Disordered - Cengage2 Eating disorders result from psychological, and not biological, causes. 3...
16
Disordered Eating: Anorexia Nervosa, Bulimia, and Pica Nutrition Scoreboard Answers on next page TRUE FALSE 1 The United States has one of the world’s highest rates of anorexia nervosa. 2 Eating disorders result from psychological, and not biological, causes. 3 People in many different cultures may consume clay, dirt, and other nonfood substances. PROPERTY OF LEARNING FOR REVIEW ONLY – NOT FOR SALE OR CLASSROOM USE CENGAGE
Transcript of Disordered - Cengage2 Eating disorders result from psychological, and not biological, causes. 3...
DisorderedEating:
AnorexiaNervosa,
Bulimia, andPica
Nutrition Scoreboard
Answ
ers
on n
ext
page
TRU
E
FALS
E
1 The United States has one of the world’s highestrates of anorexia nervosa.
2 Eating disorders result from psychological, and notbiological, causes.
3 People in many different cultures may consume clay,dirt, and other nonfood substances.
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 1
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

[ KEY CONCEPTS AND FACTS ]
• Anorexia nervosa, bulimianervosa (bulimia), binge-eating disorder, and pica arefour specific eating disor-ders. They may seriouslythreaten health.
• Eating disorders are muchmore common in femalesthan males.
• The incidence of eating dis-orders in a society is related
to the value placed onthinness by that society.
• An important route to theprevention of anorexianervosa and bulimia is tochange a society’s culturalideal of thinness and toeliminate biases againstpeople (especially women)who are not thin.
Answers to Nutrition Scoreboard
TRU
E
FALS
E
1 Anorexia nervosa is most common in the UnitedStates and other Westernized countries. It is rarelyobserved in developing, non-Westernized nations.1
2 The cause (or causes) of eating disorders is not yetknown. Both psychological and biological factorsmay play a role.
3 Although not recommended for health reasons, peo-ple in many different cultures practice pica—theregular ingestion of nonfood items such as clay and dirt.
✔
✔
✔
The Eating DisordersThree square meals a day, an occasional snack or missed meal, and caloric intakesthat average out to match the body’s need for calories—this set of practices is con-sidered “orderly” eating. Self-imposed semi-starvation, feast and famine cycles,binge eating, purging, and the regular consumption of nonfood substances such aspaint chips and clay—these behaviors are symptoms of disordered eating.
Four specific types of disordered eating patterns are officially recognized as eat-ing disorders and have been assigned diagnostic criteria. They are (1) anorexia ner-vosa, (2) bulimia nervosa, (3) binge-eating disorder, and (4) pica.2 Other forms ofdisordered eating such as compulsive overeating, restrained eating, and food preoc-cupation have been observed, but too little research exists to establish criteria fordiagnosis.
Anorexia NervosaIt’s about 9:30 on a Tuesday night. You’re at the grocery store picking upsandwich fixings and some milk. Although your grocery list contains onlyfour items, you arrive at the checkout line with a half-filled cart. The womanin front of you has only five items: a bag with about 10 green beans, anapple, a bagel, a green pepper, and a 4-ounce carton of nonfat yogurt. As shecarefully places each item into her shopping bag, you notice that she isdreadfully thin.
The woman is Alison. She has just spent half an hour selecting the foodshe will eat tomorrow. Alison knows a lot about the caloric value of foodsand makes only low-calorie choices. Otherwise, she will never get rid of herexcess fat. To Alison, weight is everything—she cannot see the skeleton-likeappearance others see when they look at her.
As a child, Alison enjoyed little independence. Decisions about her lifewere made for her, a situation that contributed to her low self-esteem. Dur-ing her teen years, Alison was overweight and clearly remembers the painful
purgingThe use of self-induced vomit-ing, laxatives, or diuretics(water pills) to prevent weight gain.
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 2
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

teasing and ridicule she had to endure. Now Alison is on her own, awayfrom home and in control in an out-of-control way.
You didn’t know this about Alison when you saw her. There is muchmore to anorexia nervosa than meets the eye.
Individuals with anorexia nervosa starve themselves (Illustra-tion 11.1). They can never be too thin—no matter how emaci-ated they may be. As shown in Illustration 11.2, people withanorexia nervosa look extraordinarily thin from the neckdown. The face and the rest of the head usually look normalbecause the head is the last part of the body to be affected bystarvation.
Instead of the normal amount of body fat (20–25% ofbody weight), people with anorexia nervosa have little fat(7–13% of body weight).3 They become cold easily and haveunusually low heart rates and sometimes an irregular heart-beat, dry skin, low blood pressure, absent or irregular men-strual cycles, infertility, and poor pregnancy outcomes (Table11.1).4 Approximately 9 in 10 women with anorexia nervosahave significant bone loss, and 38% have osteoporosis. Theextent of bone loss correlates strongly with undernutrition: thelower the body weight, the lower the bone density. Improvingcalcium and vitamin D intakes and use of bone-density drugshave limited effectiveness in rebuilding bones in females withcurrent or past anorexia nervosa.5
The Female Athlete Triad] Pediatricians, nutritionists, andcoaches are beginning to be on the lookout for eating disor-ders, menstrual cycle dysfunction, and decreased bone mineraldensity in young, female athletes. Low caloric intakes andunderweight related to eating disorders can lower estrogen lev-els and disrupt menstrual cycles. The lack of estrogendecreases calcium deposition in bones and reduces bone den-sity at a time when peak bone mass is accumulating.
Illustration 11.1A day’s diet? For a person withanorexia nervosa, it was. Thefoods shown provide approxi-mately 562 calories.
