Discharge Documents: How well do they support care ...
51
© 2018 ECRI INSTITUTE © 2018 ECRI INSTITUTE Discharge Documents: How well do they support care coordination? Erin Sparnon, MEng, Engineering Manager Polly Tremoulet, PhD, Human Factors Scientist
Transcript of Discharge Documents: How well do they support care ...

© 2018 ECRI INSTITUTE© 2018 ECRI INSTITUTE
Discharge Documents: How well do they
support care coordination?
Erin Sparnon, MEng, Engineering Manager
Polly Tremoulet, PhD, Human Factors Scientist

© 2018 ECRI INSTITUTE
© 2018 ECRI INSTITUTE
• Power Point Slides viewed here• Today’s session is recorded• Today’s slides and recording will be
posted to all PSO web portals.

© 2018 ECRI INSTITUTE
• Please submit your text questions andcomments using the Questions Panel
Remember…
How to Ask Questions

© 2018 ECRI INSTITUTE
Download Slides

© 2018 ECRI INSTITUTE
This activity has been approved for 1.0 California State Nursing contact hour
by the provider, Debora Simmons, who is approved by the California Board
of Registered Nursing, Provider Number CEP 13677.
All faculty members involved in ECRI Institute’s July 19, 2018 live webinar,
Discharge Documents – How Well Do They Support Care Coordination?
have disclosed in writing that they do not have any relevant conflicts or
financial affiliations.

© 2018 ECRI INSTITUTE
To qualify for credit:
Credit will only be issued to attendees that are individually
registered and attend the entire program. Each individual
participant must logon prior to the start of the program and remain
on the line for the entirety of the program. This is how individual
timed attendance is verified. In addition, you must complete an
attestation survey included in the post webinar evaluation at the
conclusion of the webinar. Once all that information is verified, a
certificate will be e-mailed to you within 60 days of today’s
program.
© 2018 ECRI INSTITUTE
Today’s Speaker: Dr. Patrice Tremoulet
Dr. Patrice Tremoulet is an Assistant Professor of Psychology at Rowan University and a
Human Factors consultant for Children’s Hospital of Philadelphia (CHOP) and ECRI
Institute. Before joining ECRI as a consultant, she conducted a broad range of human-
machine interaction research at Bell Laboratories, Lockheed Martin, and Drexel
University. She is currently leading a CHOP effort exploring how to ensure that children
can ride safely in self-driving vehicles and is supporting multiple ECRI projects by helping
to assess the usability of different medical devices.
Dr. Tremoulet received her Ph.D. in Psychology and a certificate in Cognitive Science
from Rutgers University, an M.S. in Operations Research from Stanford University and a
B.S.E. in Operations Research and a certificate in Engineering Management Systems
from Princeton University.

© 2018 ECRI INSTITUTE
Agenda
Learning Objectives
Motivation
■ Patient discharge documents* used for clinical information
Approach
■ Expert review to assess how well they support this use
Recommendations
Future directions
*Referred to by many names : discharge instructions, patient instructions, clinical summaries, after visit summaries, summary of care documents

© 2018 ECRI INSTITUTE
Agenda
Learning Objectives
Motivation
■ Patient discharge documents* used for clinical information
Approach
■ Expert review to assess how well they support this use
Recommendations
Future directions
*Referred to by many names : discharge instructions, patient instructions, clinical summaries, after visit summaries, summary of care documents

© 2018 ECRI INSTITUTE
Learning Objectives
1. Describe a care coordination challenge & a common ‘work-around’
2. Share our method for evaluating usability of medical documentation
3. Identify best practices for improving patient discharge documents
Terminology: human factors, usability, heuristic evaluation, heuristics, after visit summary, discharge summary

© 2018 ECRI INSTITUTE
Physicians are using patient-facing documents to
obtain information about acute care visits
Discharge summaries generated by inpatient providers’ EHR systems
often do not reach outpatient providers.
■ Poor integration/lack of interoperability
■ Inaccurate or missing contact information
■ No required timeframe for sending them & no confirmation of receipt when sent
No quick fix in sight
Patients often bring their discharge documents to follow-up visits
■ These often give more information than patients could recall on their own

