
Direct and Rapid Determination of Baclofen - Journal of Analytical
9
Journal of Analytical Toxicology, Vol. 27, July/August 2003 Direct and Rapid Determination of Baclofen (Lioresal | and Carisoprodol (Soma | in Bovine Serum by Liquid Chromatography-MassSpectrometry Irina Rudik Miksa* and Robert H. Poppenga University of Pennsylvania, School of VeterinaryMedicine, Departmentof Pathobiology, New Bolton Center, Toxicology, 382 WestStreet Road, Kennett Square, PA 19348 I Abstract Baclofen (Lioresal), a lipophilic analogue of 7-aminobutyric acid (GABA), and carisoprodol (Soma), a central nervous system depressant with an unknown mechanism of pharmacologic action, are categorized as muscle relaxants. Baclofen is used clinically in the management of spasticity and its sequelae secondary to severe chronic disorders such as multiple sclerosis and other types of spinal cord lesions. Carisoprodol is used for discomfort associated with acute and painful musculoskeletal conditions. Intoxication from these drugs occurs in both humans and animals necessitating a need for their detection in plasma/serum, tissue, and gastrointestinal contents samples. A sensitive and specific analytical method for detection and quantitation of these compounds using liquid chromatography with positive atmospheric pressure chemical ionization-mass spectrometry was developed. A rapid extraction procedure for both analytes from fortified bovine sera is described. Chromatographic separation was carried out on a Cls reverse.phase column with a gradient elution of acetonitrile and 0.25% acetic acid. The effluent was directed to the mass spectrometer with fragmentation information for baclofen and carisoprodol obtained in a scan monitoring mode. Linear standard curves for baclofen and carisoprodol were constructed based on at least two corresponding extracted ions over a concentration range of 0.1-50 pg/mL. The analysis of fortified sera samples demonstrates good accuracy and precision for the method with a limit of detection of 0.5 pg/mL for carisoprodol (n = 3) and 1 pg/mL for baclofen (n = 4) and a limit of quantitation of 2 pg/mL for both compounds. Recoveries at the limit of quantitation were between 75 and 95% for both analytes, with a 4.8-9.3% range in standard deviation. Introduction Skeletal muscle relaxants are therapeutic agents that differ substantially in their chemical, pharmacologic, pharmacoki- 9 Authorto whom correspondence should be addressed. E-mail: [email protected]. netic, and toxicologic properties (l). They are used for the treatment of acute, painful musculoskeletal conditions sec- ondary to muscle injury or spasm or chronic diseases such as multiple sclerosis. Available by prescription, skeletal muscle re- laxants include baclofen (Lioresal), carisoprodol (Soma), or- phenadrine (Norflex| cyclobenzaprine (Flexeril| methocarbamol (Robaxin| and dantrolene (Dantrium| Most of these agents act on the central nervous system (CNS) as simple depressants, although their specific pharmacologic ac- tions within the CNS differ. For example, baclofen is believed to enhance GABAA-associated neurotransmission, whereas the pharmacologic action of carisoprodol is likely related to its centrally mediated sedative effects (1,2). With the exception of dantrolene, they are rapidly and almost completely absorbed following oral administration. Metabolism A 0 0 B H2N O CI Figure1. Chemical structure for carisoprodol (A)and badofen(B). The centerof asymmetry in badofen is shownas (*). Reproduction (photocopying) of editorial content of this journal is prohibited without publisher's permission. 275 Downloaded from https://academic.oup.com/jat/article/27/5/275/752388 by guest on 09 December 2021
Transcript of Direct and Rapid Determination of Baclofen - Journal of Analytical
Journal of Analytical Toxicology, Vol. 27, July/August 2003
Direct and Rapid Determination of Baclofen (Lioresal | and Carisoprodol (Soma | in Bovine Serum by Liquid Chromatography-Mass Spectrometry
I r ina Rudik Miksa* and Robert H. Poppenga
University of Pennsylvania, School of Veterinary Medicine, Department of Pathobiology, New Bolton Center, Toxicology, 382 West Street Road, Kennett Square, PA 19348
I Abstract
Baclofen (Lioresal), a lipophilic analogue of 7-aminobutyric acid (GABA), and carisoprodol (Soma), a central nervous system depressant with an unknown mechanism of pharmacologic action, are categorized as muscle relaxants. Baclofen is used clinically in the management of spasticity and its sequelae secondary to severe chronic disorders such as multiple sclerosis and other types of spinal cord lesions. Carisoprodol is used for discomfort associated with acute and painful musculoskeletal conditions. Intoxication from these drugs occurs in both humans and animals necessitating a need for their detection in plasma/serum, tissue, and gastrointestinal contents samples. A sensitive and specific analytical method for detection and quantitation of these compounds using liquid chromatography with positive atmospheric pressure chemical ionization-mass spectrometry was developed. A rapid extraction procedure for both analytes from fortified bovine sera is described. Chromatographic separation was carried out on a Cls reverse.phase column with a gradient elution of acetonitrile and 0.25% acetic acid. The effluent was directed to the mass spectrometer with fragmentation information for baclofen and carisoprodol obtained in a scan monitoring mode. Linear standard curves for baclofen and carisoprodol were constructed based on at least two corresponding extracted ions over a concentration range of 0.1-50 pg/mL. The analysis of fortified sera samples demonstrates good accuracy and precision for the method with a limit of detection of 0.5 pg/mL for carisoprodol (n = 3) and 1 pg/mL for baclofen (n = 4) and a limit of quantitation of 2 pg/mL for both compounds. Recoveries at the limit of quantitation were between 75 and 95% for both analytes, with a 4.8-9.3% range in standard deviation.
Introduction
Skeletal muscle relaxants are therapeutic agents that differ substantially in their chemical, pharmacologic, pharmacoki-
�9 Author to whom correspondence should be addressed. E-mail: [email protected].
netic, and toxicologic properties (l). They are used for the treatment of acute, painful musculoskeletal conditions sec- ondary to muscle injury or spasm or chronic diseases such as multiple sclerosis. Available by prescription, skeletal muscle re- laxants include baclofen (Lioresal), carisoprodol (Soma), or- phenadrine (Norflex| cyclobenzaprine (Flexeril| methocarbamol (Robaxin| and dantrolene (Dantrium| Most of these agents act on the central nervous system (CNS) as simple depressants, although their specific pharmacologic ac- tions within the CNS differ. For example, baclofen is believed to enhance GABAA-associated neurotransmission, whereas the pharmacologic action of carisoprodol is likely related to its centrally mediated sedative effects (1,2).
