Disclosure – Thierry André
24
A multinational, randomized phase III study of bevacizumab with FOLFOX4 or XELOX vs. FOLFOX4 alone as adjuvant treatment for colon cancer: Results and subgroup analyses from the AVANT trial André T, Van Cutsem E, Schmoll HJ, Tabernero J, Clarke S, Moore MJ, Cunningham D, Cartwright TH, Hecht JR, Rivera F, Im SA, Bodoky G, Salazar R, Maindrault-Goebel F, Shmueli E, Bajetta E, Makrutzki M, Shang A, de Gramont A, Hoff PM, on behalf of the AVANT Investigators
description
A multinational, randomized phase III study of bevacizumab with FOLFOX4 or XELOX vs. FOLFOX4 alone as adjuvant treatment for colon cancer: R esults and s ubgroup analyses from the AVANT trial. - PowerPoint PPT Presentation
Transcript of Disclosure – Thierry André

A multinational, randomized phase III
study of bevacizumab with FOLFOX4 or
XELOX vs. FOLFOX4 alone as adjuvant
treatment for colon cancer: Results and
subgroup analyses from the AVANT trial
André T, Van Cutsem E, Schmoll HJ, Tabernero J, Clarke S,
Moore MJ, Cunningham D, Cartwright TH, Hecht JR, Rivera
F, Im SA, Bodoky G, Salazar R, Maindrault-Goebel F,
Shmueli E, Bajetta E, Makrutzki M, Shang A, de Gramont A,
Hoff PM, on behalf of the AVANT Investigators

Disclosure – Thierry André
Honoraria/consulting:
Roche
Sanofi-Aventis
For work unrelated to the AVANT study

Rationale for Adjuvant Bevacizumab
The roles of angiogenesis and VEGF in colorectal tumour growth are well established
Using anti-VEGF therapy such as bevacizumab when micrometastases are dormant and potentially reliant on VEGF may prevent the ‘angiogenic switch’1,2
Specifically in colorectal cancer, increased VEGF expression correlates with invasiveness, vascular density, metastasis and recurrence2–5
Clinical studies show that treatment with bevacizumab increases PFS and/or OS in metastatic disease5,6
1. Folkman J. N Engl J Med 19952. Carmeliet P. Nature 2000
3. Takahashi Y. Cancer Res 19954. Warren RS. J Clin Invest 1995
5. Hurwitz H. N Eng J Med 20046. Saltz L. J Clin Oncol 2008VEGF = vascular endothelial growth factor

NSABP C-08 Study Design
Duration of treatment 24 weeks 24 weeks
Primary endpoint: disease-free survival
mFOLFOX6
mFOLFOX6 + Bev(5mg/kg q 2 weeks)
Observation
Bev mono(5mg/kg q 2 weeks)
Stage II/III colon cancer
(n=2700)
R
Wolmark N. ASCO 2009Allegra C. J Clin Oncol 2010

XELOX + bevacizumab
FOLFOX4+ bevacizumab
Bevacizumab monotherapy
Bevacizumab monotherapy
Observation
Follow-up
Follow-up
Follow-upFOLFOX4
Surgery for high-risk stage II
or stage III
colon cancer (N=3451)
Bev 5 mg/kg q2w
Bev 7.5 mg/kg q3w
Bev 7.5 mg/kg q3w
AVANT Study Design
Bev 7.5 mg/kg q3w
24 weeks24 weeks 24 weeks24 weeks

Analysis Plan
Primary endpoint:
DFS in stage III patients*
– STEP 1Test global hypothesis:DFS (FOLFOX4) = DFS (FOLFOX4 + Bev) = DFS (XELOX + Bev)If p≤0.05 proceed to
– STEP 2Compare FOLFOX4 + Bev vs. FOLFOX4 and XELOX + Bev vs. FOLFOX4
Secondary endpoints:
OS in stage III patients
Safety
Non-inferiority DFS and OS: FOLFOX4 + Bev vs. XELOX + Bev (if co-primary objectives met)
*non-stratified log-rank test (two-sided, at overall 5% -level), power at least 80%

Study Conduct
Conducted worldwide:
– 330 centres
– 34 countries
– 8 regions (stratified)
3451 patients randomized:
– between 20 December 2004 and 08 June 2007
– 2867 patients with Stage III disease
Data cut-off date: 30 June 2010 (3-year minimum follow-up)
Median duration of follow-up was 48 months (range 0–66)

Patient Demographics (ITT Stage III)FOLFOX4(N=955)
FOLFOX4 + Bev(N=960)
XELOX + Bev(N=952)
Male, % 55 51 55
Median age, years 59 58 59
Race, % White / Asian 83 / 15 85 / 12 84 / 13
ECOG PS 0, % 87 86 87
Primary tumour T4, % 19 17 19
Nodal status, % N1 / N2 61 / 39 61 / 39 60 / 40
No. of lymph nodes, % <12 / ≥12 28 / 72 27 / 73 29 / 71
Median duration of follow-up, months* 48.3 48.3 48.4
*Calculated for alive patients as no. of months from randomization to last date patients known to be alive*Calculated for alive patients as no. of months from randomization to last date patients known to be alive

