Beneplan - Benefits Law & Admin Workshop - December 1 2015 - Mississauga, Ontario, Canada

GROUP INSURANCE
DISABILITY CLAIM FORMInitial assessment
4300-058 condense_2013.indd 1 2013-04-09 16:56:33

Group insurance Disability claim form – Initial assessment
Instructions for: A.Theclaimant 1. Pleasecompleteandsignthe“Claimantstatement”section.
2. Pleaseensurethatthepolicyholdercompletesandsignsthe“Policyholderstatement”section.
3. Pleaseensure thatyourphysiciancompletesandsigns the“Attendingphysicianstatement–Psychologicalconditions” if theprimaryreasonforyourabsencefromworkispsychologicalorthe“Attendingphysicianstatement–Physicalconditions”forallothercondition.Aswell,pleaseprovideyourphysicianwithacopyofyourcompleted“Claimantstatement”sothatthephysicianwillhaveyoursignedauthorizationtoreleaseinformationtoHumaniaAssurance.
4. Pleasenotethatanycostsincurredforthecompletionofthe“Attendingphysicianstatement”areyourresponsibility.
5. Pleaseensurethatalloftheabove-mentionedformsaresubmittedtoHumaniaAssuranceonatimelybasis.Submittingthemtogether will avoid unnecessary delays in the assessment of your claim.Also, please enclose a copy of the first and/or lastunemploymentchequestubandtherecordofemploymentformifapplicable.
Directdeposit 6. PleasecompleteandsignthedirectdepositauthorizationatthebottomofthispageifyouarenotalreadyusingdirectdepositwithHumaniaAssurance.Theformshouldthenbesubmittedwithyourclaiminordertohaveyourbenefitsdepositeddirectlyintoyourbankaccount,shouldyourclaimbeapproved.
B.Thepolicyholder 1. Pleasecompleteandsignthe“Policyholderstatement”section.
2. InordertoavoidunnecessarydelaysintheprocessingofLong-TermDisabilityclaims(withoutShort-TermDisability),weaskthattheseformsbecompletedandsenttoHumaniaAssuranceasfollows:
Forpolicieswithaneliminationperiodof:
- 15weeks,completedformsshouldbesenttousasofthe8thweekofabsence;- 17weeks,completedformsshouldbesenttousasofthe11thweekofabsence;- 26weeks,completedformsshouldbesenttousasofthe20thweekofabsence.
C.Thephysician 1. Pleasecompleteandsigntheappropriate“Attendingphysicianstatement”,dependingonthenatureoftheprimarydiagnosis.
1
In order to ensure confidentiality of personal information, Humania Assurance will establish a claim file in which information concerning all of your claims will be kept. Only employees or authorized agents of Humania Assurance responsible for the management of your claim shall have access to the file.
Direct deposit – Authorization
qInitialrequestfordirectdeposit qRequestforbankaccountchange qRequesttoenddirectdeposit
I Insured statement (please print)
Policyandsub-groupno. Certificateno. Insuredsurname Givenname(s)
Telephoneno.(day) Mainresidenceaddress(no.,street) Apt.
City Province Postalcode
Financialinstitutionname Financialinstitutionaddress
II Type of bank account (please print)
qChequing qSavings Pleasecompletethissectionorattachapersonalizedvoidchequetoensurethatweobtainyouraccuratebankinginformation.
Branchno.(5digitnumber) Institutionno.(3–4digitnumber) Accountno.(Allnumbers)
III Authorization
IauthorizeHumaniaAssurancetocreditallmybenefitpaymentstotheaccountmentionedonthisform.Icertifythattheinformationprovidedonthisformisaccurate,andIagreetoinformHumaniaAssuranceofanysubsequentchanges.IacceptthatthisagreementmaybecancelledatanytimebyeitherHumaniaAssurance,myself,inwritingorverbally.
