DISASTER IN SOUTH ASIA (SAARC REGION) Roy Abraham Kallivayalil MD, DPM Gen. Secretary, Indian...
30
DISASTER IN SOUTH ASIA DISASTER IN SOUTH ASIA (SAARC REGION) (SAARC REGION) Roy Abraham Kallivayalil MD, DPM Roy Abraham Kallivayalil MD, DPM Gen. Secretary, Indian Psychiatric Gen. Secretary, Indian Psychiatric Society & Society & Secretary General, SAARC Psych. Secretary General, SAARC Psych. Federation Federation Associate Professor of Psychiatry Associate Professor of Psychiatry Medical College, Kottayam, Kerala, Medical College, Kottayam, Kerala, India. India.
-
Upload
maurice-casey -
Category
Documents
-
view
218 -
download
4
Transcript of DISASTER IN SOUTH ASIA (SAARC REGION) Roy Abraham Kallivayalil MD, DPM Gen. Secretary, Indian...
DISASTER IN SOUTH ASIA DISASTER IN SOUTH ASIA (SAARC REGION)(SAARC REGION)
Roy Abraham Kallivayalil MD, DPMRoy Abraham Kallivayalil MD, DPMGen. Secretary, Indian Psychiatric Society & Gen. Secretary, Indian Psychiatric Society &
Secretary General, SAARC Psych. FederationSecretary General, SAARC Psych. FederationAssociate Professor of PsychiatryAssociate Professor of Psychiatry
Medical College, Kottayam, Kerala, India.Medical College, Kottayam, Kerala, India.
““The mental health consequences of The mental health consequences of disasters have been the subject of a disasters have been the subject of a rapidly growing research literature in rapidly growing research literature in the last few decades. Moreover they the last few decades. Moreover they have aroused an increasing public have aroused an increasing public
interest, due to the dramatic impact and interest, due to the dramatic impact and wide media coverage of many recent wide media coverage of many recent
disastrous events”disastrous events”- - Disaster & Mental Health (WPA 2005Disaster & Mental Health (WPA 2005))

SAARC REGIONSAARC REGION
7 Countries7 Countries
IndiaIndia
PakistanPakistan
BangladeshBangladesh
Sri LankaSri Lanka
NepalNepal
Bhutan Bhutan
MaldivesMaldives
TSUNAMI DISASTER IN SAARC TSUNAMI DISASTER IN SAARC REGIONREGION
Brought havoc in the regionBrought havoc in the region
Thousands diedThousands died
Several thousands injuredSeveral thousands injured
Thousands of homes washed awayThousands of homes washed away
APPROXIMATE LIVES LOST IN APPROXIMATE LIVES LOST IN SAARC REGIONSAARC REGION
Sri Lanka – 30,000Sri Lanka – 30,000
India – 20,000India – 20,000
Maldives – 1,000Maldives – 1,000
Bangladesh - 3Bangladesh - 3
PROBLEM FACING THE REGIONPROBLEM FACING THE REGION
Huge number of bereaved families, who Huge number of bereaved families, who lost father, mother, son, daughter, sibling lost father, mother, son, daughter, sibling or the entire family.or the entire family.
All belonging lost for some All belonging lost for some
No place to live No place to live
No worthwhile occupation No worthwhile occupation
Limited means of livelihoodLimited means of livelihood
SOCIAL CONSEQUENCES – SOCIAL CONSEQUENCES – SAARC REGIONSAARC REGION
Poor social supportPoor social support
Families have broken up Families have broken up
The social fabric is lostThe social fabric is lost
Schools, markets, fishing, agriculture, Schools, markets, fishing, agriculture,
places of worship destroyed.places of worship destroyed.
