Dimethyl Fumarate, an Immune Modulator and Inducer of the ...
12
of March 19, 2018. This information is current as Novel Candidate for HIV Neuroprotection Macrophage-Mediated Neurotoxicity: A Suppresses HIV Replication and and Inducer of the Antioxidant Response, Dimethyl Fumarate, an Immune Modulator Kelly L. Jordan-Sciutto and Dennis L. Kolson Patricia J. Vance, Lorraine L. Kolson, Bethany J. Wong, Stephanie A. Cross, Denise R. Cook, Anthony W. S. Chi, ol.1101868 http://www.jimmunol.org/content/early/2011/10/04/jimmun published online 5 October 2011 J Immunol Material Supplementary 8.DC1 http://www.jimmunol.org/content/suppl/2011/10/05/jimmunol.110186 average * 4 weeks from acceptance to publication Fast Publication! • Every submission reviewed by practicing scientists No Triage! • from submission to initial decision Rapid Reviews! 30 days* • Submit online. ? The JI Why Subscription http://jimmunol.org/subscription is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/About/Publications/JI/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/alerts Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved. Copyright © 2011 by The American Association of 1451 Rockville Pike, Suite 650, Rockville, MD 20852 The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology by guest on March 19, 2018 http://www.jimmunol.org/ Downloaded from by guest on March 19, 2018 http://www.jimmunol.org/ Downloaded from
Transcript of Dimethyl Fumarate, an Immune Modulator and Inducer of the ...

of March 19, 2018.This information is current as Novel Candidate for HIV Neuroprotection
Macrophage-Mediated Neurotoxicity: A Suppresses HIV Replication andand Inducer of the Antioxidant Response, Dimethyl Fumarate, an Immune Modulator
Kelly L. Jordan-Sciutto and Dennis L. KolsonPatricia J. Vance, Lorraine L. Kolson, Bethany J. Wong, Stephanie A. Cross, Denise R. Cook, Anthony W. S. Chi,
ol.1101868http://www.jimmunol.org/content/early/2011/10/04/jimmun
published online 5 October 2011J Immunol
MaterialSupplementary
8.DC1http://www.jimmunol.org/content/suppl/2011/10/05/jimmunol.110186
average*
4 weeks from acceptance to publicationFast Publication! •
Every submission reviewed by practicing scientistsNo Triage! •
from submission to initial decisionRapid Reviews! 30 days* •
Submit online. ?The JIWhy
Subscriptionhttp://jimmunol.org/subscription
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/About/Publications/JI/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/alertsReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved.Copyright © 2011 by The American Association of1451 Rockville Pike, Suite 650, Rockville, MD 20852The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

The Journal of Immunology
Dimethyl Fumarate, an Immune Modulator and Inducer ofthe Antioxidant Response, Suppresses HIV Replication andMacrophage-Mediated Neurotoxicity: A Novel Candidate forHIV Neuroprotection
Stephanie A. Cross,* Denise R. Cook,* Anthony W. S. Chi,* Patricia J. Vance,*
Lorraine L. Kolson,* Bethany J. Wong,* Kelly L. Jordan-Sciutto,† and Dennis L. Kolson*
Despite antiretroviral therapy (ART), HIV infection promotes cognitive dysfunction and neurodegeneration through persistent
inflammation and neurotoxin release from infected and/or activated macrophages/microglia. Furthermore, inflammation and im-
mune activation within both the CNS and periphery correlate with disease progression and morbidity in ART-treated individuals.
Accordingly, drugs targeting these pathological processes in the CNS and systemic compartments are needed for effective, adjunc-
tive therapy. Using our in vitro model of HIV-mediated neurotoxicity, in which HIV-infectedmonocyte-derivedmacrophages release
excitatory neurotoxins, we show that HIV infection dysregulates the macrophage antioxidant response and reduces levels of heme
oxygenase-1 (HO-1). Furthermore, restoration of HO-1 expression in HIV-infected monocyte-derived macrophages reduces neu-
rotoxin release without altering HIV replication. Given these novel observations, we have identified dimethyl fumarate (DMF), used
to treat psoriasis and showing promising results in clinical trials for multiple sclerosis, as a potential neuroprotectant and HIV
disease-modifying agent. DMF, an immune modulator and inducer of the antioxidant response, suppresses HIV replication and
neurotoxin release. Two distinct mechanisms are proposed: inhibition of NF-kB nuclear translocation and signaling, which could
contribute to the suppression of HIV replication, and induction of HO-1, which is associated with decreased neurotoxin release.
Finally, we found that DMF attenuates CCL2-induced monocyte chemotaxis, suggesting that DMF could decrease recruitment of
activated monocytes to the CNS in response to inflammatory mediators. We propose that dysregulation of the antioxidant response
during HIV infection drives macrophage-mediated neurotoxicity and that DMF could serve as an adjunctive neuroprotectant and
HIV disease modifier in ART-treated individuals. The Journal of Immunology, 2011, 187: 000–000.
Human immunodeficiency virus-1 infection of the CNScan result in cognitive, motor, and behavioral abnor-malities, collectively known as HIV-associated neu-
rocognitive disorders (HAND) (1, 2). Early in the course ofinfection, HIV traffics into the brain via infected monocytes andlymphocytes (3) and, despite antiretroviral therapy (ART), persistsin parenchymal microglia and perivascular macrophages (4–6).HIV infection of the CNS results in the immune activation ofresident glia and because HIV cannot infect neurons, neuronal
damage is mediated by neurotoxins released by these infectedand/or activated macrophages, microglia, and astrocytes. Althoughthe severity of HAND has been significantly reduced through thewidespread use of ART, the prevalence and associated morbidityremain high (∼50%) (7, 8). The persistence of HAND in indi-viduals effectively controlled for systemic viral load is incom-pletely explained, although recent evidence suggests that pro-longed inflammation in both the CNS and periphery may beresponsible (9–11).Chronic systemic inflammation is tightly linked to morbidity and
mortality in ART-treated patients, which suggests that adjunctiveanti-inflammatory drugs or immune modulators may improve cli-nical outcomes. Despite undetectable plasma viral loads, measuresof systemic inflammation correlate to cerebral spinal fluid (CSF)immune activation, CNS inflammation, and HAND (9–11). It hasbeen proposed that elevated peripheral inflammation mediatesneurocognitive decline by increasing the transendothelial migra-tion of infected and/or activated monocytes into the brain (10, 12).An increased number of microglia and macrophages in the CNScorrelates with the severity of premortem HAND, demonstratingthe importance of these cell types in mediating neurologic im-pairment (4, 13, 14). Some of the most striking evidence linkingperipheral inflammation to HAND derives from the strong asso-ciation between early and persistent damage caused to GALT byHIV infection (or SIV infection in macaques), increased microbialtranslocation, systemic immune/monocyte activation, and HANDprogression (9, 10, 15, 16). Therefore, reducing inflammation inthe periphery as well as within the CNS is expected to improveneurocognitive impairment in HIV-infected patients.
*Department of Neurology, Perelman School of Medicine, University of Pennsylva-nia, Philadelphia, PA 19104; and †Department of Pathology, School of Dental Med-icine, University of Pennsylvania, Philadelphia, PA 19104
Received for publication June 23, 2011. Accepted for publication September 6, 2011.
This work was supported by National Institutes of Health R01 Grant NS-043994 (toD.L.K.), P50 Grant NS-27405 (subproject Principal Investigator, D.L.K.), and T32Grant AG-000255 (to S.A.C.).
Address correspondence and reprint requests to Dr. Dennis Kolson, Department ofNeurology, University of Pennsylvania, 280C Clinical Research Building, 415 CurieBoulevard, Philadelphia, PA 19104. E-mail address: [email protected]
The online version of this article contains supplemental material.
Abbreviations used in this article: ARE, antioxidant response element; ART, antire-troviral therapy; CoPP, cobalt (III) protoporphyrin IX chloride; CSF, cerebral spinalfluid; DMF, dimethyl fumarate; EFZ, efavirenz; GPX1, glutathione peroxidase 1;HAND, HIV-associated neurocognitive disorders; HO-1, heme oxygenase 1; Keap1,Kelch-like ECH-associated protein 1; LDH, lactate dehydrogenase; LTR, long ter-minal repeat; MAP2, microtubule-associated protein 2; MDM, monocyte-derivedmacrophage; MMF, monomethyl fumarate; NMDAR, N-methyl-D-aspartate receptor;NQO1, NAD(P)H quinone oxidoreductase 1; Nrf2, NF E2-related factor 2; PKC,protein kinase C; ROS, reactive oxygen species; RT, reverse transcriptase; SnMP, tin(IV) mesoporphyrin IX dichloride.
