Discovering Medically Complex Patients · Discovering Medically Compromised Patients ples and basic...
24
Discovering Medically Complex Patients Chapter 18 2002 William H. Crawford, Jr. D.D.S., M.S. All rights reserved. Copying for commercial purposes is prohibited. 351 Outline Objectives A. Introduction 1. Dentistry’s Transition toward Biology and Medi- cine 2. The Need to Treat Medically Complex Patients B. Who are Medically Complex Patients? C. Discovering, Evaluating, and Managing Medically Complex Patients—An Overview D. Discovering Medically Complex Patients 1. The Health History a. Standard Health Questionnaires b. The Health History Interview 2. Physical Examination of Dental Patients a. Vital Signs b. Examination Methods c. Observation of a Patient’s General Appearance and Behavior d. Inspection and Palpation of the Head and Neck e. Measurement of Vital Signs 3. The Oral Soft Tissue Examination 4. Radiographic Examination E. Summaries 1. Components of Discovering Medically Complex Patients 2. Topic Sentence Summary 3. Questions Used in the ADA Short Health History Form 4. Questions to Ask New Dental Patients Concerning Past Medical Problems 5. Physical Examination in Dentistry 6. Technique for Measuring Blood Pressure 7. Normal Vital Signs 8. Oral Soft Tissue Examination 9. High Risk Areas for Oral Squamous Cell Carci- noma and Minor Salivary Gland Malignancies F. Study Questions After completion of this chapter, the student should be able to 1. write and identify definitions for the following terms: auscultation, brachial artery, bradycardia, chief com- plaint, family history, history of present illness, identify, inspection, Korotkoff sounds, observation, palpation, past medical history, percussion, pulse, review of sys- tems, social history, and tachycardia. 2. write and identify the relationship between longevity and outpatient medical care to increased numbers of medically complex patients seeking dental care. 3. list and identify seven categories of medically complex patients. 4. list and identify two basic steps in discovering medically complex patients 5. list and identify the six components of a health history. 6. write and identify the overall purpose of the history questionnaire. 7. list and identify ten questions to ask a new patient dur- ing a health history interview. 8. write and identify a question to ask all returning patients regarding their medical status. 9. list and identify five vital signs to be measured or assessed during a physical examination. 10. write and identify the normal values for the five vital signs measured or assessed during a physical examina- tion.
Transcript of Discovering Medically Complex Patients · Discovering Medically Compromised Patients ples and basic...
Discovering Medically Complex Patients
Chapter 18
2002 William H. Crawford, Jr. D.D.S., M.S. All rights reserved. Copying for commercial purposes is prohibited.
351
Outline Objectives
A. Introduction
1. Dentistry’s Transition toward Biology and Medi-cine
2. The Need to Treat Medically Complex Patients
B. Who are Medically Complex Patients?
C. Discovering, Evaluating, and Managing Medically Complex Patients—An Overview
D. Discovering Medically Complex Patients
1. The Health Historya. Standard Health Questionnairesb. The Health History Interview
2. Physical Examination of Dental Patientsa. Vital Signsb. Examination Methodsc. Observation of a Patient’s General Appearance
and Behaviord. Inspection and Palpation of the Head and Necke. Measurement of Vital Signs
3. The Oral Soft Tissue Examination4. Radiographic Examination
E. Summaries
1. Components of Discovering Medically Complex Patients
2. Topic Sentence Summary3. Questions Used in the ADA Short Health History
Form4. Questions to Ask New Dental Patients Concerning
Past Medical Problems5. Physical Examination in Dentistry6. Technique for Measuring Blood Pressure7. Normal Vital Signs8. Oral Soft Tissue Examination9. High Risk Areas for Oral Squamous Cell Carci-
noma and Minor Salivary Gland Malignancies
F. Study Questions
After completion of this chapter, the student should be able to1. write and identify definitions for the following terms:
auscultation, brachial artery, bradycardia, chief com-plaint, family history, history of present illness, identify, inspection, Korotkoff sounds, observation, palpation, past medical history, percussion, pulse, review of sys-tems, social history, and tachycardia.
2. write and identify the relationship between longevity and outpatient medical care to increased numbers of medically complex patients seeking dental care.
3. list and identify seven categories of medically complex patients.
4. list and identify two basic steps in discovering medically complex patients
5. list and identify the six components of a health history.6. write and identify the overall purpose of the history
questionnaire.7. list and identify ten questions to ask a new patient dur-
ing a health history interview.8. write and identify a question to ask all returning patients
regarding their medical status.9. list and identify five vital signs to be measured or
assessed during a physical examination.10. write and identify the normal values for the five vital
signs measured or assessed during a physical examina-tion.

352
Oral Medicine
Introduction
Definition of Medicine: “…the art or science of restoring or preserving health or physical con-dition, as by means of drugs, surgical operations or appliances, or manipulations: often divided into medicine proper, surgery, and obstetrics.”
Definition of Dentistry: “…the profession or science dealing with the prevention and treatment of diseases and malformations of the teeth, gums, and oral cavity, and the removal, correction, and replacement of decayed, damaged, or lost parts, including such operations as the filling and crowning of teeth, the straightening of teeth, and the construction of artificial dentures.”
Dentistry’s Transition Toward Biology and Medicine
Some believe that dentistry should merge with medicine.For years, dental visionaries have argued eloquently for dentistry to become a specialty of medicine. They point to examples of such arrangements in other countries. They emphasize that the same sorts of tissues and systems are found in and around the oral cavity as are found elsewhere. And they point to the increasing reliance of dentistry upon medicine and medicine upon dentistry in the treatment of patients. While an actual fusion of American medicine and dentistry will not occur any time soon, there is no doubt that an important transition is occur-ring within dentistry, a transition in which biologic principles and medical procedures are adopted for treatment of dental patients.
Dentistry is moving toward reliance on biology and disease prevention.Dentistry is moving from a heavy reliance on physical principles and a reparative approach to one that relies more upon biologic principles and a preventive approach to dental care. Medi-cine made this transition some years ago. The artificial heart represents medicine’s past reli-ance on a physical-reparative approach. The recent identification of the gene that may cause breast cancer exemplifies the current use of the biologic-preventive approach. In dentistry, the bonding of new materials to tooth structure and the development of dental implants are but two examples of the use of biologic principles to provide dental care. More recently, bone has been grown within cavities to cover an exposed pulps. Such advances will accelerate dentistry’s bio-logic transformation.
The Need to Treat Medically Complex Patients
It used to be that sick patients didn’t come to dental offices.In the past, dentists treated only patients who were in good health—sick patients didn’t seek dental care because they were confined or too ill. Now, for example, patients receive cancer chemotherapy as out-patients; they live at home, carry on a relatively normal life that includes seeking dental care.
More patients will be older than before; most will be under medical care.Patients are living longer. Life expectancy has increased greatly over the past several decades. Today the average life expectancy is 75 years; it was 54 years earlier in the century. The older members of US population will increase greatly in numbers over the next 30–40 years. In fact, it is estimated that 30 years from now, 3% of the population, or 8.8 million persons, will be 85 years or older. Most of these older people will be under medical treatment for one or several diseases.
