Course Syllabus Orofacial Anatomy, Histology, & Embryology ...
Upload
lauren-blakeCategory
view
221download
0
Disk Embryology, Histology and Pathology
PTP 521Musculoskeletal Diseases and
Disorders

Objectives
1. review the embryology and histology of the intervertebral disc2. discuss common pathologies of the intervertebral disc3. differentiate between disc pathologies for signs and symptoms

Guide to PT Practice
• Pattern 4F• Impaired joint mobility, motor function,
muscle performance, range of motion and reflex integrity associated with spinal disorders.
• Disk: includes such diseases and disorders– Degenerative Disc disease– Disk herniation– Intervertebral disc disorder with myelopathy

Intervertebral Disk
• Embryological Development– Mesenchymal condensations forming around the
notochord also create the disk. – Notochord within the vertebral bodies but
becomes the nucleus pulposus in the intervertebral disks

Histology of Intervertebral Disk
• Fibrous annulus fibrosus– External layer of dense
connective tissue– Composed of
overlapping laminae of fibrocartilage
– Collagen bundles arranged in a cross fiber pattern

Nucleus pulposus
– Few rounded cells within a viscous medium
• Rich in hyaluronic acid
• Type II collagen fibrils

Purpose:
–acts as a cushion between two bones
–shock absorber

Disc pressures and changes that occur because of positions

Normal disc
• Young discs that are morphologically normal.

Common Definitions of Disk Dysfunction: North American Spine Society
1. Annular fissure: a disruption of the fibers of the annulus.
• Fluid within annulus may be evident on
MRI scan
-As long as the nucleus material is contained within the annulus the pt. will not have that much pain.

2. Disk Bulge: circumferential diffuse extension of the annulus extending 3 mm or more beyond the adjacent vertebral end plates.– associated with a
mild loss of disk height
– Not considered a herniationhttp://www.rsna.org/radlex/
committee/ASSRDiscNomenclature.pdf

Herniation:
3. Disk Protrusion: Focal, asymmetric condition in which a segment of the disk extends beyond the margin of the adjacent vertebrae into the spinal canal
Focal: less than 25% of the disc circumferenceBroad Based: 25-50%
When nucleus material hits the spinal canal there is a large inflammatory reaction that is very painful and can last for a while, the material does not breakdown quickly. A “hot disk” =recently ruppurted and very painful

Herniation
4. Disk extrusion: nucleus extends beyond the annulus and posterior longitudinal ligament into the epidural space. May migrate up or down the spinal canal

Herniation
5. Disk sequestration: a free fragment of disk that is detached from the remaining portion of the disk
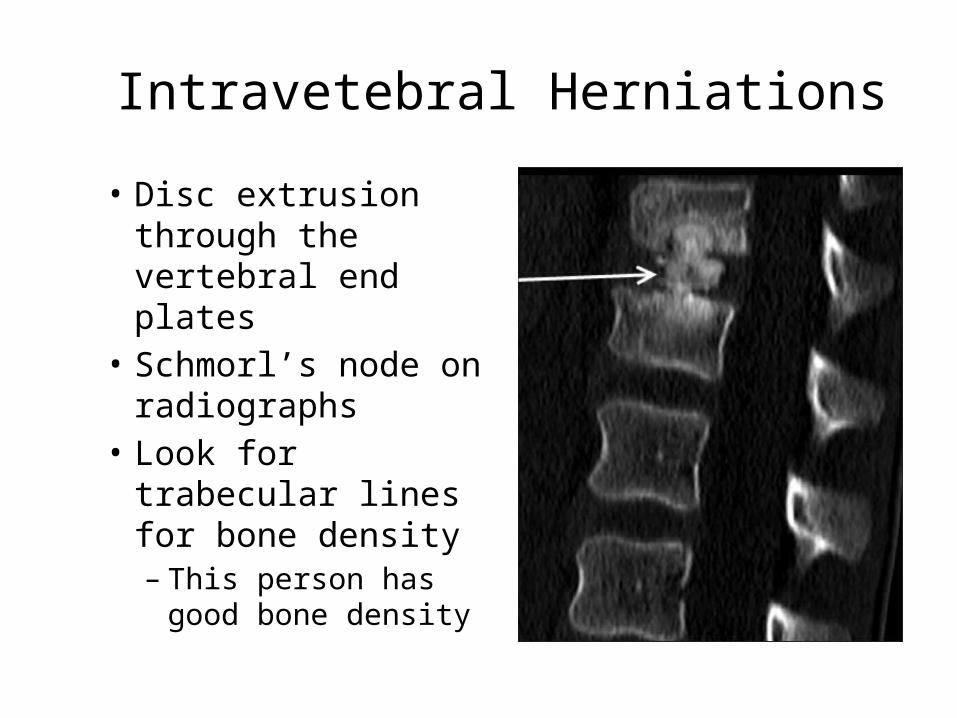
Intravetebral Herniations
• Disc extrusion through the vertebral end plates
• Schmorl’s node on radiographs
• Look for trabecular lines for bone density– This person has
good bone density

