Dissociation between plasma and monocyte-associated cytokines during sepsis
8
Eur. J. Immunol. 1991. 21: 2177-2184 Plasma and monocyte-associated cytokines 2177 Carlos Munozo+, Benoit Misseta, Catherine Fittingo, Jean-Pierre BICriot*, Jean-Carlet* and Jean-Marc CavaillonO Unit6 d’Immuno-Allergieo, Institut Pasteur and Intensive Care Unit*, H8pital Saint Joseph, Pans Dissociation between plasma and monocyte-associated cytokines during sepsis We report our investigations of circulating interleukin (IL) lp, IL 6 and tumor necrosis factor (TNF)-a, as well as cell-associated IL l a , IL lp and TNF-a in plasma and monocytes of 21 patients with sepsis syndrome and 6 patients with non-septic shock. Longitudinal studies reveal that (a) the most frequent detectable plasma cytokines were TNF-a and IL6, (b) the presence and the kinetics of circulating cytokines were independent of one other, (c) detectable levels of cytokines could be found for a long period of time, and (d) significantly higher levels of IL 6 were found for non-surviving patients. Because of the in vivo half-life of cytokines and of the existence of numerous specific high-affinity receptors, it is quite probable that detectable plasma cytokines represent the excess of produced mediators which have not been trapped by the target cells. TNF-a (410 k 65 pg/106monocytes) and IL 1fi (153 It: 60 pg/106monocytes) were frequently found associated to monocyte lysates (88% and 50%, respectively). Despite the fact that IL la is the most abundant cytokine found associated to monocytes following in vitro activation, IL la was rarely found in monocytes of intensive care unit patients (29%). No correlation was found to exist between the levels of plasma cytokines and cell-associated cytokines. Some patients had plasma TNF-a or IL 1p in the absence of the corresponding monocyte-associated cytokine. This observation suggests that cells other than monocytes can participate in the production of circulating cytokines. At the end of the longitudinal study (day 14 k 2), only 2/12 surviving patients still had plasma TNF-a,whereas 8/12 had monocyte-associated TNF-a.These results indicate that activation of monocytes still occurs in patients for whom no plasma cytokines can be detected. Thus, in addition to the measurement of plasma cytokine, measurement of cell-associated cytokine appears useful to assess cytokine production and monocyte activation in vivo. 1 Introduction Since the first observation in 1987 by Waage et al. [l] that TNF-a could be found in the plasma of patients with meningitis and septicemia, numerous authors have shown the presence of TNF-a, IFN-y, IL 1p and IL 6 in plasma or in the cerebrospinal fluid of patients with severe infections [2-121. However, controversial findings still exist concern- ing the levels of plasma cytokines, the proportion of patients with detectable cytokines and the correlation with the outcome. For example, Girardin et al. [2] found up to 1.7 ng/ml of IL 18 during Gram-negative septicemia, whereas levels found by Cannon et al. [3] did not exceed 270 pg/ml. Marks et al. [4] found circulatingTNF-a among only 36% of patients with septic shock, whereas Calandra et al. [5] found TNF-a in plasma of 79% of their patients. Several authors [2,5,7] noticed a correlation between high levels of circulating IL 1p and subsequent mortality; how- ever, Cannon et al. [3] found that non-surviving patients [I 95801 + Supported by a grant from the Fondation pour la Recherche MCdicale. Present address: Immunology Unit, INTA, Universi- dad de Chile, Casilla 15 138, Santiago 11, Chile. Correspondence: Jean-Marc Cavaillon, Unit6 d’Immuno-Allergie , Institut Pasteur, 28 rue Dr. Roux, F-75724 Paris Cedex 15, France had lower levels of this cytokine. These discrepancies between different reports may reflect the use of different technical means of measuring circulating cytokines and the rarity of longitudinal studies. Indeed, measurement of circulating cytokines in infected patients is usually only made once, upon admission to the hospital. In the present investigation we have performed longitudinal studies among septic patients admitted into an intensive care unit (ICU) and have compared the levels of circulating IL lp, TNF-a and IL6. Experiments performed in vivo with animal models have established that cytokines have a rather short half-life [13-151. Furthermore, a great variety of cells have high- affinity surface receptors for these cytokines and, thus, are able to trap them very efficiently. As a consequence, it is quite probable that measurable circulating cytokines which can be detected during a given pathology represent the “tip of the iceberg” (i.e. the excess of production) and absence of detectable cytokines in plasma does not necessarily mean that they are not being produced. To address this question we have measured cell-associated cytokines in lysates of freshly isolated monocytes. Such an approach has been recently proved useful in demonstrating monocyte activa- tion, as we reported during hemodialysis [16], or as it has been shown during cardiac bypass surgery [17]. Following monocyte activation in vitro, IL la appears to be the main cell-associated cytokine [18, 19J.Wehave, thus, studied the presence of IL la associated to monocytes as well as IL, 10 and TNF-a. 0 VCH Verlagsgesellschaft mbH, D-6940 Weinheim, 1991 0014-298Of91lO909-2177$3.50 + .25/0
