Dihydropyrimidine Dehydrogenase Activity in Human ... · the syringe was inverted carefully to mix...
7
[CANCER RESEARCH 53, 5433-5438. November 15, 1 Dihydropyrimidine Dehydrogenase Activity in Human Peripheral Blood Mononuclear Cells and Liver: Population Characteristics, Newly Identified Deficient Patients, and Clinical Implication in 5-Fluorouracil Chemotherapy1 Zhihong Lu, Ruiwen Zhang, and Robert B. Diasio2 Departments of I'luirmacology [Z. L. R. Z., R. B. D.¡and Medicine //?. R. [)./, Division of Clinical Pharmacology /R. Z., R. B. D.¡, Comprehensive Cancer Center /R. Z., R. B. D.¡,University of Alabama at Hirming/ium, Hirmiitf-lmm. Alabama 35294 ABSTRACT Dihydropyrimidine dehydrogenase (DPD) is the initial and rate-limiting enzyme in the catabolism of 5-fluorouracil (FUra), one of the most widely used anticancer drugs. Previous studies from our laboratory demon strated the clinical importance of DPD in cancer patients (G. D. Heggie, J-P. Sommadossi, D. S. Cross, W. J. Muster, and R. B. Diasio. Cancer Res., 47: 2203-2206, 1987; B. E. Harris, R. Song, S-j. Soong, and R. B. Diasio. Cancer Res., 50: 197-201, 1990), particularly in those with DPD deficiency who experience severe FUra toxicity (including death) following FUra treatment [R. B. Diasio, T. L. Beavers, and J. T. Carpenter. J. Clin. Invest., 81: 47-51, 1988; B. E. Harris, J. T. Carpenter, and R. B. Diasio. Cancer (Phila.), 68: 499-501, 1991]. We now suggest that measurement of DPD activity may be useful in routine screening of cancer patients prior to FUra treatment. In this paper, we describe the following serial studies: (a) we developed a sensitive, accurate, and precise DPD assay and a storage method to stabilize DPD activity, permitting large scale DPD screening in cancer patients; 11»we demonstrated a normal distribution (Gaussian distribution) of human DPD activity from peripheral blood mononuclear cells (PBM-DPD) in a population study. Baselines for PBM-DPD with fresh and frozen samples were 0.425 ±0.124 (SD) and 0.189 ±0.064 nmol/min/mg protein, respectively. The 95% and 99% distribution ranges for both fresh and frozen samples were also determined, providing criteria for detection of DPD-deficient patients; (c) we identified nine new patients with profound or partial DPD deficiency; (d\ we determined a baseline for human liver DPD activity, which was shown to be 0.360 ±0.182 nmol/ min/mg protein (frozen samples); in we did a preliminary evaluation of liver DPD from deficient patients. Low liver DPD activity in two deficient patients correlated with low PBM-DPD activity. Using a polyclonal anti body raised against human liver DPD in our laboratory (Z. Lu, R. Zhang, and R. B. Diasio. J. Biol. Chem., 267: 17102-17109, 1992), Western blot analysis demonstrated decreased DPD protein in the liver cytosol from DPD-deficient patients compared to normal subjects. These results may be useful in improving the effectiveness and/or lessening the toxicity of FUra chemotherapy. INTRODUCTION DPD' (EC 1.3.1.2) is the initial and rate-limiting enzyme in FUra catabolism (1-4). Although it has been thought that the cytotoxic effects of FUra are directly mediated by the anabolic pathway (1-4), studies from our laboratory have demonstrated the importance of the catabolic pathway with more than 80% of administered FUra being catabolized by DPD (5). It has also been shown that the anticancer Received 6/9/93; accepled 9/8/93. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by USPHS Grant CA-62164 and Clinical Research Center Grant RR-00032. This study was presented in part at the 29th annual meeting of the American Society of Clinical Oncology (ASCO), Orlando. FL, May 16-18, 1993. Z. L. is the recipient of the 1993 ASCO Travel Awards. 2 To whom requests for reprints should be addressed, at Department of Pharmacology, University of Alabama at Birmingham. UAB Station, Box 600, Volker Hall 101, Birming ham. AL 35294-0019. 