Direct Measurement of Vena Contracta Area by Real-Time 3-Dimensional Echocardiography for Assessing...
6
Direct Measurement of Vena Contracta Area by Real-Time 3-Dimensional Echocardiography for Assessing Severity of Mitral Regurgitation Chaim Yosefy, MD, Judy Hung, MD, Sarah Chua, MD, Mordehay Vaturi, MD, Thanh-Thao Ton-Nu, MD, Mark D. Handschumacher, BS, and Robert A. Levine, MD* We tested the hypothesis that the vena contracta (VC) cross-sectional area in patients with mitral regurgitation (MR) can be reproducibly measured by real-time 3-dimensional (3D) echocardiography and correlates well with the volumetric effective regurgitant orifice area (EROA). Earlier MR repair requires accurate noninvasive measures, but practically, the VC area is difficult to image in 2-dimensional views, which are often oblique to it. 3D echocardiography can provide an otherwise unobtainable true cross-sectional view. In 45 patients with mild or greater MR, 44% eccentric, 2-dimensional and 3D VC areas were measured and correlated with the EROA derived from the regurgitant stroke volume. Real-time 3D echocardiography of the VC area correlated and agreed well with the EROA for both central and eccentric jets (r 2 0.86, SEE 0.02 cm 2 , difference 0.04 0.06 cm 2 ,p NS). For eccentric jets, 2-dimensional echocardiography overestimated the VC width compared with 3D echocardiography (p 0.024) and correlated more poorly with the EROA (r 2 0.61 vs 0.85, p <0.001), causing clinical misclassification in 45% of patients with eccentric MR. The interobserver variability for the 3D VC area was 0.03 cm 2 (7.5% of the mean, r 0.95); the intraobserver variability was 0.01 cm 2 (2.5% of the mean, r 0.97). In conclusion, real-time 3D echocardiography accurately and reproducibly quantified the vena contracta cross-sectional area in patients with both central and eccentric MR. Rapid acquisition and intuitive analysis promote practical clinical application of this central, directly visualized, measure and its correlation with outcome. © 2009 Elsevier Inc. All rights reserved. (Am J Cardiol 2009;104:978 –983) The vena contracta (VC) area, one of the most direct as- sessments of mitral regurgitation (MR), 1–3 is ideally measured in the short axis view perpendicular to the MR flow, 4 –16 but, as Hall et al 7 noted, it is generally difficult to identify in such a plane (Figure 1). The narrowest neck of the jet is often impossible to include in any imaging plane available from transthoracic windows. The available planes cut ob- liquely across the flow stream and often include portions of the expanding jet, overestimating the VC area. This problem is magnified when the jet is eccentric 17 compared to central jets (Figure 1). The use of real-time 3-dimensional (3D) echocardiography can potentially solve this problem. 18 –22 Once we have rapidly acquired the 3D flow stream, a plane can be readily aligned with the VC even if unavailable from the transthoracic windows (Figure 1). We tested the hypoth- esis that real-time 3D echocardiography can provide such a measure of the VC area in patients with both central and eccentric MR jets and that this measurement would corre- late well with an independent volumetric measure of the effective regurgitant orifice area (EROA) derived from quantitative Doppler echocardiography. We also correlated the 3D-optimized versus standard 2-dimensional (2D)-im- aged VC width with the EROA. Methods We enrolled 49 consecutive patients with mild or greater MR as determined by color Doppler echocardiography. 15 Patients were excluded for significant mitral stenosis (area 2.0 cm 2 ), mitral prosthesis, irregular rhythm, or signifi- cant aortic insufficiency or stenosis (area 1.5 cm 2 ). The institutional review board approved the noninvasive imag- ing protocol, and all patients provided verbal informed consent. The patients underwent scanning in the left lateral decu- bitus position with a matrix-array transducer (Sonos 7500, Philips Medical Systems, Andover, Massachusetts) using the narrowest sector possible to maximize the frame rate. 3D acquisitions were obtained from a parasternal long-axis transducer orientation that aligned the central beam axis with the leaflet tips. The transducer was translated and rotated to maximize visualization of the proximal flow con- vergence region, VC, and diverging jet within this plane. 