-
Upload
carlos-munoz -
Category
Documents
-
view
216 -
download
1
Transcript of Dissociation between plasma and monocyte-associated cytokines during sepsis

Eur. J. Immunol. 1991. 21: 2177-2184 Plasma and monocyte-associated cytokines 2177
Carlos Munozo+, Benoit Misseta, Catherine Fittingo, Jean-Pierre BICriot*, Jean-Carlet* and Jean-Marc CavaillonO
Unit6 d’Immuno-Allergieo, Institut Pasteur and Intensive Care Unit*, H8pital Saint Joseph, Pans
Dissociation between plasma and monocyte-associated cytokines during sepsis
We report our investigations of circulating interleukin (IL) l p , IL 6 and tumor necrosis factor (TNF)-a, as well as cell-associated IL l a , IL l p and TNF-a in plasma and monocytes of 21 patients with sepsis syndrome and 6 patients with non-septic shock. Longitudinal studies reveal that (a) the most frequent detectable plasma cytokines were TNF-a and IL6, (b) the presence and the kinetics of circulating cytokines were independent of one other, (c) detectable levels of cytokines could be found for a long period of time, and (d) significantly higher levels of IL 6 were found for non-surviving patients. Because of the in vivo half-life of cytokines and of the existence of numerous specific high-affinity receptors, it is quite probable that detectable plasma cytokines represent the excess of produced mediators which have not been trapped by the target cells. TNF-a (410 k 65 pg/106 monocytes) and IL 1fi (153 It: 60 pg/106 monocytes) were frequently found associated to monocyte lysates (88% and 50%, respectively). Despite the fact that IL la is the most abundant cytokine found associated to monocytes following in vitro activation, IL la was rarely found in monocytes of intensive care unit patients (29%). No correlation was found to exist between the levels of plasma cytokines and cell-associated cytokines. Some patients had plasma TNF-a or IL 1p in the absence of the corresponding monocyte-associated cytokine. This observation suggests that cells other than monocytes can participate in the production of circulating cytokines. At the end of the longitudinal study (day 14 k 2), only 2/12 surviving patients still had plasma TNF-a, whereas 8/12 had monocyte-associated TNF-a.These results indicate that activation of monocytes still occurs in patients for whom no plasma cytokines can be detected. Thus, in addition to the measurement of plasma cytokine, measurement of cell-associated cytokine appears useful to assess cytokine production and monocyte activation in vivo.
1 Introduction
Since the first observation in 1987 by Waage et al. [l] that TNF-a could be found in the plasma of patients with meningitis and septicemia, numerous authors have shown the presence of TNF-a, IFN-y, IL 1p and IL 6 in plasma or in the cerebrospinal fluid of patients with severe infections [2-121. However, controversial findings still exist concern- ing the levels of plasma cytokines, the proportion of patients with detectable cytokines and the correlation with the outcome. For example, Girardin et al. [2] found up to 1.7 ng/ml of IL 18 during Gram-negative septicemia, whereas levels found by Cannon et al. [3] did not exceed 270 pg/ml. Marks et al. [4] found circulatingTNF-a among only 36% of patients with septic shock, whereas Calandra et al. [5] found TNF-a in plasma of 79% of their patients. Several authors [2,5,7] noticed a correlation between high levels of circulating IL 1p and subsequent mortality; how- ever, Cannon et al. [3] found that non-surviving patients
[I 95801 + Supported by a grant from the Fondation pour la Recherche
MCdicale. Present address: Immunology Unit, INTA, Universi- dad de Chile, Casilla 15 138, Santiago 11, Chile.
Correspondence: Jean-Marc Cavaillon, Unit6 d’Immuno-Allergie , Institut Pasteur, 28 rue Dr. Roux, F-75724 Paris Cedex 15, France
had lower levels of this cytokine. These discrepancies between different reports may reflect the use of different technical means of measuring circulating cytokines and the rarity of longitudinal studies. Indeed, measurement of circulating cytokines in infected patients is usually only made once, upon admission to the hospital. In the present investigation we have performed longitudinal studies among septic patients admitted into an intensive care unit (ICU) and have compared the levels of circulating IL lp , TNF-a and IL6.
Experiments performed in vivo with animal models have established that cytokines have a rather short half-life [13-151. Furthermore, a great variety of cells have high- affinity surface receptors for these cytokines and, thus, are able to trap them very efficiently. As a consequence, it is quite probable that measurable circulating cytokines which can be detected during a given pathology represent the “tip of the iceberg” (i.e. the excess of production) and absence of detectable cytokines in plasma does not necessarily mean that they are not being produced. To address this question we have measured cell-associated cytokines in lysates of freshly isolated monocytes. Such an approach has been recently proved useful in demonstrating monocyte activa- tion, as we reported during hemodialysis [16], or as it has been shown during cardiac bypass surgery [17]. Following monocyte activation in vitro, IL la appears to be the main cell-associated cytokine [18, 19J.We have, thus, studied the presence of IL la associated to monocytes as well as IL, 10 and TNF-a.