Dental practitioners will increasingly treat medically complex patients.All this means, of course, that dentists and dental hygienists will be providing dental care to more and more people who have more and more serious underlying medical conditions. Put another way, dentists and dental hygienists will treat more and more medically complex patients. In order to cope with these trends, dental practitioners need to understand biologic principles, acquire preventive attitudes, and learn basic medical procedures. Shortly, it will no longer be optional for dentists to safely treat medically complex patients. Since biologic princi-
Discovering Medically Compromised Patients
ples and basic medical procedures are part of the education of all dentists, it is reasonable for the public to expect dentists to provide safe care for most medically complex patients.
Who Are Medically Complex Patients?
Most patients will not identify themselves as medically complex.Occasionally a patient will wish to be identified as a medically complex patient. Such patients are usually under a physician’s care for some significant malady. They are concerned about their well being and consider dental therapy a potential threat to it. More often, however, for some reason or another, patients do not identify themselves as a potential risk. Therefore, in most circumstances it is up to the dental practitioner to make the connection between an under-lying medical condition and dental treatment. There are many circumstances where medically complex patients may require modification of dental care, most fit into one of the following categories:
Patients With A Known Medical Condition
Some patients know that they have a serious medical condition.As just mentioned, some patients know that they suffer from some medical condition. They may have had episodes of chest pain, they may be under treatment for cancer, or they have a thyroid gland disorder. These patients have been diagnosed and treated by a physician and are likely to continue to be under a physician’s care. While such patients may volunteer informa-tion about their medical status, usually the dentist must uncover this information. Whether vol-unteered or elicited, information about an underlying medical condition is important because of the risk that it may be worsened by certain dental treatment procedures.
Patients With An Undetected Medical Condition
Some patients are unaware that they have a serious medical condition.Some patients who do not have a physician or who have not visited a physician for some years may not know that they have an underlying medical condition that could be aggravated by den-tal treatment. By being alert to the signs and symptoms of important medical conditions, by assessing vital signs, and by appropriate referral to a physician, a dentist may uncover an important medical condition that could jeopardize the patients general health and her/his safety during and following dental treatment.
Patients Who Have Recovered From a Medical ConditionPatients who have recovered from a medical condition may be at risk.In some circumstances, a patient who has recovered from a disease or surgery may be predis-posed to a medical complication from dental treatment. For example, patients who have recov-ered from cardiac valve replacement surgery are predisposed to acquiring infective endocarditis. It is important that dentists know of such possibilities and determine whether their patients have the underlying medical conditions that can cause them.
Patients Taking Medications
Use of medications may complicate dental treatment.More and more patients rely on medications, prescribed or otherwise, to manage medical con-ditions. Some medications may cause physiologic changes that may cause complications dur-ing or following dental treatment. As one simple example, patients who regularly take aspirin to prevent blood clots are susceptible to prolonged bleeding after periodontal surgery.
Use of medications may provide clues about a patient’s medical status.A history of prescription medication use may provide a clue to the presence of an underlying medical condition affecting dental treatment. For instance, patients who have been prescribed digitalis preparations are likely to be suffering from congestive heart failure. The use of such
353
354
Oral Medicine
medications needs to be identified and reason for their use determined before dental treatment is started.
Patients Following A Special Diet
Special diets may provide clues about a patient’s medical status.Sometimes, physicians prescribe special diets for their patients. The discovery by a dentist of such diets may uncover a medical condition not identified by the patient. For example, low fat diets may be prescribed patients with diabetes mellitus and/or atherosclerosis. Low sodium diets are often prescribed patients suffering from arterial hypertension.
Patients Who May Transmit Disease
Patients with infectious disease may complicate dental treatment.Infectious diseases, once thought to be disappearing, are on the increase. As one consequence of the HIV/AIDS epidemic, dental personnel have taken steps to prevent transmission of pathogens in the dental office. While the steps in creating barriers to transmission have suc-ceeded, continued vigilance is required to maintain them. The numbers of patients with hepati-tis, herpes, HIV, and tuberculosis will increase greatly in future years. Infection control lapses increase the potential for patient-practitioner and patient-patient transmission of serious infec-tious diseases. In some instances patients who are known to have harbor an infectious disease need to be managed in a manner that will prevent further damage to them. On the other hand, they need to be managed in manner that will prevent transmission of their infection to the den-tist, dental personnel, and other patients.
Patients In Need Of Special Dental Care
Some patients need special dental care prior to receiving medical care.While in many situations, it is the dentist who must rely on the physician to assist in the man-agement of medically complex dental patients, it is becoming more common for physicians to solicit the help of dentists to manage medical patients. Patients scheduled to undergo some forms of cancer chemotherapy and some forms of cancer radiation may need to have an evalu-ation of their dental status—particularly with regard to the presence of disease—prior to start-ing the anticancer regimen.
Some patients need special dental care to prevent a serious medical condition.As physicians become more aware of the medical ramifications of dental disease, they increas-ingly enlist the cooperation of dentists in providing dental examinations and appropriate treat-ment to prevent serious systemic consequences. For example, the elimination of periodontal and periapical disease may prevent infective endocarditis following heart catheterization.
Table 18-1: Who are Medically Complex Patients
Medically compromised patients are those:
• with a known medical condition.• with an undetected medical condition.• who have recovered from a medical condition.• who are taking medications.• who are following a special diet.• who may transmit disease.• who are in need of special dental care.

Discovering Medically Compromised Patients
Discovering, Evaluating, and Managing Medically Complex Pa-tients—An Overview
A “system” for managing medically complex patients is emergingWhile becoming involved with the medical status of patients may seem hopelessly compli-cated, an organized, logical, simplified approach is emerging. Several authors have developed textbooks that attempt to present information pertinent to managing medically complex patients. While these texts do not yet describe a standard protocol for the identification and management of these patients, no doubt in the coming years such a protocol will emerge. What follows is a protocol constructed from the work of many individuals, some who are at USC and others from other dental schools who have written textbooks.
Identification, evaluation, and modification are the current management steps.The first step in management of medically complex patients is, obviously, to identify them. After their medical condition has been identified, it is necessary to evaluate it in the light of dental treatment that is going to be performed. Only after identification and evaluation is com-peted can modification of dental treatment be carried out intelligently and safely. Each of the elements of this interim protocol will be expanded in the following sections:
•Identification of the medically complex patient
•Evaluation of the medically complex patient
•Modification of dental treatment for the medically complex patient
Following discussion of these topics and the steps that comprise them, significant diseases affecting each body system will be reviewed and appropriate modifications in dental treatment discussed.
Discovering Medically Complex Patients
Identify: “…to recognize or establish as being a particular person or thing; verify the identity of: to identify handwriting; to identify the bearer of a check.”
Most dental patients are not medically complex.Most patients who currently seek dental care are in good health—they are not medically com-plex. While the proportion of healthy to medically complex patients will change with the aging of the population, finding medically complex patients within the typical dental practice may be a needle-in-a-haystack proposition.