AEs of Special Interest for Bevacizumab(All Patients)
Grade 3–5, %FOLFOX4(N=1126)
FOLFOX4 + Bev(N=1145)
XELOX + Bev(N=1135)
All 9 23 18
Bleeding / haemorrhage 0.5 1.2 0.4
Hypertension 1.1 10.6 10.1
Proteinuria 0.1 0.9 1.1
Fistula / abscess 0.4 1.4 0.8
GI perforation 0.1 0.7 0.2
Congestive heart failure 0.3 0.3 0.1
Wound-healing complication 0.4 0.3 0.4
Venous thromboembolism 5.4 8.0 4.6
Arterial thromboembolism 1.0 1.5 1.3
60-day mortality rate 0.2 0.4 0.5
AE onset between time of very first drug intake and 183 days after very last drug intakeAE onset between time of very first drug intake and 183 days after very last drug intake

AEs of Special Interest for Bevacizumab(All Patients)
Grade 3–5, %FOLFOX4(N=1126)
FOLFOX4 + Bev(N=1145)
XELOX + Bev(N=1135)
All 9 23 18
Bleeding / haemorrhage 0.5 1.2 0.4
Hypertension 1.1 10.6 10.1
Proteinuria 0.1 0.9 1.1
Fistula / abscess 0.4 1.4 0.8
GI perforation 0.1 0.7 0.2
Congestive heart failure 0.3 0.3 0.1
Wound-healing complication 0.4 0.3 0.4
Venous thromboembolism 5.4 8.0 4.6
Arterial thromboembolism 1.0 1.5 1.3
60-day mortality rate 0.2 0.4 0.5
AE onset between time of very first drug intake and 183 days after very last drug intakeAE onset between time of very first drug intake and 183 days after very last drug intake

Summary of Results For DFS (ITT Stage III)
FOLFOX4(N=955)
FOLFOX4 + Bev(N=960)
XELOX + Bev(N=952)
Lost to follow-up, n (%) 62 (7) 52 (5) 52 (6)
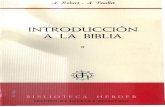
Patients with event, n (%) 237 (25) 280 (29) 253 (27)
P-value for global hypothesis p=0.2024
3-year DFS rate, % 76 73 75

DFS (ITT Stage III) Data Cut-off Date: 30 June 2010 (3-Year Minimum Follow-Up)
FOLFOX4(N=955)
FOLFOX4 + Bev(N=960)
XELOX + Bev(N=952)
HR(95% CI)
1.17(0.98, 1.39)
1.07(0.90, 1.28)
955960952
890921900
823868865
779791784
740728722
708695688
451436415
FOLFOX4FOLFOX4 + BevXELOX + Bev
Number at risk
609586580
282280268
FOLFOX4
FOLFOX4 + Bev
XELOX + Bev
Event-free rate
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
6 18 30 36 42 480 12 24
Time (months)
54 60 66 72
121123110
010
323328
000

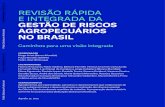
DFS: Cumulative Hazard Ratio (ITT Stage III)
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1
Time from randomization (years)
1.5 2 2.5 3
0.63 0.61
1.001.02
1.121.15
1.11 1.13 1.131.08
FOLFOX4 + Bev
XELOX + Bev
Hazard ratio

Site of Recurrence (ITT Stage III)
FOLFOX4(N=955)
FOLFOX4 + Bev(N=960)
XELOX + Bev(N=952)
Pts with tumour recurrence, %* 23 26 23
Local recurrence 4 4 5
Regional lymph nodes 2 2 2
Distant lymph nodes 4 3 3
Liver 9 9 7
Lung 5 7 6
Other 6 9 7
1 involved site, % 17 20 19
>1 involved site, % 6 6 5
*And without evidence of disease at randomization; percentages based on N*And without evidence of disease at randomization; percentages based on N

Interim OS (ITT Stage III)Median duration of follow-up 48 months (range 0–66)
FOLFOX4(N=955)
FOLFOX4 + Bev(N=960)
XELOX + Bev(N=952)
EventsHR(95% CI)
115 (12%) 151 (16%)1.31
(1.03, 1.67)
145 (15%)1.27
(0.99, 1.62)
955960952
914942920
899925908
884900894
863869861
844835840
573573546
FOLFOX4FOLFOX4 + BevXELOX + Bev
Number at risk
776763765
461449445
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
6 18 30 36 42 480 12 24
Time (months)
54 60 66 72
288269290
010
637064
000
Event-free rate FOLFOX4
FOLFOX4 + Bev
XELOX + Bev