Illustration 11.2Eating disorders occur in males as well as females, butfemales make up approximately 95% of all cases.
anorexia nervosaAn eating disorder character-ized by extreme weight loss,poor body image, and irra-tional fears of weight gain andobesity.
Phot
oEdi
t, Fe
licia
Mar
tinez
Rich
ard
Ande
rson
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 3
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

Irregular or absent menstrual cycles used to be thought of as “no big deal.”That attitude has changed, however, due to research results indicating that abnor-mal cycles in young females are related to delayed healing of bone and connectivetissue injuries, and to bone fractures and osteoporosis later in life.6
Motivations Underlying Anorexia Nervosa] The overwhelming desire tobecome and remain thin drives people with anorexia nervosa to refuse to eat, evenwhen ravenously hungry, and to exercise intensely. Half of the people with anorexiaturn to binge eating and purging—features of bulimia nervosa—in their efforts tolose weight.7 Preoccupied with food, people with anorexia may prepare wonderfulmeals for others, but eat very little of the food themselves. Family members andfriends, distressed by their failure to persuade the person with anorexia to eat,
TABLE 11.1
FEATURES OF ANOREXIA NERVOSA.Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edi-tion, Text Revision. Copyright 2000 American Psychiatric Association.
A. Essential Features1. Refusal to maintain body weight at or above 85% of normal weight for age and
height.2. Intense fear of gaining weight or becoming fat, despite being underweight.3. Disturbance in the way in which body weight or shape is experienced, undue influ-
ence of body weight or shape on self-evaluation, or denial of the seriousness of cur-rent low body weight.
4. Lack of menstrual periods in teenage females and women (missing at least three con-secutive periods).
Restricting type: Person does not regularly engage in binge-eating or purging behavior.Binge-eating type: Person regularly engages in binge-eating or purging behavior (self-induced vomiting; laxative, diuretic, or enema use).
B. Common Features in Females1. Low-calorie diet, extensive exercise, low body fat2. Soft, thick facial hair, thinning scalp hair3. Loss of heart muscle, irregular, slow heartbeat4. Low blood pressure5. Increased susceptibility to infection6. Anemia7. Constipation8. Low body temperature (hypothermia)9. Dry skin
10. Depression11. History of physical or sexual abuse12. Low estrogen levels13. Low bone density14. Infertility, poor pregnancy outcome
C. Common Features in Males1. Most of the common features in females2. Substance abuse3. Mood and other mental disorders
The average size of femalegymnasts on the U.S.Olympic team shrank from5 feet 3 inches tall and 105pounds in 1976 to 4 feet 9inches tall and 88 poundsin 1992.
ON
TH
E SI
DE
binge eatingThe consumption of a largeamount of food in a smallamount of time.
Phot
o Di
sc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 4
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

report high levels of anxiety. Although adults often describe people with anorexiaas “model students” or “ideal children,” their personal lives are usually marred bylow self-esteem, social isolation, and unhappiness.8
What Causes Anorexia Nervosa?] The cause of anorexia nervosa isn’t yet clear.It is likely that many different conditions, both psychological and biological, pre-dispose an individual to become totally dedicated to extreme thinness.9 The valuethat Western societies place on female thinness, the need to conform to society’sexpectations of acceptable body weight and shape, low self-esteem, and a need tocontrol some aspect of one’s life completely are commonly offered as potentialcauses for this disorder (Illustration 11.3).10
How Common Is Anorexia Nervosa?] It is estimated that 1% of adolescent andyoung women in the Western world and less than 0.1% of young males haveanorexia nervosa. The disorder has been reported in girls as young as 5 and inwomen through their forties;11 however, it usually begins during adolescence. It isestimated that one in ten females between the ages of 16 and 25 has “subclinical”anorexia nervosa, or exhibits some of the symptoms of the disorder.12
Certain groups of people are at higher risk of developing anorexia nervosa thanothers (Table 11.2). People at risk come from all segments of society, but tend to beoverly concerned about their weight and food, and have attempted weight loss froman early age.14
Treatment] There is no “magic bullet” treatment that cures anorexia nervosaquickly and completely. In all but the least severe cases, the disorder generally takesa good deal of time and professional help to correct. Treating the disorder is oftendifficult because few people with anorexia believe their weight needs to beincreased.15
Treatment programs for anorexia nervosa generally focus on restoring nutri-tional health and body weight, psychological counseling to improve self-esteem and
Illustration 11.3
There is a need for a morerealistic body shape on
television and in fashionmagazines.
—Vivienne Nathanson, Britishphysician, 2000
TABLE 11.2
RISK GROUPS FORANOREXIA NERVOSA.13
• Dieters
• Ballet dancers
• Competitive athletes(gymnasts, figureskaters)
• Fitness instructors
• Dietetics majors
• People with type 1(insulin dependent)diabetes
Rich
ard
Ande
rson
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 5
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

attitudes about body weight and shape, antidepressant or other medications, familytherapy, and normalizing eating and exercise behaviors. These programs are suc-cessful in 50% of people, and partially successful in most other cases.16 One-thirdof people with full recovery from anorexia nervosa will relapse within 7 years orless. By 8 years after diagnosis, 3% of people with anorexia nervosa will have diedfrom the disorder, and it claims the lives of 18% 33 years later. Results of treatmentare often excellent when the disorder is treated early.17 Unfortunately, many peoplewith the condition deny that problems exist and postpone treatment for years. Ini-tiation of treatment is often prompted by a relative, coach, or friend.18
Bulimia NervosaFinally home alone, Lisa heads to the pantry and then to the freezer. She hascarefully controlled her eating for the last day and a half and is ready to eateverything in sight.