With the exception of dantrolene, they are rapidly and almost completely absorbed following oral administration. Metabolism
A 0 0
B
H2N O
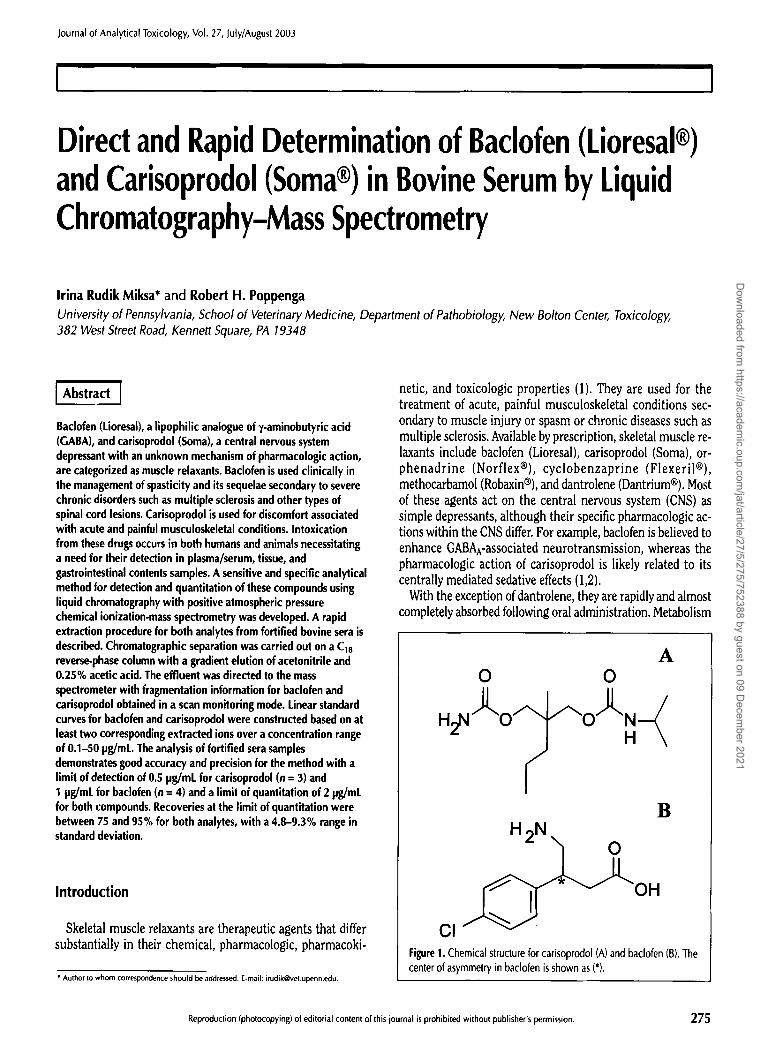
CI Figure 1. Chemical structure for carisoprodol (A) and badofen (B). The center of asymmetry in badofen is shown as (*).
Reproduction (photocopying) of editorial content of this journal is prohibited without publisher's permission. 275
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

occurs primarily in the liver with variable, but significant elim- ination of either parent compound or one or more metabolites via the urine (1). Baclofen is largely eliminated as unchanged parent drug via the urine with a plasma half-life of 2.5-4 h, whereas carisoprodol is metabolized to meprobamate and other metabolites (2) and has a plasma half-life of 1.5-6 h (1). Less than 1% of a dose of carisoprodol is eliminated via the urine un- changed.
Most muscle relaxants are not considered controlled sub- stances under federal regulations, although carisprodol and its metabolite, meprobamate, have been associated with sub- stance abuse. A number of reports indicate that carisoprodol (Figure 1A) is abused in combination with tramadol (Ultram | to obtain psychotropic effects (3). In addition, carisoprodol causes severe driving impairment when the combined plasma concentrations of carisoprodol and meprobamate are 10 IJg/mL or greater (4).
Muscle relaxants are associated with significant potential for intoxication. The American Association of Poison Control Cen- ters reported 12,688 cases of muscle relaxant exposure in 1998, with 48% of the cases exhibiting symptoms (5). Thirteen deaths resulted from the ingestion of carisoprodol, methocarbamol, cy- clobenzaprine, baclofen, or meprobamate, ingested either alone or in combination with other agents. There are a number of re- ports of baclofen overdose in children, adolescents, and adults (6-11).
Although intoxications are not as well documented in vet- erinary medicine as in human medicine, there are reports of an- imal intoxication following the ingestion of baclofen. The British Veterinary Poisons Information Service has reported, on average, 10 cases of baclofen exposure per year in dogs since 1992, with nearly all of the cases showing clinical signs (12). A presumptive case of baclofen intoxication in a dog was reported in the veterinary literature (13). More recently, three other cases involving baclofen intoxication in dogs have been re- ported (14-16).
Thus, because of possible CNS impairment at pharmacologic doses and abuse and intoxication potential for many of the skeletal muscle relaxants, analytical procedures are needed to detect these drugs in fluid, tissue, and gastrointestinal con- tent samples. Various methods for baclofen isolation from human urine and plasma and its detection have been reported. Analysis of baclofen has been achieved by high-performance liquid chromatography (HPLC) with fluorescent (17,18), UV (19-21), electrochemical (22), and amperometric detection (23). Gas-liquid chromatography with electron-capture detec- tion (24,25), flame-ionization detection (FID) (20), and mass spectrometric detection (MS) have been applied and reported as reliable methods of baclofen analysis (8,26). Other techniques such as capillary electrophoresis with laser-induced fluores- cence (27,28) and spectrophotometric detection (29) have also been reported. With recognition that baclofen has stereospecific actions on the peripheral and central nervous systems, methods were developed for detection and separation of both S-(+)- and R-(-)-enantiomers of baclofen (20,25,28,30). However, the ma- jority of the mentioned methods require some use of previously solid-phase extraction (SPE) with Sep-Pak Cl8, SCX (Waters, Milford, MA) and Bond Elut columns (Varian, Harbor City, CA)
276
Journal of Analytical Toxicology, Vol. 27, July/August 2003
derivatization agents, and baclofen tritium labeling in order to obtain limits of detection (LOD) of 0.005-0.010 IJg/mL.
A number of different methods have been presented for anal- ysis of the active metabolite of carisoprodol, meprobamate, with very limited reports available on detection and isolation of carisoprodol itself. An early HPLC study of the separation and quantitation of widely used muscle relaxant-analgesic mixtures showed that carisoprodol could be separated from phenacetin and caffeine with normal-phase silica or cyanopropylsilane columns with 3-5% accuracy (31). Direct de- tection of carisprodol in plasma was achieved on a gas chro- matograph (GC) with FID without any need for derivatization and quantitation, based on vinylbarbital as the internal standard (32). The association of carisoprodol use with meprobamate abuse and dependence and the fact that the peak carisoprodol plasma concentration of 4-7 IJg/mL after oral absorption is at- tained in 2-4 h (33) warrants the need for a sensitive and spe- cific method of carisoprodol detection in serum/plasma at low (IJg/mL) levels. Direct detection of carisoprodol in urine was re- ported not to be of practical application because of limited elimination of parent drug via urine (33).
Although HPLC with UV detection is a valuable technique, its disadvantages of detection based solely on comparison of the elution profile of baclofen and carisoprodol in a sample com- pared with that of a pure standard led to recent developments in more definite methods for analyte detection. The recently achieved interface between LC and MS has proven to be a highly effective technique in forensic and clinical toxicology for characterization of sample mixtures that are difficult to analyze under conventional HPLC-UV analysis (34-36). LC-MS methods have become widely accepted for online selective sep- aration of compounds present in animal matrices in which a very high degree of structural specificity is required of LC ef- fluent. Such application, utilizing SPE and LC-MS, was re- cently reported for baclofen detection in plasma (37).
