Disclosures - escrh.eu
8
23/05/2018 1 Sven O. Skouby, MD, DMSc Reproductive Medicine Unit Dep. Ob/Gyn. Herlev/Gentofte Hospital, Faculty of Medical and Health Sciences University of Copenhagen, Denmark PCOS intervention: On the continous clinical challenge! Disclosures • Conflicts of interests: nil 3 Herlev/Gentofte Hospital • Prevalence of PCOS: >10% • The most prevalent endocrine dysfunction among fertile women • Etiology: unknown Learning objectives 4 Herlev/Gentofte Hospital • Apart from ovarian dysfunction clinical penetration of metabolic disturbancies and CVD risk are linked to PCOS phenotypes • Intervention therapy may depend on pregnancy wish or solely metabolic or cosmetic problems • Often it is a mixture of this triade Learning objectives Natural history PCOS: Developmental origin Genetic predisposition (Insulin resistance) Central obesity Abnormal LH secretion Prenatal exposure to androgen? High LH Hyperandrogenism Anovulation Insulin resistance sos/pcos/2012
Transcript of Disclosures - escrh.eu
23/05/2018
1
Sven O. Skouby, MD, DMSc
Reproductive Medicine Unit Dep. Ob/Gyn. Herlev/Gentofte
Hospital, Faculty of Medical and Health Sciences University of
Copenhagen, Denmark
PCOS intervention: On the continousclinical challenge!
Tekst starter uden
Sted og
Enhedens
Disclosures
• Conflicts of interests: nil
Tekst starter uden
Sted og
Enhedens 3
Herlev/Gentofte Hospital
• Prevalence of PCOS: >10%
• The most prevalent endocrine dysfunction among fertile women
• Etiology: unknown
Learning objectivesTekst starter uden
Sted og
Enhedens 4
Herlev/Gentofte Hospital
• Apart from ovarian dysfunction clinical penetration of metabolic disturbancies and CVD risk are linked to PCOS phenotypes
• Intervention therapy may depend on pregnancy wish or solely metabolic or cosmetic problems
• Often it is a mixture of this triade
Learning objectives
Tekst starter uden
Sted og
Enhedens