It’s a bittersweet time for her. Lisa knows the eating binge she is preparingwill be pleasurable, but that she’ll hate herself afterward. Her stomach willache from the volume of food she’ll consume, she’ll feel enormous guilt fromlosing control, and she’ll be horrified that she may gain weight and will haveto starve herself all over again. Lisa is so preoccupied with her weight andbody shape that she doesn’t see the connection between her severe dietingand her bouts of uncontrolled eating. To get rid of all the food she is aboutto eat, she will do what she has done several times a week for the last year.Lisa avoids the horrible feelings that come after a binge by “tossing” every-thing she ate as soon as she can.
In just 10 minutes, Lisa devours 10 peanut butter cups (the regular size), a12-ounce bag of chocolate chip cookies, and a quart of mint chocolate chipice cream. Before 5 more minutes have passed Lisa will have emptied herstomach, taken a few deep breaths, thrown on her shorts, and started the 5-mile route she jogs most days. As she jogs, she obsesses about getting her138-pound, 5-foot 5-inch frame down to 115 pounds. She will fast tomor-row and see what news the bathroom scale brings.
Lisa is not alone. Bulimia nervosa occurs in 1 to 3% of young women and in about0.5% of young males in the United States.19 The disorder is characterized by regu-lar episodes of dieting, binge eating, and attempts to prevent weight gain by purg-ing; use of laxatives, diuretics, or enemas; dieting; and sometimes exercise. In mostcases, bulimia nervosa starts with voluntary dieting to lose weight. At some point,voluntary control over dieting is lost, and people feel compelled to engage in bingeeating and vomiting.20 The behaviors become cyclic: food binges are followed byguilt, purging, and dieting. Dieting leads to a feeling of deprivation and intensehunger, which leads to binge eating, and so on. Once a food binge starts, it is hardto stop.
Table 11.3 lists the features of bulimia nervosa. Approximately 86% of peoplewith this condition vomit to prevent weight gain and avoid postbinge anguish. Asmaller proportion of people use laxatives, diuretics (water pills), or enemas aloneor in combination with vomiting.22 Laxatives, enemas, and diuretics do not preventweight gain, however, and their regular use can be harmful. The habitual use of lax-atives and enemas causes “laxative dependency”—these products become necessaryfor bowel movements. Diuretics can cause illnesses by depleting the body of waterand certain minerals and disturbing its fluid balance.23
The lives of people with bulimia nervosa are usually dominated by conflictsabout eating and weight. Some affected individuals are so preoccupied with food
bulimia nervosa An eating disorder character-ized by recurrent episodes ofrapid, uncontrolled eating oflarge amounts of food in ashort period of time. Episodesof binge eating are often fol-lowed by purging.
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 6
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

that they spend days securing food, bingeing, and purging. Others experience onlyoccasional episodes of binge eating, purging, and fasting.24
Unlike those with anorexia nervosa, people with bulimia usually are not under-weight or emaciated. They tend to be normal weight or overweight.25 Like anorexianervosa, bulimia nervosa is more common among athletes (including gymnasts,weight lifters, wrestlers, jockeys, figure skaters, physical trainers, and distance run-ners) and ballet dancers than in other groups.26
Bulimia nervosa leads to major changes in metabolism. The body must con-stantly adjust to feast and famine cycles and mineral and fluid losses. Salivary glandsbecome enlarged, and teeth may erode due to frequent vomiting of highly acidicfoods from the stomach.27
TABLE 11.3
FEATURES OF BULIMIA NERVOSA.21
Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edi-tion, Text Revision. Copyright 2000 American Psychiatric Association.
A. Essential Features1. Recurrent episodes of binge eating. An episode of binge eating is characterized by
both of the following:a. Eating an amount of food within a two-hour period of time that is definitely
larger than most people would eat in a similar amount of time and under similarcircumstances.
b. A sense of lack of control over eating during the episode; a feeling that one can-not stop eating or control what or how much one is eating.
2. Recurrent inappropriate compensatory behavior in order to prevent weight gain, suchas self-induced vomiting; misuse of laxatives, diuretics, enemas, or other medications;fasting; or excessive exercise.
3. The binge eating and inappropriate compensatory behaviors both occur, on average,at least twice a week for 3 months.
4. Self-evaluation is unduly influenced by body weight and shape.5. The disturbance does not occur exclusively during episodes of anorexia nervosa.Purging type: The person regularly engages in self-induced vomiting or the misuse of laxatives, diuretics, or enemas.Nonpurging type: The person regularly engages in fasting or excessive exercise but does not regularly engage in self-induced vomiting or the misuse of laxatives, diuretics, or enemas.
B. Common Features1. Weakness, irritability2. Abdominal pain, constipation, bloating3. Dental decay, tooth erosion4. Swollen cheeks and neck5. Binge on high-calorie foods6. Eat in secret7. Normal weight or overweight8. Guilt and depression9. Substance abuse
10. Dehydration11. Impaired fertility12. History of sexual abuse
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 7
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

Is the Cause of Bulimia Nervosa Known?]
“Do you follow a special diet?” asks the dietitian at the eating disorder clinic.
“Yes,” answers the client with bulimia. “Feast or famine.”
The cause of bulimia nervosa is not known with certainty, but the scientific fingeris pointing at depression, abnormal mechanisms for regulating food intake, andfeast-and-famine cycles as possible causes.28 Fasts and restrained eating mayprompt feelings of deprivation and hunger that may trigger binge eating.29 The idealthinness may become more and more difficult to achieve as the feast-and-faminecycles continue.