Insuredsignature Date ( Y Y Y Y / M M / D D )
Accountholdersignature(ifotherthanInsured) Date ( Y Y Y Y / M M / D D )
4300-058 condense_2013.indd 2 2013-04-09 16:56:33
Group insurance Disability claim form – Initial assessment
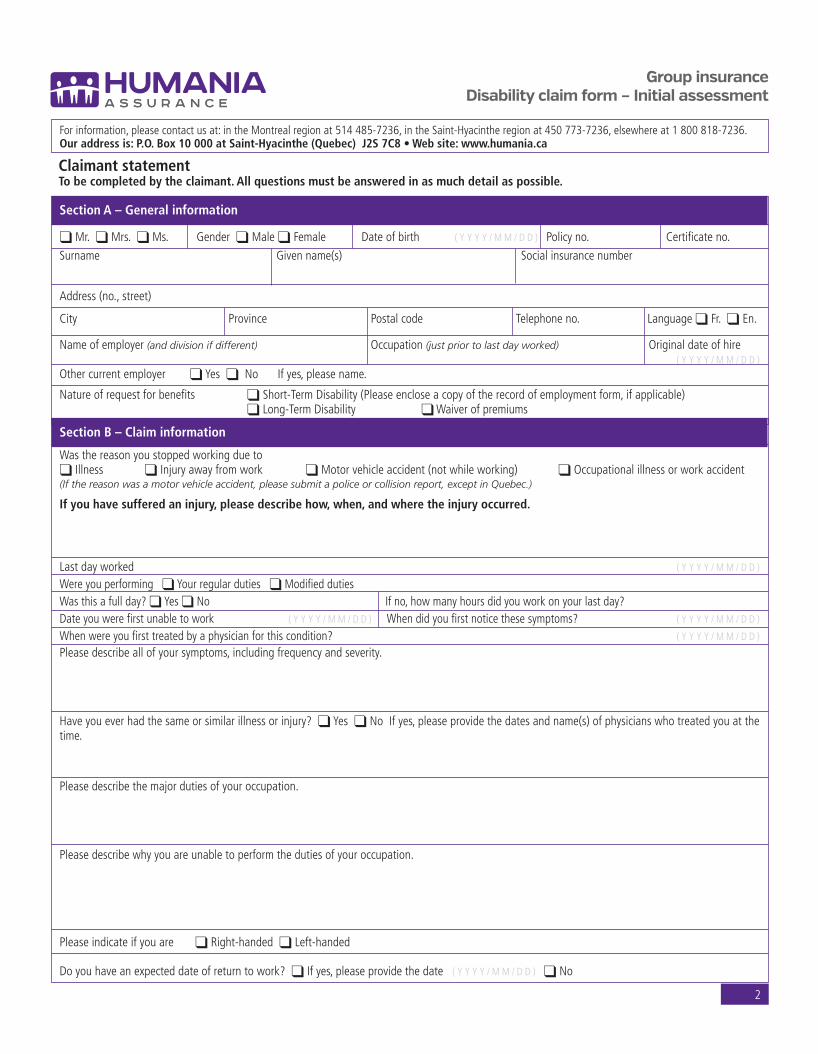
2
Forinformation,pleasecontactusat:intheMontrealregionat514485-7236,intheSaint-Hyacintheregionat450773-7236,elsewhereat1800818-7236.Our address is: P.O. Box 10 000 at Saint-Hyacinthe (Quebec) J2S 7C8 • Web site: www.humania.ca
Section A – General information
qMr.qMrs.qMs. Genderq Maleq Female Dateofbirth ( Y Y Y Y / M M / D D ) Policyno. Certificateno.
Surname Givenname(s) Socialinsurancenumber
Address(no.,street)
City Province Postalcode Telephoneno. Languageq Fr.q En.
Nameofemployer(and division if different) Occupation(just prior to last day worked) Originaldateofhire ( Y Y Y Y / M M / D D )Othercurrentemployer qYesqNo Ifyes,pleasename.
Natureofrequestforbenefits q Short-TermDisability(Pleaseencloseacopyoftherecordofemploymentform,ifapplicable) qLong-TermDisability qWaiverofpremiums
Section B – Claim information
WasthereasonyoustoppedworkingduetoqIllness qInjuryawayfromwork qMotorvehicleaccident(notwhileworking) qOccupationalillnessorworkaccident(If the reason was a motor vehicle accident, please submit a police or collision report, except in Quebec.)
If you have suffered an injury, please describe how, when, and where the injury occurred.
Lastdayworked ( Y Y Y Y / M M / D D )
WereyouperformingqYourregulardutiesqModifieddutiesWasthisafullday?qYesqNo Ifno,howmanyhoursdidyouworkonyourlastday?Dateyouwerefirstunabletowork ( Y Y Y Y / M M / D D ) Whendidyoufirstnoticethesesymptoms? ( Y Y Y Y / M M / D D )
Whenwereyoufirsttreatedbyaphysicianforthiscondition? ( Y Y Y Y / M M / D D )
Pleasedescribeallofyoursymptoms,includingfrequencyandseverity.