Copyright� 2011 by The American Association of Immunologists, Inc. 0022-1767/11/$16.00
www.jimmunol.org/cgi/doi/10.4049/jimmunol.1101868
Published October 5, 2011, doi:10.4049/jimmunol.1101868 by guest on M
arch 19, 2018http://w
ww
.jimm
unol.org/D
ownloaded from

Fumaric acid esters, including dimethyl fumarate (DMF) andits 1primary in vivo metabolite monomethyl fumarate (MMF), area class of compounds that have anti-inflammatory and immune-modulating effects in vitro and in vivo. Fumaderm, a formula-tion of DMF and other fumaric acid esters, has been used in Europesince 1995 as an effective treatment for psoriasis; its mechanism ofaction is attributed to modulation of T cell activation and infiltra-tion into plaques (17). DMF is currently under investigation foruse in multiple sclerosis and a recently completed phase III studydemonstrated a significant benefit in suppressing relapses, diseaseprogression, and brain lesion inflammation (18). Using the rodentmodel of multiple sclerosis, experimental allergic encephalomy-elitis (EAE), it was shown that DMF reduces the recruitment ofmonocytes into areas of active demyelination in the brain (19). Inin vitro model systems, DMF has been shown to inhibit proin-flammatory cytokine production and NF-kB signaling via inhibi-tion of nuclear translocation (19–22). Furthermore, DMF inducesthe expression of NF E2-related factor 2 (Nrf2)-driven antioxidantresponse genes, including heme oxygenase-1 (HO-1) and NAD(P)Hquinone oxidoreductase 1 (NQO1) (23, 24). Notably, induction ofHO-1 expression in human monocytes by hemin has been asso-ciated with suppression of HIV-1 replication (25).Because HIV replication can be strongly driven by NF-kB ac-
tivation and nuclear translocation, we hypothesized that DMFtreatment of HIV-infected monocyte-derived macrophages (HIV/MDM) would result in attenuation of HIV replication, immuneactivation, and neurotoxin production. Our in vitro system modelsmacrophage-mediated neurotoxicity during HIV infection by us-ing human MDM and rat cerebrocortical neuronal cultures. In thissystem, HIV infection of MDM results in the release of low m.w.excitotoxins that injure neurons through excessive activation of N-methyl-D-aspartate receptors (NMDAR) (26–28). In this study, wedemonstrate that DMF attenuates HIV replication, nuclear trans-location of NF-kB subunits, and TNF-a production in humanMDM. Furthermore, supernatants from DMF- and MMF-treatedHIV/MDM cultures are markedly less neurotoxic to primary neu-rons than those from nontreated HIV/MDM cultures. Suppres-sion of neurotoxin production is mediated by induction of HO-1in HIV/MDM and this suppression of neurotoxin production canoccur even without suppression of HIV replication. Finally, DMFand MMF also reduce CCL2-induced chemotaxis in human mono-cytes. This study demonstrates that DMF inhibits key steps inHAND pathogenesis through distinct effects on HIV replicationand macrophage-mediated neurotoxin production and DMF shouldbe considered as an adjunctive therapeutic for ameliorating theneurologic complications of HIV infection.
Materials and MethodsReagents
Stock solutions of DMF and MMF (Sigma-Aldrich, St. Louis, MO) wereprepared in DMSO and stored at 220˚C until use. Tin (IV) mesoporphyrinIX dichloride (SnMP) and cobalt (III) protoporphyrin IX chloride (CoPP;Frontier Scientific, Logan, UT) were prepared in 1 N NaOH and stored at220˚C until use. Stock solutions of Ara-C (Sigma-Aldrich), PHA (Sigma-Aldrich), TNF-a (R&D Systems, Minneapolis, MN), and CCL2 (Pepro-Tech, Rocky Hill, NJ) were prepared in filter-sterilized distilled water andstored at 220˚C. Stock solutions of efavirenz (EFZ; National Institutes ofHealth [NIH] AIDS Research and Reference Reagent Program, German-town, MD) were prepared in DMSO and frozen at 280˚C until use.
Isolation and culture of human monocyte-derived macrophages
All human studies were reviewed and approved by the Institutional ReviewBoard at the University of Pennsylvania. Human monocytes were preparedfrom PBMCs of healthy donors and isolated by Ficoll density gradientcentrifugation as previously described (26, 29). Monocytes were plated at1 3 106 cells/well to Cell-Bind six-well plates (Corning, Lowell, MA) and
cultured in DMEM supplemented with 10% FBS, 10% horse serum, and1% nonessential amino acids with 50 U/ml penicillin/streptomycin at 37˚C,6% CO2. Cells were cultured for 7 to 8 d and visually inspected for MDMdifferentiation before use in HIV-infection experiments. MDM were cul-tured for 7–10 d before use in noninfectious experiments.
HIV infection of MDM
Prior to infection, MDM were treated with EFZ (5 or 20 nM), MMF, and/orDMF (1–100 mM), as indicated, for 1 h. All wells were normalized for thevehicles appropriate for drug treatments (DMSO and/or NaOH). Differen-tiated MDM were exposed to 50 ng (p24 ELISA, equivalent to 1.82 60.22 kcpm/ml by reverse transcriptase [RT] activity assay) of HIV-1 Jago (R5strain) or 89.6 (R5/X4 strain) for 24 h. HIV-Jago is a macrophage-tropic CSFisolate from a patient with confirmed HIV-associated dementia (29). Virusstocks were prepared by the University of Pennsylvania Center for AIDSResearch Virology Core. Supernatants from HIV-infected or noninfected(mock) MDM were collected every 2–4 d and stored at280˚C. Supernatantswere monitored for HIV replication by quantifying viral RT activity, asanalyzed by the amount of radiolabeled deoxythymidine incorporation.
Subcellular fractionations and Western blot analysis
For whole-cell lysate collection, cells were rinsed twice with ice-cold PBS,lysed in 75 mM Tris-HCl (pH 6.8), 15% glycerol, 3.75 mM EDTA, and 3%SDS, and supplemented with Complete Protease Inhibitor Cocktail (RocheApplied Science, Indianapolis, IN) and PhosSTOP phosphatase inhibitormixture (Roche Applied Science).
To assess for nuclear translocation of NF-kB proteins, differentiatedMDM were treated with DMF for 24 h, exposed to TNF-a (1 ng/ml) for 10min, and fractionated. To prepare nuclear extracts, cells were rinsed twicein ice-cold PBS and lysed on ice for 10 min in 10 mM HEPES (pH 7.9), 10mM KCl, 10 mM EDTA, 1 mM DTT, and 0.4% Nonidet P-40 supple-mented with protease and phosphatase inhibitors. Nuclei were pelleted for3 min at 16,000 3 g and the supernatant (cytoplasmic fraction) was col-lected and stored at 220˚C. The nuclear pellet was resuspended in 20 mMHEPES (pH 7.9), 400 mM NaCl, 1 mM EDTA, 10% glycerol, 1 mM DTT,and protease and phosphatase inhibitors and incubated at 4˚C on a rockingplatform at 200 rpm for 2 h. After centrifugation at 16,000 3 g for 5 min,supernatants (nuclear fractions) were collected and stored at 220˚C. Allprotein concentrations were determined by the Detergent Compatibleprotein assay (Bio-Rad, Hercules, CA).
Cell lysates were subjected to SDS-PAGE as previously described (26)using the following Abs: rabbit anti–HO-1 (Stressgen/Enzo Life Sciences,Farmingdale, NY), mouse anti-NQO1 (Abcam, Cambridge, MA), mouseanti-Nrf2 (R&D Systems), rabbit anti-RelB (Cell Signaling Technologies,Danvers, MA), rabbit anti–NF-kB p65 (Cell Signaling Technology), rabbitanti–NF-kB p50 (Cell Signaling Technology), rabbit anti-poly(ADP-ribose) polymerase (Cell Signaling Technology), mouse anti-GAPDH (Ad-vanced Immunochemical, Long Beach, CA), and species-specific HRP-conjugated secondary Abs (Jackson ImmunoResearch Laboratories, WestGrove, PA or Cell Signaling Technology). For densitometry analysis, filmswere scanned and a fixed cursor area centered over each band was assessedfor pixel density using ImageJ (NIH, Bethesda, MD).
MDM-mediated neurotoxicity
Rat cerebrocortical neuronal cultures were prepared from embryos ofSprague–Dawley rats at day 17 of gestation, as previously described (26).All procedures were within the Animal Research: Reporting In VivoExperiments guidelines for animal research and in accordance with pro-tocols approved by the University of Pennsylvania Institutional AnimalCare and Use Committee. Cells were plated in tissue-culture dishes pre-coated with poly-L-lysine (Peptides International, Louisville, KY) andmaintained in neurobasal media plus B27 supplement (Invitrogen, Carls-bad, CA) at 37˚C and 5% CO2. Forty-eight hours after plating, cells weretreated with 10 mM Ara-C. After 7 d in vitro, approximately one-halfvolume of fresh media was added to the cells to counteract effects ofevaporation. All cultures were used between 14 and 16 d in vitro.
Cell-based microtubule-associated protein 2 (MAP2) ELISAs wereperformed on primary rat cerebrocortical cells plated at a density of 63 104
cells/well in 96-well plates. Following a 24-h exposure to HIV/MDM su-pernatant, cultures were fixed and fluorescently labeled as described (30,31) using the following reagents: mouse anti-MAP2 (Covance, Princeton,NJ), goat anti-mouse b-lactamase TEM-1 conjugate (Invitrogen), and Fluo-rocillin Green substrate (Invitrogen). Fluorescence intensity was measuredusing a fluorometric plate reader with the 480/520-nm filter set. Macro-phage supernatant was applied at a 1:10–1:50 dilution; the dilution thatgave values within the linear range of the assay is presented.
2 DMF REDUCES HIV REPLICATION AND NEUROTOXICITY
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

Immunofluorescence
Primary rat cerebrocortical cells were plated at a density of 2 3 105 cellsper 35-mm dish with glass coverslips. Following exposure to HIV/MDMsupernatant for 24 h, cultures were fixed and fluorescently labeled as de-scribed (26) using the following reagents: mouse anti-MAP2 (Sigma-Aldrich), species-specific Cy3-conjugated secondary Ab (Jackson Immu-noResearch Laboratories), and Hoechst 33342 (Invitrogen).
Lactate dehydrogenase assay
Soluble lactate dehydrogenase (LDH) in HIV/MDM culture supernatantwas measured using the Cytotoxicity Detection KitPLUS (Roche AppliedScience) according to the manufacturer’s instructions.
EMSA
Following 24 h of pretreatment with DMF, human MDM were exposed to1 ng/ml TNF-a for 10 min and nuclear protein extracts were isolated asdescribed. A total of 8 mg nuclear protein was assessed for NF-kB–DNAbinding with an EMSA kit (Panomics, Santa Clara, CA), used according tothe manufacturer’s directions. The labeled oligonucleotide for NF-kB p50binding, 59-AGTTGAGGGGACTTTCCCAGGC-39, was used.
