DISTRETTO ADDOMINALE SUPERIORE - Congressi AIRO · DISTRETTO ADDOMINALE SUPERIORE ... distress &...
40
La terapia di supporto in radioterapia oncologica 28 ottobre 2013 DISTRETTO ADDOMINALE SUPERIORE Ernesto MARANZANO Dipartimento di Oncologia, S.C. di Radioterapia Oncologica, Az. Ospedaliera, Terni
Transcript of DISTRETTO ADDOMINALE SUPERIORE - Congressi AIRO · DISTRETTO ADDOMINALE SUPERIORE ... distress &...
La terapia di supporto in radioterapia oncologica
28 ottobre 2013
DISTRETTO ADDOMINALE SUPERIORE
Ernesto MARANZANO Dipartimento di Oncologia,
S.C. di Radioterapia Oncologica, Az. Ospedaliera, Terni
1. Prevention of acute (& late) toxicity
2. Treatment/supportive therapy of acute toxicity
a. Organ-specific toxicity ( i.e., nausea, vomiting, diarrhea )
b. Evaluation of fatigue, distress & QoL
Radiotherapy-induced side effects/toxicity
1. Prevention of acute (& late) toxicity
2. Treatment/supportive therapy of acute toxicity
a. Organ-specific toxicity ( i.e., nausea, vomiting, diarrhea )
b. Evaluation of fatigue, distress & QoL
Radiotherapy-induced side effects/toxicity