The present paper contains the first report of a simple, sen- sitive, specific, and rapid multiresidue detection method for ba- clofen and carisoprodol present in bovine serum. The analysis omits any use of SPE columns and is complete within 8 min. The method of separation and detection is LC-MS with positive atmospheric pressure chemical ionization (APCI) set to run in a full-scan monitoring mode. The detection and quantitation of baclofen and carisoprodol present in bovine serum at low con- centrations was possible because of the use of a small sample volume and the ability to collect molecular and structural in- formation for coelution and interfering matrix compounds.
Material and Methods
Materials Baclofen and carisoprodol standards were purchased from
Sigma (St. Louis, MO). Acetonitrile (ACN) and glacial acetic acid were obtained from Fisher Scientific (Pittsburgh, PA). All reagents were HPLC grade. Centrifugal filter devices with sample reservoir (microcon-30) with the molecular weight limit in Daltons of 30,000 were purchased from Millipore (Bed-
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Journal of Analytical Toxicology, '4oi. 27, July/August 2003
ford, MA). Ultra Pure water system from Millipore (Milli-Q RG and Milli-RO10) was used to generate water with resistivity of 18 M~cm. The LC autosampler vials (2 mL, wide opening) designed for robotic arm tray with a 250-]JL high recovery flat-bottom inserts were purchased from Agilent Technologies (Wilmington, DE).
Preparation and analysis of standards Individual stock standards of 1000 pg/mL of baclofen and
carisoprodol were prepared by dissolving 10 mg of each com- pound in 10 mL of ultra pure water and ACN, respectively. Added to 900 tJL of ACN/water (1:1 dilution) solution was 50 lJL of each 10001Jg/mL standard to make 50 ]~g/mL stock standard mix. Serial dilutions of 50 ]Jg/mL standard mix were performed to obtain standards of 25 and 10 ]Jg/mL. Working standard mixtures of 5.0, 1.0, 0.2, and 0.1 IJg/mL were prepared by di- luting 500,200,100, and 50 IJL of 10 ]Jg/mL standard mix with the ACN/water solution to total volume of 1 mL, respectively. All samples were stored at 4~ when not in use. Prior to analysis and construction of the calibration curves, all standards were placed into microcon-30 devices and treated in the same manner as the samples.
Sample extraction and analysis Prior to fortification of bovine serum sample with baclofen
and carisoprodol, negative control serum (not containing any detectable amounts of the analytes under investigation) was an- alyzed. Aliquots of 500 IJL of negative control sera were spiked with baclofen and carisoprodol at 5.0, 2.0, 1.0, and 0.5 IJg/mL levels by adding 250, 100, 50, and 25 ]JL of 10 IJg/mL working mix to the appropriate volume of sera, respectively. Serum spikes at 0.5 ]~g/mL were performed in triplicate analysis (n = 3)with the rest of serum spikes done in replicates of four (n = 4). All samples were then placed into corresponding mi- crocon-30 devices and centrifuged for 30 rain at 14,000 • The wash-through for each sample was then transferred to an HPLC autosampler vials equipped with high recovery inserts. The samples were then ready for LC-MS analysis. No dilution factor was required for calculations.
LC-MS conditions A series 1100 LC-MSD Hewlett Packard system (Wilm-
ington, DE) was equipped with a dual LC pump, diode-array detector, degasser, column thermostat, and autosampler. A Betasil Cm reversed-phase column from Keystone Scientific (150- • 4.6-ram, 5-]~m particle size) (Bellefonte, PA) was equi- librated with the mobile phase (50% ACN-50% of 0.25% acetic acid solution in water) at 0.6 mL/min prior to analysis. The LC profiles were developed at 45~ with a mobile phase and flow rate gradients. The following elution program profile was used: 0-3 rain, 50% ACN at 0.6 mL/min; 3-5 rain to 90% at 1 mL/min; 5-6 rain hold; 6-7 rain, back to 50% ACN at 0.6 mL/min; and 7-8 rain hold. The injected sample volume for each assay was 10 IJL. The MS was set to operate in positive APCI mode without any time delays with a gain of 3, frag- mentor at 70, threshold of 50, and a step-size of 0.10. A full- scan mode was employed (ion range ofm/z 150-400) to obtain a complete representation of total ion chromatogram for both
baclofen and carisoprodol. The optimal MS conditions were de- termined by running flow injection analysis (omitting LC column) for 5.0 IJg/mL baclofen and carisoprodol individual standards. The following MS settings were utilized during final analysis: dry gas flow rate of 3 mL/min, corona at 4 IJA, nebu- lizer pressure of 50 psi nitrogen, dry gas temperature of 250~ vapor temperature was set at 300~ and capillary voltage of 2500. Ions with ra/z of 214 and 196 eluted at 2.6 rain and ions with m/z of 261, 200, and 176 were detected at 5.6 min for ba- ciofen and carisoprodol, respectively.
Linearity, limit of detection (LOD), and limit of quantitation (LOD)
Linearity of instrument standard response was determined for baclofen and carisopradol detection with two sets of standard concentrations: 5.0, 1.0, 0.2, and 0.1 IJg/mL (low range) and 50.0, 25.0, 10.0, 5.0, and 1.0 ]Jg/mL (high range). An individual 4/s-point calibration curve was constructed for each analyte based on the peak areas under the corresponding individual ex- tracted ion profiles prior to each sample analysis. A plot of con- centration versus peak area resulted in a linear curve for individual analysis of each drug (n = 3) at corresponding ex- tracted ion profiles, indicating that detection was linear from 0.1 to 5 IJg/mL (low range) and 1.0 to 50 ]Jg/mL (high range). This resulted in correlation coefficients for the low range stan- dards of 0.99998-0.99959 (m/z 214.1) and 0.99923-0.99299 (m/z 196.2), 0.99944--0.99944 (m/z 261.1), 0.99967-0.99845 (m/z 200.0), and 0.99987-0.99916 (m/z 176.0) for each standard curve repeated in triplicate for baclofen and carisoprodol, re- spectively. In the case of the high range standards, correlation coefficients obtained were as follows: 0.99991-0.99919 (m/z 214.1), 0.99957-0.99465 (m/z 196.2), 0.99974-0.99857 (m/z 261.1), 0.99983-0.99787 (m/z 200.0), and 0.9999-0.99681 (m/z 176.0). The percent standard deviation (%RSD) for all the curves was between 0.02 and 0.33%.
The LOD values were obtained by analyzing negative serum samples fortified with a mix of baclofen and carisoprodol at different concentrations and performed in replicates of 3 and 4 (see the Sample Extraction and Analysis section). LOD was de- fined as the lowest concentration of each analyte in a sample that could be detected and expressed as a concentration at a S/N ratio of 3:1. The lower limit of quantitation (LOQ) was defined as the lowest measured concentration (based on LOD analysis) that was within 25% of the true value.