3D data with Doppler color flow were automatically acquired for 7 beats using electrocardiographic gating with sus- pended respiration, Nyquist velocities of 40 to 68 cm/s, and a maximal color gain that eliminated random noise. The data sets were processed using TomTec 4D Cardio- View software (TomTec, Unterschleissheim, Germany). The 3D image was automatically cropped in the mediolat- Cardiac Ultrasound Laboratory, Massachusetts General Hospital, Har- vard Medical School, Boston, Massachusetts. Manuscript received Febru- ary 14, 2009; revised manuscript received and accepted May 13, 2009. *Corresponding author: Tel: (617) 724-1995; fax: (617) 643-1616. E-mail address: [email protected] (R.A. Levine). 0002-9149/09/$ – see front matter © 2009 Elsevier Inc. All rights reserved. www.AJConline.org doi:10.1016/j.amjcard.2009.05.043
-
Upload
chaim-yosefy -
Category
Documents
-
view
213 -
download
0
Transcript of Direct Measurement of Vena Contracta Area by Real-Time 3-Dimensional Echocardiography for Assessing...

siasofltijeOctemeleq
va
0d
Direct Measurement of Vena Contracta Area by Real-Time3-Dimensional Echocardiography for Assessing Severity of
Mitral Regurgitation
Chaim Yosefy, MD, Judy Hung, MD, Sarah Chua, MD, Mordehay Vaturi, MD,Thanh-Thao Ton-Nu, MD, Mark D. Handschumacher, BS, and Robert A. Levine, MD*
We tested the hypothesis that the vena contracta (VC) cross-sectional area in patients withmitral regurgitation (MR) can be reproducibly measured by real-time 3-dimensional (3D)echocardiography and correlates well with the volumetric effective regurgitant orifice area(EROA). Earlier MR repair requires accurate noninvasive measures, but practically, theVC area is difficult to image in 2-dimensional views, which are often oblique to it. 3Dechocardiography can provide an otherwise unobtainable true cross-sectional view. In 45patients with mild or greater MR, 44% eccentric, 2-dimensional and 3D VC areas weremeasured and correlated with the EROA derived from the regurgitant stroke volume.Real-time 3D echocardiography of the VC area correlated and agreed well with the EROAfor both central and eccentric jets (r2 � 0.86, SEE 0.02 cm2, difference 0.04 � 0.06 cm2, p �NS). For eccentric jets, 2-dimensional echocardiography overestimated the VC widthcompared with 3D echocardiography (p � 0.024) and correlated more poorly with theEROA (r2 � 0.61 vs 0.85, p <0.001), causing clinical misclassification in 45% of patientswith eccentric MR. The interobserver variability for the 3D VC area was 0.03 cm2 (7.5% ofthe mean, r � 0.95); the intraobserver variability was 0.01 cm2 (2.5% of the mean, r � 0.97).In conclusion, real-time 3D echocardiography accurately and reproducibly quantified thevena contracta cross-sectional area in patients with both central and eccentric MR. Rapidacquisition and intuitive analysis promote practical clinical application of this central,directly visualized, measure and its correlation with outcome. © 2009 Elsevier Inc. All
rights reserved. (Am J Cardiol 2009;104:978–983)ta
M
MP�ciic
bPt3twrvdfpa
V
The vena contracta (VC) area, one of the most direct as-essments of mitral regurgitation (MR),1–3 is ideally measuredn the short axis view perpendicular to the MR flow,4–16 but,s Hall et al7 noted, it is generally difficult to identify inuch a plane (Figure 1). The narrowest neck of the jet isften impossible to include in any imaging plane availablerom transthoracic windows. The available planes cut ob-iquely across the flow stream and often include portions ofhe expanding jet, overestimating the VC area. This problems magnified when the jet is eccentric17 compared to centralets (Figure 1). The use of real-time 3-dimensional (3D)chocardiography can potentially solve this problem.18–22
nce we have rapidly acquired the 3D flow stream, a planean be readily aligned with the VC even if unavailable fromhe transthoracic windows (Figure 1). We tested the hypoth-sis that real-time 3D echocardiography can provide such aeasure of the VC area in patients with both central and
ccentric MR jets and that this measurement would corre-ate well with an independent volumetric measure of theffective regurgitant orifice area (EROA) derived fromuantitative Doppler echocardiography. We also correlated
Cardiac Ultrasound Laboratory, Massachusetts General Hospital, Har-ard Medical School, Boston, Massachusetts. Manuscript received Febru-ry 14, 2009; revised manuscript received and accepted May 13, 2009.