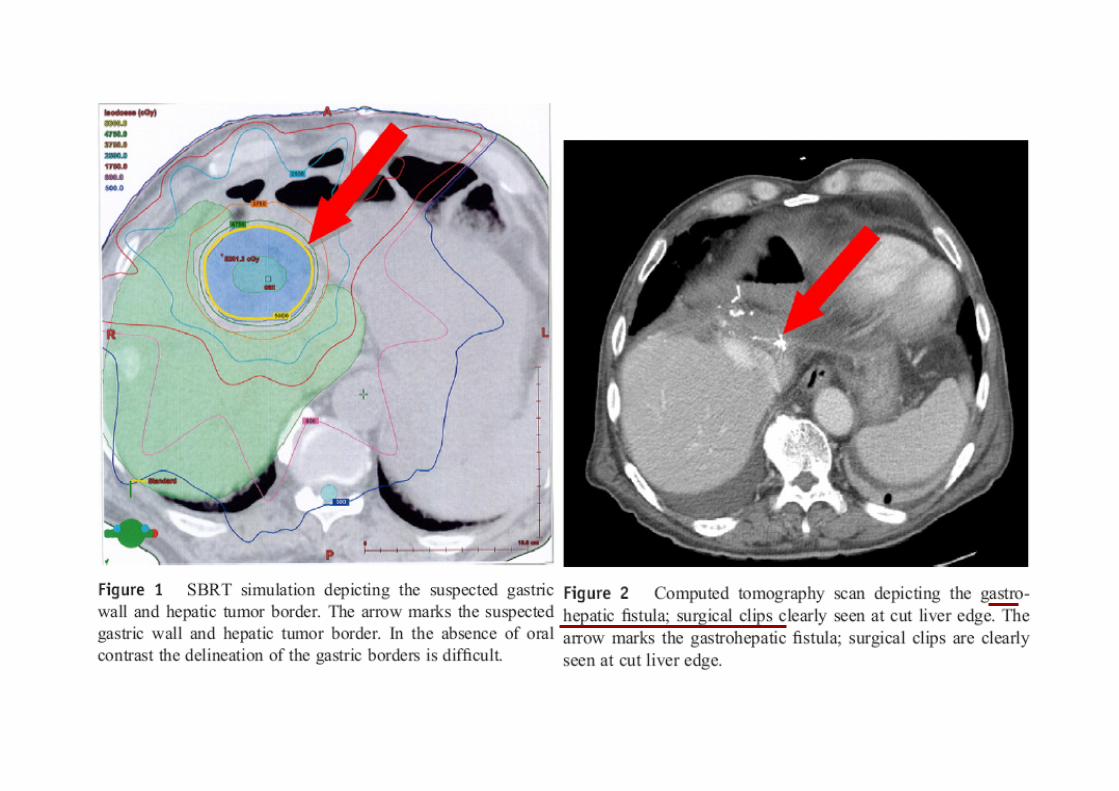
! Gastric perforation after SBRT to a liver metastasis from colon cancer
! 10 fractions of 5 Gy each for a total of 50 Gy
! No oral contrast for the delineation of the gastric wall
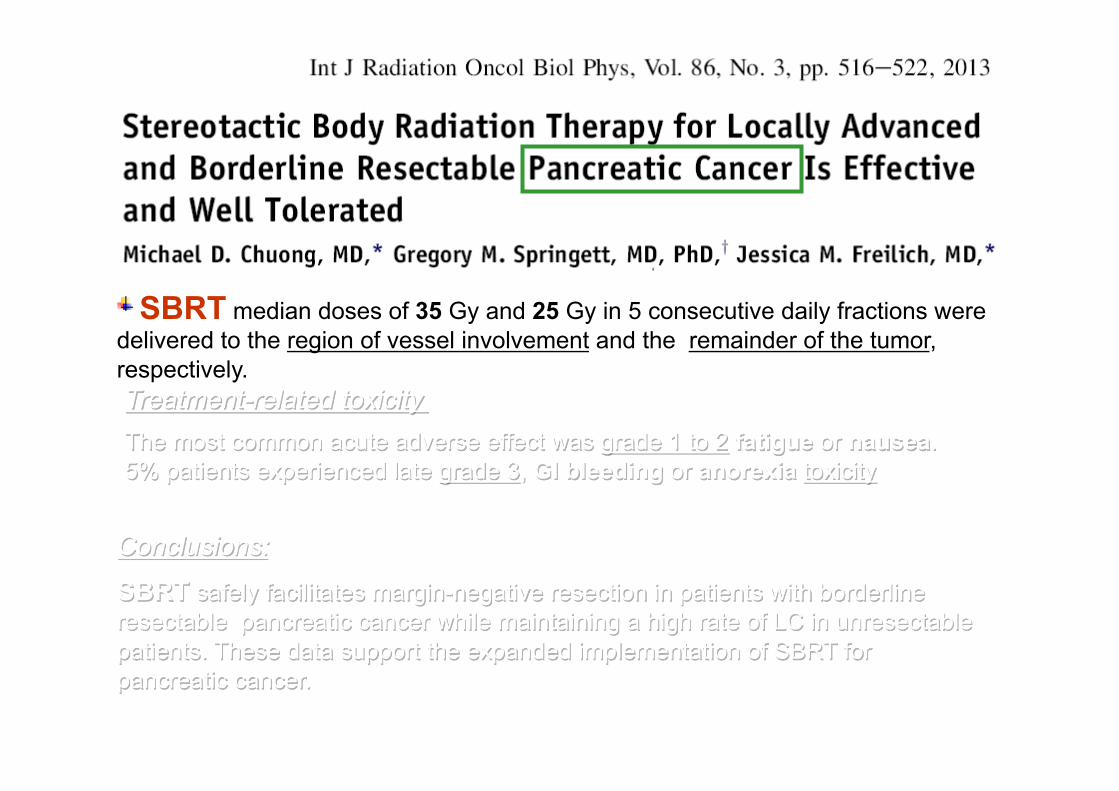
! SBRT median doses of 35 Gy and 25 Gy in 5 consecutive daily fractions were delivered to the region of vessel involvement and the remainder of the tumor, respectively.
Conclusions:
SBRT safely facilitates margin-negative resection in patients with borderline resectable pancreatic cancer while maintaining a high rate of LC in unresectable patients. These data support the expanded implementation of SBRT for pancreatic cancer.
Treatment-related toxicity
The most common acute adverse effect was grade 1 to 2 fatigue or nausea. 5% patients experienced late grade 3, GI bleeding or anorexia toxicity