Cytokine detection in culture supernatants
The concentration of TNF-a in culture supernatants was detected usingan ELISA kit (Invitrogen) and used according to the manufacturer’s in-structions. Uninfected MDM were treated with 0.067% DMSO (vehicle) orDMF for 24 h prior to exposure to 10 mg/ml PHA for 6 h. Supernatantswere collected and frozen at 280˚C until assayed.
Chemotaxis assay
Monocyte chemotaxis was assayed using the Chemicon QCM 96-well (5-mM pore size) Migration kit (Millipore, Temecula, CA) according to themanufacturer’s directions. Freshly isolated human monocytes were platedat a density of 2 3 105 cells/well in serum- and growth factor-free culturemedia to the upper chamber in the presence of DMF, MMF, or vehicle(0.02% DMSO). CCL2 (300 ng/ml) was added to the lower chamber andcells were incubated at 37˚C and 6% CO2 for 6 h (32–34). Exposure ofmonocytes to 300 ng/ml CCL2 for 6 h most consistently induced chemo-taxis, with an average of 35.3 6 20.2% above baseline. All cells that hadmigrated through the insert, including those adhered to the bottom of themembrane, were collected. For quantification, cells were lysed and labeledwith CyQuant GR dye (Molecular Probes, Invitrogen). Fluorescence wasread with the 480/520 nm filter set on a fluorometric plate reader.
Flow cytometry
Human PBMCs were cultured in RPMI 1640 supplemented with 10% FBSand 50 U/ml penicillin/streptomycin at 37˚C and 5% CO2. Following 6 h of
treatment with the indicated concentrations of DMF or DMSO vehicle,cells were washed with ice-cold FACS buffer (PBS, 1% BSA, and 0.1%NaN3) and stained with CD11b-PE (clone ICRF44; eBioscience, SanDiego, CA), CD14-PE/Cy7 (M5E2; BioLegend, San Diego, CA), andCCR2-PerCP/Cy5.5 (TG5; BioLegend) Abs. Mouse IgG2a-PerCP/Cy5.5(MOPC-173; BioLegend) was used as the isotype control for CCR2staining. Ab-stained cell suspensions were pretreated with DAPI to iden-tify dead cells. Flow cytometry was performed on an LSR II (BD Bio-sciences, Franklin Lakes, NJ). Doublets were excluded using forward sidescatter-height versus forward side scatter-width and side scatter-heightversus side scatter-width parameters. Data were analyzed using FlowJo(Tree Star, Ashland, OR). Monocytes were identified as CD11b+CD14+
cells.
Statistics
All quantifications are expressed as mean 6 SE of mean. Statisticalcomparisons were made by Student t test, one-way ANOVA plus New-man–Keuls post hoc test, or post hoc test for linear trend, as indicated. Allgraphs were generated and statistical analyses were performed usingGraphPad Prism software (GraphPad, San Diego, CA) and values of p ,0.05 were considered significant.
ResultsDMF and MMF inhibit HIV replication in human MDM
DMF and its in vivo primary metabolite MMF inhibit NF-kBsignaling, suppress the production of inflammatory mediators, andinduce an antioxidant response in a variety of cell types (19–22,24, 35, 36). NF-kB signaling has been established as a majorpathway of HIV transcriptional regulation and recent studies haveimplicated the antioxidant response enzyme HO-1 as a negativeregulator of HIV replication in monocytes (25, 37). Therefore, wehypothesized that DMF could modulate HIV replication in humanmacrophages through one or both of these mechanisms. HumanMDM infected with HIV-1 were treated with DMF or MMF andthen examined for virus replication. As shown in Fig. 1, exposureof MDM to DMF (Fig. 1A) or MMF (Fig. 1B) attenuated HIVreplication in a dose-dependent manner, as determined by culturesupernatant RT levels. Suppression of replication in MDM wasseen with the R5 CSF HIV strain Jago (Fig. 1) and the prototypicR5/X4 strain 89.6 (Supplemental Fig. 1). As shown in Supple-mental Table I, HIV replication was inhibited by an average of∼30% at MMF concentrations achieved in vivo after single-doseadministration (4.4 mM in CSF and 6.5 mM in plasma) (23, 38).
FIGURE 1. DMF and MMF attenuate HIV replica-
tion in human MDM. Human MDM infected with 50
ng HIV (p24 ELISA, equivalent to 1.82 6 0.22 kcpm/
ml by RT activity assay) were treated with DMF (A) or
MMF (B) over the course of infection at the indicated
concentrations (1–30 mM) or with 20 nM of the non-
nucleoside RT inhibitor EFZ. Culture supernatants
were collected every 2 to 3 d, as indicated, and HIV
replication was quantified by RT activity. DMF (C) and
MMF (D) cause no cytotoxicity in HIV/MDM as as-
sessed by LDH assay of supernatants harvested at day
14 postinfection. Maximum (Max) LDH release rep-
resents the soluble LDH release following cell lysis. RT
curves are representative of three to four independent
experiments, with each replicate performed on cell
preparations from different donors. LDH assays repre-
sent data averaged from three to five individual donors.
All statistical comparisons were made by one-way
ANOVA plus Newman–Keuls post hoc testing. ***p ,0.001 versus EFZ.
The Journal of Immunology 3
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

No drug toxicity was detected at concentrations up to 100 mM inHIV-infected MDM (HIV/MDM) (Fig. 1C, 1D) and noninfectedMDM (data not shown). DMF demonstrated additive effects inattenuating HIV replication when used in combination with EFZ,a nonnucleoside RT inhibitor (Supplemental Fig. 2A). There wasno observed cellular toxicity when DMF was used in combinationwith EFZ (Supplemental Fig. 2B).
DMF and MMF reduce HIV/MDM-mediated neurotoxicity
We and others (26, 29, 39) have shown that HIV-infected MDMrelease potent neurotoxins that injure neurons through overacti-vation of NMDAR and that this excitotoxicity is mediated by glu-
tamate and other low m.w. NMDAR agonists. Although the mech-anisms underlying neurotoxin production in HIV/MDM are notfully understood, suppression of HIV replication in MDM gen-erally suppresses such neurotoxicity, as demonstrated by treat-ment with EFZ (Fig. 2). Similarly, in addition to suppressingHIV replication (Fig. 1), DMF (Fig. 2A) and MMF (Fig. 2B) alsoreduce HIV/MDM neurotoxin production in a dose-dependentmanner, as assessed by neuronal survival in our in vitro HIV neu-rotoxicity model. Representative images of HIV/MDM-mediatedneurotoxicity and the protective effects of DMF and MMF areshown (Fig. 2C), in which surviving neurons are labeled for MAP2.DMF and EFZ used in combination resulted in additive effects on
FIGURE 2. DMF and MMF reduce HIV/MDM-
mediated neurotoxicity. Rat cerebrocortical cultures
were exposed to supernatant from HIV-infected mac-
rophages that were treated with DMF (A) or MMF (B)
at the indicated concentrations (1–30 mM) during the
course of infection. Neuronal survival was assessed by
MAP2 ELISA and expressed as a percentage of un-
treated (UT) cultures (n = 6). C, Representative images
of rat cerebrocortical cultures immunofluorescently
stained for MAP2 (red) and Hoechst 33324 (blue)
following 24 h treatment with the indicated HIV/MDM
supernatant. Scale bar, 50 mm. All statistical compar-
isons were made by one-way ANOVA plus Newman–
Keuls post hoc testing. ***p , 0.001 versus vehicle.
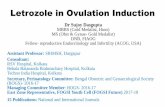
FIGURE 3. DMF inhibits NF-kB nuclear translocation, DNA binding, and TNF-a production in human MDM. DMF (A) and MMF (B) inhibit the
nuclear translocation of the NF-kB proteins RelB, p65, and p50 in human MDM in a dose-dependent manner. Cells were treated with DMF or MMF for
24 h, exposed to TNF-a (10 min), separated into cytoplasmic and nuclear fractions, and analyzed by Western blotting. Results of densitometry analysis are
presented numerically under each panel as the ratio of NF-kB protein to poly(ADP-ribose) polymerase, a nuclear marker, and loading control. Blots are
representative of four to six independent experiments, with each replicate performed on cell preparations from different donors. C, DMF inhibits nuclear
NF-kB p50 binding to DNA in TNF-a–stimulated MDM, as assessed by EMSA. Results of densitometry analysis were normalized to vehicle. D, DMF
inhibits the production of TNF-a in MDM stimulated with PHA (10 mg/ml). Values are expressed as percent TNF-a production relative to vehicle-treated
cells (227 6 11.9 pg/ml TNF-a in vehicle). Data are expressed as mean 6 SEM and averaged from four different donors. E, TNF-a production in HIV/
MDM is inhibited by DMF treatment. HIV/MDM were treated with DMF (1–30 mM) or 20 nM EFZ over the course of infection and culture supernatants
from days 14 to 15 postinfection were assayed for TNF-a by ELISA. Values represent the mean 6 SEM of data averaged from four different donors. All
statistical comparisons were made by one-way ANOVA plus Newman–Keuls post hoc testing. *p , 0.05, **p , 0.01, ***p , 0.01 versus vehicle.
4 DMF REDUCES HIV REPLICATION AND NEUROTOXICITY
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

the suppression of macrophage-mediated neurotoxicity (Supple-mental Fig. 2C), demonstrating that DMF may successfully reduceHIV replication and macrophage-mediated neurotoxicity that is notfully suppressed by ART. This neuroprotection is due to drug effectson the macrophages, as DMF and MMF do not prevent HIV/MDM-mediated neurotoxicity when applied directly to the neurons prior toaddition of HIV/MDM supernatants (data not shown).