*Corresponding author: Tel: (617) 724-1995; fax: (617) 643-1616.
TE-mail address: [email protected] (R.A. Levine).002-9149/09/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2009.05.043
he 3D-optimized versus standard 2-dimensional (2D)-im-ged VC width with the EROA.
ethods
We enrolled 49 consecutive patients with mild or greaterR as determined by color Doppler echocardiography.15
atients were excluded for significant mitral stenosis (area2.0 cm2), mitral prosthesis, irregular rhythm, or signifi-
ant aortic insufficiency or stenosis (area �1.5 cm2). Thenstitutional review board approved the noninvasive imag-ng protocol, and all patients provided verbal informedonsent.
The patients underwent scanning in the left lateral decu-itus position with a matrix-array transducer (Sonos 7500,hilips Medical Systems, Andover, Massachusetts) using
he narrowest sector possible to maximize the frame rate.D acquisitions were obtained from a parasternal long-axisransducer orientation that aligned the central beam axisith the leaflet tips. The transducer was translated and
otated to maximize visualization of the proximal flow con-ergence region, VC, and diverging jet within this plane. 3Data with Doppler color flow were automatically acquiredor 7 beats using electrocardiographic gating with sus-ended respiration, Nyquist velocities of 40 to 68 cm/s, andmaximal color gain that eliminated random noise.The data sets were processed using TomTec 4D Cardio-
iew software (TomTec, Unterschleissheim, Germany).
he 3D image was automatically cropped in the mediolat-www.AJConline.org

etm2nmrcwuVt
omam
iDpcvos
sfitvaeda
weaeEwmtse
uai
Fpntwa(ltg
979Valvular Heart Disease/3D MR Vena Contracta
ral direction to reveal the central imaging plane, which wasranslated and tilted to maximize the portions of the proxi-al flow convergence region, VC, and jet visualized (Figure
). The frame showing the largest MR flow area was mag-ified (early to mid-systolic for rheumatic or ischemic MR;id- to late systolic for mitral valve prolapse).23 The nar-
owest neck of the jet was identified, and the proximal flowonvergence region was cropped off (Figure 2). The valveas then turned to view the VC en face (Figure 2) andncropped in the mediolateral dimension to reveal the fullC cross-sectional area, which was measured, respecting
he surrounding leaflet borders.Mitral inflow was measured as the time-velocity integral
f the pulsed-wave Doppler mitral annular modal velocitiesultiplied by the mitral annular area (as an ellipse), with the
pical 4-chamber and 2-chamber diameters measured at theaximal leaflet opening.7,24,25
The MR stroke volume was calculated as the mitralnflow minus the aortic outflow, calculated using pulsedoppler echocardiography at the aortic annulus multi-lied by the annular area (circular). The EROA wasalculated as the MR stroke volume divided by the time-elocity integral of the continuous-wave Doppler MRrifice velocities.5 The EROA and VC areas were mea-ured in a blinded manner.