Natural history
PCOS: Developmental origin
Genetic predisposition(Insulin resistance)
Central obesityAbnormal LH secretion
Prenatal exposure to androgen?
High LH
Hyperandrogenism AnovulationInsulin resistance
sos/pcos/2012
23/05/2018
2
Tekst starter uden
Sted og
Enhedens
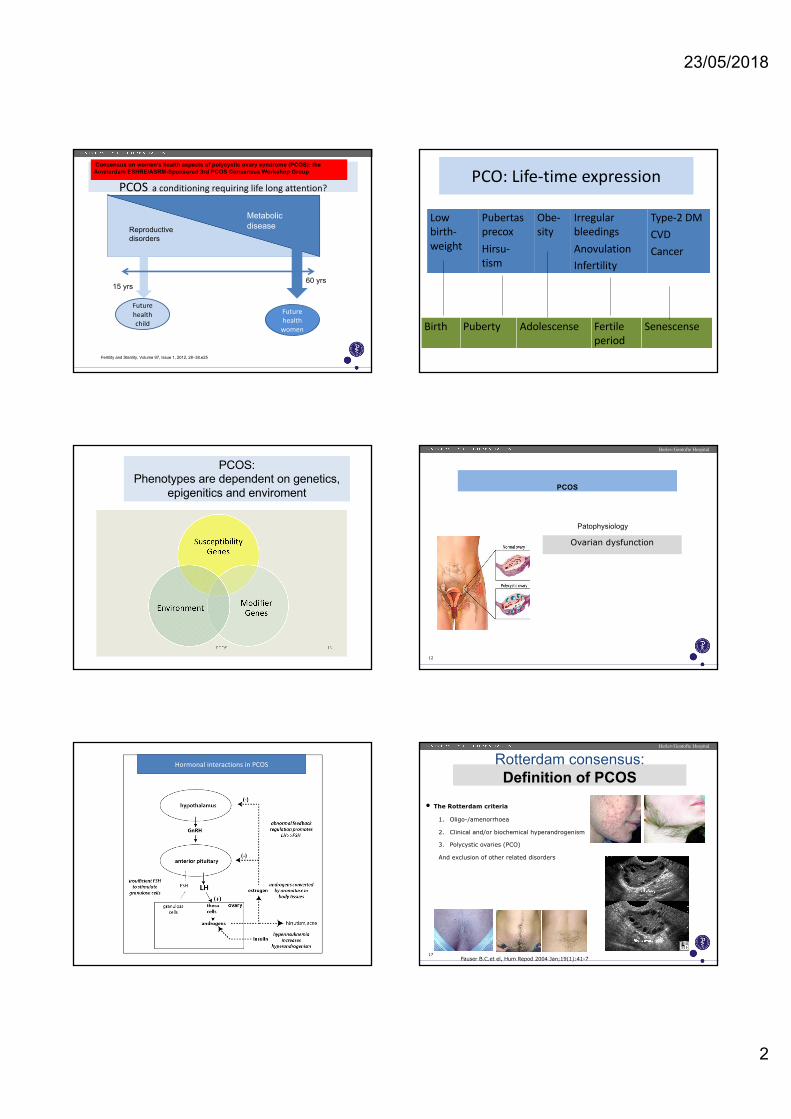
PCOS a conditioning requiring life long attention?
15 yrs60 yrs
Future healthchild
Reproductive disorders
Metabolic disease
Future health
women
Fertility and Sterility, Volume 97, Issue 1, 2012, 28–38.e25
Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group PCO: Life-time expression
Birth Puberty Adolescense Fertile period
Senescense
Lowbirth-weight
PubertasprecoxHirsu-tism
Obe-sity
Irregular bleedingsAnovulationInfertility
Type-2 DMCVDCancer
PCOS:Phenotypes are dependent on genetics,
epigenitics and enviroment Tekst starter uden
Sted og
Enhedens 12
Herlev/Gentofte Hospital
Ovarian dysfunction
PCOS
Patophysiology
Hormonal interactions in PCOS