DMF inhibits NF-kB nuclear entry, DNA binding, and TNF-aproduction in human MDM
NF-kB and TNF-a are part of a positive-feedback loop that reg-ulates the transcriptional activity of the HIV long terminal repeat(LTR). In unstimulated cells, NF-kB is unable to bind DNA due toits association with IkB proteins, which sequester NF-kB in thecytoplasmic compartment (40–42). Following exposure to an ac-tivating stimulus such as TNF-a, NF-kB is rapidly freed from theinhibitory complex and translocates into the nucleus to inducetranscriptional activation of viral and host genes. NF-kB proteinsare major modulators of the HIV LTR and are among the mostpotent activators of proinflammatory and inflammatory genes.Five members of the mammalian NF-kB/Rel family have beendescribed, including c-Rel, NF-kB1 (p50/p105), NF-kB2 (p52/p100), RelA (p65), and RelB. Functional NF-kB complexes arecomposed of heterodimer complexes containing p65, c-Rel, orRelB bound to p50 or p52 (40, 43, 44). Exposure to activatingstimuli, such as TNF-a, induces the nuclear accumulation of NF-kB proteins, DNA binding by NF-kB p50, and transcription fromthe HIV LTR (45).To determine if DMF and MMF inhibit the nuclear translocation
of NF-kB proteins in MDM, DMF- and MMF-treated MDM werestimulated with TNF-a and subjected to subcellular fractionations
before detection of NF-kB subunits by Western blotting. DMFand MMF each inhibited TNF-a–induced nuclear accumulation ofRelB, p65, and p50 in a dose-dependent manner (Fig. 3A, 3B). Wealso demonstrate that DMF inhibited the formation of the NF-kBp50–DNA complex, as assessed by EMSA (Fig. 3C). Because NF-kB signaling also induces expression of inflammatory mediators,we assessed the effects of DMF treatment on TNF-a release fromMDM. In agreement with previous reports of DMF decreasing therelease of inflammatory mediators from multiple cell types, in-cluding TNF-a, IL-1b, and IL-6 (24, 46), we found that DMF sup-presses release of TNF-a from PHA-activated MDM (Fig. 3D).Furthermore, DMF also markedly suppressed HIV-induced TNF-arelease from MDM (Fig. 3E). Thus, DMF and its primary me-tabolite, MMF, inhibit NF-kB translocation and signaling eventsthat contribute to the positive-feedback loop that modulates HIVtranscription in infected and activated MDM.
DMF restores the antioxidant response suppressed by HIVinfection in MDM
The antioxidant response is one of the cellular adaptive stress re-sponses that can modulate virus replication and host cell survival,as shown in hepatitis B and dengue 2 infection models (47, 48). Theantioxidant response maintains redox balance and counteractsoxidative damage through induction of proteins that are involvedin detoxification of reactive oxygen species (ROS). These proteinsare produced by genes with a common promoter element, theantioxidant response element (ARE), and ARE transcription ismediated by Nrf2. Under conditions of low oxidative stress, Nrf2is kept transcriptionally inactive by Kelch-like ECH-associatedprotein 1 (Keap1), which sequesters Nrf2 in the cytoplasmic com-partment (49). Following exposure to ROS or electrophiles, Keap1
FIGURE 4. DMF restores the im-
balance in the antioxidant response
caused by HIV infection. HIV infec-
tion of human MDM reduces HO-1
and GPX1 expression, as assessed by
Western blotting (A) and quantified by
densitometry analysis (B). Values in-
dicate mean 6 SEM of six different
donors. Statistical comparisons were
made by two-tailed paired t test. C,
DMF activates the Nrf2-dependent an-
tioxidant response in HIV/MDM and
restores HO-1 and GPX1 levels to that
found in uninfected mock cells, as
quantified by densitometry analysis
(D). MMF activates the Nrf2-depen-
dent antioxidant response in HIV/
MDM and restores HO-1 and GPX1
levels to that found in uninfected
mock cells (E), as quantified by densi-
tometry analysis (F). Blots are repre-
sentative of three independent experi-
ments, with each replicate performed
on cell preparations from different
donors. Densitometry data are ex-
pressed as mean 6 SEM and aver-
aged from three different donors.
*p , 0.05, **p , 0.01, ***p ,0.001 versus mock.
The Journal of Immunology 5
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

is degraded by the proteasome and Nrf2 translocates to the nucleusto drive expression of numerous genes, including HO-1, NQO1,glutathione peroxidase 1 (GPX1), and genes responsible for glu-tathione synthesis (glutamate cysteine ligase modifier, glutamatecysteine ligase catalytic subunit, and glutathione synthetase). HIVinfection is associated with increased ROS production and de-pressed levels of glutathione, the major intracellular antioxidant(50). We observed a marked reduction in the level of HO-1 ex-pression in HIV/MDM across multiple human donors, with a moremodest but nonetheless consistent reduction in GPX1 levels (Fig.4A, 4B). The effects of DMF on Nrf2 and NQO1 levels were morevariable among HIV/MDM cultures from different donors, buttrended toward increased expression relative to uninfected mock/MDM (Fig. 4A, 4B).Upon exposure of HIV/MDM to DMF, expression of Nrf2,
HO-1, GPX1, and NQO1 increased with increasing doses of DMF(Fig. 4C), suggesting a restoration of antioxidant responses inHIV-infected MDM. Both HIV infection and DMF increase totallevels of Nrf2, suggesting that although HIV infection stabilizesor induces total cellular Nrf2 levels, this is not sufficient forthe coordinated transcriptional activation of ARE-regulated genes,such as HO-1 and GPX1. DMF and MMF treatment activatestranscription of these ARE-regulated genes in HIV-infected mac-rophages, possibly by disrupting inhibitory Nrf2–Keap1 inter-actions (23). DMF restores levels of HO-1 and GPX1 to thoseobserved in uninfected MDM, whereas NQO1, which is not sup-pressed during HIV infection, is induced to levels exceeding thosein uninfected MDM (Fig. 4D). We have also confirmed that MMFcan induce the antioxidant response in HIV/MDM (Fig. 4E, 4F)and that both DMF and MMF induce the antioxidant response inuninfected MDM (data not shown). DMF induction of antioxidantresponses in MDM occurs independently of HIV infection, whichis consistent with previous findings describing induction of theantioxidant response by DMF in multiple cell types, including gliaand neurons (23, 24).
DMF inhibition of HIV replication and NF-kB signaling is notmediated by HO-1
HIV infection of human MDM results in alterations to the anti-oxidant response with a striking reduction in HO-1 levels (Fig. 4A,4B). Induction of HO-1 by hemin has been reported to decreaseHIV replication in human monocytes, suggesting that DMF’s in-duction of HO-1 may underlie its antiviral effects (25). We useda pharmacologic inhibitor of HO-1 enzymatic activity, SnMP, todetermine the potential role for HO-1 in DMF-mediated sup-pression of HIV replication and NF-kB translocation. As shown inFig. 5A, SnMP had no effect on DMF-mediated HIV suppres-sion, which suggests that DMF does not suppress HIV replicationthrough enhanced HO-1 expression and activity. We found noeffect of SnMP on DMF-mediated suppression of HIV replicationregardless of donor, level of infection, DMF dose, or timing ofSnMP addition (data not shown). We also confirmed that SnMPdoes not inhibit DMF’s suppression of TNF-a–induced nuclearaccumulation of NF-kB (Fig. 5B). In addition, we show thatan inducer of HO-1 expression, CoPP, had no effect on TNF-a–induced nuclear accumulation of NF-kB (Fig. 5B). These resultssuggest that DMF’s induction of HO-1 does not directly suppressHIV replication or NF-kB signaling.
Induction of HO-1 reduces neurotoxin production fromHIV/MDM
We sought to determine whether the suppression of HIV/MDMneurotoxin production by DMF (Fig. 2) was associated withDMF’s suppression of HIV replication and/or induction of HO-1
expression. Inhibiting HIV replication in HIV/MDM can suppressneurotoxin release in vitro, as demonstrated by EFZ treatment(Fig. 2), and similar effects of ART drugs in vivo are thought toaccount for their ability to limit the severity of HAND in ART-experienced cohorts. Although previous studies found that in-creased HO-1 activity is associated with decreased HIV replica-tion in MDM (25, 37), we found that neither inhibition of HO-1activity by SnMP treatment of MDM (Fig. 6A) nor induction ofHO-1 expression by CoPP (Fig. 6D, 6F) altered HIV replication.Remarkably, however, SnMP treatment significantly increased theneurotoxicity of MDM supernatant (Fig. 6B), even when HIVreplication was low or absent (Fig. 6C). The increase in MDM-mediated neurotoxicity was a consequence of inhibiting HO-1activity in the macrophage because SnMP was not toxic whenadded directly onto neurons (data not shown). Although CoPPdoes not attenuate HIV replication or inhibit NF-kB signaling,supernatant from CoPP-treated HIV/MDM is significantly lessneurotoxic than untreated controls with a similar level of HIVreplication (Fig. 6E). These studies demonstrate that HO-1 is acritical modulator of neurotoxin production in HIV/MDM and thatHO-1 levels can modulate HIV/MDM neurotoxicity without af-fecting HIV replication.
DMF and MMF inhibit CCL2-induced chemotaxis in humanmonocytes
The recruitment of activated and infected monocytes to the CNS inresponse to CCL2 is a key step in the pathogenesis of HAND (51,52). In a previous DMF study using the mouse EAE model, DMFreduced macrophage infiltration into the spinal cord in areas of
FIGURE 5. HO-1 does not mediate the attenuation of HIV replication or
NF-kB signaling induced by DMF. A, SnMP, an inhibitor of HO-1 enzy-
matic activity, does not inhibit DMF-mediated attenuation of HIV repli-
cation. DMF and vehicle-treated HIV/MDM were exposed to 10 mM
SnMP from days 6 to 15 postinfection. Culture supernatants were collected
every 3 d and assessed for RT activity. RT curves are representative
of three independent experiments, with each replicate performed on cell
preparations from different donors. B, SnMP and CoPP, a specific inducer
of HO-1, do not directly affect or alter DMF-mediated inhibition of the
nuclear translocation of NF-kB proteins, as assessed by Western blotting.