Many medically complex patients do not identify themselves as such.While some patients immediately and forcefully announce that they are medically complex, most do not. The more reticent patients may not appreciate that dental care may be hazardous to their health. It is easy, then, for dental practitioners to be lulled into complacency about medically complex patients. There is, therefore, great need for a standard approach to identifi-cation of medically complex patients. While there are variations, the most common and most logical first step in identification is to have all patients complete a standard health question-naire.
Discovery Evaluation Modification
Identify
To recognize; to establish as being a particular person or thing; the recognition of a medically complex den-tal patient.
355

356
Oral Medicine
The Health History
The health questionnaire is part of the health history.Administration of a pre-printed standard questionnaire is the most commonly used method to initiate the gathering of a health history. While it is possible to skip the questionnaire and elicit a history from interviewing the patient, for most dentists the self-administered questionnaire is the quickest, most accurate, and most standard method.
The health questionnaire serves only to gather patient information.It must be understood that obtaining a health history does not end with administration of a health questionnaire. To the contrary, it serves only to elicit basic information that must be checked and expanded during the patient interview.
The health history has six components.The health history is composed of 1) the chief complaint, 2) history of present illness, 3) past medical history, 4) a review of systems, 5) social history, and 6) family history
1. Why a patient seeks care is the “Chief Complaint.”It is important to know why a patient seeks dental care. Is it a check-up? Is there pain? Is a tooth missing or broken? The underlying reason why a patient seeks dental care is known as the chief complaint.
2. Learning more about the chief complaint is the “History or the Present Illness.”
Once it is known why a patients seeks care, it is important to learn as much as possible about the condition that brought her/him to the dentist. How long has the condition been present? Is there pain? What events initiated the condition? These are but a few questions that may be asked to obtain a history of the condition (history of present illness).
3. Learning about a patient’s previous diseases is the “Past Medical History.”
It is important that the dentist learn about systemic diseases or conditions that the patient once had or, even more importantly, about conditions from which the patient may now be suffering. This information is sought in the health history and, more specifically, in the health question-naire and patient interview.
4. Learning about a patient’s disease predisposition is the “Family History.”
Sometimes a history of family illness may indicate diseases to which the patient may be sub-ject. It is common for physicians to ask their patients about parent health or death to determine the risk for familial diseases (e.g. colon cancer, ischemic heart disease). The health status of family members living together may uncover a patient’s potential exposure to some infectious disease.
5. Learning about a patient’s personal habits is the “Social History.”
A history of cigarette smoking or heavy alcohol use may suggest a predisposition to oral malignancies. It is important, therefore delve to some degree into the patients personal habits as these may affect the outcome and safety of dental therapy.
6. Survey of a patient’s health by major body systems is the “Review of Systems.”
A structured review of the disease affecting the human body is usually approached by organ systems. Usually each system has its unique disease that is not duplicated elsewhere. In order not to miss anything of significance, an orderly review of systems is essential.
The health questionnaire is a required part of dental practice. The health questionnaire must be administered for all patients treated in a dental practice. It has become the standard of dental care and the American Dental Association and other impor-tant organizations have recommended its routine use. Depending on the practice location, it may be necessary to have questionnaires printed in Spanish or other non-English languages. It also may be necessary for bilingual dental personnel to help the patient with the questionnaire.
Chief Complaint
The main reason a patient seeks dental care; “Why are you seeking dental care?”
History of Present Illness
Inquiry concerning the patient’s signs and symp-toms; “Tell me about your pain (or other symptom or sign)?”
Components of the Health History
• Chief complaint• History of present illness• Past Medical History• Family History• Social History• Review of Systems
Past Medical History
Inquiry about the patient’s past medical problems; “When did you last see a physician…etc.?”
Family History
Inquiry about the medical status of a patient’s parents to determine the predispo-sition to inherited diseases.
Social History
Inquiry about a patient’s habits (e.g., smoking) that may be predisposed to cer-tain diseases.
Review of Systems
Survey of the status of major body systems: car-diovascular, respiratory, renal, endocrine, etc.
Discovering Medically Compromised Patients
All new patients must complete a health questionnaire; it should be updated annually.
For new patients the careful collection of a medical history establishes an important base line for future dental care. It is, therefore, essential that a careful medical history be completed for all new patients. It is also important that the history be updated annually and that it be repeated every five years.
Patients appreciate a practitioner’s concern for their total health.While the identification of medically complex patients is the goal of obtaining a medical his-tory, it has the added benefit of establishing rapport and communication between dentist and patient. While rare patients view the process as either intrusive or irrelevant, most appreciate the concern for their well-being and their safety.
Standard Health Questionnaires
Standard health questionnaires are available from professional societies.Although a dentist can construct her/his own health questionnaire, it makes little sense to do so. Excellent expert-constructed forms are readily available from the American Dental Associ-ation (ADA) and other professional organizations. Common usage of ADA-type forms has resulted in standardized health history collection. Dentists who use these forms are, therefore, in the mainstream of dental practice. Certainly, practitioners should be encouraged to add or reword questions on the ADA-type forms to fit special needs. As mentioned, however, it may be unwise to reinvent the wheel in this regard.
“Long” and “short” health questionnaires may be used in dental practice.There are two basic types of health questionnaires, the short form and the long form. Each has its advantages and disadvantages.
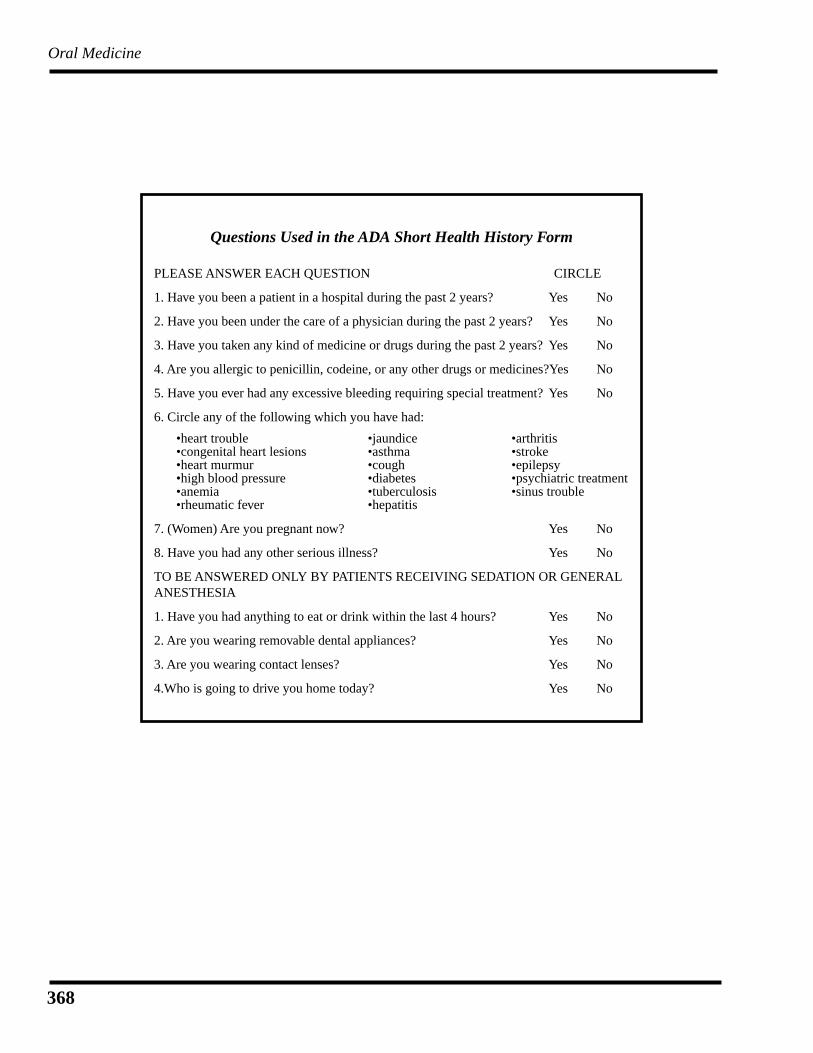
The “short” health questionnaire is used most; it is easy for patients to complete.Most dentists use the short health questionnaire. Their patients find it easy to understand and complete. Experts find it capable of extraction of pertinent information. Being brief, however, it is possible that something may be overlooked particularly if the dentist does not conduct a thorough patient health history interview. The ADA version of the short health questionnaire is composed of seven basic questions and a list of 17 diseases. There are an additional four ques-tions for those patients who are scheduled to receive intravenous sedation or anesthesia. An example of a short health questionnaire later in this chapter.
