
Disease and Lifestyle. Hertzler’s Hopes Health care is available (to all) (in Kansas) – But...
21
Disease and Lifestyle
-
Upload
shannon-nicholson -
Category
Documents
-
view
214 -
download
0
Transcript of Disease and Lifestyle. Hertzler’s Hopes Health care is available (to all) (in Kansas) – But...

Disease and Lifestyle

Hertzler’s Hopes
• Health care is available (to all) (in Kansas)– But public ignores, distrusts
• Health insurance is becoming available (but big city palace hospitals are too costly)
• Medical advertising as quackery

Hertzler, the doctor-confessor, and the new model human
• not organic disease but social-existential– Rape– Fertility issues (too little or too much)
• Change in economic status of children• Neglected and abused children
– Unrequited love– Anger– Grief– Ageing
• “all right they have high or low blood pressure and there is not use making them miserable either mentally or physical y by trying to do what just can’t be done. If they get pneumonia or a brain hemorrhage you know a kind Providence has not forgotten them.” (303)
– Dying• “Nowadays the doctor more or less ignores the bedside of the dying.”

What has changed?
• “Nervousness… not a disease but a state and one must learn to live with one’s self”– “Group practice is unsuited to the discovery of
these intimate details”
• Hertzler’s day– Society imprisons, doctors liberate
• Our day– Society liberates, doctors ….

New Medical possibilities• Amputation – authenticity or perversion?
– Apotemnophilia– Being stuck in the wrong body (anorexia precedent, sexual
reassignment) • Depression
– the conquest of invalidism or the legitimation of melancholia or the new hysteria
– Female=pathological• What produces a response cures a disease
• Anger and Polio– From dependency to disability rights
• New communities or out of control individualism?

The u.s. health care system

Costs and efficiency
• US ~ 15 % GNP, 1 of 6 $ in federal budget• Canada ~ 10% GNP (others 6-10%)• US 5.5 doctor visits/yr• Germany 12 doctor visits/yr• IMR Japan: 50% of US IMR• Administrative staff:bed
– Germany 1:7; USA 1:1
• Administrative costs, public and private– Canada 1.4%; USA 5.9%

WHO World Health Report 2006 (most recent figures for 2003)
Health care % of GDP
Health care of govt as % total govt expenditure
Govt expenditure on health care as % of total expenditure on health care
Netherlands 9.8 62.4 12.4
France 10.1 76.3 14.2
United Kingdom 8 85.7 15.8
Canada 9.9 69.7 16.7
Sweden 9.4 85.2 13.6
USA 15.2 44.6 18.5

Causes of high health care costs
• Need as supply• Over proceduring and information glut (x-ray, MRI,
or both?); xs false positives• Industry lobbying: horrible Canadian drugs• Duplication of services (gps, specialists, repeat
services)• Death as optional
– 90% of federal spending in last few months of life– .8% prevention
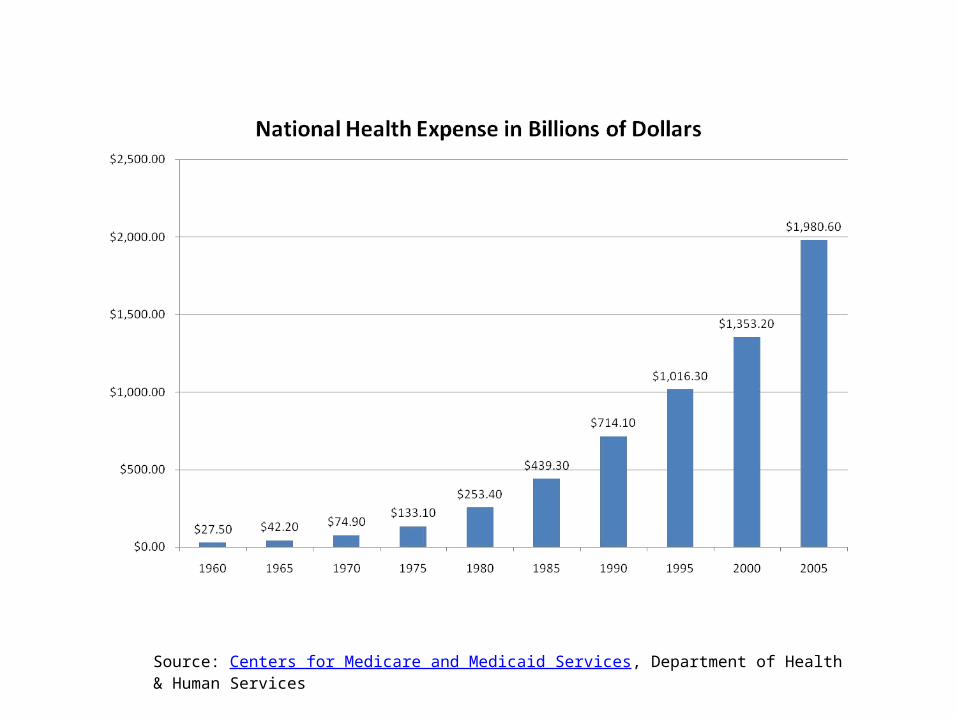
Source: Centers for Medicare and Medicaid Services, Department of Health & Human Services