Tekst starter uden
Sted og
Enhedens 17
Herlev/Gentofte Hospital
• The Rotterdam criteria
1. Oligo-/amenorrhoea
2. Clinical and/or biochemical hyperandrogenism
3. Polycystic ovaries (PCO)
And exclusion of other related disorders
Fauser B.C.et el, Hum Repod 2004 Jan;19(1):41-7
Rotterdam consensus:Definition of PCOS
23/05/2018
3
Tekst starter uden
Sted og
Enhedens
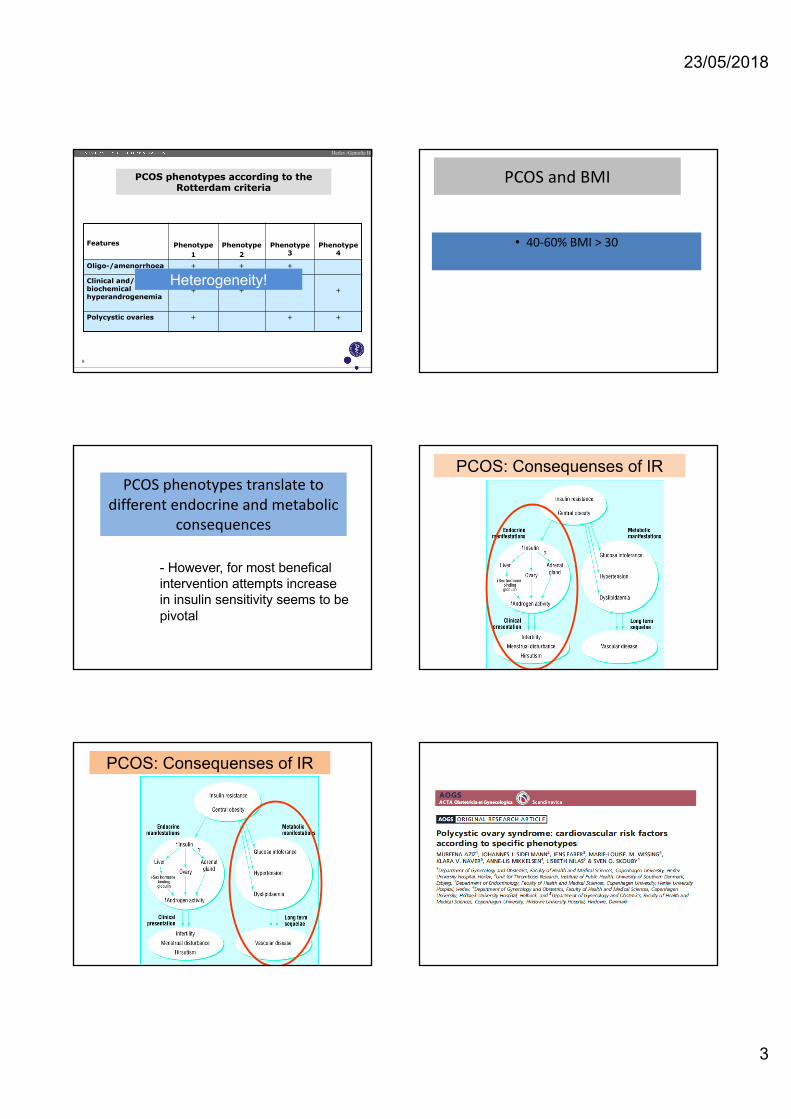
PCOS phenotypes according to the Rotterdam criteria
Features Phenotype 1
Phenotype 2
Phenotype 3
Phenotype 4
Oligo-/amenorrhoea + + +
Clinical and/or biochemical hyperandrogenemia
+ + +
Polycystic ovaries + + +
Herlev /Gentofte Hospital
8
Heterogeneity!
PCOS and BMI
• 40-60% BMI > 30
PCOS phenotypes translate to different endocrine and metabolic
consequences
- However, for most benefical intervention attempts increase in insulin sensitivity seems to be pivotal
PCOS: Consequenses of IR
PCOS: Consequenses of IR
23/05/2018
4
Tekst starter uden
