Disease Progression in Newly Diagnosed Type 2 Diabetes ...354275/s4250089_phd... · The aims of...
176
Disease Progression in Newly Diagnosed Type 2 Diabetes Mellitus Patients: A Statistical Analysis Using Clinical Practice Research Datalink (CPRD) Gijo Thomas MSc A thesis submitted for the degree of Doctor of Philosophy at The University of Queensland in 2015 School of Public Health
Transcript of Disease Progression in Newly Diagnosed Type 2 Diabetes ...354275/s4250089_phd... · The aims of...

Disease Progression in Newly Diagnosed Type 2 Diabetes Mellitus
Patients: A Statistical Analysis Using Clinical Practice Research
Datalink (CPRD)
Gijo Thomas
MSc
A thesis submitted for the degree of Doctor of Philosophy at
The University of Queensland in 2015
School of Public Health

i
Abstract
Type 2 Diabetes Mellitus is a serious disease with a long duration and considerable associated
morbidity. It affects a significant proportion of populations around the world irrespective of
economic status and its prevalence is increasing despite the efforts of clinicians, researchers, public
health professionals and policy makers. Most epidemiologic research has focused on exploring the
risk factors associated with this disease. However the present research aims to increase
understanding of the progression of the disease from initial diagnosis to death.
Aims
The aims of this thesis, from a clinical perspective, are to (a) evaluate the trajectory of blood
pressure as the disease progresses from initial diagnosis to death in a large longitudinal database of
newly diagnosed type 2 diabetes mellitus patients;, (b) within sub-cohorts based on body mass
index at time of diagnosis, explore HbA1c trajectories from diagnosis to death, particularly the
association with treatment intensity; (c) examine the 'obesity paradox'; and (d) investigate gender
specific effects of smoking on the risks of cardiovascular diseases. In addition the thesis explores
methodological issues arising with the use of large longitudinal datasets, in particular issues relating
to missing data and the effectiveness of multiple imputation as a technique to correct for this.
Methods and Results
The thesis has used a dataset of 84596 newly diagnosed type 2 diabetes mellitus patients diagnosed
between 1 January 1990 and 31 December 2005 and followed until April 2007 derived from the
United Kingdom Clinical Practice Research Datalink.
Generalised estimating equation models were used to explore the longitudinal trajectories. Cox
regression models were used to evaluate the gender specific effects of smoking and the obesity
paradox in relation to mortality risks. Separate models were created for patients with and without
cardiovascular diseases prior to diagnosis of type 2 diabetes mellitus. All models were adjusted for
the effects of other potential confounding factors.
Elevated HbA1c trajectories were associated with use of intensive medication irrespective of body
mass index at the time of diagnosis. Patients with normal body mass index at the time of diagnosis
had increased mortality risk compared to obese patients confirming the obesity paradox in type 2
diabetes mellitus. Those who died during the study had an elevated trajectory of blood pressure
compared to those who remained alive and this was statistically significant, but not clinically

ii
significant. Elevated mortality risks were observed in those with higher and lower levels of systolic
blood pressure compared to those with normal (130-139 mmHg). Considering diastolic blood
pressure of 80-84 mmHg as the reference level, diabetic patients with higher levels had significantly
increased mortality risk. Women who smoked had a higher risk of cardiovascular diseases and
mortality than men who smoked.
Conclusion
Clinical management, which aims to maintain good control over glycemic and blood pressure levels
in patients with newly diagnosed type 2 diabetes mellitus, is the most important approach to avoid
or to delay potential complications and improve survival. Special attention should be given to
women who smoke as they are exposed to increased risks of cardiovascular diseases and mortality.
Normal weight patients may also need to be managed differently due to the implications of the
obesity paradox. Individualised management of this disease by joint efforts of clinicians and
patients is the most important step in curbing this 21st century epidemic.

iii
Declaration by author
This thesis is composed of my original work, and contains no material previously published or
written by another person except where due reference has been made in the text. I have clearly
stated the contribution by others to jointly-authored works that I have included in my thesis.
I have clearly stated the contribution of others to my thesis as a whole, including statistical
assistance, survey design, data analysis, significant technical procedures, professional editorial
advice, and any other original research work used or reported in my thesis. The content of my thesis
is the result of work I have carried out since the commencement of my research higher degree
candidature and does not include a substantial part of work that has been submitted to qualify for
the award of any other degree or diploma in any university or other tertiary institution. I have
clearly stated which parts of my thesis, if any, have been submitted to qualify for another award.
I acknowledge that an electronic copy of my thesis must be lodged with the University Library and,
subject to the policy and procedures of The University of Queensland, the thesis will be made
available for research and study in accordance with the Copyright Act of 1968 unless a period of
embargo has been approved by the Dean of the Graduate School.
I acknowledge that copyright of all material contained in my thesis resides with the copyright
holder(s) of that material. Where appropriate I have obtained copyright permission from the
copyright holder to reproduce material in this thesis.
Gijo Thomas

iv
Publications during candidature
Publications incorporated in the thesis
Thomas, G., K. Khunti, V. Curcin, M. Molokhia, C. Millett, A. Majeed and S. Paul.
"Obesity Paradox in People Newly Diagnosed with Type 2 Diabetes with and without Prior
Cardiovascular Disease." Diabetes Obes Metab 16, no. 4 (2014): 317-25.
Incorporated as Chapter 6.
Conference abstracts
Paul S, Klein K, Thomas G, Khunti K. Blood Pressure Trajectories before Death in Patients
with Type 2 Diabetes. 72nd Annual Meeting of the American Diabetes Association,
Philadelphia, USA, 8-12 Jun, 2012
“Three Minute Thesis” competition at School of Population Health, University of
Queensland.
Research Higher Degree conference at UQ in 2011.
Princess Alexandra Hospital Health Symposium in 2013
Other publications during candidature
Paul S, Thomas G, Majeed A, Khunti K, Klein K. Women develop type 2 diabetes at higher
body mass indices than men. Diabetologia 2012; 55:1556-1557
Thomas G, Klein K, Paul S. Statistical challenges in analysing large longitudinal patient-
level data: The danger of misleading, clinical inferences with imputed data. Journal of the
Indian Society of Agricultural Statistics 2014; 68(2): 39-54.

v
Publications included in this thesis
Thomas, G., K. Khunti, V. Curcin, M. Molokhia, C. Millett, A. Majeed and S. Paul.
"Obesity Paradox in People Newly Diagnosed with Type 2 Diabetes with and without Prior
Cardiovascular Disease." Diabetes Obes Metab 16, no. 4 (2014): 317-25.
Incorporated as Chapter 6.
Contributor Statement of contribution
Gijo Thomas (Candidate) Developed the research questions (50%)
Conducted the literature review (50%)
Data management (60%)
Statistical analysis and interpretation (50%)
Prepared initial manuscript (45%)
Edited the paper (50%)
Kamlesh Khunti Prepared initial manuscript (10%)
Vasa Curcin Data management (40%)
Mariam Molokhia Edited the paper (5%)
Christopher Millett Edited the paper (5%)
Azeem Majeed Edited the paper (5%)
Sanjoy Paul Developed the research questions (50%)
Conducted the literature review (50%)

vi
Statistical analysis and interpretation (50%)
Prepared initial manuscript (45%)
Edited the paper (35%)

vii
Contributions by others to the thesis
Significant contributions by Professor Gail Williams to the analysis and writing of the thesis.
Statement of parts of the thesis submitted to qualify for the award of another
degree
None.

viii
Acknowledgements
This PhD program has been a major turning point in both my personal and professional life. I would
not have been able to complete this thesis without constant persuasion, support, care, patience of the
people that were with me throughout this entire journey. I would like to take this opportunity to
acknowledge those who stood by my side and whom I owe my deep gratitude.
First and foremost, I wish to express my deepest and sincere thanks to my supervisors – Professors
Gail Williams and Sanjoy Paul for their invaluable guidance and support throughout my PhD
journey. They have always generously shared wisdom during many stimulating and insightful
research discussions and paper revisions. I greatly appreciate the constant encouragement and
reassurance my supervisors provided me during my research process and living in Australia.
I have been very lucky to have undertaken my study within the School of Population Heath at the
University of Queensland, which has provided me an excellent environment in becoming a
professional researcher. I appreciate and acknowledge my Principal Supervisor Professor Gail
Williams and the School of Population Health for the additional financial assistance with travel to
conferences and meeting.
I am grateful to Associate Professor Deirdre McLaughlin who extended continuous support and
care throughout this wonderful journey. I would like to thank Ms Mary Roset, for her dedicated
administrative help during my PhD.
Finally, my most gratitude goes to my close family, for their unconditional faith and love upon me.
Without my parents encouragement and generosity, it would have never been possible to complete
this PhD. Special thanks to each and every member of my family, relatives and friends for their
consistent love, willingness to listen, expertise and help, and for their perspective and sound advice
and above all, God the Almighty, the giver of life and grace.

ix
Keywords
type 2 diabetes mellitus, cardiovascular diseases, mortality, trajectories, obesity paradox, smoking
Australian and New Zealand Standard Research Classifications (ANZSRC)
ANZSRC code: 010402, Biostatistics, 50%
ANZSRC code: 111706, Epidemiology, 50%
Fields of Research (FoR) Classification
FoR code: 1117, Public Health and Health Services, 50%
FoR code: 0104, Statistics, 50%

x
Table of Content
Abstract ................................................................................................................................................. i
Declaration by author .......................................................................................................................... iii
Publications during candidature .......................................................................................................... iv
Publications included in this thesis ...................................................................................................... v
Contributions by others to the thesis .................................................................................................. vii
Statement of parts of the thesis submitted to qualify for the award of another degree ...................... vii
Acknowledgements ........................................................................................................................... viii
Keywords ............................................................................................................................................ ix
Australian and New Zealand Standard Research Classifications (ANZSRC) .................................... ix
Fields of Research (FoR) Classification ............................................................................................. ix
Table of Content................................................................................................................................... x
List of Tables ..................................................................................................................................... xv
List of Figures .................................................................................................................................. xvii
List of Abbreviations ...................................................................................................................... xviii
Chapter 1. Introduction .................................................................................................................... 1
1.1: What is Diabetes? ..................................................................................................................... 2
1.2: Diagnosis of Diabetes Mellitus ................................................................................................. 5
1.3: The Global Burden of Type 2 Diabetes Mellitus ...................................................................... 6
1.4: Aims of the Study ..................................................................................................................... 7
Chapter 2. Literature Review ........................................................................................................... 9

xi
2.1: Current State of Research: Clinical......................................................................................... 10
2.1.1: Risks of cardiovascular disease and mortality in relation to glycaemic levels ................ 10
2.1.2: Benefits of hypertension management in T2DM patients ............................................... 12
2.1.3: BMI, glycaemic control and obesity paradox in T2DM .................................................. 13
2.1.4: Cardiovascular and mortality risks in T2DM patients – gender specific effects of
smoking ...................................................................................................................................... 14
2.2: Statistical Review.................................................................................................................... 15
2.2.1: A snapshot of statistical issues with longitudinal databases ............................................ 15
2.2.2: Missing data issues .......................................................................................................... 15
2.2.3: Multiple imputation of missing data under complex missing patterns ............................ 16
2.2.4: The measurement error problem ...................................................................................... 17
2.2.5: Survival analysis with measurement errors in risk factors (covariates) .......................... 17
2.2.6: The problem of irregular risk factor measurements ......................................................... 18
2.2.7: Survival analysis with irregularly observed time-dependent risk factors ........................ 18
2.2.8: Non-linear trajectories of risk factors and survival analysis ............................................ 18
Chapter 3. The Data ....................................................................................................................... 20
3.1: Source Data- The United Kingdom Clinical Practice Research Datalink (UK CPRD) ......... 21
3.2: Strengths of CPRD .................................................................................................................. 21
3.3: Limitations of CPRD .............................................................................................................. 22
3.4: Data Used for This Study ........................................................................................................ 23
3.5: Methods of Data Management and Data Cleaning ................................................................. 23
3.6: Description of the Demographic, Anthropometric and Clinical Study Parameters During the
Study .............................................................................................................................................. 26

xii
3.7: Prior Clinical Conditions and Family History ........................................................................ 30
3.8: Event Data ............................................................................................................................... 31
3.9: Medication Records During the Follow-Up ........................................................................... 32
3.10: Longitudinal Data ................................................................................................................. 34
Chapter 4. Gender Specific Effects of Smoking in T2DM Patients .............................................. 44
4.1: Background ............................................................................................................................. 45
4.1.1: Cardiovascular disease risks in T2DM patients ............................................................... 45
4.1.2: Gender differences in the association between cigarette smoking and coronary heart
disease and stroke....................................................................................................................... 46
4.1.3: Impact of smoking cessation on cardiovascular risk in individuals with and without
diabetes....................................................................................................................................... 47
4.2: Objectives ............................................................................................................................... 48
4.3: Methods................................................................................................................................... 48
4.3.1:Data ................................................................................................................................... 48
4.3.2: Statistical Methods ........................................................................................................... 49
4.4: Results ..................................................................................................................................... 50
4.4.1: Association between smoking and cardiovascular outcomes in individuals without a
prior history of CVD by gender ................................................................................................. 53
4.4.2: Association between smoking and cardiovascular outcomes in individuals with a prior
history of CVD ........................................................................................................................... 56
4.5: Discussion and Conclusion ..................................................................................................... 67
Chapter 5. Blood Pressure Trajectories Before Death ................................................................... 70
5.1: Background ............................................................................................................................. 71
5.2: Methods................................................................................................................................... 72

xiii
5.2.1: Data .................................................................................................................................. 72
5.2.2: Statistical Methods ........................................................................................................... 73
5.4: Results ..................................................................................................................................... 74
5.5: Discussion and Conclusions ................................................................................................... 83
Chapter 6. Obesity Paradox in Type 2 Diabetes Mellitus ............................................................. 85
6.1: Background ............................................................................................................................. 86
6.2: Research Design and Methods ................................................................................................ 87
6.2.1: Data .................................................................................................................................. 87
6.2.2: Statistical methods ........................................................................................................... 88
6.3: Results ..................................................................................................................................... 89
6.4: Discussion and Conclusions ................................................................................................. 100
Chapter 7. HbA1c Trajectories by BMI at Diagnosis and the Effect of Multiple Imputation .... 105
7.1: Background ........................................................................................................................... 106
7.2: Methods................................................................................................................................. 108
7.2.1: Data ................................................................................................................................ 108
7.2.2: Statistical Methods ......................................................................................................... 109
7.3.1: Trajectories of HbA1c by BMI categories ..................................................................... 110
7.3.2: Imputed data versus original data .................................................................................. 121
7.4: Discussion and Conclusion ................................................................................................... 123
Chapter 8. General Discussion and Conclusions ......................................................................... 126
8.1: Thesis Research Objectives .................................................................................................. 127
8.2: Limitatatios of This Thesis ................................................................................................... 130

xiv
8.3: Recommendations for Future Research ................................................................................ 131
8.4: Conclusions ........................................................................................................................... 132
References ........................................................................................................................................ 133
Appendix 1: Proportion of available and missing data at each time window ................................. 150
Appendix 2: STATA syntax for multiple imputation ...................................................................... 154

xv
List of Tables
Table 1.1: Type 2 Diabetes Mellitus and IGT of 20-79 year old adults 15
........................................... 6
Table 3.1: Yearly distribution of patients who were newly diagnosed with T2DM .......................... 24
Table 3.2: Descriptive characteristics of 84,596 newly diagnosed T2DM patients at the time of
diagnosis............................................................................................................................................. 26
Table 3.3: Description of Previous Medical History in the Cohort. .................................................. 31
Table 3.4: Description of current clinical events and all-cause mortality in patients with T2DM .... 32
Table 3.5: Record of current medication in the patients with T2DM ................................................ 33
Table 4.1: Baseline characteristics of the Clinical Practice Research Datalink (CPRD) by smoking
status in women and men (1990-2005). ............................................................................................. 51
Table 4.2: Adjusted gender specific hazard ratios (95% confidence intervals) associated with CVD
and all-cause mortality by smoking status in individuals without prior history of CVD from the
Clinical Practice Research Datalink (CPRD) (1990 – 2005) ............................................................. 54
Table 4.3: Adjusted gender specific hazard ratios (95% confidence intervals) associated with CVD
and all-cause mortality by smoking status in individuals with prior history of CVD from the Clinical
Practice Research Datalink (CPRD) (1990 – 2005) ........................................................................... 57
Table 4.4: Gender specific absolute risks and adjusted risk difference for smoking habits associated
with CVD and all-cause mortality in individuals without prior history of CVD per 1000 person
years from the Clinical Practice Research Datalink (CPRD) (1990 – 2005) ..................................... 63
Table 4.5: Gender specific absolute risks and adjusted risk difference for smoking habits associated
with CVD and all-cause mortality in individuals with prior history of CVD from the Clinical
Practice Research Datalink (CPRD) (1990 – 2005) ........................................................................... 65
Table 5.1: Descriptive statistics of the study cohorts, at the time of diagnosis. ................................ 74
Table 5.2: The effects of risk factors on longitudinal measures of blood pressure over the two year
period immediately before death or censoring ................................................................................... 76

xvi
Table 5.3: Odds ratios (95% CI) for mortality associated with different blood pressure categories,
compared to reference categories of 130-139 mmHg and 80-84 mmHg for systolic and diastolic
blood pressures. Estimates are separately provided for adjusted and univariate (unadjusted) models.
............................................................................................................................................................ 80
Table 6.1: Basic characteristics of study cohort by BMI Categories for patients without prior CVD
............................................................................................................................................................ 89
Table 6.2: Basic characteristics of study cohort by BMI Categories for patients with prior CVD ... 92
Table 6.3: Proportions and rates of events by BMI Categories for patients without prior CVD ....... 93
Table 6.4: Proportions and rates of events by BMI Categories for patients with prior CVD ............ 94
Table 6.5: Estimates of hazard ratios and their 95% confidence intervals for mortality and
cardiovascular events from multivariate stratified Cox regression models with obese category
(BMI≥30 kg/m2) as reference, for patients without prior CVD and by age categories. The BMI unit
is kg/m2. ............................................................................................................................................. 95
Table 6.6: Estimates of hazard ratios and their 95% confidence intervals for mortality and
cardiovascular events from multivariate stratified Cox regression models with obese category
(BMI≥30 kg/m2) as reference, for patients with prior CVD and by age categories. The BMI unit is
kg/m2. ................................................................................................................................................. 97
Table 7.1: Descriptive statistics of the T2DM study cohort ............................................................ 111
Table 7.2: Trajectories of HbA1c before death/censoring in all patients and according to treatment
strategies........................................................................................................................................... 116
Table 7.3: Mortality risk associated with longitudinal HbA1c measurements, by treatment
strategies, in different BMI categories. ............................................................................................ 120
Table 7.4: Proportions of missing data in HbA1c measured longitudinally in the 5 year period
before death or censoring, according to BMI categories of the patients at the time of their diagnosis
with T2DM. ...................................................................................................................................... 121
Table 7.5: Comparison of the HbA1c trajectory in imputed data and original data ........................ 122

xvii
List of Figures
Figure 1.1: Insulin action in normal and diabetic patients 2. ................................................................ 3
Figure 1.2: Major diabetes complications 2 ......................................................................................... 4
Figure 3.1: Density plots of anthropometric, clinical and biochemical parameters .......................... 28
Figure 3.2: Longitudinal distributions of the study parameters overall and by gender ..................... 35
Figure 4.1: The health consequences causally associated with smoking 74
....................................... 46
Figure 4.2: Adjusted hazard ratios and 95% confidence intervals for current smoking versus former
smoking by gender in diabetic patients without prior CVD. ............................................................. 59
Figure 5.1: Mean (95% CI) of longitudinal measures of systolic blood pressure during the two year
period prior to death or censoring ...................................................................................................... 78
Figure 5.2: Mean (95% CI) of longitudinal measures of diastolic blood pressure during the two year
period prior to death or censoring ...................................................................................................... 78
Figure 6.1: Density plots of BMI for different age groups for (A) cohort without prior CVD and (B)
cohort with prior CVD ....................................................................................................................... 91
Figure 6.2: Directed acyclic graph representing causal effects of BMI on mortality ........................ 99
Figure 6.3: Cumulative hazard plots for all-cause mortality across the BMI categories for all
patients and by age categories in cohort without prior CVD ........................................................... 102
Figure 7.1: Density plots of HbA1c (%) at time of diagnosis in normal, overweight and obese
patients. ............................................................................................................................................ 113
Figure 7.2: Trajectories of HbA1c (%) over the 5 year period immediately before death/censoring,
by treatment strategies. .................................................................................................................... 114
Figure 7.3: Trajectories of HbA1c by mortality status and baseline BMI ....................................... 117
Figure 8.1: Clinical management of T2DM 190
................................................................................ 131

xviii
List of Abbreviations
ACE Angiotensin-converting enzyme
ACM All-cause mortality
ADA American Diabetes Association
ARB Angiotensin-II receptor blocker
BF Body fat
BIC Bayesian Information Criteria
BMI Body mass index
BP Blood pressure
CABG Coronary artery bypass graft
CAD Coronary artery disease
CHD Coronary heart disease
CPM Cardio protective medications
CPRD Clinical Practice Research Datalink
CVD Cardiovascular disease
CVE Cardiovascular event
DBP Diastolic blood pressure
DM Diabetes mellitus
FBG Fasting blood glucose
FPG Fasting plasma glucose
GEE Generalised estimating equation
GP General practices

xix
GPRD General Practice Research Database
HbA1c Glycated haemoglobin
HDL High density lipoproteins
HF Heart failure
IFG Impaired fasting glucose
IGR Impaired glucose regulation
IGT Impaired glucose tolerance
IQR Inter quartile range
LDL Low density lipoproteins
LOCF Last observation carried forward
MAR Missing at random
MCAR Missing completely at random
MI Myocardial infarction
MNAR Missing not at random
MONW Metabolically obese but normal weight
NSAID Nonsteroidal anti-inflammatory drugs
OAD Oral anti-diabetes
OGTT Oral glucose tolerance test
ORC Ordinary regression calibration
PAD Peripheral arterial disease
SBP Systolic blood pressure
SD Standard deviation

xx
T1DM Type 1 diabetes
T2DM Type 2 diabetes
UK United Kingdom
UK CPRD United Kingdom Clinical Practice Research Datalink
WHO World Health Organization
2-h PG 2-Hour plasma glucose

xxi
This study is based in part on data from the UK Medicines and Healthcare products Regulatory
Agency. However, the interpretation and conclusions contained in this study are those of the
author/s alone.

1
Chapter 1. Introduction

2
1.1: What is Diabetes?
Diabetes mellitus (DM) is a major public health problem world-wide. It is a significant health care
challenge of the 21st century. The World Health Organization (WHO) has defined diabetes as a
metabolic endocrine disorder characterised by chronic hyperglycaemia, with disorders of
carbohydrate, fat and protein metabolism occurring as a result of deficiencies in insulin secretion,
insulin action, or both 1. As it is an endocrine disorder affecting glucose regulation, the condition is
characterised by high blood glucose levels. Insulin regulates blood glucose levels in the human
body by stimulating the uptake of glucose by muscles and organs. Under normal physiological
conditions, it is a hormone released from the pancreas when blood glucose levels are high.
However, in diabetic patients, inadequate secretion of insulin from the pancreas, or defective insulin
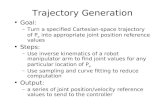
utilisation, leads to the development of high blood glucose levels. Figure 1.1 explains the action of
insulin in normal, as well as in diabetic, patients 2.
Diabetes is usually classified into three types:
Type 1 diabetes (T1DM)
Type 2 diabetes (T2DM)
Gestational diabetes
T1DM is also known as pancreatic endocrine insufficiency. It is an autoimmune condition. Patho-
physiologically, T1DM occurs due to the destruction of the β cells of the pancreas. Since
endogenous insulin production is affected, treatment of this type of diabetes requires daily
administration of insulin. The precise cause of T1DM is still unknown, and according to current
medical knowledge, it is not preventable and it may be as a result of some viral infections.
In T2DM (also known as nonpancreatic insufficiency), insulin is produced in normal or even high
amounts but the response of body cells to insulin is defective, leading to insulin resistance 3. Insulin
resistance is a physiological condition in which cells of the body fail to utilise secreted insulin
effectively.
The direct and indirect costs of diabetes management are increasing day by day. Direct costs
include those associated with medical care, drugs, insulin, self monitoring equipment, and other
materials. . Indirect costs arise from the reduction or loss of income or reduced quality of life.
Indirect costs may be higher than direct costs. Cost of diabetes management is about 14 billion
pounds per year 4.

3
Figure 1.1: Insulin action in normal and diabetic patients 2.
The leading pathophysiological cause of T2DM is the failure of pancreatic β cells. Failure in these
cells leads to inadequate secretion of insulin, and increased insulin resistance in the liver, fat tissues
and muscles. Physical inactivity and obesity lead to insulin resistance, increased production of
glucose by the liver, and decreased glucose uptake in skeletal muscles. In order to compensate, β
cells increase insulin secretion, but the progressive failure of β cells leads to hyperglycaemia and
finally Type 2 diabetes Mellitus 5. T2DM usually results from a progressive insulin secretory defect
on background of insulin resistance 6. Individuals with T2DM can live with an undiagnosed
condition for many years. As a result of high blood glucose levels, body organs are damaged during
this undiagnosed period. Many individuals are diagnosed with T2DM only when they develop
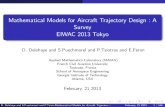
complications of diabetes. The major complications associated with diabetes are outlined in Figure
1.2.
As a chronic disease, complications of DM may affect the functioning of various organ systems,
and account for much of the morbidity and mortality associated with this disease. These chronic
complications can be broadly classified into two major categories: vascular and non-vascular.
Vascular complications are further divided according to whether they are microvascular
(retinopathy, neuropathy, and nephropathy) or macrovascular (coronary artery disease [CAD],
peripheral arterial disease [PAD], and cerebrovascular disease). Conditions such as gastroparesis,
infections, and skin changes constitute the non-vascular complications of diabetes.

4
Figure 1.2: Major diabetes complications 2

5
The increased risks of vascular and non-vascular diseases are directly associated with the duration
of hyperglycaemia. Chronic hyperglycaemia remains the major cause of microvascular
complications. Randomised controlled clinical trials, and epidemiologic studies have convincingly
demonstrated that a reduction in chronic hyperglycaemia in T2DM patients prevents or delays
microvascular complications such as retinopathy, neuropathy, and nephropathy 7-10
. Studies have
reported an increased risk of cardiovascular disease (CVD) in patients with DM and also reported a
two to four-fold increase in coronary artery disease events and mortality in patients with T2DM
8,11,12. A meta-analysis of intensive glycaemic control, and macrovascular complications in T2DM
patients also suggests that a strict lowering of glucose levels reduces the risk of major
cardiovascular events 12
. Factors such as dyslipidemia and hypertension also play important roles in
the development of the macrovascular complications of T2DM 8.
Gestational diabetes is a clinical condition observed in pregnant women as a result of insulin
resistance and subsequent high blood glucose levels. This condition develops as a result of insulin
action being blocked, probably by placental hormones. Normally, gestational diabetes resolves after
the birth of the baby. Still, women with gestational diabetes are highly likely to have the same
condition in subsequent pregnancies and are at higher risk of developing T2DM during their lives.
1.2: Diagnosis of Diabetes Mellitus
Usually, diagnosis of diabetes is made on the basis of levels of plasma glucose in the blood,
measured either with the fasting plasma glucose (FPG) test or the 2-hour plasma glucose (2-h PG)
level after a 75-g oral glucose tolerance test (OGTT) 13
. Recently, the American Diabetes
Association (ADA) suggested the use of glycated haemoglobin (HbA1c) as the preferred method
for confirming diabetes (using the criterion HbA1c ≥ 6.5%) 13
.
The onset of T2DM in most cases occurs as a latent phase of glucose intolerance or impaired
glucose regulation (IGR). This condition of impaired glucose regulation is known as pre-diabetes,
and is characterised by impaired fasting glycaemia and/or impaired glucose tolerance. This pre-
diabetes group is identified as being an intermediate group of individuals whose glucose levels,
although not meeting the criteria for diabetes, are nevertheless too high to be considered normal.
These individuals in this group have impaired fasting glucose (IFG) and impaired glucose tolerance
(IGT) if their FPG levels are between 100 mg/dl (5.6 mmol/l) and 125 mg/dl (6.9 mmol/l), and their
2-h OGTT values are between 140 mg/dl (7.8 mmol/l) and 199 mg/dl (11.0 mmol/l), respectively.
These categories are used by the ADA to identify individuals with a high risk of diabetes 13,14
.

6
HbA1c is the gold standard biomarker for measuring blood glucose levels and thus for identifying
diabetes status. HbA1c is a laboratory test that measures average blood sugar over a three month
period. The last three months contributes to the overall HbA1c value, thus justifying considering
any alteration in HbA1c within the last six weeks to be a result of dietary modification or treatment
in this period 14
. The HbA1c cut-off points for disease determination are: less than 5.7% (normal);
5.7% to 6.4% (pre-diabetes); 6.5% or higher (diabetes) 13
.
1.3: The Global Burden of Type 2 Diabetes Mellitus
T2DM is one of the most common non-communicable diseases and affects 382 million people
worldwide. In most high-income countries, T2DM is one of the major causes of death, ranking
fourth or fifth. A comparison of prevalence estimates for 2013 and 2035 is given in Table 1.1
Table 1.1: Type 2 Diabetes Mellitus and IGT of 20-79 year old adults 15
2013 2035
Total world population (billions) 7.2 8.7
Adult population (20-79 years, billions) 4.6 5.9
Type 2 Diabetes Mellitus
Global prevalence (%) 8.3 10.1
Number of people with diabetes (millions) 382 592
IGT
Global prevalence (%) 6.9 8.0
Number of people with IGT (millions) 316 471
The number of people with diabetes is increasing rapidly. The prevalence of diabetes across all age
groups was 2.4% in 2000 16
. However, according to a recent report by the International Diabetes
Federation, the global prevalence of diabetes in the year 2013 was 8.3% 2, representing a more than
threefold increase in estimated prevalence over the last decade. The number of diabetic patients is
currently more than 382 million worldwide, up from 171 million in 2000, and is expected to reach
592 million by 2035 2,16,17
– a 55% increase over two decades, if the trends continue 15
. The
estimated number of deaths associated with diabetes was almost 4 million in 2010. This figure, in
the adult diabetic population, is estimated to increase by 69%, for developing countries, and 20%,

7
for developed countries, by 2030 18,19
. These statistics demonstrate that diabetes is a global
epidemic.
1.4: Aims of the Study
As outlined earlier, T2DM is a chronic progressive condition that leads to various serious health
complications if not managed properly. The dramatic increase in the number of T2DM patients has
been attributed to lifestyle changes that have occurred over the past five decades. Globalisation has
resulted in remarkable changes to lifestyle, political systems, environments and human behaviour 20
.
It is of major clinical importance to implement lifestyle changes and regular health monitoring to
improve the quality of life of persons diagnosed with this disease. Disease progression and the
development of concomitant medical conditions must be addressed in an effective way.
Risk factors associated with T2DM, such as smoking, blood pressure and obesity, are controllable.
Imbalances in the glycaemic index of such patients will result in microvascular and microvascular
complications.
The United Kingdom Prospective Diabetes Study (UKPDS) showed that cigarette smoking was a
significant and independent risk factor for coronary heart disease, stroke and peripheral vascular
disease in people newly diagnosed with T2DM 21-23
. Various researchers have shown significant
differences between men and women in mortality and cardiovascular risks 24-27
– this need to be
considered in the context of increasing uptake of smoking by women in some populations.
Recent clinical trials and epidemiological studies have created concern and confusion over the
possible adverse effects of rigorous glycaemic control (measured by HbA1c) and over-intensive
blood pressure (BP) control on vascular events and all-cause mortality (ACM) in people with
T2DM 7,9,12,28-42
. High levels of comorbidity may diminish the benefits of achieving tight control,
owing to the complex interplay of multiple conditions and risk factors, including body weight, BP
and lipids 41
. Although some studies have explored the effect of baseline or ‘mean’ HbA1c and BP
on ACM 38,39,43,44
, the trajectory effects of HbA1c or BP, observed longitudinally over a long period
of time, on vascular events and ACM are as yet known.
As diabetes is a progressive disease, robust risk assessments for vascular and other diseases can
only be achieved by understanding the interchange of longitudinally measured risk factors and
medications with each other and over time. In addition, recent epidemiological studies have
reported conflicting results about the possible association between insulin treatment and an

8
increased risk of cancer in people with T2DM 45-53
. These reports indicate an urgent need to carry
out a detailed exploration of the long-term dynamics of risk factors and the effects of their possible
interactions on vascular and other adverse events in people with T2DM, under different treatment
regimens at a population level. The present study looks at the dynamics of HbA1c as a potential
indicator of glycaemic variations from a large longitudinal cohort of newly diagnosed T2DM
patients. While it is acknowledged that other risk factors such as BMI and dyslipidaemia also vary
over time in these patients, analyses have been limited to baseline measures.
The present study uses longitudinal primary-care based data, gathered from newly diagnosed T2DM
patients observed during the period of 1990 to 2005 – obtained from the United Kingdom Clinical
Practice Research Datalink (UK CPRD).
The study has both clinical and statistical aims and will address the following clinical questions
using innovative statistical methodologies to analyse complex longitudinal primary care data.
The aims are:
1. To evaluate the evidence that the association between smoking and the risk of
cardiovascular disease and mortality, among patients newly diagnosed with type 2 diabetes,
differs by sex in those with and without cardiovascular diseases before diagnosis.
2. To examine the trajectories of blood pressure in patients with T2DM, in relation to
mortality.
3. To examine the obesity paradox in people newly diagnosed with T2DM, with and without
CVD prior to diagnosis.
4. To examine HbA1c trajectories, by body mass index (BMI), and how these are associated
with mortality in patients with T2DM; as well as to investigate the effects of missing data,
using multiple imputation.

