A:37-47, 1985.
9. Azzopardi, J. G. Cystic disease and carcinoma in problems in breast pathology. In: J. G. Azzopardi (ed.) Problems in Breast Pathology, pp. 92-112.Philadelphia: W. B. Saunders Co., 1979.
10. Haagensen, C. D., Bodian, C., and Haagensen, D. E., Jr. (eds.), In: BreastCarcinoma: Risk and Detection. Philadelphia: W. B. Saunders Co., 1981.
11. Love, S. M., Gelman, R. S., and Silen, W. Fibrocystic "disease" of thebreast—a nondisease? N. Engl. J. Med., 307: 1010-1014, 1982.
12. Dupont, W. D., and Page, D. L. Risk factors for breast cancer in womenwith proliferative breast disease. N. Engl. J. Med., 312:146-151, 1985.
13. Garcia, M., Capony, F., Derocq, D., Simon, D., Pau, B., and Rochefort, H.Monoclonal antibodies to the estrogen-regulated M, 52,000 glycoprotein:characterization and immunodetection in MCF7 cells. Cancer Res., 45:709-716, 1985.
14. Westley, B., and Rochefort, H. A secreted glycoprotein induced by estrogenin human breast cancer cell lines. Cell, 20: 352-362, 1980.
15. Rochefort, H., Chalbos, D., Capony, F., Garcia, M., Veith, F., Vignon, F.,and Westley, B. Effect of estrogen in breast cancer cells in culture: releasedproteins and control of cell proliferation. Prog. Clin. Biol. Res., ¡42:37-51,1985.
16. Veith, F. O., Capony, F., Garcia, M., Chantelard, J., Pujol, H., Veith, F.,Zajdela, A., and Rochefort, H. Release of estrogen-induced glycoprotein witha molecular weight of 52,000 by breast cancer cells in primary culture. CancerRes., 43: 1861-1868, 1983.
17. Garcia, M., Salazar-Retana, G., Richer, G.. Domergue, J., Capony, F., Pujol,H., Laffargue, F., Pau, B., and Rochefort, H. Immunohistochemical detectionof the estrogen-regulated M, 52,000 protein in primary breast cancers butnot in normal breast and uterus. J. Clin. Endocrinol. Metab., 59: 564-566,1984.
18. Sternberger, L. A., Hardy, P. H., Cuculis, J. J., and Meyer, H. G. Theunlabeled antibody enzyme method of immunohistochemistry. Preparationand properties of soluble antigen-antibody complexes (horseradish peroxi-dase-antihorseradish peroxidase) and its use in identification of spirochetes.J. Histochem. Cytochem.. IS: 315-333, 1970.
19. Page, D. L., Van der Zwaag, R., Rogers, L. W., Williams, L. T., Walker, W.E., and Hartmann, W. H. Relation between component parts of fibrocysticdisease complex and breast cancer. J. Nati. Cancer Inst., 61: 1055-1063,1978.
20. Korenman, S. The endocrinology of breast cancer. Cancer (Phila.), 46: 874-878, 1980.
21. Cavalié-Barthez,G., Chambón, M., Garcia, M., Hallowes, D., Veith, F.,Vignon, F., and Rochefort, H. Effect of estradici on non-malignant humanmammary cells in primary culture. Ann. NY Acad. Sci., in press, 1986.
22. Allegra, J. C., Lippman, M. E., Green, L., Barlock, A., Simon, R.,Thompson,E. B., Huff, K. K.. and Griffin. W. Estrogen receptor values in patients withbenign breast disease. Cancer (Phila.), 44: 228-231, 1979.
23. Barthelemi, H., Bressot, N., Cavalié-Barthez,G., Larrousse, M., Rodière,M., Lamarque, J. L., Domergue, J., Laffargue, F., Pujol, H., and Rochefort,H. Récepteursdes oestrogènes, de la progestéroneet des glucocorticoides:comparaison entre mastopathies diffuses fibrokystiques et fibroadenomeslocalisés.Senologia, 4: 211-217, 1984.
24. Jacquemier, J. D., Rolland, R. D., and Vague, D. Relationship betweensteroid receptor and epithelial cell proliferation in benign fibrocystic diseaseof the breast. Cancer (Phila.), 49: 2534-2536, 1982.
25. Nenci, I., Marchetti, E., Querzoli, P., and Bagni, A. Toward understandingmammary preneoplasia: the estrogen receptor-promotion hypothesis. Prog.Surg. Pathol., 6: in press, 1986.
26. Vignon, F., Capony, F., Chambón, M., Freiss, G., Garcia, M., and Rochefort,H. Autocrine growth stimulation of the MCF7 breast cancer cells by theestrogen-regulated M, 52,000 protein. Endocrinology, IIS: 1537-1545,1986.
27. Salomon, D. S., Zwiebel, J. A., Bano, M., Losonczy, I., Fennel, P., andKidwell, W. R. Presence of transforming growth factors in human breastcancer cells. Cancer Res., 44:4069-4077, 1984.
28. Haagensen, D. E., Jr., and Mazoujian, G. Relationship of glycoproteins inhuman breast cystic disease fluid to breast carcinoma. In: A. Angeli, H. L.Bradlow, and L. Dogliotti (eds.), Endocrinology of Cystic Breast Disease,pp. 149-168. New York: Raven Press, 1983.
29. Chambón, P., Dierich, A., Gaub, M. P., Jakowlev, S., Jongstra, J., Krust,A., Lepennec, J. P., Oudet, P., and Reudelhuber, T. Promoter elements ofgenes coding for proteins and modulation of transcription by estrogens andprogesterone. Recent Prog. Hor. Res., 40: 11-40, 1984.
3738