© 2018 ECRI INSTITUTE
Why Study Physician Use of Patient Discharge Documents?
Patient-facing documents used for care coordination more often than
inpatient providers realize*
■ Problems that prevent discharge summaries from being shared with outpatient providers
are not going to be resolved quickly
Other studies* assess them from the perspective of patients and caregivers
■ few have considered usability from the perspective of outpatient providers
Patient discharge documents must be improved to better support care
coordination AND to be more usable by patients and caregivers
*Gorry, T., Personal communication with ECRI Institute. 2017.
**Sarzynski, E., et al., 2016; Federman, A.D., et al., 2017; Unnewehr, M., et al., 2015; Newnham, H., et al., 2017.

© 2018 ECRI INSTITUTE
ECRI Team’s Novel Approach
Develop ‘medical document usability heuristics’ to enable expert reviews of
documents produced by electronic health record (EHR) systems
Conduct collaborative expert reviews with human factors and clinical experts
Assess simulations of discharge documents produced by EHR systems

© 2018 ECRI INSTITUTE
Four step process
1. Create simulated patient
discharge documents
2. Develop ‘medical
documentation heuristics’
3. Experts apply heuristics to
identify & rate usability issues
4. Generate recommendations
to improve usability

© 2018 ECRI INSTITUTE
What did we assess?
2 Patient discharge
document examples From hospitals w/
different EHR vendors
2 pediatric test patients,Created by National Institutes of
Standards and Technology (NIST)
■ 2 year old with ear infection
■ 16 year old with injured knee
1. Simulated patient discharge
documents
4 simulated
documents

© 2018 ECRI INSTITUTE
Two different approaches1. Simulated
patient discharge documents
Hospital partner 2 created an
anonymized version of a discharge
document from an actual patient
(replacing patient information with
fictitious data)
ECRI created simulations, replacing
the anonymized patient data with
NIST test patient data, and
replacing hospital and doctor
names with fictitious ones
Hospital partner 1 created an
electronic health record for each of
the NIST patient cases
Hospital partner 1 used its EHR
system to produce discharge
documents for these test patients
ECRI created simulations of those
documents (replacing hospital and
doctor names with fictitious ones)

© 2018 ECRI INSTITUTE
Developing heuristics
Reviewed previously validated heuristics for:
■ software user interfaces
■ medical devices
■ online documentation usability heuristics
Eliminated those that don’t apply (most!)
Consulted literature on “good” writing
■ Generic writing guidelines
■ Medical documentation specific guidelines (extensive)
Extracted relevant recommendations
Removed duplicates & transformed recommendations into heuristics
2. Medical Documentation
Heuristics

© 2018 ECRI INSTITUTE
Developing Heuristics, Continued
Organized heuristics into 5 general categories*
■ Readability
■ Minimalism
■ Comprehensibility
■ Content
■ Organization
Developed examples for each retained candidate
* Easier to perform evaluations & communicate results
2. Medical Documentation
Heuristics
© 2018 ECRI INSTITUTE
Heuristic Category Definitions
Readability: Information is presented in a manner that is easy to read.
Content: All presented information is relevant to either a clinical expert or the
patient/caregiver and no needed information is missing.
Comprehensibility: It is easy for readers to make sense of presented information.
Minimalism: Information is presented as simply and succinctly as possible.
Organization: Information is ordered logically and grouped into reasonably-sized
sections with prominent and meaningful headings and subheadings.
2. Medical Documentation
Heuristics
© 2018 ECRI INSTITUTE
Heuristic Evaluation
Four teams, each comprised of a clinician and a human factors engineer
■ Clinical experts all experienced as primary care providers
■ Human factors experts all currently working in healthcare
Human Factors experts introduced heuristics and explained evaluation
process to clinical experts
Clinical experts provided severity ratings for each potential issue:
■ 0= not an issue; 1=cosmetic, 2=minor, 3=major, 4=catastrophic
3. Apply heuristics to identify & rate usability issues

© 2018 ECRI INSTITUTE

© 2018 ECRI INSTITUTE
23
Content, Organization issues
Readability & Content issues

© 2018 ECRI INSTITUTE
24
Organization issue
Minimalism & Readability issues

© 2018 ECRI INSTITUTE

© 2018 ECRI INSTITUTE
INSERT H2P1 screenshots here….