9
Chapter 2. Literature Review
This chapter is a comprehensive account of the current status of research in the field of diabetes
mellitus. Each chapter of this thesis contains separate focused literature reviews. In addition, one
chapter (6) has been published as an article with a literature review that overlaps with Section 2.1,
and substantial sections of Section 2.2 have contributed to a published article.

10
2.1: Current State of Research: Clinical
Diabetes is a serious chronic disease that is growing rapidly, affecting nearly 382 million people
worldwide, and requires continuous medical care once diagnosed 2,13,15,19,54
. Both T1DM and T2DM
are associated with a reduced lifespan, largely because of micro- and macrovascular complications
of the disease 33,34
. Continuous effort by patients to self-manage their treatment is very important in
preventing acute complications from arising 13
. These complications increase in frequency and
severity as the duration of the disease lengthens. The authors of a recent seven year prospective
study – evaluating premature mortality and comorbidities in young diabetic patients – concluded
that patients who became diabetic at a younger age had similar or poorer metabolic control than
those who were older at the time of their diagnosis 55
. This study also reported that a significant
difference in the proportion of younger (56.1%) and older (69.2%) T2DM patients who use oral
anti-diabetes medications 55
.
2.1.1: Risks of cardiovascular disease and mortality in relation to glycaemic levels
Epidemiological studies have consistently suggested a relationship between glycaemic control and
vascular events in patients with T2DM. However, results from intervention trials have been less
conclusive 9,12,28-32,40,43,56,57
. A meta-analysis by Zhang et al. reported that, in patients with T2DM,
increased risks of adverse cardiovascular outcomes are associated with chronic hyperglycaemia 58
.
The gold standard biomarker to measure glycaemic status is glycated haemoglobin (HbA1c) 59
. A
recent study evaluating the diagnostic value of HbA1c suggested that it is predictive of
cardiovascular disease risk in diabetic patients 60
. It is also possible for patients to have normal
levels of HbA1c at the time of their diagnosis, even if their diagnosis had been made on the basis of
high fasting blood glucose (FBG) or fasting plasma glucose (FPG) levels 61
. In the United Kingdom
Prospective Diabetes Study (UKPDS), newly diagnosed T2DM patients who had not previously
suffered from CVD were found to have reduced HbA1c levels (from 8% to 7%), but this was not
associated with a reduction in subsequent cardiovascular events 7,31,33
. The 16% risk reduction for
myocardial infarction (MI), reported in the UKPDS, was not statistically significant. Three recent
landmark studies, the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial28
, the
ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release
Controlled Evaluation) trial29
, and the VADT (Veteran Affairs Diabetes Trial) study30
, sought to
determine the effect of lowering glucose to near-normal levels on cardiovascular risk in patients
with established T2DM. The compelling message from all these studies is that maintaining

11
glycaemic levels at near-normal values for a median of 3.5 to 5.6 years does not reduce
cardiovascular events within that time frame, with the exception of the progression of albuminuria,
nephropathy and retinopathy. However, an analysis of 10-year post-trial follow-up results from the
UKPDS provides a more optimistic view of the potential benefits of glycaemic control 31,32
. The
relative risk reduction for MI and ACM were significant in participants who initially received
intensive glucose lowering treatment compared with those in the conventional treatment arm.
Consequently the outcome of the debate on the importance of glycaemic control in preventing
macrovascular complications remains undetermined.
The trials referred to above used multifactorial treatment strategies. Therefore, the potential risk
reduction specifically attributable to glucose lowering is difficult to isolate. Doing so would require
a very large number of patients and a much longer follow-up time. Different pharmacological
agents and comorbid conditions have varying effects on vascular outcomes, irrespective of the
extent to which they contribute to glycaemic control. The UKPDS reported a significant interaction
effect between HbA1c and SBP, with 21% and 11% risk reductions in ‘any diabetes related end
point’, for 1% and 10 mmHg reductions in HbA1c and SBP, respectively 38
. A recent study
conducted using the General Practice Research Database (GPRD) reported 52% and 79% higher
risks of ACM associated with lower and higher levels of HbA1c, compared to the HbA1c decile
with the lowest hazard (median HbA1c 7.5%) 39
. However, rather than considering the entire
trajectories for glycaemic measures, researchers considered the updated mean of HbA1c in their
analyses. Gebregziabher et al. (2010)40
explored the time-varying effect of HbA1c trajectories on
ACM, using a large cohort of T2DM patients from the US Veterans Affairs registry database. The
baseline HbA1c was associated with a two-fold increased risk of mortality. However, trajectory
analysis of HbA1c with 8821 patients and an average of 4.5 years follow-up time showed a non-
significant hazard estimate of 7.3 (95% CI: 0.9 – 57.1). The wide confidence interval of this risk
estimate in a large data set with an overall mortality rate of 15.3% is difficult to understand.
It is clinically important to understand the ‘residual’ beneficial effect of HbA1c management, after
eliminating the joint effects of other factors. Addressing uncertainty related to the potential benefits
of glycaemic control requires a closer look at the trajectories of different related risk factors over
time.
A review by Ismail et al. suggests that the glycaemic targets in T2DM patients should be
individualised – according to age, present status and duration of the disease, micro- and
macrovascular diseases, and lifestyle – for improved management of the disease and control of
glycaemic levels 62
.

12
This implies the need for a longitudinal analysis (at the population level, using a large primary care
dataset) of the long-term trajectories of HbA1c, as well as other, related risk factors, and the effects
these trajectories have on disease outcomes, using appropriate statistical techniques to ensure
robustness of interpretation.
2.1.2: Benefits of hypertension management in T2DM patients
Most clinical trials mentioned above also analysed the potential benefit of hypertension
management in patients with T2DM, with specifically designed treatment arms. Hypertensive
T2DM patients are at an increased risk of morbidity and mortality from cardiovascular events. The
estimated prevalence of hypertension in adults with diabetes is 20–60%, which is 1.5–3 times
higher than that in age-matched individuals without diabetes 54
. Another important risk factor is
body weight, which has been directly associated with hypertension and poor glycaemic control. A
10 kg weight gain during middle age (40-49 years) increases the risk of developing diabetes by a
factor of 21 63
. T2DM is frequently accompanied by an advanced age and obesity, both of which
increase the risk of hypertension, making it difficult to ascribe elevated BP solely to diabetes 44
. In
the presence of uncontrolled hypertension, there is a consistent positive association between
elevated systolic blood pressure and increased risk of micro- and macrovascular diseases 38,39
.
However, the BP arms of the ADVANCE, ACCORD and VADT studies have generated
contradictory messages. The BP arm of the ADVANCE study suggests that the lowering of BP is
additive with intensive glucose control in reducing the risk of cardiovascular mortality and all-cause
mortality in people with T2DM 35
. In that study, intensive BP lowering reduced the risk of
cardiovascular death by 18%, but did not significantly reduce composite macrovascular outcomes.
The ACCORD BP study36
, targeting a systolic blood pressure (SBP) of less than 120 mmHg
compared with less than 140 mmHg, reported no significant benefit of intensive BP lowering
treatment on the rate of a composite outcome of fatal and nonfatal major cardiovascular events. The
VADT findings suggest a significantly higher risk of cardiovascular events in T2DM patients with a
SBP of 140 mmHg or higher and a DBP of 70 mmHg or lower, compared with normal BP levels 37
.
It is important to note here that the ADVANCE trial had no specified BP goals, and the mean SBP
in the intensive therapy group (135 mmHg), intensive and standard therapies resulted in similar
levels of systolic blood pressure (127 mmHg). On the other hand, the UKPDS suggested an additive
effect of glycaemia and BP, with significant benefits achieved by treating both risk factors
simultaneously 38
. It is possible that five years is not long enough to observe significant cardiac
benefits from the normalisation of BP in patients with T2DM, especially when other effective

13
treatments, including statins and aspirin, are frequently used 36
. This necessitates much longer
longitudinal data at the population level to better understand these clinical issues. A study by
Cederholm et al. reported a lower risk of CVD in T2DM patients within a blood pressure range of
about 130-135/75-79 mmHg 64
.
Given the inconsistent conclusions of the above mentioned clinical trials, long-term BP trajectories,
at a population level, and their relationship to vascular events and ACM should be explored, so that
management of BP in T2DM patients can be improved.
2.1.3: BMI, glycaemic control and obesity paradox in T2DM
It has been shown that obesity plays a major role in the pathophysiology of T2DM and its
macrovascular complications 65-67
. It has also been suggested that an adverse metabolic profile in
patients with normal weight increases the risk of subsequent development of T2DM and other CVD
65,66,68. A recent study explored the relationship between obesity, glycaemic control and
cardiovascular risk factors in T2DM patients who were not receiving insulin treatment and
concluded that cardiovascular risk factors become more important as patients became more obese
65. This study also reported that younger age and more recent onset of the disease were associated
with higher BMIs, suggesting that the development of an obese condition at an early age could be a
significant factor underlying the increase in T2DM incidence 65
. Further, studies have reported that
individuals of normal weight have a substantial risk of developing T2DM and CVD 66,68
. These
risks are attributed to their confrontational metabolic status, which includes insulin resistance and
other related diseases 65
. This suggests that it is not necessary to be overweight or obese for the
development and progression of T2DM. A study by Andersson et al. reported that in T2DM patients
who were overweight or obese, high HbA1c levels at diagnosis were associated with increased
cardiovascular and mortality risks 69
.
Although the majority of T2DM patients may be obese70
, recent studies have raised the issue of an
obesity paradox 71,72
. The concept of the obesity paradox runs counter to common beliefs about
T2DM. A study by Carnethon et al. concluded that patients who were of a normal weight at the time
of their diagnosis with T2DM had higher mortality rates than those who were overweight and obese
72. However, potential interaction effects between cardiovascular and glycaemic risk factors were
not addressed in their analysis. A recent study by Ganz et al. reported a strong and independent
association between BMI and T2DM diagnosis, with the effect size increasing together with BMI,
suggesting that the majority of T2DM patients may be obese at the time of their diagnosis 73
.

14
2.1.4: Cardiovascular and mortality risks in T2DM patients – gender specific effects of
smoking
Cigarette smoking is an important chronic disease risk factor in both diabetic and non-diabetic
populations. Globally, it is recognised as one of the leading causes of premature mortality 15,74
. In
the United States, 22% of adults are smokers and cigarette smoking remains a major cause of
premature death (20 million), according to the latest reports by the National Centre for Chronic
Disease Prevention and Health Promotion 74
. T2DM patients who are smokers have higher blood
glucose levels and less effective glycaemic control compared to their non-smoking diabetic
counterparts 75
.
In T2DM patients, cigarette smoking is directly associated with risks of micro- and macrovascular
diseases and renal complications, which may result in elevated mortality risks. Various research
studies have shown that cigarette smoking is an important and self-regulating risk factor for
coronary heart disease, stroke and peripheral vascular diseases in T2DM patients 21-23
. A recent
systematic review and meta-analysis by Quin et al. in diabetic patients reported that cigarette
smoking is associated with a 48% increased mortality risk, 54% increased risk of coronary heart
disease, 44% increased risk of stroke, and 52% increased risk of myocardial infarction 76
.
Several studies have reported similar risks for cardiovascular mortality in T2DM patients without
coronary heart disease (CHD) and non-diabetic patients with CHD 77,78
. A meta-analysis by Kanaya
et al. reported that men with diabetes suffered from more CHD deaths than women with diabetes 27
.
One of the major causes of death in diabetic patients is stroke. According to a recent study in the
US, the predicted number of stroke-related deaths in women, by the year 2050, will be higher, by
68000, than that of men, because women have more events of stroke and a lower recovery rate 79,80
.

15
2.2: Statistical Review
2.2.1: A snapshot of statistical issues with longitudinal databases
Longitudinal studies prospectively investigate the same group of individuals over a period of time
and are of great importance in clinical research. These longitudinal databases serve as knowledge
repositories, containing a large amount of information on changing health outcomes, concomitant
risk factors and treatment. Appropriate analyses of these databases potentially facilitates an
understanding of disease progression and identification of factors which might be useful in slowing
or reversing this. In particular, primary care databases have special advantages, as they capture
population level information at the first point of contact patients have for many health problems,
and, particularly for chronic diseases, the ongoing features of disease and treatment. Interestingly,
such databases will capture changes in various measures of lifestyle, and their impact on health
outcomes, including complications. This allows the identification of the effects of lifestyle on
disease occurrence, as well as the effects of lifestyle changes made at the individual level on health.
In addition, effects of changes in health policy, such as those aimed at reducing tobacco use, can be
monitored.
There are also disadvantages that must be considered in evaluating the validity of findings from
studies that use primary care databases. These relate to missing or incomplete data issues or loss-to-
follow-up, quality of data management, measurement errors (particularly in risk factors or clinical
data), and the irregular timing of measurements, which may occur according to disease
exacerbations rather than routinely. Statistical analyses must also have sufficient flexibility to
explore non-linear trajectories of risk factors and health outcomes.
2.2.2: Missing data issues
Most primary care databases, including the CPRD (former GPRD), have non-trivial proportions of
missing data for key variables 51,81
. Various approaches have been used to deal with missing data in
large clinical databases. These include complete case analysis (including only patients with
complete records), exclusion of variables with incomplete data from the analysis, inclusion all
available data using maximum likelihood based approaches or imputation based approaches 51,82,83
.
However, these approaches for dealing with missing data may lead to selection bias, substantial
reduction in the power of the study, and misleading conclusions 52,83,84
. Whichever technique is

16
used, there is a possibility that false associations may be shown, or associations which exist may
fail to be identified or be incorrectly estimated. It is necessary to understand the mechanisms behind
missing data in order to evaluate the potential for invalid conclusions.
2.2.3: Multiple imputation of missing data under complex missing patterns
Multiple imputation is one of the most advanced and powerful techniques for handling missing
data84
, and is increasingly used to adjust for missing data in the analyses of longitudinal data 82,84-90
.
Despite the increasing use of multiple imputation, its implementation may be complex and very few
publications provide sufficient detail on the methods used, the underlying assumptions or the extent
to which the results can be regarded as more reliable than those generated by other approaches 87,90
.
The main obstacle for the appropriate implementation of multiple imputation in longitudinal data is
a lack of understanding of the mechanisms giving rise to missing data. Various categories of
missingness have been described 83,91
. Data may be missing at random (MAR) or missing not at
random (MNAR). MAR is said to occur if the probability distribution of the observed missing
pattern, given the observed data, does not depend on the values of the unobserved data. MNAR
occurs if missingness depends not only on the observed data, but also on the unobserved values. In
health care data, MNAR could arise because of the health states of the patients and residential
changes. Mental health data is particularly prone to MNAR – people who have been diagnosed as
depressed are less likely than others to report their mental status. Clearly the mean mental status
score for the available data will provide a biased estimate of the mean compared to that obtained
with complete data. One study has suggested that blood pressure data was not recorded randomly in
the GPRD, as subjects with more blood pressure readings tended to have higher recorded values 92
.
Analysis of MNAR data is a considerable statistical challenge that requires modelling of the
missingness 93
. Although multiple imputation of missing data which is MNAR can theoretically be
dealt with, this is rarely discussed in the literature and available multiple imputation software
almost uniformly assumes MAR 87,90
. Complications of MNAR adjustment occur because of the
need to extend the MAR imputation model to include an informative model for dropouts. Carpenter
et al. (2007) first addressed this issue with simple sensitivity analyses 94
. They proposed first
imputing the missing data under MAR and obtaining parameter estimates for each imputed data set
in the usual way. Then the overall MNAR parameter estimate was a weighted average of these
parameter estimates, where the weights depend on the assumed degree of departure from MAR.
Daniels et al. (2008) discussed strategies for Bayesian modelling and sensitivity analysis in order to
draw inferences from incomplete data under MNAR 95
. In some settings (based on simulated data),

17
this approach gave results that more closely agreed with those obtained from joint modelling as the
number of imputations increased. However, these studies did not address the core issue of
developing a theoretical framework and a standardised protocol for application.
2.2.4: The measurement error problem
Longitudinal data, especially clinical databases, have an inherent problem caused by erroneous
measurements. Random measurement errors in regression covariates bias the estimates of
regression coefficients towards the null, and can result in a true association being found to be
statistically non-significant 96
. Although there are many methods for measurement error correction,
these methods remain rarely used in analysing longitudinal data, despite the ubiquity of
measurement error. Most clinical and epidemiological studies that use generalised linear models to
analyse the longitudinal healthcare data fail to address this critical issue.
2.2.5: Survival analysis with measurement errors in risk factors (covariates)
Clinical and epidemiological studies with longitudinal data seek to explore the effects of disease
risk factors on disease outcome(s). Application of the Cox regression model in these studies is very
common. However, while fitting the Cox model with time-independent or time-varying covariates,
adjustments for measurement errors in risk factors is rare.
Failure time models subject to covariate measurement errors or missing covariates have aroused
much interest over the past two decades. Several studies have demonstrated the impact of
measurement errors by deriving the induced hazard function in the presence of covariate
measurement error and have advocated several methods for drawing inferences 97-99
. The most
popular approach in this context is the ordinary regression calibration (ORC) approach. Although
ORC is approximately valid and efficient for measurement error correction of relative risk estimates
from the Cox model with time-independent risk factors when the disease is rare, it is not adaptable
for use with time-varying risk factors. As researchers are more interested in exploring the risks
associated with time-varying risk factors, it is very important to develop an appropriate
methodological framework for survival analysis using time-varying covariates with measurement
errors. There is very limited methodological literature on this topic 99
. In addition, clinical and
behavioural risk factor variables may be either continuous or semi-continuous. Correction for
measurement errors in semi-continuous data is a non-trivial statistical problem. The need to explore
time-varying effects of various risk factors on disease outcomes requires development of

18
appropriate joint models for survival time and longitudinally observed risk factors with
measurement errors. Validation and sensitivity analyses of models with continuous and semi-
continuous risk factor data are needed.
2.2.6: The problem of irregular risk factor measurements
In most longitudinal health care data, clinical and biochemical measurements are not available in
equally-spaced periods of time. Data are usually recorded when a particular patient has a clinical or
laboratory assessment performed for specific reasons. This creates a potential problem for aligning
data according to a pre-specified timeline common to all patients to facilitate appropriate analyses.
For example, the HbA1c measurement in diabetes patients reflects the accumulation of blood
glucose over a period of three months. However, HbA1c data for individual patients are unlikely to
be available exactly every three months, with the result that it is difficult to create specific time-
aligned data to explore the trajectory of this crucial risk factor over time and to assess the
consequent outcomes (such as CVD or mortality).
2.2.7: Survival analysis with irregularly observed time-dependent risk factors
Most methods described in the literature for joint modelling of irregularly measured longitudinal
and event time data are quite complex 10,44
. It is very important to account for the differences in
observation frequency between individual patients, for example by including time elapsed since the
last observation. Interaction effects of this time elapsed with time-varying risk factors will
potentially occur, affecting the interpretation of risk estimates. Unfortunately, clinical and
epidemiological studies dealing with this aspect are rare.
2.2.8: Non-linear trajectories of risk factors and survival analysis
The trajectories of clinical and biochemical risk factors are often non-linear 100
. For example,
several epidemiological studies and long-term outcome trials in diabetes have revealed clear non-
linearity in the long-term growth pattern of HbA1c 31
. Joint modelling of survival time and
longitudinal risk factor data generally assumes a proportional hazards model for the survival times
and a linear mixed-effects model for the longitudinal data. The literature is rich in methods
developed under this framework, which includes both parametric and semi-parametric methods 101
.
However, the linear random effects model may not be suitable for the non-linear covariate process,
and literature is scarce in this field 100
. Tapsoba et al. (2009) has proposed a polynomial regression

19
model to model non-linearity in covariates, while developing a joint model for time-to-event and
longitudinal data 102
. However, this approach lacks generalisability especially when dealing with U-
shaped non-linearity.
In summary longitudinal studies suffer from problems of missing data, irregular and erroneous
measurements. The available standard statistical tools are not suitable for addressing these complex
issues while simultaneously exploring their trajectories of key risk factors and their association with
events or outcomes. Current longitudinal studies often ignore these issues, with the potential for
producing misleading results and the subsequent implementation of practices which lack an
appropriate evidence based. Future research should concentrate on how current methodologies can
be generalised to improve the accuracy and reliability of the analysis of outcomes in longitudinal
studies.

20
Chapter 3. The Data

21
3.1: Source Data- The United Kingdom Clinical Practice Research Datalink (UK
CPRD)
The recent widespread implementation of electronic recording and nation-wide linkage of patient
data from primary care practices in developed countries has provided an enormous opportunity for
clinical, epidemiological and health policy research. The Clinical Practice Research Datalink
(CPRD) is the world's largest computerised database of anonymised longitudinal medical records
from primary care, linked with other healthcare data, in the United Kingdom (UK). At present, data
are being collected on about 10 million active patients, from more than 700 primary care practices
throughout the UK 103
. The database is used internationally for research by the pharmaceutical
industry, clinical research organisations, regulators, government departments and leading academic
institutions. Participating practices are expected to follow a systematic protocol for collecting
demographic and clinical data. Anonymised data are regularly submitted to CPRD. The accuracy
and reliability of CPRD data have been accepted internationally, as a result of extensive research in
the fields of health sciences and epidemiology 103,104
.
Complete medical histories of patients are available from as early as 1987 – beginning as the
General Practice Research Database (GPRD) in 1987, and becoming the CPRD in recent years –
and entries continue to be updated from routine clinical consultations. Data obtained from patients
at the time of their consultation with GPs include demographic data (age, sex and registration
information); medical data, including diagnoses (from routine GP visits, consultations,
hospitalisations, emergency care), prescription data with date, formulation, strength, quantity,
indications for all new prescriptions, events leading to the withdrawal of a drug or treatment; and
data concerning preventative treatments (including vaccinations and prescription contraceptives).
Other information collected includes smoking, height, weight, pregnancy, birth, death, date of
entering the practice, date of leaving the practice, and laboratory results. Occurrences of important
medical events prior to a patient registering with a CPRD centre are also recorded.
Diagnosis of a disease is entered into the CPRD using Read Codes, which are alphanumeric codes
derived from a thesaurus of clinical terms that categorises and defines illnesses 103
.
3.2: Strengths of CPRD
One of the major advantages of using this database for research purposes is that, it narrows the
research to a clearly defined population that will allow a researcher to select comparative subgroups

22
of patients from the same source population. In general, because the database is broadly
representative of the UK population, selecting patient and control groups from the same cohort will
result in selection biases being minimised. This enhances the validity of epidemiologic studies and
thus increases the ability of findings to be generalised 103
. In addition, investigators can study
families by, for example, linking health events in mothers and children 103
.
The size of the longitudinal databases, as well as the length of time they have been in use, allow the
investigation of rare diseases that have incidence rates of less than 1 per 10,000 person-years, with
sufficient statistical power. Good agreement and accuracy have been observed between prescription
data captured from specialist information and the medical record 103
.
The CPRD allows the researcher to access original medical records, providing more complete
information on the patient’s health history, thus enabling researchers to verify information captured
on death, and advice from specialists 103
.
3.3: Limitations of CPRD
One of the major limitations of the CPRD is incompleteness of data. Information in the CPRD is
taken from the medical record obtained by the GP, and it is expected that data submitted by the GP
will be complete. However, it is possible that all information from specialist consultations and
hospital admissions may not be entered into the CPRD. Therefore, relevant information required for
a specific study may be lacking. Some clinics may not maintain complete data on patients, or make
sufficient effort to enter data as required. Missing data could include communications from
specialists, discharge summaries from hospitals, and test results from pathology laboratories. Such
data may be received in hard copy, and extra time is needed for manual entry. Some GP centres
may only enter information that affects patient care. For example, only abnormal results may be
entered into the CPRD 103
.
Non-significant medical events are more likely to be missed than medically significant diagnoses or
events. Data on medication given directly to the patient (i.e. not requiring a prescription to be
written) and hospital treatments are not readily available. The movement of patients from one GP to
another GP is not captured in this database 103
.

23
3.4: Data Used for This Study
Inclusion Criteria: data on 84596 newly diagnosed type 2 diabetes mellitus patients, aged 18-99
years, who were diagnosed with T2DM between 1 January 1990 to 31 December 2005, and who
were followed-up on until April 2007.
Source variables: data includes demographic, anthropometric, clinical and laboratory variables with
relevant dates, previous medical history, current medication with codes and prescription dates, and
disease events (including death), together with their dates.
Demographic and anthropometric measurements include the age at which the patient was diagnosed
with diabetes, sex, smoking and alcohol consumption status, deprivation score (an indication of
socio-economic status), weight and BMI.
Clinical data includes SBP and diastolic blood pressure (DBP) (mmHg). Biochemical
measurements include HbA1C (%), fructose, albumin, serum creatinine, triglycerides (mmol/L),
low density lipoproteins (LDL), high density lipoproteins (HDL), and total cholesterol.
Occurrences of medical conditions such as myocardial infarction (MI), stroke, heart failure (HF),
coronary heart disease (CHD), peripheral artery disease (PAD), angina, angioplasty, coronary artery
bypass graft (CABG), neuropathy, retinopathy and renal complications were also available, with
dates. Medical history included amputations, arthrosclerosis, coma, seizures, multiple sclerosis,
fractures, revascularizations, and surgeries prior to the diagnosis of diabetes.
Family histories of cardiovascular events such as MI and hypercholesterolemia were also available,
though family histories of diabetes were not. Medication data included prescription of metformin,
sulphonylurea, rosiglitazone, pioglitazone, meglitazone, insulin, statins, beta blockers, angiotensin-
converting enzyme/angiotensin-II receptor blocker (ACE/ARB), aspirin, and Nonsteroidal anti-
inflammatory drugs (NSAIDs).
3.5: Methods of Data Management and Data Cleaning
A total of 84596 patient records were obtained by initially screening 84633 patients. Thirty-seven
patients were excluded as a result of date of death being reported as prior to the date of diagnosis of
diabetes. The numbers (%) of newly diagnosed T2DM patients in each year are listed below (Table
3.1).

24
Table 3.1: Yearly distribution of patients who were newly diagnosed with T2DM
Year N (%)
1990 1187 (1.4)
1991 1570 (1.9)
1992 1708 (2.0)
1993 1917 (2.3)
1994 2031 (2.4)
1995 2371 (2.8)
1996 2784 (3.3)
1997 3273 (3.9)
1998 3985 (4.7)
1999 4917 (5.8)
2000 7015 (8.3)
2001 8958 (10.6)
2002 10031 (11.9)
2003 10417 (12.3)
2004 11278 (13.3)
2005 11154 (13.2)
Total 84596
Clinical, anthropometric, and laboratory variables for all individuals were organised into six-
monthly windows to provide longitudinal data for the follow-up period of 17 years from 1990 to
2007. In cases where an individual have more than one recorded values for the parameters under
consideration, one representative value within the timeframe of six months was selected.
Detailed exploration of this longitudinal data identified outliers and clinically implausible values,
which might have arisen as a result of measurement or data entry error. Values below and above the
clinically acceptable range were removed from the final dataset of 84596 patients.

25
For patients who remained alive, the last follow-up date was set to 1 December 2007 for censoring
purposes and obtained the date of death for others who died. Time-to-death was calculated using the
date of diagnosis and the modified death date (which included the last follow-up date for patients
who remained alive).
Time to first cardiovascular event and to onset of use of medications was similarly calculated, with
a censoring indicator. Cardiovascular disease included MI, stroke, HF, CHD, PAD, angina,
angioplasty, and CABG.
A variable was created identifying the oral diabetes drugs (OAD) prescribed; these were metformin,
sulphonylurea, rosiglitazone, pioglitazone, or meglitazone.
Patients were categorised according to their use of hypertensive medications, and, more generally,
cardio protective medications (CPM), which included ACE/ARB, beta blockers or statins.
During the follow-up, study subjects may have experienced a specific disease condition at different
time points. Each of these events was recorded as an independent event, together with date of
occurrence. As a result, a patient may have multiple records of the same disease, but the total
number of occurrences of each of these events are not directly available from CPRD data.
Consequently, the total number of occurrences of each of these events had to be separately
calculated.
Identification of the true missing cases in longitudinal data
Missing data is a common occurrence in all longitudinal studies and the CPRD is no exception.
Missing values may be ‘actual’ as well as ‘not in follow-up’. A missing value is ‘actual’ if the
timing of the measurement occurs within the follow-up period, but no value is available. In
longitudinal studies missingness can occur if the patient follow-up time is left or right censored; this
can be considered as the second type of missingness. The values for this period are also recorded as
missing.
The number and percentage of actual missing observations in the anthropometric and clinical data
over each time point are listed in the Appendix. Each of the individual missing is identified as
whether it is ‘actual’ or ‘not in follow-up’ using SAS 9.2.

26
3.6: Description of the Demographic, Anthropometric and Clinical Study Parameters
During the Study
The study population of 84596 newly diagnosed T2DM patients comprised 45855 males (54.2%)
and 38741 females (45.8%) with a mean (SD) age of 62.36 (13.27) years. Of these patients, 41482
(49.0%) were never-smokers, and 13598 (16.1%) were current smokers with 32.1% former
smokers. A major proportion of the patients consumed alcohol (n=54605; 64.5%). Descriptive
statistics of the baseline clinical and laboratory parameters are given in Table 3.2.
Table 3.2: Descriptive characteristics of 84,596 newly diagnosed T2DM patients at the time of
diagnosis
N Mean or % Range
Age 84596 62.4 (13.3) 18 to 99
Male* 45855 54.2
Female* 38741 45.8
Smoking status*
Never 41482 49.0
Former 27125 32.1
Current 13598 16.1
Alcohol consumption*
None 19238 22.7
Former users 2963 3.5
Current users 54605 64.5
Deprivation score ** 84621 19.05 (24)
Height (m) 18405 1.68 (0.10) 1.12 to 2.22
Weight (kg) 50928 86.25 (19.45) 30.4 to 295
BMI (kg/m2) 49292 30.55 (6.24) 15.2 to 95.3
SBP (mmHg) 58370 141(19) 62 to 244
DBP (mmHg) 58368 81 (10) 30 to 170
HbA1c 38175 7.85(1.96) 1.3 to 21.2
HbA1c** 7.3(2)

27
LDL 13917 2.91(1.04) 0.2 to 14.3
HDL 16696 1.23(0.42) 0.2 to 17.0
Triglycerides** 22062 1.80(1) 0.2 to 24.9
Total cholesterol 23280 5.15(1.43) 0.8 to 20.7
* n (%), ** Median (IQR)
Baseline distributions, by gender, of continuous anthropometric, clinical and biochemical study
parameters have been examined using kernel density plots. This particular method is commonly
used to smooth sample data into a continuous probability density function. In this procedure, a
known density function (the kernel) is averaged across the observed data points to create a smooth
approximation.
The kernel density estimate, f (n), of a set of n points of density f is defined as:
where K is the kernel function h is the smoothing parameter.
In constructing the kernel density plots, the Epanechikov kernel was selected. The possible
differences in the distributions of individual parameters, by gender, were tested using a non-
parametric Mann-Whitney test. Significance levels (P values) are displayed in the individual density
plots in Figure 3.1 (Fig: 3.1A to Fig: 3.1N).