0 VCH Verlagsgesellschaft mbH, D-6940 Weinheim, 1991 0014-298Of91lO909-2177$3.50 + .25/0

2178 C. Munoz, B. Misset, C. Fitting et al. Eur. J. Immunol. 1991. 21: 2177-2184
2 Materials and methods
2.1 Patients
Twenty-seven patients admitted to the ICU were studied. Twenty-one fullfilled the criteria for "sepsis syndrome" as described by Bone et al. [20], including evidence of an infectious site and signs of inadequate organ perfusion. Of these, 12 met the criteria for septic shock [sepsis syndrome plus a systolic blood presure (BP) <90 mm Hg or a decrease from baseline in systolic BP > 40 mm Hg] and 7 met the criteria for adult respiratory distress syndrome (ARDS; bilateral alveolar infiltrates, pulmonary wedged pressure < 18 mm Hg and Pa02/FiO2 < 150 with positive expiratory pressure I 5 cm H20). The infectious conditions included pneumonia (n = 7), perinitis (n = 4), catheter-related sep- sis (n = =3), pyelonephritis (n = 2), infectious aortic aneu- rism (n = l ) , aortic graft sepsis (n = l ) , Gram-negative septicemia due to granulocytopenia (n = 1), endocarditis (n = 1) and meningitis (n = l).The pathogenic agents were Gram-negative bacilli (GNB) in 6 cases, Gram-positive cocci (GPC) in 7 cases, association of GNB and GPC in 7 cases, and Mycobacteriurn tuberculosis in 1 case. Eleven patients were bacteremic. The 6 remaining patients were admitted because of cardiogenic shock (n = 3), hemorr- hagic shock (n = 2) or hypovolemic shock (n = 1). The simplified acute physiological score (SAPS) [21] on admis- sion was 12.7 k 4.2 (mean f SD) for the 21 septic patients and 12.7 f 4.3 for the 6 non-septic patients. Treatment of infected patients included antibiotics, morphine, benzodia- zepine, heparin, cathecholamine, insulin and several occa- sional drugs. Eleven patients died in the ICU. Healthy controls (n = 8) were donors from the blood bank and research workers from our laboratory. The protocol had been approved by the ethical commitee of the Saint Joseph Hapit al.
2.2 Collection of blood samples
Blood was collected within 2 days after admission of the patients in the ICU, thereafter daily for the 3 following days, and then weekly until discharge, death or day 21 if the patients were still in the ICU. Last measurements were performed on day 14 k 1.5 (range 5-21) for surviving patients and on day 10 f 2.5 (range 1-21) for non-surviving patients.
2.3 Plasma
Twenty milliliters of blood was drawn on EDTA. Blood was immediately placed on ice and processed within 2 h. Two hundred microliters of aprotinin (0.67 TUI/ml of blood; Sigma, St. Louis, MO) was added and tubes centrifuged at 400 x g, 4"C, for 10 min. Plasma was transferred into Eppendorf (Hamburg, FRG) tubes and re-centrifuged at 10000 x g, 4°C for 5 min. Plasma was then aliquoted and kept at -30°C.
2.4 Monocytes
Cell pellets were resuspended in 25 ml RPMI 1640 medium (Gibco, Uxbridge, GB) and centrifuged over Ficoll (MSL,
Eurobio, Paris, France) for 25 min at 150 x g at room temperature. After washing, PBMC were counted and nonspecific esterase (NSE) staining performed [22]. NSE+ cells (5 x 105)/0.5 ml RPMI medium/well (24-well multid- ish plates, Falcon, Oxnard, CA) were allowed to adhere for 1 h as previously described [23].
2.5 Collection of cell-associated cytokine content
Immediately after adherence, nonadherent cells were removed, adherent cells washed and 0.5 ml of fresh RPMI medium was added. Plates were then frozen as previously described [24]. Three cycles of freezing-thawing were performed before harvesting the cell lysate which was subsequently centrifuged and kept at -30 "C until cytokine contents were assessed.
2.6 IL6 bioassay
IL 6 activity was determined using the specific 7TD1 IL6-dependent cell line [25], kindly provided by Dr. J.Van Snick (Ludwig Institute for Cancer Research, Brussels, Belgium). Cells were cultured at a density of 1200 cells/well (96-well multidish plates, Falcon) in 100 pl of RPMI medium supplemented with antibiotics, 2-ME (5 x lop5 M) and 10% FCS, in the presence of either serial dilutions of cell SN or heat-inactivated (30 min, 56°C) plasma. After 4 days of culture at 37 "C, the proliferation was monitored by a staining method [26]. Briefly, 125 pg of tetrazolium salt (thiazolyl blue, M7T) were added to each well and after 1 to 2 h of incubation at 37"C, the test was stopped with 100 pl/well of extraction buffer (20% SDS, 50% dimethyl- formamide in H20, 2.5% 1 N HCl, 2.5% of an 80% acetic acid solution, pH7.4). After an overnight incubation at 37 "C the absorbance was measured at 540 nm using an automated microELISA autoreader. One unit of IL6 corresponds to half the maximum growth rate of the hybridoma cells. IL6 activity detected in SN of LPS- stimulated monocytes and in plasma was completely abol- ished by the addition of 10 pg rabbit polyclonal anti-human IL6 antibodies (Genzyme, Boston, MA).