Emotional Consequences seen Emotional Consequences seen commonly in the regioncommonly in the region
Acute grief regionAcute grief region
Acute psychotic episodesAcute psychotic episodes
Hysterical conversion Hysterical conversion
Depressive disordersDepressive disorders
Recurrence of psychosis Recurrence of psychosis
Suicidal ideation and DSHSuicidal ideation and DSH
PTSDPTSD
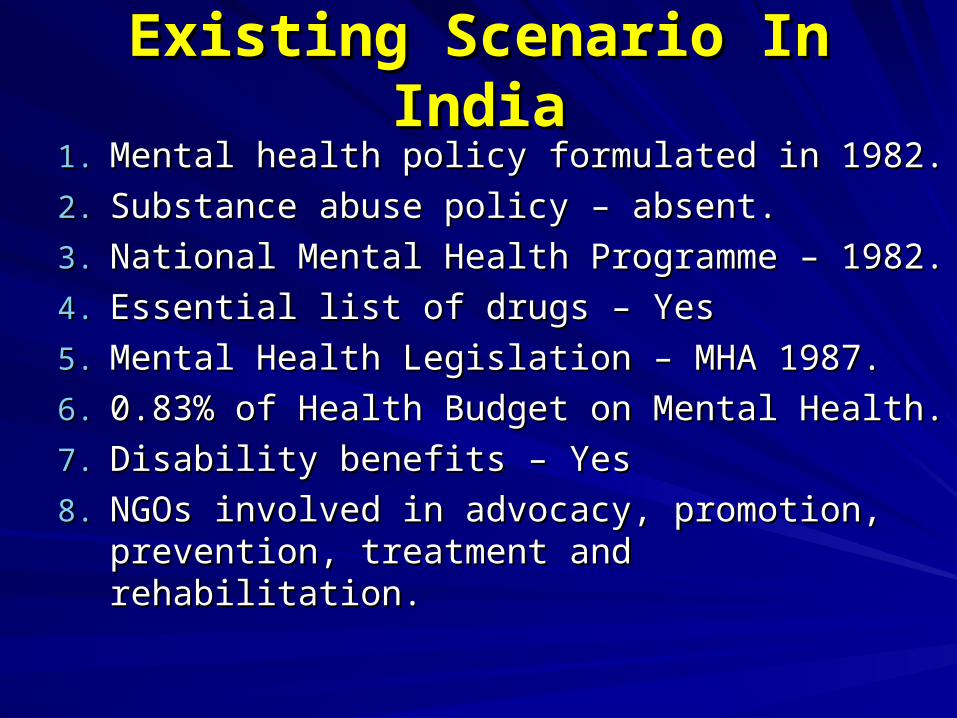
Existing Scenario In IndiaExisting Scenario In India1.1. Mental health policy formulated in 1982.Mental health policy formulated in 1982.
2.2. Substance abuse policy – absent.Substance abuse policy – absent.
3.3. National Mental Health Programme – 1982.National Mental Health Programme – 1982.
4.4. Essential list of drugs – Yes Essential list of drugs – Yes
5.5. Mental Health Legislation – MHA 1987.Mental Health Legislation – MHA 1987.
6.6. 0.83% of Health Budget on Mental Health.0.83% of Health Budget on Mental Health.