Human MDM were treated with 10 mM SnMP, 10 mM CoPP, and/or 100
mM DMF for 24 h before treatment with 1 ng/ml TNF-a (10 min) and
subcellular fractionation. Western blot is representative of three indepen-
dent experiments, with each replicate performed on cell preparations from
different donors.
6 DMF REDUCES HIV REPLICATION AND NEUROTOXICITY
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

active demyelination (19). We hypothesized that DMF could in-hibit chemotaxis of human monocytes in response to chemotacticcytokines, such as CCL2. We found that DMF and MMF inhibitedchemotaxis in freshly isolated human monocytes in response toCCL2 in a dose-dependent manner (Fig. 7A, 7B). Furthermore, wefound that DMF reduced the expression of the CCL2 receptorCCR2 in freshly isolated human CD11b+CD14+ monocytes within6 h of treatment (Fig. 7C, 7D), without causing death (Fig. 7E).These results indicate that DMF and MMF can decrease monocytechemotaxis in response to CCL2 and that this effect is associatedwith downregulation of CCR2 expression.
DiscussionMonocytes and macrophages are major reservoirs for HIV in boththe periphery and CNS and they facilitate the spread of virus totarget cells, allow for viral persistence, and serve as major con-tributors to inflammation-mediated pathology. Despite currentART, latently infected monocytes and CD4+ T lymphocytes per-sist, resulting in inflammation in the periphery and in the CNS inup to 50% of patients on ART (7, 8). Although ART will remain
the mainstay of HIV therapy, effective adjunctive therapies thatsuppress inflammation, improve morbidity, and improve long-termcognitive outcomes are greatly needed. The immunomodulatorDMF, which is effective for the treatment of psoriasis and showspromising results for multiple sclerosis treatment in recent clini-cal trials, is an attractive candidate as a safe adjunctive neuro-protectant against HIV. We have demonstrated that physiologi-cally relevant doses of DMF and its primary metabolite MMF (23,38) affect key steps in the pathogenesis of HAND in our in vitromodel system by inhibiting HIV replication, neurotoxin produc-tion, NF-kB signaling, and TNF-a production in human MDM andby reducing monocyte chemotaxis in response to CCL2. Theseresults suggest that DMF could serve as an effective neuro-protectant in HAND and have beneficial effects on systemic HIVdisease progression as well.We have shown that DMF and MMF attenuate macrophage-
mediated neurotoxicity following HIV infection by simulta-neously attenuating viral replication and inducing HO-1 expres-sion. Furthermore, induction of HO-1 can significantly decreasemacrophage-mediated neurotoxicity even without decreasing
FIGURE 6. HO-1 induction reduces neurotoxin production in HIV/MDM without affecting HIV replication. SnMP, an inhibitor of HO-1 enzymatic activity,
does not directly affect HIV replication (A) and supernatant from these SnMP-treated HIV/MDM is significantly more neurotoxic (B), despite equal levels of HIV
replication. C, Uninfected mock/MDM and 20 nM EFZ-treated HIV/MDM, which normally produce minimal neurotoxins, are significantly more neurotoxic when
treated with 10 mM SnMP. D, CoPP, a specific inducer of HO-1 expression, does not directly affect HIV replication and supernatant from these CoPP treated HIV/
MDM is significantly less neurotoxic (E), despite high levels of virus replication. F, CoPP treatment exponentially increases HO-1 levels without greatly altering
the other components of the antioxidant response, as assessed by Western blotting. For A and C, SnMP or CoPP was added at day 6 postinfection onwards and
culture supernatants were collected every 3 d and assessed for RT activity. RT curves are representative of three independent experiments, with each replicate
performed on cell preparations from different donors. For neuronal survival assays, survival was assessed by MAP2 ELISA and expressed as a percentage of
untreated (UT) cultures (n = 6). Statistical comparisons were made by one-way ANOVA plus Newman–Keuls post hoc testing. Western blot is representative of
three independent experiments, with each replicate performed on cell preparations from different donors. Two film exposures (short and long) of HO-1 are
presented to demonstrate the extent of HO-1 induction over basal levels. ***p , 0.001 versus vehicle-treated paired condition.
The Journal of Immunology 7
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

HIV replication. Consequently, DMFmay be an especially relevanttherapeutic in patients who have relatively good virologic controlbut still suffer from neurologic complications of HIV. We haveshown that HIV infection of MDM results in a dysregulation ofthe antioxidant response with an especially prominent reduction inHO-1 levels associated with supernatant neurotoxicity and thatDMF treatment restores HO-1 levels and reduces neurotoxinproduction in macrophages. In activated microglia, an oxidativeburst is required for the release of excitotoxic glutamate (53),demonstrating that alterations to cellular oxidative state can me-diate the production and/or release of MDM neurotoxins. DMF’sability to decrease HIV replication and neurotoxin production bydistinct mechanisms makes it an especially attractive therapeuticcandidate for HAND. Furthermore, macrophage- and microglia-mediated neurotoxicity contribute to many other neurologic dis-orders including multiple sclerosis, Alzheimer’s disease, amyo-trophic lateral sclerosis, Huntington’s disease, and stroke/reperfusion injury, for which therapeutics for restoring oxidativebalance resultant from the disease state have been investigated/prescribed (54).Numerous proinflammatory factors contribute to HIV disease
pathogenesis in both the peripheral and CNS compartments. TNF-a, IL-6, IL-1b, IFN-g, and other proinflammatory cytokines areelevated in the blood and CSF of HIV-infected patients (55–58).Among these, TNF-a is the most potent mediator of inflammationand is induced early after HIV monocytic infection and its ex-pression continues to increase over the course of infection (59–61). It is well established that TNF-a exposure upregulates HIVreplication by initiating a signaling cascade that activates thenuclear translocation of NF-kB (62–65). We have shown thatDMF and MMF attenuate TNF-a–mediated NF-kB signaling inhuman macrophages and reduce nuclear NF-kB levels, which areexpected to decrease transcription from the HIV LTR. However,
the NF-kB and TNF-a signaling loop may not entirely mediateDMF’s antiviral activity. Attenuation of HIV replication occurs atlow concentrations, as does induction of the ARE, whereas in-hibition of NF-kB signaling may be more relevant at concen-trations of$15 mM. Future studies are necessary to assess the roleof the antioxidant response, including NQO1 and the cellular re-dox state, in mediating HIV infection and replication. DMF mayalter the expression of the HIV coreceptors CXCR4 and CCR5,similarly to the observed downregulation of cell-surface CCR2.It has been reported that antioxidants decrease the stability ofmRNA transcripts for CXCR4 and CCR5 in human monocytes,suggesting that DMF treatment may directly reduce HIVentry intohuman monocytes (66).However, DMF’s ability to inhibit NF-kB and TNF-a signaling
following both PHA stimulation and HIV infection has clearimplications for the physiologic reduction of neuroinflammationand cytokine-induced neuronal injury. Elevated TNF-a levels in-crease monocyte entry into the brain, promote HIV replication,and drive inflammatory cascades, thereby enhancing the produc-tion of neurotoxins in the CNS from MDM, microglia, and astro-cytes (67). Therefore, dampening TNF-a–driven processes mightalso afford neuroprotection against HIV. Indeed, TNF-a is linkedto glutamine synthetase and glutamate import in macrophages(68) and DMF’s inhibition of TNF-a–driven processes may fur-ther decrease the release of excitatory neurotoxins, such as glu-tamate, in HIV/MDM. In human macrophages, we have shownthat DMF is a potent suppressor of NF-kB nuclear translocation,subsequent binding to DNA and expression of NF-kB–dependentgenes. Therefore, DMF is a particularly good therapeutic candi-date for pathological states characterized by macrophage-driveninflammation and NF-kB signaling.Although not directly dependent upon HO-1, DMF’s antioxidant
properties are likely mediating the inhibition of NF-kB activity.
FIGURE 7. DMF and MMF reduce CCL2-induced
chemotaxis in human monocytes. DMF (A) and MMF
(B) inhibit CCL2-induced chemotaxis in freshly iso-
lated human monocytes in a dose-dependent manner.
Values are expressed as percent migration of unstim-
ulated cells (0 ng/ml CCL2) (n = 10–22). DMF de-
creases CCR2 expression on CD11b+CD14+ PBMCs
(C) following 6 h of treatment, as quantified (D). E,
DMF does not cause significant cell death over 6 h of
treatment in freshly isolated human monocytes, as
measured by DAPI positivity in CD11b+CD14+-gated
PBMCs. For all experiments, values represent data
averaged from three different donors. All statistical
comparisons were made by one-way ANOVA plus
Newman–Keuls post hoc testing. Results of posttest for
linear trend are also presented. **p , 0.01 versus ve-
hicle. US, unstimulated cells.