Haveyoueverhadthesameorsimilarillnessorinjury?qYesqNoIfyes,pleaseprovidethedatesandname(s)ofphysicianswhotreatedyouatthetime.
Pleasedescribethemajordutiesofyouroccupation.
Pleasedescribewhyyouareunabletoperformthedutiesofyouroccupation.
Pleaseindicateifyouare qRight-handedqLeft-handed
Doyouhaveanexpecteddateofreturntowork?qIfyes,pleaseprovidethedate( Y Y Y Y / M M / D D ) qNo
Claimant statementTo be completed by the claimant. All questions must be answered in as much detail as possible.
4300-058 condense_2013.indd 3 2013-04-09 16:56:33

Group insurance Disability claim form – Initial assessment
3
Claimant statement (continued)
Section C – Health care professionals information
Pleaselistallofthehealthcareprofessionalsyouhaveconsultedin the last 12 months,startingwiththemostrecent,includingfamilyphysicians,specialists,chiropractors,psychologists,etc.Ifthespaceprovidedbelowisinsufficient,pleaseattachaseparatepageandlisttheadditionalhealthcareprofessionals.
Name Consultedfrom( Y Y Y Y / M M / D D ) to ( Y Y Y Y / M M / D D )
Address(no.,street)
Telephoneno. Faxno. Specialty
Name Consultedfrom( Y Y Y Y / M M / D D ) to ( Y Y Y Y / M M / D D )
Address(no.,street)
Telephoneno. Faxno. Specialty
Name Consultedfrom( Y Y Y Y / M M / D D ) to ( Y Y Y Y / M M / D D )
Address(no.,street)
Telephoneno. Faxno. Specialty
Section D – Other income information
Ifyouhaveappliedfor,orarereceivinganyincomefromanyofthefollowingsources,pleasecompletetheappropriatesectionbelowandsubmitacopyofyournoticeofacceptanceorrefusal,ifapplicable.
Source
Claim no., contact name, telephone no. Have you Are you receiving
Monthly applied? payment? Amount Yes No Yes No Pending
Worker’sComp–CSST,WSIB,WCB q q q q q
Crimevictimscompensation(IVAC) q q q q q
CanadaPensionPlan–Disability q q q q q
CanadaPensionPlan– q q q q q Retirement
QuebecPensionPlan(QPP)– q q q q q Disability
QuebecPensionPlan(QPP)– q q q q q RetirementEmploymentInsurance q q q q q
Provincialautoinsurance–SAAQ q q q q q
Otherinsurer q q q q q
Section E – Claimant authorization and declaration
Iauthorizeanyhealthcareprofessional,hospital,clinic,pharmacist,provincialhealthinsuranceplan,rehabilitationagency,insurer,employeroranyotherpersonororganizationinpossessionofinformationconcerningmyselftoreleasetoHumaniaAssurance,allmedical,financialorotherinformationdeemedrelevantintheassessmentofmyclaim.IauthorizeHumaniaAssuranceInc.,toconductallnecessaryinvestigationsrequiredinordertoverifythevalidityofmyclaim.IacceptthatHumaniaAssurance,willusetheinformationprovidedinthisformandanypriorclaimsunderthesameplanforthemanagementofmyclaimandforproductionofstatisticalreports.Icertifythattheinformationcontainedinthisformistrueandcomplete.This authorization is valid for the complete duration of the present claim. A photocopy of this authorization is as valid as the original.
Name(pleaseprint) Signature
Policyno. Date(YYYY/MM/DD)
4300-058 condense_2013.indd 4 2013-04-09 16:56:34

Group insurance Disability claim form – Initial assessment
4
Policyholder statementTo be completed by the policyholder. All questions must be answered in as much detail as possible.
Forinformation,pleasecontactusat:intheMontrealregionat514485-7236,intheSaint-Hyacintheregionat450773-7236,elsewhereat1800818-7236.Our address is: P.O. Box 10 000 at Saint-Hyacinthe (Quebec) J2S 7C8 • Web site: www.humania.ca
Section A – Policyholder information
Nameofpolicyholder(Employer/Union/Association) Nameofsubsidiaryordivision(ifdifferent)
Address(no.,street)
City Province Postalcode Telephoneno.