28
Figure 3.1: Density plots of anthropometric, clinical and biochemical parameters
A B
C D
E F

29
G H
I J
K L

30
3.7: Prior Clinical Conditions and Family History
Of the 84596 patients, 2.8 % (n=2380) had a history of myocardial infarction (MI), 3.7 % (n=3172)
had had stroke, 5% (n=4221) had had heart failure, and 10.3% (n=8732) had had coronary heart
disease (CHD). Nearly 2.3% (n=1948) previously suffered from peripheral artery disease (PAD),
and 11.4% (n=9650) of the patients had had angina. Only 1% (n=881) had had angioplasty
performed, and nearly 2% (n=1956) had undergone coronary artery bypass graft (CABG) surgery
(Table 3.3). Approximately 23% of the patients (n=19432) had had some type of cardiovascular
event, and approximately 1% of the patients had a family history of angina and/or MI (Table 3.3).
Over the follow-up of 17 years in T2DM patients, it is possible to develop different cardiovascular
events such as MI, stroke, HF, CHD, PAD etc. Those who had a history of these diseases prior to
the diagnosis of T2DM have a greater chance of developing them again. A new variable was
created (both CVD) to indicate whether the patient had experienced any CVD solely prior to the
diagnosis, during the follow-up or both.
M N

31
Table 3.3: Description of Previous Medical History in the Cohort.
Previous medical history n %
MI 2380 2.80
Stroke 3172 3.70
Heart failure 4221 5.00
CHD 8732 10.3
PAD 1948 2.3
Angina 9650 11.4
Angioplasty 881 1.0
CABG 1596 1.9
Any cardiovascular event* 19432 23.0
Neuropathy 2866 3.4
Family history
MI 885 1.0
Angina 638 0.8
Hypercholesterolemia 126 0.1
Any cardiovascular event*: (MI or stroke or HF or CHD or PAD or angina or angioplasty or
CABG)
3.8: Event Data
Calculation of time-to-event data:
The time to all clinical and non-clinical events relevant to this study, as well as death, were
available in the original CPRD database. This information was collected from various sources,
including GP diaries, hospital records, etc. Time-to-event was calculated in days by subtracting the
date the patient was diagnosed with diabetes from the date the first event under consideration was
reported.
Approximately 3.4% of patients (n=2873) had experienced at least one non-fatal MI, and 5.4%
(n=4600) had suffered at least one non-fatal stroke during the follow-up period. Approximately

32
5.6% (n=4726) of patients had had at least one episode of heart failure, 2.5% (n=2078) had PAD,
and about 8.5% (n=7191) had CHD. Nearly 17.8% (n=15050) had had at least one of these
aforementioned cardiovascular events or diseases. Almost 6.9% (n=5840) of the patients had angina
and 0.8% (n=689) had undergone angioplasty. 5% (n=4186) of patients had developed cancer. A
total of 11084 (13.1%) patients died during the follow-up period after diagnosis of diabetes. Details
on the events are presented in Table 3.4.
Table 3.4: Description of current clinical events and all-cause mortality in patients with
T2DM
Event Proportion of patients with
at least one event n (%)
Median (range) no.
of events during the
follow-up*
Median time to first
event (Days)*
Non-fatal MI 2873 (3.40) 2 (17) 1108
Non-fatal Stroke 4600 (5.40) 2 (30) 1053
Heart failure 4726 (5.6) 1 (31) 973
PAD 2078 (2.5) 1 (10) 1018
CHD 7191(8.5) 926
Angina 5840 (6.9)
Coronary
angioplasty
689 (0.8)
CABG 826 (1.0)
Any CVE 16659 (19.7)
Cancer 4186 (4.90) 1112
Death 11084 (13.1) 1259
* Median (range) no. of events during the follow-up and median time to first event is calculated for
each study parameter separately. ** Any cardiovascular event (CVE): MI, stroke, HF, CHD, PAD,
angina, angioplasty, or CABG.
3.9: Medication Records During the Follow-Up
More than 74% of the patients had been treated with at least one oral anti-diabetes drug, with
approximately 63% (n=52846) and 46% (n=38609) on metformin or sulphonylurea, respectively.
Approximately 34.2% (n=28958) had been taking both metformin and sulphonylurea. About 11%

33
of the patients had been taking rosiglitazone at some stage during the follow-up. Only 4% of the
patients had been treated with pioglitazone. Of the 84596 patients, 11.7% (n=9909) had been treated
with insulin of any kind during the follow-up period (Table 3.5), though information regarding the
type and doses was not available. Almost 10.5% (n=8895) of patients had been taking insulin with
at least one OAD.
The majority of patients (71%, n=60033) had been undergoing statin treatment, with about 64%
(n=53986) on ACE/ARB and about 34% (n=28604) on beta blockers (Table 3.5). A large
proportion of subjects (70.9%; n=59972) had been taking either type of hypertensive medication
(beta blockers or ACE/ARB) during the follow-up period. T2DM patients in this study cohort were
taking different medications for different clinical conditions at the same time, i.e., an individual
who have been diagnosed with T2DM may suffer from other concomitant diseases such as
hypertension, dyslipidaemia etc. and be receiving medications to control each of these clinical
conditions.
Table 3.5: Record of current medication in the patients with T2DM
Current medication n %
Metformin 52846 62.5
Sulphonylurea 38609 45.6
Rosiglitazone 9486 11.2
Pioglitazone 3319 3.9
Meglitazone 970 1.1
Any Oral anti-diabetic drug 62689 74.1
Insulin 9909 11.7
Statins 60033 71.0
Beta Blockers 28604 33.8
ACE/ARB 53986 63.8
Any hypertensive medication 59972 70.9

34
3.10: Longitudinal Data
Seventeen year longitudinal data of anthropometric, clinical and biochemical parameters for the
newly diagnosed T2DM patients from UK CPRD are arranged in six-monthly time window. The
longitudinal distributions of these study parameters over the entire follow-up period are presented in
Figure 3.2 (Figures 3.2A to 3.2R), using mean (SE) or median (IQR), as appropriate, for the whole
cohort, as well as by gender.

35
Fig
ure
3.2
: L
on
git
ud
inal
dis
trib
uti
on
s of
the
stu
dy p
ara
mete
rs o
ver
all
an
d b
y g
end
er
A
B
BM
I-O
ver
all
SB
P-O
ver
all
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

36
C
D
DB
P-O
ver
all
Hb
A1
c-O
ver
all
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

37
E
F
LD
L-O
ver
all
HD
L-O
ver
all
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

38
BM
I-F
emal
e B
MI-
Mal
e
Mo
nth
s M
on
ths
H
G
Mean+-2 SE
Mean+-2 SE

39
SB
P-F
emal
e S
BP
-Mal
e
Mo
nth
s M
on
ths
I J
Mean+-2 SE
Mean+-2 SE

40
K
L
DB
P-F
emal
e D
BP
-Mal
e
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

41
M
N
Hb
A1
c-F
emal
e D
BP
-Fem
ale
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

42
O
P
LD
L-F
emal
e D
BP
-Mal
e
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2 SE

43
Q
R
HD
L-F
emal
e L
DL
-Fem
ale
Mo
nth
s M
on
ths
Mean+-2 SE
Mean+-2SE

44
Chapter 4. Gender Specific Effects of Smoking in T2DM Patients

45
Evaluation of the gender specific effects of smoking on cardiovascular and mortality outcomes
among newly diagnosed diabetic men and women
4.1: Background
Cigarette smoking has caused a major and avoidable public health disaster across the world, in both
developed and developing nations. According to a recent report by the National Centre for Chronic
Disease Prevention and Health Promotion, more than 20 million premature deaths have been caused
by cigarette smoking 74
. According to that report, 22% of adults in the US are smokers. The
causally-linked damage that cigarette smoking has on various human organ systems is depicted in
figure 4.1. As is clear from the figure, smoking affects all organs of the body, resulting in drastic
quality of life reductions. Smoking is a modifiable risk factor for many chronic diseases, such as
cardiovascular disease, cancer, chronic lung disease, asthma, and diabetes. Type 2 diabetes mellitus
is a multifactorial, chronic, non-communicable disease. Recent increases in the prevalence of
T2DM patients have been attributed to a dramatic increase in overweight and obese persons in both
high- and low-income countries 66
. Research has shown that smoking is associated with higher risks
of T2DM. The driving forces behind the increased risks are insulin sensitivity, accumulation of
abdominal adipose tissue, and pancreatic β cell dysfunction. The effect of smoking on T2DM can
be influenced by physical status such as being overweight 105
. According to a study by Patja et al.
on middle aged Finnish men and women, smoking is highly detrimental in patients with higher
BMIs 106
.
4.1.1: Cardiovascular disease risks in T2DM patients
Cigarette smoking is an important chronic disease risk factor in both diabetic and non-diabetic
populations. Globally, it is recognised to be one of the leading causes of premature mortality 15,74
.
The major cause of mortality in patients with T2DM are cardiovascular (microvascular,
macrovascular) and renal complications, which are directly related to cigarette smoking. As a result,
smoking further exacerbates the increased mortality risk of patients with diabetes. The United
Kingdom Prospective Diabetes Study (UKPDS) showed that cigarette smoking was a significant
and independent risk factor for coronary heart disease, stroke and peripheral vascular disease in
people newly diagnosed with T2DM 21-23
. A recent systematic review and meta-analysis of diabetic
patients reported that cigarette smoking is associated with a 48% increased mortality risk, 54%
increased risk of coronary heart disease, 44% increased risk of stroke, and 52% increased risk of
myocardial infarction 76
.

46
Figure 4.1: The health consequences causally associated with smoking 74
4.1.2: Gender differences in the association between cigarette smoking and coronary heart
disease and stroke
Studies have shown that cardiovascular mortality in T2DM patients without coronary heart disease
(CHD) is same as that of those with CHD and without T2DM 77,78
. Differences between gender, in
the mortality risk observed in patients with CHD, women having poorer prognoses than men 107
.
Older age, occurrences of major comorbid conditions, and clinical conditions that are clinically
difficult to manage are some of the major reasons behind poor outcomes in women who had CHD
27.
A major cause of death in diabetic patients is stroke. According to a recent report conducted in the
US, the predicted number of deaths from stroke in women by 2050 will be higher, by 68000 deaths,

47
than that of men due to the higher number of events and lower recovery among women 79,80
. Gender
differences in stroke cases have been observed in epidemiological studies, and successful
prevention and management options have been significantly affected by this gender difference 79
.
There are a number of reasons underlying the adverse effects of T2DM being more significant in
women than in men. The longer life expectancy of women compared to men could be one of the
reasons why women suffer a higher number of strokes than men 108
. According to other studies, the
sources of gender differences in cardiovascular disease risks are differences in levels of the risk
factors of cardiovascular diseases. For example, T2DM women had significantly higher blood
pressure levels and lipid profiles than men with T2DM 24
. Another possible reason for the higher
risk in diabetic women is that women with T2DM may be less likely to receive appropriate
treatment 109
.
Coronary artery disease is one of the major causes of death among both men and women 110
.
Previous studies have shown that the relative risks of CHD and mortality, in relation to T2DM,
were higher in women than in men when compared to their diabetes-free counterparts. Previous
studies have also shown that the relative risks of fatal CHD attributed to T2DM were 50% higher in
women than in men 24
. Smoking is considered an important risk factor for arterial hypertension and
diabetes management 111,112
.
4.1.3: Impact of smoking cessation on cardiovascular risk in individuals with and without
diabetes
The meta-analysis conducted by Willi et al. (2007), based on 25 prospective cohort studies (1.2
million patient records), reported a 44% (95% CI of rate ratio: 1.31, 1.58) increased risk of incident
diabetes (T2DM) associated with active smoking 113
. Fagard (2009) reported a significantly
increased risk of mortality and coronary heart disease (CHD) associated with smoking in patients
with hypertension and diabetes 111
.
However, smoking cessation, after ten years, normalises the subsequent risk of CHD to values
similar to those of never-smokers 114-117
. A study by Chaturvedy et al. on diabetes patients showed
that the all-cause mortality risk in former smokers was 50% higher for patients who stopped
smoking within the previous nine years and 25% higher for individuals who stopped smoking more
than ten years prior, compared to those who had never smoked 117
. This study also showed that risks
remained high several years after quitting smoking and were highly dependent on the duration of

48
smoking 117
. Another study by Kengne et al. has shown that, irrespective of diabetes status, smoking
cessation was associated with a 19% reduction in cardiovascular risk 118
.
4.2: Objectives
The objectives of this chapter are to:
1. quantify the risk of cardiovascular diseases and all-cause mortality associated with current
smoking, separately for women and men with diabetes.
2. determine whether there are significant gender differences in the relationship between
smoking and cardiovascular outcomes, and all-cause mortality in individuals with diabetes.
3. examine the benefits of smoking cessation on the risk of cardiovascular diseases and all-
cause mortality in men and women with diabetes.
4.3: Methods
4.3.1:Data
The Clinical Practice Research Datalink (CPRD) is a large proprietary, anonymised, longitudinal
dataset derived from primary care in the United Kingdom. The CPRD contains clinical information,
including diagnoses, mortality, laboratory results and prescription data 119,120
. The primary data set
for this retrospective cohort study includes data from 84596 individuals, aged 18 to 99 years, who
were newly diagnosed with T2DM between January 1990 and December 2005, and who have been
registered with their general practice for at least 12 months 121
. Rigorous classification techniques
were used to ensure the correct identification of patients with T2DM (Chapter 3). The following
information was extracted: age, gender, smoking status (defined as current, former or never
smoker), BMI, blood pressure recordings (systolic and diastolic), HbA1c, lipid measurements,
history of cardiovascular diseases before the diagnosis of diabetes; the recorded clinical events
during follow-up included CVD (myocardial infarction, stroke, heart failure, angina, coronary heart
disease, peripheral arterial disease, and conditions requiring angioplasty or coronary artery bypass
graft), diabetic neuropathy, renal complications, along with dates of events. The date of death was
derived from modified GPRD death codes. Specific disease Read codes capture data as part of
routine care (including investigations) or as a result of hospitalisation or emergency care 120,122-124
.

49
Among these 84596 individuals, 82205 had complete data on smoking status at diagnosis of
diabetes, as well as complete data on other demographic information. The data for prescribed
medications, with prescription dates, after diagnosis of diabetes—including use of oral anti-diabetes
drugs, ACE/ARB, beta blocker, statin and other concomitant medications—were obtained. The
patients who were prescribed with any one of ACE/ARB, beta blockers or statins were, collectively,
categorised as patients under treatment with cardio protective medications. The patients who were
taking either ACE/ARB or beta blockers were defined as patients under treatment with hypertensive
medications.
Ethics approval for the use of CPRD data was granted by the Independent Scientific Advisory
Committee in June 2014.
4.3.2: Statistical Methods
Summary statistics for the study population are presented by number (percentage), mean (SD) or
median (IQR), as appropriate. Differences between the smoking groups were tested with Student’s
t-test for near normally distributed continuous variables and the Pearson chi-square test for
categorical variables. Separate Cox regression models were used to evaluate the risk associated with
smoking (current versus former, and current versus never) for each of the cardiovascular events and
all-cause mortality during follow-up. All Cox models were tested for the proportional hazard
assumption and satisfied this assumption.
In order to quantify the risk associated with each of the individual components of the cardiovascular
disease under consideration, multivariate models were fitted separately for all patients and for
patients with and without a previous history of cardiovascular disease. Patients with previous
cardiovascular disease would be more likely to have more attention given to their medical condition
and disease progression.
Gender specific risks were estimated using the lincom statement in Stata, which calculates the
individual effects as a linear combination of estimators of coefficients of model terms. The P-values
used in the test for interaction between gender and smoking are given in the text, together with
gender specific hazard ratios. Separate models were used for mortality and each of the
cardiovascular events, after adjusting for the effects of age, alcohol consumption, baseline BMI,
baseline HbA1c, treatment with OADs, hypertensive medications and cardio protective
medications. The gender specific absolute risks and adjusted risk difference associated different
smoking behaviours had calculated separately for men and women.

50
4.4: Results
In the study cohort (n=82205), 45.5% were female, with a mean (SD) age of 64 (14) years; the male
cohort was younger, with a mean age of 61 (12) years. The characteristics of the population, by sex
and smoking status, are given in Table 4.1. In general, at their time of diagnosis with T2DM,
women were more likely than men to be older, marginally obese, and had significantly higher levels
of SBP, LDL, and HDL than men. A subgroup analysis by gender and smoking status also
supported the finding that women recorded higher values for these clinical measurements than men.
However levels of DBP, HbA1c and triglycerides were higher in men at the start of the study. The
proportions of current smokers (60%) and former smokers (67%) were higher in men. Distributions
of all baseline demographic characteristics, clinical histories, laboratory measurements, and
medications during the follow-up are presented in Table 4.1, separately for men and women and by
smoking status.
The proportion of never, former and current smokers who had MI during the follow up was higher
among men compared to women (2.57 vs 3.56, 3.07 vs 4.56% and 2.90 vs 3.54%). CHD was higher
in all the three smoking categories (never, former and current) among men compared to their
women counterparts. The combined cardiovascular disease event (any cardiovascular event) was
higher among current smoking men (n=1582, 19.26%) compared to currently smoking women
(n=899, 16.69%). Similarly the proportion of patients with any CVD was higher in men for former
smokers and never smokers compared to their respective women counterparts. The consumption of
oral anti diabetes drugs, hypertensive medications and cardio protective medications during the
follow-up were similar between men and women.

51
Tab
le 4
.1:
Base
lin
e ch
ara
cter
isti
cs o
f th
e C
lin
ical
Pra
ctic
e R
esea
rch
Da
tali
nk
(C
PR
D)
by s
mok
ing s
tatu
s in
wom
en a
nd
men
(1990
-2005).
W
om
en
Men
S
mok
ing s
tatu
s at
base
lin
e
Sm
ok
ing
sta
tus
at
base
lin
e
N
ever
F
orm
er
Cu
rren
t N
ever
F
orm
er
Cu
rren
t
No. of
pati
ents
(%
) 23028
9017
5385
18
45
4
18
10
8
82
13
Age
(yea
rs)*
65 (
14)
65 (
12)
64 (
14)
60
(1
3)
63
(1
1)
57
(1
2)
Bod
y M
ass
Ind
ex (
kg/m
2)*
31.0
2 (
6.8
9)
31.9
8 (
6.8
4)
31.6
7 (
7.2
3)
29
.84
(5.8
8)
29
.93
(5.1
3)
29
.89
(5.6
9)
SB
P (
mm
Hg)*
143 (
20)
143 (
19)
139 (
20)
14
0 (
18)
14
0 (
18)
13
9 (
18)
DB
P (
mm
Hg)*
81 (
10)
80 (
10)
80 (
10)
82
(1
0)
81
(1
0)
81
(1
0)
LD
L-c
(m
mol/
l)*
3
.03 (
1.0
6)
2.9
7 (
1.0
9)
3.0
6 (
1.0
8)
2.8
4 (
0.9
9)
2.7
5 (
1.0
0)
2.8
9 (
1.0
3)
HD
L-c
(m
mol/
l)*
1.3
3 (
0.4
2)
1.3
2 (
0.4
7)
1.2
4 (
0.3
8)
1.0
5 (
0.3
4)
1.1
6 (
0.3
4)
1.1
3 (
0.5
5)
Tri
gly
ceri
des
(m
mol/
l)*
2
.01 (
1.2
4)
2.1
5 (
1.2
2)
2.5
8 (
1.7
8)
2.2
0 (
1.7
8)
2.2
1 (
1.6
4)
2.7
9 (
2.2
4)
HbA
1c
(%)*
7
.81 (
1.9
5)
7.8
0 (
1.9
2)
7.9
2 (
1.9
7)
7.8
6 (
1.9
9)
7.7
8 (
1.9
3)
8.0
9 (
2.0
0)

52
Cli
nic
al
his
tory
n (
%)
Myoca
rdia
l In
farc
tion
#
591 (
2.5
7)
277 (
3.0
7)
156 (
2.9
0)
65
7 (
3.5
6)
82
5 (
4.5
6)
29
1 (
3.5
4)
Str
oke#
1
347 (
5.8
5)
480 (
5.3
2)
250 (
4.6
4)
89
0 (
4.8
2)
10
09
(5
.57
) 4
04
(4
.92
)
Hea
rt f
ailu
re#
1219 (
5.2
9)
603 (
6.6
9)
210 (
3.9
0)
92
1 (
4.9
9)
11
97
(6
.61
) 3
49
(4
.25
)
Coro
nar
y H
eart
Dis
ease
#
1458 (
6.3
3)
746 (
8.2
7)
363 (
6.7
4)
16
21
(8
.78
) 2
21
1 (
12
.21
) 6
74
(8
.21
)
Per
ipher
al A
rter
ial
Dis
ease
#
301 (
1.3
1)
245 (
2.7
2)
169 (
3.1
4)
29
5 (
1.6
0)
69
4 (
3.8
3)
35
1 (
4.2
7)
An
y c
ardio
vas
cula
r ev
ent#
3978 (
17.2
7)
1831 (
20.3
1)
899 (
16.6
9)
33
98
(18
.41
) 4
43
6 (
24
.50
) 1
58
2 (
19
.26
)
Dea
th#
2843 (
12.3
5)
1037 (
11.5
0)
682 (
12.6
6)
21
81
(11
.82
) 2
18
0 (
12
.04
) 1
08
0 (
13
.15
)
Ora
l an
ti-d
iab
etes
dru
g#
17044 (
74.0
1)
6724 (
74.5
7)
4028 (
74.8
0)
13
57
7 (
73
.57)
13
53
2 (
74
.73)
62
91
(76
.60
)
Hyp
erte
nsi
ve
med
icat
ion
s#
16385 (
71.1
5)
6898 (
76.5
0)
3459 (
64.2
3)
12
99
9 (
70
.44)
14
05
4 (
77
.61)
53
14
(64
.70
)
Car
dio
pro
tect
ive
med
icat
ions#
1
9699 (
85.5
4)
8140 (
90.2
7)
4538 (
84.2
7)
15
74
5 (
85
.32)
16
47
1 (
90
.96)
68
33
(83
.20
)
Dura
tion o
f fo
llow
-up (
yea
rs)*
6
.31 (
3.6
9)
6.1
5 (
3.6
0)
5.9
1 (
3.5
1)
6.2
5 (
3.6
5)
6.1
9 (
3.5
3)
5.9
9 (
3.5
8)
* m
ean (
stan
dar
d d
evia
tio
n),
# n
(%
)

53
4.4.1: Association between smoking and cardiovascular outcomes in individuals without a
prior history of CVD by gender
i. Current smokers vs. former smokers
In patients without a history of a cardiovascular disease prior to the diagnosis of T2DM, women
who are current smokers had significantly higher risk of MI, compared to current smoking men and
women who were former smokers (HR, 95% CI: 6.66, 2.32-19.11, P-value:<0.001). However the
mortality risk was higher among men (HR, 95% CI of HR:1.58, 1.26-1.97 ) compared to women
(HR, 95% CI: 1.42, 1.08-1.85, P-value:<0.001), (Table 4.2, Figure 4.2).
ii. Current smokers vs. never-smokers
The analysis of current smokers against never-smokers suggested that women who currently smoke
face a higher risk of cardiovascular disease and death compared to men who currently smoke. In
patients without a prior history of CVD, a significantly higher risk of MI, heart failure, CHD and
death was reported among women who smoke. The risk associated with PAD was significantly
higher in men (HR, 95 % CI: 4.7, 1.52-14.49, P-value:<0.001) compared to women (HR, 95 % CI:
3.1, 0.75-12.41) (Table 4.2, Figure 4.3).
Among patients without a history of CVD, the interactions between gender and being a former
smoker on the risk of heart failure and mortality were significant (P < 0.01 for both). Significant
interactions between gender and current smoking were observed for the risks of MI and mortality (P
< 0.05, P < 0.01, respectively). Other cardiovascular diseases showed no such interactions.

54
Tab
le 4
.2:
Ad
just
ed g
end
er s
pec
ific
haza
rd r
ati
os
(95%
con
fid
ence
in
terv
als
) ass
oci
ate
d w
ith
CV
D a
nd
all
-cau
se m
ort
ali
ty b
y s
mok
ing s
tatu
s
in i
nd
ivid
uals
wit
hou
t p
rior
his
tory
of
CV
D f
rom
th
e C
lin
ical
Pra
ctic
e R
esea
rch
Data
lin
k (
CP
RD
) (1
990 –
2005)
Ou
tcom
e
C
urr
ent
Vs
Form
er
Cu
rren
t V
s N
ever
N
o.
even
ts
HR
(95%
CI)
P
-valu
e H
R (
95
% C
I)
P-v
alu
e
MI
Men
295
1.8
1 (
0.8
0,
4.0
8)
0.1
5
1.7
1 (
0.7
5,
3.8
8)
0.2
0
Wom
en
196
6.6
6 (
2.3
2,
19.1
1)
< 0
.001
7.8
6 (
3.4
2,
18
.06
) <
0.0
01
Str
oke
Men
614
1.5
1 (
0.9
3,
2.4
3)
0.0
9
1.4
8 (
0.9
1,
2.4
0)
0.1
1
Wom
en
653
1.5
3 (
0.8
5,
2.7
6)
0.1
6
1.4
9 (
0.8
9,
2.4
9)
0.1
3
Hea
rt F
ailu
re
Men
133
1.1
8 (
0.3
2,
4.3
4)
0.8
0
0.6
9 (
0.2
0,
2.4
1)
0.5
7
Wom
en
175
1.8
0 (
0.6
4,
5.0
2)
0.2
6
8.6
0 (
2.7
4,
27
.02
) <
0.0
01
CH
D
Men
1462
0.9
3 (
0.6
7,
1.2
9)
0.6
7
1.3
4 (
0.9
5,
1.8
9)
0.0
9
Wom
en
958
1.2
0 (
0.7
9,
1.8
3)
0.3
9
1.5
2 (
1.0
4,
2.2
4)
0.0
3
PA
D
Men
50
2.0
5 (
0.8
1,
5.1
9)
0.1
3
4.6
9 (
1.5
2,
14
.49
) 0
.00
7
Wom
en
33
1.5
8 (
0.3
5,
7.1
7)
0.5
5
3.0
6 (
0.7
5,
12
.41
) 0
.11

55
Dea
th
Men
3212
1.5
8 (
1.2
6,
1.9
7)
< 0
.001
1.4
7 (
1.1
8,
1.8
4)
0.0
01
Wom
en
2973
1.4
2 (
1.0
8,
1.8
5)
0.0
1
2.6
0 (
2.0
2,
3.3
5)
< 0
.00
1

56
4.4.2: Association between smoking and cardiovascular outcomes in individuals with a prior
history of CVD
I. Current smokers vs. former smokers
In patients with history of a CVD prior to their diagnosis with T2DM, women who smoked had a
significantly higher risk of MI (HR, 95% CI: 1.90, 1.16-3.13, P = 0.01) than men. The risks
associated with PAD (HR, 95% CI: 1.68, 1.28-2.20, P < 0.001) and mortality (HR, 95% CI: 2.04,
1.41-2.96, P-value:<0.001) were higher in women compared to men. (Table 4.3, Figure 4.4)
II. Current smokers vs. never-smokers
In this comparison, significantly higher hazard ratios were observed in women, for both PAD (HR,
95% CI: 2.87, 2.19-3.77, P < 0.001) and mortality (HR, 95% CI: 2.43, 1.72-3.44, P < 0.001) than
men (Table 4.3, Figure 4.5).
In patients who had had CVD prior to their T2DM diagnosis, a significant interaction between
gender and current smoking was observed for mortality.
The gender specific adjusted risk difference per 1000 person years among former smokers and
current smokers according to their cardiovascular disease status is given in Table 4.4 and Table 4.5.
In patients without cardiovascular disease prior to diagnosis women reported higher cases of
individual cardiovascular diseases per 1000 person years. The adjusted risk differences for MI in
women among former and current smokers were almost 5 and 6 per 1000 person years compared to
their never smoking counterparts. Similarly the risk difference associated with mortality was higher
in women by 26 per 1000 person years among current smoking diabetes patients. In patients with
cardiovascular disease prior to the diagnosis of T2DM, mortality risk difference was higher in
women who were former (35 vs 19) and current (48 vs 18) smokers per 1000 person years
compared to never smoking diabetic patients.

57
Tab
le 4
.3:
Ad
just
ed g
end
er s
pec
ific
haza
rd r
ati
os
(95%
con
fid
ence
in
terv
als
) ass
oci
ate
d w
ith
CV
D a
nd
all
-cau
se m
ort
ali
ty b
y s
mok
ing s
tatu
s
in i
nd
ivid
uals
wit
h p
rior
his
tory
of
CV
D f
rom
th
e C
lin
ical
Pra
cti
ce R
esea
rch
Data
lin
k (
CP
RD
) (1
990 –
2005)
Ou
tcom
e
C
urr
ent
Vs
Form
er
Cu
rren
t V
s N
ever
N
o.
even
ts
HR
(95%
CI)
P
-valu
e H
R (
95
% C
I)
P-v
alu
e
MI
Men
1478
0.8
9 (
0.6
3,
1.2
5)
0.5
0
1.0
9 (
0.7
1,
1.6
6)
0.7
0
Wom
en
828
1.9
0 (
1.1
6,
3.1
3)
0.0
1
0.7
1 (
0.4
9,
1.0
1)
0.0
6
Str
oke
Men
1689
1.2
2 (
0.8
9,
1.6
5)
0.2
1
0.9
6 (
0.6
9,
1.3
2)
0.7
9
Wom
en
1424
1.0
2 (
0.6
7,
1.5
6)
0.9
1
0.8
9 (
0.6
1,
1.3
2)
0.5
7
Hea
rt F
ailu
re
Men
2334
0.9
9 (
0.7
6,
1.3
0)
0.9
4
1.0
5 (
0.7
9,
1.4
0)
0.7
4
Wom
en
1857
1.0
6 (
0.7
4,
1.5
3)
0.7
3
1.1
2 (
0.8
0,
1.5
8)
0.5
1
CH
D
Men
3044
0.8
0 (
0.6
4,
1.0
0)
0.0
5
0.7
9 (
0.6
3,
1.0
1)
0.0
6
Wom
en
1609
1.2
6 (
0.8
9,
1.7
7)
0.1
9
0.9
5 (
0.7
0,
1.2
9)
0.7
3
PA
D
Men
682
1.5
2 (
1.2
7,
1.8
4)
<0.0
01
2.5
7 (
2.0
5,
3.2
2)
<0
.00
1
Wom
en
1290
1.6
8 (
1.2
8,
2.2
0)
<0.0
01
2.8
7 (
2.1
9,
3.7
7)
<0
.00
1

58
Dea
th
Men
1589
1.5
9 (
1.2
3,
2.0
6)
<0.0
01
1.5
5 (
1.1
8,
2.0
5)
0.0
02
Wom
en
2229
2.0
4 (
1.4
1,
2.9
6)
<0.0
01
2.4
3 (
1.7
2,
3.4
4)
<0
.00
1

59
Fig
ure
4.2
: A
dju
sted
haza
rd r
ati
os
an
d 9
5%
con
fid
ence
in
terv
als
for
curr
ent
smok
ing v
ersu
s fo
rm
er s
mok
ing b
y g
end
er i
n d
iab
etic
pati
ents
wit
hou
t p
rior
CV
D.

60
Fig
ure
4.3
: A
dju
sted
haza
rd r
ati
os
an
d 9
5%
con
fid
ence
in
terv
als
for
curr
ent
smok
ing v
ersu
s n
ever
-sm
ok
ers
by g
end
er i
n d
iab
etic
pati
ents
wit
hou
t p
rior
CV
D.

61
Fig
ure
4.4
: A
dju
sted
haza
rd r
ati
os
an
d 9
5%
con
fid
ence
in
terv
als
for
curr
ent
smok
ing v
ersu
s fo
rm
er s
mok
ing b
y g
end
er i
n d
iab
etic
pati
ents
wit
h p
rior
CV
D.

62
Fig
ure
4.5
: A
dju
sted
haza
rd r
ati
os
an
d 9
5%
con
fid
ence
in
terv
als
for
curr
ent
smok
ing v
ersu
s n
ever
-sm
ok
ers
by g
end
er i
n d
iab
etic
pati
ents
wit
h p
rior
CV
D.