The “long” health questionnaire is more complete; if used, less will be missed.The longer health questionnaire is most commonly used in learning situations—in dental schools and in dental auxiliary programs. Actually, because it is more comprehensive than the short form, it should be used in dental practices as well. This form has the advantage of assist-ing in the identification of diseases or conditions that may be missed using the shorter version.
The USC Patient Questionnaire is an example of the long health questionnaire.A variation on the ADA long form is used at the USC School of Dentistry. This USC form will be the basis of further discussions in this course. USC calls its health questionnaire the “patient questionnaire.” The information contained in this document is organized into several sections; under these are a number of questions that are to be answered “yes” or “no.” Some lines are included for more specific information.
Review of Systems—The first page of the USC Patient Questionnaire is devoted primarily to a list of 66 diseases categorized under 6 systems: 1) cardiovascular, 2) respiratory, 3) musculosk-eletal-CNS-developmental, 4) gastrointestinal-genitourinary, 5) hematologic-endocrine-immune, and 6) psychiatric. The patient is asked “do you have or have you had any of the fol-lowing.”
Family History—This section includes three conditions or groups (diabetes, heart diseases, bleeding disorders) that may represent inherited or familial diseases.
Allergies—This section includes four substances or groups of substances (antibiotics, anesthet-
357
358
Oral Medicine
ics, analgesics, latex products) to which the patient is to report an allergic reaction. A line is provided for inclusion of “other” allergic substances.
Females—Under this section are three questions pertinent to females: pregnancy, birth control, breast feeding.
Dental History—Here, the patient is asked three questions about pain, nervousness, and unfa-vorable dental experiences.
Social History—Three questions covering tobacco, alcohol, and drug use/addiction are pre-sented in this section. Lines are provided for answers to additional questions (What kind? How much? How many years?).
Other Conditions—Lines are provided for the answer to the following question: “Do you have any other conditions not already mentioned?”
Hospitalization/Surgery—Here again, lines are provided to include any past hospitalization and surgical procedures.
Medications History—Lines are provided to list any medications taken in the last six months.
Soft Tissue Examination—Drawings and labelled lines are provided for the practitioner to indi-cate and describe abnormalities discovered in the soft tissue examination.
Significant Radiographic Findings—Lines are provided for the practitioner to describe any abnormalities discovered in radiographic examination.
The Health History Interview
Again, the health questionnaire serves only to acquire information; an interview is necessary.The health history interview is an essential part of the health history. Far too often, obtaining the health history for a patient new to a dental practice starts and ends with the health question-naire. Some dentists seem to feel uncomfortable asking patients about their general health; no doubt some of these feel uncomfortable “playing doctor.” Whatever the reason for skipping discussion of a patient’s general health, the sooner a regular routine is established the sooner the dental practitioner will be comfortable in the role.
Start the interview by asking about the chief complaint.It is a good idea to begin the interview with inquiry about the patient’s chief complaint. Some open-ended question like “Why are you seeking dental care” will serve as an opener. By start-ing with the initiating dental problem, the practitioner is showing interest in solving the patient’s problem and, at the same time establishing rapport.
Continue with questions about the chief complaint (history of the present illness).Continuing with the dental problem that is at hand, it is logical to continue with questions about the condition that brought the patient to the dentist. If there is a specific problem, a tooth-ache for example, now is the time to ask a general open-ended question about it: “Tell me about your toothache.” Depending on the responses, you might follow with more specific ques-tions about the onset, duration, and type of pain. If on the other hand the patient has no specific problem but is seeking a dental “checkup,” you might begin with another open-ended question like “Tell me about your past dental treatment.” Depending on the response, more specific fol-low-up questions will come to mind.
Move on to inquiring about the patient’s general health (past medical history).With the patient’s completed health questionnaire in hand, the dentist now asks the patient questions about her/his general health and about specific conditions they identified on the ques-tionnaire. During the interview it is recommended that ten topics be covered: (1) When and why did you last see a physician? (2) Who is your physician? (3) Have you ever had a serious disease? (4) Tell me about any operations or hospital stays you ever had. (5) Tell me about any dietary restrictions you are following. (6) Tell me about any medications you have taken in the
Discovering Medically Compromised Patients
last year or so. (7) Have you ever had an adverse reaction to any substance? (8) Tell me about your response to this (these) question(s) on your health questionnaire. (9) Tell me about any complications you ever experienced with past dental treatments (10) Do you have any condi-tions, diseases, or abnormalities not mentioned on your health questionnaire? For returning patients, the dentist should, at the very least, ask (again with the health questionnaire in hand) “Tell me about any changes in your health since your last visit.”
Make Notes of the Patient’s ResponsesIt is essential that notes of responses be made in the patient’s permanent record. These need not be formal; they need not be typed. Handwritten words and phrases are all that are needed to remind the practitioner of the responses at a subsequent visit or, God forbid, in court. On the USC form, unfortunately, there is no place for such comments. There is a place on the ADA short form that such comments can be placed; a formal “remarks” section is provided on the ADA long form. When using the USC form, it is recommended that patient comments be placed adjacent to the appropriate question or in the margins. Whether in a formal location or in the margins, these remarks should be dated and initialed.
Physical Examination of Dental Patients
A complete oral examination is an essential part of dental care.It is normal and appropriate for dental practitioners to focus their attention on conditions affecting the teeth and the periodontium. Because of this understandable interest in teeth and periodontium, it is easy to overlook examination of the remainder of the mouth, where, by the way, potentially disfiguring or life-threatening diseases may lurk. (The oral examination is known as the soft tissue examination; it will be covered later).