The narrowest anteroposterior VC dimension was mea-ured from the 3D image and independently from a magni-ed 2D parasternal long-axis view imaged at 2.5 MHz, with
he central beam through the leaflet tips and maximizedisualization of the proximal flow convergence region, VC,nd proximal jet. The VC width was defined as the narrow-st width of the proximal jet measured at or in the imme-iate vicinity of the MR orifice at the leaflet tips6,26 andveraged for 3 cardiac cycles.
The VC area as determined using 3D echocardiographyas compared with the EROA from quantitative Doppler
chocardiography (independent data) by linear regressionnalysis and Bland-Altman analysis of agreement for thentire population and for the central and eccentric jets.ccentric jets adhered to the mitral leaflets and left atrialall throughout their course. The VC using the 2D and 3Dethods were compared by paired t test and correlated with
he quantitative Doppler EROA by linear regression analy-is, with the F test to compare variances for the central andccentric jets.
As a check on the pulsed-wave Doppler measurementssed to calculate the EROA, we measured the mitral inflownd aortic outflow in 10 additional patients with no aorticnsufficiency and no or trace physiologic MR by color
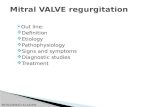
igure 1. (A) Eccentric jet: schematic indicating how view from standardarasternal transducer position sections the proximal MR jet oblique to itsarrowest neck or VC and overestimates the VC cross-sectional area. Arue cross-sectional plane (arrows) is unavailable from transthoracic 2Dindows but can be positioned through the jet after 3D acquisition. Ao �
orta; LA � left atrium; LV � left ventricle; RV � right ventricle.B) Central jet: obliquity is avoided for central jets when the left ventricularong axis parallels the chest wall. (C) Central jet: oblique cardiac orienta-ion relative to the chest wall also positions transthoracic 2D echocardio-
raphic views oblique to the VC.
Dci(i
oEmbd
R
ioT
wtw
Fmm the VC
TP
V
AMMAERMIMR
980 The American Journal of Cardiology (www.AJConline.org)
oppler echocardiography to ensure they were not signifi-antly different by paired t test. The (mitral inflow � aorticnflow)/(mitral inflow) was calculated to obtain its SDrange of calculated regurgitant fraction in the absence ofmportant MR) and to test the mean value versus 0.
Two independent observers repeated the measurementsf the 3D-derived VC area and width, 2D VC width, andROA in 10 patients. One observer repeated the measure-ents 1 month later. The observer variability was assessed
y linear regression analysis and as the SD of the observer
igure 2. (A) 3D cardiac image is automatically cropped in a mediolateralaximize portions of the proximal flow convergence region, VC, and diveore proximal flow region cropped. (D) The valve is then turned to view
able 1atient characteristics
ariable To(n �
ge 64.2 �ale/female 28itral valve inflow SV (ml) 121.7 �ortic valve outflow SV (ml) 60.0 �jection fraction 36.0 �egurgitant volume by Doppler echocardiography (ml) 61.71 �itral regurgitant fraction (%) 40.58 �
schemic heart disease 26 (itral valve prolapse 10 (heumatic heart disease 9 (
* p �0.05 for total versus central, total versus eccentric, and eccentricSV � stroke volume.
ifferences as a percentage of the pooled mean values. c
esults
Of the 49 patients enrolled, 4 were excluded because ofmaging limitations affecting the ability to quantify the VCr EROA, leaving 45 patients (28 men and 17 women,able 1) in the study.
The VC area by 3D echocardiography correlated wellith the quantitative Doppler EROA in the entire popula-
ion (Figure 3; r2 � 0.86, SEE 0.02 cm2) and in patientsith central and eccentric MR jets (r2 � 0.92, SEE 0.02
n to reveal the central imaging plane; this plane is translated and tilted tot visualized in it. (B,C) The narrowest neck of the jet is identified and the
en face and measure its area.