© 2018 ECRI INSTITUTE
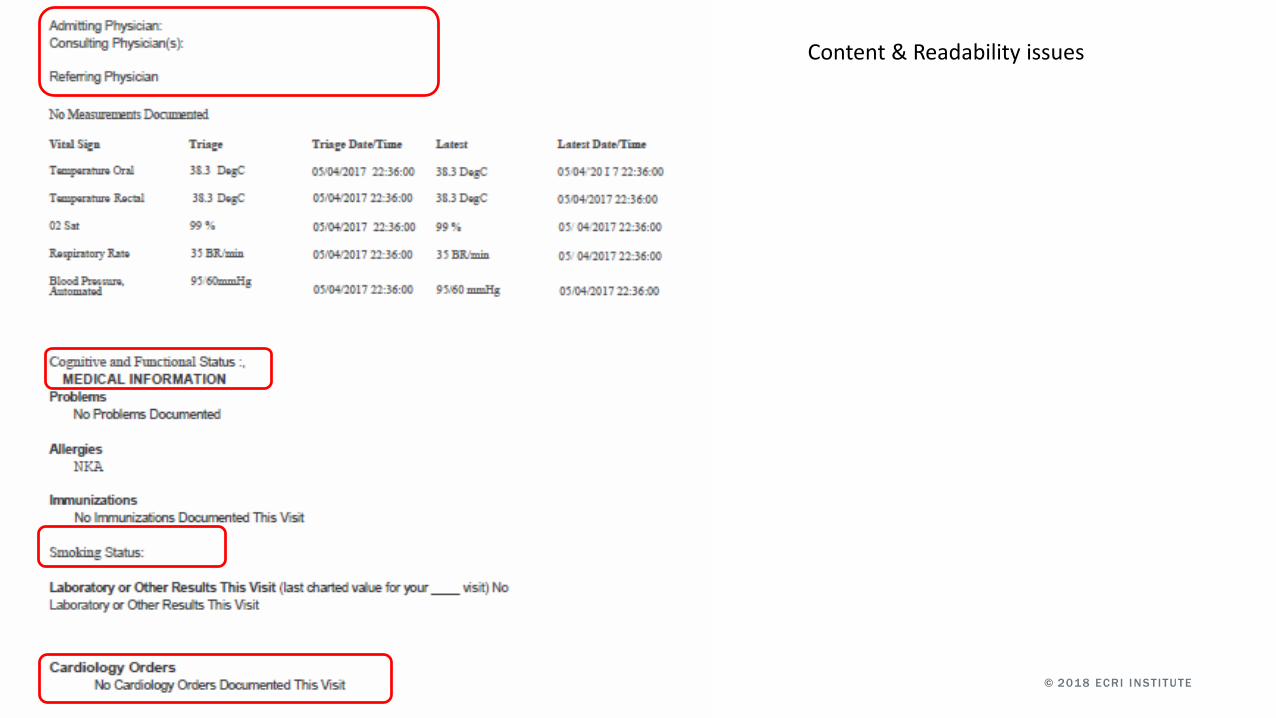
Content & Readability issues
Comprehensibility issues
© 2018 ECRI INSTITUTE
Content & Readability issues

© 2018 ECRI INSTITUTE
Usability issue counts and average severity ratings for each evaluated document, grouped by heuristic category
Hospital 1, Patient 1 (severity)
Hospital 1, Patient 2 (severity)
Hospital 2, Patient 1 (severity)
Hospital 2, Patient 2 (severity)
Total (severity)
Readability 15 (2.33) 15 (2.2) 9 (2.66) 8 (2.31) 47 (1.9)
Minimalist 4 (2.25) 3 (2.67) 8 (2.75) 8 (2.88) 23 (2.11)
Comprehensibility 6 (2.33) 5 (2.2) 12 (3.08) 8 (2.88) 31 (2.1)
Content 15 (2.47) 15 (2.63) 17 (2.94) 25 (2.96) 72 (2.2)
Organization 9 (1.89) 10 (1.7) 16 (2.73) 16 (2.78) 51 (1.82)
TOTAL 49 (2.25) 48 (2.28) 62 (2.83) 65 (2.76) 224 (2.57)
Severity scale: 1 = cosmetic, 2 = minor, 3 = major, 4 = catastrophic
RESULTS