Vital Signs
An abbreviated physical examination (vital signs) is also essential.It is even easier to overlook making basic assessment of the patient’s overall health by forego-ing a brief physical examination. Actually, it is not necessary or even desirable for dentists to perform a physical examination in the sense that a physician performs it. In fact, if such an examination is needed, a physician should do it. That being stated, it is, nevertheless, the den-tist’s responsibility to observe the overall appearance and to measure her/his patient’s vital signs. The physical examination conducted by the dentist, then, is a simple, brief procedure that will provide important information.
Measuring vital signs provide a baseline and may uncover serious disease.There are two basic reasons for measuring vital signs for dental patients. First, these measure-ments serve as a base line against which later measurements can be compared. Second, they may, in themselves, indicate some significant underlying abnormality (e.g. arterial hyperten-sion).
Examination Methods
Observation, inspection, palpation, percussion, & auscultation are examination methods.Observation: “…an act or instance of noticing or perceiving.” Observation refers to examin-ing the patient from afar. As a patient enters the operatory’ the dental practitioner should observe her/his general appearance and her/his general physical status.
Inspection: “…the act of inspecting or viewing, especially carefully or critically.” During the examination, particularly the soft tissue part, the operator must look at the features of, for example, a lesion up close. This close, careful, examination is called inspection.
Palpation: “…the act of examination by touch, especially for the purpose of diagnosing dis-ease or illness.” Touching a part of a patient—a structure or a lesion, for example—is known as palpation. This procedure is of particular importance in the soft tissue portion of the physical examination.
Physical Examination
Investigation into a patient’s health status by observing, feeling, and measuring observable characteristics.
Observation
Examining of physical characteristics from a dis-tance.
Inspection
Examination of a physical characteristic up close.
Palpation
Examination by touch.
359
360
Oral Medicine
Percussion: “…the striking or tapping of the surface of a part of the body for diagnostic or therapeutic purposes.” Occasionally, it is necessary to tap on a tooth to determine if periapical disease is present. This tapping act is known as percussion. Other than this example, percus-sion has limited applicability in examinations conducted by dental practitioners.
Auscultation: “…the act of listening, either directly or through a stethoscope or other instru-ment, to sounds within the body as a method of diagnosis.” Other than listening to the func-tioning temporomandibular joint with a stethoscope, auscultation is of limited use in dental physical examinations.
Observation of a Patient’s General Appearance and Behavior
Observe a patient’s general appearance and measure vital signs.As mentioned, the physical examination recommended for the average general practice in den-tistry consists of two parts: 1) observation of general appearance and 2) measurement of vital signs.
A patient’s general appearance and demeanor provides important information.A great deal can be learned by observing patients in the waiting room, as they enter the opera-tory, as they sit in the dental chair, as they talk during the interview, and as they leave. These observations should include, but not be limited, to the following:
Dress and Grooming—Observe the level of care in dress and grooming. Sick or disturbed patients often let these external appearances deteriorate.
Agility and Energy—Observe the presence of absence of energy and enthusiasm. The degree to which patients are alert and aware of their surroundings may indicate the absence or presence of disease. Similarly, the facility with which patients are able to sit, stand, and walk may also indicate their general state of health. Also, observe the patients weight; overly obese individu-als may be afflicted with one of several systemic diseases.
Demeanor—Observe the patient’s behavior toward dental treatment, toward family members, and toward office staff. Presence of unprovoked belligerence or abnormal response to ordinary events may indicate psychological disorders or, at the very least, future management difficul-ties.
Breathing—Observe whether or not patients have difficulty in catching their breath after walk-ing from the waiting room and sitting in the dental chair. If they cannot talk for several minutes after being seated, it may indicate the presence of serious underlying cardiac and/or pulmonary disease.
Odors—Observe any unusual body odors. Tobacco and alcohol odors are common and may indicate potential systemic disease (lung/oral cancer or cirrhosis). Acetone breath may indicate that a patient suffers from uncontrolled diabetes mellitus. Putrefied breath odor may indicate oral or pulmonary infections. Generally unpleasant body odor may speak volumes about a patient’s grooming habits.
Inspection and Palpation of the Head and Neck
Inspection and palpation of the face may reveal important diseases.Dental practitioners operate very close to a patient’s face. Given the proximity, there is ample opportunity to observe the eyes, skin, and other facial parts.
Eyes—Some diseases manifest with eye changes. Hyperthyroidism is often accompanied by bulging eyes (exophthalmos); jaundice may appear first as yellow sclera.
Skin—Observe and inspect the skin of the face for obvious lesions. Basal cell carcinoma and melanoma are common in the skin of older people. Observe the skin elsewhere for bruises, ecchymoses, jaundice, or cyanosis. These changes may indicate presence of serious underlying diseases.
Percussion
Examination by striking or tapping.
Auscultation
Examination by listening.

Discovering Medically Compromised Patients
Swellings, Asymmetries, Anomalies—Observe the face for obvious swellings of the parotid glands, the thyroid gland, or the jaws. Look for palsy of the face or other obvious asymmetries. Also note any obvious developmental defects such as cleft lip.
Parotid and Submandibular Glands—The parotid and submandibular glands should be pal-pated to disclose any growths in their substance.
Temporomandibular Joint—The temporomandibular joint should be palpated along with the parotid glands. It is customary to have the patient open and close the mouth as the condyles are being felt. Any cracking, grinding (crepitus), or other abnormality should be noted.
Observation, inspection, and palpation of the neck may reveal important diseases.The structures of the neck should be observed, inspected, and palpated. Enlarged lymph nodes may indicate the presence of serious disease. An enlarged thyroid gland indicates disease in that structure. Distention of the veins passing through the neck may indicate congestive heart failure.
Observation of Other Body Parts
Observation of other body parts may reveal important diseases.Hands—Observe the hands for skin changes mentioned above. Also note the presence of club-bing of the fingers and cyanosis or hemorrhage under the fingernails. These changes are indica-tors of serious underlying disease.
Legs and Ankles—If they are exposed, observe the ankles and legs for signs of swelling. Swol-len ankles may indicate the presence of dependent edema, a hallmark of congestive heart fail-ure.
Abdomen—Observe whether or not the abdomen is obviously enlarged compared with other body parts. An enlarged abdomen in an otherwise slender person may indicate the presence of ascites, a hallmark of serious underlying disease.
Measurement of Vital Signs
Blood Pressure Measurement
Measurement of blood pressure is a simple way of assessing a patient’s health.Blood pressure is an important vital sign. If pressure in arteries is higher than normal for long periods of time, it can cause irreversible damage to blood vessels and the heart. It can be mea-sured directly by placing a measuring device directly into a blood vessel. This is sometimes carried out by physicians in measurement of pressure in, for example, the portal vein or the pulmonary artery.
Indirect blood pressure measurement is a reliable, easily-mastered procedure.Usually, however, blood pressure is measured by a simple non-invasive indirect technique, a procedure that can be implemented by patients, technicians, dental assistants, dental hygien-ists, and dentists alike. This indirect procedure requires three devices: 1) a stethoscope, 2) a pressure cuff, and 3) a pressure gauge (the sphygmomanometer). It measures pressure in the brachial artery in the antecubital fossa. The usual steps involved in measuring blood pressure are listed on a summary page near the end of this chapter.