Section B – Claimant information
Surname Givenname(s)
Policyno. Divisionno. Classno. Socialinsurancenumber Certificateno. Permanentemployee?q YesqNo
Natureofrequestforbenefits q Short-TermDisability(pleaseencloseacopyoftherecordofemploymentform,ifapplicable) qLong-TermDisability qWaiverofpremiums
Pleaseprovidethedateonwhichthisclaimantwasfirstcoveredunderthispolicy. ( Y Y Y Y / M M / D D )
Wastheemployeeactivelyatworkwhentheabsencebegan/lossoccured?q YesqNoIfno,pleasecomment.
Whatwastheclaimant’sdateofhire?( Y Y Y Y / M M / D D ) Lastdateofwork?( Y Y Y Y / M M / D D ) Forseenreturntoworkdate?( Y Y Y Y / M M / D D )
Ifalreadybackatwork,whatwasthestartdate?( Y Y Y Y / M M / D D )qPart-timeqFull-timeqTemporaryassignmentqLightdutiesqGradual–Pleaseprovidethereturntoworkprotocol
Whatwastheclaimant’smainreasonfortheabsence?q IllnessqInjuryawayfromworkq Motorvehicleaccident(notwhileworking)qOccupationnalillnessorworkrelatedaccident
Pleaseindicatethehoursofworkinanormalworkweek.
Mon__________Tues___________Wed___________Thur___________Fri___________Sat___________Sun__________(If shift work, please provide work schedule.)
Whatwastheclaimant’sgrossweeklysalaryasofhis/herlastdayofwork?$____________________
Wastheclaimant q Salaried qHourly qOncall
Didtheclaimantreceiveanyincomeduringthedisabilityperiod?q Yes qNoIfyes,pleaseselectoneofthefollowing: q Vacation qMaternityleave q Sickdaysq Employmentinsurance(pleaseencloseacopyoftherecordofemploymentform) qStatutoryholidays q Other_________________
Amount$_______________________ From______________________________to______________________________
Hastheclaimantsubmittedaclaimtothefollowinggovernmentbodies?q WSIB/WCB/CSST qEmploymentinsurance(Pleaseencloseacopyoftherecordofemploymentform) q CPP qQPP(RRQ)q SAAQ–Provincialautomobileinsuranceboard q CrimeVictimCompensationAct
( Y Y Y Y / M M / D D ) ( Y Y Y Y / M M / D D )
4300-058 condense_2013.indd 5 2013-04-09 16:56:34

Group insurance Disability claim form – Initial assessment
5
Section C – Occupational information
Whatwastheclaimant’sregularoccupationimmediatelypriortohis/herstoppingwork?
Weretheclaimant’sdutiesmodifiedfromhis/herregularoccupation?q YesqNo
Pleasedescribethisemployee’sregularoccupation(orattachacopyofthejobdescription)aswellasanymodifications.
Thefollowingphysicaldemandsanalysisoftheclaimant’soccupationistobecompletedbyhis/hersupervisor.Intheappropriatecolumn,pleasespecifytheaverageamountoftime(inhours)thefollowingactivitiesareregularlyperformed:
I) atanyonetimewithoutabreak(approximately)and;II) intotalthroughouttheday(approximately)
Physical demands analysis
I II
1. Sitting
2. Standing
3. Driving
4. Bending
5. Climbingupanddownthestairs
6. Lifting 0–10poundsq 10–20poundsq 20–50poundsq 50pounds+q withliftingdevice? Yesq Noq
7. Pushing/Pulling 0–10poundsq 10–20poundsq 20–50poundsq 50pounds+q
Pleasedescribeworkenvironment(i.e.:temperature,noiselevels,chemical/dustexposure,etc.).
Doestheclaimantwearpersonalprotectiveequipment(i.e.:safetyglasses/footwear,respiratoryprotection,earprotection,etc.)?Ifyes,pleasedescribe.
Isthereanycircumstancesorfactsthatwouldcauseyoutoquestionthevalidityoftheclaim?q YesqNoIfyes,pleaseexplain.
Icertifythattheinformationgivenaboveistrueandcomplete. Date ( Y Y Y Y / M M / D D )
Name(pleaseprint) Telephoneno.