Treatment] The cornerstone of bulimia treatment is nutrition and psychologicalcounseling to break the feast-and-famine cycles. Replacing the disordered pattern ofeating with regular meals and snacks often reduces the urge to binge and the needto purge. Psychological counseling aimed at improving self-esteem and attitudestoward body weight and shape goes hand in hand with nutrition counseling. Inmany cases, antidepressants are a useful component of treatment.30 The full recov-ery of women with bulimia nervosa is higher than that for anorexia nervosa. Nearlyall women with bulimia achieve partial recovery, but one-third will relapse intobingeing and purging within 7 years.31 Bulimia nervosa usually improves substan-tially during pregnancy; about 70% of women with the condition will improve theireating habits for the sake of their unborn baby.32
Binge-Eating DisorderPsychiatrists now recognize an eating disorder called binge-eating disorder (Table11.4). People with this condition tend to be overweight or obese, and one-third aremale.34 Like individuals with bulimia nervosa, people with binge-eating disorder eatseveral thousand calories’ worth of food within a short period of time during a soli-tary binge, feel a lack of control over the binges, and experience distress or depres-sion after the binges occur. People must experience eating binges twice a week onaverage over a period of 6 months to qualify for the diagnosis. Unlike individuals
with bulimia nervosa, however, people with binge-eating disorder don’tvomit, use laxatives, fast, or exercise excessively in an attempt to control
weight gain.35
It is estimated that 9 to 30% of people in weight-control pro-grams and 30 to 90% of obese people have binge-eating disor-der.36 The condition is far less common (2 to 5%) in the generalpopulation.37 Stress, depression, anger, anxiety, and other nega-tive emotions appear to prompt binge-eating episodes. Prelimi-nary evidence indicates that binge-eating disorder may be relatedto a genetic mutation that impairs control of normal eatingbehavior.38
The Treatment Approach to Binge-Eating Disorder] Thetreatment of binge-eating disorder focuses on both the disor-dered eating and the underlying psychological issues.39 Personswith this condition will often be asked to record their foodintake, indicate bingeing episodes, and note feelings, circum-stances, and thoughts related to each eating event (Illustration11.4). This information is used to identify circumstances thatprompt binge eating and practical alternative behaviors that may
restrained eatingThe purposeful restriction offood intake below desiredamounts in order to controlbody weight.
binge-eating disorderAn eating disorder character-ized by periodic binge eating,which normally is not followedby vomiting or the use of laxa-tives. People must experienceeating binges twice a week onaverage over a period of 6months to qualify for the diagnosis.
TABLE 11.4
FEATURES OF BINGE-EATING DISORDER.33
1. Rapid consumption of extremely largeamounts of food (several thousand calories)in a short period of time
2. Two or more such episodes of binge eatingper week over a period of 6 months
3. Binge eating by oneself
4. Lack of control over eating or an inability tostop eating during a binge
5. Postbinge-eating feelings of self-hatred,guilt, and depression or disgust
6. Purging, fasting, excessive exercise, or othercompensation for high-calorie intakes notpresent
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 8
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE
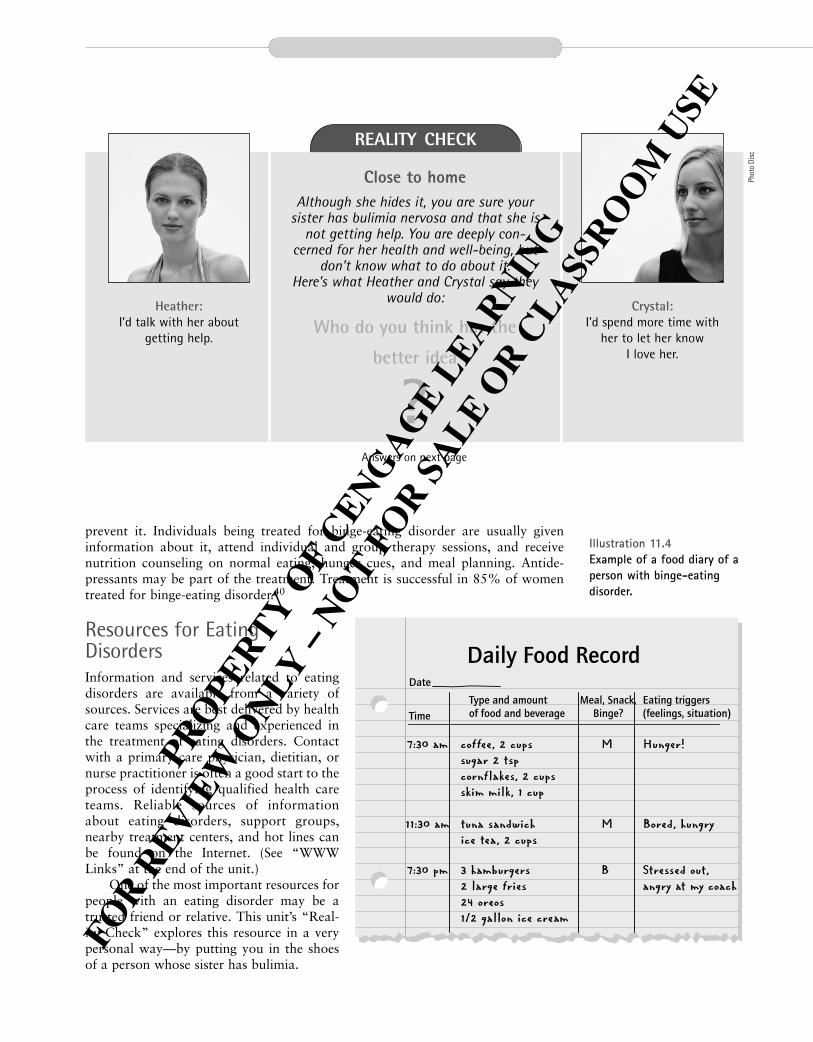
prevent it. Individuals being treated for binge-eating disorder are usually giveninformation about it, attend individual and group therapy sessions, and receivenutrition counseling on normal eating, hunger cues, and meal planning. Antide-pressants may be part of the treatment. Treatment is successful in 85% of womentreated for binge-eating disorder.40
Resources for EatingDisordersInformation and services related to eatingdisorders are available from a variety ofsources. Services are best delivered by healthcare teams specializing and experienced inthe treatment of eating disorders. Contactwith a primary care physician, dietitian, ornurse practitioner is often a good start to theprocess of identifying qualified health careteams. Reliable sources of informationabout eating disorders, support groups,nearby treatment centers, and hot lines canbe found on the Internet. (See “WWWLinks” at the end of the unit.)