Several blood pressure readings should be takenIt is recommended that several readings be taken over a 30 minute period. Between readings it is usual to talk to the patient (conduct the medical history) leaving the cuff in place. By the time the third reading is taken, the patient will no doubt feel more relaxed producing a more reliable resting blood pressure reading. For obese individuals it may be necessary to place the cuff on the lower arm and listen to Korotkoff sounds at the wrist (radial artery).
Blood Pressure
Measurement of the force acting upon the walls of blood vessels; indirectly measured by compressing and releasing the brachial artery.
Korotkoff Sounds
Sounds heard while mea-suring a patient’s blood pressure; caused by blood turbulence.
361
362
Oral Medicine
Pulse Measurement
Measuring pulse indirectly measures heart rate.Each beat of the heart creates a pressure wave that is transmitted along the elastic and distribut-ing arteries. At several points around the body, a distributing artery is close enough to the sur-face for the pressure waves to be felt. These waves are felt as regularly spaced blood vessel throbs. The throbs, or pulses, are counted in order to determine the number of pressure waves (pulses) occurring in a certain period of time (usually one minute). Since these pulses are caused by ejection of blood from the heart, they are accurate measures of the number of heart beats per minute.
Measuring pulse is usually done at the wristIn dentistry, there are three locations where determination of heart rate by “taking a patient’s pulse” can be measured: 1) the radial artery at the wrist, 2) the carotid artery in the neck, and 3) the brachial artery in the antecubital fossa. Patients are used to having their pulse taken at the wrist; therefore, a dentist taking a pulse at this location should meet with acceptance. The radial artery can be felt at the thumb side of the inside wrist. The pulse should be measured with two fingers: the middle and ring fingers, or the middle and index fingers. It should never be felt with the thumb as the operator’s own thumb pulse may interfere with obtaining the patient’s pulse. While it is desirable to count the pulse for a full minute, it us customary to count it for 15 seconds and then multiply the result (mentally) by four. It is also common to measure a patient’s pulse by palpating the carotid artery in the neck. This pulse can be felt by locating the thyroid cartilage (Adam’s apple) and then moving laterally toward the sterno-cleidomastoid muscle until the pulse is felt. Again, the middle and ring or index fingers should be used. Once the pulse is located, it is counted just as at the wrist. It is uncommon to take the pulse in the antecubital fossa. However, special circumstances may require it. Once the pulse is located here, the procedure outlined above is used.
Sixty–eighty beats/minute is a normal pulse.A normal measurement is between 60 and 80 pulses per minute. A heart rate (remember that measurement of the pulse is an indirect measurement of heart rate) over 80 may indicate the presence of tachycardia (increased heart rate). A heart rate under 60 beats per minute is classi-fied as bradycardia (decreased heart rate).
Measurement of Respiration Rate
Measurement of the rate of breathing at rest is another important vital sign. This measurement is accomplished by observing the rise and fall of the chest for a period of time, usually one minute. Here again, it is customary to measure respiration for 15 seconds and then multiply the result by 4. Normal breathing rates range from 16-18 per minute. Abnormally high rates may indicate the presence of great anxiety or underlying systemic disease. In order to obtain an accurate measurement, it is usually desirable to measure respiration without the patient being aware of it. A dental assistant might be trained to observe respiration while the operator is otherwise involved with the examination.
Measurement of Temperature, Weight, and Height
Assessment of temperature, weight, and height finish measurement of vital signs.Body Temperature—While it is certainly appropriate to measure body temperature orally, it may not be necessary to do so routinely unless, of course, an infection is suspected. Normal
oral temperature is 98.6o F. (37o C.). Temperature is measured by placing an thermometer under the tongue for several minutes. It is important that the thermometer be sterile and that it
register a temperature well below 98.6o F. prior to placing it in the mouth. Disposable ther-mometers are available and are commonly used.
Body Weight—While abnormal thinness or heaviness may indicate serious underlying disease, it is not feasible to weigh patients in the typical dental office. Instead, it is sufficient to estimate whether or not the patient is over or underweight and to ask two questions: 1) “What is your
Pulse
Indirect measurement of heart rate by feeling and counting pressure waves in an artery (usually the radial artery).
Brachial Artery
The large distributing artery of the upper arm; blood flow through this vessel is used to determine blood pressure.
Radial Artery
One of two major arteries of the lower arm; can be felt as it passes over the radius at the wrist.
Carotid Artery
A major artery supplying blood to the head; can be felt in the neck between the thyroid cartilage and the sternocleidomastoid mus-cle.
Antecubital Fossa
The concavity on the flexor surface of the arm at the elbow; the brachial artery and median cubital vein are located here.
Tachycardia
Rapid heart rate; 100-190 beats per minute.
Bradycardia
Decreased heart rate; less than 60 beats per minute.
Discovering Medically Compromised Patients
current weight?” and 2) “Has your weight changed significantly over the last two years?”
Body Height—Here again, it is not usual to measure a patient’s height in the typical dental office. Instead, it is sufficient to ask the patient: “What is your height?” or “How tall are you?”
The Oral Soft Tissue Examination
A complete oral examination includes inspection of the oral soft tissues.No oral examination is complete without examination of the soft tissues of the head and neck. While few disagree with this statement, the fact is that few dentists actually perform soft tissue examinations. A recent report from the Center of Disease Control (CDC) indicated that only 14% of patients have ever had a “cancer examination,” or, in other words, have ever had a soft tissue examination. It is natural and understandable for dental practitioners to focus on their area of interest and specialization. It is, for example, natural for general practitioners to focus on teeth; their “complete” examination may begin and end with the teeth. Similarly it is natural for periodontists and dental hygienists to focus on the periodontium; their “complete” exami-nation may begin and end with the periodontium. Whether it is natural or not, it is simply unac-ceptable that soft tissue examinations are performed so rarely. After all, the examination is simple, painless, and brief.
Patients increasingly will come to demand oral soft tissue examinations.Patients are becoming much more health conscious and are coming to expect dentists to be concerned about the onset of cancer in their mouths. Patients will accept the performance of a soft tissue examination; they will come to expect no less of their dentist. Given the need, given patient acceptance, and given that after some practice, an oral soft tissue exam can be con-ducted in two minutes, it is difficult to understand the reticence of most dentists from providing this service to their patients.
Establishing a standard soft tissue examination routine is important.It is very important to establish a standard routine when conducting a soft tissue examination. Performing the examination the same way every time, will prevent lapses that could be disas-trous. For example it may be that the mouth floor and ventral tongue were missed on a particu-lar examination, and an incipient cancer missed. Such a routine is presented below.
1. The Lips
Start by examining the lips. The upper lip should be grasped gently between the thumbs and index fingers of both hands. While inspecting the surfaces described below, palpate the lip for submucosal masses. First inspect the red portion (vermilion) for surface lesions. Then, by everting the lip, similarly examine the labial mucosa, labial vestibular mucosa, and anterior gingiva—again noting any abnormalities. Upon reaching the corners of the mouth (commissure), continue the eversion, inspection, and palpation of the lower lip (vermilion, labial mucosa, vestibular mucosa, and ante-rior gingiva).