Central(n � 25)
Eccentric(n � 20)
p Value
62.9 � 6.4 65.1 � 4.1 NS16/10 12/7 NS
112.1 � 19.4 131.4 � 27.2 NS57.7 � 14.1 62.3 � 15.4 NS34.3 � 10.6 38.3 � 8.2 NS
54.41 � 17.81 69.02 � 18.04 �0.05*40.03 � 12.39 41.14 � 7.42 NS
15 113 73 6
central.
directiorging je
tal45)
4.5/17
25.314.810.819.1810.10
58%)22%)20%)
versus
m2, and r2 � 0.86, SEE 0.02 cm2, respectively; Figure 3).

Ts
waEt
i00
tt
Fj by dir
Fo
981Valvular Heart Disease/3D MR Vena Contracta
he differences between the VC area and EROA were notignificant (0.04 � 0.06 cm2; Figure 3).
The VC width from 2D and 3D echocardiography agreedell for the central jets (0.64 � 0.20 vs 0.61 � 0.15 cm),
nd both correlated well with the quantitative DopplerROA (r2 � 0.81 and r2 � 0.82, respectively; Figure 4). For
igure 3. Linear regression analysis of 3D VC area versus quantitative Doets (B,C). (D) Bland-Altman analysis of differences between 3D VC area
igure 4. Linear regression analysis of 2D and 3D VC width versus volumeverestimation by 2D echocardiography for eccentric jets.
he eccentric jets, the 2D VC width overestimated the min- E
mal dimension by 3D echocardiography (0.65 � 0.13 vs.54 � 0.16 cm, p � 0.024), with poorer correlation (r2 �.61 vs r2 � 0.85, p �0.001; Figure 4).
According to the published cutoffs, the 2D overestima-ion produced clinical misclassifications not resulting fromhe 3D approach: 5 of 5 patients with eccentric MR and an
ROA for the total MR population (A) and those with central and eccentricect tracing and effective regurgitant orifice area by quantitative Doppler.
OA for central (A) and eccentric (B) MR jets, showing clinically important
ppler E
tric ER
ROA �0.2 cm2 (mild MR) had a 2D VC width of �0.4

coco
Dc0N
rtrE0V0ts
D
fqtriapocc
lIfi
2taatiflcstbpVwcEtqsda
blblcatnpempo
Fo mitatio
982 The American Journal of Cardiology (www.AJConline.org)
m (moderate MR); 4 (36%) of 11 patients with an EROAf 0.2 to 0.4 cm2 (moderate MR) had a 2D VC width �0.7m (severe MR), for a total misclassification rate of 45% (9f 20 patients).15
In 10 patients with no or trace MR, the quantitativeoppler mitral inflow and aortic outflow were not signifi-
antly different (91.5 � 8.3 versus 87.8 � 9.9 ml/beat, p �.11). The calculated regurgitant fraction was 2 � 6% (p �S vs 0), indicating a reasonable range of variability.Measurements of the 3D VC area by the 2 observers cor-
elated well (r � 0.95, SD of differences 0.03 cm2 or 7.5% ofhe mean). The intraobserver variability was 0.01 cm2 (2.5%;� 0.97). The observer variability for quantitative DopplerROA was 0.03 cm2 for the 2 observers (7.5%; r � 0.93) and.02 cm2 (r � 0.94) for 1. The observer agreement for the 3DC width had a SD of 0.02 cm for 2 observers (r � 0.92) and.01 cm (r � 0.95) for intraobserver variability (6% and 3% ofhe mean, respectively). For the 2D VC width, the interob-erver r was 0.95 (SD 0.06 cm).
iscussion
The increasing trend to repair MR before left ventricularunction deterioration demands accurate noninvasive MRuantification.15 The VC, the smallest area of flow beyondhe orifice, is a central measure, reflecting the EROA, andequires standardized measurement.6,11 2D images are lim-ted in describing the full VC area, which can vary in shapemong patients and at different sites across a valve. Inractical experience, a true short-axis view of the VC isften difficult to obtain in standard 2D views,7 which oftenut obliquely across the proximal jet owing to either jet orardiac angulation relative to the beam (Figure 1).