SBRT median doses of 35 Gy and 25 Gy in 5 consecutive daily fractions were delivered to the region of vessel involvement and the remainder of the tumor, respectively.
Conclusions:
SBRT safely facilitates margin-negative resection in patients with borderline resectable pancreatic cancer while maintaining a high rate of LC in unresectable patients. These data support the expanded implementation of SBRT for pancreatic cancer.
Treatment-related toxicity
The most common acute adverse effect was grade 1 to 2 fatigue or nausea. 5% patients experienced late grade 3, GI bleeding or anorexia toxicity
CASE REPORT
Scenario ! 61-year-old woman with renal cell carcinoma (clear-cell type) and cutaneous metastases.
! Sorafenib as a first line treatment, 400 mg twice a day. ! Five weeks later, severe low back pain. At MRI lytic bone metastasis of the L4.
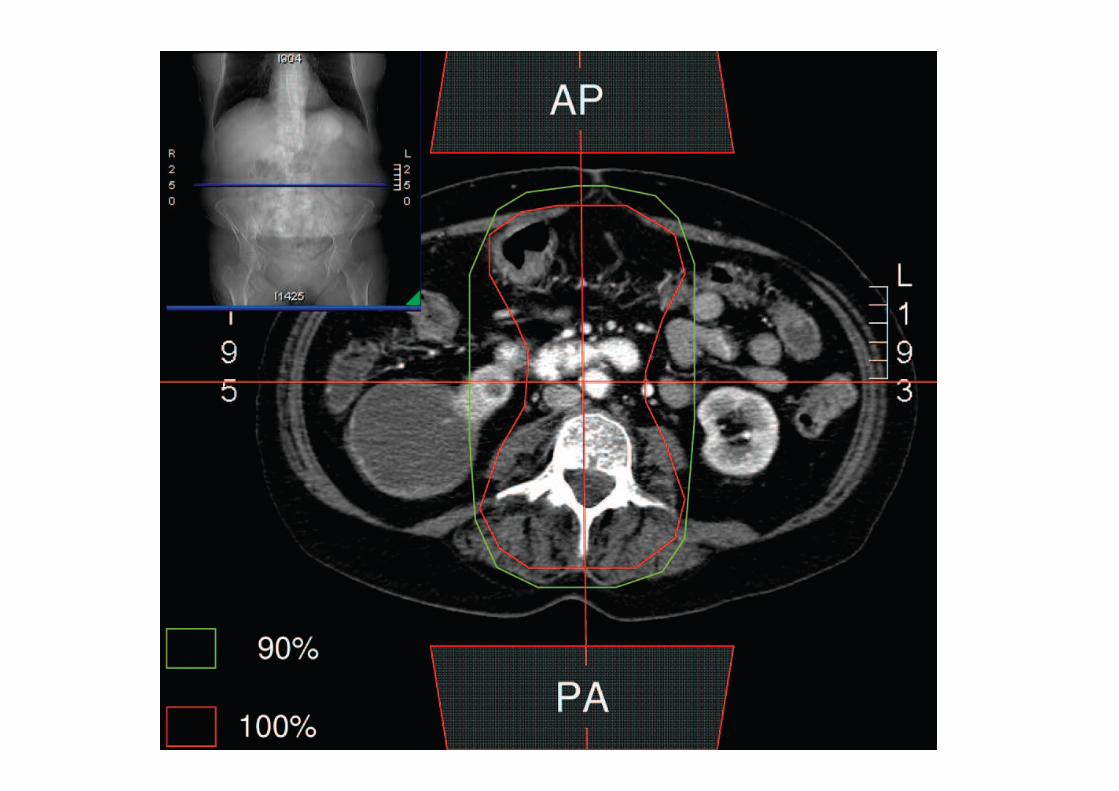
! Palliative radiotherapy on L3-L5 (8 Gy in one fraction). ! Worthy to note: Sorafenib was stopped 2 days before RT and started again 3 days later.
Scenario
! One week after radiotherapy the patient was admitted to hospital with abdominal pain, diarrhea, and dehydration.
! She died the next day.
! The autopsy revealed multiple perforations of the transverse and sigmoid colon with fecal peritonitis.
! Biopsy specimens of the colon showed ischemic enteritis with radiation-effects and vascular changes with thrombus formation, but no evidence of tumor metastases
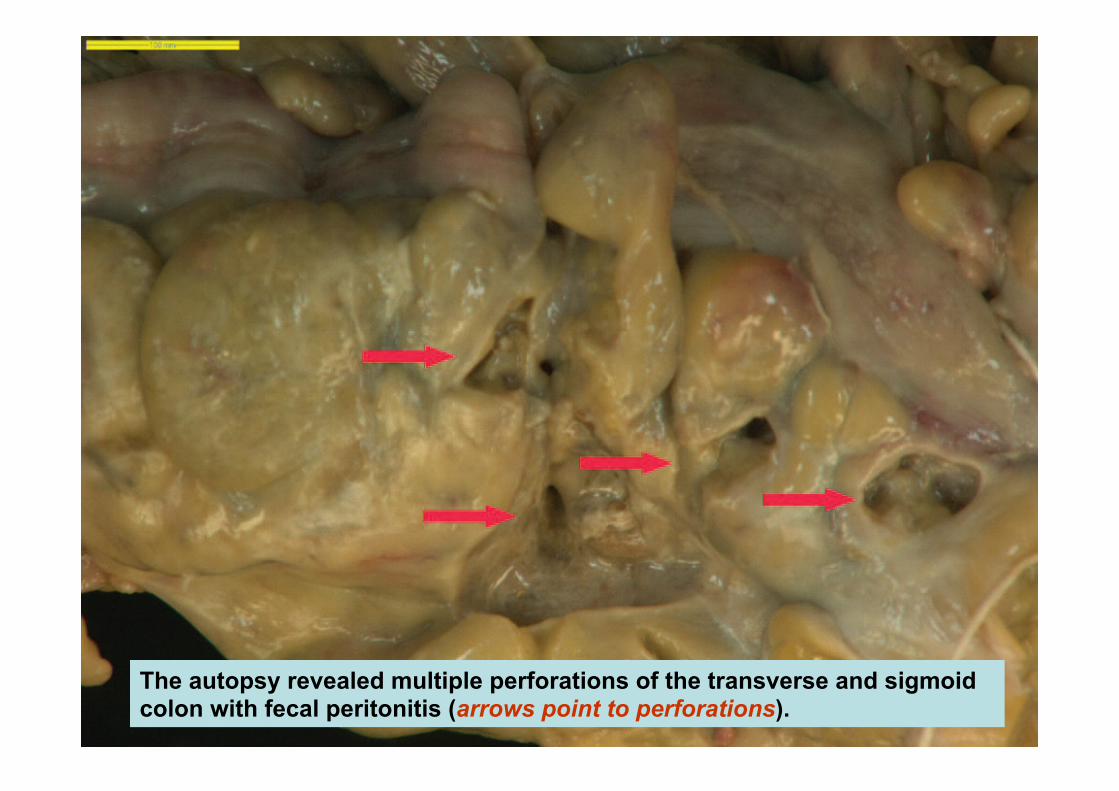
The autopsy revealed multiple perforations of the transverse and sigmoid colon with fecal peritonitis (arrows point to perforations).
What was the cause/s of this so severe toxicity?