1 The abbreviations used are: DPD, dihydropyrimidine dehydrogenase; FUra, 5-fluo rouracil; PBM cells, peripheral blood mononuclear cells; SDS-PAGE. sodium dodecyl sulfate-polyacrylamide gel electrophoresis; HPLC. high-performance liquid chromatog- raphy. efficacy of FUra is related to DPD activity in an experimental animal tumor model (6). We (7) and others (8, 9) have demonstrated that DPD activity is correlated with FUra pharmacokinetics, suggesting an im portant role in the regulation of FUra metabolism and thus determin ing the amount of FUra available for anabolism. DPD activity in humans (7, 10) and experimental animals (11-14) follows a circadian pattern, which is inversely correlated with FUra plasma level in cancer patients treated with FUra by continuous infusion (7). Additional studies with competitive DPD inhibitors (15-18) have also shown the importance of DPD in FUra chemotherapy. More importantly, the role of DPD in FUra chemotherapy has been shown in cancer patients with confirmed (19-21) or suspected (22, 23) DPD deficiency. These patients experienced severe FUra toxicity (in cluding death) following FUra treatment. A clinical pharmacological study of one of these deficient patients (19) demonstrated minimal catabolism of FUra with a 10-fold longer FUra half-life compared to patients with normal DPD activity. Familial studies (19-21) have demonstrated that this pharmacogenetic syndrome follows an autoso- mal recessive pattern of inheritance. Although extensive studies in DPD biochemistry have been con ducted with experimental animals and crude human tissue prepara tions (24-27), little has been known about human DPD until recently. In our laboratory, human liver DPD has recently been purified and characterized with preparation of a polyclonal antibody to DPD (28, 29), permitting further investigation of DPD in cancer patients. Given the frequent use of FUra in cancer chemotherapy, the im portance of DPD in FUra pharmacokinetics, and the clinical signifi cance of DPD deficiency, we suggest the potential value of DPD screening in cancer patients prior to and during FUra treatment. In order to provide the basis for large scale DPD screening in cancer patients, the following studies were undertaken: (a) development of a sensitive, accurate, precise, and clinically useful DPD assay; (b) es tablishment of a baseline for DPD activity and criteria for diagnosis of partial and profound DPD deficiency; (c) identification of additional patients with DPD deficiency; (d) determination of liver DPD activity in the general population and in cancer patients with DPD deficiency initially identified by PBM-DPD assay. In addition, using a polyclonal antibody raised from purified human liver DPD (28), we also con ducted Western blot analyses to determine if DPD protein in the liver cytosol from DPD- deficient patients was decreased compared to that of normal subjects. The serial studies reported in this paper demon strate the potential value of measuring DPD activity. We believe that determination of DPD activity in cancer patients prior to and/or during FUra treatment may be beneficial in improving the clinical effective ness of FUra. MATERIALS AND METHODS Chemicals and Radiochemicals FUra, bovine serum albumin. NADPH, and Histopaque were purchased from the Sigma Chemical Co. (St. Louis, MO). ['H]FUra (25 Ci/mmol) was obtained from New England Nuclear Corp. (Boston. MA). The purity of 5433 on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Dihydropyrimidine Dehydrogenase Activity in Human ... · the syringe was inverted carefully to mix...

[CANCER RESEARCH 53, 5433-5438. November 15, 1
Dihydropyrimidine Dehydrogenase Activity in Human Peripheral BloodMononuclear Cells and Liver: Population Characteristics, NewlyIdentified Deficient Patients, and Clinical Implication in5-Fluorouracil Chemotherapy1
Zhihong Lu, Ruiwen Zhang, and Robert B. Diasio2
Departments of I'luirmacology [Z. L. R. Z., R. B. D.¡and Medicine //?. R. [)./, Division of Clinical Pharmacology /R. Z., R. B. D.¡,Comprehensive Cancer Center /R. Z.,R. B. D.¡,University of Alabama at Hirming/ium, Hirmiitf-lmm. Alabama 35294
ABSTRACT
Dihydropyrimidine dehydrogenase (DPD) is the initial and rate-limitingenzyme in the catabolism of 5-fluorouracil (FUra), one of the most widely
used anticancer drugs. Previous studies from our laboratory demonstrated the clinical importance of DPD in cancer patients (G. D. Heggie,J-P. Sommadossi, D. S. Cross, W. J. Muster, and R. B. Diasio. Cancer Res.,47: 2203-2206, 1987; B. E. Harris, R. Song, S-j. Soong, and R. B. Diasio.Cancer Res., 50: 197-201, 1990), particularly in those with DPD deficiency
who experience severe FUra toxicity (including death) following FUratreatment [R. B. Diasio, T. L. Beavers, and J. T. Carpenter. J. Clin. Invest.,81: 47-51, 1988; B. E. Harris, J. T. Carpenter, and R. B. Diasio. Cancer(Phila.), 68: 499-501, 1991]. We now suggest that measurement of DPD