63
Tab
le 4
.4:
Gen
der
sp
ecif
ic a
bso
lute
ris
ks
an
d a
dju
sted
ris
k d
iffe
ren
ce f
or
smok
ing h
ab
its
ass
oci
ate
d w
ith
CV
D a
nd
all
-cau
se m
ort
ali
ty i
n
ind
ivid
uals
wit
hou
t p
rior
his
tory
of
CV
D p
er 1
000 p
erso
n y
ears
fro
m t
he
Cli
nic
al
Pra
cti
ce R
esea
rch
Data
lin
k (
CP
RD
) (1
990 –
2005)
Outc
om
e
Abso
lute
ris
k
Ris
k D
iffe
rence
N
ever
sm
oker
s F
orm
er s
moker
s C
urr
ent
smo
ker
s F
orm
er
Cu
rren
t
MI
M
en
1.2
1 (
0.9
9,
1.4
5)
1.2
2 (
0.9
9,
1.4
9)
1.2
5 (
0.9
4,
1.6
7)
0.9
8
0.8
6
W
om
en
0.8
5 (
0.7
0,
1.0
3)
0.7
4 (
0.5
2,
1.0
6)
1.5
0 (
1.0
9,
2.0
7)
4.8
1
5.8
3
Str
oke
M
en
2.5
6 (
2.2
5,
2.9
2)
3.2
0 (
2.8
2,
3.6
2)
2.4
6 (
2.0
1,
3.0
3)
1.3
1
1.2
3
W
om
en
3.6
3 (
3.2
9,
3.9
9)
2.9
9 (
2.5
0,
3.5
8)
2.8
3 (
2.2
4,
3.5
7)
1.9
2
1.7
8
Hea
rt F
ailu
re
M
en
0.7
1 (
0.5
6,
0.9
1)
0.5
7 (
0.4
3,
0.7
7)
0.6
5 (
0.4
4,
0.9
7)
0.1
3
-0.2
2
W
om
en
1.0
2 (
0.8
5,
1.2
2)
0.9
1 (
0.6
6,
1.2
6)
0.7
1 (
0.4
5,
1.1
3)
0.8
2
7.7
5
CH
D
M
en
6.1
8 (
5.6
8,
6.7
3)
8.4
3 (
7.7
9,
9.1
1)
5.7
2 (
4.9
9,
6.5
6)
-0.4
3
2.1
0
W
om
en
4.6
5 (
4.2
7,
5.0
7)
5.9
8 (
5.2
7,
6.8
0)
5.2
9 (
4.4
6,
6.2
7)
0.9
3
2.4
2
PA
D

64
M
en
0.1
3 (
0.7
6,
0.2
3)
0.2
4 (
0.1
5,
0.3
7)
0.5
4 (
0.3
5,
0.8
4)
0.1
4
0.4
8
W
om
en
0.1
3 (
0.0
8,
0.2
1)
0.2
2 (
0.1
2,
0.4
2)
0.3
6 (
0.1
8,
0.6
8)
0.0
8
0.2
7
Dea
th
M
en
15
.16 (
14.3
8,
15.9
9)
15.2
1 (
14.3
6,
16.1
1)
18.5
4 (
17
.20
, 19
.98
) 8
.79
7.1
3
W
om
en
16
.08 (
15.3
6,
16.8
3)
15.5
7 (
14.4
0,
16.8
4)
18.5
9 (
16
.99
, 20
.35
) 6
.75
25
.73

65
Tab
le 4
.5:
Gen
der
sp
ecif
ic a
bso
lute
ris
ks
an
d a
dju
sted
ris
k d
iffe
ren
ce f
or
smok
ing h
ab
its
ass
oci
ate
d w
ith
CV
D a
nd
all
-cau
se m
ort
ali
ty i
n
ind
ivid
uals
wit
h p
rior
his
tory
of
CV
D f
rom
th
e C
lin
ical
Pra
cti
ce R
esea
rch
Data
lin
k (
CP
RD
) (1
990 –
2005)
Outc
om
e
Abso
lute
ris
k
Ad
just
ed r
isk d
iffe
ren
ce
N
ever
sm
oker
s F
orm
er s
moker
s C
urr
ent
smo
ker
s F
orm
er
Cu
rren
t
MI
M
en
22.0
9 (
20.2
6,
24.0
9)
20.5
8 (
19.0
8,
22.1
9)
19.5
8 (
17
.17
, 22
.32
) -2
.43
1.9
9
W
om
en
16.5
6 (
15.1
1,
18.1
4)
16.4
5 (
14.4
4,
18.7
3)
17.5
1 (
14
.47
, 21
.18
) 1
4.9
0
-4.8
0
Str
oke
M
en
27.3
1 (
25.2
4,
29.5
5)
22.2
3 (
20.6
7,
23.9
2)
26.5
2 (
23
.64
, 29
.75
) 6
.01
-1.0
9
W
om
en
34.9
8 (
32.7
5,
37.3
5)
25.5
9 (
23.0
1,
28.4
5)
28.8
3 (
24
.75
, 33
.57
) 0
.70
-3.8
5
Hea
rt F
ailu
re
M
en
37.8
4 (
35.3
7,
40.4
7)
36.4
7 (
34.4
1,
38.6
5)
28.6
6 (
25
.70
, 31
.96
) -0
.38
1.8
9
W
om
en
42.8
9 (
40.4
1,
45.5
2)
43.9
3 (
40.4
3,
47.7
2)
32.9
9 (
28
.61
, 38
.03
) 2
.57
5.1
5
CH
D
M
en
48.4
5 (
45.5
4,
51.5
5)
52.3
1 (
49.7
2,
55.0
3)
41.8
4 (
38
.07
, 45
.99
) -9
.69
-10
.17
W
om
en
33.9
1 (
31.7
1,
36.2
5)
37.5
6 (
34.3
1,
41.1
2)
37.2
8 (
32
.52
, 42
.74
) 8
.82
-1.7
0
PA
D

66
M
en
11.6
0 (
10.3
2,
13.0
4)
20.6
4 (
19.1
3,
22.2
6)
30.5
0 (
27
.38
, 33
.98
) 6
.03
18
.21
W
om
en
10.0
6 (
8.9
6,
11.3
0)
16.9
4 (
14.9
0,
19.2
6)
27.3
8 (
23
.44
, 31
.99
) 6
.84
18
.81
Dea
th
M
en
32.0
4 (
29.9
2,
34.3
2)
28.5
4 (
26.8
4,
30.3
6)
31.9
9 (
28
.99
, 35
.31
) 1
8.9
0
17
.62
W
om
en
32.9
4 (
30.9
3,
35.0
7)
26.9
3 (
24.4
2,
29.7
0)
32.3
0 (
28
.21
, 36
.98
) 3
4.2
6
47
.10

67
Multivariate Cox regression models for CVD and mortality risks suggest that diabetic women who
smoke are at a higher risk of these diseases, after adjusting for the effects of age at diagnosis,
alcohol consumption (never, former and current), baseline measurements of BMI, HbA1c, and the
consumption of OADs, hypertensive medications and cardioprotective medications.
Smoking cessation in those who were free from prior CVD results in the significant reduction, by
15%, of the risk of MI. Similarly, smoking cessation was associated with 51% and 30 % reductions
in mortality risk in those with and without prior episodes of CVD, respectively.
4.5: Discussion and Conclusion
In a large, population level cohort of patients with newly diagnosed T2DM, with 5.4 years of
median follow-up, smoking, irrespective of status (former/current, versus never-smokers), was
associated significantly with an increased risk of cardiovascular events and all-cause mortality in
women who have histories with and without CVD prior to their diagnosis with T2DM. Thus,
cigarette smoking increased what were already elevated cardiovascular and mortality risks.
Key strengths of this analysis include a large sample – taken from routine clinical practice with over
5.4 years follow-up – of individuals with T2DM, complete (non-missing) data on smoking status at
the time of diagnosis, detailed information on medications and cardiovascular events, and a focus
on mortality. Further, complete and reliable descriptions of cardiovascular events, along with the
times that they occurred were also available. The use of multivarite modelling techniques, to
account for the evaluation of risk factors, added further strength to the robustness of the estimates
obtained in this analysis.
The limitations of this study include the non-availability of data regarding (1) smoking status at the
end of the study, (2) frequency of smoking, (3) adherence to medications during the follow-up
period, and (4) some demographic variables such as ethnicity. This analysis also could not account
for changes in smoking behaviour over the follow-up time.
In this analysis, the gender specific effects of smoking on CVD and mortality suggest an increased
risk among diabetic women compared to men, which is consistent with other epidemiological
studies of gender specific effects 24,125,126
. When gender specific effects of smoking were compared,
there was some evidence to suggest a stronger coronary and mortality hazard in women, when
compared with men. This is consistent with the findings from previous reviews of the gender
specific impact of coronary risk in both diabetic patients and the general population 24,76
. The

68
mechanisms which might account for the higher risk of CVD and death in women who smoke
(current and former) compared to men is presently unknown. One potential explanation for this
could be undertreatment of T2DM in women compared to men. Although this study does not
provide any evidence to support this hypothesis, a study on gender desparities in treatment of
cardiac risk factors in diabetic patients concludes that women with diabetes receive less treatment
than diabetic men 127
.
A meta-analysis by Qin et al. reports that diabetic smokers have higher risks of MI, stroke, CHD
and all-cause mortality than their non-smoking counterparts 76
. Another meta analyses by Huxley et
al. on the gender stratified risk of coronary heart disease in patients wth cigarette smoking
concluded that smoking women had a significantly (25%) increased risk of coronary heart disease
than men 126
.
Studies have reported that patients with diabetes have an increased risk of MI 128,129
. The mortality
risk due to MI is double than that of their non-diabetic counterparts 128
. The risk for MI associated
with smoking is higher in diabetic patients 129
. Nilsson et al. (2009) 129
observed a 70% increased
risk of first-incident fatal/non-fatal MI among smokers. In this study, for both all patients
(n=82205) and patients without prior CVD (n=63166), current smokers had a 30% (95% CI of HR:
1.16, 1.46) and 77% (95% CI of HR: 1.35, 2.31) increased risk of MI compared to never-smokers.
In former smokers, the risk for MI was higher by 21% (95% CI of HR: 1.10, 1.32).
Patients with T2DM have 2- to 5-fold increased risk of stroke compared with those without diabetes
130. The UKPDS
22 and FIELD
131 studies have explored the association of smoking with the risk of
stroke in patients with T2DM. Hankey et al. (2012)131
observed that older patients with a history of
stroke were at the highest risk of stroke. They reported a 52% increased risk of stroke associated
with current smokers (combining patients with/without prior stroke). In this study, with all patients
(n=82205) current smokers had a 26% increased risk of stroke (95% CI of HR: 1.15, 1.38), which
was similar to the risk observed in patients without prior CVD (n=63166). However, among
patients with a history of vascular diseases before the diagnosis of diabetes, smoking was not
associated with any significant increase in the risk of stroke (95% CI of HR: 0.93, 1.16) after
adjusting for various risk factors including age.
Studies have reported that cardiovascular diseases have developed 7 to 10 years later in women
compared to men, and it is important to mention that CVD remain as a major cause of death in
women above 65 years 132
. As a result of misunderstanding that pre-menopausal women are
‘protected’ against cardiovascular disease, the real risk in women is underestimated. Research by

69
Towfighi et al. reported that the prevalence of MI has increased in midlife women aged 35 to 54,
but in men the prevalence has declined 133
. The possible biological mechanisms for women to be at
higher risk of cardiovascular diseases relate to the hormonal, genetic and metabolic differences
between men and women 134
.
Another interesting observation in this analysis is the significantly increased risks of major
cardiovascular events associated with smoking in patients without any CVD prior to their diagnosis
with T2DM (Table 4.2). The comparisons across different smoking categories (current versus
former smokers, current versus never-smokers), based on their prior cardiovascular disease history,
suggest sub-optimal management of diabetes in patients without such an event. It is possible that
the patients in this group, irrespective of smoking category, fail to maintain good compliance with
protective medications.
This study uses a large, longitudinal primary care dataset with median follow-up of 5.4 years to
address the recent controversial issue of gender specific risks associated with CVD and mortality in
patients with or without a cardiovascular event prior to T2DM diagnosis. The conclusions are that
(1) women who are exposed to smoking (current/former smokers versus never-smokers) are at a
higher risk to CVD and mortality than men; (2) in the absence of a CVE prior to T2DM diagnosis in
these patients there remains an increased risk of a CVE and mortality in women compared to men;
(3) patients who smoked (current or former smokers) and had a CVE before their diagnosis with
T2DM also had amplified risks compared to never-smokers, the risk in these patients being slightly
lower than that of the patients without a prior CVE, posssibly due to the effect of cardio protective
medications.

70
Chapter 5. Blood Pressure Trajectories Before Death

71
Trajectory analysis of blood pressure before death in patients with type 2 diabetes
5.1: Background
Hypertension is a commonly occurring comorbid condition in diabetes cases, affecting a significant
proportion of patients. Guidelines for the treatment of hypertension in patients with type 2 diabetes
recommend maintaining a systolic/diastolic blood pressure below 140/80 mmHg 135
. Anti-
hypertensive medications, along with lifestyle modifications, are advised for patients with a blood
pressure above 140/80 mmHg. Exploratory analyses of data taken in the Action in Diabetes and
Vascular Disease: Preterax and Diamicron MR Controlled Evaluation (ADVANCE) trial reported
that additional lowering of blood pressure by 5.6/2.2 mmHg in patients with type 2 diabetes was
associated with 18% and 14% reductions in CVD and all-cause mortality respectively, when
compared with placebo 136
. However, an analysis of Action to Control Cardiovascular Risk in
Diabetes (ACCORD) trial data showed no benefit of tighter blood pressure control in patients with
T2DM 36
. The meta-analysis conducted by McBrien et al.137
reported no significant association
between intensive blood pressure lowering and mortality in patients with T2DM. Similarly, a recent
systematic review conducted by Jicheng et al.138
reported no clear benefit of intensive blood
pressure control on mortality. Further, a retrospective cohort study on about 126,000 newly
diagnosed patients with T2DM reported that a systolic/diastolic blood pressure below 130/80
mmHg during the year following diagnosis with diabetes was not associated with improved survival
139. However, information regarding changes in blood pressure over time and its possible effects on
mortality are very limited.
Only a few studies have examined the blood pressure trajectories of people with diabetes. A post
hoc analysis of UKPDS data reported a significant risk reduction in mortality, by 9-16%, for every
10 mmHg decrement in systolic blood pressure 38
. This study explored the updated mean blood
pressure observed over time, and not changes in blood pressure over time. The VADT study
reported increased risk of cardiovascular events associated with the joint effects of high systolic and
diastolic blood pressure over a period of 7 years 37
. However, two recent studies have suggested that
lowering blood pressure can increase mortality in patients with T2DM 140,141
. In a small cohort of
326 elderly patients (older than 75 years), van Hateren et al.140
reported significant increases (15%
and 22%) in mortality risk for each 10 mmHg decrease in systolic and diastolic blood pressure,
respectively. However, in the cohort of 555 patients aged between 60-75 years, no association
between blood pressure and mortality was observed 140
. Another study, based on a cohort of 3766

72
patients who had had T2DM for 3 years, reported that the rate of decline of blood pressure was
more rapid in those people who died than those who remained alive 141
.
Although analyses from both studies adjusted for various confounding factors, including
medications, the robustness and generalisability of these findings remain weak, primarily because of
the likelihood of selection bias and analytical issues. However, these findings clearly suggest a need
to explore blood pressure trajectories longitudinally at population level, as changes in blood
pressure over time could be significantly associated with a change in the risk of death
12,32,35,36,41,139,142-147. This would have important implications for clinical practice, as it would imply
that a rapid change in blood pressure, whether a consequence of medical treatment or due to
physiological changes, could be a predictor of higher mortality in people with T2DM. In this
analysis, with a large cohort of patients who have had diabetes for at least 3 years, and whose data
are available from the Clinical Practice Research Datalink (CPRD), the aim was to explore blood
pressure trajectories over time and their association with mortality risk.
5.2: Methods
5.2.1: Data
The Clinical Practice Research Datalink (CPRD) is one of the largest proprietary, anonymised
longitudinal data sets derived from United Kingdom primary care. This database contains clinical
information including diagnoses, mortality, laboratory results and prescription data (Chapter 3). The
primary data set for this retrospective cohort study was derived from 84596 individuals aged 18 to
99 who had been newly diagnosed with T2DM between January 1990 and December 2005,
followed until April 2007, and who had been registered with the general practice for at least 12
months.
Clinical and laboratory measures for all individuals were arranged on the basis of 6-monthly
windows, providing 6-monthly longitudinal data during the whole period of follow-up. The cohort
for this study was selected under the following conditions: the patients should have had diabetes for
at least 3 years with no missing anthropometric and clinical measure data at the time of diagnosis,
and complete data was present for the last four 6-monthly (two year period) measurements of both
systolic and diastolic blood pressure immediately before death or censoring. A dataset of 18583
patients satisfying these conditions was used to explore the longitudinal trajectory of blood pressure
during the two years immediately before death or censoring. Patients with a diagnosis of heart

73
failure either prior to their diagnosis with T2DM or during follow-up were excluded to avoid
reverse causality, because patients who have experienced heart failure are very likely to have lower
blood pressure levels than those who have not.
The following information was extracted: age, gender, smoking status (defined as current, former or
never smoker), BMI, blood pressure recordings (systolic and diastolic), HbA1c, history of CVD
before the diagnosis of diabetes, and the recorded clinical events during follow-up, which included
CVD (myocardial infarction, stroke, angina, coronary heart disease, peripheral arterial disease,
angioplasty and coronary artery bypass graft), along with the dates of these events. Detailed
information regarding the use of anti-hypertensive and cardio protective medications (including
ACE inhibitors, beta blockers, statins and other concomitant medications) was obtained from
prescription data, together with dates. Dates of death were derived from modified CPRD death
codes. Specific disease Read codes capture data as part of routine care (including investigations) or
as a result of hospitalisation or emergency care 120,122-124
. Ethics approval for the use of CPRD data
was granted by the Independent Scientific Advisory Committee in June 2014.
5.2.2: Statistical Methods
Summary statistics were presented by number (percentage), mean (SD), or median (IQR), as
appropriate. Calculations of the median (IQR) duration of diabetes were based on the time from
diagnosis of T2DM to the time at which the first of the last four blood pressure measurements were
taken. The average duration of follow-up was calculated from the time of diagnosis of diabetes to
the end of the follow-up period.
To compare the longitudinal trajectory levels of systolic and diastolic blood pressure by mortality
status, generalised estimating equation (GEE) regression models were used with approximately
normally distributed blood pressure measurements and ‘unstructured’ correlation patterns among
the longitudinal measurements 148
. Multivariate GEE models were fitted with adjustments for age,
sex, duration of diabetes, history of CVD, BMI and HbA1c at diagnosis, current CVD events, anti-
hypertensive and cardio protective medications.
To evaluate the effects of changes in systolic and diastolic blood pressure on mortality risk, over
two years, mixed-effects logistic regression models were fitted, with adjustments for the risk factors
described above. Separate models were fitted for all patients and for patients with and without a
history of CVD (except heart failures).

74
Systolic and diastolic blood pressures were categorized into blocks of 10 mmHg and 5 mmHg
respectively, to evaluate the mortality risks associated with different levels of blood pressure over
time. Odds ratios and their bootstrapped 95% confidence intervals were obtained. To evaluate the
interaction effects of age and blood pressure (continuous measures) on mortality risk, interaction
parameters were included in the logistic regression models, and probabilities of death, along with
their 95% confidence intervals, were plotted against blood pressure measurements on a two-
dimensional plane.
5.4: Results
In the cohort of 18583 patients who had four consecutive 6-monthly (2 years) blood pressure
measurements taken in the period before death or censoring, 53% were male, 13% were smokers,
the mean (SD) age was 67 (11) years, 22% (n=4,164) had had at least one cardiovascular event
before their diagnosis of diabetes, and 21.5% (n=3,999) had had at least one cardiovascular event
during the course of 6.8 years of median follow-up. Cardiovascular events included non-fatal MI,
stroke, CHD, PAD, angina, angioplasty and CABG. The mean (SD) age of this cohort at the time of
diagnosis with diabetes was 62 (11) years. Over a median follow-up period of 6.8 years from the
time of diagnosis of diabetes, 1025 (5.5%) patients died (Table 5.1).
Table 5.1: Descriptive statistics of the study cohorts, at the time of diagnosis.
Without Previous
CVD
With Previous
CVD All Patients
N 14419 4164 18583
Age at Diagnosis (years) 61 (12 ) 66 (10) 62 (11)
Male# 7369 (51.1) 2538 (61.0) 9907 (53.3)
Smoking status
Ex-smoking 4896 (34.2) 1815 (43.8) 6711 (36.3)
Current smoking 1786 (12.5) 552 (13.3) 2338 (12.7)
Age < 68#(years) 7431 (51.5) 1446 (34.7) 8877 (47.8)
Age ≥ 68#(years) 6988 (48.5) 2718 (65.3) 9706 (52.2)
Duration of Diabetes (years)$* 4.0 (3.0, 6.5) 4.0 (3.0, 6.5) 4.0 (3.0, 6.5)

75
SBP (mmHg) 139 (16) 139 (17) 139 (16)
<130 mmHg 3177 (22.0) 994 (23.9) 4171 (22.4)
130-140 mmHg 3918 (27.2) 1062 (25.5) 4980 (26.8)
≥140mmHg 7324 (50.8) 2108 (50.6) 9432 (50.8)
DBP (mmHg) 78 (9) 76 (10) 77 (10)
<80 mmHg 7004 (48.6) 2420 (58.1) 9424 (50.7)
80-85 mmHg 4320 (30.0) 1102 (26.5) 5422 (29.2)
≥85 mmHg 3095 (21.5) 642 (15.4) 3737 (20.1)
BMI (kg/m2) 30.5 (6.0) 30.0 (5.7) 30.4 (6.0)
HbA1c (%) 8.0 (2.0) 7.8 (1.9) 7.9 (2.0)
Duration of Follow-up*(years) 6.8 (5.3, 9.4) 6.9 (5.4, 9.6) 6.8 (5.3, 9.4)
Current CVEs
MI 75 (0.5) 599 (14.4) 674 (3.6)
Stroke 318 (2.2) 819 (19.7) 1137 (6.1)
PAD 12 (0.1) 664 (15.9) 676 (3.6)
CHD 915 (6.3) 1137 (27.3) 2052 (11.0)
Angina 1327 (9.2) 657 (15.8) 1984 (10.7)
Angioplasty 102 (0.7) 141 (3.4) 243 (1.3)
CABG 122 (0.8) 187 (4.5) 309 (1.7)
Any cardiovascular event 1724 (12.0) 2275 (54.6) 3999 (21.5)
Current medications
Metformin 10912 (75.7) 2955 (71.0) 13867 (74.6)
Sulphonylurea 7912 (54.9) 2381 (57.2) 10293 (55.4)
Rosiglitazone 2615 (18.1) 581 (14.0) 3196 (17.2)
Pioglitazone 992 (6.9) 242 (5.8) 1234 (6.6)
Any oral anti-diabetes drug 12076 (83.8) 3401 (81.7) 15477 (83.3)
Insulin 2130 (14.8) 754 (18.1) 2884 (15.5)
Statins 11959 (82.9) 3795 (91.1) 15754 (84.8)
ACE/ARB 11324 (78.5) 3588 (86.2) 14912 (80.2)
Betablockers 5443 (37.7) 2630 (63.2) 8073 (43.4)

76
Hypertensive medications 12094 (83.9) 3897 (93.6) 15991 (86.1)
All-Cause Mortality# 694 (4.8) 331 (7.9) 1025 (5.5)
*Median (IQR), #
No. (%), $Measurements at the start of the cohort
Recorded vascular events during the follow-up period, along with a record of medication history,
are presented in Table 5.1. The proportion of patients with a history of previous cardiovascular
event(s) was higher in those who died (32%) compared to those who remained alive (22%). The
proportions for any cardiovascular event(s) during the follow-up were 44% and 20% respectively
for those who died and for those who remained alive. The proportion of patients with both previous
and current cardiovascular events was significantly higher (25%) in those who died compared to
those remained alive (11.5%). Most patients in the cohort (86%) were taking anti-hypertensive
medications (ACE/ARB or beta blocker) for a median (IQR) prescription duration of 5 (3, 6) years.
Blood pressure trajectories are plotted in Figures 5.1 and 5.2, using mean (95% CI) values. Overall,
these 2-year trajectories clearly suggest significantly higher blood pressure levels in those who died
(Table 5.2). Patients who died, on average had significantly higher systolic blood pressures, by 5
mmHg (95% CI: 3-6 mmHg), and diastolic blood pressures, by 1 mmHg (95% CI: 0.1 - 2.1
mmHg), before death, compared to those who remained alive. These estimates were adjusted for
various factors, as described in the methods section. Male patients had consistently lower systolic
blood pressures during the two year period, compared with females – by 1 mmHg (p < 0.01) on
average. However, male patients had marginally higher diastolic blood pressure trajectories during
the follow-up period. Age and duration of diabetes were statistically significant contributing factors
to higher systolic blood pressure trajectories.
Table 5.2: The effects of risk factors on longitudinal measures of blood pressure over the two
year period immediately before death or censoring
Variable
Regression Coefficient
(95% CI) P-value
SBP
Dead vs. Alive 4.4 (2.5, 6.3) <0.01
Age(years)* 0.23(0.20, 0.26) <0.01
Duration of Diabetes 0.18 (0.04, 0.31) <0.01
Male -0.70 (-1.2,-0.12) 0.01
Baseline BMI 0.10 (0.05, 0.15) <0.01

77
Baseline HbA1c 0.30 (0.12, 0.41) <0.01
Hypertensive Medications 5.7 (4.9, 6.5) <0.01
Cardio protective medications -1.00 (-2.75, 0.75) 0.26
CVD prior to diagnosis -2.4 (-3.35, -1.50) <0.01
CVD during follow-up -1.9 (-3.0, -0.76) <0.01
CVD in both prior and during
follow-up -1.8 (-2.79, -0.71) <0.01
DBP
Dead vs. Alive 1.1 (0.11, 2.1) 0.03
Age(years)* -0.19 (-0.20, -0.17) <0.01
Duration of Diabetes -0.14 (-0.22, -0.07) <0.01
Male 0.76 (0.42, 1.10) <0.01
Baseline BMI 0.15 (0.12, 0.18) <0.01
Baseline HbA1c 0.04 (-0.04, 0.13) 0.31
Hypertensive Medications -1.28 (0.80, 1.75) <0.01
Cardio protective medications -0.27 (-1.40, 0.85) 0.63
CVD prior to diagnosis -1.31 (-1.83, 0.78) <0.01
CVD during follow-up -1.31 (-2.01, -0.60) <0.01
CVD in both prior and during
follow-up -2.19 (-2.80, -1.58) <0.01
*at start of the study; GEE model: SBPit or DBPit ~ Agei + Sexi + Duration of Diabetes i + Baseline
BMI + Baseline HbA1c + Anti-hypertensive Medications + Cardio protective medications+ CVD
status+ Eventi; i for subject, t for time

78
Figure 5.1: Mean (95% CI) of longitudinal measures of systolic blood pressure during the two
year period prior to death or censoring
Figure 5.2: Mean (95% CI) of longitudinal measures of diastolic blood pressure during the
two year period prior to death or censoring

79
Patients taking anti-hypertensive medications had significantly higher systolic blood pressures – by
about 6 mmHg during the two year period before death or censoring – but no clinically meaningful
difference was observed in diastolic levels. Patients with a systolic/diastolic blood pressure
consistently above 130/80 mmHg for the two years before the event had a significantly increased
mortality risk – by 52% (odds ratio: 1.52; 95% CI: 1.25, 1.84) and 95% (odds ratio: 1.95; 95% CI:
1.76, 2.16) in younger and older patients, respectively.
Systolic blood pressure during the two year period immediately before death or censoring was
higher by 2 mmHg (p < 0.01) in those who experienced at least one stroke during the follow-up.
The proportions of patients with a prior or current history of non-fatal stroke in the cohort were 5%
(n=850) and 6% (n=1337), respectively. Of the patients who had a prior history of stroke, 86%
experienced at least one event of stroke during the follow-up.
Adjusting for risk factors, including blood pressure, patients who experienced at least one non-fatal
stroke (6%, n=1137) and non-fatal MI (4%, n=674) during the follow-up period had three-fold
(odds ratio: 2.7, CI: 2.2, 3.2) and four-fold (odds ratio: 4.1, CI: 3.3, 5.1) increased mortality risks,
respectively.
Compared to patients with a systolic blood pressure between 130-139 mmHg during the two year
period immediately before death or censoring, patients with higher systolic blood pressures had a
significantly higher mortality risk (Table 5.3). This higher mortality risk pattern was similar for
patients with and without a history of CVD. Overall, patients with a systolic blood pressure below
110 mmHg had a 56% increased mortality risk.

80
Tab
le 5
.3:
Od
ds
rati
os
(95%
CI)
for
mo
rtali
ty a
ssoci
ate
d w
ith
dif
fere
nt
blo
od
pre
ssu
re c
ate
gori
es, co
mp
are
d t
o r
efer
ence
cate
gori
es o
f 130-1
39
mm
Hg a
nd
80
-84 m
mH
g f
or
syst
oli
c an
d d
iast
oli
c b
lood
pre
ssu
res.
Est
ima
tes
are
sep
ara
tely
provid
ed f
or
ad
just
ed a
nd
un
ivari
ate
(un
ad
just
ed)
mod
els.
W
ith
ou
t C
VD
W
ith
CV
D
All
Pati
ents
O
R (
95%
CI)
P
-valu
e O
R (
95%
CI)
P
-va
lue
OR
(9
5%
CI)
P
-va
lue
Syst
oli
c b
loo
d p
ress
ure
(m
mH
g)
Mo
del
1 (
un
adju
sted
)*
SB
P c
ateg
ory
<110 m
mH
g
1.6
4 (
1.1
5,
2.3
4)
0.0
07
1.5
1 (
0.9
6,
2.3
8)
0.0
7
1.6
7 (
1.2
7,
2.2
1)
< 0
.01
110-1
19 m
mH
g
1.0
0 (
0.8
0,
1.2
5)
0.9
8
0.9
5 (
0.7
0,
1.2
8)
0.7
4
1.0
2 (
0.8
5,
1.2
1)
0.8
5
120-1
29 m
mH
g
1.0
1 (
0.8
6,
1.1
8)
0.9
2
0.8
5 (
0.6
6,
1.0
8)
0.1
8
0.9
7 (
0.8
5,
1.1
0)
0.6
0
130-1
39 m
mH
g
1.0
0
–––
1.0
0
––
–
1.0
0
––
–
140-1
49 m
mH
g
1.4
5 (
1.2
8,
1.6
4)
< 0
.01
1.3
8 (
1.1
5,
1.6
6)
0.0
01
1.4
4 (
1.2
9,
1.5
9)
< 0
.01
150-1
59 m
mH
g
2.4
1 (
2.0
7,
2.8
2)
< 0
.01
2.1
5 (
1.7
0,
2.7
2)
<0
.01
2.3
5 (
2.0
6,
2.6
7)
< 0
.01
≥160 m
mH
g
4.3
5 (
3.7
0,
5.1
0)
< 0
.01
3.3
0 (
2.6
2,
4.1
7)
<0
.01
4.0
6 (
3.5
6,
4.6
3)
< 0
.01
Mo
del
2 (
adju
sted
)*
SB
P c
ateg
ory
<110 m
mH
g
1.6
2 (
1.1
2,
2.3
5)
0.0
1
1.4
7 (
0.9
2,
2.3
5)
0.1
0
1.5
6 (
1.1
7,
2.0
9)
0.0
03

81
110-1
19 m
mH
g
1.0
2 (
0.8
1,
1.2
8)
0.8
9
0.9
6 (
0.7
0,
1.3
2)
0.8
1
1.0
0 (
0.8
3,
1.2
0)
0.9
8
120-1
29 m
mH
g
0.9
9 (
0.8
5,
1.1
7)
0.9
3
0.8
4 (
0.6
6,
1.0
8)
0.1
8
0.9
4 (
0.8
2,
1.0
7)
0.3
6
130-1
39 m
mH
g
1.0
0
–––
1.0
0
––
–
1.0
0
––
–
140-1
49 m
mH
g
1.3
6 (
1.2
0,
1.5
5)
< 0
.01
1.3
0 (
1.0
7,
1.5
7)
0.0
07
1.3
4 (
1.2
1,
1.4
9)
< 0
.01
150-1
59 m
mH
g
2.2
3 (
1.9
0,
2.6
3)
< 0
.01
1.9
9 (
1.5
7,
2.5
2)
< 0
.01
2.1
6 (
1.8
9,
2.4
7)
< 0
.01
≥160 m
mH
g
3.7
1 (
3.1
3,
4.3
9)
< 0
.01
3.0
2 (
2.3
8,
3.8
3)
< 0
.01
3.4
8 (
3.0
3,
4.0
0)
< 0
.01
Dia
sto
lic
blo
od
pre
ssure
(m
mH
g)
Mo
del
1 (
un
adju
sted
)*
DB
P c
ateg
ory
<70 m
mH
g
0.9
4 (
0.8
0,
1.1
0)
0.4
3
0.6
8 (
0.5
4,
0.8
4)
< 0
.01
0.8
9 (
0.7
8,
1.0
1)
0.0
6
70-7
4 m
mH
g
0.9
3 (
0.8
2,
1.0
6)
0.2
6
0.6
8 (
0.5
6,
0.8
2)
< 0
.01
0.8
6 (
0.7
8,
0.9
6)
0.0
07
75-7
9 m
mH
g
0.6
2 (
0.5
3,
0.7
2)
< 0
.01
0.6
8 (
0.5
5,
0.8
4)
< 0
.01
0.6
5 (
0.5
8,
0.7
3)
< 0
.01
80-8
4 m
mH
g
1.0
0
–––
1.0
0
––
–
1.0
0
––
–
85-8
9 m
mH
g
0.8
4 (
0.7
1,
0.9
9)
0.0
33
1.0
4 (
0.8
2,
1.3
3)
0.7
2
0.8
8 (
0.7
7,
1.0
0)
0.0
5
90-9
4 m
mH
g
1.5
2 (
1.2
9,
1.7
9)
< 0
.01
1.4
5 (
1.1
1,
1.8
9)
0.0
06
1.4
7 (
1.2
8,
1.6
9)
< 0
.01
≥95 m
mH
g
1.6
6 (
1.3
2,
2.0
9)
< 0
.01
1.7
5 (
1.2
3,
2.5
0)
0.0
02
1.6
4 (
1.3
5,
1.9
9)
< 0
.01
Mo
del
2 (
adju
sted
)*
DB
P c
ateg
ory
<70 m
mH
g
0.6
1 (
0.5
1,
0.7
2)
< 0
.01
0.5
7 (
0.4
6,
0.7
2)
< 0
.01
0.5
9 (
0.5
2,
0.6
8)
< 0
.01
70-7
4 m
mH
g
0.7
3 (
0.6
4,
0.8
3)
< 0
.01
0.6
3 (
0.5
2,
0.7
7)
< 0
.01
0.7
0 (
0.6
3,
0.7
8)
< 0
.01

82
75-7
9 m
mH
g
0.5
7 (
0.4
9,
0.6
6)
< 0
.01
0.7
0 (
0.5
7,
0.8
6)
0.0
01
0.6
1 (
0.5
4,
0.6
9)
< 0
.01
80-8
4 m
mH
g
1.0
0
–––
1.0
0
––
–
1.0
0
––
–
85-8
9 m
mH
g
0.9
7 (
0.8
1,
1.1
4)
0.6
8
1.1
5 (
0.9
0,
1.4
8)
0.2
7
1.0
2 (
0.8
9,
1.1
7)
0.7
7
90-9
4 m
mH
g
1.7
6 (
1.4
8,
2.0
8)
< 0
.01
1.6
2 (
1.2
3,
2.1
2)
< 0
.01
1.7
2 (
1.4
9,
1.9
9)
< 0
.01
≥95 m
mH
g
2.0
1 (
1.5
8,
2.5
5)
< 0
.01
2.2
0 (
1.5
4,
3.1
3)
< 0
.01
2.0
8 (
1.7
1,
2.5
4)
< 0
.01

83
5.5: Discussion and Conclusions
This population-based analysis of blood pressure trajectories prior to death provides new
information on the dynamics of blood pressure in patients with T2DM with median (IQR) duration
of 4.0 (3.0 - 6.5) years. Both systolic and diastolic blood pressure trajectories were higher for the
two year period before death. In patients who died, the adjusted systolic blood pressure trajectories
were higher, by 7 mmHg (95% CI: 6-8 mmHg) and 6 mmHg (95% CI: 4-8 mmHg), in age groups
above and below 68 years, respectively. In older patients who died, diastolic blood pressure
trajectories were higher, on average by 3 mmHg (95% CI: 2-3.3 mmHg), compared to those who
remained alive. For patients younger than 68 years, there was a significant difference in the
diastolic blood pressure trajectories between those who died and those who were alive, by 1 mmHg,
although this may not be a clinically important difference. While several studies have reported a fall
in diastolic blood pressure with aging149-151
, these studies did not model the dynamics of this inverse
relationship longitudinally in relation to the mortality risk of patients with T2DM.
Significantly increased mortality rates were observed in patients experiencing one or more
cardiovascular events. Among those who died, 13%, 17% and 44% had experienced at least one MI,
stroke, and any cardiovascular event, respectively, during the follow-up period. Several studies,
including the ACCORD trial and the recent meta-analysis by McBrien et al. (2012), have reported a
reduced risk of stroke at lower systolic blood pressure levels 12,36,137
. McBrien et al. (2012) reported
a significant 35% risk reduction (relative risk: 0.65; 95% CI: 0.48 – 0.86) for stroke in patients
treated with an intensive blood pressure lowering strategy (systolic/diastolic: 130/80 mmHg)
compared to treatment with standard blood pressure targets (systolic/diastolic: 140-160 / 85-100
mmHg). In this analysis, older patients with systolic/diastolic blood pressures above 130/80 mmHg
and above 140/80 mmHg respectively had 12% (95% CI of odds ratio: 1.02 - 1.22; p=0.019) and
14% (95% CI of odds ratio: 1.04 - 1.26; p=0.007) significantly increased risks of stroke. However,
systolic and diastolic blood pressures were not significantly associated with stroke in patients under
68 years.
Rogers et al. (2011) reported a significantly higher decline in mean systolic blood pressure, by 3.2
mmHg/year, in T2DM patients who died, compared to a decline of 0.7 mmHg/year in those who
were alive 141
. In the present study, using a more comprehensive data set and complete consecutive
blood pressure measurements available for the duration of the year immediately before death or
censoring, no clinically significant decline in blood pressure was observed before death.