POSSIBLE CAUSES OF THIS SO SEVERE TOXICITY
ü Sorafenib? It could be. Intestinal perforation is reported as a rare Sorafenib-induced side effect
ü Radiotherapy dose?
Probably not. 8-Gy single dose does not exceed the 25 x 2Gy considered the maximum intestinal tolerated dose
POSSIBLE CAUSES OF THIS SO SEVERE TOXICITY
ü Timing of Sorafenib & RT association? Probably yes. Too few days between interruption of Sorafenib and RT administration
ü Radiotherapy technique?
Probably yes!

Prevention of acute (& late) toxicity
Radiotherapy-induced side effects/toxicity
Radiation Oncologist is a clinician who: ! has to prescribe RT using the right technique/technology (in palliative setting too);
! has to know drugs and their side effects;
! has to know the previous treatment administered to each patient and suggest the optimal timing between chemo/targeted therapy and RT.

1. Prevention of acute (& late) toxicity
2. Treatment/supportive therapy of acute toxicity
a. Organ-specific toxicity ( i.e., nausea, vomiting, diarrhea )
b. Evaluation of fatigue, distress & QoL
Radiotherapy-induced side effects/toxicity

Radiother Oncol. 2005 Sep;76(3):227-33

! 45 Italian radiation oncology centres & 1020 recruited patients
! Emesis occurred in 27.9% patients.
! Statistically significant risk factors were concomitant chemotherapy, previous experience of vomiting, irradiated site (upper abdomen) and field size (>400 cm2).
! An antiemetic drug was given only to a minority (17%) of patients receiving RT, and the prescriptions were prophylactic in 12.4% and symptomatic in 4.6%.
! Different compounds and a wide range of doses and schedules were used
2010

Purpose: To investigate international patterns of practice in the management of radiation therapy-induced nausea and vomiting (RINV).
Results: In total, 1022 responses were received. Risk estimates and management decisions for the minimal- and high-risk cases varied little and were in line with guideline standards, whereas those for the low- and moderate-risk cases varied greatly. The serotonin (5-HT3) receptor antagonists were the most commonly recommended prophylactic agents.
Conclusions: RINV are under-studied treatment sequelae. New observational and translational studies are needed to allow for individual patient risk assessment and to refine antiemetic guideline management recommendations.

Results 176 trainees from 11 countries responded. Only 28 % were aware of any anti-emetic guideline (!).
Results Of the 11 high-emetic-risk radiotherapy cohorts: 2, 8 (73%), and 1 received 5-HT3RAs for durations longer than, equal to, or shorter than the duration of RT, respectively.
Of the 22 moderate or low-emetic-risk radiotherapy cohorts: 5, 14 (64%), and 3 received 5-HT3RAs for durations longer than, equal to, or shorter than the duration of RT, respectively.
Conclusion Future studies should compare different timings and durations of therapy with common efficacy endpoints to develop effective and cost-efficient antiemetic strategies.

2013
! 45 Italian radiation oncology centres & 1020 recruited patients
! 82/147 (14.6%) pts had diarrhoea. The median minimum number of daily events was 1 (range 1–7) with a median maximum events of 3 (range 1–23).
! Statistically significant risk factors were concomitant tumour site (abdomen-pelvis), therapeutic purpose and field size (>400 cm2).
! 82/147 pts (56.2%) had a drug prescription for diarrhoea
! Different drugs and a wide range of doses and schedules were used

Diarrhea
2004
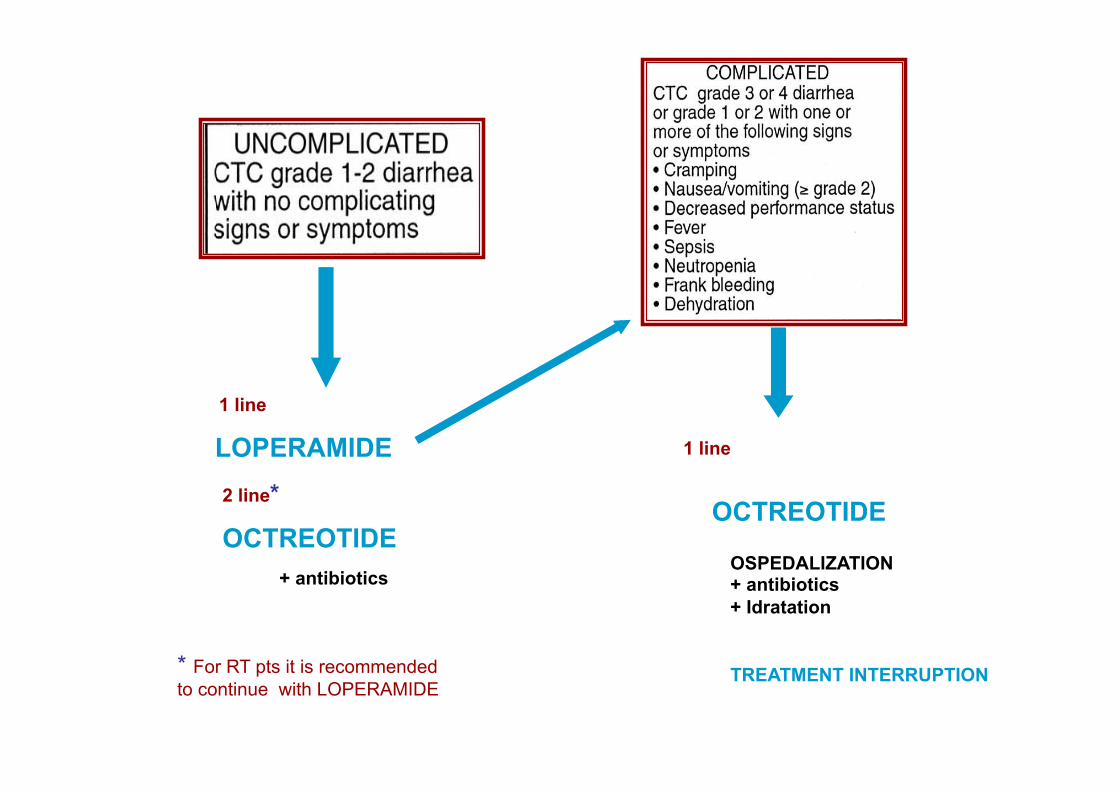
LOPERAMIDE
OCTREOTIDE
1 line
2 line*
1 line
OCTREOTIDE
+ antibiotics
* For RT pts it is recommended to continue with LOPERAMIDE
OSPEDALIZATION + antibiotics + Idratation TREATMENT INTERRUPTION