activity may be useful in routine screening of cancer patients prior to FUratreatment. In this paper, we describe the following serial studies: (a) wedeveloped a sensitive, accurate, and precise DPD assay and a storagemethod to stabilize DPD activity, permitting large scale DPD screening incancer patients; 11»we demonstrated a normal distribution (Gaussiandistribution) of human DPD activity from peripheral blood mononuclearcells (PBM-DPD) in a population study. Baselines for PBM-DPD with
fresh and frozen samples were 0.425 ±0.124 (SD) and 0.189 ±0.064nmol/min/mg protein, respectively. The 95% and 99% distribution rangesfor both fresh and frozen samples were also determined, providing criteriafor detection of DPD-deficient patients; (c) we identified nine new patients
with profound or partial DPD deficiency; (d\ we determined a baseline forhuman liver DPD activity, which was shown to be 0.360 ±0.182 nmol/min/mg protein (frozen samples); in we did a preliminary evaluation ofliver DPD from deficient patients. Low liver DPD activity in two deficientpatients correlated with low PBM-DPD activity. Using a polyclonal anti
body raised against human liver DPD in our laboratory (Z. Lu, R. Zhang,and R. B. Diasio. J. Biol. Chem., 267: 17102-17109, 1992), Western blot
analysis demonstrated decreased DPD protein in the liver cytosol fromDPD-deficient patients compared to normal subjects. These results may be
useful in improving the effectiveness and/or lessening the toxicity of FUrachemotherapy.
INTRODUCTION
DPD' (EC 1.3.1.2) is the initial and rate-limiting enzyme in FUra
catabolism (1-4). Although it has been thought that the cytotoxiceffects of FUra are directly mediated by the anabolic pathway (1-4),
studies from our laboratory have demonstrated the importance of thecatabolic pathway with more than 80% of administered FUra beingcatabolized by DPD (5). It has also been shown that the anticancer
Received 6/9/93; accepled 9/8/93.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
1Supported by USPHS Grant CA-62164 and Clinical Research Center GrantRR-00032. This study was presented in part at the 29th annual meeting of the AmericanSociety of Clinical Oncology (ASCO), Orlando. FL, May 16-18, 1993. Z. L. is therecipient of the 1993 ASCO Travel Awards.
2 To whom requests for reprints should be addressed, at Department of Pharmacology,
University of Alabama at Birmingham. UAB Station, Box 600, Volker Hall 101, Birmingham. AL 35294-0019.
1 The abbreviations used are: DPD, dihydropyrimidine dehydrogenase; FUra, 5-fluorouracil; PBM cells, peripheral blood mononuclear cells; SDS-PAGE. sodium dodecylsulfate-polyacrylamide gel electrophoresis; HPLC. high-performance liquid chromatog-
raphy.
efficacy of FUra is related to DPD activity in an experimental animaltumor model (6). We (7) and others (8, 9) have demonstrated that DPDactivity is correlated with FUra pharmacokinetics, suggesting an important role in the regulation of FUra metabolism and thus determining the amount of FUra available for anabolism. DPD activity inhumans (7, 10) and experimental animals (11-14) follows a circadian
pattern, which is inversely correlated with FUra plasma level in cancerpatients treated with FUra by continuous infusion (7). Additionalstudies with competitive DPD inhibitors (15-18) have also shown the
importance of DPD in FUra chemotherapy.More importantly, the role of DPD in FUra chemotherapy has been
shown in cancer patients with confirmed (19-21) or suspected (22, 23)
DPD deficiency. These patients experienced severe FUra toxicity (including death) following FUra treatment. A clinical pharmacologicalstudy of one of these deficient patients (19) demonstrated minimalcatabolism of FUra with a 10-fold longer FUra half-life compared topatients with normal DPD activity. Familial studies (19-21) havedemonstrated that this pharmacogenetic syndrome follows an autoso-
mal recessive pattern of inheritance.Although extensive studies in DPD biochemistry have been con
ducted with experimental animals and crude human tissue preparations (24-27), little has been known about human DPD until recently.
In our laboratory, human liver DPD has recently been purified andcharacterized with preparation of a polyclonal antibody to DPD (28,29), permitting further investigation of DPD in cancer patients.