Sted og
Enhedens 25
Herlev/Gentofte Hospital
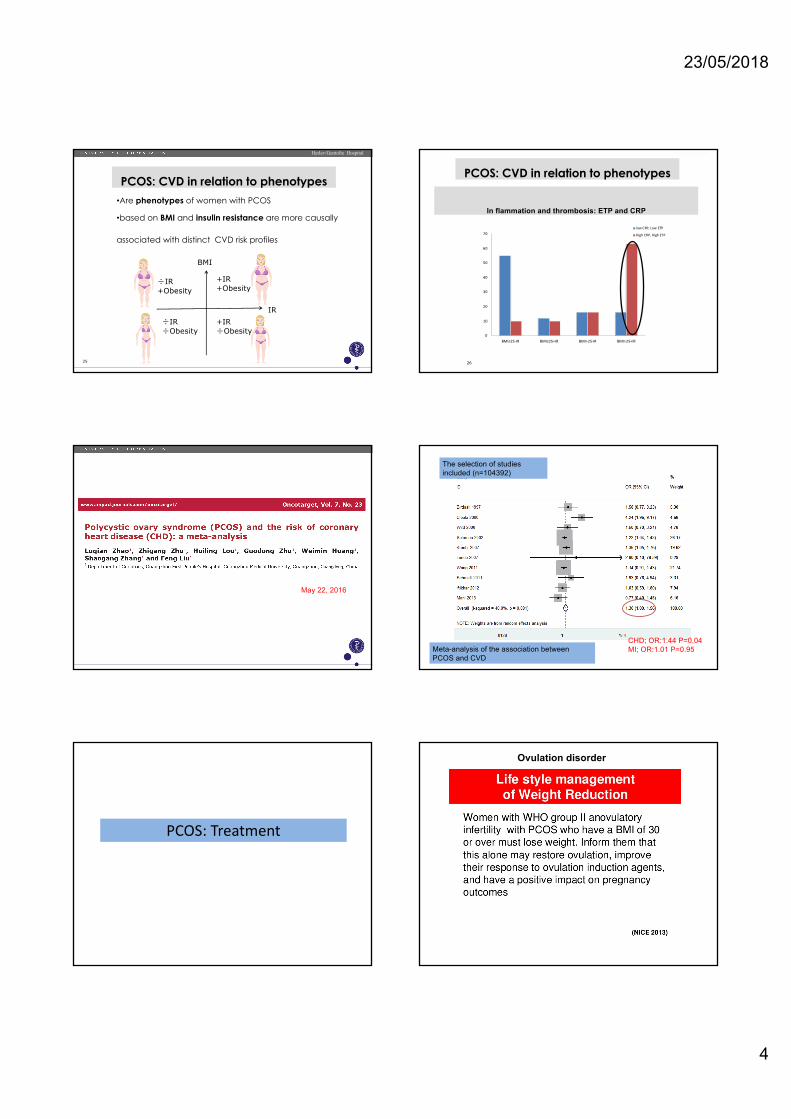
•Are phenotypes of women with PCOS
•based on BMI and insulin resistance are more causally
associated with distinct CVD risk profiles
PCOS: CVD in relation to phenotypes
BMI
IR
+IR+Obesity
+IR�Obesity
�IR�Obesity
�IR+Obesity
26
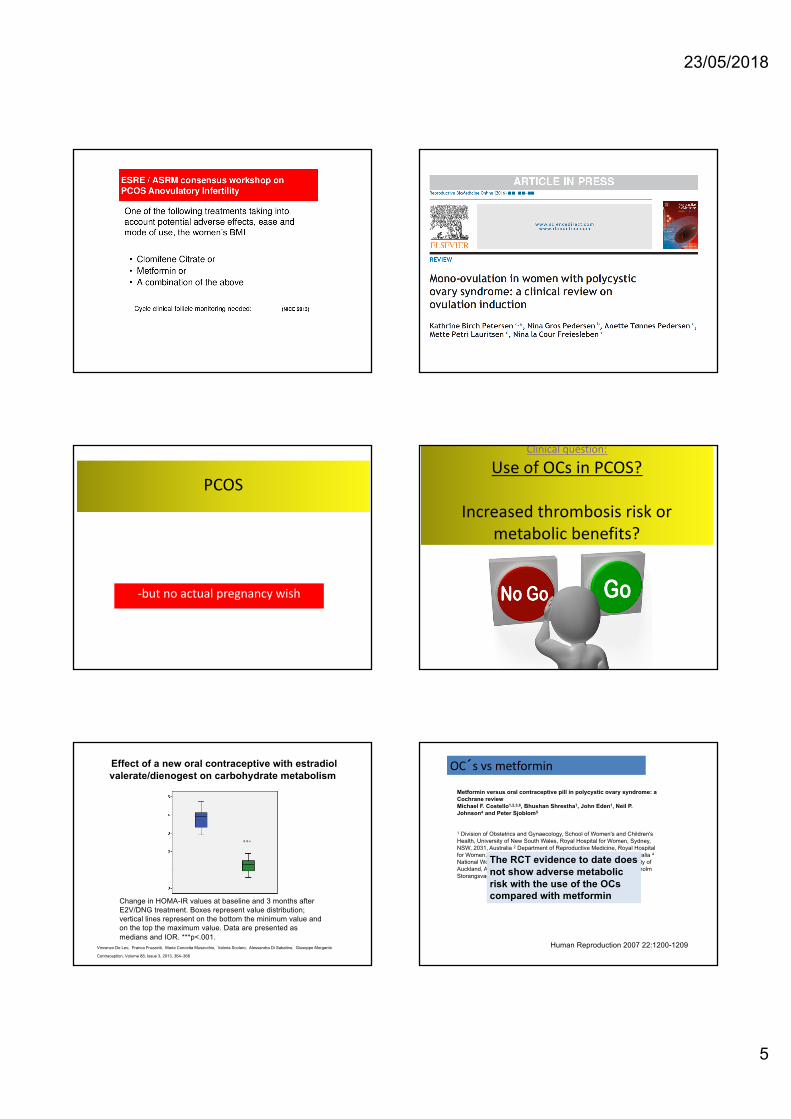
Herlev Hospital
0
10
20
30
40
50
60
70
BMI≤25-IR BMI≤25+IR BMI>25-IR BMI>25+IR
low CRP, Low ETP
High CRP, High ETP
In flammation and thrombosis: ETP and CRP
PCOS: CVD in relation to phenotypes
Tekst starter uden
Sted og
Enhedens
May 22, 2016
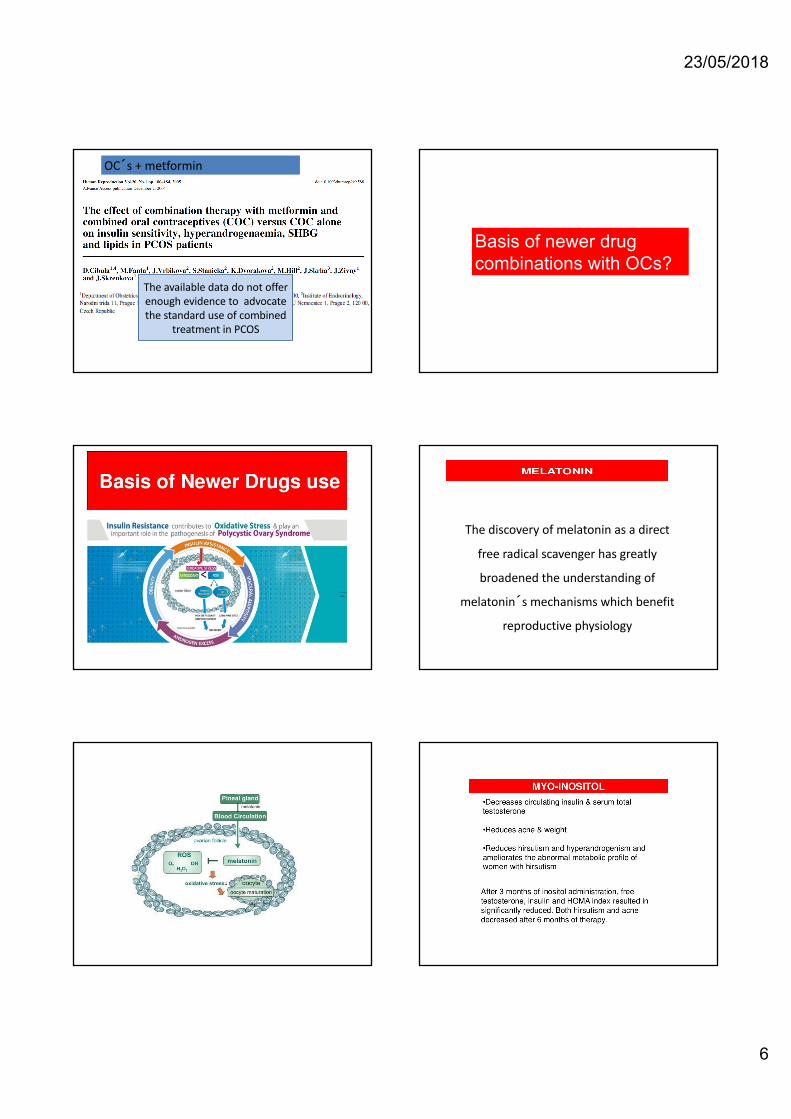
The selection of studies
included (n=104392)
Meta-analysis of the association between
PCOS and CVD
CHD; OR:1.44 P=0,04
MI; OR:1.01 P=0.95
PCOS: Treatment
Ovulation disorder
23/05/2018
5
-but no actual pregnancy wish
PCOS
Clinical question:
Use of OCs in PCOS?
Increased thrombosis risk or metabolic benefits?