HOW PREVENT RT-INDUCED DIARRHEA: N.C.I. SUGGESTIONS
1. Prevention of acute (& late) toxicity
2. Treatment/supportive therapy of acute toxicity
a. Organ-specific toxicity ( i.e., nausea, vomiting, diarrhea )
b. Evaluation of fatigue, distress & QoL
Radiotherapy-induced side effects/toxicity

What Is FATIGUE? It is an illness characterized by prolonged, debilitating, weakness severe enough to affect one or more aspects of a person's life. It is also characterized by multiple nonspecific symptoms such as headaches, recurrent sore throats, muscle/joint pains, memory and concentration difficulties.
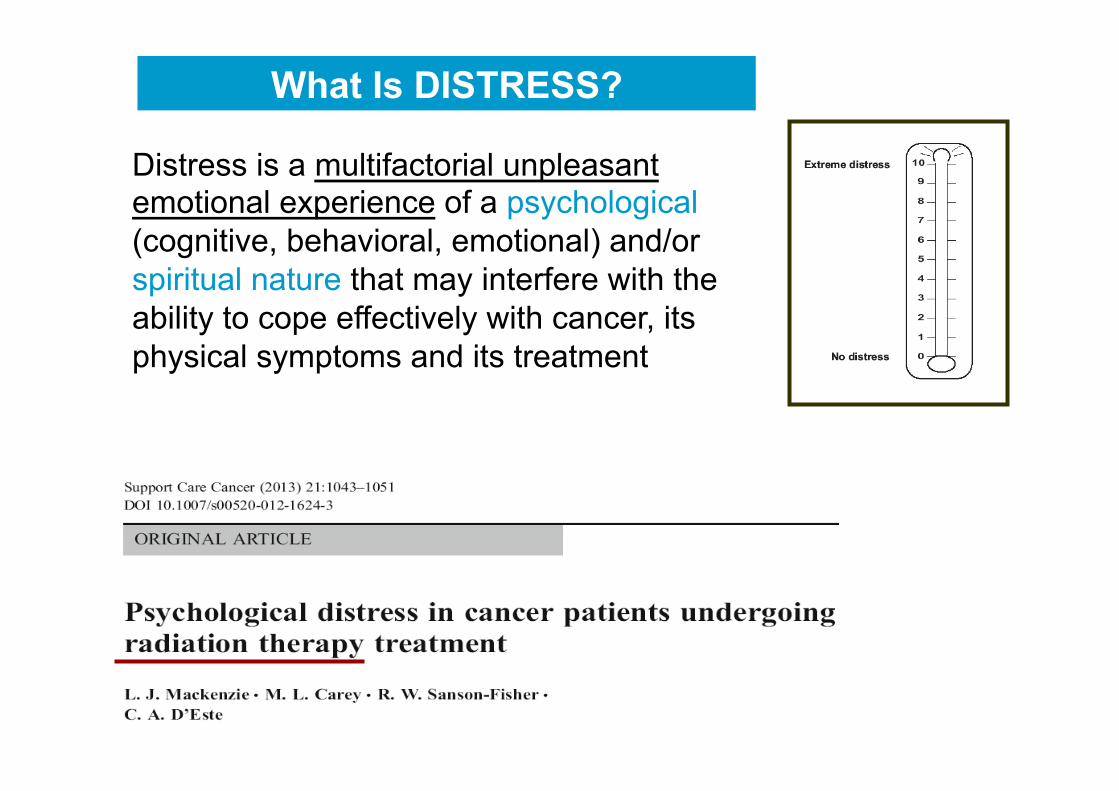