Precision Precision of standard mixtures and serum spikes was deter-
mined by three consecutive injections of 10-]JL aliquots of a 1.0 ]~g/mL baclofen and carisopradol standard mix and a 2-1Jg/mL serum spike. The area under the extracted ion peaks was es- tablished via Hewlett Packard integration algorithm and was observed to be reproducible. The %RSD values for the areas under the peak for the three analyses of 1.0 IJg/mL standard and for 2 ~g/mL fortified sera were 3.3% and 1.0% at ra/z 214 and 2.0% and 5.1% at m/z 196 for baclofen, respectively. Similar data was obtained for carisoprodol with %RSD of 6.2% and 14.4% at m/z 261, 10.4% and 9.8% at m/z 200, and 8.0% and 7.3% at m/z 176 for a standard mix and spike, respectively.
277
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Table I. Sample Baclofen Recovery Based on Two Extracted Ions Followed in a Full-Scan Monitoring Mode
Concentration* Ion 214 t Ion 214 Ion 196 Ion 196 (pg/mt) (%Rec.)* (%RSD)* (%Rec.) (%RSD) Results
0,5 75,5 6.3 nd** nd 1.0 93.3 7.7 61.6 2.1 2.0 94.0 21 75.1 16 5.0 91,2 5.9 67.8 5.6
* Negative control serum was fortified as described in the Methods section. Concentrations of baclofen used to spike each sample are listed in pg/mL.
r The specific ions monitored. * Analytes percent recovery (%Rec.) and %RSD were calculated as described in
the Extraction Efficiency section. Data for 05 pg/mL spike is reported based on triplicate (n = 3) analysis. The rest of analyses were performed for n = 4 replicates.
"" nd, not detected.
Table II. Sample Drug Recovery Based on Three Extracted Ions Followed in a Full-Scan Monitoring Mode for Carisoprodol Fortified Serum*
Ion 261 Ion 200 Ion 176 Concentration
(pg/mt) %Rec. %RSD %Rec. %RSD %Rec. %RSD
0.5 44.5 1.5 72.7 3.9 50.1 5,6 I ,O 62.5 11 78.6 3.6 702 6,0 2,0 90.0 19 83.0 11 94.8 8.9 5,0 105 5.8 102 3.9 103 1.8
' Dala and analyqs w(,m pt,r)~*rmed as des~ ribed in L~ble I.
j 2.6 ~ A
0 . 6 0.4 0.2 0
i . . . . 1 . . . . J . . . . i . . . . . . . i . . . . ] . . . . J . . . .
0 1 2 3 4 5 6 7
xt04|
60 5O 4O 3O
2 0
t ~ .
Time {mln}
Figure 2. Chromatographic profiles for 10 pg/mL working standard mix of badofen and carisoprodol. The LC profile was developed at 254 nm by a gradient elution at 45~ (A) (see the Methods section). A UV peak for baclofen was observed at 2.6 min (absorbance of 0.8 units). Total ion spectrum of 10 pg/mL standard mix followed in positive APCI full-scan mode is shown in (B), Peaks 1 and 2 (with 3-rain separation) corre- spond to badofen and carisoprodol, respectively.
Journal of Analy t ica l Toxicology, Vol. 27, July/August 2003
the sample. The percent drug recovery with corresponding %RSD was determined for each serum sample fortified with both analytes at four different concentrations. Individual stan- dard calibration curves and quantitation were based on the peak areas of extracted ions. The data is summarized in Tables I and II.
1
Chromatography and mass spectra In order to determine elution profiles and mass spectral be-
havior of baclofen and carisoprodol, individual lO-pg/mL stan- dards were analyzed by LC-MS (data not shown).
x l 0 "
A 2
Extraction efficiency Extraction efficiency was expressed in terms of concentration
of the drug recovered versus initial concentration used to spike
Time (min) x l O 3
1 2 B
. . . . . . . . 1 '2 . . . . '3 . . . . '4 . . . . '5 . . . . '6 . . . . '7 . . . .
Time (min} Figure 3. Total ion mass spectral profiles of baclofen and carisoprodo[ in 0.5 pg/mL standard analyzed prior to microcon-30 treatment (A) and after filtration procedure (B). All results were obtained under identical con- ditions as described in the Methods section. Peaks 1 and 2 correspond to baclofen and carisoprodol, respectively.
278
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Journal of Analytical Toxicology, Vol. 27, July/August 2003
Chromatographic separation of 10 p~mL working standard mix of baclofen and carisoprodol and their total ion MS profile is shown in Figure 2. Baclofen elution resulted in maximal UV signal of 0.8 mAU, with no absorbance seen for carisoprodol (Figure 2, panel A). The corresponding total mass spectral ion chromatogram obtained for a mixture of two analytes at 10 IJg/mL collected in a full-scan monitoring mode of MS with pos- itive APCI (m/z range 150-400) is shown in panel B (Figure 2). The peaks for baclofen and carisoprodol were detected at 2.6 and
A
1130
= ,Q .~,m,
20 �84
m / z 2 1 8 ~ m / z 2 0 0 . . v ~ m / Z 176
Oi r iO , ~ ! I ill .
H,,N I O j"1~"l ~ O i " ~ N ~ ! " / ' H \
I ~ + ~ , ~ : 261
~ [ o
~ r l ,
m
I ' " "
2OO mlz
o .
r
�9 i
300
B
1 0 0 �84
80 �84
I:
es
OH
, m/z 196
m/z 179 [M+H~, m/z 214
=
. ~ 4 0
t H o l t L ~ '-i:- ' "! "~ ".~'"-i-" b. , .
200 300 m#z
Figure 4. Complete MS fragmentation data obtained for carisoprodol (A) and baclofen (B)in a full-scan monitoring mode. Both spectra were col- lected for 2 pglmL standard mix under identical conditions after mi- crocon-30 treatment (see the Methods section). Structures of daughter ions for each compound are shown in corresponding insets to (A) and (B). Peaks labeled by (*) are those that were routinely monitored. Summary of the ions observed for both analytes and their abundances are presented in Table III.
5.6 min, respectively, and were well resolved under the elution conditions (see the Methods section).
Prior to any sample analysis, all standards were treated with the microcon-30 filtration device in order to account for any changes in analyte behavior. A complete mass spectral ion pro- file of a 0.5 pg/mL working standard mix of baclofen and cariso- prodol obtained in a positive APCI MS full-scan mode before and after microcon-30 treatment is shown and compared in Figure 3. The standard analyzed prior to any filtration yielded two well-resolved peaks for baclofen and carisoprodol without any additional mass spectral response. A slightly different total ion chromatogram with slight loss of abundance in a carisoprodol peak was seen for the treated standard, minor additional peaks seemed to arise, but not overlap the analytes of interest as a re- sult of sample filtration procedure (Figure 3B). Thus, a com- plete fragmentation profile of both analytes present in a standard before (data not shown) and after microcon-30 treat- ment was obtained (Figure 4).