Given the frequent use of FUra in cancer chemotherapy, the importance of DPD in FUra pharmacokinetics, and the clinical significance of DPD deficiency, we suggest the potential value of DPDscreening in cancer patients prior to and during FUra treatment. Inorder to provide the basis for large scale DPD screening in cancerpatients, the following studies were undertaken: (a) development of asensitive, accurate, precise, and clinically useful DPD assay; (b) establishment of a baseline for DPD activity and criteria for diagnosis ofpartial and profound DPD deficiency; (c) identification of additionalpatients with DPD deficiency; (d) determination of liver DPD activityin the general population and in cancer patients with DPD deficiencyinitially identified by PBM-DPD assay. In addition, using a polyclonal
antibody raised from purified human liver DPD (28), we also conducted Western blot analyses to determine if DPD protein in the livercytosol from DPD- deficient patients was decreased compared to that
of normal subjects. The serial studies reported in this paper demonstrate the potential value of measuring DPD activity. We believe thatdetermination of DPD activity in cancer patients prior to and/or duringFUra treatment may be beneficial in improving the clinical effectiveness of FUra.
MATERIALS AND METHODS
Chemicals and Radiochemicals
FUra, bovine serum albumin. NADPH, and Histopaque were purchasedfrom the Sigma Chemical Co. (St. Louis, MO). ['H]FUra (25 Ci/mmol) was
obtained from New England Nuclear Corp. (Boston. MA). The purity of
5433
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DPD ACTIVITY AND KUra CHIAMO 11IHKAI'Y
unlabeled and labeled FUra was confirmed by HPLC (30) to be greater than99%. Acrylamide and prestained molecular weight markers were purchasedfrom Bio-Rad (Richmond. CA). Alkaline phosphatase-labeled goat anti-rabbitantibody, nitro blue tetrazolium, and 5-bromo-4-chloro-3-indolyl phosphate
toluidine salt were obtained from Southern Biotechnology (Birmingham. AL).All other solvents and reagents were purchased in the highest grade available.
The major buffer (buffer A) used in both the enzyme preparation and DPDassay contained 35 HIMpotassium phosphate (pH 7.4), 2.5 mM magnesiumchloride, and 10 mM 2-mercaptoethanol. Since NADPH, the critical cofactor inthe enzyme reaction, is light sensitive and unstable with long-term storage, it
was freshly prepared.
Determination of PBM-DPD Activity in a Normal Population and
Patients
Healthy Volunteers. One hundred twenty-four healthy volunteers partici
pated in this study. This normal population consisted of faculty, staff, andstudents from the University and its affiliated units. Among them, DPD activitywas also determined with frozen samples from 109 subjects, along with another 14 frozen samples from healthy volunteers. The characteristics of thispopulation are listed in Table 1. Informed consent was obtained from eachhealthy volunteer, using an institutionally approved protocol.
Cancer Patients. In collaboration with more than 20 medical institutions,25 cancer patients who were treated with FUra (in combination with otheragents) and had experienced moderate to severe drug-related toxicity were
assayed for DPD activity. Consent was obtained from each patient.Blood Collection and Isolation of PBM Cells. Because of a known ar
cadian pattern of DPD activity (7), blood samples were collected between 8a.m. and 10 a.m. Blood samples (25-50 ml) were drawn from a peripheral veininto a 60-ml syringe containing 5 ml heparin (1000 units/ml). After collection,
the syringe was inverted carefully to mix heparin and blood. The blood samplewas then loaded onto a centrifuge tube containing 15 ml Histopaque. Aftercentrifugation at 500 X g for 30 min at 25°C,the PBM cell fraction (located
between the plasma fraction and Histopaque) was carefully removed andwashed 3 times with phosphate-buffered saline. Contaminating RBC were
hypotonically lysed. The resulting PBM cells were used in the subsequentassay (as fresh sample) or rapidly frozen (-70°C) and kept in fetal calf serum
prior to use (as frozen sample).To confirm that frozen samples would be useful in the population study, a
comparison of the results from fresh samples and frozen samples was performed in 109 healthy volunteers. After isolation, PBM cells were divided intotwo equal samples: one was used immediately (as fresh sample); another wasfrozen and kept in a freezer (-70°C) for 5 days and then assayed (as frozen
sample).Preparation of PBM Cytosol. Fresh PBM cells or slowly thawed frozen
PBM cells were suspended in buffer A and then placed in an ice bath and lysedby sonication (3 times for 10 s with a 30-s interval between sonication). Aftercentrifugation at 14,000 X g for 15 min at 4°C,the supernatant was removed
Table 1 PBM-DPD aciniiy in healthy volunteers(with fresh samples and frozen samples)
ParametersMean
activity(nmol/min/mg)SDSEDistribution95%
range99%rangeCharacteristicsnSexMalesFemalesRaceCaucasianNon-CaucasianAge
(yr)20304050Fresh
sample0.4250.1240.0110.182-0.6680.105-0.74512456
(45.2)"68
(54.8)77(62.1)47
(37.9)45
(36.3)39(31.5)25
(20.2)15(12.1)Frozen
sample0.1890.0640.0060.064-0.3140.024-0.35412355
(44.7)°68
(55.3)74
(60.2)49(39.8)39(31.7)42
(34.2)25(20.3)17(13.8)
' Numbers in parentheses, percentage.