84
Key strengths of this analysis include a large cohort of individuals with T2DM from routine clinical
practice with a median follow-up of about 7 years, complete (non-missing) longitudinal blood
pressure data, detailed information regarding medications and cardiovascular events, and a focus on
mortality. With consecutive 6-monthly longitudinal data on systolic and diastolic blood pressure
immediately before death or censoring, for more than 18583 patients over a 2 year period, and a
5.5% death rate, the study had sufficient statistical power to make robust inferences about the
trajectory levels of blood pressure by mortality. Further, information was available on the duration
of treatment with anti-hypertensive and other cardio protective medications, as well as the
occurrence and timing of cardiovascular events; these were useful in generating robust conclusions.
To reduce possible selection bias, patients who had had diabetes for a minimum of 3 years were
chosen for the analysis. The use of sophisticated modelling techniques, to account for time-varying
measurements of risk factors, added further strength to the robustness of the estimates obtained in
this analysis. Analytical approaches allowed for dynamic clinical data with skewness and high
longitudinal variability.
The limitations of this study include the non-availability of (1) data on heart rate; (2) data on
adherence to medications, during the follow-up period; and (3) data on ethnicity. In addition,
adherence to the study protocol for collecting biomedical and anthropometric measurements was
inconsistent. However, these issues are unlikely to affect the robustness of the results of this study
due to the large sample size, and the alignment of longitudinal data in time-windows.
In conclusion, the population level analyses of blood pressure trajectories leading up to death
provide clear messages for intensive blood pressure control and related management policies in
primary care. The findings suggest that people with T2DM who died have a more rapid decline in
blood pressure in the period before death than people who remained alive, but this decline was not
clinically significant. Increased mortality risks were observed with both higher and lower levels of
SBP and DBP. Patients are reviewed at least annually in primary care and these findings provide
further support for continued monitoring and blood pressure in people with T2DM to be tightly
controlled. These findings should be considered in future iterations of clinical practice guidelines.

85
Chapter 6. Obesity Paradox in Type 2 Diabetes Mellitus
This chapter was published as “Thomas G, Khunti K, Curcin V, et al. Obesity paradox in people
newly diagnosed with type 2 diabetes with and without prior cardiovascular disease. Diabetes,
obesity & metabolism 2014;16:317-25”

86
Obesity Paradox in People Newly Diagnosed With Type 2 Diabetes With and Without
Prior Cardiovascular Disease
6.1: Background
Type 2 diabetes mellitus is a metabolic disease which accounts for over 90% of people with
diabetes 19,54
. Although the majority of these patients may belong to the obese category70
based on
their body weight, recent studies have raised the issue of “obesity paradox” in patients with T2DM
71,72. Carnethon et al. (2012)
72, in a recent study reported increased mortality in adult patients with
normal body weight at the time of diagnosis of diabetes. Using pooled data from five studies
(n=2625), the study reported that patients with normal body weight (BMI < 25 kg/m2
) at the time of
diagnosis of T2DM had 52% significantly increased risk of cardiovascular death and two-fold
increased risk of all-cause mortality, compared to overweight (BMI ≥ 25 kg/m2
and < 30 kg/m2) or
obese (BMI ≥ 30 kg/m2) patients
72. Although this study looked at some of the relevant risk factors
while evaluating the risks in normal weight patients compared to overweight or obese, the study did
not account for the possible interactions between the cardiovascular and glycaemic risk factors. In
addition, due to the relatively small sample size, the robustness of the inferences is weak and hence
the generalisation of the findings warrants further explorations.
Lague et al. (2013)152
, using a large Scottish cohort evaluated the association of BMI within one
year of diagnosis of T2DM with the risk of cause-specific mortality, separately for men and women.
Using BMI 25 to < 30 kg/m2 as a reference group, they reported 22% and 32% increased mortality
risk in men and women respectively with BMI ranging between 20 to 25 kg/m2. Although the study
excluded death within two years of diagnosis of T2DM, the differential risks among patients with
and without the history of cardiovascular diseases were not evaluated.
Two other studies, Translating Research Into Action for Diabetes (TRIAD)153
and the PROactive
study154
, reported increased mortality risk in established T2DM patients who were normal weight at
the start of the study or lost weight during the follow-up. Although the “obesity paradox” is well
studied in some other diseases including chronic kidney disease155-159
, little is known about the
association of normal body weight at the diagnosis of diabetes with cardiovascular risk and
mortality.

87
Nevertheless, these studies have made important contributions to encourage research to explore the
“obesity paradox” in patients with T2DM. Separately for patients with and without history of
cardiovascular diseases before the diagnosis of T2DM, the aims of our study were:
1. to explore the rates of cardiovascular events (CVE) and all-cause mortality in a large cohort
of newly diagnosed people with T2DM among different BMI categories;
2. to evaluate the risks of cardiovascular disease and mortality in normal weight and
overweight patients compared to obese patients with adjustments for relevant risk factors;
and to
3. evaluate the possible interactions of age, body weight and glycaemic level (measured by
HbA1c) on cardiovascular risks and all-cause mortality.
6.2: Research Design and Methods
6.2.1: Data
The General Practice Research Database (GPRD) is a large proprietary, anonymised longitudinal
data sets derived from United Kingdom primary care. The GPRD contains clinical information
including diagnoses, mortality, laboratory results and prescription data 119,120
. The primary data set
for this retrospective cohort study includes data from 84596 individuals aged 18 to 90 years with a
new diagnosis of T2DM between January 1990 and April 2007, who had been registered with their
general practice for at least 12 months 121
. Rigorous classificaction techniques were used to ensure
correct identification of patients with T2DM 121,123
. The following information was extracted: age,
gender, smoking status (defined as current, ex or never smoker), BMI, blood pressure recordings
(systolic and diastolic), HbA1c, lipid measures, history of cardiovascular diseases before the
diagnosis of diabetes and the recorded clinical events during follow-up included cardiovascular
diseases (myocardial infarction, stroke, heart failure, angina, coronary heart disease, peripheral
arterial disease, angioplasty and coronary artery bypass graft), diabetic neuropathy, renal
complications along with dates of events. The date of death was derived from modified GPRD
death codes. Specific disease Read codes capture data as part of routine care (including
investigations) or as a result of hospitalisation or emergency care 120,122-124
.
A cohort of 47509 patients with newly diagnosed T2DM was selected for this study, who had
complete information on age, sex, smoking status, deprivation score based on the Index of Multiple
Deprivation160,161
, BMI, HbA1c, blood pressure, and clinical (event) history before diagnosis and

88
during the follow-up. Only patients with BMI of 19 Kg/m2 or more were included. To eliminate the
bias due to possible latent illness, we chose patients who did not experience any cardiovascular
event or did not die within 2 years of diagnosis of diabetes. Of the cohort of 47509 patients, the
number of patients with and without the history of cardiovascular diseases before diagnosis were
10237 and 37272 respectively.
6.2.2: Statistical methods
The summary statistics were presented by number (percentage), mean (SD), or median (IQR), as
appropriate. The median duration of follow-up was calculated from the time of diagnosis of
diabetes to the end of the follow-up. Non-parametric Kruskal-Wallis test or the Chi-square test were
used to compare different study parameters across the BMI categories. The death rates and their
95% confidence intervals per 1000 person-years under different BMI categories were calculated
using standard life-table analysis technique.
To explore the association of BMI at diagnosis with the risk of CVE and all-cause mortality during
follow-up, two different stratified Cox regression models were fitted: (1) simple model, adjusted for
age, sex, smoking status, SBP, DBP, HbA1c and BMI categories; (2) extended model included
LDL, HDL and triglyceride measures at diagnosis, apart from the variables included in the simple
model. Stratified Cox regression model with “deprivation score” as the stratification factor was used
because of the failure of the “proportionality assumption” associated with the covariates in the Cox
regression models. The deprivation score identify the most deprived areas across the United
Kingdom. It combines a number of indicators, chosen to cover a range of economic, social and
housing issues, into a single deprivation score for each small area in the country. The indices are
used widely to analyse patterns of deprivation. Additional analyses were conducted by matching
age at diagnosis by BMI categories using the Censored Exact Matching method (a generalisation of
Propensity Score method) 162
. The bootstrapped and robust estimates of the confidence intervals of
hazard ratios were obtained, and the quality of model fits were assessed using the Bayesian
Information Criteria (BIC).
Age and HbA1c were categorised at their median levels. The categories of BMI were defined as
“normal weight” (BMI> 18.5 kg/m2 & < 25 kg/m
2), ‘overweight’ (BMI ≥ 25 & < 30 kg/m
2) and
‘obese’ (BMI ≥ 30 kg/m2).

89
6.3: Results
In the cohort of 37272 patients without prior CVD (Cohort 1), 53% were male, 17% current
smokers, mean (SD) age was 60 (13) years with 49% (n=18298) aged > 60 years (median age),
BMI 30.8 (6.3) kg/m2 and HbA1c 7.9 (2.0)%. The proportions of patients in normal, overweight
and obese categies were 15%, 36% and 49% respectively (Table 6.1). Younger patients (aged ≤ 60
years) had higher BMI levels (mean BMI: 32.3 kg/m2) compared to the patients aged > 60 years
(mean BMI: 29.1 kg/m2) (Figure 6.1). The distributions of all anthropometric, clinical and
laboratory measures were significantly different across the BMI categories (Table 6.1).
Table 6.1: Basic characteristics of study cohort by BMI Categories for patients without prior
CVD
BMI Categories (kg/m2)
<25 ≥25 & <30 ≥30 All
n (%) 5720 (15.3) 13347 (35.8) 18205 (48.8) 37272
Age (Years)* 64 (13) 62 (12) 57 (12) 60 (13)
Age > 60# 3658 (64.0) 7603 (57.0) 7037 (38.7) 18298 (49.1)
Men# 2968 (51.9) 8041 (60.2) 8735 (48.0) 19744 (53.0)
Current smokers# 1026 (18.2) 1954 (14.8) 3108 (17.2) 6088 (16.5)
Previous smokers# 1509 (26.7) 4453 (33.8) 5832 (32.4) 11794 (32.0)
BMI(Kg/m2)* 22.8 (1.8) 27.5 (1.4) 35.6 (5.3) 30.8 (6.3)
Deprivation Score** 18.2 (9.9, 30.9) 17.8 (9.7, 30.9) 18.4 (10.5, 33.5) 18.2 (10.2, 32.7)
SBP (mmHg)* 138 (20) 140 (18) 141 (18) 140 (18)
DBP (mmHg)* 78 (10) 81 (10) 83 (10) 81 (10)
HbA1c (%)* 8.1 (2.3) 7.9 (2.0) 7.9 (1.9) 7.9 (2.0)
HbA1c ≥7·5# 4131 (72.2) 9425 (70.6) 12784 (70.2) 26340 (70.7)
LDL (mmol/L)* 2.9 (1.0) 3.0 (1.0) 3.0 (1.0) 3.0 (1.0)
HDL (mmol/L)* 1.3 (0.4) 1.2 (0.3) 1.2 (0.4) 1.2 (0.4)
Triglyceride
(mmol/L) **
1.5 (1.0, 2.1) 1.8 (1.3, 2.6) 2.0 (1.4, 2.8) 1.8 (1.3, 2.6)
# n(%) * mean (SD) ** median (first quartile, third quartile)

90
In the cohort of 10237 patients with prior cardiovascular disease (Cohort 2), 61% were male, 15%
current smokers, mean (SD) age was 67 (10) years with 46% (n=4725) aged > 68 years (median
age), BMI 30.1 (5.7) kg/m2 and HbA1c 7.7 (1.9)%. The proportions of patients in normal,
overweight and obese categies were 16%, 39% and 45% respectively (Table 6.2, p<0.01). Younger
patients (aged ≤ 68 years) had higher BMI levels (mean BMI: 31.3 kg/m2) compared to the
compared to the patients aged > 68 years (mean BMI: 28.6 kg/m2) (Figure 6.1).

91
Fig
ure
6.1
: D
ensi
ty p
lots
of
BM
I fo
r d
iffe
ren
t age
gro
up
s fo
r (A
) co
hort
wit
hou
t p
rior
CV
D a
nd
(B
) co
hort
wit
h p
rior
CV
D

92
Table 6.2: Basic characteristics of study cohort by BMI Categories for patients with prior
CVD
BMI Categories (kg/m2)
<25 ≥25 & <30 ≥30 All
n (%) 1623 (15.9) 4005 (39.1) 4609 (45.0) 10237
Age (yrs)* 71 (9) 68 (10) 64 (10) 67 (10)
Age > 68# 1058 (65.2) 2024 (50.5) 1643 (35.6) 4725 (46.2)
Men# 895 (55.1) 2674 (66.8) 2638 (57.2) 6207 (60.6)
Current smokers# 271 (16.9) 584 (14.6) 657 (14.3) 1,512 (14.8)
Previous smokers# 593 (36.9) 1783 (44.7) 2075 (45.2) 4451 (43.7)
BMI(Kg/m2)* 22.9 (1.7) 27.5 (1.4) 34.8 (4.7) 30.1 (5.7)
Deprivation Score** 20.1 (10.2, 33.9) 20.1 (10.7, 35.0) 21.6 (11.6, 37.1) 20.7 (11.1, 35.0)
SBP (mmHg)* 141 (21) 140 (19) 141 (19) 141 (19)
DBP (mmHg)* 77 (11) 78 (10) 80 (11) 79 (11)
HbA1c (%)* 7.6 (2.0) 7.7 (1.9) 7.7 (1.8) 7.7 (1.9)
HbA1c ≥7·5# 1092 (67.3) 2734 (68.3) 3169 (68.8) 6995 (68.3)
LDL (mmol/L)* 2.6 (1.0) 2.6 (1.0) 2.6 (1.0) 2.6 (1.0)
HDL (mmol/L)* 1.3 (0.4) 1.2 (0.3) 1.2 (0.5) 1.2 (0.4)
Triglyceride
(mmol/L) **
1.5 (1.1, 2.1) 1.8 (1.3, 2.5) 2.0 (1.4, 2.7) 1.8 (1.3, 2.6)
# n(%) * mean (SD) ** median (first quartile, third quartile)
The median duration of follow-up was 5 and 5.6 years in Cohort 1 and Cohort 2 respective, and was
similar across all BMI categories within individual cohort. In Cohort 1, 4.7% died of whom 82%
were aged > 60 years (Table 6.3). The proportions of death in normal weight, overweight and obese
patients were 8.1%, 5.1% and 3.4% respectively. The overall death rate was significantly higher
among patients with normal weight (13.1/1000 person years) compared to higher BMI categories in
this Cohort. Older patients (> 60 years) had all most 5-fold higher death rate compared to the
younger patients, consistently over all BMI categories. During median 5 years of follow-up, 7.2%
patients experienced atleast one CVE, and older patinets had significantly higher risk of CVE across
all BMI categories (Table 6.3). Patients with BMI below 30 kg/m2 experienced significantly higher
CVE (8%) compared to the obese patients (6.3%).

93
Table 6.3: Proportions and rates of events by BMI Categories for patients without prior CVD
BMI Categories (kg/m2)
<25 ≥25 & < 30 ≥30 All
Follow-up
duration (yrs)**
5.2 (3.5, 7.8) 5.1 (3.5, 7.6) 4.9 (3.4, 7.0) 5.0 (3.4, 7.3)
Current CVD#
Overall 463 (8.1) 1,070 (8.0) 1,146 (6.3) 2,679 (7.2)
Age ≤ 60 106 (5.1) 327 (5.7) 548 (4.9) 981 (5.2)
Age > 60 357 (9.8) 743 (9.8) 598 (8.5) 1,698 (9.3)
Death#
Overall 462 (8.1) 683 (5.1) 617 (3.4) 1762 (4.7)
Age ≤ 60 55 (2.7) 101 (1.8) 163 (1.5) 319 (1.7)
Age > 60 407 (11.1) 582 (7.7) 454 (6.5) 1,443 (7.9)
Death rate (95% CI) /1000 person years
Overall 13.1 (12.0, 14.4) 8.6 (7.9, 9.2) 6.0 (5.5, 6.5) 8.1 (7.7, 8.5)
Age ≤ 60 4.1 (3.1, 5.3) 2.8 (2.3, 3.4) 2.5 (2.2, 3.0) 2.8 (2.5, 3.1)
Age > 60 18.7 (17.0, 20.6) 13.2 (12.2, 14.3) 11.8 (10.7, 12.9) 13.8 (13.1, 14.6)
# n(%) ** median (first quartile, third quartile)
Among patients in Cohort 2, 12.8% died of whom 58% were aged over 68 years (Table 6.4). The
proportions of death in normal weight, overweight and obese patients were 20%, 13.7% and 9.5%
respectively. The overall death rate was significantly higher among patients with normal BMI
(30.1/1000 person years) compared to higher BMI categories in this Cohort. Older patients (> 68
years) had more than 2-fold higher death rate compared to the younger patients, consistently over
all BMI categories. During median 5.6 years of follow-up, 52% patients experienced atleast one
CVE, and normal weight patients had significantly higher incidence of CVE (59.3%) compared to
the overweight (52.8%) and obese patients (48.8%). The CVE proportions were similar between
younger and older patients across all BMI categories.

94
Table 6.4: Proportions and rates of events by BMI Categories for patients with prior CVD
BMI Categories (kg/m2)
<25 ≥25 & < 30 ≥30 All
Follow-up duration
(yr)**
5.8 (3.8, 8.4) 5.7 (3.8, 8.2) 5.3 (3.7, 7.7) 5.6 (3.7, 8.0)
Current CVD#
Overall 963 (59.3) 2115 (52.8) 2248 (48.8) 5326 (52.0)
Age ≤ 68 347 (61.4) 1068 (53.9) 1425 (48.0) 2840 (51.5)
Age > 68 616 (58.2) 1047 (51.7) 823 (50.1) 2486 (52.6)
Death#
Overall 324 (20.0) 548 (13.7) 436 (9.5) 1308 (12.8)
Age ≤ 68 70 (12.4) 175 (8.8) 207 (7.0) 452 (8.2)
Age > 68 254 (24.0) 373 (18.4) 229 (13.9) 856 (18.1)
Death rate (95% CI) /1000 person years
Overall 30.1 (27.0, 33.6) 21.1 (19.4, 22.9) 15.4 (14.0, 16.9) 20.1 (19.0, 21.2)
Age ≤ 68 16.3 (12.9, 20.6) 12.5 (10.8, 14.5) 10.9 (9.5, 12.5) 12.1 (11.0, 13.3)
Age > 68 39.2 (34.7, 44.3) 31.3 (28.3, 34.6) 24.5 (21.5, 27.8) 30.8 (28.8, 33.0)
# n(%) ** median (first quartile, third quartile)
Compared to patients with BMI > 30 kg/m2, normal weight patients had 47% (95% CI of HR: 1.29,
1.69) and 30% (95% CI of HR: 1.11, 1.53) significantly higher mortality risk among patients in
Cohort 1 and Cohort 2 respectively (Table 6.5 and Table 6.6). In Cohort 1, the increased mortality
risk among the normal weight patients were similar between patients below and above the age of 60
years (Table 6.5). However in Cohort 2, significant association of normal body weight (compared to
obese patients) with mortality was observed only among older patients (95% CI of HR: 1.22, 1.82,
p<0.001). The risk estimates for mortality associated with normal weight and over-weight patients
were also similar for the age-matched cohorts. No increased CVE risk was observed in normal and
overweight categories among patients in Cohort 1. However in Cohort 2, patients with BMI < 25
kg/m2 had 13% higher risk of CVE (95% CI of HR: 1.03, 1.23, p=0.007) compared to the obese
patients (Table 6.6).

95
Tab
le 6
.5:
Est
imate
s of
haza
rd r
ati
os
an
d t
hei
r 95%
con
fid
ence
in
terv
als
for
mort
ali
ty a
nd
card
iovasc
ula
r ev
ents
fro
m m
ult
ivari
ate
str
ati
fied
Cox r
egres
sion
mod
els
wit
h o
bes
e ca
tegory
(B
MI≥
30 k
g/m
2)
as
refe
ren
ce, fo
r p
ati
ents
wit
hou
t p
rior
CV
D a
nd
by a
ge
cate
gori
es. T
he
BM
I u
nit
is k
g/m
2.
M
ort
ali
ty
A
ge≤
60
A
ge>
60
Ov
era
ll
H
R (
95%
CI)
P
-Valu
e H
R (
95%
CI)
P
-Valu
e H
R (
95
% C
I)
P-V
alu
e
Age
> 6
0
4.7
1 (
4.0
9,
5.4
2)
<0
.00
1
Men
vs
Wom
en
1.0
1 (
0.7
7,
1.3
1)
0.9
5
1.2
4 (
1.1
, 1.3
9)
<0.0
01
1.2
(1
.08
, 1
.33)
0.0
01
Ex
-Sm
oker
s*
1.4
3 (
1.0
6,
1.9
3)
0.0
2
1.1
1 (
0.9
7,
1.2
6)
0.1
25
1.1
7 (
1.0
4,
1.3
2)
0.0
09
Curr
ent
Sm
oker
s*
1.5
6 (
1.1
4,
2.1
4)
0.0
06
1.4
8 (
1.2
5,
1.7
5)
<0.0
01
1.5
2 (
1.3
1,
1.7
6)
<0
.00
1
SB
P (
mm
Hg)
1.0
2 (
1.0
1,
1.0
3)
<0.0
01
1.0
1 (
1.0
1,
1.0
1)
<0.0
01
1.0
1 (
1.0
1,
1.0
1)
<0
.00
1
DB
P (
mm
Hg)
0.9
8 (
0.9
6,
0.9
9)
0.0
05
0.9
8 (
0.9
8,
0.9
9)
<0.0
01
0.9
8 (
0.9
8,
0.9
9)
<0
.00
1
HbA
1c
≥7·5
%**
1
.13 (
0.8
2,
1.5
5)
0.4
71
1.2
1 (
1.0
5,
1.3
9)
0.0
07
1.2
(1
.06
, 1
.36)
0.0
05
BM
I<25
1.5
(1.0
4,
2.1
6)
0.0
29
1.4
6 (
1.2
6,
1.7
) <
0.0
01
1.4
7 (
1.2
9,
1.6
9)
<0
.00
1
BM
I 25 t
o <
30
1
.23 (
0.9
3,
1.6
2)
0.1
5
1 (
0.8
8, 1.1
4)
0.9
89
1.0
4 (
0.9
2,
1.1
7)
0.5
72
BM
I ≥
30
refe
rence

96
C
ard
iovasc
ula
r E
ven
ts
H
R (
95%
CI)
P
-Valu
e H
R (
95%
CI)
P
-Valu
e H
R (
95
% C
I)
P V
alu
e
Age
≥ 6
0
- -
- -
1.9
7 (
1.7
9,
2.1
6)
<0
.00
1
Men
vs
Wom
en
1.3
1 (
1.1
3,
1.5
1)
<0.0
01
1.1
3 (
1.0
2,
1.2
6)
0.0
25
1.1
6 (
1.0
7,
1.2
7)
0.0
01
Ex
-Sm
oker
s*
1.4
3 (
1.2
1,
1.6
9)
<0.0
01
1.1
6 (
1.0
3,
1.3
1)
0.0
13
1.2
4 (
1.1
2,
1.3
6)
<0
.00
1
Curr
ent
Sm
oker
s*
1.4
7 (
1.2
2,
1.7
8)
<0.0
01
0.9
5 (
0.7
9,
1.1
4)
0.5
6
1.1
6 (
1.0
2,
1.3
2)
0.0
19
SB
P (
mm
Hg)
1.0
1 (
1.0
1,
1.0
2)
<0.0
01
1 (
1,
1.0
1)
0.0
86
1.0
1 (
1, 1
.01
) <
0.0
01
DB
P (
mm
Hg)
0.9
9 (
0.9
8,
1)
0.0
45
0.9
9 (
0.9
9,
1)
0.1
11
0.9
9 (
0.9
9,
1)
0.0
34
HbA
1c
≥7·5
%**
0
.99 (
0.8
4,
1.1
8)
0.9
53
0.9
9 (
0.8
8,
1.1
1)
0.8
42
0.9
9 (
0.9
, 1
.09)
0.8
7
BM
I<25
0
.83 (
0.6
5,
1.0
7)
0.1
55
1.0
7 (
0.9
3,
1.2
4)
0.3
41
0.9
8 (
0.8
7,
1.1
1)
0.7
62
BM
I 25 t
o <
30
0
.96 (
0.8
3,
1.1
2)
0.6
23
1 (
0.8
9, 1.1
3)
0.9
5
0.9
8 (
0.9
, 1
.08)
0.7
35
BM
I ≥
30
refe
rence
*re
fere
nce
cat
egory
is
nev
er-s
mok
ers,
** re
fere
nce
cat
egory
is
HbA
1c
< 7
.5%

97
Tab
le 6
.6:
Est
imate
s of
haza
rd r
ati
os
an
d t
hei
r 95%
con
fid
ence
in
terv
als
for
mort
ali
ty a
nd
card
iovasc
ula
r ev
ents
fro
m m
ult
ivari
ate
str
ati
fied
Cox r
egres
sion
mod
els
wit
h o
bes
e ca
tegory
(B
MI≥
30 k
g/m
2)
as
refe
ren
ce, fo
r p
ati
ents
wit
h p
rior
CV
D a
nd
by a
ge
cate
gori
es. T
he
BM
I u
nit
is
kg/m
2.
M
ort
ali
ty
A
ge≤
68
A
ge>
68
Ov
era
ll
H
R (
95%
CI)
P
Valu
e H
R (
95%
CI)
P
Valu
e H
R (
95
% C
I)
P V
alu
e
Age
> 6
8
2.9
(2
.53
, 3
.32)
<0
.00
1
Men
vs
Wom
en
1.5
2 (
1.2
, 1.9
4)
0.0
01
1.4
5 (
1.2
3,
1.7
) <
0.0
01
1.4
3 (
1.2
6,
1.6
3)
<0
.00
1
Ex
-Sm
oker
s*
1.1
2 (
0.8
8,
1.4
2)
0.3
64
0.9
2 (
0.7
7,
1.0
9)
0.3
22
0.9
6 (
0.8
4,
1.1
) 0
.59
5
Curr
ent
Sm
oker
s*
1.3
2 (
0.9
9,
1.7
7)
0.0
63
1.4
1 (
1.1
, 1.8
1)
0.0
07
1.4
3 (
1.1
9,
1.7
2)
<0
.00
1
SB
P (
mm
Hg)
1.0
1 (
1, 1.0
2)
0.0
02
1 (
1,
1.0
1)
0.0
69
1.0
1 (
1, 1
.01
) 0
.00
1
DB
P (
mm
Hg)
0.9
8 (
0.9
7,
0.9
9)
0.0
01
1 (
0.9
9, 1.0
1)
0.8
14
0.9
9 (
0.9
8,
1)
0.0
12
HbA
1c
≥7·5
%**
1
.05 (
0.7
9,
1.3
8)
0.7
56
1.2
9 (
1.0
8,
1.5
5)
0.0
05
1.1
6 (
1, 1
.35
) 0
.04
8
BM
I<25
1
.04 (
0.7
5,
1.4
4)
0.8
31
1.4
9 (
1.2
2,
1.8
2)
<0.0
01
1.3
0 (
1.1
1,
1.5
3)
0.0
02
BM
I 25 t
o <
30
0
.93 (
0.7
4,
1.1
7)
0.5
35
1.1
7 (
0.9
7,
1.4
) 0.0
94
1.0
5 (
0.9
1,
1.2
) 0
.5
BM
I ≥
30
refe
rence

98
C
ard
iovasc
ula
r E
ven
ts
H
R (
95%
CI)
P
Valu
e H
R (
95%
CI)
P
Valu
e H
R (
95
% C
I)
P V
alu
e
Age
≥ 6
8
- -
- -
1.2
1 (
1.1
4,
1.2
9)
<0
.00
1
Men
vs
Wom
en
1.2
5 (
1.1
4,
1.3
7)
<0.0
01
1.0
9 (
0.9
9,
1.1
9)
0.0
84
1.1
6 (
1.0
9,
1.2
4)
<0
.00
1
Ex
-Sm
oker
s*
1.0
1 (
0.9
1,
1.1
1)
0.9
14
1 (
0.9
1, 1.1
) 0.9
88
1.0
1 (
0.9
4,
1.0
8)
0.7
93
Curr
ent
Sm
oker
s*
1.1
3 (
1, 1.2
7)
0.0
45
1 (
0.8
5, 1.1
8)
0.9
81
1.1
2 (
1.0
3,
1.2
3)
0.0
12
SB
P (
mm
Hg)
1.0
1 (
1, 1.0
1)
<0.0
01
1 (
1,
1.0
1)
0.0
27
1 (
1,
1.0
1)
<0
.00
1
DB
P (
mm
Hg)
1 (
0.9
9, 1)
0.5
97
1 (
1,
1.0
1)
0.2
16
1 (
1,
1.0
1)
0.2
82
HbA
1c
≥7·5
%**
1.2
2 (
1.1
, 1.3
5)
<0.0
01
1.1
1 (
1.0
1,
1.2
3)
0.0
37
1.1
6 (
1.0
8,
1.2
4)
<0
.00
1
BM
I<25
1.1
3 (
0.9
8,
1.3
) 0.0
85
1.1
4 (
1.0
2,
1.2
9)
0.0
27
1.1
3 (
1.0
3,
1.2
3)
0.0
07
BM
I 25 t
o <
30
0.9
8 (
0.9
, 1.0
7)
0.6
92
1.0
3 (
0.9
3,
1.1
4)
0.6
13
0.9
9 (
0.9
3,
1.0
6)
0.8
21
BM
I ≥
30
refe
rence
*re
fere
nce
cat
egory
is
nev
er-s
mok
ers,
** re
fere
nce
cat
egory
is
HbA
1c
< 7
.5%

99
The possible interaction effects of BMI seperately with age and HbA1c at baseline were evaluated
using two approaches. First, for both cohorts, the interaction of these three risk factors
(age×BMI×HbA1c) were statistically significant in time-to-event models for both CVE and all-
cause mortality. Secondly, we used the interaction of categories of age, BMI and HbA1c at
diagnosis in the time-to-event analyses. In Cohort 1, compared to younger patients with obesity,
younger patients with normal weight and older patients with normal weight had 48% and 7-fold
significantly increased mortality risks respectively. A significant interaction between body weight
and glucose levels was also observed in relation to the risk of mortality, after adjusting for other
factors as described in the simple model. Compared to patients with HbA1c below 7.5% and BMI >
30 kg/m2 at diagnosis of diabetes, normal weight patients with HbA1c < 7.5% and normal weight
patients with HbA1c ≥ 7.5% had more than two-fold increased mortality risks respectively (HR:
2.18 and 2.06 respectively). The interaction effect of BMI and HbA1c on the mortality risk is
modified/affected by the distribution of age. This interaction effect was however not significant in
relation to the risk of cardiovascular events.
This exploration can be further considered with the concept of collider bias as depicted by Figure
6.2. BMI and age are directly associated with HbA1c. These two factors collide with HbA1c which
enhances the mortality risk. Aging and BMI are associated with mortality along different pathways
as specified in Figure 6.2.
Figure 6.2: Directed acyclic graph representing causal effects of BMI on mortality

100
Overall, older patients and smokers had significantly higher risks of CVE and all-cause mortality in
both cohorts of patients. Men had significantly higher risks of CVE and death compared to women
in both study cohorts. Men were on average 2 and 4 years younger than women in Cohort 1 and
Cohort 2 respectively. As an additional exploration, we conducted separate analyses for men and
women for both cohorts, to explore the risks of CVE and death associated with normal weight,
compared to obese patients. No differences in risks in relation to normal weight were observed,
compared to what we have observed with combined male-female data.
Among patients without prior cardiovascular diseases, the proportions of current or ex-smokers in
the normal, overweight and obese categories were 45%, 49% and 50% respectively. Compared to
obese patients, the increased mortality risk in normal weight patients were similar between never
smokers (HR,95% CI of HR: 1.38, 1.14-1.67) and current/ex-smokers (HR, 95% CI of HR: 1.60,
1.33-1.94). After incorporating the occurrence of any cardiovascular event during the follow-up as a
competing risk, the mortality risks associated with normal weight patients were higher by 51%
(95% CI of HR: 1.29, 1.76) compared to the obese patients. It is therefore unlikely that residual
confounding explains the association between smoking and mortality
We explored the possible protective or deleterious effects of treatment with metformin and
sulphonylurea in the study cohorts, while evaluating the association of BMI at diagnosis with the
mortality risk. In Cohort 1, among patients treated with metformin within 6 months of diagnosis
(n=24986), the proportion of death were significantly higher in the normal weight category (5.6%)
and overweight category (4.1%), compared to those who were obese (3.1%). This provides strong
evidence that the observed increased mortality risk associated with normal weight is independent of
the protective effects of treatment with metformin. Among those treated with both metformin and
sulphonylurea during follow-up (n=12444), the proportion of deaths was significantly higher in
normal weight patients (4.6%) and overweight patients (2.6%), compared to obese patients (2.1%)
(p=0.001). In patients treated with insulin during follow-up (n= 3490, Cohort 1), the proportions of
death were significantly higher in normal weight patient (8.6%) and over weight patients (6.6%),
compared to the obese patients (4.2%) (p<0.01).
6.4: Discussion and Conclusions
In this study, using a large longitudinal primary care database with median follow-up of 5 years, we
have addressed the recent controversial issue of the obesity paradox in the context of cardiovascular
risks and all-cause mortality in patients with newly diagnosed T2DM. One of the novelties of this

101
study is the use of two separate cohorts of patients with and without the history of CVD prior to the
diagnosis of diabetes. This study allows us to draw the robust epidemiological inferences that - (1)
patients with normal weight at the onset of T2DM have significantly increased mortality risk,
compared to obese patients; (2) the increased mortality risks in normal weight patients are evident
in people both with and without previous history of cardiovascular diseases; (3) among patients
without prior cardiovascular diseases, the increased mortality risks in the normal weight category do
not differ statistically significantly between patients below and above the age of 60 years; (4) the
increased risk of cardiovascular events in normal weight patients is only evident in those with
previous history of cardiovascular diseases; (5) significant interaction of age, BMI and glycaemic
level is evident in relation to risk of CVE and mortality among patients without prior cardiovascular
diseases.
The patterns of mortality risk associated with normal weight patients were similar between older
and younger patients in the cohort without prior cardiovascular disease. However, among patients
with prior cardiovascular disease (Cohort 2), the increased mortality risk associated with normal
weight was evident only among patients with age over 68 years (HR: 1.49, p<0.01). The patterns of
mortality risks associated with BMI categories were structurally different for the two age groups as
evident from the hazard plots in Figure 6. 2, even after adjusting for the additive and interactive
effects of other risk factors. The addition of other risk factors, as described in the extended model
did not alter the findings from the simple model.