Real-time 3D echocardiography18–22,27 can solve this prob-em, but its practicality and accuracy must be established.nitial studies have shown accuracy for the VC in aortic insuf-
igure 5. 2D VC width can also be oblique to the true VC minor dimensiof the measured VC width with the true minor dimension. This is not a li
ciency and ventricular septal defect by reconstructing rotated m
D views28–30; however, that approach is limited by the needo maintain a fixed transducer position during a prolongedcquisition. Real-time 3D echocardiography has considerablyccelerated and simplified image acquisition, and the naviga-ion tools available on-board the scanner itself provides anntuitively reasonable and rapid method for standardizing theow stream dimensions. By viewing the jet from the side andropping through its narrowest neck, we can obtain a cross-ectional view of the VC that would be unavailable fromransthoracic windows. Although volumetric scanning withroad-beam formation might limit the lateral resolution, thearasternal acquisition in the present study allowed most of theC circumference to be imaged with the axial beam resolution,hich should be preserved.9 The results showed excellent
orrelation and agreement with an independent measure of theROA derived from the regurgitant volume and have quanti-
atively confirmed the tracking of values reported with semi-uantitative angiographic grade.27 The results were equallytrong for eccentric jets, the most difficult to transect perpen-icularly in 2D views,8,17 and the reproducibility was clinicallycceptable.
The linear VC width was equivalent for central jets byoth 2D and 3D techniques, because it is measured from aong-axis view. However, for eccentric jets, the VC widthy 2D echocardiography was overestimated and correlatedess well with the EROA, producing frequent clinical mis-lassification. This might relate to a tendency to measure anpparent VC width delineated by the leaflet portions wherehe jet is seen to exit in 2D images, instead of at the truearrowest neck, 1 border of which might lie somewhatroximal to the apparent leaflet exit in 3 dimensions forccentric jets (Figure 1). For an eccentric jet, the overesti-ation might also relate to an oblique orientation of the 2D
lane relative to the minor axis of the VC, which is thenverestimated relative to a true minor axis intersected by the
n eccentrically originating jet (B); 3D echocardiography allows alignmentn for central jets (A).
n for a
ore adjustable 3D cropping plane (Figure 5). Little et al22

fmifefipi
bmabcetddcpfiv
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
983Valvular Heart Disease/3D MR Vena Contracta
ound that the MR severity and orifice shape affected agree-ent of real-time 3D echocardiography VC area with prox-
mal flow convergence region-derived EROA, but they alsoound a clear superiority of three-dimensions in assessingccentric jets, thereby strengthening the validity of ourndings, particularly in relation to eccentric jets. This ap-roach is exciting and a potential new standard for analyz-ng this important clinical problem.
One theoretical advantage of the 3D approach is that a 2Deam, if exactly perpendicular to the laminar VC flow, willeasure a negligible Doppler velocity component. In the 3D
pproach, the beam need not be perpendicular to the flowecause the cross-sectional view is derived only by subsequentropping. Concerns about limited lateral resolution at the lat-ral orifice will be minimized by the counterbalancing effect ofhe surrounding leaflet tissue that circumscribes the color areaetermined by the tissue priority algorithm of the ultrasoundisplay. Although no ideal reference standard is available foromparison, quantitative Doppler echocardiography uses com-letely independent data, and its correct application was veri-ed in 10 patients without MR, showing no significant MRolume and low variability.7,24,25
1. Ling LH, Enriquez-Sarano M, Seward JB, Orszulak TA, Schaff HV,Bailey KR, Tajik AJ, Frye RL. Early surgery in patients with mitralregurgitation due to flail leaflets: A long-term outcome study. Circu-lation 1997;96:1819–1825.
2. Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Isch-emic mitral regurgitation: long-term outcome and prognostic implica-tions with quantitative Doppler assessment. Circulation 2001;103:1759–1764.
3. Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, Detaint D,Capps M, Nkomo V, Scott C, Schaff HV, Tajik AJ. Quantitativedeterminants of the outcome of asymptomatic mitral regurgitation.N Engl J Med 2005;352:875–883.
4. Grayburn PA, Fehske W, Omran H, Brickner ME, Lüderitz B. Mul-tiplane transesophageal echocardiographic assessment of mitral regur-gitation by Doppler color flow mapping of the vena contracta. Am JCardiol 1994;74:912–917.
5. Enriquez-Sarano M, Seward JB, Bailey KR, Tajik AJ. Effective re-gurgitant orifice area: a noninvasive Doppler development of an oldhemodynamic concept. J Am Coll Cardiol 1994;23:443–451.
6. Mele D, Vandervoort P, Palacios I, Rivera JM, Dinsmore RE,Schwammenthal E, Marshall JE, Weyman AE, Levine RA. Proximaljet size by Doppler flow mapping predicts severity of mitral regurgi-tation: clinical studies. Circulation 1995;91:746–754.
7. Hall SA, Brickner ME, Willet EL, Irani WN, Afridi I, Grayburn PA.Assessment of mitral regurgitation severity by Doppler color flowmapping of the vena contracta. Circulation 1997;95:636–642.
8. Zhou X, Jones M, Shiota T, Yamada L, Teien D, Sahn DJ. Venacontracta imaged by Doppler color flow mapping predicts the severityof eccentric mitral regurgitation better than color jet area: a chronicanimal study. J Am Coll Cardiol 1997;30:1393–1398.
9. Thomas JD. How leaky is that mitral valve? Simplified Dopplermethods to measure regurgitant orifice area. Circulation 1997;95:548 –550.
0. Buck T, Mucci RA, Guerrero JL, Holmvang G, Handschumacher MD,Levine RA. The power-velocity integral at the vena contracta: a newmethod for direct quantification of regurgitant volume flow. Circula-tion 2000;102:1053–1061.
1. Roberts BJ, Grayburn PA. Color flow imaging of the vena contracta inmitral regurgitation: technical considerations. J Am Soc Echocardiogr2003;16:1002–1006.
2. Quere JP, Tribouilloy C, Enriquez-Sarano M. Vena contracta widthmeasurement: theoretic basis and usefulness in the assessment ofvalvular regurgitation severity. Curr Cardiol Rep 2003;5:1101–1115.
3. Lesniak-Sobelga A, Olszowska M, Pienazek P, Podolec P, Tracz W.
Vena contracta width as a simple method of assessing mitral valveregurgitation: comparison with Doppler quantitative methods. J HeartValve Dis 2004;13:608–614.
4. Buck T, Plicht B, Hunold P, Mucci RA, Erbel R, Levine RA. Broad-beam spectral Doppler sonification of the vena contracta using matrix-array technology: a new solution for semiautomated quantification ofmitral regurgitant flow volume and orifice area. J Am Coll Cardiol2005;45:770–779.
5. Zoghbi WA, Enriquez-Sarano M, Foster E, Grayburn PA, Kraft CD,Levine RA, Nihoyannopoulos P, Otto CM, Quinones MA, RakowskiH, Stewart WJ, Waggoner A, Weissman NJ. American Society ofEchocardiography report: recommendations for evaluation of the se-verity of native valvular regurgitation with two-dimensional andDoppler echocardiography. J Am Soc Echocardiogr 2003;16:777–802.
6. Foster GP, Isselbacher EM, Rose GA, Torchiana DF, Akins CW,Picard MH. Accurate localization of mitral regurgitant defects usingmultiplane transesophageal echocardiography. Ann Thorac Surg 1998;65:1025–1031.
7. Shiota T, Jones M, Teien D, Yamada I, Passafini A, Knudson O, SahnDJ. Color Doppler regurgitant jet area for evaluating eccentric mitralregurgitation: an animal study with quantified mitral regurgitation.J Am Coll Cardiol 1994;24:813–819.