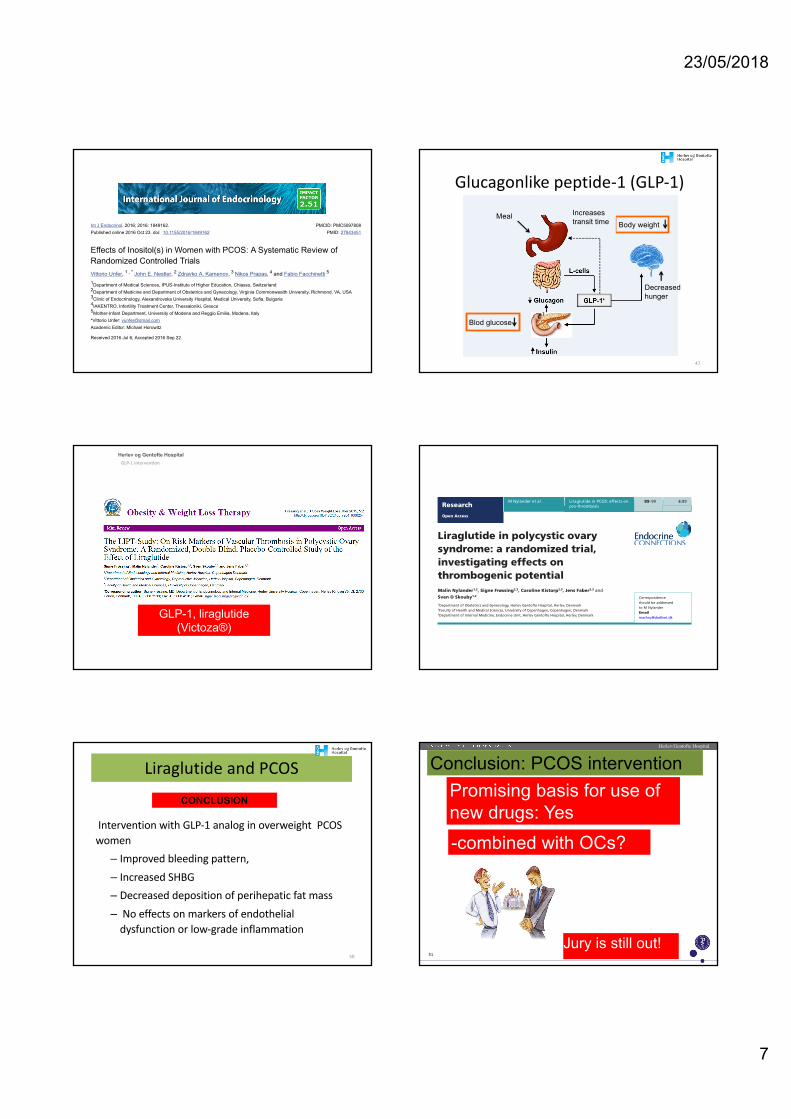
Change in HOMA-IR values at baseline and 3 months after
E2V/DNG treatment. Boxes represent value distribution;
vertical lines represent on the bottom the minimum value and
on the top the maximum value. Data are presented as
medians and IOR. ***p<.001.
Vincenzo De Leo, Franca Fruzzetti, Maria Concetta Musacchio, Valeria Scolaro, Alessandra Di Sabatino, Giuseppe Morgante
Effect of a new oral contraceptive with estradiol valerate/dienogest on carbohydrate metabolism
Contraception, Volume 88, Issue 3, 2013, 364–368
Metformin versus oral contraceptive pill in polycystic ovary syndrome: a Cochrane reviewMichael F. Costello1,2,3,6, Bhushan Shrestha1, John Eden1, Neil P. Johnson4 and Peter Sjoblom5
1 Division of Obstetrics and Gynaecology, School of Women's and Children's Health, University of New South Wales, Royal Hospital for Women, Sydney, NSW, 2031, Australia 2 Department of Reproductive Medicine, Royal Hospital for Women, Sydney, NSW, Australia 3 IVFAustralia, Sydney, NSW, Australia 4National Women's Department of Obstetrics and Gynaecology, University of Auckland, Auckland, New Zealand 5 Fertility Centre Scandinavia, Stockholm Storangsvagen 10, Stockholm, Sweden
OC�s vs metformin
Human Reproduction 2007 22:1200-1209
The RCT evidence to date does not show adverse metabolicrisk with the use of the OCs compared with metformin
23/05/2018
6
The available data do not offer enough evidence to advocate the standard use of combined
treatment in PCOS
OC�s + metformin
Basis of newer drug combinations with OCs?