2.7 TNF-a RIA
The TNF-a RIA was based on the competitive inhibition assay for TNF-a developed by Van der Meer et al. [27], with minor modifications. In every assay, 10 TNF-a standards (RhBne Poulenc,Vitry/Seine, France) containing 0,40,80, 150, 300, 600, 1250, 2500, 5000 and 1OOOOpg/ml were included. All standards and cell SN or cell lysate samples were diluted in a BSA buffer.TNF-a in plasma was assessed in undiluted samples. On day 1, 100 p1 of a rabbit anti- TNF-a antiserum (kindly provided by Catherine Rougeot, Institut Pasteur, Paris) diluted 1 : 10000 in order to preci- pitate 35% of the radiolabeled TNF, was added to 100 yl of standards or samples.To determine the nonspecific binding, 100 p1 of BSA buffer was added to a tube instead of the sample. Subsequently, 300 p1 of BSA buffer was added to each tube. After vortexing, the tubes were incubated for 24 h at room temperature. On day 2, 100 pl of 1251-labeled TNF-a solution (30 pCi/pg = 111 kBq/pg, New England Nuclear, Boston, MA) containing approximatively

Eur. J. Immunol. 1991. 21: 2177-2184 Plasma and monocyte-associated cytokines 2179
On day 1, Luxlon ELISA microtiter plates were coated with 100 p1 of mouse IgGl anti-rhIL la mAb (10 pg/ml in sodium carbonate buffer) and incubated 2 h at 37 "C. The plates were washed three times with 0.1% Tween-20PBS. Standards (0,10,30,100,300,1000,3000 and 10000 pg/ml rhILla) or cell SN or cell lysate samples, diluted in 1% BSA, 0.1% Tween-20/PBS, were added to coated wells and incubated overnight at 4°C. On day2, the plates were washed three times and 100 pl of the second mouse anti-rhIL la mAb (IgG2b; 1 : 2000 in BSA/Tween/PBS) added to each well. Plates were incubated for 3 h at 37 "C. After washing, 100 pl of peroxidase conjugate anti-mouse IgG2b (1 : 1000; ICN; Irvine, CA) were added to each well and the platesleft for 1 ha t 37 "C. After washing, enzymatic activity was detected with a phosphate citrate buffer containing 1 mg/ml o-phenylenediamine dihydro-chloride (Sigma) and hydrogen peroxide (0.06%). The reaction was stopped with 50 pl of 3 N HCl and the absorbance read at 491 nm in a microplate reader (Titertek multiskan MC340, Flow Lab., Baar, Switzerland). The levels of IL la in the samples were calculated by reference to the standard curve. The detection limit of I L l a was 15 pg/ml. All cytokine measurements have been assessed using the international standards obtained from the National Institute for Biologi- cal Standards and Controls (Herfordshire).
10000 cpm was added to each tube, and after vortexing left for a further incubation of 24 h at room temperature. On day 3, 500 pl of BSA buffer containing 6% PEG 8000 (Sigma), 1% horse anti-rabbit IgG (C. Rougeot, Institut Pasteur) and 0.1% normal rabbit serum were added. Tubes were vortexed, incubated for 1 h at room temperature and then centrifuged at 1500 x g for 15 min at room tempera- ture.Thereafter, the SN were discarded and the tubes kept inverted for 30 min and drained on absorbent paper. Tubes were counted in a gamma counter and the value for nonspecific binding subtracted. All standards and samples were expressed as a percentage of the standard containing noTNF-a (zero standard). The concentrations of TNF-a in pg/ml on the logarithmic X axis were plotted against the binding percentage on a logarithmic Y axis. The standard curve obtained was used to determine the TNF-a concen- trations in the samples. The detection limit was 70 pg/ml (set binding of 95% of zero standard).
2.8 ILll3 RIA
To remove putative factors present in plasma that might interfere with IL 1p RIA, a chloroform extraction was performed as described by Cannon et al. [28]. One milliliter of chloroform was transferred into a 1.5 ml Eppendorf tube containing 500 pl of plasma. Each tube was mixed vigor- ously for 10 min and centrifuged at 10 OOO x g for 10 min at 4 "C. This operation was repeated twice. The tube was left undisturbed for 20 rnin at room temperature. The aqueous phase was collected and stored at -30°C until assaying. A similar RIA protocol as that used for TNF-a measurement was used to determine the IL l p concentration. Standard IL 1p was obtained from RhGne Poulenc, rabbit anti-IL 1p antiserum diluted (1 : 100) was purchased from Genzyme and 1251-labeled IL l p (126-253 pCi/pg) from NEN. On day 3, 500 pl of BSA buffer containing 6% PEG 8000,1% of sheep anti-rabbit IgG (Sigma) and 0.05% normal rabbit serum were added to each tube. Determination of I L l p concentrations in plasma and samples were calculated as described above. The detection limit was 70 pg/ml.
2.9 IL la ELISA
IL la concentrations were determined by a specific ELISA method developed in our laboratory using two anti-IL la mAb which have been obtained in collaboration with J-C MaziC (Hydrolab, Institut Pasteur). Following immuniza- tion of BALB/c mice with human recombinant ILla (hrIL l a , kindly provided by RhGne Poulenc), spleen cells were fused with X63-Ag8.653 mouse myeloma cells [29]. Hybridoma cells were then tested for antibody production against I L l a by ELISA. Cells from positive wells were cloned by LD in microtiter plates. Ig subclass determina- tion was performed using mAb isotyping from Amersham Int. (Amersham, GB). Hybridomas were expanded for antibody production by i.p. injection into pristane-primed mice. Two antibodies were selected: one mAb (28-9) is an IgG1, and the other (2-12) is an IgG2b. These do not recognize the same epitope on the I L l a molecule, as judged by competition ELISA and do not bind to ILlp . Both inhibit the biological activity of IL la in the thymocyte co-mitogenic assay.
2.10 Statistical analysis
Statistical analysis was carried out using the paired or unpaired Student's t-test.