One of the most important resources forpeople with an eating disorder may be atrusted friend or relative. This unit’s “Real-ity Check” explores this resource in a verypersonal way—by putting you in the shoesof a person whose sister has bulimia.
Illustration 11.4Example of a food diary of aperson with binge-eating disorder.
Daily Food RecordDate
TimeType and amountof food and beverage
Eating triggers(feelings, situation)
Meal, Snack,Binge?
7:30 am coffee, 2 cupssugar 2 tspcornflakes, 2 cupsskim milk, 1 cup
M Hunger!
11:30 am tuna sandwichice tea, 2 cups
M Bored, hungry
7:30 pm 3 hamburgers2 large fries24 oreos1/2 gallon ice cream
B Stressed out,angry at my coach
REALITY CHECKPortion Distortion
Close to homeAlthough she hides it, you are sure your
sister has bulimia nervosa and that she isnot getting help. You are deeply con-
cerned for her health and well-being, butdon’t know what to do about it.
Here’s what Heather and Crystal say theywould do:
Who do you think has the
better idea
?
Heather: I’d talk with her about
getting help.
Crystal: I’d spend more time with
her to let her know I love her.
Answers on next page
Phot
o Di
sc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 9
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

Undieting: The Clash between Culture and Biology
There is a saying that women underreport their weight and men overreport theirheight. Clearly there are cultural norms at work here.
—L. Cohen, 200142
The pressure to conform to society’s standard of beauty and acceptability is thoughtto be a primary force underlying the development of eating disorders.43 Childrenacquire prevailing cultural values of beauty before adolescence. As early as age 5,American children learn to associate negative characteristics with people who areoverweight and positive characteristics with those who are thin.44 Standards ofbeauty defined by models and movie and television stars often include thinness, but
ANSWERS TO REALITY CHECK
Close to homeBoth ideas are admirable and deserve a
thumbs-up. Heather’s idea is aimed directly athelping her sister consider treatment and maybe the appropriate action to take sometimes.There is a way to talk to a relative or friendabout your concerns for them that may helpboth of you. Learn more about it from the
information presented in Table 11.5.
�Heather
�Crystal
TABLE 11.5
HELPING A FAMILY MEMBER OR FRIEND WITH AN EATING DISORDER.
Whether at work, home, or play, many of us experience anxiety and a sense of helplessnesswhen someone we love is living with an eating disorder. We may feel compelled to takeaction to help, but aren’t sure what to do or how to do it. Here are some tips on how toexpress your concerns to a friend or relative with an eating disorder.
1. Gather information about services for people with eating disorders to share with yourfriend or relative.
2. Talk with your friend or relative privately when there is enough time to fully discuss theissue. Tell them you are worried and that they may need to seek help.
3. Encourage your friend or relative to express his or her feelings, and then listen intently.Be accepting about the feelings that are expressed. Be ready to talk to them more aboutit in the future.
4. Do not argue with your friend or relative about whether she or he has an eating disor-der. Let your friend or relative know you heard what was said, but that you are con-cerned that he or she may not get better without treatment.
5. Seek emergency medical help in life-threatening situations.
Only individuals with an eating disorder can make the decision to get help. Knowledge thatpeople who love them will be around to support them and their decision to seek treatmentmay help encourage the person with an eating disorder to take action.41
Phot
o Di
sc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 10
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

the body shape portrayed as best is often unhealthfully thin and unattainable bymany. The disparity between this ideal and what people normally weigh has led towidespread discontent. Approximately 50% of normal-weight adult women are dis-satisfied with their weight; and many diet, binge, and purge occasionally or fast inan attempt to reach the standard of beauty set for them.45
A movement toward acceptance of body size, fashionable attire for larger peo-ple, full-size models, and a more realistic view of individual differences in bodyshapes is emerging slowly in America (Illustration 11.5). Acceptance of a realisticstandard of body weight and shape—one that corresponds to health and physicalfitness—and respect for people of all body sizes may be the most effective measuresthat can be taken to prevent anorexia nervosa, bulimia nervosa, and binge-eatingdisorder.
PicaWhen did I start eating clay? I know it might sound strange to you, but Istarted craving clay in the summer of ’58. It was a beautiful spring morn-ing—it had just rained. I smelled something really sweet in the breeze com-ing in my bedroom window. I went outside and knew instantly where thesweet smell was coming from. It was the wet clay that lies all around myhouse. I scooped some up and tasted it. That’s when and how I started mycraving for that sweet-smelling clay. I keep some in the fridge now because ittastes even better cold.
A most intriguing type of eating disorder, pica has been observed in chimpanzeesand in humans in many different cultures since ancient times.46 The history and per-sistence of pica might suggest that the practice has its rewards. Nevertheless, impor-tant health risks are associated with eating many types of nonfood substances.
pica (pike-eh)The regular consumption ofnonfood substances such asclay or laundry starch.