7.7. Disability benefits – YesDisability benefits – Yes
8.8. NGOs involved in advocacy, promotion, NGOs involved in advocacy, promotion, prevention, treatment and rehabilitation.prevention, treatment and rehabilitation.
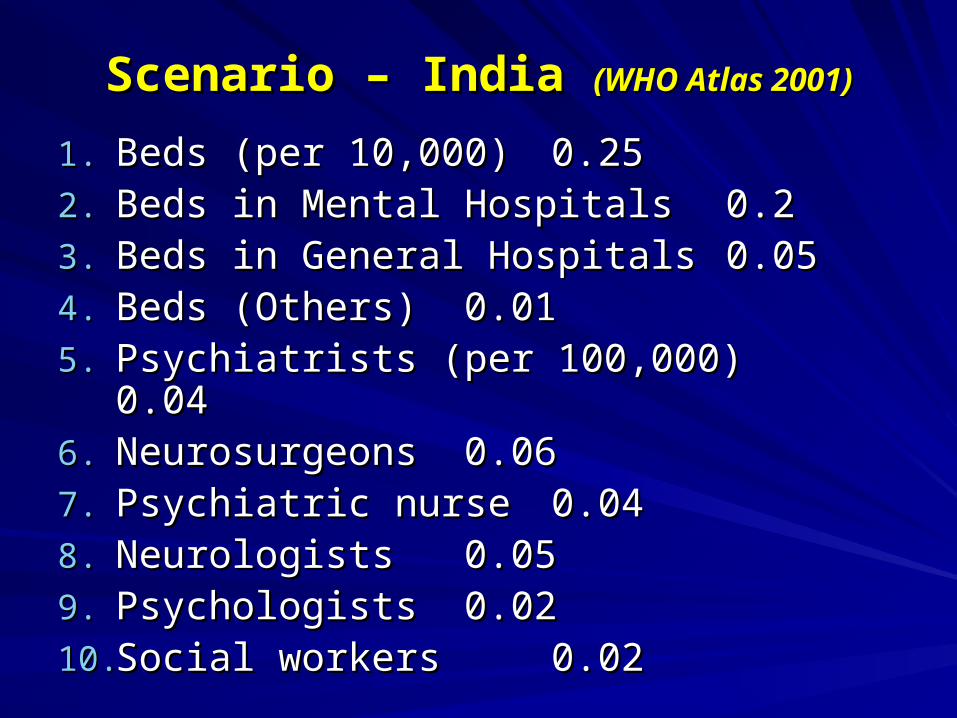
Scenario – India Scenario – India (WHO Atlas 2001)(WHO Atlas 2001)
1.1. Beds (per 10,000)Beds (per 10,000) 0.250.252.2. Beds in Mental HospitalsBeds in Mental Hospitals 0.20.23.3. Beds in General HospitalsBeds in General Hospitals 0.050.054.4. Beds (Others)Beds (Others) 0.010.015.5. Psychiatrists (per 100,000)Psychiatrists (per 100,000)
0.040.046.6. Neurosurgeons Neurosurgeons 0.060.067.7. Psychiatric nursePsychiatric nurse 0.040.048.8. NeurologistsNeurologists 0.050.059.9. PsychologistsPsychologists 0.020.0210.10.Social workers Social workers 0.020.02
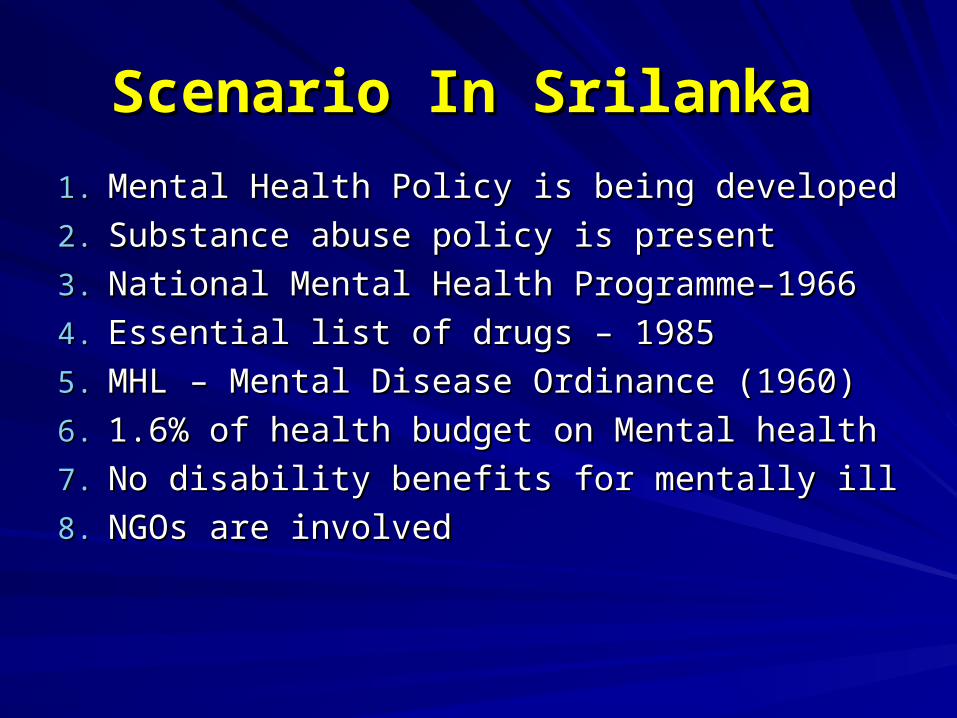
Scenario In Srilanka Scenario In Srilanka