3 Results
3.1 Longitudinal study of plasma cytokines in septic patients
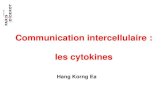
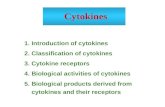
Plasma of septic patients drawn at different intervals following their admission to the ICU contained significant levels of cytokines, whereas no circulating cytokines were detected in plasma of healthy donors. Eight different examples are given in Fig. 1. Such kinetics indicate inde- pendent variations of the different cytokines ( i .e . IL lp , TNF-a and IL6): the presence and maximum levels for one given cytokine imply neither the presence nor the peak for another cytokine. The levels of circulating cytokines were usually higher during the course of ICU stay than at admission. For example, 3 out of the 21 septic patients who had no detectable plasma TNF-a initially, had significant levels of TNF-a later on. Maximum levels of circulating cytokines among septic patients are shown in Fig. 2. Circulating TNF-a and IL 6 were found in 86% and 81% of the septic patients, respectively. Importantly, only IL 6 plasma levels (initial as well as maximum) correlated with outcome. TNF-a was higher among septic non-surviving patients; however, initial or maximum levels of TNF-a among surviving and non-surviving septic patients were not statistically different. Initial and maximum levels of IL l p were lower, although not significantly, among patients with fatal outcome when compared to survivers. No IL la could be detected in any sera. No significant difference was noticed between patients with Gram-negative or Gram- positive infections (data not shown).

2180 C. Munoz, B. Misset, C. Fitting et al.
AM1
Eur. J. Irnrnunol. 1991. 21: 2177-2184
TNFo
Figure 1. Longitudinal study of circulating TNF-a (grey bars), IL 1p (dark bars) and IL6 (hatched bars) in eight septic patients (pa- tients MOR, SAN and BOU did not survive). TNF-a and IL l p are expressed as pg/ml (left Z axis) and IL6 as uni tshl (right Z axis). White bar represent values under detection limit.
3.2 Cell-associated cytokines in freshly isolated observed from time to time, with only 25% of the first determinations among septic patients being positive, and 50% of the septic patients having cell-associated IL 1@ at
Monocyte-associated -IL l a , IL l(3 and TNF-a levels at any time during the follow up of their monocytes.The most admission and during ICU stay (maximum levels) are frequent (88% of septic patients) and the most abundant shown in Table 1. Lower levels of IL 1@ and TNF-a were (410 ? 65 pg/106 monocytes) cell-associated cytokine was observed at admission, as compared to latter observations. TNF-a. Cell-associated IL la and IL l(3 were never I L l a was very rarely found in cell lysates. IL1@ was detected in freshly isolated monocytes from healthy
monocytes

Eur. J. Immunol. 1991. 22: 2177-2184 Plasma and monocyte-associated cytokines 2181
Table 1. Comparison between levels of monocyte-associated cyto- kines measured among septic patients (n = 16) ad admission and maximum levels observed during the longitudinal study
A
VO I KON MAR SAN MOR LET DOY PAR AM I J A N BOU DUB cou BIN GIL FER HAL
RAE ICA
LER EXj Survival (mean f SEM A43 ?. = Non survival (mean + SEM 217 nc/
: 25 pglml) f 41 pg/ml)
ULL v ; I
0 100 200 300
P m l
B
LET. ICA.
MAR. KON. cou. LER. JAN. MOR. DEL. VOI. BOU.
AMI.
DOY,
0 250 500 750 1000 1250
P m l
C
RAE MOR KON. JAN. VOI.
SAN LER.
MAR BOU. BIN AM I DOY ICA cou LET
46,000 40,000 30.000 11.800
Survival (mean f SEM = 638 * 158 ulml) DEL = Non survival (mean f SEM 15205 f 6430 ulrnl) FER GIL
0 2000 4000 6000 8000 10000 ulrnl
Figure 2. Maximum levels of circulating TNF-a, IL 1p and IL 6 among the septic patients. Hatched bars and black bars represent surviving and non-surviving patients, respectively. Symbol ( X ) indicates patients with detectable plasma TIW-a or IL l p but without detectable monocyte-associated corresponding cytokine, and symbol (0) indicates patients without detectable circulating TNF-a or IL 1p but with monocyte-associated corresponding cytokine. Mean values of TNF-a and IL l p were not statistically different between surviving or non-surviving patients, whereas the difference was significant for IL6 (p = 0.009). Cell-associated cytokines were not determined for patientsVOI and JAN. Dotted lines represent the detection limits.
Ph' Initial Maximum determinationa) observationa)
IL la <Detection limitc) 29 t 14C) NS")
IL1 p 41 k 19 153 5 60 0.046
410 t 65 O.(H)I TNF-a 275 f 58
(6%; < 15- 25)e) (25% ; < 15-90]
(25%; < 70-190) (50%; < 70-900)
(81%; < 70-620) (88%: < 70-700)
a) pg /W monocytes. b) Comparison between first and maximum levels (paired Stu-
dent's t-test). c) Mean5SEM. d) Not significant. e) % positive patients and range.
donors, and most of these did not haveTNF-a associated to their monocytes (50 f 29 pg/106 monocytes). Similar levels of cell-associated cytokines were found within cells of surviving or non-surviving patients (data not shown). No correlation was. found between the levels of cell-associated IL 16 and TNF-a in circulating monocytes and the levels of plasma cytokines. Some patients without detectable circu- lating TNF-a or IL 16 had the monocyte-associated corres- ponding cytokine and, inversely, some patients with circu- lating TNF-a or IL l p did not have any detectable mono- cyte-associated corresponding cytokine (see Fig. 2). Final- ly, at the end of the longitudinal study, most of the surviving patients no longer had plasmaTNF-a whereas most of them still had cell-associated TNF-a (Table 2). No significant difference was observed between the different type of infections.