8. De Castro S, Salandin V, Cartoni D, Valfrè C, Salvador L, Magni G,Adorisio R, Papetti F, Beni S, Fedele F, Pandian NG. Qualitative andquantitative evaluation of mitral valve morphology by intraoperativevolume-rendered three-dimensional echocardiography. J Heart ValveDis 2002;11:173–180.
9. Sugeng L, Spencer KT, Mor-Avi V, DeCara JM, Bednarz JE, WeinertL, Korcarz CE, Lammertin G, Balasia B, Jayakar D, Jeevan-Andam V,Lang RM. Dynamic three-dimensional color flow Doppler: an im-proved technique for the assessment of mitral regurgitation. Echocar-diography 2003;20:265–273.
0. Monaghan MJ. Role of real time 3D echocardiography in evaluatingthe left ventricle. Heart 2006;92:131–136.
1. Sugeng L, Weinert L, Lang RM. Real-time 3-dimensional color Dopp-ler flow of mitral and tricuspid regurgitation: feasibility and initialquantitative comparison with 2-dimensional methods. J Am Soc Echo-cardiogr 2007;20:1050–1057.
2. Little SH, Pirat B, Kumar R, Igo SR, McCulloch M, Hartley CJ, Xu J,Zoghbi WA. Three-dimensional color Doppler echocardiography fordirect measurement of vena contracta area in mitral regurgitation: invitro validation and clinical experience. J Am Coll Cardiol Imaging2008;1:695–704.
3. Schwammenthal E, Chen C, Benning F, Block M, Breithardt G,Levine RA. Dynamics of mitral regurgitant flow and orifice area:physiologic application of the proximal flow convergence method:clinical data and experimental testing. Circulation 1994;90:307–322.
4. Ascah KJ, Stewart WJ, Jiang L, Guerrero JL, Newell JB, Gillam LD,Weyman AE. A Doppler-two-dimensional echocardiographic methodfor quantitation of mitral regurgitation. Circulation 1985;72:377–383.
5. Enriquez-Sarano M, Bailey KR, Seward JB, Tajik AJ, Krohn MJ,Mays JM. Quantitative Doppler assessment of valvular regurgitation.Circulation 1993;87:841–848.
6. Weyman AE. Principles and Practice of Echocardiography, 2nd ed.Philadelphia: Lea & Febiger; 1994.
7. Khanna D, Vengala S, Miller AP, Nanda NC, Lloyd SG, Ahmed S,Sinha A, Mehmood F, Bodiwala K, Upendram S, Gownder M, DodHS, Nunez A, Pacifico AD, McGiffin DC, Kirklin JK, Misra VK.Quantification of mitral regurgitation by live three-dimensional trans-thoracic echocardiographic measurements of vena contracta area.Echocardiography 2004;21:737–743.
8. Mori Y, Shiota T, Jones M, Wanitkun S, Irvine T, Li X, Delabays A,Pandian NG, Sahn DJ. Three-dimensional reconstruction of the colorDoppler-imaged vena contracta for quantifying aortic regurgitation:studies in a chronic animal model. Circulation 1999;30:1611–1617.
9. Ishii M, Hashino K, Eto G, Tsutsumi T, Himeno W, Sugahara Y, MutaH, Furui J, Akagi T, Ito Y, Kato H. Quantitative assessment of severityof ventricular septal defect by three-dimensional reconstruction ofcolor Doppler-imaged vena contracta and flow convergence region.Circulation 2001;103:664–669.
0. Ishii M, Jones M, Shiota T, Yamada I, Sinclair B, Heinrich RS,Yoganathan AP, Sahn DJ. Temporal variability of vena contracta andjet areas with color Doppler in aortic regurgitation: a chronic animal
model study. J Am Soc Echocardiogr 1998;11:1064–1071.