Table III. Summary of Fragmentation Ions' and their Abundances Observed for Baclofen and Carisoprodol
Baclofen Carisoprodol
Ion ( r e ~ z ) Abundance t Ion ( m / z ) Abundance
154.2 22 158.0 30 179,0 15 176.0 100 196.2 65 200.0 25 214.1 100 218.0 15 245.0 5 238.0 10 322.0 5 261.1 40
- - 285.0 5
"Fragmentation was performed by positive APCI-MS in a full-scan monitoring mode as described in the Methods section. Data presented is for 2 pg/mL working standard mix of baclofen and carisoprodol.
t. Relative abundance is reported for each ion.
xl~ MSD 214
' d . . . . . . . . . . ,.'A.JL. . . . . . . . . . . . . . . t 2 3 4 5 e
zl~ 4 IdSO116 i ;too IB
. . . . ; . . . . ~ . . . . ~ . . . . ~ . . . . , ~ ; ' ' -
. . . . ; . . . . ~ . . . . ; . . . . ~ . . . . ; ; ;
l ip I, II~ 200 211
-o T , , . . . . . . . . . . . . . . . . . . : . . . . . . . . . . . . . 1 2 ~ 4 s 6 7
o . , , . . . . �9 . . . . ; . . : , . - . : . . . .
Time (rain)
Figure 5. Total extracted ion current profile obtained for 0.5 pg/mL working standard mix of baclofen and carisoprodol via a positive APCI MS in a full-scan mode. Peaks for baclofen are labeled as IA (2.68 min) and I B (2.67 rain) with m/z 214 and 196, respectively. Peaks labeled as 2A-2C (elution time between 5.7 and 5.8 min) are for carisoprodol de- tection with m/z of 261,200, and 176, respectively.
279
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Different degrees of fragmentation were observed for baclofen and carisoprodol with a complete fragmentation pattern of both drugs presented in Figure 4. In each case the generation of the parental ions ([M+H] § was detected, with m/z 261.1 (40% abundance, panel A) and 214.1 (100% abundance, Panel B) for carisoprodol and baclofen, respectively. Additional fragmenta- tion of carisoprodol resulted in ions of m/z 218.0, 200.0, and 176.0 that could be interpreted as the loss of [NH2C=O], 43.04 amu with deprotonation, loss of [NH2COOH] protonated form (61.05 amu), and loss of [(CH3)2-CH-NH-C=O] with 85.1 ainu, from [M+H] + parent ion, respectively (inset of panel A, Figure 4). Fragmentation of baclofen using positive APCI-MS in a full- scan mode resulted in a loss of water ion with ra/z of 196.2 ([M+H-H20]) with abundance of 65% and a loss of chloride molecule, rn/z 179.0 ([M+H-CI]) and abundance of 15% (graph- ical representation in inset of panel B, Figure 4). A complete summary of carisoprodol and baclofen fragmentation ions and their relative abundances is reported in Table III. For identifi- cation, ions at m/z 214.1 and 196.2 were followed for baclofen and ions with m/z of 261.1, 200.0, and 176.0 were those of carisoprodol (Figure 4). The m/z 238 ion appearing in the frag- mentation pattern of carisoprodol was determined to be struc- turally nonspecific (Figure 4A) resulting only after microcon-30 treatment of the standards and was omitted from use in analyte identification.
Calibrations curves and precision In order to avoid any significant drawback of acquiring data
across a wide mass range (m/z 150-400) and to make direct comparison between standards and sample spikes, calibrations curves were constructed for each analyte based on extracted current ion profiles of four microcon-30 pretreated standards in a low range of 0.1-5.0 IJg/mL. Extracted ion current profiles
, 1 0 4
3~I ;i A 3ot/I 251 '!
• 4
4 5
25
20
15
10
5
3 4 5 6 7
B
1 2
" . . . . 4 5 6
Time (min) Figure 6. Typical mass spectral profile for a drug-free bovine serum after sample treatment procedure is shown in (A). No peaks were observed be- tween 2.6 and 8�9 min. Total ion current chromatogram for a 2-pg/mL fortified serum sample is shown in (B). Peaks observed for baclofen and carisoprodol are labeled 1 and 2, respectively.
Journal of Analytical Toxicology, Vol. 27, July/August 2003
used in analyte identification for 0.5 pg/mL standard mix are shown in Figure 5. The abundance of detected peaks (m/z 214 and 196 for baclofen and 261,200, and 176 for carisorpodol) were at least 3 times that of the signal-to-noise ratio (instru- ment background detection) with the same retention times and 3 min separation observed in total mass spectrum.
xtO = MSO214 j / ~ A
1 2 3 4 5 6 7
] MSD 196 , I
2 0 0 . . . . I . . . . I . . . . I . . . . I . . . . I . . . . I . . . . I . . . .
1 2 3 4 5 6 7
] MSD 261 i
0 . . . . I . . . . I . . . . I . . . . ~ . . . . I . . . . I . . . . I . . . .
1 2 3 4 5 6 7
100 MSD 200
1 2 3 4 5 6 7
5001 MSD 176
0 . . . . J 4 5
Time (min) 7
x 102 MSD 214 IA B
1 2 3 4 5 6 7
IB
1 2 3 4 5 6 7
�9 MSD 261 2A
'~176 L 0~-T~'~ ' - i ' I . . . . I . . . . [ . . . . L ' ' ' "1 ' I . . . . I r ~ - -
1 2 3 4 5 6 7
2B 100~ MSD 200
~ - - ~ - ; ' ~ ' I . . . . 1 . . . . I . . . . I . . . . i . . . . i . . . .
1 2 3 4 5 6 7
001 MSD 176 ~ 2C
1 2 3 4 5 6 7 T ime (min)
Figure 7. Extracted ion current profiles obtained for a drug-free (A) and 2 pg/mL baclofen- and carisoprodol-fortified serum (B) samples. No ions of m/z for baclofen (2.6 min) and carisoprodol (5.6 min) were ob- sewed for the control sample as shown by arrows in (A). Ions for baclofen with m/z of 214 and 196 (1A-1 B) and carisoprodol with m/z 261,200, and 176 (2A-2C) were seen for a spiked sample (B).
280
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Journal of Analytical Toxicology, Vol. 27, July/August 2003
The linearity of response in 0.1-5.0-~g/mL concentration ranges for each analyte suggested that analysis of fortified sam- ples could be accomplished with satisfactory intraday preci- sion (repeatability) and interday precision (reproducibility). A plot of each extracted current ion peak area versus concentra- tion was determined in triplicate, resulted in linear curves with correlation coefficients (R 2) greater than 0.993 for baclofen and than 0.998 for carisoprodol. The data indicated that detec- tion was linear up to the highest fortified serum concentration analyzed, 5.0 IJg/mL.
Detection of baclofen and carisoprodol in fortified serum samples
A midlevel standard (1 IJg/mL) was injected prior to each sample analysis in order to demonstrate that the system was stable. The initial retention time window and relative ion in- tensities were checked. Negative control serum sample treated through the amicon-30 system (see the Methods section) was assayed by positive APCI-MS in a full-scan mode prior to each sample fortification. Total mass spectral ion chromatogram for a negative serum is shown in Figure 6A. The drug-free sample produced no response for any characteristic ions of baclofen and carisoprodol at their corresponding retention times. The drug- free serum was spiked at four different concentrations of a stan- dard mix of baclofen and carisoprodol (5.0, 2.0, 1.0, and 0.5 IJg/mL) and repeated at least in triplicate analysis. Figure 6B shows a complete mass spectral chromatogram of a drug-free serum spiked at a 2 ~g/mL and subjected to the sample purifi- cation procedure. The absence of matrix interferences at the re- tention times of analytes of interest and clean peak resolution suggest that sufficient sample purification was achieved. Mass spectral peak behavior and elution profile of baclofen and cariso- prodol in the fortified sample when compared with a control serum demonstrates the specificity of the method. A mass spec- tral fragmentation pattern for a peak eluted at 2.4 min in a drug-free serum yielded m/z of 166.2 as the primary ion (data not shown). None of the characteristic ions for baclofen or carisoprodol were seen.