3.3 Non-septic shock patients
Plasma cytokines could also be detected in patients with non-septic shock. Similarly to the infected group, we found
Table 2. Mean values of circulating TNF-a and monocyte-asso- ciated TNF-a detected at the end of the longitudinal study among septic patients
Surviving Non-surviving (n = 12) (n = 6)
Mean day of the last measurement: 1 4 5 2 105 3 Plasma TNF-a 24 Itr 16"' 12s 5 S3b)
Monocyte-associated 233 f 67") 372 k 90 (17%; <70-150)c) (67%; <70-20)
TNF-a (67%: < 70-580)" (100%0~ 100-600)
a) pg/ml. b) Comparison between surviving and non-surviving in patients:
c) YO Positive patients and range. d) pg/106 monocytes.
p = 0.03.

2182
Table 3. Circulating and monocyte-associated cytokines in patients with non-septic shock
C. Munoz, B. Misset, C. Fitting et al. Eur. J. Immunol. 1991. 21: 2177-2184
Maximum levels of plasma cytokines
Patients Type of S/NSh) ILlS TNF-a IL6 shocka) ( P g W (pglml) ( U W
1 Hypo S 80 190 400 2 Hem S 430 320 1100 3 Hem S 400 170 800 4 Card NS 90 160 (320 5 Card NS <70 260 (320 6 Card NS €70 230 t 3 2 0
large amounts of monocyte-associated TNF-a and observed that cell-associated IL 1p was more frequent than IL la (Table 3).
4 Discussion
Although circulating cytokines have been well documented in septic patients since 1987 [l-121, few longitudinal studies have been carried out to determine maximum levels of plasma cytokines and, to our knowlegde, only one report deals with simultaneous measurements of the three main cytokines, IL lp , IL6 and TNF-a [7]. However, in this last study the follow up did not exceed 36 h. We observed that levels of cytokines estimated within 48 h of admission of the patient into the ICU, were very often lower than later determinations. Altogether, 86% of the septic patients had at any moment circulating TNF-a. This high percentage, compared to other reports [l, 4, 8, 111 very likely reflects the fact that we performed a longitudinal study. Amounts of plasma TNF-a (range: < 70-350 pg/ml) are compatible with most other studies. Although non-surviving patients had higher amounts of circulating TNF-a than surviving ones, the difference was not significant for TNF-a levels either at admission or with maximum values. The absence of correlation we observed between TNF-a levels and fatal outcome, contrary to other reports [l, 2,5,7,11,12] might be due to the small number of patients.We did not find that high levels of IL 1p correlated with fatal issue as shown by other authors [2, 5, 71. Indeed, our results are closer to those reported by Cannon et nl. [3]. who found lower circul;itiiig 11. 11-i Icvcls ;imong non-surviving patients. Ikspitc the potential role t h a t 11. I may play in LPS shock I . 3 l l . II- I m a y ;ilso h;ivc sonic favorable activities such as d~.cIc-;rsirip rscliemi~~/rcpc.rlusio~i infury a s recently rcportcd \.;I 1. c w tiivoriiig antimicrobial i m m u n i t y (32-3-11.
Kcg;irding the prcscncc of 11-(> in plasma. our data is in agrccmcut n ith prcvious reports showing that 1L6 lcvcls corrclatc w i t h oiitcomc 17. 101. Indccd. we found that first Jctcrniinations ;is \vcII ;is maximum observations correlate v. i t h prognosis. 'l'hc ~xittci-ns ot the three cytokincs clearly intlic;itc t h a t thcir i l r 1.ir.o procliiclion are independcnt. For ~ w r i i p l e . 11- I ( ; C;III tw clc~cc-tccl in the absence of TNF-u aiicl iiicrc.;isc.\ i n II. I[-! o r 11.0 are not correlated with an iiicrc;isc iiiTYl~-(~.. 0 1 1 the contrary. ;I rise o f circulating ILO ot(cn par;illcls ; I tlccrcasc of .I'NF-ct. This may reflect the
Maximum levels of mono- cyte-associated cytokines
(pg/106 cells) ILlp TNF-a ILla
270 260 <15 a) Hypo: hypovolemic (pancreati- 320 600 35 tis); Hem: hemorrhagic (rup- 290 660 60 tured aortic aneurism); Card: <80 140 <15 cardiogenic (myocardial infarc- 240 260 <15 tion). 140 300 <15 b) S: surviving, NS: non-surviv-
ing.
inhibitory activity of IL 6 reported in in vitro experiments [35, 361.
During follow-up studies, all 6 patients with a non-septic shock had plasma TNF-a, 4/6 had IL 1p and 316 had IL6. These observations are in agreement with different reports indicating the presence of circulating cytokines in several pathologies in the absence of infection. Patients with heart failure [37,38] and hemorrhage [39] were reported to have elevated plasma levels of TNF-a. Similarly, plasma IL6 has been shown to be a marker for tissue damage [40,41]. No correlation was observed for these patients between high levels of any cytokines and the outcome.