8 DMF REDUCES HIV REPLICATION AND NEUROTOXICITY
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

We hypothesize that such effects are due to DMF’s modulation ofthe macrophage intracellular redox state as activation of the an-tioxidant response has been shown to block NF-kB activity andHIV transcription (69–71). Furthermore, classical (a and b), novel(d), and atypical (z) protein kinase C (PKC) isotypes can modulatethe nuclear translocation and transcriptional activity of NF-kB andPKC is activated by oxidative stress and inhibited by antioxidants(72–76). In addition to potential effects on PKC, DMF may alsoaffect the phosphorylation of IkB kinases and subsequent phos-phorylation and degradation of IkB proteins (21, 36). Finally,DMF may affect NF-kB–dependent transcription by modulatingthe preferred composition of NF-kB homo- and heterodimers thatform after nuclear translocation has occurred. The intracellularoxidative state can affect levels of NF-kB p50 homodimers, whichdo not possess transactivation domains and are thought to act astranscriptional repressors of NF-kB heterodimer-responsive genes(77–79). We are currently examining the role of DMF and MMFin modulating the activation state of the macrophage, which wouldaffect the cell’s relative sensitivity to proinflammatory signals andthereby contribute to decreased NF-kB signaling.Although other antioxidants have been considered as potential
therapeutics for HAND through direct effects on macrophages orneurons, DMF is unique in its ability to inhibit CCL2-inducedmonocyte chemotaxis. Monocyte transmigration across theblood–brain barrier is dependent upon production of chemokines,such as CCL2, in the CNS and the activation of monocytes in theperiphery. Levels of CCL2 in the CSF correlate with CSF viralload and with the clinical severity of HAND (51, 52, 80–83) andCCL2 is produced by brain macrophages, astrocytes, and endo-thelial cells in response to inflammatory mediators and HIVproteins (84–86). Not only does DMF decrease TNF-a productionand NF-kB signaling in MDM, both of which have been impli-cated in CCL2 production, but DMF and MMF also inhibit CCL2-driven monocyte chemotaxis, possibly by modulation of CCR2expression. DMF and MMF may modulate the cell-surface ex-pression of CCR2 by inducing the antioxidant response and con-sequently altering the redox state of the cell. It has been dem-onstrated that direct antioxidants are capable of reducing thetranscript stability of CCR2, which has been linked to decreasedcell-surface expression and CCL2-induced chemotaxis in humanmonocytes (66). These findings in our in vitro model systempredict suppression of transendothelial migration of monocytesinto the CNS during HIV infection. Furthermore, it has beenreported that DMF modulates adhesion molecule expression inhuman endothelial cells by inhibiting TNF-a–induced expressionof ICAM-1, VCAM-1, and E-selectin (35). Expression of each ofthese adhesion molecules has been linked to monocyte entry intothe CNS after HIV infection and downregulation by DMF isexpected to further inhibit monocyte entry into the CNS. Giventhese findings, DMF should be considered as a potential thera-peutic for other neuroinflammatory diseases associated withCCL2-induced recruitment of leukocytes to the CNS.With this study, we identify DMF as a candidate adjunctive
therapy and potential neuroprotectant against HIV. We believe thisis the first demonstration that HIV infection dysregulates com-ponents of the antioxidant response in humanmacrophages and thatrestoration of HO-1 levels, specifically, can reduce macrophage-mediated neurotoxicity. To our knowledge, DMF is the first pro-posed neuroprotectant that reduces CCL2-mediated monocytechemotaxis as a component of its mechanism of action. Further-more, we have shown that DMF attenuates HIV replication as-sociated with decreased TNF-a and NF-kB signaling. Given thesefindings, we propose that DMF should be considered a relevanttherapeutic candidate for neurologic disorders and other compli-
cations of HIV-infection mediated by monocyte and macrophageinflammation.
AcknowledgmentsWe thank Dr. Samantha S. Soldan for technical assistance, intellectual con-
tributions, and critical review of the manuscript. We also thank Dr. Stefan
Lanker of Biogen Idec and Dr. Francisco Gonzalez-Scarano for helpful
discussions, Margaret Maronski for expert preparation of primary rodent
neuronal cultures, and Dr. Natalia Nedelsky for thoughtful critique and
editing of the manuscript. The following reagent was obtained through the
National Institutes of Health AIDS Research and Reference Reagent Pro-
gram, Division of AIDS, National Institute of Allergy and Infectious Dis-
eases, National Institutes of Health (EFZ, catalog number 4624).
DisclosuresD.L.K. has served as a paid consultant to Teva Neurosciences and Biogen
Idec, Inc. and serves on the advisory committee to the National Institutes of
Health/National Institute of Mental Health National NeuroAIDS Tissue
Consortium. The other authors have no financial conflicts of interest.
References1. Antinori, A., G. Arendt, J. T. Becker, B. J. Brew, D. A. Byrd, M. Cherner,
D. B. Clifford, P. Cinque, L. G. Epstein, K. Goodkin, et al. 2007. Updated re-search nosology for HIV-associated neurocognitive disorders. Neurology 69:1789–1799.
2. McArthur, J. C., J. Steiner, N. Sacktor, and A. Nath. 2010. Human immuno-deficiency virus-associated neurocognitive disorders: Mind the gap. Ann. Neurol.67: 699–714.
3. Dunfee, R., E. R. Thomas, P. R. Gorry, J. Wang, P. Ancuta, and D. Gabuzda.2006. Mechanisms of HIV-1 neurotropism. Curr. HIV Res. 4: 267–278.
4. Petito, C. K., E. S. Cho, W. Lemann, B. A. Navia, and R. W. Price. 1986.Neuropathology of acquired immunodeficiency syndrome (AIDS): an autopsyreview. J. Neuropathol. Exp. Neurol. 45: 635–646.
5. Ho, D. D., T. R. Rota, R. T. Schooley, J. C. Kaplan, J. D. Allan, J. E. Groopman,L. Resnick, D. Felsenstein, C. A. Andrews, and M. S. Hirsch. 1985. Isolation ofHTLV-III from cerebrospinal fluid and neural tissues of patients with neurologicsyndromes related to the acquired immunodeficiency syndrome. N. Engl. J. Med.313: 1493–1497.
6. Koenig, S., H. E. Gendelman, J. M. Orenstein, M. C. Dal Canto,G. H. Pezeshkpour, M. Yungbluth, F. Janotta, A. Aksamit, M. A. Martin, andA. S. Fauci. 1986. Detection of AIDS virus in macrophages in brain tissue fromAIDS patients with encephalopathy. Science 233: 1089–1093.
7. Robertson, K. R., M. Smurzynski, T. D. Parsons, K. Wu, R. J. Bosch, J. Wu,J. C. McArthur, A. C. Collier, S. R. Evans, and R. J. Ellis. 2007. The prevalenceand incidence of neurocognitive impairment in the HAART era. AIDS 21: 1915–1921.
8. Sacktor, N., M. P. McDermott, K. Marder, G. Schifitto, O. A. Selnes,J. C. McArthur, Y. Stern, S. Albert, D. Palumbo, K. Kieburtz, et al. 2002. HIV-associated cognitive impairment before and after the advent of combinationtherapy. J. Neurovirol. 8: 136–142.
9. Brenchley, J. M., D. A. Price, T. W. Schacker, T. E. Asher, G. Silvestri, S. Rao,Z. Kazzaz, E. Bornstein, O. Lambotte, D. Altmann, et al. 2006. Microbialtranslocation is a cause of systemic immune activation in chronic HIV infection.Nat. Med. 12: 1365–1371.
10. Ancuta, P., A. Kamat, K. J. Kunstman, E. Y. Kim, P. Autissier, A. Wurcel,T. Zaman, D. Stone, M. Mefford, S. Morgello, et al. 2008. Microbial trans-location is associated with increased monocyte activation and dementia in AIDSpatients. PLoS ONE 3: e2516.
11. Eden, A., R. W. Price, S. Spudich, D. Fuchs, L. Hagberg, and M. Gisslen. 2007.Immune activation of the central nervous system is still present after .4 years ofeffective highly active antiretroviral therapy. J. Infect. Dis. 196: 1779–1783.
12. Persidsky, Y., M. Stins, D. Way, M. H. Witte, M. Weinand, K. S. Kim, P. Bock,H. E. Gendelman, and M. Fiala. 1997. A model for monocyte migration throughthe blood-brain barrier during HIV-1 encephalitis. J. Immunol. 158: 3499–3510.
13. Glass, J. D., H. Fedor, S. L. Wesselingh, and J. C. McArthur. 1995. Immuno-cytochemical quantitation of human immunodeficiency virus in the brain: cor-relations with dementia. Ann. Neurol. 38: 755–762.
14. Anthony, I. C., S. N. Ramage, F. W. Carnie, P. Simmonds, and J. E. Bell. 2005.Influence of HAART on HIV-related CNS disease and neuroinflammation. J.Neuropathol. Exp. Neurol. 64: 529–536.
15. Brenchley, J. M., D. A. Price, and D. C. Douek. 2006. HIV disease: fallout froma mucosal catastrophe? Nat. Immunol. 7: 235–239.
16. Brenchley, J. M., and D. C. Douek. 2008. HIV infection and the gastrointestinalimmune system. Mucosal Immunol. 1: 23–30.
17. Hoxtermann, S., C. Nuchel, and P. Altmeyer. 1998. Fumaric acid esters suppressperipheral CD4- and CD8-positive lymphocytes in psoriasis. Dermatology 196:223–230.
18. 2011. Trial watch: Phase III success for Biogen’s oral multiple sclerosis therapy.Nat. Rev. Drug Discov. 10: 404.
The Journal of Immunology 9
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

19. Schilling, S., S. Goelz, R. Linker, F. Luehder, and R. Gold. 2006. Fumaric acidesters are effective in chronic experimental autoimmune encephalomyelitis andsuppress macrophage infiltration. Clin. Exp. Immunol. 145: 101–107.
20. Stoof, T. J., J. Flier, S. Sampat, C. Nieboer, C. P. Tensen, and D. M. Boorsma.2001. The antipsoriatic drug dimethylfumarate strongly suppresses chemokineproduction in human keratinocytes and peripheral blood mononuclear cells. Br.J. Dermatol. 144: 1114–1120.
21. Seidel, P., I. Merfort, J. M. Hughes, B. G. Oliver, M. Tamm, and M. Roth. 2009.Dimethylfumarate inhibits NF-kappaB function at multiple levels to limit airwaysmooth muscle cell cytokine secretion. Am. J. Physiol. Lung Cell. Mol. Physiol.297: L326–L339.