Illustration 11.5The trend toward size acceptance. Acceptance of arealistic standard of body weight and shape—one thatcorresponds to health and physical fitness—and respect forpeople of all body sizes may be the most effective measuresthat can be taken to prevent anorexia nervosa, bulimianervosa, and binge-eating disorder.
Phot
o Di
sc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 11
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

The characteristics of pica are summarized in Table 11.6. Young children andpregnant women are most likely to engage in the practice; for unknown reasons, itrarely occurs in men.47 It most commonly takes the form of geophagia (clay or dirteating), pagophagia (ice eating), amylophagia (laundry starch and cornstarch eat-ing), or plumbism (lead eating). A potpourri of nonfood substances, listed in Table11.7, may be consumed.
Pica has a forceful calling card:
Pica permits the mind no rest until it is satisfied.48
It is not clear why pica exists, although several theories have been proposed.
Geophagia Some people very much like to eat certain types of clay or dirt. Those who do oftenreport that the clay or dirt tastes or smells good, quells a craving, or helps relievenausea or an upset stomach. The belief that certain types of clay provide relief from
geophagia (ge-oh-phag-ah)Clay or dirt eating.
pagophagia (pa-go-phag-ah)Ice eating.
amylophagia (am-e-low-phag-ah)Laundry starch or cornstarcheating.
plumbismLead (primarily from old paintflakes) eating.
TABLE 11.6
CHARACTERISTICS OF PICA.
A. Essential features: Regular ingestion of nonfood substances such as clay, paint chips,laundry starch, paste, plaster, dirt, or hair.
B. Other common features: Occurs primarily in young children and pregnant women in thesouthern United States.
TABLE 11.7
A PARTIAL LIST OF NONFOOD SUBSTANCES REPORTED TO BE CONSUMED BY INDIVIDUALSWITH PICA.
Animal droppings
Baking soda
Burnt matches
Cigarette butts
Clay
Cloth
Coal
Coffee grounds
Cornstarch
Crayons
Dirt
Foam rubber
Hair
Laundry starch
Leaves
Mothballs
Nylon stockings
Paint chips
Paper
Paste
Pebbles
Plaster
Sand
String
Wool
Phot
o Di
sc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 12
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

stomach upsets may have some validity: a component of some clays is used in nau-sea and diarrhea medicines. There is no evidence that geophagia is motivated by aneed for minerals found in clay or dirt, however.49
Although the reasons given for clay and dirt ingestion make the practice under-standable, the consequences to health outweigh the benefits. Clay and dirt con-sumption can block the intestinal tract and cause parasitic and bacterialinfections.50 The practice is also associated with iron-deficiency and sickle-cell ane-mia in some individuals.51
PagophagiaHave you ever known somebody who constantly crunches on ice? That person mayhave a 9-in-10 chance of being iron deficient. Regular ice eating, to the extent of oneor more trays of ice cubes a day, is closely associated with an iron-deficient state. Iceeating usually stops completely when the iron deficiency is treated.52
Ice eating may be common during pregnancy. In one study of women from low-income households in Texas, 54% of pregnant women reported eating largeamounts of ice regularly. Ice eaters had poorer iron status than other pregnantwomen who did not eat ice.53
AmylophagiaThe sweet taste and crunchy texture of flaked laundry starch are attractive to a smallnumber of women, especially during pregnancy. If the laundry starch preferred is notavailable, cornstarch may be used in its place. Laundry starch is made from unre-fined cornstarch. The taste for starch almost always disappears after pregnancy.54
Laundry starch and cornstarch have the same number of calories per gram asdo other carbohydrates (4 calories per gram). Consequently, starch eating providescalories and may reduce the intake of nutrient-dense foods. In addition, starch maycontain contaminants because it is not intended for consumption. Starch eaters’diets are generally inferior to the diets of pregnant women who don’t consumestarch, and their infants are more likely to be born in poor health.55
PlumbismThe consumption of lead-containing paint chips poses a major threat to the healthof children in the United States and many other countries (Illustration 11.6). Manyolder homes and buildings, especially those found in substandard housing areas, arecovered with lead-based paint and its dried-up flakes. Children may develop leadpoisoning if they eat the sweet-tasting paint flakes or inhale lead from contaminateddust and soil near the buildings. An estimated 1 million young children in the UnitedStates have elevated blood lead levels.56
High levels of exposure to lead can cause profound mental retardation anddeath in young children. Low levels of exposure can lead to hearing problems,growth retardation, reduced intelligence, and poor classroom performance. Chil-dren with lead poisoning are more likely to fail or drop out of school than childrennot exposed to lead in their environment.57
Eating disorders affect the health and well-being of over a million people in theUnited States. Although there are treatment strategies, such as counseling and theremoval of lead-based paints from old houses and apartments, the solution to eat-ing disorders lies in their prevention. With the exception of certain types of pica dis-cussed here, the most effective way to prevent eating disorders may be to adjust ourexpectations and cultural norms to reflect reality.
Illustration 11.6The regular consumption oflead-based paint chips fromold houses is a major causeof lead poisoning in youngchildren.
Phot
oEdi
tPh
oto
Disc
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 13
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

Nutrition UP CLOSEEating Attitudes Test
FOCAL POINT: Discover if your eating attitudes and behaviors are within a normal range.
Date Age Gender
Height Present weight How long at present weight?
Highest past weight How long ago?
Lowest past weight How long ago?