What Is DISTRESS?
Distress is a multifactorial unpleasant emotional experience of a psychological (cognitive, behavioral, emotional) and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms and its treatment
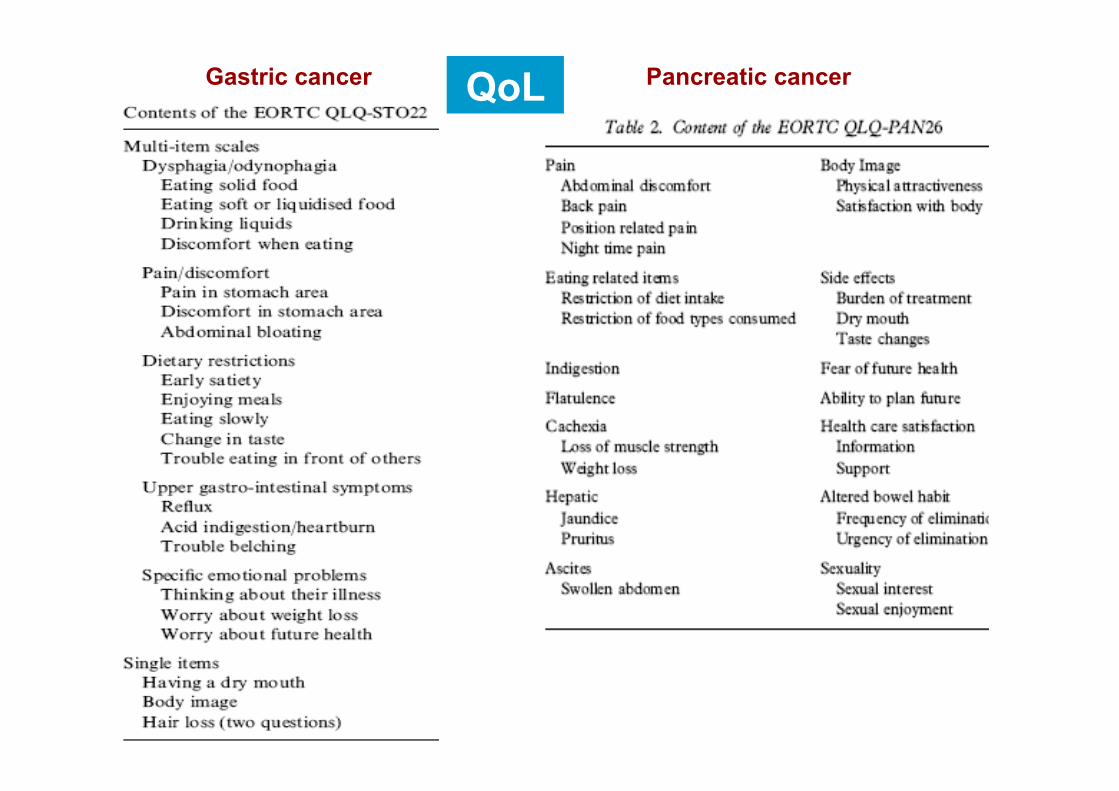
Gastric cancer Pancreatic cancer QoL
DISTRESS
FATIGUE
QoL
CLINICAL ONCOLOGY HIGH TECHNOLOGY

SCYLLA CHARYBDIS
CLINICAL ONCOLOGY HIGH TECHNOLOGY
RADIATION ONCOLOGY
Radiation Oncology will direct successfully between clinic (Scylla) and technology (Charybdis), and will survive as an independent discipline
My wishful thinking
P. Rubin, ASTRO 1980, modified