Signatureoftheauthorizedperson Jobtitle
Policyholder statement (continued)
4300-058 condense_2013.indd 6 2013-04-09 16:56:34

Group insurance Disability claim form – Initial assessment
Section A – Information about the patient
Surname Givenname(s)
Dateofbirth ( Y Y Y Y / M M / D D ) Height Weight
Attending physician statement – physical conditionsIn order for Humania Assurance to properly assess your patient’s claim for Disability Benefits, it is important that you answer the following questions in as much detail as possible. Please note that any costs incurred in the completion of this form are the responsibility of the patient.
Forinformation,pleasecontactusat:intheMontrealregionat514489-8404,intheSaint-Hyacintheregionat450-773-7170,elsewhereat1800773-8404.Our address is: P.O. Box 10 000 at Saint-Hyacinthe (Quebec) J2S 7C8 • Web site: www.humania.ca
Section B – Diagnosis
Whatistheprimarydiagnosis?
Whendidthesymptomsfirstappearordateaccidentoccured? ( Y Y Y Y / M M / D D )
Whatwasthedateofthepatient’sfirstvisitforhis/hercurrentcondition? ( Y Y Y Y / M M / D D )
Whatwasthedateofthepatient’sfirstvisitasregardstothepresentdisabilityperiod? (YYYY/MM/DD)
Accordingtotheanamnesisandyourclinicalexam,isyourpatient’sconditiontheresultofanaccidentaleventq YesqNoPleaseelaborate:
Ifyourpatienthasanorthopaedicand/ormusculo-skeletalcondition,hasanX-ray,MRI,oranyothertestsbeenperformed?q YesqNoIfyes,pleaseattachacopyoftheresultsoftheX-ray,MRI,oranyothertestswhichmayhavebeenperformed.
Isthereasecondarydiagnosisoradditionalcomplicationwhichmightaffectthedurationofthedisability?q YesqNoIfyes,pleaseelaborate.
Pleaseprovideacompletelistofthepatient’ssymptoms(includingseverityandfrequency),identifyingwhichofthesymptomslistedyouhaveobjectivelyobserved.
Whatarethepatient’scurrentlimitations(thingsthathe/shecannot do)?Pleasebespecific.
Whatarethepatient’scurrentrestrictions(thingsthathe/sheshould notdo)?Pleasebespecific.
Pleaseindicatethedatethepatientstoppedworkingorperforminghis/herdailyactivitiesbasedonyourrecommendation. ( Y Y Y Y / M M / D D )
Ifapotentialreturntoworkdateorreturntodailyactivitieshasbeendiscussed,pleaseprovidethedateandindicateifthereturnis ( Y Y Y Y / M M / D D )qPart-timeqFull-timeqTemporaryassignmentqLightdutiesqGradual–Pleaseprovidethereturntoworkprotocol
Hasthepatienteverhadthesameorsimilarcondition?q YesqNoIfyes,pleaseprovidedatesandcompletedescription.
Isthepatient’sconditionduetoinjuryorsicknessarisingoutofhis/heremployment?q YesqNoIfyes,pleaseelaborate.