Source: Centers for Medicare and Medicaid Services, Department of Health & Human Services

Source: Centers for Medicare and Medicaid Services, Department of Health & Human Services

• Varieties of health care provision• HMO — free access or standard• Capitation systems/contract systems• Indemnification insurance/major medical
(Blue Cross/Blue Shield• Medicare (2.1% of income)• Single payer?

General problems
• 1. For profit + capitation = underprovision of service • Precertification, Service review• 2. Indemnification + free access = overprovision of medical services• What is medical need?• If medical services are profit making activities there will be incentive to
use more of them — to create medical demand (flexible demand).• If medical services must be provided under a set fee (capitation) there
will be incentive to use less of them (inflexible demand)• If medical services are charged at cost, there will be neither incentive nor
disincentive to use services.– But… what is cost?
• The role of the gatekeeper (pcp)

The American Hospital
• 40% over capacity• Hospital consolidation• Subsidy of charity care• Iatrogenic infection — nosocomial (resistant
bacteria)• Mistakes with medication• The rise of the patient care technician• Institute of Medicine, NAS, 7/2000 — hospital error,
100,000 deaths/year

The Hill-Burton Act, 1946
• Purpose: expand supply of hospitals to underserved areas by offering partial federal funds and accelerated depreciation– Underserved areas can’t meet matching funds
expectations– Accelerated depreciation leads to incentive to
expand, needed or not– More procedures to pay for more technology– Result: supply-driven medical industry: hospital
occupancy 60%

HMO Origins: what do HMOs have to do with health maintenance?
• Against the threat of socialized medicine — a private sector solution
• Health Maintenance Act of 1973• Paul Elwood, Jackson Hole Conferences• Collects fees-- contracts with practitioners to
provide all necessary services

Presumptions of HMOs
• The Mayo model/1st generation hmo• 1. Coordination of pcp to coordinate with
specialists• 2. Emphasis on prevention, vaccination,
healthy behavior, screening• 3. Use of primary (family) doctor, over the
impersonal clinic• 4. Reduce cost through share facilities

The fate of HMOs
• Away from the Mayo clinic• Non-profit to profit• Control of Doctors to control by insurance providers• Away from prevention• Gatekeepers as naysayers — bonuses for cherry-picking
and cheapness• Precertification/prescription restriction/service review• Lack of concern with follow up care• Better deals for bigger customers/providers

Improvements of HMOs?
• Right to specialists• Right to information about finances• Independent review of complaints• Emergency room access• HMOs as regulated utilities• End of for-profit? Minnesota, Connecticut

Who should decide?
• Individual: everyone should get all they ask?• Provider: buy anything you can afford?• Insurance companies: we can get healthy
people better bargains• Society: medicine is an element of equality












![Paper Trails: Missing Manuscripts / Lost Livesusers.clas.ufl.edu/burt/ book chapter three[1].doc · Web viewTurnagainst his critique of deconstrucitonas thwarted messianism—ignores](https://static.fdocuments.in/doc/165x107/5e78aa6e7299a80e4c649a0d/paper-trails-missing-manuscripts-lost-book-chapter-three1doc-web-view-turnagainst.jpg)