Time from Recurrence / New Occurrence to Death (ITT Stage III patients)
FOLFOX4 + BevN=259
XELOX + BevN=228
HR(95% CI)
1.23( 0.95, 1.60)
1.10(0.84, 1.44)
222259228
178209193
135158158
111104110
656579
343947
748
FOLFOX4FOLFOX4 + BevXELOX + Bev
Number at risk
161626
212
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
6 18 30 36 42 480 12 24Time (months)
54 60 66 72
000
000
000
000
FOLFOX4
FOLFOX4 + Bev
XELOX + Bev
Event-free rate
Recurrence/new occurrence Recurrence/new occurrence

Subgroup analysis

Hazard Ratio for DFS by Subgroup(ITT Stage III): FOLFOX4 + Bev vs FOLFOX4
All
Age category (years)
Category
T stage
1681
1915
204
1366345
1.17
1.17
1.23
1.270.95
EstimateN
234 1.19
Gender 898 1.321017 1.07
Race category* 2541604
2.181.09
No. of lymph nodes analyzed 5301379
1.261.13
N stage 1175740
1.370.99
Subgroup
All
<70
T3T4
≥70
Other
Hazard ratio
0.2 0.4 0.6 1 2 3 4 5 6 10 20
Favours FOLFOX4+Bev Favours FOLFOX4Favours FOLFOX4+Bev Favours FOLFOX4
FemaleMale
Asian
White
<12≥12
N1N2
*Other races contain very small number of patients (n=55) and therefore not displayed*Other races contain very small number of patients (n=55) and therefore not displayed

Hazard Ratio for DFS by Subgroup(ITT Stage III): XELOX + Bev vs FOLFOX4
All
Age category (years)
Category
T stage
EstimateN
Gender
Race category*
No. of lymph nodes analyzed
N stage 1157750
1.140.99
1907 1.07
1652 1.04255 1.28
197 0.84
1349 1.07361 1.11
8571050
1.111.04
2621586
1.521.04
5441359
1.061.08
Subgroup
All
<70
T3T4
≥70
Other
Hazard ratio
0.2 0.4 0.6 1 2 3 4 5 6 10 20
Favours XELOX+Bev Favours FOLFOX4Favours XELOX+Bev Favours FOLFOX4
FemaleMale
Asian
White
<12≥12
N1N2
*Other races contain very small number of patients (n=55) and therefore not displayed*Other races contain very small number of patients (n=55) and therefore not displayed

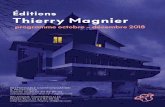
DFS by N Stage (ITT Stage III)
585370590370572380
550340562359545355
528295541327533332
506273501290495289
487253464264462260
475233451244448240
305146279157267148
FOLFOX4 III N1FOLFOX4 III N2FOLFOX4 + Bev III N1FOLFOX4 + Bev III N2XELOX + Bev III N1XELOX + Bev III N2
Number at risk
411198379207376204
19092
18199
17791
784375487436
000100
221020131711
000000
N2
N1
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.70.8
0.9
1.0
6 18 30 36 42 480 12 24
Time (months)
54 60 66 72
Event-free rate
FOLFOX4 (N1)
FOLFOX4 (N2)
FOLFOX4 + Bev (N1)
FOLFOX4 + Bev (N2)
XELOX + Bev (N1)
XELOX + Bev (N2)
60%
40%

Summary and Conclusions
Addition of bevacizumab to FOLFOX4 or XELOX did not prolong DFS in adjuvant treatment of stage III colon cancer
– chemotherapy alone arm was favoured numerically
Bevacizumab treatment effect was not constant over time
– transient favourable effect can be seen within 1 year, which is in-line with NSABP C-08
– although transient favourable effect is more dominant in N2 subgroup, overall treatment effect is lost
Further subgroup analysis results for DFS were consistent with those seen in overall stage III colon cancer population
Immature OS data suggest a potential detriment. Follow up will continue until at least June 2012, for 5 years minimum follow up for analysis of OS
Biomarker programme might help us to understand results seen with bevacizumab in the adjuvant setting

Food for Thought
Why is an active therapy in advanced disease not active in the adjuvant setting?
Is it something different?
Is bevacizumab induction of tumour cell dormancy possible?
Is induction of pro-survival pathway and tumour resistance a possibility?
Does bevacizumab show any transient favourable effect in relation to action on undetectable macro-metastases?
1. Goss PE. Nat Rev Cancer 2010 2. Almog N. Cancer Lett 2010
3. Naumov GN. Clin Exp Metastasis 20094. Ebos JM. Clin Cancer Res 2009
1. Goss PE. Nat Rev Cancer 2010 2. Almog N. Cancer Lett 2010
3. Naumov GN. Clin Exp Metastasis 20094. Ebos JM. Clin Cancer Res 2009

Acknowledgments
Thanks to the following:
Patients and their families
Investigators, study coordinators and nurses at 330 centres in 34 countries
AVANT study team at Genentech, Roche & Chugai

Thank you for your attention