Answer the following questions using these responses:
A = always S = sometimes U = usually R = rarely O = often N = never
1. I am terrified of being overweight.
2. I avoid eating when I am hungry.
3. I find myself preoccupied with food.
4. I have gone on eating binges where I feel that I may not be able to stop.
5. I cut my food into very small pieces.
6. I am aware of the calorie content of the foods I eat.
7. I particularly avoid foods with a high-carbohydrate content.
8. I feel that others would prefer that I ate more.
9. I vomit after I have eaten.
10. I feel extremely guilty after eating.
11. I am preoccupied with a desire to be thinner.
12. I think about burning up calories when I exercise.
13. Other people think I am too thin.
14. I am preoccupied with the thought of having fat on my body.
15. I take longer than other people to eat my meals.
16. I avoid foods with sugar in them.
17. I eat diet foods.
18. I feel that food controls my life.
19. I display self-control around food.
20. I feel that others pressure me to eat.
21. I give too much time and thought to food.
22. I feel uncomfortable after eating sweets.
23. I engage in dieting behavior.
24. I like my stomach to be empty.
25. I enjoy trying new rich foods.
26. I have the impulse to vomit after meals.
Feedback (including scoring) can be found at the end of Unit 11.
Source: McSherry JA. Progress in the diagnosis of anorexia nervosa. Journal of the Royal Society of Health 1986;106:8–9. (Eating Attitudes Test developed by
Dr. Paul Garfinkel.)
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 14
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

Key Terms amylophagia, page 11-12
anorexia nervosa, page 11-3
binge eating, page 11-4
binge-eating disorder, page 11-8
bulimia nervosa, page 11-6
geophagia, page 11-12
pagophagia, page 11-12
pica, page 11-11
plumbism, page 11-12
purging, page 11-2
restrained eating, page 11-8
www linkswww.anad.orgThis site, from the National Association ofAnorexia Nervosa and Associated Disorders,provides free hot line counseling, anational network of support groups, andhealth care referrals.
www.nedic.caThe National Eating Disorder Info Center inToronto provides information and resourceson eating disorders and weight preoccupa-tion, and a telephone support line, infor-mation on support groups, and listings ofCanada-wide treatment resources.
www.nationaleatingdisorders.orgDeclare independence from a weight-obsessed world on this site. Click on “seek-
ing treatment” to learn about componentsof treatment of eating disorders and loca-tion of nearby care providers.
www.edreferral.comThis site includes basic information on eat-ing disorders along with specific informa-tion on treatment and recovery for men,pregnant women, and others with eatingdisorders.
www.naafa.orgFrom the National Association to AdvanceFat Acceptance, Inc., this site is dedicatedto improving the quality of life for fatpeople. It takes on policies and practicesrelated to size discrimination and promotessize acceptance by individuals and society.
www.mirror-mirror.org/eatdis.htmSubject categories allow you to select top-ics such as myths and realities of eatingdisorders, where to get help, recovery, andlinks to other Web sites.
www.hedc.orgHarvard’s Eating Disorders Center’s siteprovides facts about eating disorders,answers to FAQs (frequently asked ques-tions), advice on how to help a friend,child, or self with an eating disorder, andwhere to find help.
Notes1. Lake AJ et al. Effect of Western culture
on women’s attitudes to eating and per-ceptions of body shape. Int J Eat Disord2000;27:83–9.
2. American Psychiatric Association. Diag-nostic and statistical manual of mentaldisorders: DMS-IV, 4th ed., Text Revi-sion. Washington, DC: 2000.
3. Mazess RB, Barden HS, Ohlrich ES.Skeletal and body-composition effects ofanorexia nervosa. Am J Clin Nutr 1990;52:438–41.
4. Eating disorders. Facts about eating dis-orders and the search for solutions.National Institute of Mental Health,Bethesda, MD, 2001. www.nimh.nih.gov.
5. Grinspoon S et al. Prevalence and pre-dictive factors for regional osteopenia inwomen with anorexia nervosa. AnnIntern Med 2000;133:790–4.
6. Beals KA, Manore MM. Disorders ofthe female athlete triad among collegiateathletes. Int J Sports Nutr Exer Metab2002;12:281–93.
7. APA, DMS-IV.
8. Omizo SA, Oda EA. Anorexia nervosa:psychological considerations for nutri-
tion counseling. J Am Diet Assoc 1988;88:49–51.
9. Tamburrino MB, McGinnis RA.Anorexia nervosa: a review. PanminervaMed 2002;44:301–11.
10. Eating disorders (www. nimh.nih.gov);and Patel DR et al., Eating disorders,Indian J Pediatr 1998;65:487–94.
11. Eating disorders (www. nimh.nih.gov);and Feldman W, Feldman E, GoodmanJT, Culture versus biology: children’sattitudes toward thinness and fatness,Pediatrics 1988;81:190–4.
12. Grinspoon, Prevalence and predictivefactors for regional osteopenia.
13. Grinspoon, Prevalence and predictivefactors for regional osteopenia; andWorobey J, Schoenfeld D, Eating disor-dered behavior in dietetics students andstudents in other majors, J Am DietAssoc 1999;99:1100–2.
14. Grinspoon, Prevalence and predictivefactors for regional osteopenia.
15. APA, DMS-IV.
16. Robinson PH, Recognition and treat-ment of eating disorders in primary andsecondary care, Alimentary Pharmacol
& Thera 2000;14:367–77; and Patel etal., eating disorders.
17. Herzog DB et al., Recovery and relapsein anorexia and bulimia nervosa: a 7.5year follow-up study, J Am Acad Child& Adol Psychiatr 1999;38:829–37; Her-zog DB et al, Mortality in eating disor-ders: a descriptive study, Int J EatDisord 2000;28:20–6; and Tamburrinoand McGinnis, Anorexia nervosa: areview.