In animal models the half-life of TNF-a is around 6-7 min [13]. A biphasic plasma clearance has been described for IL 1p [14] and IL6 [15] with an initial fast disappearance of 3 min and a second slower one (1-4 h). In this context, the fact that cytokines can be detected in plasma over a long period of time suggests an intensive production.The origin of these circulating cytokines remains to be fully eluci- dated. Although we found monocyte-associated TNF-a and IL 1p their levels did not correlate with the circulating ones. In the literature, little information is available on cell-associated cytokines in freshly isolated monocytes, and to our knowledge it is the first time that cell-associated cytokines are reported in septic and non-septic shock. Since it is well known that IL 1 can accumulate within activated monocytes, investigations have been performed mainly for this cytokine [16, 171. IL la is the main cell-associated form of K 1 in LPS-stimulated human monocytes [18, 19].Thus, we were surprised to very rarely find I L l a within the adherent cells isolated from septic patients. Of interest was the discovery of frequent cell-associated TNF-a (90% of patients) in freshly isolated monocytes. Furthermore, the average levels at admission (275 k 58 pg/106 moncoytes) or the maximum ones (410 k 65 pg/106 monocytes) were particularly elevated compared to cell-associated TNF-a which could be detected in in vitro LPS-activated human monocytes (Le. 98 * 43 pg/106 monocytes; C. Munoz, unpublished results). Despite the fact that we never found a correlation between plasma levels of TNF-a and its content within monocytes, it is noteworthy that in both cases, TNF-ci was the most frequently detected cytokine. This absence of a correlation between plasma and cell content vducs might suggest that circulating monocytes are not the o n l y sources of circulating cytokines and that other cells

Eur. J. Immunol. 1991.21: 2177-2184
such as Kupffer cells, spleen M@ or alveolar M@ could also participate in this production.
The exact nature of monocyte-associated cytokines remains to be fully established. They may be cytokines present within the cytoplasm or on the cell surface, either as a membrane component or bound to their receptors. It is quite probable that it was mainly cytoplasmic cytokines. IL la constitutes the only membrane form of IL 1, and we mainly found IL l p which can be accumulated within the cell. The absence of monocyte-associated cytokines among some patients who had detectable plasma cytokines sug- gests that cell-associated forms do not represent cytokines bound to their receptor. The exact nature of the inducer(s) remains also to be established. Although bacterial products are putative stimuli in sepsis, the presence of cell-associated cytokines within monocytes from patients with noninfec- tious shock suggests that some factors generated during stress are probable activators of monocytes. In addition, one cannot exclude that one or many of the numerous drugs given to the patients may participate to the monocyte activation.
Interestingly, at the end of the survey of surviving patients, when detectable plasma TNF-a was mostly no longer found, monocyte-associated TNF-a was still observed. These data indicate that cell activation still occurs in these ICU patients and suggests that the measurement of cell- associated cytokine might be a more accurate assessment of cytokine production in vivo than evaluation of plasma cytokine.
We are very grateful to Dr. Jean-Claude Mazie' (Hybridolab, lnstitut Pasteur) for his fruitful collaboration in the preparation of anti- human IL I u mAb. We thank Frangoise Fouque (Departement des Enseignements, Institut Pasteur) for her contribution in setting up the ELISA for IL I u, Catherine Rougeot (Unit6 de RIA, Institut Pasteur) for her gift of rabbit anti-human TNF-a and her valuable help in establishing the RIA for TNF-a, and Dr. Jacques Van Snick (Ludwig Institute for Cancer Research, Brussels) for his gift of the 7TDI cell line. We thank Marie-Franqoise Dumay (Intensive Care Unit, Hdpital St. Joseph) for her efficient collaboration.
Received May 21, 1991.
5 References Waage, A., Halstensen, A. and Espevik, T., Lancet 1987. i: 355. Girardin, E., Grau, G. E., Dayer, J. M., Roux-Lombard, F!, The J5 Study Group and Lambert, P. H., N. Engl. J. Med. 1988. 319: 397. Cannon, J. G. ,Tompkins, R. G., Gelfand, J. A., Michie, H. R., Stanford, G. G., Van Der Meer, J. W. M., Endres, S., Lonnemann, G., Corsetti, J, Chernow, B., Wilmore, D. W., Wolff, S. M., Burke, J. F. and Dinarello, C. A., J. Infect. Dis. 1990. 161: 79. Marks, J. D., Berman-Marks, C., Luce, J. M., Montgomery, A. B., Turner, J., Metz, C. A. and Murray, J. F., Am. Rev. Respir. Dis. 1990. 141: 94. Calandra, T., Baumgartner, J. D., Grau, G. E., Wu, M. M., Lambert, P. H., Schellekens, J.,Verhoef, J., Glauser, M. F! and The Swiss-Dutch J5 Immunoglobulin Study Group, J. Infect. Dis. 1990. 161: 982.
6 Mustafa, M. M., Mertsola, J., Ramilo, O., Saez-Llorens, X., Risser, R. C. and McCracken G. H., Jr., J. Infect. Dis. 1989. 160: 891.