2. The Side of the Mouth
After inspection and palpation of the lips, move on to the cheeks. There is no need to reposition one of your hands; pick up a mouth mirror with the other. This instrument is used to direct light onto mucosal surfaces and to move the tongue aside.
Starting on one side or the other, palpate the cheeks for submucosal masses. Direct light onto the buccal mucosa; inspect it for surface lesions. Similarly, inspect the buc-cal vestibular mucosa and the buccal gingivae.
3. The Roof of the Mouth
Using your index finger, palpate the hard palate for submucosal nodules; pay particu-lar attention to the palate opposite the maxillary molar teeth. Now directing light onto the surface, inspect the palatal mucosa and the palatal gingiva for surface lesions.
363
364
Oral Medicine
4. The Back of the Mouth
The structures that encircle the posterior mouth—soft palate, tonsillar pillars, and posterior pharyngeal wall—are areas where oral squamous carcinoma (“oral cancer”) frequently lurks. These structures, then, are high risk areas for development of this disease.
Directing light onto the soft palate, inspect it and the uvula for surface lesions. It is usually necessary to use the back of the mouth mirror to gently depress the tongue. To prevent a gag reflex, encourage the patient to breath naturally through the nose, not the mouth. Directing light to the right and left, inspect the tonsillar pillars for surface lesions. Now, depressing the tongue while the patient says “aah,” inspect the posterior pharyngeal wall for surface lesions.
5. The Tongue
Moving the mouth mirror between the tongue and lower molars, direct light onto the lingual gingivae to look for surface lesions. Then, ask the patient to touch the back of the front teeth with the tip of the tongue. With the tongue in this position it is possible to inspect the ventral mucosa and the floor of the mouth for surface lesions. Remem-ber that oral cancers often occur in these areas: they are areas of high risk. With the tongue still raised, inspect the lingual gingiva for surface lesions.
Leaving the mouth for an instant, pick up a piece of sterile gauze. After asking the patient to extend the tongue out of the mouth, gently grasp the end of it with the gauze (to keep it from slipping). Extending the tongue a little further (prevent the ventral surface from being cut on the lower teeth), palpate it between the thumb and index finger of the free hand. Inspect the dorsum for surface lesions. Move the tongue gen-tly to one side inspecting the lateral surface from tip to base (lingual tonsils) for lesions. The lateral surface of the tongue is another area of high risk for oral cancer. Move the tongue to the other side to inspect the remaining lateral surface.
Finally, place a finger of one hand in the floor of the mouth and press upward on the outside against it in an effort to palpate for masses. This may be difficult because of the contraction of the mylohyoid muscles.
Soft tissue examination results must be recorded in the patient’s chart.Results of the soft tissue examination are to be recorded in the spaces provided. Lesions can be located on drawings and pertinent facts about them (size, color, demarcation, etc.) can be noted near the drawing or in a nearby space. It is usual to use the abbreviation “NSF” (no significant findings) on lines referencing specific oral locations (e.g. “Mucosa,” “Palate,” “Tongue”). Not-ing the absence of disease in this way suggests that a careful examination was conducted and that no area was missed.
Radiographic Examination
Examination of radiographs is an essential part of an complete oral examination.Radiography textbooks describe the details of radiographic examination of the structures inside and adjacent to the mouth. Obviously radiographs are an important part of most oral examinations. These films should be examined for evidence of bony abnormalities and/or bony lesions. Usually these manifest as radiolucencies, radiopacities, or a combination of the two. The size, location, and appearance of intrabony lesions must be recorded.
Radiographic findings must be recorded in the patient’s chart.It does little good to perform a thorough physical examination if notations are not made. While forms vary, all should have locations to record appropriate findings. On the back of the USC Patient Questionnaire are a number of such locations; some have been described already. On the USC form, abnormalities observed on the radiographic examination are to be recorded on the lines provided.
365
Discovering Medically Compromised Patients
Summary of Components of Discovering Medically Complex Patients
Discovery
The Health History
••Questionnaire
••Interview
The Physical Examination
••Body
••Vital Signs
••Oral Soft Tissues
••Oral Hard Tissues
Evaluation
Modification
366
Oral Medicine
Summary
A. Introduction1. Dentistry’s Transition Toward Biology and Medicine
a. Some believe that dentistry should merge with medicine.b. Dentistry is moving toward reliance on biology and disease prevention.
2. The Need to Treat Medically Complex Patientsa. It used to be that sick patients didn’t come to dental offices.b. More patients will be older than before; most will be under medical care.c. Dental practitioners will increasingly treat medically complex patients.
B. Who Are Medically Complex Patients?1. Most patients will not identify themselves as medically complex.2. Patients With a Known Medical Condition
• Some patients know that they have a serious medical condition.3. Patients With an Undetected Medical Condition
• Some patients are unaware that they have a serious medical condition.4. Patient Who Have Recovered From a Medical Condition
• Patients who have recovered from a medical condition may be at risk.5. Patients Taking Medications
a. Use of medications may complicate dental treatment.b. Use of medications may provide clues about a patient’s medical status.
6. Patients Following a Special Diet• Special diets may provide clues about a patient’s medical status.
7. Patients Who May Transmit Disease• Patients with infectious disease may complicate dental treatment.
8. Patients in Need of Special Dental Carea. Some patients need special dental care prior to receiving dental care.b. Some patients need special dental care to prevent a serious medical condition.
C. Discovering, Assessing, and Managing Medically Complex Patients—An Overview1. A “system” for managing medically complex patients is emerging2. Identification, evaluation, and modification are the current management steps.
D. Discovering Medically Complex Patients1. Most dental patients are not medically complex.2. Many medically complex patient’s do not identify themselves as such.3. The Health History
a. The health questionnaire is part of the health history.b. The health questionnaire serves only to gather patient information.c. The health history has six components.
(1) Why a patient seeks care is the “Chief Complaint.”(2) Learning more about the chief complaint is the “History or the Present Illness.”(3) Learning about a patient’s previous diseases is the “Past Medical History.”(4) Learning about a patient’s disease predisposition is the “Family History.”(5) Learning about a patient’s personal habits is the “Social History.”(6) Survey of a patient’s health by major body systems is the “Review of Systems.”
d. The health questionnaire is a required part of dental practice. (1) All new patients must complete a health questionnaire; it should be updated annually.(2) Patients appreciate a practitioner’s concern for their total health.
e. Standard health questionnaires are available from professional societies.(1) “Long” and “short” health questionnaires may be used in dental practice.(2) The “short” health questionnaire is used most; it is easy for patients to complete.(3) The “long” health questionnaire is more complete; if used, less will be missed.
f. The Health History Interview(1) Again, the health questionnaire serves only to acquire information; an interview is necessary.(2) Start the interview by asking about the chief complaint.(3) Continue with questions about the chief complaint (history of the present illness).(4) Move on to inquiring about the patient’s general health (past medical history).(5) Make Notes of the Patient’s Responses
Discovering Medically Compromised Patients
4. Physical Examination of Dental Patientsa. A complete oral examination is an essential part of dental care.b. An abbreviated physical examination (vital signs) is also essential.c. Measuring vital signs provide a baseline and may uncover serious disease.d. Observation, inspection, palpation, percussion, & auscultation are examination methods.e. Observe a patient’s general appearance and measure vital signs.f. A patient’s general appearance and demeanor provides important information.g. Inspection and palpation of the face may reveal important diseases.h. Observation of other body parts may reveal important diseases.i. Measurement of a patient’s vital signs is an essential part of dental care.