The discovery of melatonin as a direct
free radical scavenger has greatly
broadened the understanding of
melatonin�s mechanisms which benefit
reproductive physiology
23/05/2018
7
Go to:Go to:
Go to:Go to:
Int J Endocrinol. 2016; 2016: 1849162.Published online 2016 Oct 23. doi: 10.1155/2016/1849162
PMCID: PMC5097808PMID: 27843451
Effects of Inositol(s) in Women with PCOS: A Systematic Review ofRandomized Controlled TrialsVittorio Unfer, John E. Nestler, Zdravko A. Kamenov, Nikos Prapas, and Fabio Facchinetti
Department of Medical Sciences, IPUS-Institute of Higher Education, Chiasso, SwitzerlandDepartment of Medicine and Department of Obstetrics and Gynecology, Virginia Commonwealth University, Richmond, VA, USAClinic of Endocrinology, Alexandrovska University Hospital, Medical University, Sofia, BulgariaIAKENTRO, Infertility Treatment Center, Thessaloniki, GreeceMother-Infant Department, University of Modena and Reggio Emilia, Modena, Italy
*Vittorio Unfer: [email protected] Editor: Michael Horowitz
Received 2016 Jul 6; Accepted 2016 Sep 22.
Copyright © 2016 Vittorio Unfer et al.
This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution,and reproduction in any medium, provided the original work is properly cited.
This article has been cited by other articles in PMC.
Abstract
Polycystic ovary syndrome (PCOS) is a common endocrine disorder, with complex etiology andpathophysiology, which remains poorly understood. It affects about 5–10% of women of reproductiveage who typically suffer from obesity, hyperandrogenism, ovarian dysfunction, and menstrualirregularity. Indeed, PCOS is the most common cause of anovulatory infertility in industrializednations, and it is associated with insulin resistance, type 2 diabetes mellitus, and increasedcardiovascular risk. Although insulin resistance is not included as a criterion for diagnosis, it is acritical pathological condition of PCOS. The purpose of this systematic review is the analysis of recentrandomized clinical trials of inositol(s) in PCOS, in particular myo- and D-chiro-inositol, in order tobetter elucidate their physiological involvement in PCOS and potential therapeutic use, alone and inconjunction with assisted reproductive technologies, in the clinical treatment of women with PCOS.
1. Introduction
Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders affecting womenof reproductive age. PCOS is associated with a wide range of maladies, such as hormonal andmetabolic impairments, ovarian dysfunction, and menstrual irregularity. According to the Rotterdamcriteria developed in 2003, PCOS is diagnosed if two out of the three following features are met:chronic oligo- or anovulation, anatomically polycystic ovaries on ultrasonography, and clinical and/orbiochemical hyperandrogenism [1]. Although not included as criteria, insulin resistance andhyperinsulinemia are important etiologic factors associated with the typical clinical signs and hormonaldisorders of PCOS. Indeed, insulin resistance along with hyperinsulinemia affects approximately 40–50% of PCOS patients, both lean and obese [2–6]; however, in obese women with PCOS theprevalence of insulin resistance accompanied by compensatory hyperinsulinemia approaches 80% [7].Treatment of PCOS with insulin-sensitizing drugs, such as metformin, troglitazone, and pioglitazone,has been shown to improve ovulatory function and reduce circulating androgens, corroborating thecritical link between insulin resistance and the pathogenesis of this syndrome. Of these insulin-
1 , * 2 3 4 5
12345
47
Glucagonlike peptide-1 (GLP-1)
Blod glucose
Body weightMeal
MæthedDecreased hunger
Increases transit time
Herlev og Gentofte HospitalGLP-1 intervention
5/23/18 48
GLP-1, liraglutide (Victoza®)
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