102
Fig
ure
6.3
: C
um
ula
tive
haza
rd p
lots
for
all
-cau
se m
ort
ali
ty a
cro
ss t
he
BM
I ca
tegori
es f
or
all
pati
ents
an
d b
y a
ge
cate
gori
es i
n c
oh
ort
wit
hou
t
pri
or
CV
D

103
The strengths of our study include: a large longitudinal primary care data with newly diagnosed
T2DM; separate analyses for patients with and without prior history of cardiovascular disease; long
median follow-up period of 5-years with about 286,000 person-years of follow-up; complete data
on important risk factors; well identified and validated cardiovascular events and death with dates;
and a robust analytical approach which accounts for the possible interaction effects between age,
index of BMI and glycaemic levels in the incident diabetes patients, and a careful assessment to
achieve the most robust risk estimates through the development of stratified Cox regression models.
Some of these crucial aspects were not addressed in the important study recently published by
Logue et al152
and Carnethon et al (2012) 72
. The interaction effects of BMI and HbA1c at the
diagnosis of diabetes in the context of the “obesity paradox” is a novel finding, and should
encourage researchers to conduct further clinical and epidemiological studies in this field.
The death rates in the study conducted by Carnethon et al72
on only 2652 incident diabetes patients
were reported to be 28.5/1000 person-year and 15.2/1000 person-years respectively for normal
weight and overweight plus obese patients. Among patients with/without prior cardiovascular
diseases, our observed death rates in the normal, overweight and obese categories were 30.1/13.1,
21.1/8.6 and 15.4/6.0 per 1000 person-years respectively. In addition, in older patients, the observed
death rates among patients without prior cardiovascular diseases were about 5-fold higher in all
BMI categories. Our observed all-cause mortality risks associated with normal weight patients for
the two study cohorts are not directly comparable with other studies, as we have compared normal
weight as well as overweight patients with the obese group, separately for patients with and without
history of cardiovascular diseases before diagnosis of diabetes. Logue at al152
reported 22% and
32% increased mortality risk associated with normal weight compared to overweight patients for
males and females respectively. In our cohort of patients without a prior history of cardiovascular
disease, these estimates were 21% (p=0.052) and 55% (p<0.01) respectively for male and female
patients.
In recent studies, Flegal et al.156
and Heymsfield et al.155
have discussed the limitations of using
BMI as a marker of adiposity, and waist circumference is recommended as an additional surrogate
marker of the health risks associated with adiposity. BMI as a marker of adiposity has its own
weaknesses, and waist circumference is recommended as an additional surrogate marker of the
health risks associated with adiposity 155,156
. Some studies have suggested that individuals with
normal body weight but high body fat (BF) content (called metabolically obese normal weight
individuals) have a higher prevalence of cardiometabolic dysregulation and are at higher risk for
cardiovascular mortality 72
. A significant limitation of using BMI is its failure to differentiate
between an elevated BF and preserved or increased lean mass, especially in patients with a BMI

104
below 30 kg/m2. However, BMI has many advantages as a surrogate of BF, such as simplicity and
reproducibility, and is commonly used in most of the clinical and epidemiological studies as a
measure of adiposity. The GPRD contains limited information on ethnicity, and on waist and hip
circumference. Earlier studies have suggested that normal weight patients with T2DM could have a
different genetic profile, which warrants a detailed ethnicity-based exploration 163,164
.
Smoking status is a potentially important modifier of the association between anthropometric risk
factors, cardiovascular outcomes and all-cause mortality. We have used the ‘crude’ information on
smoking status at the time of diagnosis of diabetes, as detailed information on duration, timing and
change of smoking status during follow-up was not available. Although we had information on oral
anti-diabetes drugs within 6 months of diagnosis of diabetes, we could not study the contributions
of medications for other illnesses that could be associated with higher mortality. Another weakness
of this study is the unavailability of the cause of death.
Our population level exploratory study provides robust estimates of cardiovascular and mortality
risks associated with normal body weight at the time of diagnosis of diabetes, but the possible
mechanisms behind this are unknown 71,72,165
. Some potential reasons have been discussed by
Carnethon et al72
, which include the possible existence of latent illness in patients with lower body
weight that predisposes to mortality. We have explored two separate cohorts with and without the
history of vascular diseases before diagnosis of diabetes, and also ensured that the possible bias due
to existence of latent illness is eliminated by excluding patients with any cardiovascular event or
death within two years of diagnosis. One approach to understanding the mechanism and the
dynamics of this aspect would be to explore the trajectories of body weight, body fat and clinical
risk factors over time during the follow-up in different BMI categories, after adequately taking
account of the genetic factors and ongoing treatment regimens. In addition, further research needs to
be focused on potential mechanisms for this association.
In conclusion, patients with normal weight and overweight at the time of diagnosis of type 2
diabetes have significantly increased rates and risk of mortality compared to the obese patients.

105
Chapter 7. HbA1c Trajectories by BMI at Diagnosis and the
Effect of Multiple Imputation

106
Trajectories of HbA1c by body mass index and its association with mortality in patients with
type 2 diabetes mellitus - a five year longitudinal population level study and the comparison of
results with data obtained by multiple imputation
7.1: Background
Type 2 diabetes mellitus is a non-communicable metabolic disease. Individuals with this disease
have a reduced life expectancy, and elevated risk of developing microvascular and macrovascular
complications, as well as many other complications that can result in diminished quality of life 1,11
.
The occurrences of these complications are directly associated with the duration of the disease and
the level of hyperglycaemia. The diagnostic criterion for identifying T2DM uses plasma glucose
level or glycated haemoglobin (HbA1c), which is an average glucose level measured over a period
of two to three months, rather than a single point value.
The discovery of insulin was a major milestone in the history of T2DM. Since then, the primary
goal in the treatment of patients with T2DM has been to normalise or near normalise blood glucose
levels 166,167
. Glucose lowering treatments must be increasingly intensified to sustain near-normal
glycaemia because T2DM is a progressive disease with deterioration of β-cells over time 166
. All
patients with T2DM are advised to make lifestyle modifications to enhance weight loss and increase
physical activity 168-170
.
Obesity is one of the most important modifiable risk factors for T2DM and the majority of patients
with T2DM are overweight or obese 171,172
. Body weight has a vital role in the prevention and
treatment of patients with T2DM, because high body weight magnifies the characteristic feature of
T2DM, insulin resistance. An overall increase in the number of obese individuals in both
developing and developed countries has been associated with increasing prevalence of T2DM -
more than 380 million people suffer from T2DM worldwide 15
. As such, obesity is a major risk
factor for T2DM 173
. BMI is widely accepted and used as to identify obesity in individuals.
Obesity has been proven to be an important risk factor among the complex array of contributory
factors, for the development of T2DM and its associated atherosclerotic vascular complications 66,67
.
Contrary to the popular belief, studies have shown that in comparison to overweight or obese
individuals, T2DM patients of normal weight are at a higher risk of atherosclerotic vascular disease
and mortality associated with T2DM 72,174
. There exists a subset of normal weight individuals with
physiological characteristics of obese individuals and are prone to develop T2DM 66,68
. They are
denoted as metabolically obese but normal weight (MONW) patients and are characterised by a

107
confrontational metabolic status, which includes insulin resistance, hyperinsulinemia and other
related diseases 65,68
. This reiterates the fact that it is not necessary to be overweight or obese for the
development and progression of T2DM.
Glycaemic variation in T2DM patients, measured by HbA1c, over time according to BMI levels,
remains understudied and its role in disease progression is not clear. One of the aims of this chapter
is to explore the long-term longitudinal trajectories of HbA1c, by body mass index at the time of
diagnosis of T2DM.
It is also important to explore the relationships between HbA1c levels and complications associated
with intensive treatment. Therapeutic strategies to control or reduce HbA1c levels in diabetic
patients, thereby reducing complications associated with diabetes, has been supported by some but
not all clinical trials 175
. Data from epidemiologic studies and some clinical trials have been used to
support guidelines for maintaining HbA1c or blood glucose levels in T2DM patients within or near-
normal levels, despite a lack of direct evidence concerning the risks and benefits of doing so 13,28
.
Analyses of data from the ACCORD trial have confirmed that an excessive all-cause mortality risk
was associated with an intensive glycaemic treatment strategy in people with T2DM 28
. However,
epidemiologic studies suggest that greater degrees of hyperglycaemia in people with T2DM,
reflected by elevated HbA1c levels, are associated with higher risks of both mortality and CVD.
These risks have been estimated to increase by 18% (for CVD) and 12-14% (for mortality) for each
1% increase in HbA1c 7,28,176,177
.
All trials addressed the effect of intensively controlling glycaemic levels and the benefits and risks
associated with intensive therapy; other studies have evaluated CVD and mortality risks associated
with intensive treatment in T2DM patients. However, none focused on the obesity status of
individuals at the time of their diagnosis, nor did they address the modification of these changes by
BMI status at the time of diagnosis.
Inferences based on large longitudinal datasets are of great interest in the current research climate.
One of the inherent problems associated with such datasets is missingness in the observations.
Missingness in covariates may lead to various problems associated with the selection of variables,
and diminished power and bias in the result estimates 178
. In most randomised clinical trials, the
‘last observation carried forward’ (LOCF) is a common approach for dealing with missing data 179
.
But in longitudinal observational studies, deletion of the cases with any missing values, called
complete case (CC) analysis179,180
, is often used. A detailed exploration of the technical and
statistical challenges associated with missing data in clinical research is given in Chapter 2.

108
By considering these unmet immediate clinical and statistical needs, the aims of this cohort study
were to:
1. explore and compare the five year trajectories of HbA1c before death in T2DM patients
classified as ‘normal weight’, ‘overweight’ or ‘obese’ at the time of their diagnosis.
2. compare the mortality risk associated with intensive treatment and longitudinal HbA1c
measurements immediately before death, within treatment groups, stratified by BMI.
3. compare trajectories using the original data and the data obtained from multiple imputation.
7.2: Methods
7.2.1: Data
The Clinical Practice Research Datalink contains the largest set of longitudinal primary care data
derived from primary care practices in the United Kingdom. The CPRD contains clinical
information including diagnoses, mortality, laboratory results and prescription of medications
details 120,181
. The primary data set for this retrospective cohort study includes data from 84596
individuals aged between 18 and 99 who were newly diagnosed with T2DM in the period between
1990 and 2005, followed up until April 2007, and who had been registered with the general practice
for at least 12 months. Detailed information about the data is given in Chapter 3.
To explore the trajectories of HbA1c and to assess the mortality risks of people in each of the BMI
categories at the time of their diagnosis, a dataset of 7030 patients with T2DM was created based on
the following inclusion criteria.
Patients were diagnosed between 1 January 1990 to 1 December 2002, ensuring a minimum follow-
up of five years. They were also required to have:
1. HbA1c measured at the time of diagnosis.
2. BMI measured at the time of diagnosis.
3. a minimum of six HbA1c measurements taken during the five years immediately before
death or censoring; these were based on six-monthly longitudinal windows, thus ensuring
more than 50% of the longitudinal data over the last 5 years before death/censoring.

109
Date of death was derived from modified GPRD death codes captured as part of routine care
(including investigations) or as a result of hospitalisation or emergency care 182
. Ethics approval for
the use of CPRD data was granted by the Independent Scientific Advisory Committee in June 2014.
The following information was extracted: demographic characteristics and factors, including age,
gender, smoking status (defined as current, former or never smokers), BMI, blood pressure
recordings (systolic and diastolic), HbA1c, previous and current clinical conditions included
cardiovascular events (myocardial infarction, stroke, heart failure, coronary heart disease, peripheral
artery disease, angina, angioplasty, coronary artery bypass graft), medication data by dates
(including use of metformin, sulphonylurea, rosiglitazone, pioglitazone, meglitazone, insulin,
ACE/ARB, beta blocker, statin and other concomitant medications) identified from prescription
records, and all-cause mortality. Two new variables, named ‘any previous CVD’ and ‘any current
CVD’, have been defined as composite outcomes measuring the occurrence of any CVD before
T2DM diagnosis and any CVD during the follow-up period, respectively.
Based on prescription data for oral anti-diabetes (OAD) drugs and insulin, the study population was
classified into two groups: patients receiving intensive treatment, and those not receiving intensive
treatment. Patients taking at least two OADs and insulin made up the intensive group.
Categories of BMI were defined as ‘normal weight’ (BMI greater than 18 kg/m2 and less than 25
kg/m2), ‘overweight’ (BMI at least 25 kg/m
2 and less than 30 kg/m
2) and ‘obese’ (BMI at least 30
kg/m2). The average duration of follow-up was calculated from the time of diagnosis with diabetes
until the end of the follow-up period.
7.2.2: Statistical Methods
Summary statistics were presented by number (percent), mean (SD), or median (IQR), as
appropriate. The chi-square test was used to assess relationships between categorical variables. One
way analysis of varience (ANOVA), using the Bonferroni adjustment for multiple comprisons, was
used to evaluate mean differences in clinical and biochemical parameters across BMI categories.
Epanechikov Kernal density plots were used to plot the densities of HbA1c at the time of diagnosis
within BMI categories.
Separate multivariate GEE regression models were used, assuming approximately normally
distributed HbA1c measurements and an unstructured correlation structure to evaluate longitudinal
trajectories of HbA1c during the five years before death or censoring. This model was adjusted for:

110
the effects of age (using a cut-point of 65 years), sex, HbA1c at diagnosis, CVD status (no CVD
either prior or during the follow-up period, previous CVD only, current CVD during follow-up
only, CVD prior to diagnosis and during the follow-up period), CPM, and intensive treatment in
normal, overweight and obese patients based on their BMI at the time of their diagnosis. Evaluation
of mortality risk in these patients, according to their BMI status, was assessed with separate GEE
models using a binomial distribution and an independent correlation structure after adjusting for:
age, sex, HbA1c at diagnosis, CVD status, CPM, and intensive treatment.
The number of missing HbA1c measurements was calculated for each time window, and, for their
effect on the exploration of longitudinal trajectories, a comparison between multiply imputed data
and original data was conducted.
Multiple imputation is a simulation-based statistical technique consisting of three steps.
1. An imputation step: following selection of a set of predictors for an imputation model, the
required number of imputed datasets are created, in which predicted values under the model
replace missing values.
2. An estimation step: a specific statistical analysis is performed on each of the imputed
datasets created by imputation. This step is also known as imputed data analysis.
3. A pooling step: results obtained from different imputed data analyses are combined to form
a single multiple imputation estimate, and to estimate the appropriate precision of this
estimate, taking account between and within imputation variation.
A total of 100 imputations were performed to impute the longitudinal values of HbA1c from the
following covariates: age greater than 65 years, sex, baseline HbA1c, CVD status, cardio protective
medications and intensive treatment. These imputed datasets are further analysed using statistical
methods described above. The STATA syntax used for multiple imputations is given in Appendix
2.
7.3: Results
7.3.1: Trajectories of HbA1c by BMI categories
In the cohort of 7030 newly diagnosed T2DM patients, 54% were male, with a mean (SD) age of 61
(11) years, BMI of 30.39 (5.91) kg/m2, and HbA1c of 8.2 (2.08)%. The proportions of normal
weight, overweight and obese patients were 15% (n=1040), 39% (n=2778) and 46% (n=3212),
respectively. Nearly 40% of patients were 65 or older, the majority of which were overweight

111
(n=1301, 45.7%) or obese (n=990, 34.8%) at the time of their diagnosis. Detailed descriptive
characteristics of the study population are given in Table 7.1
Table 7.1: Descriptive statistics of the T2DM study cohort
Normal Overweight Obese P value
n 1040 2778 3212
Age at Diagnosis (yrs) 64 (12) 63 (11) 58 (11)
Age ≥65 554 (53.3) 1301 (46.8) 990 (30.8) <0.001
Male# 550 (52.8) 1722 (62.0) 1520 (47) <0.001
Smoking status <0.001
Never smokers# 566 (55.0) 1336 (48.0) 1545 (48.0)
Ex-smoker# 317 (30.6) 1116 (40.4) 1227 (38.4)
Current smoker# 152 (14.7) 311 (11.3) 425 (13.3)
SBP (mmHg)* 141 (20) 142 (19) 144 (18)
DBP (mmHg)* 80 (10) 81 (10) 84 (10)
BMI (Kg/m2)* 22.9 (1.7) 27.5 (1.4) 35.3 (5.0)
HbA1c (%)* 8.5 (2.3) 8.3 (2.1) 8.0 (2.0)
LDL (mmol/L)* 3.4 (1.1) 3.3 (1.0) 3.2 (1.0)
HDL (mmol/L)* 1.3 (0.4) 1.2 (0.3) 1.2 (0.7)
Tryglyceride**
(mmol/L) 1.7 (1.2, 2.4) 1.9 (1.4, 2.8) 2.1 (1.5, 3.0)
Previous Cardiovascular diseases
Myocardial infarction# 41 (3.9) 88 (3.2) 88 (2.7) 0.14
Stroke# 55 (5.3) 108 (3.9) 96 (3.0) <0.01
Heart failure# 38 (3.7) 125 (4.5) 170 (5.3) 0.07
CHD# 85 (8.2) 322 (11.6) 301 (9.4) <0.01
PAD# 40 (3.9) 102 (3.7) 75 (2.3) <0.01
Angina# 93 (8.9) 326 (11.7) 367 (11.4) 0.04
Any Previous CVD# 240 (23.1) 679 (24.4) 695 (21.6) 0.03
Current Cardiovascular diseases
Myocardial infarction# 42 (4.0) 87 (3.1) 82 (2.6) 0.04
Stroke# 69 (6.6) 149 (5.4) 135 (4.2) <0.01

112
Heart failure# 40 (3.9) 130 (4.7) 172 (5.4) 0.12
CHD# 109 (10.5) 266 (9.6) 310 (9.7) 0.68
PAD# 41 (3.9) 105 (3.8) 79 (2.5) <0.01
Angina# 104 (10.0) 279 (10.0) 327 (10.2) 0.97
Any Current CVD# 244 (23.5) 631 (22.7) 681 (21.2) 0.19
Death# 50 (4.8) 118 (4.3) 114 (3.6) 0.14
Current medication
Metformin# 668 (64.2) 2210 (79.6) 2794 (87.0) <0.001
Sulphonylurea# 752 (72.3) 1748 (62.9) 1725 (53.7) <0.001
Rosiglitazone# 175 (16.8) 504 (18.1) 772 (24.0) <0.001
Pioglitazone# 51 (4.9) 177 (6.4) 250 (7.8) <0.01
Insulin# 219 (21.1) 407 (14.7) 489 (15.2) <0.001
Beta blockers# 349 (33.6) 1124 (40.5) 1321 (41.1) <0.001
ACEARB# 700 (67.3) 2091 (75.3) 2558 (79.6) <0.001
CPM# 966 (92.9) 2667 (96.0) 3111 (96.7) <0.001
Intensive treatment 171 (16.4) 361 (13.0) 434 (13.5) 0.02
*mean (SD), **median (Q1, Q3), #n (%)
Patients who were obese at their time of diagnosis with T2DM were younger than those who were
normal weight or overweight, with a mean age of 58 (SD of 11). Higher HbA1c levels were
observed in patients of normal weight (mean, SD: 8.5, 2.3) compared to those with higher BMIs.
The density plots (by BMI status) of HbA1c at the time of diagnosis with T2DM are depicted in
Figure 7.1.

113
Figure 7.1: Density plots of HbA1c (%) at time of diagnosis in normal, overweight and obese
patients.
The proportion of patients with a history of CVD prior to their diagnosis with diabetes was higher
in overweight (n=679, 24%) and obese (n=695, 22%) patients compared with those of normal
weights; these differences were significant across BMI categories (Table 7.1).
Almost 22% (n=1556) of patients experienced at least one CVD after being diagnosed with T2DM;
that is, during the follow-up period (Table 7.1). A total of 282 (4.01%) patients died. The proportion
of deaths did not vary significantly across BMI categories.
Metformin was the most prescribed anti-diabetic medication for those in the cohort, followed by
sulphonylurea (Table 7.1). The proportion of those prescribed these medications varied significantly
across BMI categories. Significantly higher proportions of overweight and obese patients were
prescribed these medications compared to patients of normal weights.
The trajectories of HbA1c over the five year period immediately before death or censoring – in
normal, overweight and obese patients – varied significantly depending on the treatment strategy
they were provided with. This information is presented graphically in Figure 7.2

114
Figure 7.2: Trajectories of HbA1c (%) over the 5 year period immediately before
death/censoring, by treatment strategies.
7.2a: Normal weight patients
Figure 7.2b: Overweight patients

115
Figure 7.2c: Obese patients
The aim of intensive treatment with medication is to control (lower) glycaemic levels. However,
patients receiving intensive treatments had significantly higher levels of HbA1c throughout the five
years before death or censoring across all BMI categories. HbA1c levels of patients in the intensive
treatment group fluctuated throughout the follow-up period. The multivariate model showed that
patients undergoing intensive treatment had higher levels of HbA1c (%), for all categories of BMI –
i.e. for patients who were overweight, obese, or of normal weight, by 1.07% (95% CI:1.02, 1.11),
1.23% (95% CI:1.19, 1.28), and 0.94% (95% CI: 0.87, 1.01), respectively, after adjusting for the
effects of other potentially confounding factors (Table 7.2). Older patients had significantly lower
levels of HbA1c over the five years compared to their younger counterparts, across all BMI
categories. Obese males had significantly higher HbA1c levels then obese females. High levels of
HbA1c over the five years were associated significantly with the HbA1c level measured at the time
of diagnosis with T2DM. Although HbA1c at the time of diagnosis contributed significantly to the
higher levels of HbA1c over the five years before death or censoring, patients who were of a normal
weight had higher levels of HbA1c compared to those who were overweight or obese (0.19 versus
0.15 and 0.16) (Table 7.2). CVD status was not associated with HbA1c levels in patients who were
of a normal weight. There were significant reductions in HbA1c levels in overweight and obese
patients, although these reductions were of marginal clinical importance. Significant reductions (of
marginal clinical importance) were also observed in overweight patients who experienced a CVD
event prior to diagnosis and during the follow-up period. The same pattern of reductions were also
observed in obese patients who experienced a CVD event during the follow-up period.

116
Tab
le 7
.2:
Tra
ject
ori
es o
f H
bA
1c
bef
ore
dea
th/c
enso
rin
g i
n a
ll p
ati
ents
an
d a
ccord
ing t
o t
reatm
ent
stra
tegie
s.
N
orm
al
Wei
gh
t
Over
wei
gh
t
Ob
ese
R
egre
ssio
n
Co
-eff
icie
nt
(95%
CI)
P-v
alu
e R
egre
ssio
n
Co-e
ffic
ien
t (9
5%
CI)
P-v
alu
e R
egre
ssio
n
Co
-eff
icie
nt
(95
% C
I)
P-v
alu
e
Age≥
65
-0
.23
(-0
.28,
-0.1
7)
<0.0
01
-0.2
2 (
-0.2
5,
-0.1
9)
<0
.00
1
-0.2
5 (
-0.2
9,
-0.2
2)
<0
.00
1
Sex
0
.03
(-0
.02,
0.0
8)
0.2
8
-0.0
2 (
-0.0
5,
0.0
2)
0.3
3
0.0
6 (
0.0
3,
0.0
9)
<0
.00
1
HbA
1c
0.1
9 (
0.1
8,
0.2
0)
<0.0
01
0.1
5 (
0.1
4,
0.1
6)
<0
.00
1
0.1
6 (
0.1
5,
0.1
7)
<0
.00
1
Pri
or
CV
D
0.0
2 (
-0.0
7,
0.1
2)
0.6
3
-0.0
2 (
-0.0
7,
0.0
3)
0.4
6
-0.0
1 (
-0.0
6,
0.0
5)
0.8
5
Curr
ent
CV
D
0.0
5 (
-0.0
4,
0.1
5)
0.2
4
-0.0
4 (
-0.0
9,
0.0
2)
0.2
3
-0.0
7 (
-0.1
3,
-0.0
1)
0.0
2
Both
CV
D
-0.0
5 (
-0.1
3,
0.0
2)
0.1
5
-0.0
9 (
-0.1
3,
-0.0
4)
<0
.00
1
-0.0
4 (
-0.0
9,
0.0
1)
0.1
1
CP
M
-0.0
9 (
-0.1
9,
0.0
2)
0.0
9
-0.1
7 (
-0.2
5,
-0.0
9)
<0
.00
1
-0.0
1 (
-0.1
0,
-0.0
8)
0.8
2
Inte
nsi
ve
trea
tmen
t
0.9
4 (
0.8
7,
1.0
1)
<0.0
01
1.0
7 (
1.0
2,
1.1
1)
<0
.00
1
1.2
3 (
1.1
9,
1.2
8)
<0
.00
1

117
An overall exploration of the trajectories of HbA1c in patients who were of of normal weight,
overweight and obese showed that differences in levels of HbA1c (measured longitudinally over
five years) were not statistically significantly different between patients who died and those who
remained alive. However, obese patients who died, or were censored at the end of the follow-up
period, had significantly lower levels of HbA1c than those who remained alive (Figure 7.3).
Figure 7.3: Trajectories of HbA1c by mortality status and baseline BMI
Figure 7.3a: Normal weight

118
Figure 7.3b: Overweight
Figure 7.3c: Obese

119
Analyses of the mortality risk associated with longitudinally measured HbA1c levels, and other
covariates based on their BMI levels at time of diagnosis, are given in Table 7.3. These showed a
14% increased mortality risk for every 1% increase in HbA1c over the five years immediately
before death or censoring – for patients of a normal weight (OR, 95% CI: 1.14, 0.92-1.43). This
increased mortality risk was clinically but not statistically significant. Overweight (OR, 95% CI:
1.06, 0.94-1.21) and obese (OR, 95% CI: 1.02, 0.90-1.14) patients also had higher (but statisitically
nonsignificant) risks, but compared to patients of a normal weight, the risks were lower – although
still clinically significant (Table 7.3). Older patients had a significantly increased mortality risk
compared to younger patients, across all BMI categories. Patients who were 65 years or older and of
normal weight at the time of their diagnosis had an almost six fold increased mortality risk when
compared to their younger counterparts (OR, 95% CI: 5.7, 2.29-14.35 ). Similarly, overweight and
obese older patients had a five- and three- fold increased mortality risk compared to the younger age
group, respectively (OR, 95% CIs: 4.7, 2.84-7.94, and 3.4, 2.26-5.20).
In patients of normal weight, females had a two- fold significantly increased mortality risk
compared to males, (OR, 95% CI: 2.04, 1.08-3.82). Patients who were prescribed cardioprotective
medications during the follow-up period had a significantly reduced mortality risk across all BMI
categories. Compared to patients who were free from CVD both prior to their diagnosis with T2DM
and during the follow-up, those who had at least one episode of CVD during the follow-up and
those who had had both previous and current episodes of CVD had higher mortality risks, for all
BMI categories (Table 7.3).