Extracted ion current profiles for all ions used in identifica- tion of both drugs were determined and compared for a drug- free and fortified serum samples. Extracted ion current profiles for a negative serum shown in Figure 7A confirmed that no characteristic peaks of either analyte at their elution times and m/z values were observed. Figure 7B corresponds to the ex- tracted current ion profiles of a 2-~g/mL fortified serum sample. The chromatograms demonstrate that the peak behavior and elution pattern are the same as compared with the standard working mixture (Figure 5).
Analyte recovery, rOD, and LOQ Sample percent recovery and %RSD based on extracted ion
current profiles were determined for a range of sample fortifi- cation concentrations, 0.5-5.0 IJg/mL, and results are summa- rized in Tables I and II. Peaks at rn/z 214 and 196 for baclofen in a 1-1Jg/mL fortified sample and peaks at rn/z 261,200, and 176 for carisoprodol in a 0.5-~g/mL spiked sample were inte- grated and quantitated based on individual calibration curves and compared with the initial concentrations of fortified sam-
pies. Sample percent recovery fell into a range of 62-93% for ba- clofen (%RSD of 2.1-7.7) and 62-79% for carisoprodol (%RSD of 3.6-11). Fortification of drug-free serum with 0.5 I~g/mL of baclofen resulted in 75.5% recovery atrn/z 214 (n = 3, %RSD of 6.31) with no peaks observed at m/z 196.
Response of a single quantitation ion expressed in concen- tration units is frequently used to determine the LOD. However, the possibility of single ion detection below the concentration at which the method can be used to adequately identify the drug was considered. Thus, LOD in this report is defined as the lowest analyte concentration at which at least two characteristic ions are present in fortified serum sample at a signal-to-noise ratio greater than 3. The values of LODs were determined to be 1 IJg/mL (n = 4) and 0.5 pg/mL (n = 3) for baclofen and cariso- prodol, respectively. LOQ was based on data showing results within + 25% sample recovery of the target concentration for at least two ions used in analyte identification. Thus, LOQ of 2 ~g/mL was determined for both drugs under full-scan moni- toring mode of MS (n = 4, Tables I and II).
Discussion
Skeletal muscle relaxants have different modes of action within the central or peripheral nervous systems, which result in their pharmacologic and toxicologic effects. Unfortunately, adverse reactions to pharmacologic doses or clinical signs fol- lowing intoxication are not sufficiently unique to distinguish ex- posure to a specific relaxant. In addition, there are substantial differences in the pharmacokinetics of the various relaxants. Thus, there is a need for a simple and rapid analytical screening procedure to detect these compounds in various fluid, tissue, and gastrointestinal samples at both pharmacologically and toxicologically significant concentrations.
In the present study, a fast analytical approach for the simul- taneous extraction and quantitative screening of baclofen and carisoprodol was developed without tedious chromatographic separation and SPE. LC-MS with the soft ionization technique of positive APCI produced molecular ions without recourse to HPLC separation allowing identification of individual compo- nents of the mixture. The quantitative and qualitative analysis of all concentrations used (0.1-50 I~g/mL) was based on at least two characteristic extracted current ion profiles for each com- pound detected under positive APCI-MS.
Running an analysis in full-scan monitoring mode is known to produce less sensitive LODs as compared with the same de- tection performed under selected ion-monitoring (SIM) mode of MS. However, to gain a better understanding in behavior of baclofen and carisoprodol under present study conditions, a complete report was done in a full-scan monitoring mode of MS. Internal standards were not used in this initial study in view of the reproducibility of the method and the ability to detect both drugs at their therapeutic ranges. Sensitivity and detection in scan mode (range ofrn/z 150-400) was sufficient for reliable identification of baclofen and carisoprodol at the lower thera- peutic range. The ability to base the analysis on at least two ex- tracted ions for both drugs will allow for later studies to be run
281
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021
under SIM mode, lowering LODs, and producing more accurate results.
Therapeutic doses of baclofen result in blood concentrations of 0.08-0.40 ]Jg/mL (2). In a fatal human overdose, a concen- tration of 17 ]Jg/mL was detected (1). Pharmacokinetic studies report that at blood concentrations of 10-300 tJg/mL baclofen, approximately 30% of total drug can be bound to serum pro- teins (2). If serum albumin (66 kDa) is involved in binding of baclofen, then the sample purification method described in this study would lead to loss of protein-bound drug. The loss of some fraction of the analyte should be considered when ana- lyzing serum samples in baclofen ingestion cases. However, re- coveries reported in this study are not affected because only free drug was present for detection in fortified serum samples.
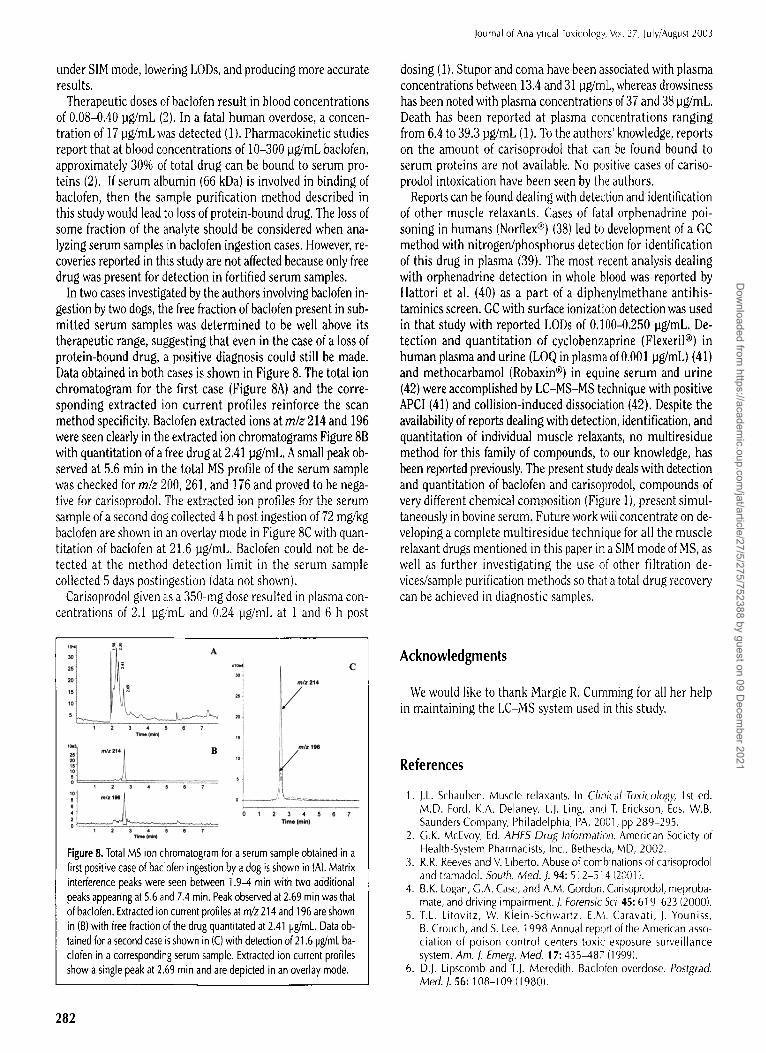
In two cases investigated by the authors involving baclofen in- gestion by two dogs, the free fraction of baclofen present in sub- mitted serum samples was determined to be well above its therapeutic range, suggesting that even in the case of a loss of protein-bound drug, a positive diagnosis could still be made. Data obtained in both cases is shown in Figure 8. The total ion chromatogram for the first case (Figure 8A) and the corre- sponding extracted ion current profiles reinforce the scan method specificity. Baclofen extracted ions at m/z 214 and 196 were seen clearly in the extracted ion chromatograms Figure 8B with quantitation of a free drug at 2.41 llg/mL. A small peak ob- served at 5.6 min in the total MS profile of the serum sample was checked for m/z 200, 261, and 176 and proved to be nega- tive for carisoprodol. The extracted ion profiles for the serum sample of a second dog collected 4 h post ingestion of 72 mg/kg baclofen are shown in an overlay mode in Figure 8C with quan- titation of baclofen at 21.6 tJg/mL. Baclofen could not be de- tected at the method detection limit in the serum sample collected 5 days postingestion (data not shown).