18. Treating eating disorders, HarvardWomen’s Health Watch 1996 May:4–5;and When eating goes awry: an updateon eating disorders, Food Insight 1997Jan/Feb:35.
19. Eating disorders (www. nimh.nih.gov).
20. Faris PL et al. Effect of decreasing affer-ent vagal activity with ondansetron onsymptoms of bulimia nervosa: a ran-domized, double-blind trial. Lancet2000;355:792–70.
21. APA, DMS-IV.
22. APA, DMS-IV.
23. Robinson, Recognition and treatment ofeating disorders.
24. APA, DMS-IV.
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 15
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE

25. APA, DMS-IV.
26. Edell D, Beware of personal trainerswith their looks, IDEA Health and Fit-ness Source. www.healthcentral.com/drdean/ DeanFullTextTopics.cfm?ID=41044&src=n2, accessed 9/2000; andWhen eating goes awry: an update oneating disorders.
27. APA, DMS-IV.
28 Faris et al., Effect of decreasing affer-ent vagal activity; and Tolstoi LG. Therole of pharmacotherapy in anorexianervosa and bulimia. J Am Diet Assoc1989;89:1640–6.
29. Herzog DB, Copeland PM. Bulimianervosa—psyche and satiety (editorial).N Engl J Med 1988;319:716–8.
30. Robinson, Recognition and treatmentof eating disorders; and Eating disor-ders III, Disease definition, epidemiol-ogy, and natural history, www.mentalhealth.com, accessed 12/2000.
31. Herzog et al., Recovery and relapse inanorexia and bulimia nervosa.
32. Hohlstein LA. Eating disorders pro-gram. American Dietetic Associationannual meeting, Boston, 1997 Oct 27.
33. APA, DMS-IV.
34. Eating disorders (www.nimh.nih.gov).
35. Fairburn CG et al. Distinctionsbetween binge eating disorder andbulimia nervosa. Arch Gen Psychiatry2000;57:659–65.
36. Branson R et al. Binge eating as amajor phenotype of melanocortin 4receptor gene mutations. N Engl J Med2003;348:1096–103.
37. Hohlstein, Eating disorders program;and Basdevant A et al. Prevalence ofbinge eating disorder in different popu-lations of French women. Int J Eat Dis-ord 1999;18:309–15.
38. Eating disorders III, disease definition;and Branson et al., Binge eating.
39. Hay PJ, Bacaltchuk J. Psychotherapyfor bulimia nervosa and bingeing(Cochrane Review). In: The CochraneLibrary, Issue 2, 2003.
40. Fairburn et al., Distinctions betweenbinge eating disorder and bulimia nervosa.
41. Eating Disorder Referral and Informa-tion Center, www.edreferral.com andHarvard’s Eating Disorders Center,www.hedc.org, accessed 6/03.
42. Cohen, LA, Nutrition and cancer pre-vention. Nutr Today 2001;36:78–9.
43. Lake et al., Effect of Western cultureon women’s attitudes.
44. Feldman et al., Culture vs. biology.
45. Branson et al., Binge eating as a majorphenotype; and Zuckerman DM, ColbyA, Ware NC, Layerson JS. The preva-lence of bulimia among college students.Am J Public Health 1986;76:1135–7.
46. Cooper M. Pica: a survey of the histor-ical literature as well as reports fromthe fields of veterinary medicine andanthropology. Springfield (IL): CharlesC. Thomas; 1957.
47. Edwards CH, McDonald S, MitchellJR, et al. Clay- and cornstarch-eatingwomen. J Am Diet Assoc 1959;35:810–15.
48. Craign FW. Observations on cachexiaAfricana or dirt-eating. Am J Med Sci1935;17:365.
49. Johns T, Duquette M. Detoxificationand mineral supplementation as func-tions of geophagy. Am J Clin Nutr1991;53: 448–56.
50. APA, DMS-IV.
51. Korman SH, Pica as a presenting symp-tom in childhood celiac disease, Am JClin Nutr 1990;51:139; and Hack-worth SR, Williams LL. Pica for foamrubber in patients with sickle-cell dis-ease. South Med J 2003; 96:81–3.
52. Reynolds RD, Binder HJ, Miller MB,Chang WWY, Horan S, Pagophagiaand iron deficiency anemia, Ann InternMed 1968;69:435–40; and ColtmanCA Jr., Pagophagia and iron lack,JAMA 1969;207:513–16.
53. Rainville AJ. Pica practices of pregnantwomen are associated with lowermaternal hemoglobin level at delivery. JAm Diet Assoc 1998;98:293–6.
54. Edwards et al., Clay- and cornstarch-eating women.
55. Edwards et al., Clay- and cornstarch-eating women.
56. Child health USA. Washington, DC:Maternal and Child Health Bureau,U.S. PHS;2000.
57. Child health USA.
Nutrition UP CLOSEEating Attitudes Test
Feedback for Unit 11Never = 3Rarely = 2
Sometimes = 1Always, usually, and often = 0
A total score under 20 points may indicate abnormal eating behavior. If you think you have an eating disor-der, it is best to find out for sure. Careful evaluation by a qualified health professional is necessary toexclude any possible underlying medical reasons for your symptoms. Contacting a physician, nurse practi-tioner, dietitian, or the student health center is an important first step. You may wish to show your EatingAttitudes Test to the health professional.
Brown_U11_1-16.qxd 5/21/04 10:43 AM Page 16
PROPE
RTY OF
LEARNIN
G
FOR R
EVIEW
ONLY –
NOT FOR SA
LE OR C
LASSROOM
USE
CENGAGE