DOI: 10.1530/EC-16-0113http://www.endocrineconnections.org © 2017 The authors
Published by Bioscientifica Ltd
63
Endo
crin
e Co
nnec
tion
s
6:3 89–99M Nylander et al. Liraglutide in PCOS: effects on pro-thrombosis
Endo
crin
e Co
nnec
tion
s
Open Access
Liraglutide in polycystic ovary syndrome: a randomized trial, investigating effects on thrombogenic potentialMalin Nylander1,2, Signe Frøssing2,3, Caroline Kistorp2,3, Jens Faber2,3 and Sven O Skouby1,2
1Department of Obstetrics and Gynecology, Herlev Gentofte Hospital, Herlev, Denmark2Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark3Department of Internal Medicine, Endocrine Unit, Herlev Gentofte Hospital, Herlev, Denmark
Abstract
Polycystic ovary syndrome (PCOS) is associated with increased risk of venous thromboembolism (VTE) and cardiovascular disease (CVD) in later life. We aimed to study the effect of liraglutide intervention on markers of VTE and CVD risk, in PCOS. In a double-blind, placebo-controlled, randomized trial, 72 overweight and/or insulin-resistant women with PCOS were randomized, in a 2:1 ratio, to liraglutide or placebo 1.8 mg/day. Endpoints included between-group difference in change (baseline to follow-up) in plasminogen activator inhibitor-1 levels and in thrombin generation test parameters: endogenous thrombin potential, peak thrombin concentration, lag time and time to peak. Mean weight loss was 5.2 kg (95% CI 3.0–7.5 kg, P < 0.001) in the liraglutide group compared with placebo. We detected no effect on endogenous thrombin potential in either group. In the liraglutide group, peak thrombin concentration decreased by 16.71 nmol/L (95% CI 2.32–31.11, P < 0.05) and lag time and time to peak increased by 0.13 min (95% CI 0.01–0.25, P < 0.05) and 0.38 min (95% CI 0.09–0.68, P < 0.05), respectively, but there were no between-group differences. There was a trend toward 12% (95% CI 0–23, P = 0.05) decreased plasminogen activator inhibitor-1 in the liraglutide group, and there was a trend toward 16% (95% CI −4 to 32, P = 0.10) reduction, compared with placebo. In overweight women with PCOS, liraglutide intervention caused an approximate 5% weight loss. In addition, liraglutide affected thrombin generation, although not significantly differently from placebo. A concomitant trend toward improved fibrinolysis indicates a possible reduction of the baseline thrombogenic potential. The findings point toward beneficial effects of liraglutide on markers of VTE and CVD risk, which should be further pursued in larger studies.
Introduction
With a prevalence of 10%, polycystic ovary syndrome (PCOS) is the most common endocrine disorder among women of fertile age (1). The diagnosis is based on the three Rotterdam criteria: oligo-/amenorrhea, androgen excess
and polycystic ovaries, where a minimum of two should be fulfilled and other etiologies excluded (2). The Rotterdam criteria encompass an ovarian dysfunction, but it is evident that PCOS also has a metabolic component, covering
10.1530/EC-16-0113
Correspondence should be addressed to M Nylander Email [email protected]
Key Words
f polycystic ovary syndrome
f liraglutide
f GLP-1 analog
f thrombin generation
f plasminogen activator inhibitor-1
f low-grade inflammation
Endocrine Connections(2017) 6, 89–99
89–99Liraglutide in PCOS: effects on pro-thrombosis
M Nylander et al.ResearchOpen Access
89:6
Liraglutide and PCOS
Intervention with GLP-1 analog in overweight PCOS women– Improved bleeding pattern, – Increased SHBG– Decreased deposition of perihepatic fat mass– No effects on markers of endothelial
dysfunction or low-grade inflammation
50
CONCLUSIONTekst starter uden
Sted og
Enhedens 51
Herlev/Gentofte Hospital
Promising basis for use of new drugs: Yes
Jury is still out!
-combined with OCs?
Conclusion: PCOS intervention
23/05/2018
8
THANK YOU!