Carisoprodol given as a 350-mg dose resulted in plasma con- centrations of 2.1 IJg/mL and 0.24 IJg/mL at 1 and 6 h post
71 ;'t :: /t
1 2 a 4 s e 7
is il
1 2 ~ 4 ~ 8 7
;] ..... 1
]oJ
mlz 214
m/It 196 io., /
I
1 2 3 4 5 6 7 Time (mln)
Figure 8. Total MS ion chromatogram for a serum sample obtained in a first positive case of baclofen ingestion by a dog is shown in (A), Matrix interference peaks were seen between 1.9-4 rain with two additional peaks appearing at 5.6 and 7.4 min. Peak observed at 2.69 min was that of baclofen. Extracted ion current profiles at m/z 214 and 196 are shown in (B) with free fraction of the drug quantitated at 2.41 pg/mL. Data ob- tained for a second case is shown in (C) with detection of 21.6 pg/mL ba- clofen in a corresponding serum sample. Extracted ion current profiles show a single peak at 2.69 min and are depicted in an overlay mode.
282
Journal of Analytical Toxicology, Vol. 27, July/August 2003
dosing (1). Stupor and coma have been associated with plasma concentrations between 13.4 and 31 IJg/mL, whereas drowsiness has been noted with plasma concentrations of 37 and 38 tJg/mL. Death has been reported at plasma concentrations ranging from 6.4 to 39.3 lJg/mL (1). To the authors' knowledge, reports on the amount of carisoprodo[ that can be found bound to serum proteins are not available. No positive cases of cariso- prodol intoxication have been seen by the authors.
Reports can be found dealing with detection and identification of other muscle relaxants. Cases of fatal orphenadrine poi- soning in humans (Norfiex | (38) led to development of a GC method with nitrogen/phosphorus detection for identification of this drug in plasma (39). The most recent analysis dealing with orphenadrine detection in whole blood was reported by Hattori et al. (40) as a part of a diphenylmethane antihis- taminics screen. GC with surface ionization detection was used in that study with reported LODs of 0.100-0.250 1Jg/mL. De- tection and quantitation of cyclobenzaprine (Flexeril | in human plasma and urine (LOQ in plasma of 0.001 IJg/mL) (41) and methocarbamol (Robaxin | in equine serum and urine (42) were accomplished by LC-MS-MS technique with positive APCI (41) and collision-induced dissociation (42). Despite the availability of reports dealing with detection, identification, and quantitation of individual muscle relaxants, no multiresidue method for this family of compounds, to our knowledge, has been reported previously. The present study deals with detection and quantitation of baclofen and carisoprodol, compounds of very different chemical composition (Figure 1), present simul- taneously in bovine serum. Future work will concentrate on de- veloping a complete multiresidue technique for all the muscle relaxant drugs mentioned in this paper in a SIM mode of MS, as well as further investigating the use of other filtration de- vices/sample purification methods so that a total drug recovery can be achieved in diagnostic samples.
Acknowledgments
We would like to thank Margie R. Cumming for all her help in maintaining the LC-MS system used in this study.
References
1. I.L. Schauben. Muscle relaxants. In Clinical Toxicology, 1st ed. M.D. Ford, K.A. Delaney, L.J. Ling, and T. Erickson, Eds. W.B. Saunders Company, Philadelphia, PA, 2001, pp 289-295.
2. G.K. McEvoy, Ed. AHFS Drug Inforn~ation. American Society of Health-System Pharmacists, Inc., Bethesda, MD, 2002.
3. R.R. Reeves and V. Liberto. Abuse of combinations of carisoprodol and tramadol. South. Med. J. 94:572-514 {20(11 ).
4. B.K. Logan, G.A. Case, and A.M Gordon. Carisoprodol, meproba- mate, and driving impairment. J. Forensic Sci. 45:619-623 (2000).
5. T.L. Litovitz, W. Klein-Schwartz, E.M. Caravati, J. Youniss, B. Crouch, and S. Lee. 1998 Annual report of the American asso- ciation of poison control centers toxic exposure surveillance system. Am. J. Emerg. Med. ] 7:435~.87 (1999).
6. D.J. Lipscomb and T.J. Meredith. Baclofen overdose. Postgrad. Med. J. 56:108-109 (]980).
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021

Journal of Analytical Toxicology, Vol. 27, July/August 2003
7. S. Nugent, M.D. Katz, and T.E. Little. Baclofen overdose with car- diac conduction abnormalities: case report and review of the lit- erature. J. Toxicol. Clin. Toxicol. 24:321-328 (1986}.
8. A.D. Fraser, W. MacNeil, and A.F. Isner. Toxicological analysis of a fatal baclofen (Lioresal) ingestion. J. Forensic Sci. 36:1596-1602 (1991).
9. T.H. Lee, S.S. Chen, S.L. Su, and S.S. Yang. Baclofen intoxication: report of four cases and review of the literature. Clin. Neuropharm. 15:56-62 (1992).
10. R.J. Roberge, T.G. Martin, M. Hodgman, J.G. Benitez, and J.E. Brunswick. Supraventricular tachyarrhythmia associated with baclofen overdose. J. Toxicol. Clin. Toxicol. 32:291-297 (1994).
11. D.E. Cooke and M.A. Glasstone. Baclofen poisoning in children. Vet. Hum. Toxicol. 36:448-450 (1994).
12. A. Campbell and M. Chapman. Handbook of Poisoning in Dogs and Cats, 1st ed., Blackwell Science Ltd., Oxford, U.K., 2000.
13. D.V. Hecht and K. Allenspach. Presumptive baclofen intoxication in a dog. J. Vet. Emerg. Critical Care. 8:49-54 (1998).