(a) Sagittal slab contact radiograph at the L3-4 level in a 74-year-old man shows a Schmorl node (black arrow) in the distal VEP of L3 and shows a vacuum phenomenon in the
intervertebral disk (white arrow).
Pfirrmann C W A , Resnick D Radiology 2001;219:368-374
©2001 by Radiological Society of North America

Disk Degeneration:Musculoskeletal Practice Pattern 4F
Pathology: similar process of normal joint degeneration as OA
• Process of disk degeneration is a cell-mediated response to progressive structural failure
• Water content in disk: – Young 89%-90% – Elderly drops to ~70%.
• Decrease in water content leads to a decrease in ability to weight bear
• Causes a breakdown of the annulus fibrosis

• Tears in the annulus are marginal at first, then radial tears and finally disk herniation.
• Disk height is less, joints are closer together, get an alteration in joint mechanics.
• Alteration leads to facet joint laxity and subluxation
• Osteophytes develop as the joints try to re-establish their normal position

Radiographs: Lateral view
• Narrowing of joint space between vertebrae
• Osteophyte and sclerosis of the joint margins
Clinical Symptoms:
• Acute onset: severe pain along a dermatomal pattern
• Dull or aching discomfort
• Occurs below the level of the severe pain
• Discomfort worsens with fatigue, tension, postural factors and neck extension
Signs:
• Muscle spasms or palpable firmness in the cervical muscles
• Increase in point tenderness of muscles
• May lose cervical ROM but usually not function
• Radicular signs and symptoms may occur

Common signsa. Tender to palpate, muscle spasms and trigger points common
b. Distraction of spine decreases pain
c. AROM and PROM will have pain with movement
d. No capsular pattern of limitation. (Limits in Rotatoin=side-bending, followed by extension)
e. Posture: abnormal flattening of the normal lordosis

Other:
• Lumbar Spine:– Most common areas are L4-5 and L5-S1
• Cervical Spine:– Most common areas are C5-6 and C 6-7

Diskitis
• Definition: disk space infection• Inflammatory lesion of the intervertebral disk• Occurs in adults but more commonly in children
younger than 10• Self Limiting• Vertebral Endplates or disk or both
• Etiology:– Bacterial or viral infection– Auto-immune disease
24
Clinical Manifestations• Symptoms:
– Low grade fever (less than 102 dg)
– Irritability– Back pain– Abdominal Pain
• Signs: Kids:– Refusal to walk– Pain with hip extension– Decrease mobility in the
back– Stiffness– Radiographs may show a
narrow disk space– MRI positive for
inflammation– CBC: elevated WBC
25

Treatment
• Radiological changes in adult:– Vertebral collapse– Kyphosis– Bony ankylosis
• Medication to treat inflammation– Pain relief– Anti-inflammatory
medication– Bed Rest
26