6
4300-058 condense_2013.indd 7 2013-04-09 16:56:34
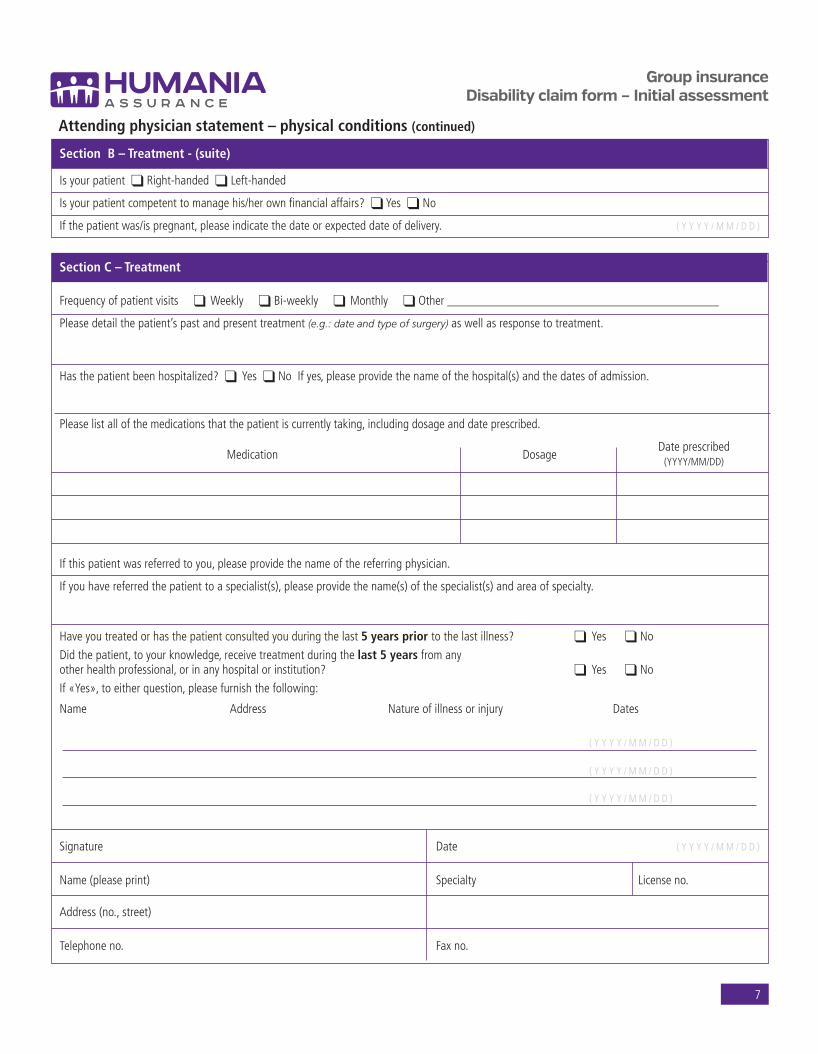
Group insurance Disability claim form – Initial assessment
7
Section B – Treatment - (suite)
IsyourpatientqRight-handedqLeft-handed
Isyourpatientcompetenttomanagehis/herownfinancialaffairs?qYesqNo
Ifthepatientwas/ispregnant,pleaseindicatethedateorexpecteddateofdelivery. ( Y Y Y Y / M M / D D )
Section C – Treatment
Frequencyofpatientvisitsq WeeklyqBi-weeklyq MonthlyqOther___________________________________________
Pleasedetailthepatient’spastandpresenttreatment(e.g.: date and type of surgery)aswellasresponsetotreatment.
Hasthepatientbeenhospitalized?q YesqNoIfyes,pleaseprovidethenameofthehospital(s)andthedatesofadmission.
Pleaselistallofthemedicationsthatthepatientiscurrentlytaking,includingdosageanddateprescribed.
Medication
Dosage
Dateprescribed (YYYY/MM/DD)
Ifthispatientwasreferredtoyou,pleaseprovidethenameofthereferringphysician.
Ifyouhavereferredthepatienttoaspecialist(s),pleaseprovidethename(s)ofthespecialist(s)andareaofspecialty.
Haveyoutreatedorhasthepatientconsultedyouduringthelast5 years prior tothelastillness? q Yes qNo
Didthepatient,toyourknowledge,receivetreatmentduringthelast 5 yearsfromanyotherhealthprofessional,orinanyhospitalorinstitution? q Yes qNo
If«Yes»,toeitherquestion,pleasefurnishthefollowing:
Name Address Natureofillnessorinjury Dates
Signature Date ( Y Y Y Y / M M / D D )
Name(pleaseprint) Specialty Licenseno.
Address(no.,street)
Telephoneno. Faxno.
Attending physician statement – physical conditions (continued)
( Y Y Y Y / M M / D D )
( Y Y Y Y / M M / D D )
( Y Y Y Y / M M / D D )
4300-058 condense_2013.indd 8 2013-04-09 16:56:34

Group insurance Disability claim form – Initial assessment
8
Section A – Information about the patient
Surname Givenname(s)
Dateofbirth ( Y Y Y Y / M M / D D ) Height Weight
Section B – Diagnosis
PleaseindicatethediagnosisusingDSM–IVMultiaxialevaluationnomenclatureandcodenumbers.
I
II
III
IV
V
Isthereasecondarydiagnosisoradditionalcomplicationwhichmightaffectthedurationofthedisability?q YesqNoIfyes,pleaseelaborate.