and used in the subsequent enzyme assay. Using the method of Bradford (31),the amount of protein in the sample was determined prior to enzyme assay in
order to add the appropriate amount of protein into the reaction mixture.Enzyme Assay. DPD activity was determined by radioassay, measuring the
catabolites of FUra formed by reverse-phase HPLC (30). The reaction mixturecontained 200 JIM NADPH, 20 /J.M['HjFUra, buffer A, and enzyme solution
(250-1000 fig total protein) in a final volume of 1 ml. The mixture wasincubated at 37°C,and 175 jj,l of the reaction sample were taken out at various
times (5, 10, 20, 30, and 60 min) and mixed with the same volume of ice-coldethanol to stop the reaction. The mixture was then kept in a freezer (-20°C) for
30 min and subsequently filtered through a 0.2 urn Aero filter (GelmanSciences. Ann Arbor, Ml) prior to HPLC analysis.
Reverse-Phase HPLC Analysis. Separation of FUra and its cataboliteswas performed by reverse-phase HPLC using a method we have described in
detail previously (30).
Determination of Liver DPD Activity in "Normal" Donors
Human livers were obtained from the National Disease Research Interchange, Philadelphia, PA, and the University Tissue Procurement Service. Theprotocol used in this study was approved by National Disease Research Interchange and the Institutional Review Board at this university. The slowlythawed liver tissues were washed with ice-cold physiological saline (0.9%
NaCl), weighed, minced, and homogenized in 4 volumes of buffer A in thepresence of 0.25 M sucrose, 1 HIMbenzamidine, 1 HIMaminoethylisothiouro-
nium bromide, and 5 mM EDTA. The resulting homogenate was centrifuged at100,000 x g for 60 min at 4°C.The cytosolic fraction was removed and used
in the subsequent assay. Prior to enzyme assay, the amount of protein in eachsample was determined in order to add the appropriate amount of protein. Theenzyme reaction and HPLC analysis were performed using the above methods.
Calculation of DPD Activity
For each sample, five determinations were run at various incubation times.After HPLC analysis, the amount of FUra catabolites at each time point wasquantitated. The data were plotted using products formed (y) versus time (x)to calculate the slope of the reaction (products formed/min) by linear regression analysis. The slope was then divided by the amount of protein added toobtain the final result (DPD activity expressed as nmol/min/mg protein). Incancer patients with DPD deficiency, at least two separate assays were per
formed.
liiiiiiniiulil.il Analysis (Western Blot)
The primary antibody used in the study was the purified rabbit polyclonalantibody generated against human liver DPD (28). A 7% SDS-PAGE was
performed using the freshly prepared liver supernatant centrifuged at 100,000X g. SDS-PAGE was carried out in a 1.0-mm-thick 7% (w/v) polyacrylamidegel containing 0.375 MTris-HCl (pH 8.8) and 0.1% SDS. Samples were mixedwith an equal volume of sample buffer (0.0625 M Tris-HCl, pH 6.8-10%glycerol-0.2% SDS (w/v)-80 mM 2-mercaptoethanol) and then boiled for 5
min. Electrophoresis was performed at a constant current of 30 mA for 45 minat 25°C.The proteins were transferred from the gel to a nitrocellulose filter
following the method described previously by Towbin et al. (32). Followingincubation overnight at 4°Cwith the primary antibody (diluted 1:2000) in a
120 min borate-saline solution containing 1% (w/v) bovine serum albumin (pH8.5), the nitrocellulose filter was washed with borate-saline containing 0.5%(v/v) Tween 20 and then incubated with a secondary, alkaline phosphatase-
labeled goat anti-rabbit antibody. The location of immunoreactive proteins on
the nitrocellulose filter was detected in a 0.1 Msodium carbonate buffer (100ml), pH 9.5, containing 30 mg nitro blue tetrazolium (added as a 1-ml solutiondissolved in 70% dimethylformamide) and 15 mg 5-bromo-4-chloro-3-indolylphosphate toluidine salt (added as a 1-ml solution dissolved in 100% dimeth
ylformamide).