1.1. Mental Health Policy is being developedMental Health Policy is being developed
2.2. Substance abuse policy is presentSubstance abuse policy is present
3.3. National Mental Health Programme–1966National Mental Health Programme–1966
4.4. Essential list of drugs – 1985Essential list of drugs – 1985
5.5. MHL – Mental Disease Ordinance (1960)MHL – Mental Disease Ordinance (1960)
6.6. 1.6% of health budget on Mental health1.6% of health budget on Mental health
7.7. No disability benefits for mentally illNo disability benefits for mentally ill
8.8. NGOs are involved NGOs are involved
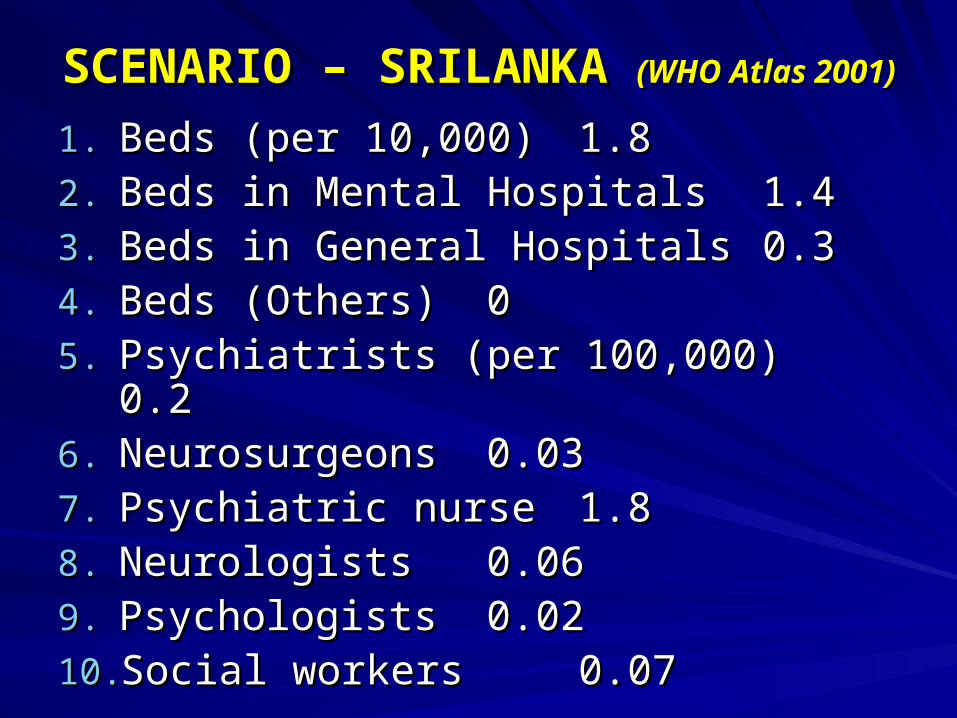
SCENARIO – SRILANKA SCENARIO – SRILANKA (WHO Atlas (WHO Atlas 2001)2001)
1.1. Beds (per 10,000)Beds (per 10,000) 1.81.82.2. Beds in Mental HospitalsBeds in Mental Hospitals 1.41.43.3. Beds in General HospitalsBeds in General Hospitals 0.30.34.4. Beds (Others)Beds (Others) 005.5. Psychiatrists (per 100,000)Psychiatrists (per 100,000)