Whendidsymptomsfirstappear? ( Y Y Y Y / M M / D D )
Pleaseprovideacompletelistofyourpatient’ssymptoms(includingseverityandfrequency),identifyingwhichofthesymptomslistedyouhaveobjectivelyobserved.
Whatwasthedateofthepatient’sfirstvisitforhis/hercurrentcondition? ( Y Y Y Y / M M / D D )
Whatwasthedateofthepatient’sfirstvisitduringthepresentdisabilityperiod? ( Y Y Y Y / M M / D D )
Pleasedescribethepatient’sinitialreasonforseekingtreatment.Wasthereaprecipitatingevent?
Isyourpatient’sconditioncauseddirectlyorindirectlybyhis/heremployment?q YesqNoIfyes,pleaseelaborate.
Whatarethepatient’scurrentlimitations(thingsthathe/shecannotdo)?Pleasebespecific.
Whatarethepatient’scurrentrestrictions(thingsthathe/sheshould notdo)?Pleasebespecific.
Isyourpatientcompetenttomanagehis/herownfinancialaffairs?q YesqNo
Pleaseindicatethedatethepatientstoppedworkingorperforminghis/herdailyactivitiesbasedonyourrecommendation. ( Y Y Y Y / M M / D D )
Ifapotentialreturntoworkdateorreturntodailyactivitieshasbeendiscussed,pleaseprovidethedateandindicateifthereturnis ( Y Y Y Y / M M / D D )qPart-timeqFull-timeqTemporaryassignmentqLightdutiesqGradual–Pleaseprovidethereturntoworkprotocol
Attending physician statement – psychological conditionsIn order for Humania Assurance to properly assess your patient’s claim for Disability Benefits, it is important that you answer the following questions in as much detail as possible. Please note that any costs incurred in the completion of this form are the responsibility of the patient.
Forinformation,pleasecontactusat:intheMontrealregionat514489-8404,intheSaint-Hyacintheregionat450-773-7170,elsewhereat1800773-8404.Our address is: P.O. Box 10 000 at Saint-Hyacinthe (Quebec) J2S 7C8 • Web site: www.humania.ca
4300-058 condense_2013.indd 9 2013-04-09 16:56:34

Group insurance Disability claim form – Initial assessment
9
Section C – Treatment
Frequencyofpatientvisitsq WeeklyqBi-weeklyq MonthlyqOther___________________________________________Pleasedetailthepatient’spastandpresenttreatment(includingpsychotherapy),responsetotreatment,andcompliance.
Hasthepatientbeenhospitalized?q YesqNoIfyes,pleaseprovidethenameofthehospital(s)andthedatesofadmission.
Pleaselistallofthemedicationsthatthepatientiscurrentlytaking,includingdosageanddateprescribed.
Medication Dosage Dateprescribed
(YYYY/MM/DD)
Haveyoutreatedorhasthepatientconsultedyouduringthelast 5 years priortothelastillness? q Yes qNo
Didthepatient,toyourknowledge,receivetreatmentduringthelast 5 yearsfromanyotherhealthprofessionalorinanyhospitalorinstitution? q Yes qNo
If«Yes»,toeitherquestion,pleasefurnishthefollowing:
Name Address Natureofillnessorinjury Dates
Attending physician statement – psychological conditions (continued)
( Y Y Y Y / M M / D D )
( Y Y Y Y / M M / D D )
Section D – Functional capacities evaluation
Pleaseprovideyouropinionastotheextentofthepatient’simpairmentinperformingthefollowingonasustainedbasis:None: noimpairmentinthisarea. Moderately severe:impairmentsignificantlyaffectsabilitytofunction.Mild:suspectedimpairmentofslightimportancewhichdoesnotaffectfunctionalability. Severe:extremeimpairmentofabilitytofunction.Moderate:impairmentaffectsbutdoesnotprecludeabilitytofunction.
None Mild Moderate Moderately
Severe
severe1. Abilitytorelatetofriendsandfamilymembers q q q q q
2. Abilitytoattendtopersonalcare(bathing,cooking,etc.) q q q q q
3. Abilitytocarryouthouseholdchores q q q q q
4. Abilitytorelatetoco-workersandsupervisors q q q q q
5. Performworkwherecontactwithotherswillbeminimal q q q q q
6. Understand,carryout,andrememberinstructions q q q q q
7. Performtasksinvolvingminimalintellectualeffortorrepetitivetasks q q q q q
8. Performvariedtasks q q q q q
9. Abilitytofollowaregularworkschedule q q q q q
10. Makeindependentjudgements q q q q q
11. Performintellectuallycomplextasksrequiringhigherlevelsofreasoning,math, andlanguageskills
q q q q q
12. Superviseormanageothers q q q q q
Signature Date ( Y Y Y Y / M M / D D )
Name(pleaseprint) Specialty Licenseno.