5. The Oral Soft Tissue Examinationa. A complete oral examination includes inspection of the oral soft tissues.b. Patients increasingly will come to demand oral soft tissue examinations.c. Establishing a standard soft tissue examination routine is important.
(1) The Lips(2) The Side of the Mouth(3) The Roof of the Mouth(4) The Back of the Mouth(5) The Tongue
d. Soft tissue examination results must be recorded in the patient’s chart.6. Radiographic Examination
a. Examination of radiographs is an essential part of an complete oral examination.b. Radiographic findings must be recorded in the patient’s chart.
367
368
Oral Medicine
Questions Used in the ADA Short Health History Form
PLEASE ANSWER EACH QUESTION CIRCLE
1. Have you been a patient in a hospital during the past 2 years? Yes No
2. Have you been under the care of a physician during the past 2 years? Yes No
3. Have you taken any kind of medicine or drugs during the past 2 years? Yes No
4. Are you allergic to penicillin, codeine, or any other drugs or medicines?Yes No
5. Have you ever had any excessive bleeding requiring special treatment? Yes No
6. Circle any of the following which you have had:
7. (Women) Are you pregnant now? Yes No
8. Have you had any other serious illness? Yes No
TO BE ANSWERED ONLY BY PATIENTS RECEIVING SEDATION OR GENERAL ANESTHESIA
1. Have you had anything to eat or drink within the last 4 hours? Yes No
2. Are you wearing removable dental appliances? Yes No
3. Are you wearing contact lenses? Yes No
4.Who is going to drive you home today? Yes No
•heart trouble •jaundice •arthritis•congenital heart lesions •asthma •stroke•heart murmur •cough •epilepsy•high blood pressure •diabetes •psychiatric treatment•anemia •tuberculosis •sinus trouble•rheumatic fever •hepatitis

369
Discovering Medically Compromised Patients
Questions to Ask New Dental Patients Concerning Past Medical Problems
1. “When and why did you last see a physician?”
2. “Who is your physician?”
3. “Have you ever had a serious disease?”
4. “Tell me about any operations or hospital stays you ever had.”
5. “Tell me about any dietary restrictions you are following.”
6. “Tell me about any medications you have taken in the last year or so.”
7. “Have you ever had an adverse reaction to any substance?”
8. “Tell me about your response to this (these) question(s) on your health questionnaire.”
9. “Tell me about any complications you ever experienced with past den-tal treatments.”
10. “Do you have any conditions, diseases, or abnormalities not mentioned on your health questionnaire?”
Question to Ask Returning Dental Patients Concerning Past Medical Problems
•“Tell me about any changes in your health since your last visit.”
370
Oral Medicine
Physical Examination in Dentistry
General Appearance
•Dress and Grooming
•Agility
•Demeanor
•Breathing
•Odors
The Face
•Eyes
•Skin
•Swelling, Asymmetries, Anomalies
•Parotid and Submandibular Glands
•Temporomandibular Joint
The Neck
•Thyroid Gland
•Cervical Lymph Nodes
Other Body Parts
•Hands
•Legs and Ankles
•Abdomen
Vital Signs
•Blood Pressure
•Pulse
•Respiration
•Weight

371
Discovering Medically Compromised Patients
Technique for Measuring Blood Pressure
1.Place pressure cuff on the upper arm.
2.Place the stethoscope over the brachial artery in the antecubital fossa; listen; there should be no sounds because during normal blood flow there is no turbulence; it is turbulence that generates sounds in blood vessels.
3.The cuff is inflated about 30 to 40 mmHg above the anticipated systolic reading. This compresses the brachial artery against the humerus briefly stopping blood flow through it. There should be no sounds in the brachial artery.
4.Cuff pressure is gradually released. As blood passes the cuff constriction, turbulence is created causing sounds (Korotkoff sounds).
5.The pressure reading on sphygmomanometer at which the first sound is heard is recorded as the systolic pressure (usually between 110 and 140 mmHg).
6.The cuff pressure is released further. The pressure at which the sounds dis-appear (normal flow resumes) is recorded as the diastolic pressure (usually between 70 and 90 mmHg).
372
Oral Medicine
Normal Vital Signs
Blood Pressure
•Systolic = 100–140 mmHg
•Diastolic = 60–90 mmHg
Pulse
•60–90 beats per minute
Respiration
•16–18 breaths per minute
Temperature
•98.6oF., 37oC.
Weight
•Varies; Less than 200 lbs.
Height
•Varies; 5’0”–6”6’
373
Discovering Medically Compromised Patients
Oral Soft Tissue Examination
1. The Lips
•Vermilion
•Labial Mucosae
•Vestibular Mucosae
•Anterior Gingivae
2. The Side of the Mouth
•Buccal Mucosae
•Vestibular Mucosae
•Buccal Gingivae
3. The Roof of the Mouth
•Palatal Mucosa
•Palatal Gingivae
4. The Back of the Mouth
•Soft Palate
•Uvula
•Tonsillar Pillars
•Posterior Pharyngeal Wall
5. The Tongue
•Ventral Tongue
•Floor of Mouth
•Lingual Gingivae
High Risk Areas for Oral Squamous Cell Carcinoma
•Lateral Tongue
•Ventral Tongue
•Floor of Mouth
•Soft Palate
•Tonsillar Pillars
High Risk Areas for Minor Salivary Gland Malignancies
•Lateral Hard Palate
•Lips
•Floor of Mouth
Oral Medicine
Study Questions:
1. The of definition of the term “observation” when use inreference to a physical or dental soft tissue examinationis1. “the act of inspecting or viewing, especially care-
fully or critically.”2. “the act of examination by touch.”3. “the striking or tapping of a surface of the body.”4. “the act of listening to body sounds.”5. “an act of instance or noticing or perceiving.”
2. During the abbreviated physical examination, a patient’sagility and energy is assessed by1. observation.2. inspection.3. palpation.4. percussion.5. auscultation.
3. Patients who are “on a diet” may be medically complexbecause the diet may1. have caused them to lose weight.2. have been prescribed by a physician.3. be low in protein.4. be low in fat.5. be high in carbohydrate.
4. Learning about the condition for which a patient seeksdental care is called the1. “past medical history.”2. “chief complaint.”3. “family history.”4. “review of systems.”5. “history of present illness.”
5. Health questionnaires should be administered 1. only for patients with obvious health problems.2. only for patients who are not under a physician’s
care.3. for all patients.4. only for patients taking prescribed medications.5. only for patients following a special diet.
374
Additional Readings:
6. Of the following, which is NOT a high risk area for thedevelopment of oral squamous cell carcinoma?1. Floor of the mouth2. Tonsillar pillars3. Hard palate4. Soft palate5. Lateral tongue