120
Tab
le 7
.3:
Mort
ali
ty r
isk
ass
oci
ate
d w
ith
lon
git
ud
inal
Hb
A1c
mea
sure
men
ts, b
y t
rea
tmen
t st
rate
gie
s, i
n d
iffe
ren
t B
MI
cate
gori
es.
N
orm
al
Over
wei
gh
t O
bes
e
O
R (
95%
CI)
P
-valu
e O
R (
95%
CI)
P
-va
lue
OR
(9
5%
CI)
P
-va
lue
Age≥
65
5
.74 (
2.2
9,
14.3
5)
<0.0
01
4.7
5 (
2.8
4,
7.9
4)
<0
.00
1
3.4
2 (
2.2
6,
5.2
0)
<0
.00
1
Mal
e 2
.04 (
1.0
8,
3.8
2)
0.0
2
1.0
6 (
0.7
1,
1.5
9)
0.7
7
1.3
5 (
0.9
0,
2.0
0)
0.1
4
Bas
elin
e H
bA
1c
1.0
2 (
0.8
7,
1.2
1)
0.7
9
1.0
8 (
0.9
8,
1.1
8)
0.1
2
1.0
9 (
0.9
9,
1.2
0)
0.0
9
CP
M
0.2
0 (
0.0
8,
0.4
9)
<0.0
01
0.1
6 (
0.0
8,
0.3
1)
<0
.00
1
0.2
6 (
0.1
1,
0.6
1)
0.0
02
Pri
or
CV
D
2.2
7 (
0.7
3,
7.1
1)
0.1
5
1.2
0 (
0.5
4,
2.6
6)
0.6
4
1.0
2 (
0.4
2,
2.4
9)
0.9
5
Curr
ent
CV
D
5.9
3 (
2.3
1,
15.2
4)
<0.0
01
2.8
4 (
1.5
4,
5.2
2)
0.0
01
5.2
3 (
3.0
1,
9.0
9)
<0
.00
1
Both
CV
D
7.4
2 (
3.4
7,
15.9
0)
<0.0
01
5.2
8 (
3.2
6,
8.5
6)
<0
.00
1
5.8
6 (
3.6
2,
9.4
8)
<0
.00
1
Inte
nsi
ve
Tre
atm
ent
0.6
7 (
0.2
6,
1.7
5)
0.4
1
0.6
4 (
0.3
2,
1.2
6)
0.2
0
0.9
2 (
0.5
1,
1.6
5)
0.7
6
Lon
git
udin
al A
1c
1.1
4 (
0.9
2,1
.43)
0.2
3
1.0
6 (
0.9
4,
1.2
1)
0.3
2
1.0
2 (
0.9
0,
1.1
4)
0.7
7

121
7.3.2: Imputed data versus original data
The proportions of missing data in the longitudinal measurements of HbA1c by BMI status are
given in Table 7.4. During the last four years before death, the proportion of missing observations
in HbA1c measurements were generally consistent in all three categories of BMI. However, during
the last year – that is, the one immediately before death or censoring – this proportion increased by
more than 50%, an effect that was similar for all BMI categories.
Table 7.4: Proportions of missing data in HbA1c measured longitudinally in the 5 year period
before death or censoring, according to BMI categories of the patients at the time of their
diagnosis with T2DM.
HbA1c
(Longitudinal)
Normal
n(%)
Overweight
n(%)
Obese
n(%)
-54 months 197 (18.9) 496 (17.9) 537 (16.7)
-48 months 181 (17.4) 533 (19.2) 633 (19.7)
-42 months 212 (20.4) 498 (17.9) 612 (19.1)
-36 months 194 (18.7) 498 (17.9) 571 (17.8)
-30 months 186 (17.9) 462 (16.6) 564 (17.6)
-24 months 174 (16.7) 463 (16.7) 550 (17.1)
-18 months 184 (17.7) 489 (17.6) 599 (18.7)
-12 months 185 (17.8) 494 (17.8) 655 (20.4)
-6 months 274 (26.4) 636 (22.9) 765 (23.8)
Death/Censoring 533 (51.3) 1441 (51.9) 1676 (52.2)
Analyses of HbA1c trajectories based on the multiply imputed datasets and the original data with
missing HbA1c recordings is given in Tables 7.5 (7.5a – 7.5c). Comparison of these, which apply
the same mode for the trajectories of HbA1c within BMI categories, shows similar estimates. This
indicates that the original dataset with missing values was a representative sample of the complete
longitudinal set of HbA1c measurements, at least for the purpose of this analysis.

122
Table 7.5: Comparison of the HbA1c trajectory in imputed data and original data
Table 7.5a: Normal weight
MVNI Original
Regression
co-efficient
P value Regression
co-efficient
P value
Age ≥ 65 -0.24 (-0.29, -0.18) <0.001 -0.23 (-0.28, -0.17) <0.001
Sex 0.01 (0.03, 0.06) 0.58 0.03 (-0.02, 0.08) 0.28
HbA1c 0.18 (0.17, 0.19) <0.001 0.19 (0.18, 0.20) <0.001
Prior CVD 0.01 (-0.08, 0.10) 0.85 0.02 (-0.07, 0.12) 0.63
Current CVD 0.05 (-0.03, 0.14) 0.21 0.05 (-0.04, 0.15) 0.24
Both CVD -0.06 (-0.14, 0.004) 0.06 -0.05 (-0.13, 0.02) 0.15
CPM -0.08 (-0.17, -0.01) 0.09 -0.09 (-0.19, 0.02) 0.09
Intensive treatment 1.23 (1.19, 1.28) <0.001 0.94 (0.87, 1.01) <0.001
Table 7.5b: Overweight
MVNI Original
Regression
co-efficient
P value Regression
co-efficient
P value
Age ≥ 65 -0.23 (-0.26, -0.20) <0.001 -0.22 (-0.25, -0.19) <0.001
Sex -0.01 (-0.03, 0.02) 0.74 -0.02 (-0.05, 0.02) 0.33
HbA1c 0.15 (0.14, 0.15) <0.001 0.15 (0.14, 0.16) <0.001
Prior CVD -0.01 (-0.07, 0.03) 0.47 -0.02 (-0.07, 0.03) 0.46
Current CVD -0.03 (-0.08, 0.02) 0.29 -0.04 (-0.09, 0.02) 0.23
Both CVD -0.09 (-0.14, 0.05) <0.001 -0.09 (-0.13, -0.04) <0.001
CPM -0.16 (-0.24, -0.08) <0.001 -0.17 (-0.25, -0.09) <0.001
Intensive treatment 1.08 (1.03, 1.12) <0.001 1.07 (1.02, 1.11) <0.001

123
Table 7.5c: Obese
MVNI Original
Regression
co-efficient
P value Regression
co-efficient
P value
Age ≥ 65 -0.25 (-0.28, -0.22) <0.001 -0.25 (-0.29, -0.22) <0.001
Sex 0.06 (0.03, 0.09) <0.001 0.06 (0.03, 0.09) <0.001
HbA1c 0.15 (0.15, 0.16) <0.001 0.16 (0.15, 0.17) <0.001
Prior CVD -0.02 (-0.07, 0.03) 0.39 -0.01 (-0.06, 0.05) 0.85
Current CVD -0.06 (-0.12, -0.01) 0.01 -0.07 (-0.13, -0.01) 0.02
Both CVD -0.05 (-0.09, 0.01) 0.02 -0.04 (-0.09, 0.01) 0.11
CPM -0.02 (-0.11, 0.05) 0.53 -0.01 (-0.10, -0.08) 0.82
Intensive treatment 1.23 (1.19, 1.28) <0.001 1.23 (1.19, 1.28) <0.001
7.4: Discussion and Conclusion
This analysis of 7030 newly diagnosed T2DM patients from the UK primary health care practice
database showed that longitudinally measured levels of HbA1c over the five years immediately
before death or censoring were consistently higher in patients who received intensive treatment,
irrespective of their BMI status at the time of diagnosis. That is, patients who were normal weight,
overweight and obese at the time of diagnosis had higher levels of HbA1c, despite undergoing
intensive treatment, which was aimed at reducing glycaemic levels to normal or near-normal levels.
Changes in HbA1c levels over the five years immediately before death or censoring was not
significantly different for patients who died and those who remained alive. While the amount of
missing data in the longitudinally measured HbA1c values was about 20% at each time point
(except for the last measurement), a comparison of HbA1c trajectories for the inputed data set and
the original data showed a very similar pattern.
The large sample size used – 7030 newly diagnosed T2DM patients for whom longitudinal
measurements of HbA1c over the five years immediately before death or censoring – was the major
advantage of this analysis. By ensuring, during data selection, that more than 50% of the
longitudinal HbA1c measurements were present (at least 6 measurements over the ten possible

124
measurements in the six monthly windows for all 7030 patients), potential issues related to the
missingness of data were minimised to a great extent. Complete data on covariates used in GEE
analysis and multiple imputation was another strength. As mentioned above, although the number
of missing HbA1c measurements for each of the time points was quite high, the trajectory analysis
gave similar results using both imputed and original data, indicating that data were missing at
random, at least for the purposes of this analysis. The prescription of medication data and the
occurences of other diseases during the follow-up period helped ensure the CVD history of patients
was more precise. The application of appropriate statistical methods – multivariate analysis
adjusting for the effects of other confounding covariates – added additional strength to this analysis.
The exploration of trajectories of HbA1c stratified by BMI categories at the time of diagnosis is a
very novel concept, as the majority of the studies in this area have evaluated the mortality risks
associated with weight gain, or the relationship between higher BMIs and transitions in glycaemic
levels 72,155,156,183
.
The limitations of this study include the non-availability of data regarding: (1) dietary habits – to
evaluate their association with disease progression, as dietary habits are directly associated with
BMI; (2) compliance with medications during the follow-up period; (3) lifestyle modifications
made by patients after their diagnosis with T2DM.
Previous studies have reported that approximately 80% of patients with T2DM are overweight or
obese 184
. Intensive lifestyle modifications, including improving physical activity and medications,
are of considerable importance for diabetic patients in the control of their glycaemic levels and the
associated CVD risk factors 185
.
A study by Watson et al.186
that explored the changes in HbA1c, weight and BMI after the initiation
of insulin treatment in T2DM patients reported that it had helped to improve glycaemic levels,
across all BMI categories, in the six months after its administration; but for the period between six
and 24 months little change occurred. This study also reported that obese patients required higher
levels of insulin to control their glycaemic levels. However, two years after the initiation of insulin
treatment, additional insulin supplements did not substantially improve glycemic levels as before.
The trajectory analysis by BMI status of newly diagnosed T2DM patients, exploring the changes to
HbA1c over the five years before death, demonstrates that patients undergoing intensive treatment
had significantly higher levels of HbA1c compared to those who were not. Intensive treatment with
insulin in T2DM patients is initiated when treatment with oral anti-diabetes drugs alone fails to
achieve reductions of HbA1c to an expected level 169
. The study design of Watson et al.186
clearly

125
states that study subjects included patients on oral therapy as well. Therefore, the treatment
described can be considered as an intensive therapy, as it encompasses the administration of both
oral anti-diabetes drugs and insulin. Watson’s study also reported that the attainment of glycaemic
control was differently achieved within different BMI categories, and that 26-31% of obese patients
had attained HbA1c 7.5% or lower, compared with 41% of patients of normal weight. This clearly
suggests that intensive therapy could be more effective in the control of glycaemic levels of normal
weight patients. Another study, by Carnethon et al., reports that adults who were of a normal weight
at the time of their diagnosis with T2DM had higher mortality risks compared to overweight and
obese adults 72
.
One of the most important challenges in longitudinal studies and randomised controlled trials is that
a large amount of missing data, as a result of loss to follow-up, potentially results in reduced
statistical power and considerable reductions in internal validity, if data are not missing completely
at random (MCAR), with additional challenges associated with the analysis of incomplete data 187
.
The most popular method for handling missing data is multiple imputation. This process replaces
missing values with values predicted under a statistical model derived from the known data. It has
been demonstrated that multiple imputation is very efficient, even in cases where a relatively small
number of imputations is used 84,188
. In this analysis, a high number of imputations (100
imputations) was used. A comparion of the results generated using these the imputed and original
datasets has shown very similar findings. The design of this study minimised the amount of data
missing, which is the best way to address this problem of missingness; however it cannot be
completely avoided in real clinical research.
This novel trajectory analysis not only confirms the general clinical belief that overweight and
obese patients have higher HbA1c levels, but normal weight patients may also have much higher
levels than are to be expected, even when treated with intensive therapies. The mortality risks
associated with HbA1c were clinically significant for patients in all BMI categories. More clinical
attention must be given to normal weight patients, for the better clinical management of this
disease.

126
Chapter 8. General Discussion and Conclusions

127
8.1: Thesis Research Objectives
The aims of this thesis are restated below:
Objective 1: to evaluate the gender specific effects of smoking on cardiovascular and mortality
outcomes in newly diagnosed diabetic men and women (Chapter 4).
Objective 2: to examine blood pressure trajectories before death in patients with type 2 diabetes
mellitus (Chapter 5).
Objective 3: to examine the obesity paradox in people newly diagnosed with T2DM, with and
without prior cardiovascular disease (Chapter 6).
Objective 4: to examine HbA1c trajectories, by body mass index, and how these are associated with
mortality in patients with T2DM; as well as to investigate the effects of missing data, using multiple
imputation. (Chapter 7)
Each of these objectives address important clinical questions associated with the management of
T2DM (from the perspective of the disease being non-curable, but controllable, once diagnosed).
This thesis is based on a statistical analysis of a large longitudinal study (17 year follow-up) of
84596 newly diagnosed T2DM patients. Data was taken from the UK CPRD, which allowed
changes in key indicators of disease progression – from diagnosis until death or censoring – to be
tracked. Aspects of self-management and appropriate clinical care are described with reference to
each of these objectives. Findings from each of the above mentioned objectives, and their relevance
to the current clinical management of diabetes, are discussed in this chapter.
Chapter 4 confirms the existence of gender disparities in relation to the effects of smoking in
patients newly diagnosed with T2DM. Complications associated with T2DM considered in this
analysis were CVD, as well as all-cause mortality. An increased risk of cardiovascular diseases and
mortality was observed among women, based on comparisons among never smokers, former
smokers and current smokers. These analyses were stratified by CVD history prior to diagnosis with
T2DM, and CVD that developed during the follow-up period. Results were consistant with other
studies that had explored gender differences in diabetic patients, in the risks associated with CVD
and mortality attributable to smoking 24,125,126
. The finding that diabetic women who smoked had
higher coronary and mortality risks was consistent with previous researches 24,76
. The reason for
these higher risks, compared to men, is still unknown, although delays in diagnosis, or the sub-

128
optimal clinical management of T2DM in women have been proferred as reasons. This analysis did
not address the undertreatment of diabetes in women. However, a study by Wexler et al. has
confirmed diminished diabetic treatment in women compared to men 127
.
Chapter 5 explores the longitudinally measured trajectories of both systolic and diastolic blood
pressure, and their association with mortality risk in newly diagnosed T2DM patients. This analysis
clearly shows that patients who died during the study had significantly higher systolic and diastolic
blood pressures for the two years immediately before death or censoring compared to those who
survived. A study by Rogers and collegues reported a clinically and statistically significant rapid
decline in both measurements of blood pressure in diabetic patients who died compared to patients
who remained alive 141
. However, results of the present analyses are based on a substantially higher
sample size (N = 18583) of patients newly diagnosed with T2DM, as well as complete blood
pressure measurements taken immediately before death or censoring. A clinically significant
decline in blood pressure was not seen, although trajectories were higher in patients who died
compared to those who remained alive.
Chapter 6 of this thesis addresses the obesity paradox in relation to the risks associated with CVD
and mortality in patients newly diagnosed with T2DM 174
. The obesity paradox has been defined as
the presence of an increased risk of CVD or mortality in patients of a normal weight compared to
obese patients. An exploration of this paradox was stratified accoding to CVD history – one of the
innovations of this study. This analysis demonstrates that patients with a normal weight at the time
of diagnosis with T2DM have a significantly increased mortality risk compared to those who were
obese. This was observed both in patients with and without prior CVD. In those who were of a
normal weight and had no prior CVD, older patients (categorised on the basis of age at diagnosis –
above or below 60 years) were not statistically different from younger patients in their increased
mortality risk. Results from these analyses, examining the association between all-cause mortality
and BMI category, are not comparable to those from other studies, as risks in the present analyses
were estimated in normal and overweight patients and compared to obese patients, stratified by
previous CVD statuses. However a recent study by Logue et al. explored the relationship between
BMI and mortality in T2DM patients, reported that males and females of normal weights had
significantly increased mortality risks compared to overweight patients – by 22% and 32%,
respectively 152
.
The clinical research question discussed in Chapter 7 is an exploration of HbA1c trajectories in
response to treatment strategy, for different BMI categories at the time of diagnosis with T2DM,
which is a novel approach. A statistical issue discussed in this chapter is the performance of the

129
multiple imputation method, assessed by comparing estimates obtained from analyses of the
incomplete data set and an imputed data set, which estimated the missing values of the
longitudinally measured variables.
The trajectory analysis showed that patients who received intensive treatment had significantly
higher levels of HbA1c over the five years immediately before death or censoring; this effect was
observed for patients within each of normal, overweight or obese BMI categories at the time of
diagnosis. Patients of a normal weight also had higher HbA1c levels, despite being intensively
treated with medication(s) aimed at controlling (lowering) HbA1c. Analysis of the change in
HbA1c over the five years immediately before death showed an increased mortality risk for those in
each of the three BMI categories. These inceased risks were clinically, though not statistically,
significant and are directly associated with the obesity paradox 174
in T2DM patients. The overall
trajectories of HbA1c were not significantly different for patients who died and those who remained
alive, within each of the BMI categories. However, in obese patients, HbA1c levels were
significantly lower in those patients who died during the follow-up period.
The novelty of this analysis and the uniqueness of the study is that, unlike most other studies which
have explored mortality risks associated with weight gain and transitions of glycaemic levels within
different categories of BMI 72,155,156,183
, this study focused on the trajectories of HbA1c in each of
these BMI categories.
The adequacy of multiple imputation in dealing with missing data in clinical research was examined
in relation to the HbA1c analyses. It has been shown that multiple imputation is a very effective
method for dealing with missing data, even when a relatively small number of imputations are made
84,188. The original longitudinal data set of 7030 patients was missing almost 20% of the HbA1c data
for each time point. However, when comparing results from the original data and the imputed data,
these were very similar for both. This suggests that, despite its incompleteness, the dataset can
provide useful insights into disease progression in diabetic patients

130
8.2: Limitatatios of This Thesis
Some of the main limitations are described below.
Data for some key variables were not available. These included:
1. Ethnicity
2. Changes in socio-economic variables over time
3. More detailed data regarding lifestyle factors
a. Smoking status over time, intensity of smoking, cigerettes per day
b. Dietary habits
c. Physical exercise
4. Compliance with medication, doasages
5. Cause-specific mortality
The population of the United Kingdom is a mixture of many different ethnic groups 189
. The
analyses in this thesis could not account for the possible metabolic differences between ethnic
groups, as well as differences in body structure. Socio-economic and demographic data were
available for the time of diagnosis, but not for subsequent time points, so changes during the
follow-up period could not be accounted for.
It is the usual practice for clinicians to advise patients to make lifestyle changes, by modifying diet,
exercise and smoking habits, for example. This dataset did not have information regarding any
advice that was given or possible changes made by patients in response, and so these could not be
included in analyses. Similarly, data concerning changes to smoking status were unavailable. It was
therefore not possible to measure the protective effects of post-diagnosis smoking cessation in these
diabetic patients. Information about the number of cigerettes smoked per day, as well as changes to
smoking habits made, was not available, and so patients could not be categorised according to the
intensity of their smoking.
However, the major limitation of the thesis is that it was focused on macrovascular disease, and the
microvascular complications of T2DM were not considered. Long term T2DM is associated with
microvascular diseases, such as diabetic retinopathy and diabetic neuropathy. Similarly, changes in
related biochemical parametes, such as serum creatinine and albumin over time, were not addressed.

131
8.3: Recommendations for Future Research
The development of T2DM could occur as a result of an interplay between genes and environmental
factors, which influences insulin producing cells in the body. T2DM is a chronic, metabolic
disorder affecting vital systems of the body, such as the brain, liver, heart and kidneys. A complex
interplay of various factors, such as age, smoking habits, alcohol consumption, dietary
modifications, and adherence to clinical interventions, directly influence the glycaemic profile of a
person who has been diagnosed with the disease. The clinical management of T2DM encompasses a
variety of approaches, including lifestyle modifications and clinical interventions. The standard
clinical treatment plan for T2DM is illustrated in Figure 8.1.
Figure 8.1: Clinical management of T2DM 190
This thesis outlines the increased risk of CVD and mortality for women who smoke. Although this
research did not aim to explore the driving factors that cause these increased risks in women, they
might be attributable to under-treatment or sub-optimal clinical management of diabetic women.
Therefore, further research should be conducted to explore these reasons further.
Body types and dietary intakes vary between different ethnic groups; further research is needed to
examine these differences, so that clinical management of the disease can be improved. Changes in

132
glycaemic levels are also associated with socio-economic status, an effect that is possibly mediated
by lifestyle patterns. Research should also aim to address glycaemic transitions, in relation to the
overweight/obesity transition, with a lengthy follow-up time, so as to inform optimal clinical
management of the disease.
8.4: Conclusions
The prevalence of T2DM is at an all-time high, leading to increased concern from patients,
clinicians, researchers and policy makers. Although much research is being conducted in this field,
victims of this disease and the number of complications associated with it are also increasing in
both developed and developing countries. The objective of this thesis was to generate conclusions
that will assist the scientific community and clinicians to provide better clinical management and
improved quality of life for patients.
Earlier diagnosis and appropriate clinical management of T2DM will result in increased survival
and improved quality of life for patients. It is of great importance to maintain good control of blood
pressure and glycaemic levels in T2DM patients, as this research has demonstrated that a higher
mortality risk is associated with higher and lower blood pressures (SBP, DBP) and higher levels of
HbA1c. The existence of the obesity paradox could be due to the overconfidence of patients who
have a normal BMI at the time of their diagnosis with T2DM. Such patients may feel that they are
at a low risk and therefore do not need to modify their lifestyles to the degree that an overweight or
obese patient should. Clinicians must emphasise the chronic, but controllable, nature of this disease,
and that only with proper lifestyle modifications and theraputic management can future risks be
minimised.
Overall, the findings suggest that more attention must be given to glycaemic and blood pressure
controls in T2DM patients. Also, appropriate clinical management of the disease has to be ensured
in women and patients of normal weight. Awareness of the potential benefits of smoking cessation,
and the benefits of lifestyle changes, in relation to the increased chance of survival they offer, has to
be enhanced. Further research, aimed at primary prevention and improved management and control
of T2DM, is needed to reduce the incidence, prevalence, and complications of this multi-faceted
disease.

133
References
1. Chowdhury TA. Diabetes management in clinical practice. London: Springer; 2014.
2. Idf diabetes atlas International Diabetes Federation. (Accessed 3 March 2014, at
http://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf.)
3. Diabetes treatment. (Accessed 1 December, 2014, at
http://www.emcell.com/en/list_of_diseases/diabetes_treatment.htm.)
4. Cost of diabetes. (Accessed 25 February, 2015, at http://www.diabetes.co.uk/cost-of-
diabetes.html.)
5. Defronzo RA. Banting lecture. From the triumvirate to the ominous octet: A new paradigm
for the treatment of type 2 diabetes mellitus. Diabetes 2009;58:773-95.
6. //www.who.int/mediacentre/factsheets/fs312/en/index.html on 1July 2011.
7. Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and
microvascular complications of type 2 diabetes (ukpds 35): Prospective observational study. BMJ
2000;321:405-12.
8. Powers AC. Diabetes mellitus. In: Kasper dl, fauci as, longo dl, braunwald e, hauser sl,
jameson jl, editors. Harrison’s Principles of Internal Medicine 17th ed New York (NY): McGraw-
Hill 2008:2275-310.
9. Skyler JS, Bergenstal R, Bonow RO, et al. Intensive glycemic control and the prevention of
cardiovascular events: Implications of the accord, advance, and va diabetes trials: A position
statement of the american diabetes association and a scientific statement of the american college of
cardiology foundation and the american heart association. Diabetes Care 2009;32:187-92.
10. Ohkubo Y, Kishikawa H, Araki E, et al. Intensive insulin therapy prevents the progression
of diabetic microvascular complications in japanese patients with non-insulin-dependent diabetes
mellitus: A randomized prospective 6-year study. Diabetes Res Clin Pract 1995;28:103-17.
11. Fowler MJ. Microvascular and macrovascular complications of diabetes. Clinical Diabetes
2008;26:77-82.

134
12. Turnbull FM, Abraira C, Anderson RJ, et al. Intensive glucose control and macrovascular
outcomes in type 2 diabetes. Diabetologia 2009;52:2288-98.
13. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes
Care 2014;37:S14-S80.
14. Mostafa SA, Davies MJ, Srinivasan BT, Carey ME, Webb D, Khunti K. Should glycated
haemoglobin (hba1c) be used to detect people with type 2 diabetes mellitus and impaired glucose
regulation? Postgrad Med J 2010;86:656-62.
15. International diabetes federation. Idf diabetes atlas. International Diabetes Federation, 2014.
(Accessed 2 September 2014, at http://www.idf.org/diabetesatlas/6e/Update2013.)
16. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for
the year 2000 and projections for 2030. Diabetes Care 2004;27:1047-53.
17. Gakidou E, Mallinger L, Abbott-Klafter J, et al. Management of diabetes and associated
cardiovascular risk factors in seven countries: A comparison of data from national health
examination surveys. Bull World Health Organ 2011;89:172-83.
18. Roglic G, Unwin N. Mortality attributable to diabetes: Estimates for the year 2010. Diabetes
Res Clin Pract 2010;87:15-9.
19. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010
and 2030. Diabetes Research and Clinical Practice 2010;87:4-14.
20. Zimmet PZ, Magliano DJ, Herman WH, Shaw JE. Diabetes: A 21st century challenge. The
Lancet Diabetes & Endocrinology 2014;2:56-64.
21. Turner RC, Millns H, Neil HAW, et al. Risk factors for coronary artery disease in non-
insulin dependent diabetes mellitus: United kingdom prospective diabetes study (ukpds: 23). BMJ
1998;316:823-8.
22. Kothari V, Stevens RJ, Adler AI, et al. Ukpds 60: Risk of stroke in type 2 diabetes estimated
by the uk prospective diabetes study risk engine. Stroke; a journal of cerebral circulation
2002;33:1776-81.

135
23. Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA, Holman RR. Development and
progression of nephropathy in type 2 diabetes: The united kingdom prospective diabetes study
(ukpds 64). Kidney International 2003;63:225-32.
24. Huxley R, Barzi F, Woodward M. Excess risk of fatal coronary heart disease associated with
diabetes in men and women: Meta-analysis of 37 prospective cohort studies. BMJ 2006;332:73-8.
25. Peters SA, Huxley RR, Woodward M. Diabetes as risk factor for incident coronary heart
disease in women compared with men: A systematic review and meta-analysis of 64 cohorts
including 858,507 individuals and 28,203 coronary events. Diabetologia 2014;57:1542-51.
26. Peters SAE, Huxley RR, Woodward M. Diabetes as a risk factor for stroke in women
compared with men: A systematic review and meta-analysis of 64 cohorts, including 775?385
individuals and 12?539 strokes. The Lancet 2014;383:1973-80.
27. Kanaya AM, Grady D, Barrett-Connor E. Explaining the sex difference in coronary heart
disease mortality among patients with type 2 diabetes mellitus: A meta-analysis. Archives of
internal medicine 2002;162:1737-45.
28. Effects of intensive glucose lowering in type 2 diabetes. New England Journal of Medicine
2008;358:2545-59.
29. The ADVANCE Collaborative Group. Intensive blood glucose control and vascular
outcomes in patients with type 2 diabetes. New England Journal of Medicine 2008;358:2560-72.
30. VADT Study group. Glucose control and vascular complications in veterans with type 2
diabetes. N Engl J Med 2009;360:129-39.
31. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive
glucose control in type 2 diabetes. N Engl J Med 2008;359:1577-89.
32. Ray KK, Seshasai SRK, Wijesuriya S, et al. Effect of intensive control of glucose on
cardiovascular outcomes and death in patients with diabetes mellitus: A meta-analysis of
randomised controlled trials. Lancet 2009;373:1765-72.
33. Effect of intensive blood-glucose control with metformin on complications in overweight
patients with type 2 diabetes (ukpds 34). Uk prospective diabetes study (ukpds) group. Lancet
1998;352:854-65.

136
34. The effect of intensive treatment of diabetes on the development and progression of long-
term complications in insulin-dependent diabetes mellitus. The diabetes control and complications
trial research group. N Engl J Med 1993;329:977-86.
35. Patel A, MacMahon S, Chalmers J, et al. Effects of a fixed combination of perindopril and
indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus
(the advance trial): A randomised controlled trial. Lancet 2007;370:829-40.
36. The ACCORD Study Group. Effects of intensive blood-pressure control in type 2 diabetes
mellitus. New England Journal of Medicine 2010;362:1575-85.
37. Anderson RJ, Bahn GD, Moritz TE, Kaufman D, Abraira C, Duckworth W. Blood pressure
and cardiovascular disease risk in the veterans affairs diabetes trial. Diabetes Care 2011;34:34-8.
38. Stratton I, Cull C, Adler A, Matthews D, Neil H, Holman R. Additive effects of glycaemia
and blood pressure exposure on risk of complications in type 2 diabetes: A prospective
observational study (ukpds 75). Diabetologia 2006;49:1761-9.
39. Currie CJ, Peters JR, Tynan A, et al. Survival as a function of hba1c in people with type 2
diabetes: A retrospective cohort study. The Lancet 2010;375:481-9.
40. Gebregziabher M, Egede LE, Lynch CP, Echols C, Zhao Y. Effect of trajectories of
glycemic control on mortality in type 2 diabetes: A semiparametric joint modeling approach. Am J
Epidemiol 2010;171:1090-8.
41. Holman RR, Paul SK, Bethel MA, Neil HA, Matthews DR. Long-term follow-up after tight
control of blood pressure in type 2 diabetes. N Engl J Med 2008;359:1565-76.
42. Montori VM, Fernandez-Balsells M. Glycemic control in type 2 diabetes: Time for an
evidence-based about-face? Ann Intern Med 2009;150:803-8.
43. Cederholm J, Zethelius B, Nilsson PM, Eeg-Olofsson K, Eliasson B, Gudbjornsdottir S.
Effect of tight control of hba1c and blood pressure on cardiovascular diseases in type 2 diabetes: An
observational study from the swedish national diabetes register (ndr). Diabetes Res Clin Pract
2009;86:74-81.
44. Maddox TM, Ross C, Tavel HM, et al. Blood pressure trajectories and associations with
treatment intensification, medication adherence, and outcomes among newly diagnosed coronary
artery disease patients. Circ Cardiovasc Qual Outcomes 2010;3:347-57.

137
45. Hemkens LG, Grouven U, Bender R, et al. Risk of malignancies in patients with diabetes
treated with human insulin or insulin analogues: A cohort study. Diabetologia 2009;52:1732-44.
46. Jonasson JM, Ljung R, Talback M, Haglund B, Gudbjornsdottir S, Steineck G. Insulin
glargine use and short-term incidence of malignancies-a population-based follow-up study in
sweden. Diabetologia 2009;52:1745-54.
47. Colhoun HM. Use of insulin glargine and cancer incidence in scotland: A study from the
scottish diabetes research network epidemiology group. Diabetologia 2009;52:1755-65.
48. Currie CJ, Poole CD, Gale EA. The influence of glucose-lowering therapies on cancer risk
in type 2 diabetes. Diabetologia 2009;52:1766-77.
49. Pocock SJ, Smeeth L. Insulin glargine and malignancy: An unwarranted alarm. Lancet
2009;374:511-3.
50. De Vries F, van Staa TP, Leufkens HG. Proton pump inhibitors, fracture risk and selection
bias: Three studies, same database, two answers. Osteoporos Int 2011;22:1641-2.
51. Green J, Czanner G, Reeves G, Watson J, Wise L, Beral V. Oral bisphosphonates and risk of
cancer of oesophagus, stomach, and colorectum: Case-control analysis within a uk primary care
cohort. BMJ 2010;341.
52. Vries Fd. Two studies, same data source, two answers. BMJ 2010;341.
53. Newcomb PA, Trentham-Dietz A, Hampton JM. Bisphosphonates for osteoporosis
treatment are associated with reduced breast cancer risk. Br J Cancer 2010;102:799-802.
54. Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics—2010
update: A report from the american heart association. Circulation 2010;121:e46-e215.
55. Chan JC, Lau ES, Luk AO, et al. Premature mortality and comorbidities in young-onset
diabetes: A 7-year prospective analysis. The American journal of medicine 2014;127:616-24.
56. Xu L, Chan WM, Hui YF, Lam TH. Association between hba1c and cardiovascular disease
mortality in older hong kong chinese with diabetes. Diabetic medicine : a journal of the British
Diabetic Association 2012;29:393-8.
57. Huang ES, Liu JY, Moffet HH, John PM, Karter AJ. Glycemic control, complications, and
death in older diabetic patients: The diabetes and aging study. Diabetes Care 2011;34:1329-36.

138
58. Zhang Y, Hu G, Yuan Z, Chen L. Glycosylated hemoglobin in relationship to cardiovascular
outcomes and death in patients with type 2 diabetes: A systematic review and meta-analysis. PloS
one 2012;7:e42551.
59. Lenters-Westra E, Schindhelm RK, Bilo HJ, Slingerland RJ. Haemoglobin a1c: Historical
overview and current concepts. Diabetes Res Clin Pract 2013;99:75-84.
60. Bhaktha G, Nayak BS, Mayya S, Shantaram M. Is hba1c a risk factor for type 2 diabetic
subjects without macro and micro vascular complications? Archives of physiology and
biochemistry 2012;118:69-71.
61. Veloso AG, Siersma V, Heldgaard PE, de Fine Olivarius N. Patients newly diagnosed with
clinical type 2 diabetes mellitus but presenting with hba1c within normal range: 19-year mortality
and clinical outcomes. Primary care diabetes 2013;7:33-8.
62. Ismail-Beigi F, Moghissi E, Tiktin M, Hirsch IB, Inzucchi SE, Genuth S. Individualizing
glycemic targets in type 2 diabetes mellitus: Implications of recent clinical trials. Ann Intern Med
2011;154:554-9.
63. Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett WC. Obesity, fat distribution, and
weight gain as risk factors for clinical diabetes in men. Diabetes Care 1994;17:961-9.
64. Cederholm J, Gudbjornsdottir S, Eliasson B, Zethelius B, Eeg-Olofsson K, Nilsson PM.
Blood pressure and risk of cardiovascular diseases in type 2 diabetes: Further findings from the
swedish national diabetes register (ndr-bp ii). Journal of hypertension 2012;30:2020-30.
65. Vazquez LA, Rodriguez A, Salvador J, Ascaso JF, Petto H, Reviriego J. Relationships
between obesity, glycemic control, and cardiovascular risk factors: A pooled analysis of cross-
sectional data from spanish patients with type 2 diabetes in the preinsulin stage. BMC Cardiovasc
Disord 2014;14:153.
66. Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes
mellitus-present and future perspectives. Nat Rev Endocrinol 2012;8:228-36.
67. Milicevic Z, Raz I, Beattie S, et al. Natural history of cardiovascular disease in patients with
diabetes: Role of hyperglycemia. Diabetes Care 2008;31:S155 - S60.
68. Conus F, Rabasa-Lhoret R, Péronnet F. Characteristics of metabolically obese normal-
weight (monw) subjects. Applied Physiology, Nutrition, and Metabolism 2007;32:4-12.