Address(no.,street)
Telephoneno. Faxno.
4300-058 condense_2013.indd 10 2013-04-09 16:56:34

Authorization
I authorize any health care professional, hospital, clinic, pharmacist, provincial health insurance plan, rehabilitation agency, insurer, employer or any other person or organization inpossession of information concerning myself to release to Humania Assurance all medical, financial or other information deemed relevant in the assessment of my claim.
I authorize Humania Assurance to conduct all necessary investigations required in order to verify the validity of my claim. I accept that Humania Assurance will use the informationprovided for this claim and any prior claims under the same plan for the management of my claim and for production or statistical reports.
This authorization is valid for the complete duration of the present claim. A photocopy of this authorization is as valid as the original.
4300-013 - Rév. 04/2013
Name (please print) Signature
Policy no. Date (YYYY/MM/DD)Humania Assurance Inc., 1555 Girouard Street West, P.O. Box 10000, Saint-Hyacinthe, Quebec J2S 7C8
Authorization
I authorize any health care professional, hospital, clinic, pharmacist, provincial health insurance plan, rehabilitation agency, insurer, employer or any other person or organization inpossession of information concerning myself to release to Humania Assurance all medical, financial or other information deemed relevant in the assessment of my claim.
I authorize Humania Assurance to conduct all necessary investigations required in order to verify the validity of my claim. I accept that Humania Assurance will use the informationprovided for this claim and any prior claims under the same plan for the management of my claim and for production or statistical reports.
This authorization is valid for the complete duration of the present claim. A photocopy of this authorization is as valid as the original.
4300-013 - Rév. 04/2013
Name (please print) Signature
Policy no. Date (YYYY/MM/DD)Humania Assurance Inc., 1555 Girouard Street West, P.O. Box 10000, Saint-Hyacinthe, Quebec J2S 7C8
Authorization
I authorize any health care professional, hospital, clinic, pharmacist, provincial health insurance plan, rehabilitation agency, insurer, employer or any other person or organization inpossession of information concerning myself to release to Humania Assurance all medical, financial or other information deemed relevant in the assessment of my claim.
I authorize Humania Assurance to conduct all necessary investigations required in order to verify the validity of my claim. I accept that Humania Assurance will use the informationprovided for this claim and any prior claims under the same plan for the management of my claim and for production or statistical reports.
This authorization is valid for the complete duration of the present claim. A photocopy of this authorization is as valid as the original.
4300-013 - Rév. 04/2013
Name (please print) Signature
Policy no. Date (YYYY/MM/DD)Humania Assurance Inc., 1555 Girouard Street West, P.O. Box 10000, Saint-Hyacinthe, Quebec J2S 7C8
4300-013 293c_04-2013_4300-013.qxd 2013-04-09 09:47 Page 4
To avoid any delay in the assessment of your claim, please complete and sign all the authorizations below, even if you completed the one found on page 3 of this document.
4300-058 condense_2013.indd 11 2013-04-09 16:58:00

4300-058 condense_2013.indd 12 2013-04-09 16:56:36

Group insurance Disability claim form – Initial assessment
12
Notes and Comments
4300-058 condense_2013.indd 13 2013-04-09 16:56:36

Group insurance Disability claim form – Initial assessment
13
Notes and Comments
4300-058 condense_2013.indd 14 2013-04-09 16:56:36

Group insurance Disability claim form – Initial assessment
14
Notes and Comments
4300-058 condense_2013.indd 15 2013-04-09 16:56:36

4300-058 Rév. 04/2013
HUMANIA ASSURANCE INC.
1555 Girouard Street West, P.O. Box 10 000, Saint-Hyacinthe (Quebec) J2S 7C8Montreal region: 514 485-7236Saint-Hyacinthe region: 450 773-7236Other region: 1 800 818-7236Web site : www.humania.ca
4300-058 condense_2013.indd 16 2013-04-09 16:56:36