22. Loewe, R., W. Holnthoner, M. Groger, M. Pillinger, F. Gruber,D. Mechtcheriakova, E. Hofer, K. Wolff, and P. Petzelbauer. 2002. Dime-thylfumarate inhibits TNF-induced nuclear entry of NF-kappa B/p65 in humanendothelial cells. J. Immunol. 168: 4781–4787.
23. Linker, R. A., D. H. Lee, S. Ryan, A. M. van Dam, R. Conrad, P. Bista, W. Zeng,X. Hronowsky, A. Buko, S. Chollate, et al. 2011. Fumaric acid esters exertneuroprotective effects in neuroinflammation via activation of the Nrf2 antiox-idant pathway. Brain 134: 678–692.
24. Lehmann, J. C., J. J. Listopad, C. U. Rentzsch, F. H. Igney, A. von Bonin,H. H. Hennekes, K. Asadullah, and W. D. Docke. 2007. Dimethylfumarateinduces immunosuppression via glutathione depletion and subsequent inductionof heme oxygenase 1. J. Invest. Dermatol. 127: 835–845.
25. Devadas, K., and S. Dhawan. 2006. Hemin activation ameliorates HIV-1 in-fection via heme oxygenase-1 induction. J. Immunol. 176: 4252–4257.
26. O’Donnell, L. A., A. Agrawal, K. L. Jordan-Sciutto, M. A. Dichter, D. R. Lynch,and D. L. Kolson. 2006. Human immunodeficiency virus (HIV)-induced neu-rotoxicity: roles for the NMDA receptor subtypes. J. Neurosci. 26: 981–990.
27. Kaul, M., J. Zheng, S. Okamoto, H. E. Gendelman, and S. A. Lipton. 2005. HIV-1 infection and AIDS: consequences for the central nervous system. Cell DeathDiffer. 12(Suppl 1): 878–892.
28. Lipton, S. A. 2004. Failures and successes of NMDA receptor antagonists:molecular basis for the use of open-channel blockers like memantine in thetreatment of acute and chronic neurologic insults. NeuroRx 1: 101–110.
29. Chen, W., J. Sulcove, I. Frank, S. Jaffer, H. Ozdener, and D. L. Kolson. 2002.Development of a human neuronal cell model for human immunodeficiencyvirus (HIV)-infected macrophage-induced neurotoxicity: apoptosis induced byHIV type 1 primary isolates and evidence for involvement of the Bcl-2/Bcl-xL-sensitive intrinsic apoptosis pathway. J. Virol. 76: 9407–9419.
30. White, M. G., Y. Wang, C. Akay, K. A. Lindl, D. L. Kolson, and K. L. Jordan-Sciutto. 2011. Parallel high throughput neuronal toxicity assays demonstrateuncoupling between loss of mitochondrial membrane potential and neuronaldamage in a model of HIV-induced neurodegeneration. Neurosci. Res. 70: 220–229.
31. Wang, Y., M. G. White, C. Akay, R. A. Chodroff, J. Robinson, K. A. Lindl,M. A. Dichter, Y. Qian, Z. Mao, D. L. Kolson, and K. L. Jordan-Sciutto. 2007.Activation of cyclin-dependent kinase 5 by calpains contributes to human im-munodeficiency virus-induced neurotoxicity. J. Neurochem. 103: 439–455.
32. Eugenin, E. A., K. Osiecki, L. Lopez, H. Goldstein, T. M. Calderon, andJ. W. Berman. 2006. CCL2/monocyte chemoattractant protein-1 mediates en-hanced transmigration of human immunodeficiency virus (HIV)-infected leu-kocytes across the blood-brain barrier: a potential mechanism of HIV-CNSinvasion and NeuroAIDS. J. Neurosci. 26: 1098–1106.
33. Janic, B., A. S. Iskander, A. M. Rad, H. Soltanian-Zadeh, and A. S. Arbab. 2008.Effects of ferumoxides-protamine sulfate labeling on immunomodulatory char-acteristics of macrophage-like THP-1 cells. PLoS ONE 3: e2499.
34. Chiou, W. F., H. C. Ko, and B. L. Wei. 2011. Evodia rutaecarpa and three majoralkaloids abrogate influenza A virus (H1N1)-induced chemokines productionand cell migration. Evid. Based Complement. Alternat. Med. 2011: 750513.
35. Vandermeeren, M., S. Janssens, M. Borgers, and J. Geysen. 1997. Dimethylfuma-rate is an inhibitor of cytokine-induced E-selectin, VCAM-1, and ICAM-1 ex-pression in human endothelial cells. Biochem. Biophys. Res. Commun. 234: 19–23.
36. Vandermeeren, M., S. Janssens, H. Wouters, I. Borghmans, M. Borgers, R. Beyaert,and J. Geysen. 2001. Dimethylfumarate is an inhibitor of cytokine-induced nucleartranslocation of NF-kappa B1, but not RelA in normal human dermal fibroblastcells. J. Invest. Dermatol. 116: 124–130.
37. Devadas, K., I. K. Hewlett, and S. Dhawan. 2010. Lipopolysaccharide suppressesHIV-1 replication in human monocytes by protein kinase C-dependent hemeoxygenase-1 induction. J. Leukoc. Biol. 87: 915–924.
38. Litjens, N. H., J. Burggraaf, E. van Strijen, C. van Gulpen, H. Mattie,R. C. Schoemaker, J. T. van Dissel, H. B. Thio, and P. H. Nibbering. 2004.Pharmacokinetics of oral fumarates in healthy subjects. Br. J. Clin. Pharmacol.58: 429–432.
39. Jiang, Z. G., C. Piggee, M. P. Heyes, C. Murphy, B. Quearry, M. Bauer, J. Zheng,H. E. Gendelman, and S. P. Markey. 2001. Glutamate is a mediator of neuro-toxicity in secretions of activated HIV-1-infected macrophages. J. Neuro-immunol. 117: 97–107.
40. Baldwin, A. S., Jr. 1996. The NF-k B and I k B proteins: new discoveries andinsights. Annu. Rev. Immunol. 14: 649–683.
41. Ganchi, P. A., S. C. Sun, W. C. Greene, and D. W. Ballard. 1992. I kappa B/MAD-3 masks the nuclear localization signal of NF-kappa B p65 and requiresthe transactivation domain to inhibit NF-kappa B p65 DNA binding. Mol. Biol.Cell 3: 1339–1352.
42. Henkel, T., U. Zabel, K. van Zee, J. M. Muller, E. Fanning, and P. A. Baeuerle.1992. Intramolecular masking of the nuclear location signal and dimerizationdomain in the precursor for the p50 NF-kappa B subunit. Cell 68: 1121–1133.
43. Kilareski, E. M., S. Shah, M. R. Nonnemacher, and B. Wigdahl. 2009. Regu-lation of HIV-1 transcription in cells of the monocyte-macrophage lineage.Retrovirology 6: 118.
44. Neumann, M., H.-W. Fries, C. Scheicher, P. Keikavoussi, A. Kolb-Maurer,E.-B. Brocker, E. Serfling, and E. Kampgen. 2000. Differential expression ofRel/NF-kappaB and octamer factors is a hallmark of the generation and matu-ration of dendritic cells. Blood 95: 277–285.
45. Duh, E. J., W. J. Maury, T. M. Folks, A. S. Fauci, and A. B. Rabson. 1989. Tumornecrosis factor alpha activates human immunodeficiency virus type 1 throughinduction of nuclear factor binding to the NF-kappa B sites in the long terminalrepeat. Proc. Natl. Acad. Sci. USA 86: 5974–5978.
46. Wilms, H., J. Sievers, U. Rickert, M. Rostami-Yazdi, U. Mrowietz, andR. Lucius. 2010. Dimethylfumarate inhibits microglial and astrocytic in-flammation by suppressing the synthesis of nitric oxide, IL-1beta, TNF-alphaand IL-6 in an in-vitro model of brain inflammation. J. Neuroinflammation 7: 30.
47. Chen, T. H., P. Tang, C. F. Yang, L. H. Kao, Y. P. Lo, C. K. Chuang, Y. T. Shih,and W. J. Chen. 2011. Antioxidant defense is one of the mechanisms by whichmosquito cells survive dengue 2 viral infection. Virology 410: 410–417.
48. Schaedler, S., J. Krause, K. Himmelsbach, M. Carvajal-Yepes, F. Lieder,K. Klingel, M. Nassal, T. S. Weiss, S. Werner, and E. Hildt. 2010. Hepatitis Bvirus induces expression of antioxidant response element-regulated genes byactivation of Nrf2. J. Biol. Chem. 285: 41074–41086.
49. Itoh, K., N. Wakabayashi, Y. Katoh, T. Ishii, K. Igarashi, J. D. Engel, andM. Yamamoto. 1999. Keap1 represses nuclear activation of antioxidant re-sponsive elements by Nrf2 through binding to the amino-terminal Neh2 domain.Genes Dev. 13: 76–86.
50. Dworkin, B. M., W. S. Rosenthal, G. P. Wormser, and L. Weiss. 1986. Seleniumdeficiency in the acquired immunodeficiency syndrome. J. Parenter. EnteralNutr. 10: 405–407.
51. Cinque, P., L. Vago, M. Mengozzi, V. Torri, D. Ceresa, E. Vicenzi, P. Transidico,A. Vagani, S. Sozzani, A. Mantovani, et al. 1998. Elevated cerebrospinal fluidlevels of monocyte chemotactic protein-1 correlate with HIV-1 encephalitis andlocal viral replication. AIDS 12: 1327–1332.
52. Zink, M. C., G. D. Coleman, J. L. Mankowski, R. J. Adams, P. M. Tarwater,K. Fox, and J. E. Clements. 2001. Increased macrophage chemoattractantprotein-1 in cerebrospinal fluid precedes and predicts simian immunodeficiencyvirus encephalitis. J. Infect. Dis. 184: 1015–1021.