14. R. CahilI-Morasco, K. Moulin, and D.V. Hecht. Successful treat- ment of baclofen (Lioresal) overdose in a dog. In 2001 North American Congress of Clinical Toxicology. Marcel Dekker, Inc., Montreal, Quebec, Canada, 2001, p 504.
15. R.H. Poppenga, I. Rudik, W. Herndon, and T. Melgarejo. Baclofen intoxication in a Norwich Terrier puppy. In American Association of Veterinary Laboratory Diagnosticians, Hershey, PA, 2001, p 46.
16. W.K. Rumbeiha, W.E. Braselton, and A. Caceres. Baclofen toxicosis in a dog: death by pharmacist. In American Association of Veteri- nary Laboratory Diagnosticians, Hershey, PA, 2001, p 48.
17. E.W. Wuis, R.J. Dirks, T.B. Vree, and E. Van Der Kleyn. High-per- formance liquid chromatographic analysis of baclofen in plasma and urine of man after precolumn extraction and derivatization with o-phthaldialdehyde. J. Chromatogr. 337:341-350 (1985).
18. S. Tosunoglu and L. Ersoy. Determination of baclofen in human plasma and urine by high-performance liquid chromatography with fluorescence detection. Analyst. 120:373-375 (1995).
19. E.W. Wuis, L.E.C. Van Beijsterveldt, R.J.M. Dirks, T. B. Vree, and E. Van Der Kleyn. Rapid simultaneous determination of baclofen and its 7-hydroxy metabolite in urine by high-performance liquid chromatography with ultraviolet detection. ]. Chromatogr. 420: 212-216 (1987).
20. H. Spahn, D. Kraub, and E. Mutschler. Enantiospecific high-per- formance liquid chromatographic (HPLC) determination of ba- clofen and its fluoro analogue in biological material. Pharmac. Res. 5:107-112 (1988).
21. A.M. Rustum. Simple and rapid reversed-phase high-performance liquid chromatographic determination of baclofen in human plasma with ultraviolet detection. J. Chromatogr. 487" 107-115 (1989).
22. L. Millerioux, M. Brault, V. Gualano, and A. Mignot. High-perfor- mance liquid chromatographic determination of baclofen in human plasma. J. Chromatogr. A 729:309-314 (1996).
23. G.M. Wall and J.K. Baker. Determination of baclofen and alpha-ba- clofen in rat liver homogenate and human urine using solid-phase extraction, o-phthalaldehyde-tert-butyl thiol derivatization and high-performance liquid chromatography with amperometric de- tection. J. Chromatogr. 491:151-162 (1989).
24. G. Kochak and F. Honc. Improved gas-liquid chromatographic method for the determination of baclofen in plasma and urine. J. Chromatogr. 310:319-326 (1984).
25. A. Sioufi, G. Kaiser, F. Leroux, and J. P. Dubois. Determination of the S(+)- and R(-)-enantiomers of baclofen in plasma and urine by gas chromatography using a chirat fused-silica capillary column and an electron-capture detector. J. Chromatogr. 450:221-232 (1988).
26. C.-G. Swahn, H. Beving, and G. Sedvall. Mass fragmentographic determination of 4-amino-3-p-chlorophenylbutyric acid (baclofen) in cerebrospinal fluid and serum. J. Chrornatogr. 162:433-438 (1979).
27. M.-T. Chiang, S. Y. Chang, and C.-W. Whang. Analysis of ba- clofen by capillary electrophoresis with laser-induced fluores- cence detection. J. Chromatogr. A 877:233-237 (2000).
28. M.-T. Chiang, S. Y. Chang, and C.-W. Whang. Chiral analysis of ba- clofen by 0~-cyclodextrin-modified capillary electrophoresis and laser-induced fluorescence detection. Electrophoresis 22:123-127 (2001).
29. L. Ersoy. A spectrophotometric method for the determination of ba- clofen. Pharmazie. 40" 903-904 (1985).
30. R.P. Weatherby, R.D. Allan, and G. A. Johnston. Resolution of the stereoisomers of baclofen by high performance liquid chromatog- raphy. J. Neurosci. Meth. 10:23-28 (1984).
31. I.L. Honigberg, J.T. Stewart, and M. Smith. Liquid chromatography in pharmaceutical analysis IX: determination of muscle relaxant- analgesic mixtures using normal phase chromatography. J. Pharm. ScL 67:675-679 (1978).
32. R Kintz, R Mangin, A.A. Lugnier, and A.J. Chaumont. A rapid and sensitive gas chromatographic analysis of meprobamate or cariso- prodol in urine and plasma. J. Anal. ToxicoL 12:73-74 (1988).
33. R.A. Littrell, L.R. Haynes, and V. Stillner. Carisoprodol (Soma): a new and cautious perspective on an old agent. South MedJ. 86: 753-756 (1993).
34. M. Careri, A. Mangia, and M. Musci. Applications of liquid chro- matography-mass spectrometry interfacing systems in food anal- ysis: pesticide, drug and toxic substance residues. J. Chromatogr. A 727:153-184 (1996).
35. H.H. Maurer. Liquid chromatography-mass spectrometry in forensic and clinical toxicology. J. Chromatogr. B 713:3-25 (1998).
36. R Marquet and G. Lachatre. Liquid chromatography-mass spec- trometry: potential in forensic and clinical toxicology. J. Chro- matogr. B 733:93-118 (1999).
37. M. Flardh, and B.-M. Jacobson. Sensitive method for the determi- nation of baclofen in plasma by means of solid-phase extraction and liquid chromatography-tandem mass spectrometry. J. Chro- matogr. A 846:169-173 (1999).
38. A.E. Robinson, A.T. Holder, R.D. McDowall, R. Powell, and H. Sattar. Forensic toxicology of some orphenadrine-related deaths. Forensic Sci. Int. 9:53-62 (I 977).
39. M. Contin, R. Riva, F. Albani, and A. Baruzzi. Simple and rapid GLC method for the determination of orphenadrine in human plasma. Biomed. Chromatogr. 2:193-194 (1987).
40. H. Hattori, S. Yamamoto, M. lwata, E. Takashima, T. Yamada, and O. Suzuki. Determination of diphenylmethane antihistaminic drugs and their analogues in body fluids by gas chromatography with sur- face ionization detection. J. Chromatogr. 581:213-218 (I 992).
41. M. Constanzer, C. Chavez, and B. Matuszewski. Development and comparison of high-performance liquid chromatography methods with tandem mass spectrometric and ultraviolet ab- sorbance detection for the determination of cyclobenzaprine in human plasma and urine. J. Chromatogr. B 666:117-I 26 (I 995).
42. R.M. Koupai-Abyazani, B. Esaw, and B. Laviolette. Determina- tion of methocarbamol in equine serum and urine by high-perfor- mance liquid chromatography with ultraviolet detection and atmospheric pressure ionization-mass spectrometric confirmation. J. Anal. Toxicol. 21:301-305 (I 997).
Manuscript received June I0, 2002; revision received November 15, 2002.
283
Dow
nloaded from https://academ
ic.oup.com/jat/article/27/5/275/752388 by guest on 09 D
ecember 2021


