0.20.26.6. Neurosurgeons Neurosurgeons 0.030.037.7. Psychiatric nursePsychiatric nurse 1.81.88.8. NeurologistsNeurologists 0.060.069.9. PsychologistsPsychologists 0.020.0210.10.Social workers Social workers 0.070.07
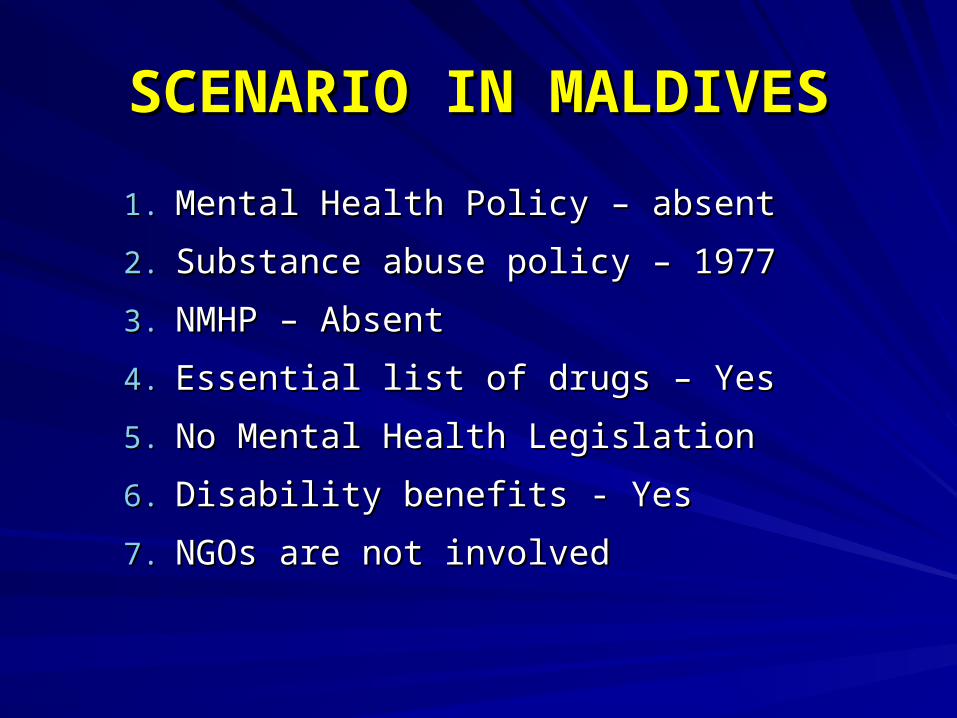
SCENARIO IN MALDIVESSCENARIO IN MALDIVES
1.1. Mental Health Policy – absent Mental Health Policy – absent
2.2. Substance abuse policy – 1977Substance abuse policy – 1977
3.3. NMHP – Absent NMHP – Absent
4.4. Essential list of drugs – YesEssential list of drugs – Yes
5.5. No Mental Health Legislation No Mental Health Legislation
6.6. Disability benefits - YesDisability benefits - Yes
7.7. NGOs are not involvedNGOs are not involved
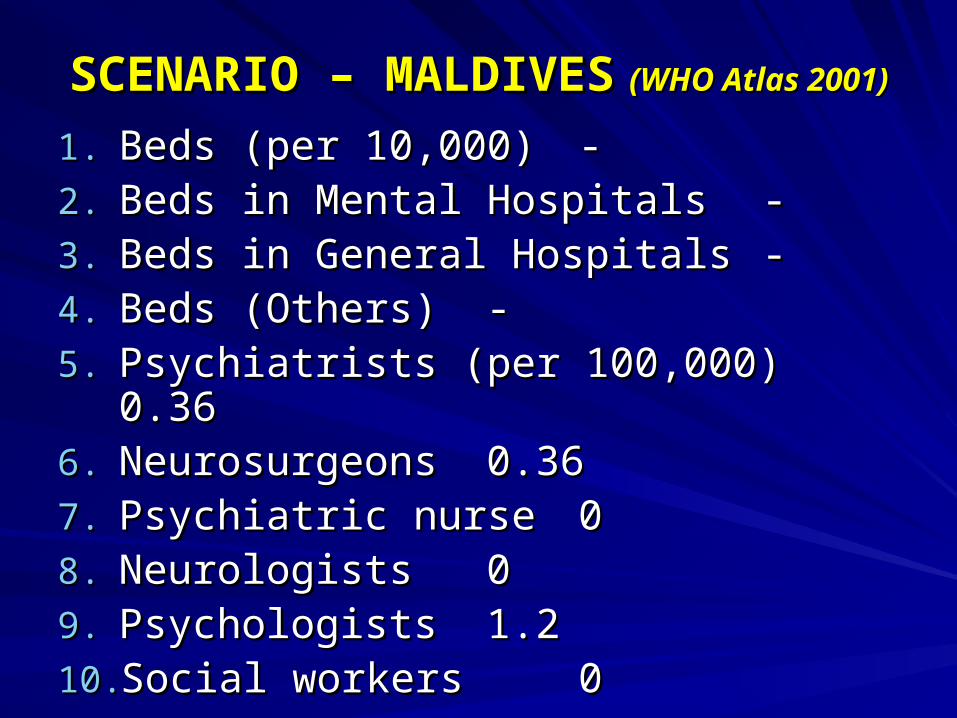
SCENARIO – MALDIVESSCENARIO – MALDIVES (WHO Atlas 2001)(WHO Atlas 2001)