© 2018 ECRI INSTITUTE

© 2018 ECRI INSTITUTE
Clear and consistently formatted section labels and sub-section headings, using white space to ensure the document is legible
Patient and provider information up front and clearly labelled

© 2018 ECRI INSTITUTE
Clear, organized table explains how to arrange follow-up appointments
Medication information and instructions clearly labeled and listed

© 2018 ECRI INSTITUTE© 2018 ECRI INSTITUTE
Best Practice Recommendations
Given that EHR-generated patient discharge documentation may be the primary
information source for the outpatient provider, how can we make them more
usable and understandable for that provider?
4. Generated recommendations
to improve usability
© 2018 ECRI INSTITUTE
Detailed Recommendations: Content
1. Include 6 items Joint Commission mandates for
hospital discharge summaries:
■ Reason for Hospitalization
■ Significant Findings
■ Procedure and Treatment provided
■ Patient’s discharge condition
■ Patient and family instructions
■ Attending physician’s signature
2. Ensure any information relevant to outpatient physician
and patient follow-up care can be included in document
4. Generated recommendations
to improve usability
© 2018 ECRI INSTITUTE
Detailed Recommendations: Content
3. Ensure headers and footers contain meaningful information
4. Ensure proper use of medical, nonmedical, and billing terminology
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations: Organization
5. Establish consensus across stakeholders on standardized order and format
for presenting information
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations: Organization
6. If multiple diagnoses are present, make sure they are
clearly defined and differentiated, and that primary
diagnosis is explained up front.
7. Ensure that content matches headings and sub-
headings in each section
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations:
Readability
8. Use consistent font size and type, indents, and
spacing throughout document
9. Ensure sufficient & consistent use of color and contrast
10. Emphasize important information in each section
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations: Readability
11. Within each section, present discrete ideas and information as
separate bullets or paragraphs
12. Balance text and white space
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations: Comprehensibility
& Minimalism
13. Present information clearly and concisely
14. Use consistent terminology
15. Remove irrelevant information
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
Detailed Recommendations: Comprehensibility
16. Explain any abbreviations
4. Generated recommendations
to improve usability

© 2018 ECRI INSTITUTE
It’s Not Just patient discharge documents:
Improving care coordination in the long term
Establish policies on timeliness of distributing discharge documents.
Configure EHR systems so they provide confirmations or failure notices
about delivery of information to outpatient providers.
Pressure vendors to make systems inter-operable
Adopt Joint Commission mandate on discharge summary components

© 2018 ECRI INSTITUTE
Summary
Spread the word: patient-facing discharge
documents are being used for clinical
communication
ECRI offers guidance to improve discharge
documents so they support clinical communication
AND are easier for patients to use

© 2018 ECRI INSTITUTE
Summary: What can Hospitals do?
Learn how information from EHR gets pulled into generated documents
■ Ensure headings and subheadings match the content
■ Emphasize important information in each section
Work with vendors to modify EHR modules used to generate documents
■ Add new section(s) specifically directed towards clinical readers

© 2018 ECRI INSTITUTE
Summary: What can EHR vendors do?
Use our heuristics to guide the redesign of generic templates used to generate
clinical documentation
■ Establish standardized, logical order and format to present information
Important information upfront
Get feedback from document recipients
Follow Joint Commission’s Standard IM.6.10
Give acute care provider organizations more flexibility
■ Enable users to add supplementary notes or additional content into automatically
generated sections