139
69. Andersson C, van Gaal L, Caterson ID, et al. Relationship between hba1c levels and risk of
cardiovascular adverse outcomes and all-cause mortality in overweight and obese cardiovascular
high-risk women and men with type 2 diabetes. Diabetologia 2012;55:2348-55.
70. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes
care 2012;35:S64-S71.
71. Florez H C-FS. Beyond the obesity paradox in diabetes: Fitness, fatness, and mortality.
JAMA: The Journal of the American Medical Association 2012;308:619-20.
72. Carnethon MR, De Chavez PJ, Biggs ML, et al. Association of weight status with mortality
in adults with incident diabetes. JAMA : the journal of the American Medical Association
2012;308:581-90.
73. Ganz ML, Wintfeld N, Li Q, Alas V, Langer J, Hammer M. The association of body mass
index with the risk of type 2 diabetes: A case-control study nested in an electronic health records
system in the united states. Diabetology & metabolic syndrome 2014;6:50.
74. National Center for Chronic Disease P, Health Promotion Office on S, Health. Reports of
the surgeon general. The health consequences of smoking-50 years of progress: A report of the
surgeon general. Atlanta (GA): Centers for Disease Control and Prevention (US); 2014.
75. Is smoking harmful for diabetics? (Accessed 20 November 2014, at
http://www.quit.org.au/about/frequently-asked-questions/how-does-smoking-affect-my-
body/smoking-and-diabetes.html.)
76. Qin R, Chen T, Lou Q, Yu D. Excess risk of mortality and cardiovascular events associated
with smoking among patients with diabetes: Meta-analysis of observational prospective studies.
International journal of cardiology 2013;167:342-50.
77. Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart
disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior
myocardial infarction. New England Journal of Medicine 1998;339:229-34.
78. Lin GM, Li YH, Lin CL, Wang JH, Han CL. Gender differences in the impact of diabetes on
mortality in patients with established coronary artery disease: A report from the eastern taiwan
integrated health care delivery system of coronary heart disease (et-chd) registry, 1997-2006.
Journal of cardiology 2013;61:393-8.

140
79. Zhao W, Katzmarzyk P, Horswell R, Wang Y, Johnson J, Hu G. Sex differences in the risk
of stroke and hba1c among diabetic patients. Diabetologia 2014;57:918-26.
80. Reeves MJ, Bushnell CD, Howard G, et al. Sex differences in stroke: Epidemiology, clinical
presentation, medical care, and outcomes. The Lancet Neurology 2008;7:915-26.
81. Cooper C, Steinbuch M, Stevenson R, Miday R, Watts NB. The epidemiology of
osteonecrosis: Findings from the gprd and thin databases in the uk. Osteoporos Int 2010;21:569-77.
82. Hippisley-Cox J, Coupland C, Vinogradova Y, Robson J, May M, Brindle P. Derivation and
validation of qrisk, a new cardiovascular disease risk score for the united kingdom: Prospective
open cohort study. BMJ 2007;335:136.
83. Molenberghs G, Kenward MG. Missing data in clinical studies. Chichester; Hoboken, NJ:
Wiley; 2007.
84. Rubin D. Multiple imputation for non-response in surveys. New York John Wiley and
Sons; 1987.
85. Greenland S, Finkle WD. A critical look at methods for handling missing covariates in
epidemiologic regression analyses. Am J Epidemiol 1995;142:1255-64.
86. Klebanoff MA, Cole SR. Use of multiple imputation in the epidemiologic literature. Am J
Epidemiol 2008;168:355-7.
87. Nevalainen J, Kenward MG, Virtanen SM. Missing values in longitudinal dietary data: A
multiple imputation approach based on a fully conditional specification. Stat Med 2009;28:3657-69.
88. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in
epidemiological and clinical research: Potential and pitfalls. Bmj 2009;338:b2393.
89. Weiner MG, Barnhart K, Xie D, Tannen RL. Hormone therapy and coronary heart disease in
young women. Menopause 2008;15:86-93.
90. White IR, Carlin JB. Bias and efficiency of multiple imputation compared with complete-
case analysis for missing covariate values. Stat Med 2010;29:2920-31.
91. Rubin D. Multiple imputation for nonresponse in surveys: New York: John Wiley and Sons;
2004.

141
92. Delaney JA, Moodie EE, Suissa S. Validating the effects of drug treatment on blood
pressure in the general practice research database. Pharmacoepidemiol Drug Saf 2008;17:535-45.
93. DunningT, Freedman D. Modeling selection effects. Social Science Methodology Sage:
London 2008.
94. Carpenter JR, Kenward MG, White IR. Sensitivity analysis after multiple imputation under
missing at random: A weighting approach. Stat Methods Med Res 2007;16:259-75.
95. Daniels MJ, Hogan JW. Missing data in longitudinal studies:Strategies for bayesian
modeling and sensitivity analysis. Chapman & Hall/CRC, Boca Raton,2008.
96. Chesher A. The effect of measurement error. Biometrika 1991;78:451-62.
97. Zhou H, Pepe MS. Auxiliary covariate data in failure time regression. Biometrika
1995;82:139-49.
98. Zhou H, Wang CY. Failure time regression with continuous covariates measured with error.
Journal of the Royal Statistical Society: Series B (Statistical Methodology) 2000;62:657-65.
99. Liao X, Zucker DM, Li Y, Spiegelman D. Survival analysis with error-prone time-varying
covariates: A risk set calibration approach. Biometrics 2011;67:50-8.
100. Wu L, Liu W, Hu XJ. Joint inference on hiv viral dynamics and immune suppression in
presence of measurement errors. Biometrics 2010;66:327-35.
101. Diggle PJ, Sousa I, Chetwynd AG. Joint modelling of repeated measurements and time-to-
event outcomes: The fourth armitage lecture. Stat Med 2008;27:2981-98.
102. Tapsoba Jde D, Lee SM, Wang CY. Joint modeling of survival time and longitudinal data
with subject-specific changepoints in the covariates. Stat Med 2011;30:232-49.
103. Gprd™ database description. (Accessed 8 March 2014, at
http://www.itmat.upenn.edu/ctsa/acard/docs/all_Description_GPRD_FINAL.pdf )
104. General practice research database. (Accessed 1 March 2012, at
http://www.gprd.com/home/.)

142
105. Rasouli B, Grill V, Midthjell K, Ahlbom A, Andersson T, Carlsson S. Smoking is associated
with reduced risk of autoimmune diabetes in adults contrasting with increased risk in overweight
men with type 2 diabetes: A 22-year follow-up of the hunt study. Diabetes Care 2013;36:604-10.
106. Patja K, Jousilahti P, Hu G, Valle T, Qiao Q, Tuomilehto J. Effects of smoking, obesity and
physical activity on the risk of type 2 diabetes in middle-aged finnish men and women. Journal of
Internal Medicine 2005;258:356-62.
107. Galcera-Tomas J, Melgarejo-Moreno A, Garcia-Alberola A, et al. Prognostic significance of
diabetes in acute myocardial infarction. Are the differences linked to female gender? International
journal of cardiology 1999;69:289-98.
108. Gibson CL. Cerebral ischemic stroke: Is gender important[quest]. J Cereb Blood Flow
Metab 2013;33:1355-61.
109. Tonstad S, Rosvold EO, Furu K, Skurtveit S. Undertreatment and overtreatment with
statins: The oslo health study 2000-2001. J Intern Med 2004;255:494-502.
110. Lee WL, Cheung AM, Cape D, Zinman B. Impact of diabetes on coronary artery disease in
women and men: A meta-analysis of prospective studies. Diabetes Care 2000;23:962-8.
111. Fagard RH. Smoking amplifies cardiovascular risk in patients with hypertension and
diabetes. Diabetes Care 2009;32:S429-S31.
112. Jee SH, Foong AW, Hur NW, Samet JM. Smoking and risk for diabetes incidence and
mortality in korean men and women. Diabetes Care 2010.
113. Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J. Active smoking and the risk of type
2 diabetes: A systematic review and meta-analysis. JAMA : the journal of the American Medical
Association 2007;298:2654-64.
114. Chaturvedi N, Rai H, Ben-Shlomo Y. Lay diagnosis and health-care-seeking behaviour for
chest pain in south asians and europeans. Lancet 1997;350:1578-83.
115. Critchley Ja CS. Mortality risk reduction associated with smoking cessation in patients with
coronary heart disease: A systematic review. JAMA : the journal of the American Medical
Association 2003;290:86-97.

143
116. Sherman JJ. The impact of smoking and quitting smoking on patients with diabetes.
Diabetes Spectrum 2005;18:202-8.
117. Chaturvedi N, Stevens L, Fuller JH, Group TWHOMS. Which features of smoking
determine mortality risk in former cigarette smokers with diabetes? The world health organization
multinational study group. Diabetes Care 1997;20:1266-72.
118. Kengne AP, Nakamura K, Barzi F, et al. Smoking, diabetes and cardiovascular diseases in
men in the asia pacific region. Journal of Diabetes 2009;1:173-81.
119. Khan TA, Vohra HA, Paul S, Rosin MD, Patel RL. Axillary and tympanic membrane
temperature measurements are unreliable early after cardiopulmonary bypass. European journal of
anaesthesiology 2006;23:551-4.
120. Majeed A. Sources, uses, strengths and limitations of data collected in primary care in
england. Health Statistics Quarterly 2004;21:5-14.
121. Sadek AR, van Vlymen J, Khunti K, de Lusignan S. Automated identification of miscoded
and misclassified cases of diabetes from computer records. Diabetic medicine : a journal of the
British Diabetic Association 2012;29:410-4.
122. Curcin V, Bottle A, Molokhia M, Millett C, Majeed A. Towards a scientific workflow
methodology for primary care database studies. Statistical Methods in Medical Research
2010;19:378-93.
123. De Lusignan S, Khunti K, Belsey J, et al. A method of identifying and correcting miscoding,
misclassification and misdiagnosis in diabetes: A pilot and validation study of routinely collected
data. Diabetic Medicine 2010;27:203-9.
124. de Lusignan S, Nitsch D, Belsey J, et al. Disparities in testing for renal function in uk
primary care: Cross-sectional study. Family practice 2011;28:638-46.
125. Juutilainen A, Kortelainen S, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Gender
difference in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care
2004;27:2898-904.
126. Huxley RR, Woodward M. Cigarette smoking as a risk factor for coronary heart disease in
women compared with men: A systematic review and meta-analysis of prospective cohort studies.
The Lancet 2011;378:1297-305.

144
127. Wexler DJ, Grant RW, Meigs JB, Nathan DM, Cagliero E. Sex disparities in treatment of
cardiac risk factors in patients with type 2 diabetes. Diabetes Care 2005;28:514-20.
128. Luo M, Guan X, Luczak ED, et al. Diabetes increases mortality after myocardial infarction
by oxidizing camkii. The Journal of Clinical Investigation 2013;123:1262-74.
129. Nilsson PM, Cederholm J, Eeg-Olofsson K, et al. Smoking as an independent risk factor for
myocardial infarction or stroke in type 2 diabetes: A report from the swedish national diabetes
register. European Journal of Cardiovascular Prevention & Rehabilitation 2009;16:506-12.
130. Stamler J, Vaccaro O, Neaton JD, Wentworth D, Group TMRFITR. Diabetes, other risk
factors, and 12-yr cardiovascular mortality for men screened in the multiple risk factor intervention
trial. Diabetes Care 1993;16:434-44.
131. Hankey GJ, Anderson NE, Ting R-D, et al. Rates and predictors of risk of stroke and its
subtypes in diabetes: A prospective observational study. Journal of Neurology, Neurosurgery &
Psychiatry 2013;84:281-7.
132. Maas A, Appelman YEA. Gender differences in coronary heart disease. Netherlands Heart
Journal 2010;18:598-602.
133. Towfighi A, Zheng L, Ovbiagele B. Sex-specific trends in midlife coronary heart disease
risk and prevalence. Archives of internal medicine 2009;169:1762-6.
134. Grundtvig M, Hagen TP, German M, Reikvam Å. Sex-based differences in premature first
myocardial infarction caused by smoking: Twice as many years lost by women as by men.
European Journal of Cardiovascular Prevention & Rehabilitation 2009;16:174-9.
135. American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes
Care 2013;36:S11-S66.
136. Poulter NR. Blood pressure and glucose control in subjects with diabetes: New analyses
from advance. Journal of hypertension 2009;27:S3-S8 10.1097/01.hjh.0000354417.70192.be.
137. McBrien K, Rabi DM, Campbell N, et al. Intensive and standard blood pressure targets in
patients with type 2 diabetes mellitus: Systematic review and meta-analysis. Archives of internal
medicine 2012:1-8.

145
138. Lv J, Neal B, Ehteshami P, et al. Effects of intensive blood pressure lowering on
cardiovascular and renal outcomes: A systematic review and meta-analysis. PLoS Med
2012;9:e1001293.
139. Vamos EP, Harris M, Millett C, et al. Association of systolic and diastolic blood pressure
and all cause mortality in people with newly diagnosed type 2 diabetes: Retrospective cohort study.
British Medical Journal 2012;345.
140. van Hateren KJJ, Landman GWD, Kleefstra N, et al. Lower blood pressure associated with
higher mortality in elderly diabetic patients (zodiac-12). Age and Ageing 2010;39:603-9.
141. Rogers MAM, Ward K, Gure TR, et al. Blood pressure trajectories prior to death in patients
with diabetes. Diabetes care 2011;34:1534-9.
142. Pearson JD, Morrell CH, Brant LJ, Landis PK, Fleg JL. Age-associated changes in blood
pressure in a longitudinal study of healthy men and women. J Gerontol A Biol Sci Med Sci
1997;52.
143. Landahl S, Bengtsson C, Sigurdsson J, Svanborg A, Svardsudd K. Age-related changes in
blood pressure. Hypertension 1986;8:1044-9.
144. Bangalore S, Kumar S, Lobach I, Messerli FH. Blood pressure targets in subjects with type
2 diabetes mellitus/impaired fasting glucose. Circulation 2011.
145. Executive summary: Standards of medical care in diabetes—2010. Diabetes Care
2010;33:S4-S10.
146. Cooper-DeHoff RM, Gong Y, Handberg EM, et al. Tight blood pressure control and
cardiovascular outcomes among hypertensive patients with diabetes and coronary artery disease.
JAMA: The Journal of the American Medical Association 2010;304:61-8.
147. Williams B. Hypertension and the "j-curve". J Am Coll Cardiol 2009;54:1835-6.
148. Zeger SL, Liang KY. Models for longitudinal data: A generalized estimating equation
approach. Biometrics 1986;42:121-30.
149. Osher E, Stern N. Diastolic pressure in type 2 diabetes. Diabetes Care 2008;31:S249-S54.
150. Okayama A, Kadowaki T, Okamura T, Hayakawa T, Ueshima H, Group oboTNDR. Age-
specific effects of systolic and diastolic blood pressures on mortality due to cardiovascular diseases

146
among japanese men (nippon data80*). Journal of hypertension 2006;24:459-62
10.1097/01.hjh.0000209981.43983.cf.
151. Ma RCW, Yang X, Ko GTC, et al. Effects of systolic and diastolic blood pressures on
incident coronary heart disease and all-cause death in chinese women with type 2 diabetes: The
hong kong diabetes registry. Journal of Diabetes 2009;1:90-8.
152. Logue J, Walker JJ, Leese G, et al. Association between bmi measured within a year after
diagnosis of type 2 diabetes and mortality. Diabetes Care 2013;36:887-93.
153. McEwen LN, Kim C, Karter AJ, et al. Risk factors for mortality among patients with
diabetes: The translating research into action for diabetes (triad) study. Diabetes Care
2007;30:1736-41.
154. Doehner W, Erdmann E, Cairns R, et al. Inverse relation of body weight and weight change
with mortality and morbidity in patients with type 2 diabetes and cardiovascular co-morbidity: An
analysis of the proactive study population. International journal of cardiology 2012;162:20-6.
155. Heymsfield SB, Cefalu WT. Does body mass index adequately convey a patient's mortality
risk? JAMA : the journal of the American Medical Association 2013;309:87-8.
156. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with
overweight and obesity using standard body mass index categories: A systematic review and meta-
analysis. JAMA : the journal of the American Medical Association 2013;309:71-82.
157. Eknoyan G. Obesity, diabetes, and chronic kidney disease. Curr Diab Rep 2007;7:449-53.
158. Othman M, Kawar B, El Nahas AM. Influence of obesity on progression of non-diabetic
chronic kidney disease: A retrospective cohort study. Nephron Clin Pract 2009;113:c16-23.
159. Eknoyan G. Obesity and chronic kidney disease. Nefrologia 2011;31:397-403.
160. The english indices of deprivation 2004 (revised). 2007. (Accessed 18 September, 2011, at
http://www.communities.gov.uk/publications/communities/englishindices.)
161. Gray J, Millett C, O'Sullivan C, Omar RZ, Majeed A. Association of age, sex and
deprivation with quality indicators for diabetes: Population-based cross sectional survey in primary
care. Journal of the Royal Society of Medicine 2006;99:576-81.

147
162. Iacus SM, King G, Porro G. Causal inference without balance checking: Coarsened exact
matching. Political Analysis 2011.
163. Romero-Corral A, Somers VK, Sierra-Johnson J, et al. Normal weight obesity: A risk factor
for cardiometabolic dysregulation and cardiovascular mortality. European Heart Journal
2010;31:737-46.
164. Perry JR, Voight BF, Yengo L, et al. Stratifying type 2 diabetes cases by bmi identifies
genetic risk variants in lama1 and enrichment for risk variants in lean compared to obese cases.
PLoS genetics 2012;8:e1002741.
165. Greenberg JA. The obesity paradox in the us population. The American Journal of Clinical
Nutrition 2013;97:1195-200.
166. Hemmingsen B, Lund SS, Gluud C, et al. Targeting intensive glycaemic control versus
targeting conventional glycaemic control for type 2 diabetes mellitus. The Cochrane database of
systematic reviews 2013;11:Cd008143.
167. Bliss M. Resurrections in toronto: The emergence of insulin. Hormone research 2005;64
Suppl 2:98-102.
168. Rodbard H, Jellinger P, Davidson J, et al. Statement by an american association of clinical
endocrinologists/american college of endocrinology consensus panel on type 2 diabetes mellitus:
An algorithm for glycemic control. Endocrine Practice 2009;15:540-59.
169. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2
diabetes: A patient-centered approach. Position statement of the american diabetes association (ada)
and the european association for the study of diabetes (easd). Diabetologia 2012;55:1577-96.
170. Idf clinical guidelines task force. Global guideline for type 2 diabetes. Brussels:
International diabetes federation 2012.
171. Hauner H. Managing type 2 diabetes mellitus in patients with obesity. Treatments in
endocrinology 2004;3:223-32.
172. Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. Effect of intensive glucose
lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2
diabetes: Meta-analysis of randomised controlled trials2011.

148
173. Merlotti C, Morabito A, Ceriani V, Pontiroli AE. Prevention of type 2 diabetes in obese at-
risk subjects: A systematic review and meta-analysis. Acta diabetologica 2014.
174. Thomas G, Khunti K, Curcin V, et al. Obesity paradox in people newly diagnosed with type
2 diabetes with and without prior cardiovascular disease. Diabetes, obesity & metabolism
2014;16:317-25.
175. Goff Jr DC, Gerstein HC, Ginsberg HN, et al. Prevention of cardiovascular disease in
persons with type 2 diabetes mellitus: Current knowledge and rationale for the action to control
cardiovascular risk in diabetes (accord) trial. The American Journal of Cardiology 2007;99:S4-S20.
176. Selvin E, Marinopoulos S, Berkenblit G, et al. Meta-analysis: Glycosylated hemoglobin and
cardiovascular disease in diabetes mellitus. Ann Intern Med 2004;141:421-31.
177. Gerstein HC, Pogue J, Mann JFE, et al. The relationship between dysglycaemia and
cardiovascular and renal risk in diabetic and non-diabetic participants in the hope study: A
prospective epidemiological analysis. Diabetologia 2005;48:1749-55.
178. Arnold AM, Kronmal RA. Multiple imputation of baseline data in the cardiovascular health
study. American Journal of Epidemiology 2003;157:74-84.
179. Descalzo MA, Garcia VV, Gonzalez-Alvaro I, et al. Tackling missing radiographic
progression data: Multiple imputation technique compared with inverse probability weights and
complete case analysis. Rheumatology (Oxford, England) 2013;52:331-6.
180. Symmons DP. Methodological issues in conducting and analyzing longitudinal
observational studies in rheumatoid arthritis. The Journal of rheumatology Supplement 2004;69:30-
4.
181. Khan NF, Harrison S, Rose P. Validity of diagnostic coding within the general practice
research database: A systematic review. British Journal of General Practice 2010;60:e128-e36(9).
182. De Lusignan S. Codes, classifications, terminologies and nomenclatures: Definition,
development and application in practice. Informatics in Primary Care 2005;13:65–9.
183. Blume SW, Li Q, Huang JC, Hammer M, Graf TR. Variation in the risk of progression
between glycemic stages across different levels of body mass index: Evidence from a united states
electronic health records system. Current medical research and opinion 2014:1-10.

149
184. Sluik D, Boeing H, Montonen J, et al. Associations between general and abdominal
adiposity and mortality in individuals with diabetes mellitus. American Journal of Epidemiology
2011;174:22-34.
185. Unick JL, Beavers D, Jakicic JM, et al. Effectiveness of lifestyle interventions for
individuals with severe obesity and type 2 diabetes: Results from the look ahead trial. Diabetes Care
2011;34:2152-7.
186. Watson L, Wilson BP, Alsop J, Kumar S. Weight and glycaemic control in type 2 diabetes:
What is the outcome of insulin initiation? Diabetes, Obesity and Metabolism 2011;13:823-31.
187. Elobeid MA, Padilla MA, McVie T, et al. Missing data in randomized clinical trials for
weight loss: Scope of the problem, state of the field, and performance of statistical methods. PloS
one 2009;4:e6624.
188. Nakai M, Ke W. Review of the methods for handling missing data in longitudinal data
analysis. International Journal of Mathematical Analysis 2011;5:1-13.
189. Ethnicity in the united kingdom in 2011. (Accessed 9 November 2014, 2014,
190. Design and management of insulin therapy: Integrating the new treatment tools. (Accessed
11 November 2014, at http://www.medscape.org/viewarticle/563289.)

150
Ap
pen
dix
1:
Pro
port
ion
of
ava
ila
ble
an
d m
issi
ng
data
at
each
tim
e w
ind
ow
Pro
port
ion o
f av
aila
ble
and m
issi
ng d
ata
at e
ach t
ime
win
dow
on
anth
ropom
etri
c an
d c
linic
al p
aram
eter
s of
new
ly d
iagnose
d T
2D
M p
atie
nts
fro
m U
K
CP
RD
A.
BM
I
V
ali
d c
ase
s M
issi
ng
case
s
Vali
d c
ase
s M
issi
ng c
ase
s
Va
lid
ca
se
Mis
sin
g c
ase
s
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
Mo
nth
s N
%
N
%
6
49
28
8
58
.8
34
48
6
41.2
42
2
90
77
4
6.3
33698
53.7
7
8
12
50
9
39
.3
19
32
3
60
.7
12
452
30
54
.5
37
70
7
45.5
48
25585
45.2
31075
54.8
8
4
10
67
9
38
.8
16
83
3
61
.2
18
43
42
3
52
.9
38
70
7
47.1
54
22580
43.8
28955
56.2
9
0
92
67
38
.4
14
88
8
61
.6
24
39
51
2
49
.0
41
10
2
51.0
60
19437
42.3
26563
57.7
9
6
80
11
38
.3
12
90
4
61
.7
30
35
90
9
48
.1
38
71
1
51.9
66
17010
41.2
24284
58.8
1
02
69
54
37
.2
11
75
4
62
.8
36
32
35
5
47
.2
36
12
9
52.8
72
14591
40.4
21494
59.6
1
08
61
09
37
.4
10
24
2
62
.6
114
54
21
37
.2
91
59
62.8
150
2305
35.2
4252
64.8
1
86
65
9
30
.1
15
34
69
.9
120
46
99
37
.1
79
60
62.9
156
1909
34.6
3614
65.4
1
92
47
8
30
.8
10
76
69
.2
126
41
22
36
.5
71
73
63.5
162
1687
34.9
3150
65.1
1
98
31
0
26
.7
84
9
73
.3
132
35
94
36
.8
61
79
63.2
168
1322
33.4
3
2636
66.6
2
04
13
7
23
.0
45
8
77
.0
138
30
87
35
.4
56
23
64.6
174
1101
32.5
2284
67.5
2
10
45
1
5.6
2
44
84
.4
144
26
72
36
.1
47
39
63.9
180
854
32.3
1794
67.7

151
B.
SB
P
V
ali
d c
ase
s M
issi
ng
case
s
Vali
d c
ase
s M
issi
ng c
ase
s
Va
lid
ca
se
Mis
sin
g c
ase
s
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
Mo
nth
s N
%
N
%
6
583
70
69
.5
256
15
30
.5
48
3
30
15
5
8.1
2
38
07
4
1.9
9
0
12
01
1
49
.6
12
20
9
50
.4
12
582
44
70
.0
249
32
30
.0
54
2
93
47
5
6.8
2
23
45
4
3.2
9
6
10
37
9
49
.6
10
59
5
50
.5
18
560
10
68
.0
263
38
32
.0
60
2
51
11
5
4.5
2
09
89
4
5.5
1
02
91
34
4
8.7
9
63
4
51
.3
24
515
30
63
.8
292
93
36
.2
66
2
19
28
5
3.0
1
94
83
4
7.0
1
08
78
96
4
8.2
8
50
1
51
.8
30
467
14
62
.5
280
86
37
.5
72
1
87
77
5
1.9
1
74
21
4
8.1
1
14
70
61
4
8.2
7
57
5
51
.8
36
418
47
60
.9
268
15
39
.1
78
1
62
43
5
0.9
1
56
96
4
9.1
1
86
60
93
4
7.9
6
61
9
52
.1
42
376
53
59
.8
252
96
40
.2
84
1
38
39
5
0.2
1
37
42
4
9.8
1
26
54
01
4
7.6
5
93
6
52
.4
132
4
663
4
7.5
5
145
5
2.5
162
2
18
4
45
.0
26
70
5
5.0
1
92
63
0
40
.4
92
9
59
.6
138
4
043
4
6.2
4
705
5
3.8
168
1
71
2
43
.1
22
59
5
6.9
1
98
41
9
35
.9
74
7
64
.1
144
3
487
4
6.8
3
956
5
3.2
174
1
45
7
42
.9
19
39
5
7.1
2
04
19
3
32
.2
40
7
67
.8
150
2
997
4
5.5
3
590
5
4.5
180
1
13
0
42
.5
15
27
5
7.5
2
10
77
2
6.6
2
12
7
3.4
156
2
479
4
4.7
3
068
5
5.3
186
8
76
3
9.6
1
33
4
60
.4

152
C.
DB
P
V
ali
d c
ase
s M
issi
ng
case
s
Vali
d c
ase
s M
issi
ng c
ase
s
Va
lid
ca
se
Mis
sin
g c
ase
s
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
6
583
68
69
.5
256
17
30
.5
48
3
30
10
5
8.1
2
38
12
4
1.9
9
0
12
01
2
49
.6
12
20
8
50
.4
12
5
8245
7
0.0
2
4931
3
0.0
54
2
93
46
5
6.8
2
23
46
4
3.2
9
6
10
38
0
49
.5
10
59
4
50
.5
18
5
6005
6
8.0
2
6342
3
2.0
60
2
51
13
5
4.5
2
09
87
4
5.5
1
02
91
35
4
8.7
9
63
3
51
.3
24
5
1526
6
3.8
2
9297
3
6.2
66
2
19
28
5
3.0
1
94
83
4
7.0
1
08
78
97
4
8.2
8
50
0
51
.8
30
4
6713
6
2.5
2
8087
3
7.5
72
1
87
74
5
1.9
1
74
24
4
8.1
1
14
70
62
4
8.3
7
57
4
51
.7
36
4
1845
6
0.9
2
6817
3
9.1
78
1
62
42
5
0.9
1
56
97
4
9.1
1
86
60
93
4
7.9
6
61
9
52
.1
42
3
7652
5
9.8
2
5297
4
0.2
84
1
38
40
5
0.2
1
37
41
4
9.8
1
26
54
02
4
7.6
5
93
5
52
.4
132
4
663
4
7.5
5
145
5
2.5
162
2
18
4
45
.0
26
70
5
5.0
1
92
63
0
40
.4
92
9
59
.6
138
4
043
4
6.2
4
705
5
3.8
168
1
71
2
43
.1
22
59
5
6.9
1
98
41
8
35
.8
74
8
64
.2
144
3
487
4
6.8
3
596
5
3.2
174
1
45
8
42
.9
19
38
5
7.1
2
04
19
3
32
.2
40
7
67
.5
150
2
997
4
5.5
3
590
5
4.5
180
1
13
0
42
.5
15
27
5
7.5
2
10
77
2
6.6
2
12
7
3.4
156
2
478
4
4.7
3
069
5
5.3
186
8
76
3
9.6
1
33
4
60
.4

153
D.
Hb
A1
c
V
ali
d c
ase
s M
issi
ng
case
s
Vali
d c
ase
s M
issi
ng c
ase
s
Va
lid
ca
se
Mis
sin
g c
ase
s
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
Mon
ths
N
%
N
%
6
381
75
45
.6
456
16
54
.4
48
2
67
56
4
7.2
2
99
40
5
2.8
9
0
10
01
1
41
.4
14
17
4
58
.6
12
4
6325
5
5.8
3
6701
4
4.2
54
2
37
55
4
6.1
2
78
24
5
3.9
9
6
86
73
4
1.4
1
22
59
5
8.6
18
4
4767
5
4.5
3
7441
4
5.5
60
2
03
14
4
4.1
2
57
04
5
5.9
1
02
76
85
4
1.1
1
10
33
5
8.9
24
4
0312
5
0.0
4
0360
5
0.0
66
1
79
14
4
3.4
2
33
88
5
6.6
1
08
66
18
4
0.5
9
74
2
59
.5
30
3
7352
5
0.0
3
7303
5
0.0
72
1
54
71
4
2.8
2
06
49
5
7.2
1
14
60
21
4
1.2
8
57
7
58
.8
36
3
3314
4
8.6
3
5201
5
1.4
78
1
33
88
4
2.0
1
84
66
5
8.0
1
86
51
69
4
0.8
7
50
7
59
.2
42
3
0290
4
8.2
3
2523
5
1.8
84
1
14
69
4
1.7
1
60
67
5
8.3
1
26
45
73
4
0.5
6
72
4
59
.5
132
4
026
4
1.2
5
754
5
8.8
162
1
87
6
38
.8
29
64
6
1.2
1
92
52
7
33
.9
10
26
1
.2
138
3
450
3
9.5
5
280
6
0.5
168
1
49
6
37
.7
24
69
6
2.3
1
98
35
8
30
.7
80
7
69
.3
144
2
969
4
0.0
4
456
6
0.0
174
1
28
1
37
.8
21
07
6
2.2
2
04
16
0
26
.8
43
8
73
.2
150
2
625
3
9.9
3
946
6
0.1
180
9
60
3
6.2
1
69
3
63
.8
21
0
59
2
0.6
2
28
7
9.4
156
2
103
3
8.0
3
427
6
2.0
186
7
62
3
4.7
1
43
3
65
.3

154
Appendix 2: STATA syntax for multiple imputation
set seed 4385
mi set mlong
mi register imp A1c1 A1c2 A1c3 A1c4 A1c5 A1c6 A1c7 A1c8 A1c9 A1c10
mi impute mvn A1c1 A1c2 A1c3 A1c4 A1c5 A1c6 A1c7 A1c8 A1c9 A1c10=AGEGE65 SEX
HBA1C6 i.CVDINT CPM MT2, add(100)
mi reshape long A1c, i(PTID) j(Index1)
mi estimate: xtgee A1c AGEGE65 SEX HBA1C6 CPM i.CVDINT MT2 if bmi6cat==0,
family(gaussian) link(identity) corr(ind)
mi estimate: xtgee A1c AGEGE65 SEX HBA1C6 CPM i.CVDINT MT2 if bmi6cat==1,
family(gaussian) link(identity) corr(ind)
mi estimate: xtgee A1c AGEGE65 SEX HBA1C6 CPM i.CVDINT MT2 if bmi6cat==2,
family(gaussian) link(identity) corr(ind)



![[XLS]assets.publishing.service.gov.uk · Web viewFEV1 ref values - men Analysis - smokers - men Years at stage diagnosed at 55 Impact assumptions >> Progression analysis Life expectancy](https://static.fdocuments.in/doc/165x107/5af1fea37f8b9ac62b90ab04/xls-viewfev1-ref-values-men-analysis-smokers-men-years-at-stage-diagnosed.jpg)