Statistical Analysis
The differences among the groups by sex, age, and race were analyzed bythe Student / test or analysis of variance as appropriate. To determine thedistribution pattern in the general population, probability testing was used totest the hypothesis that the sample population distribution of DPD activityfollows a normal distribution (Gaussian distribution). Following confirmation
5434
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DPD ACTIVITY AND FUra CHEMOTHERAPY
of a normal distribution, additional statistical parameters were calculated,including mean, SD, SE, and the 95% and 99% distribution ranges. In determining the correlation of DPD activity between fresh samples and frozensamples, Pearson correlation coefficients were calculated.
RESULTS
Optimal Assay Conditions and Evaluation of the PBM-DPD
Assay. In the present study, we optimized the assay conditions forquantitation of PBM-DPD activity, particularly in samples with de
creased PBM cells commonly seen in cancer patients with leukopenia.In brief, the conditions included: substrate (FUra) concentration at 20H.M;enzyme reaction maintained at pH 7.4 and 37°C;incubation time
between 5 and 60 min; and a protein level of PBM cytosol between 25and 100 /u.g/100 /j.1reaction mixture. Substrate and product inhibitionwere observed with PBM-DPD. Both protein (enzyme) level and
incubation time were shown to be critical factors in determining DPDactivity.
Statistical analysis further confirmed that the above method wassensitive (lowest detectable products being 0.005 nmol), accurate, andprecise (the inter- and intraday coefficients of variations being less
than 5%). Evaluation of the stability of DPD with frozen PBM cellsindicated that decreased DPD activity (—50%) occurred in the freez
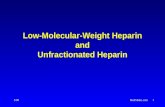
ing process, but DPD activity was stable afterwards for at least 1month (data not shown). The correlation coefficient between freshsample and frozen sample was 0.858 with statistical significance (Fig.1; P < 0.0001).
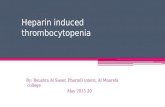
Population Distribution of PBM-DPD Activity. With freshly prepared samples, PBM-DPD activities in 124 healthy volunteers were
shown to follow a normal or Gaussian distribution (Fig. 2). Furthercross-analysis revealed that there was no significant difference among
groups by sex, race, or age (Table 2). Using a normal distributionmodel, several statistical parameters were calculated, including mean,SD, SE, and 95% and 99% distribution ranges (Table 1) for thepopulation. The 95% or 99% distribution range (i.e., theoretically95% or 99% persons in population have a DPD activity in the corresponding range) was subsequently used in the identification of DPDdeficiency (see below).
With frozen samples, PBM-DPD activities in 123 healthy volun
teers (among them were 109 paired samples from the above study withfresh samples) were also shown to follow a normal distribution (datanot shown) with no differences in sex, age, or race. Using a normaldistribution model, several statistical parameters for the population
0.4
0.3-
t
'S - 0.2-
>."'>'S
aCuO
0.1-
0.00.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
DPD Activity (nmol/min/mg protein)(Fresh Samples)
Fig. 1. Relationship between PBM-DPD activity with fresh samples and PBM-DPDwith frozen samples. Statistical analysis demonstrated that there is a strong correlation (r= 0.858; P < 0.0001).
PBM-DPD Activity (nmol/min/mg protein)
Fig. 2. Population distribution of PBM-DPD activity in 124 healthy volunteers. Statistical analysis demonstrated that PBM-DPD activity follows a normal distribution (Gaus
sian distribution).
Table 2 Comparison of PBM-DPD activity in healthy volunteers grouped by sex, race,and age (with fresh samples)
GroupMenCaucasianNon-CaucasianSubtotalWomenCaucasianNon-CaucasianSubtotalAge
(yr)20304050n37195640286845392515DPD
activity (mean ±SE)0.413
±0.0160.386±0.0300.404
±0.0150.431
±0.0200.460±0.0260.443±0.0160.413
±0.0140.456±0.0210.431±0.0300.373±0.031
were also calculated, including mean, SD, SE, and 95% and 99%distribution ranges (Table 1). As with the fresh samples above, the95% or 99% distribution range was used for identification of DPDdeficiency with frozen samples.
New Cases of DPD Deficiency. Using the above methods, wecollaborated with medical oncologists within our university and atmore than 20 medical institutions and have been able to identify 9 newdeficient patients who experienced moderate to severe FUra toxicitiesincluding mucositis, granulocytopenia, neuropathy, and death. Thecharacteristics, therapy, major toxicity, and DPD activity (expressedas a percentage of mean DPD activity in population) are shown inTables 3 and 4. Three profoundly deficient patients, listed in Table 3,experienced Grade V toxicity (death). DPD activity in this group wasless than 10% of the mean DPD activity in the general population andbelow the lower limit of the 99% distribution range. Six partiallydeficient patients listed in Table 4 experienced Grade II-III toxicity.
DPD activity was less than 30% of the mean DPD activity in thegeneral population and below the lower limit of the 95% distributionrange.