© 2018 ECRI INSTITUTE
Conclusions
Long term: better EHR
interoperability will help improve
coordination of care
Short term, improve discharge
documents
■ Make them more usable for both
providers and patients
© 2018 ECRI INSTITUTE
Next Steps: Future Directions
Expand scope
■ Consider care coordination needs of different types of outpatient providers
■ Assess usability from patient perspective
Apply heuristics to assess discharge summaries & other medical documents
Collect stakeholder inputs & develop user requirements
■ Work with EHR vendors and inpatient and outpatient providers to redesign discharge
document templates
© 2018 ECRI INSTITUTE
Questions
Polly Tremoulet
Human Factors Scientists, Health Devices Group
ECRI Institute
Erin Sparnon
Engineering Manager, Health Devices Group
ECRI Institute

© 2018 ECRI INSTITUTE
References
ECRI Institute. Postacute care, aging services, primary care: hospitals look beyond their walls. Contin Care Risk
Manage [online]. 2016 Nov 18 [cited 2017 Sep 14].
Australian Commission on Safety and Quality in Health Care (2011), Electronic Discharge Summary Systems Self-
Evaluation Toolkit, ACSQHC, Sydney. https://www.safetyandquality.gov.au/wp-content/uploads/2012/01/EDS-self-
eval-toolkit-sept2011.pdf
Health Information and Quality Authority (2013), National Standard for Patient Discharge Summary Information, HIQA,
Ireland. https://www.hiqa.ie/system/files/National-Standard-Patient-Discharge-Summary.pdf
Maher B., Drachsler H., Kalz M., et al. Use of mobile applications for hospital discharge letters – improving handover
at point of practice. https://pdfs.semanticscholar.org/6d6c/4af54b15e26f167f7be6db106094f54c4bd5.pdf
National Academy of Sciences. Overview of issues involved in creating better discharge instructions. In: Facilitating
patient understanding of discharge instructions: workshop summary. Washington (DC): National Academies Press;
2014 Dec 1.
Sarzynski, E., et al., Opportunities to improve clinical summaries for patients at hospital discharge. BMJ Qual Saf,
2016: p. bmjqs-2015-005201.
Federman, A.D., et al., Patient and clinician perspectives on the outpatient after-visit summary: a qualitative study to
inform improvements in visit summary design. Journal of the American Medical Informatics Association, 2017. 24(e1):
p. e61-e68.

© 2018 ECRI INSTITUTE
References, continued
Unnewehr, M., et al., Optimizing the quality of hospital discharge summaries–a systematic review and practical
tools. Postgraduate medicine, 2015. 127(6): p. 630-639.
Newnham, H., et al., Discharge communication practices and healthcare provider and patient preferences,
satisfaction and comprehension: A systematic review. Int J Qual Health Care, 2017: p. 1-17.
Solan LG, Sherman SN, DeBlasio D, Simmons JM. Communication challenges: a qualitative look at the relationship
between pediatric hospitalists and primary care providers. Academic pediatrics. 2016 Jul 31;16(5):453-9.
Coghlin DT, Leyenaar JK, Shen M, et al.. Pediatric discharge content: a multisite assessment of physician
preferences and experiences. Hospital pediatrics. 2014 Jan;4(1):9.
Shen MW, Hershey D, Bergert L, et al. Pediatric hospitalists collaborate to improve timeliness of discharge
communication. Hospital Pediatrics. 2013 Jul 1;3(3):258-65.
Ruth JL, Geskey JM, Shaffer ML, Bramley HP, Paul IM. Evaluating communication between pediatric primary care
physicians and hospitalists. Clinical pediatrics. 2011 Oct;50(10):923-8.
Nguyen OK, Kruger J, Greysen SR, Lyndon A, Goldman LE. Understanding how to improve collaboration between
hospitals and primary care in postdischarge care transitions: A qualitative study of primary care leaders'
perspectives. Journal of hospital medicine. 2014 Nov 1;9(11):700-6.

© 2018 ECRI INSTITUTE
Next PSO Webinar
September 20th
Keeping Staff Safe in Acute Care and in the
Community
Partnering with Virginia PSO and their providers
■ Carilion Clinic Home Health
■ UVa Medical Center