53. Barger, S. W., M. E. Goodwin, M. M. Porter, and M. L. Beggs. 2007. Glutamaterelease from activated microglia requires the oxidative burst and lipid perox-idation. J. Neurochem. 101: 1205–1213.
54. Uttara, B., A. V. Singh, P. Zamboni, and R. T. Mahajan. 2009. Oxidative stressand neurodegenerative diseases: a review of upstream and downstream antiox-idant therapeutic options. Curr. Neuropharmacol. 7: 65–74.
55. Ciardi, M., M. K. Sharief, E. J. Thompson, A. Salotti, V. Vullo, F. Sorice, andA. Cirelli. 1994. High cerebrospinal fluid and serum levels of tumor necrosisfactor-alpha in asymptomatic HIV-1 seropositive individuals. Correlation withinterleukin-2 and soluble IL-2 receptor. J. Neurol. Sci. 125: 175–179.
56. Breen, E. C., A. R. Rezai, K. Nakajima, G. N. Beall, R. T. Mitsuyasu, T. Hirano,T. Kishimoto, and O. Martinez-Maza. 1990. Infection with HIV is associatedwith elevated IL-6 levels and production. J. Immunol. 144: 480–484.
57. Kobayashi, S., Y. Hamamoto, N. Kobayashi, and N. Yamamoto. 1990. Serumlevel of TNF alpha in HIV-infected individuals. AIDS 4: 169–170.
58. Ownby, R. L., A. M. Kumar, J. Benny Fernandez, I. Moleon-Borodowsky,L. Gonzalez, S. Eisdorfer, D. Waldrop-Valverde, and M. Kumar. 2009. Tumornecrosis factor-alpha levels in HIV-1 seropositive injecting drug users. J. Neu-roimmune Pharmacol. 4: 350–358.
59. Esser, R., W. Glienke, H. von Briesen, H. Rubsamen-Waigmann, and R. Andreesen.1996. Differential regulation of proinflammatory and hematopoietic cytokines inhuman macrophages after infection with human immunodeficiency virus. Blood 88:3474–3481.
60. Folks, T. M., S. W. Kessler, J. M. Orenstein, J. S. Justement, E. S. Jaffe, andA. S. Fauci. 1988. Infection and replication of HIV-1 in purified progenitor cellsof normal human bone marrow. Science 242: 919–922.
61. Koyanagi, Y., W. A. O’Brien, J. Q. Zhao, D. W. Golde, J. C. Gasson, andI. S. Chen. 1988. Cytokines alter production of HIV-1 from primary mono-nuclear phagocytes. Science 241: 1673–1675.
62. Poli, G., A. Kinter, J. S. Justement, J. H. Kehrl, P. Bressler, S. Stanley, andA. S. Fauci. 1990. Tumor necrosis factor alpha functions in an autocrine mannerin the induction of human immunodeficiency virus expression. Proc. Natl. Acad.Sci. USA 87: 782–785.
63. Butera, S. T., B. D. Roberts, and T. M. Folks. 1993. Regulation of HIV-1 ex-pression by cytokine networks in a CD4+ model of chronic infection. J.Immunol. 150: 625–634.
64. Nabel, G., and D. Baltimore. 1987. An inducible transcription factor activatesexpression of human immunodeficiency virus in T cells. Nature 326: 711–713.
65. West, M. J., A. D. Lowe, and J. Karn. 2001. Activation of human immuno-deficiency virus transcription in T cells revisited: NF-kappaB p65 stimulatestranscriptional elongation. J. Virol. 75: 8524–8537.
66. Saccani, A., S. Saccani, S. Orlando, M. Sironi, S. Bernasconi, P. Ghezzi,A. Mantovani, and A. Sica. 2000. Redox regulation of chemokine receptor ex-pression. Proc. Natl. Acad. Sci. USA 97: 2761–2766.
67. Fiala, M., D. J. Looney, M. Stins, D. D. Way, L. Zhang, X. Gan, F. Chiappelli,E. S. Schweitzer, P. Shapshak, M. Weinand, et al. 1997. TNF-alpha opensa paracellular route for HIV-1 invasion across the blood-brain barrier. Mol. Med.3: 553–564.
10 DMF REDUCES HIV REPLICATION AND NEUROTOXICITY
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from

68. Porcheray, F., C. Leone, B. Samah, A. C. Rimaniol, N. Dereuddre-Bosquet, and
G. Gras. 2006. Glutamate metabolism in HIV-infected macrophages: implica-
tions for the CNS. Am. J. Physiol. Cell Physiol. 291: C618–C626.69. Schreck, R., P. Rieber, and P. A. Baeuerle. 1991. Reactive oxygen intermediates
as apparently widely used messengers in the activation of the NF-kappa B
transcription factor and HIV-1. EMBO J. 10: 2247–2258.70. Roederer, M., F. J. Staal, P. A. Raju, S. W. Ela, L. A. Herzenberg, and
L. A. Herzenberg. 1990. Cytokine-stimulated human immunodeficiency virus
replication is inhibited by N-acetyl-L-cysteine. Proc. Natl. Acad. Sci. USA 87:
4884–4888.71. Staal, F. J., M. Roederer, P. A. Raju, M. T. Anderson, S. W. Ela,
L. A. Herzenberg, and L. A. Herzenberg. 1993. Antioxidants inhibit stimulation
of HIV transcription. AIDS Res. Hum. Retroviruses 9: 299–306.72. Asehnoune, K., D. Strassheim, S. Mitra, J. Yeol Kim, and E. Abraham. 2005.
Involvement of PKCalpha/beta in TLR4 and TLR2 dependent activation of NF-
kappaB. Cell. Signal. 17: 385–394.73. Sun, Z., C. W. Arendt, W. Ellmeier, E. M. Schaeffer, M. J. Sunshine, L. Gandhi,
J. Annes, D. Petrzilka, A. Kupfer, P. L. Schwartzberg, and D. R. Littman. 2000.
PKC-theta is required for TCR-induced NF-kappaB activation in mature but not
immature T lymphocytes. Nature 404: 402–407.74. Boscoboinik, D., A. Szewczyk, C. Hensey, and A. Azzi. 1991. Inhibition of cell
proliferation by alpha-tocopherol. Role of protein kinase C. J. Biol. Chem. 266:
6188–6194.75. Gopalakrishna, R., Z.-H. Chen, and U. Gundimeda. 1995. Modifications of
cysteine-rich regions in protein kinase C induced by oxidant tumor promoters
and enzyme-specific inhibitors. Methods Enzymol. 252: 132–146.76. Gopalakrishna, R., U. Gundimeda, and Z.-H. Chen. 1997. Cancer-preventive
selenocompounds induce a specific redox modification of cysteine-rich regions
in Ca(2+)-dependent isoenzymes of protein kinase C. Arch. Biochem. Biophys.
348: 25–36.
77. Cristofanon, S., F. Morceau, A. I. Scovassi, M. Dicato, L. Ghibelli, andM. Diederich. 2009. Oxidative, multistep activation of the noncanonical NF-kappaB pathway via disulfide Bcl-3/p50 complex. FASEB J. 23: 45–57.
78. Hoberg, J. E., A. E. Popko, C. S. Ramsey, and M. W. Mayo. 2006. IkappaBkinase alpha-mediated derepression of SMRT potentiates acetylation of RelA/p65 by p300. Mol. Cell. Biol. 26: 457–471.
79. Zhou, L. Z. H., A. P. Johnson, and T. A. Rando. 2001. NF kappa B and AP-1mediate transcriptional responses to oxidative stress in skeletal muscle cells.Free Radic. Biol. Med. 31: 1405–1416.
80. Letendre, S. L., E. R. Lanier, and J. A. McCutchan. 1999. Cerebrospinal fluidbeta chemokine concentrations in neurocognitively impaired individuals infectedwith human immunodeficiency virus type 1. J. Infect. Dis. 180: 310–319.
81. Conant, K., A. Garzino-Demo, A. Nath, J. C. McArthur, W. Halliday, C. Power,R. C. Gallo, and E. O. Major. 1998. Induction of monocyte chemoattractantprotein-1 in HIV-1 Tat-stimulated astrocytes and elevation in AIDS dementia.Proc. Natl. Acad. Sci. USA 95: 3117–3121.
82. Kelder, W., J. C. McArthur, T. Nance-Sproson, D. McClernon, and D. E. Griffin.1998. Beta-chemokines MCP-1 and RANTES are selectively increased in ce-rebrospinal fluid of patients with human immunodeficiency virus-associateddementia. Ann. Neurol. 44: 831–835.
83. Sozzani, S., M. Introna, S. Bernasconi, N. Polentarutti, P. Cinque, G. Poli,A. Sica, and A. Mantovani. 1997. MCP-1 and CCR2 in HIV infection: regulationof agonist and receptor expression. J. Leukoc. Biol. 62: 30–33.
84. Gu, L., B. Rutledge, J. Fiorillo, C. Ernst, I. Grewal, R. Flavell, R. Gladue, andB. Rollins. 1997. In vivo properties of monocyte chemoattractant protein-1. J.Leukoc. Biol. 62: 577–580.
85. Guillemin, G. J., J. Croitoru-Lamoury, D. Dormont, P. J. Armati, and B. J. Brew.2003. Quinolinic acid upregulates chemokine production and chemokine re-ceptor expression in astrocytes. Glia 41: 371–381.
86. Lehmann, M. H., S. Masanetz, S. Kramer, and V. Erfle. 2006. HIV-1 Nefupregulates CCL2/MCP-1 expression in astrocytes in a myristoylation- andcalmodulin-dependent manner. J. Cell Sci. 119: 4520–4530.
The Journal of Immunology 11
by guest on March 19, 2018
http://ww
w.jim
munol.org/
Dow
nloaded from