Table 3 New patients with profound DPD deficiency identified by PBM-DPD Assay
Patient12SexFFAge(yr)6275RaceB"CCancerBreastColonTherapyCMFFUraToxicityGrade
VGradeVPBM-DPDactivity07.06.0
neuropathy73 C Colon FUra + Grade V
folinic acid6.0
" DPD activity in PBM cells was expressed as the percentage of the mean PBM-DPD
activity of the population (Table 1).h B, black; C, Caucasian; CMF, cyclophosphamide-methotrexate-FUra.
5435
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DPD ACTIVITY AND FUra CHEMOTHERAPY
Table 4 M-H patients with partial DPD deficiency identified by PBM-DPD assay
Patient456789SexFMF
FFFAge(y)586473374175RaceC*CCBCCCancerRectalRectalColonBreastColonColonTherapyFUra
infusionFUrainfusionFUra
infusionCMFFUraFUraMajor
toxicityMucositisMucositisGranulocytopenia
MucositisMucositisGranulocytopeniaPBM-DPDactivity0
(%)18.028.017.0
10.026.019.0
M.W.Marker Pt.6 Pt.2 Normal
Subject
" DPD activity in PBM cells was expressedas the percentageof the mean PBM-DPD
activity of the population (Table 1)." C, Caucasian; B, black; CMF. cyclophosphamide-methotrexale-FUra.
We have been able to conduct familial studies with four of thepatients (patients 1 and 2 in Table 3; patients 5 and 7 in Table 4) andconfirmed an autosomal recessive pattern of inheritance (data notshown).
Liver DPD Activity in "Normal" Donors. Using frozen liversamples. DPD activities of 59 "normal" donor livers collected over the
preceding 24 months were determined and shown to follow a normaldistribution (data not shown) with no differences in age and race,although the DPD activity of females was slightly higher than that ofmales. The means and SD as well as the SE of liver DPD activity ineach group by sex, age, and race are shown in Table 5.
Liver DPD Activity and DPD Protein in Deficient Patients.After their deaths, liver DPD activities of two patients initially identified as being DPD deficient by PBM-DPD assay were determined.
Interestingly, liver DPD activities in the two patients correlated withtheir PBM-DPD activity. Patient 6, whose PBM-DPD activity was17% of the mean PBM-DPD activity of the normal population, had a
liver DPD of 38.9% of the mean liver DPD activity of the normalpopulation. Patient 2 had activities of 6% for PBM-DPD and 14.7%for liver DPD. These results suggest a relationship between PBM-DPD activity and liver-DPD activity. Using affinity-purified poly-
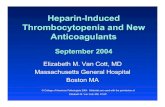
clonal antibody against human DPD. Western blot analysis revealedthat DPD protein was significantly decreased in liver cytosol from thetwo patients compared with normal subjects. As illustrated in Fig. 3,with an equal amount of protein loaded onto the gel, the DPD proteinband for patient 6 had a lower density compared to the normal subjects; an even lower density was seen with patient 2. These resultssuggest a relationship between DPD activity and DPD protein in theliver.
DISCUSSION
Recent studies have shown the important role that DPD has in FUracatabolism with regulation of the availability of FUra for anabolism,
Table 5 Liver DPI) activity in "Normal" donors (with frozen samples)
GroupTotalMenCaucasianNon-CaucasianSubtotalWomenCaucasianNon-CaucasianSubtotalAge"
(yr)20304050M70n59291342143174lu61111217DPD
activity (mean±SE)0.360
±0.0240.340
±0.0310.303±0.0450.328±0.0250.471
±0.0510.291±0.1390.439
±0.0490.369
±0.1130.410±0.0640.280±0.0460.291±0.0570.335±0.0570.415±0.041
205.0 kD
116.5kl)
80.0 kD
49.5 kD
Fig. 3. Immunoblot analysis of liver DPD from deficient patients and normal subjects.Each lane (/*/. 6, Pi. 2, and Normal Subject ) contains 200 /¿gof crude liver cytosol. M. W.,
molecular weight; kD, molecular weight in thousands.
potentially determining the resultant anticancer efficacy and/or toxicity of FUra. However, the clinical value of determination of DPDactivity has not been widely appreciated. This is due to limited knowledge of "normal" DPD activity in the general population and the
relationship between PBM-DPD and liver DPD, as well as the un
availability of a sensitive and reproducible assay. The major purposeof the present study was initially to develop and evaluate an assay thatcan be used in DPD screening and subsequently to determine thedistribution of DPD activity (in both PBM-DPD and liver DPD) in the
general population. Results from the present study suggest that measurement of DPD activity could be performed routinely in cancerpatients prior to FUra treatment.