1.1. Beds (per 10,000)Beds (per 10,000) --2.2. Beds in Mental HospitalsBeds in Mental Hospitals --3.3. Beds in General HospitalsBeds in General Hospitals --4.4. Beds (Others)Beds (Others) --5.5. Psychiatrists (per 100,000)Psychiatrists (per 100,000)
0.360.366.6. Neurosurgeons Neurosurgeons 0.360.367.7. Psychiatric nursePsychiatric nurse 008.8. NeurologistsNeurologists 009.9. PsychologistsPsychologists 1.21.210.10.Social workers Social workers 00
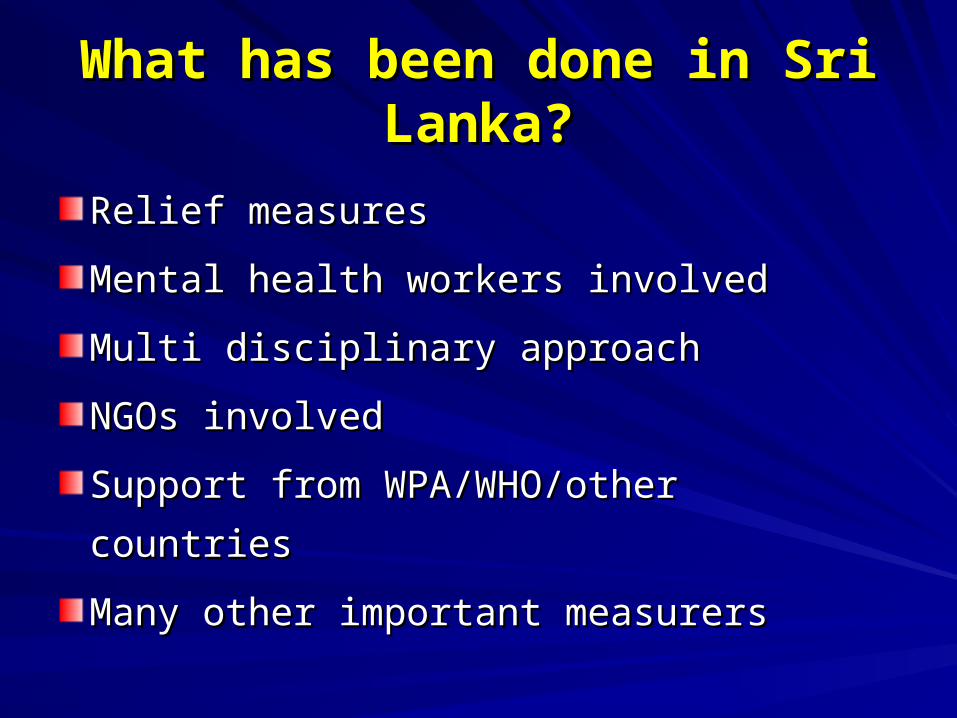
What has been done in Sri What has been done in Sri Lanka?Lanka?
Relief measuresRelief measures
Mental health workers involvedMental health workers involved
Multi disciplinary approachMulti disciplinary approach
NGOs involvedNGOs involved
Support from WPA/WHO/other countriesSupport from WPA/WHO/other countries
Many other important measurersMany other important measurers
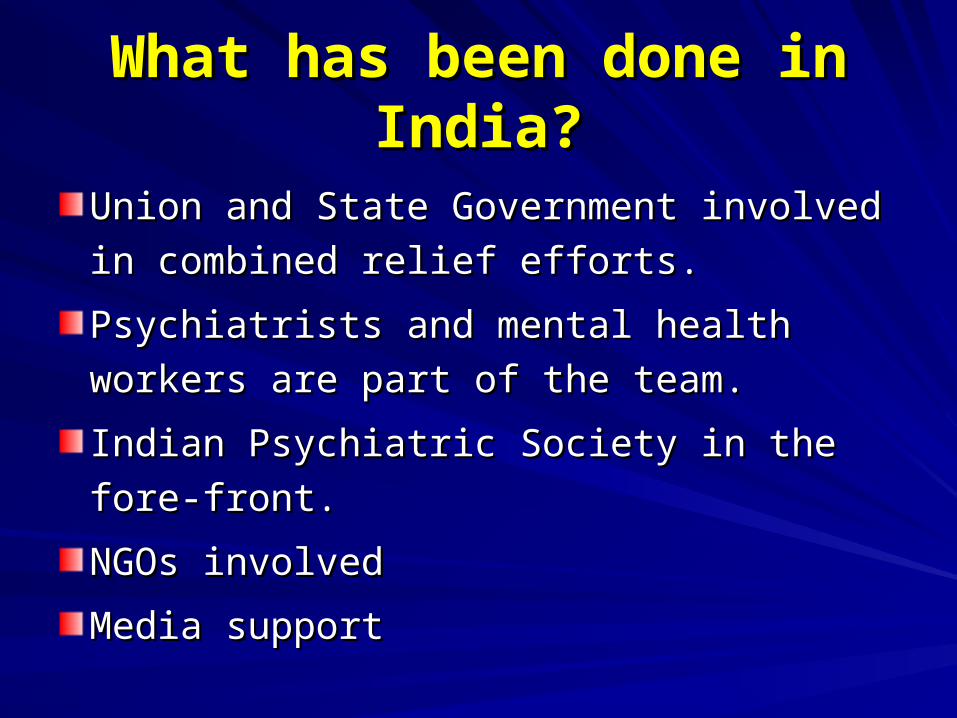
What has been done in India?What has been done in India?