I
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
Plasma and monocyte-associated cytokines 2183
- Waage, A., Brandtzaeg, €!, Halstensen, A., Kierulf, €! and Espeiik, T., J. Exp. Mid. 1989. 169: 333. Helfgott, D. C., Tatter, S. B., Santhanam, U., Clarick, R. H., Bhardwaj, N., May, L.T. and Sehgal, I? B., J. Irnmunol. 1989. 142: 948. Hack, C. E., De Groot, E. R., Felt-Bersma, R. J. F., Nuijens, J. H., Strack Van Schijndel, R. J. M., Eerenberg-Belmer, A. J. M.,Thijs, L. G. and Aarden, L. A., Blood 1989. 74: 1704. De Groot, M. A., Martin, M. A., Densen, F!, Pfaller, M. A. and Wenzel, R. P., J. Am. Med. Assoc. 1989. 262: 249. Marano, M. A., Fong,Y., Moldawer, L. L.,Wei, H., Calvano, S. E. ,Tracey, K. J., Bane, F? S., Manogue, K., Cerami, A., Shires, G. T. and Lowry, S. F., Surg. Gynecol. Obstet. 1990. 170: 32. Offner, F., Philippt, J.,Vogelaers, D., Colardyn, F., Baele, G., Baudrihaye, M.,Vermeulen, A. and Leroux-Roels, G., J. Lab. Clin. Med. 1990. 116: 100. Beutler, B. A., Milsark, I. W. and Cerami, A., J . lmmunol. 1985.135: 3972. Klapproth, J., Castell, J., Geiger,T., Andus,T. and Heinrich, R C., Eur. J. lrnmunol. 1989. 19: 1485. Castell, J. V., Geiger, T., Gross, V , Andus, T., Walter, E., Hirano,T., Kishimoto,T. and Heinrich, P. C., Eur. J . Biochem. 1988. 177: 357. Haeffner-Cavaillon, N., Cavaillon, J. M., Ciancioni, C., Bacle, F., Delons, S. and Kazatchkine, M. D., Kidney Int. 1989. 35: 1212. Haeffner-Cavaillon, N., Roussellier, N., Ponzio, O., Carreno, M. F!, Laude, M., Carpentier, A. and Kazatchkine, M. D., J. Thorac. Cardiovasc. Surg. 1989. 98: 1100. Endres, S., Cannon, J. G., Ghorbani, R., Dempsey, R. A., Sisson, S. D., Lonnemann, G. ,Van der Meer, J. W. M., Wolff, S. M. and Dinarello, C. A., Eur. J. lmmunol. 1989. 19: 2321. Cavaillon, J. M. and Haeffner-Cavaillon, N., Cytokine 1990.2: 313. Bone, R. C., Fishe, C. J., Clemmer,T. P., Slotman, G. J., Metz, G. A., Balk, R. A. and The Methylprednisolone Severe Sepsis Study Group, Crit. Care Med. 1989. 17: 389. Le Gall, J. R., Loirat, l?, Alperovitch, A., Glaser, F!, Granthil, C., Mathieu, D., Mercier, F! , Thomas, R. and Vilers, D., Crit. Care Med. 1984. 12: 975. Tucker, S. B., Pierre, R . V and Jordon, R. E., J. Immunol. Methods 1977. 14: 267. Cavaillon, J. M., Fitting, C. and Haeffner-Cavaillon, N., Eur. J. Imrnunol. 1990. 20: 253. Cavaillon, J. M., Fitting, C., Haeffner-Cavaillon, N., Kirsch, S. J. and Warren, H. S., Infect. Immun. 1990. 58: 2375. Van Snick, J., Cayphas, S. ,Vink, A,, Uyttenhove, C., Coulie, F! G., Rubira, M. R. and Simpson, R. J., Proc. Natl. Acad. Sci. USA 1986. 83: 9679. Hansen, M. B., Nielsen, S. E. and Berg, K., J. Immunol. Methods 1989. 119: 203. Van der Meer, J.W. M., Endres, S., Lonnemann, G., Cannon, J. G., Ikejima,T., Okusawa, S., Gelfand, J. A. and Dinarello, C. A.. J. Leuk. Biol. 1988. 43: 216.
28 Cannon, J. G., Van der Meer, J. W. M., Kwiatkowski, D., Endres, S., Lonnemann, G., Burke, J. F. and Dinarello, C. A., Lymphokine Res. 1988. 7: 457.
29 Kearney, J. F., Radbruch, A., Liesegang, B. and Rajewsky, K., J. lmmunol. 1979. 123: 1548.
30 Ohlsson, K., Bjork, l?, Bergenfeld, M., Hageman, R. and Thompson, R. C., Nature 1990. 348: 550.
31 Brown, J. M., White, C. W., Terada, L. S., Grosso, M. A., Shanley, l? F., Mulvin, D.W., Banerjee, A.,Whitman, G. J. R., Harken, A. H. and Repine, J. E., Proc. Natl. Acad. Sci. USA 1990. 87: 5026.
32 Czuprynski, C.J., Brown, J. F.,Young, K. M., Cooley, A. J. and Kurtz, R. S., J. Immunol. 1988. 140: 962.
33 Minami, A., Fujimoto, K., Ozaki,Y. and Nakamura, S., Infect. Irnrnun. 1988. 56: 3116.
34 Morikage, T., Mizushima, Y., Sakamoto, K. and Yano, S., Cancer Res. 1990. 50: 2099.

2184 C. Munoz, B. Misset, C. Fitting et al.
35 Aderka, D., Le, J. and Vilcek, J., J. Irnmunol. 1989. 143:
36 Schindler, R., Mancilla, J., Endres, S., Ghorbani, R., Clark, S.
37 Maury, C. €? J. and Teppo, A. M., J. Internal Med. 1989. 225:
38 Levine, B., Kalman, J., Mayer, L., Fillit, H. M. and Packer, M.,
3517.
C. and Dinarello, C. A., Blood 1990. 75: 40.
333.
N . Engl. J. Med. 1990. 323: 236.
Eur. J. Immunol. 1991. 21: 2177-2184
39 Ayala, A., Perrin, M.M., Meldrum, D. R., Ertel, W. and Chaudry, I. H., Cytokine 1990. 2: 170.
40 Nijsten, M. W. N., De Groot, E. R. ,Ten Duis, H. J., Klasen, H. J., Hack, C. E. and Aarden, L. A., Lancet 1987. ii: 921.
41 Nishimoto, N.,Yoshizaki, K., Tagoh, H., Monden, M., Kishi- moto, S., Hirano, T. and Kishimoto, T., Clin. Imrnunol. Imrnunopathol. 1989. 50: 399.