Union and State Government involved in Union and State Government involved in
combined relief efforts.combined relief efforts.
Psychiatrists and mental health workers Psychiatrists and mental health workers
are part of the team.are part of the team.
Indian Psychiatric Society in the fore-front. Indian Psychiatric Society in the fore-front.
NGOs involvedNGOs involved
Media supportMedia support


Role of Indian Psychiatric SocietyRole of Indian Psychiatric Society
Formed a special task force for Tsunami Formed a special task force for Tsunami Disaster relief on 29-12-2004. Disaster relief on 29-12-2004.
Chairman – Dr. S. NambiChairman – Dr. S. Nambi
Co-Chairmen – from all the five zonesCo-Chairmen – from all the five zones
Convenor – Dr. P. Joseph VargheseConvenor – Dr. P. Joseph Varghese
Co-convenor – Dr. Varghese P. PunnooseCo-convenor – Dr. Varghese P. Punnoose
Members – Presidents and Secretaries of Members – Presidents and Secretaries of affected states.affected states.
The IPS Task ForceThe IPS Task Force
Mobilized country wide effortsMobilized country wide efforts
Co-ordinated the relief measurers Co-ordinated the relief measurers
Encouraged participation by allEncouraged participation by all
All the zones and the states participatedAll the zones and the states participated
Co-ordinated by IPS President and Gen. Co-ordinated by IPS President and Gen.
Secretary.Secretary.
IPS – Technical Advisory IPS – Technical Advisory CommitteeCommittee
Members who had valuable experience in Members who had valuable experience in
disastersdisasters
– Dr. Mohan K. Issac (NIMHANS)Dr. Mohan K. Issac (NIMHANS)
– Dr. N.G. Desai (IHBAS, Delhi)Dr. N.G. Desai (IHBAS, Delhi)
– Dr. K. Shekhar (NIMHANS, Bangalore) Dr. K. Shekhar (NIMHANS, Bangalore)
– Dr. R.H. Bakre (Gandhi Nagar, Gujrat)Dr. R.H. Bakre (Gandhi Nagar, Gujrat)
– Dr. Mohan Agashe (Pune)Dr. Mohan Agashe (Pune)
Contributions to PM’s FundContributions to PM’s Fund
IPS Members –mobilized IPS Members –mobilized
contributions to the Prime Minister’s contributions to the Prime Minister’s
National Relief Fund (PMNRF).National Relief Fund (PMNRF).
Kept in touch with PMO.Kept in touch with PMO.
Role of SAARC Psychiatric Role of SAARC Psychiatric FederationFederation
Mobilized support for relief measurers in Mobilized support for relief measurers in
the region.the region.
Provided technical expertise Provided technical expertise
Encouraged members to work in other Encouraged members to work in other
countries.countries.
Enlisted regional cooperation and Enlisted regional cooperation and
participation.participation.
The South-Asia Region The South-Asia Region - Looking Ahead - Looking Ahead
Dearth of trained psychiatrist and mental Dearth of trained psychiatrist and mental
health professionals.health professionals.
Time consuming rehabilitation measurersTime consuming rehabilitation measurers
The notorious “red-tape”The notorious “red-tape”
Media interest is waning Media interest is waning
Paucity of resources.Paucity of resources.
Plan for the FuturePlan for the Future
Involvement of all stake holdersInvolvement of all stake holders
Mobilizing National and International Mobilizing National and International expertiseexpertise
Equitable distribution of resources within Equitable distribution of resources within each country.each country.
Rehabilitation holds the keyRehabilitation holds the key
Mental health needs higher priority Mental health needs higher priority
““A Disaster is an empirical A Disaster is an empirical falsification of human action, the falsification of human action, the
proof of the incorrectness of proof of the incorrectness of human beings’ conceptions on human beings’ conceptions on
nature and culture”nature and culture”
- - Juan J. Lopez - IborJuan J. Lopez - Ibor