The initial study optimized the assay conditions for determiningDPD activity. In subsequent studies evaluating storage conditions, wedemonstrated that the freezing process affected PBM-DPD initially
but no significant change in enzyme activity was observed duringstorage (at least for 1 month). This method has been demonstrated tobe sensitive, accurate, and precise. More importantly, DPD activity infresh and frozen samples was strongly correlated, permitting utilization of frozen samples in large scale screening in the general population and in routine testing in the clinic.
Prior to a large scale study of DPD activity in patients, one needsto clearly determine the population distribution of DPD activity andestablish criteria for identification of deficient patients. Furthermore,it is necessary to determine whether there are any differences in DPDactivity for different groups by sex, age, or race. In a study of cancerpatients. Milano et al. (33) reported a possible influence of sex onFUra clearance and suggested that it may be related to variations inDPD activity. However, a more recent study from the same laboratory(23) demonstrated no significant sex difference in DPD activity. It isworth noting that these results were obtained from a relatively smallsample of the cancer patient population consisting of 66 patients withonly 10 females being studied. In the present population study with124 subjects (45% males and 55% females), statistical analysis demonstrated a normal distribution of PBM-DPD activity with no signifi
cant difference among groups by sex, race, or age. These resultsenabled us to establish a baseline for future DPD screening in thegeneral population.
Since fresh samples are not always available, one also must establish a baseline for frozen samples. Despite the difference in absolutevalues of DPD activity, there was a strong correlation between freshand frozen samples. A normal distribution of DPD activity with frozensamples was also observed similar to that with fresh samples, permitting us to use frozen samples to determine DPD activity in cancerpatients (particularly from other institutions) and permitting establishment of criteria for identification of DPD deficiency.
5436
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DfD ACTIVITY AND FUra CHEMOTHERAPY
Given the wide use of FUra in the clinic and the presence of severetoxicity (including death) in patients with DPD deficiency, it would hedesirable to determine DPD activity in cancer patients prior to administration of FUra. Clinical investigations in the present study furthersupport this suggestion. In addition to three cases reported previouslyfrom this laboratory (19-21), we identified nine new patients with
profound or partial DPD deficiency in the present study, stronglysuggesting that DPD deficiency is more frequent than previouslythought. Using the established baseline for DPD activity, we suggestthat the lower limit of the 95% distribution range be used as a criterionfor identification of DPD deficiency.
Although the liver is thought to be the major site of FUra metabolism (34), it is not practical to directly determine liver DPD activity inpatients for diagnosis or research purposes. Since the number of freshhuman liver samples available for research purposes is limited, in thepresent study, we determined the baseline for human liver DPD usingfrozen liver tissues from "normal" donors. These samples appeared tobe free of disease and were rapidly frozen and kept at -70°C. The
DPD activity in frozen liver tissues had been shown previously in ourlaboratory to be stable at least for 2 years (data not shown). Theseresults are also consistent with a study with rat liver in our laboratory.4
We found no significant difference between fresh liver samples andfrozen samples (storage period from 1 week to 6 months). With 59"normal" liver samples, a baseline for liver DPD activity was deter
mined (Table 5), demonstrating no significant difference in race andage, while mean liver DPD activity of females was slightly higherthan that of males.
The present study is the first in which decreased liver DPD activitywas demonstrated in cancer patients with DPD deficiency initiallyidentified by PBM-DPD. More interestingly, there was a suggestedrelationship between liver DPD and PBM-DPD. Considering the similar population distribution pattern of PBM-DPD and liver DPD andthe above evidence, we suggest that PBM-DPD could be used as amarker for DPD activity in general. In the two DPD-deficient patients,
Western blot analysis demonstrated decreased DPD protein in the livercytosol compared with normal subjects. Further characterization ofthe DPD protein from these deficient patients is currently under investigation in our laboratory.
In addition to its obvious importance to DPD-deficient patients,
measurement of DPD activity is also potentially important in thetherapeutic use of FUra in other cancer patients as well. Theoretically,assay of DPD activity could be used to adjust the FUra dose to beadministered prior to or during treatment in order to improve theeffectiveness of FUra chemotherapy and/or decrease drug-related tox
icity. Further studies are needed to confirm the relationship betweenDPD activity and FUra therapeutic effectiveness and toxicity in cancerpatients, using a prospective pharmacoepidemiological study design.
Another potential use of measurement of DPD activity is related tothe use of DPD inhibitors. Several groups have suggested a role forDPD inhibitors in improving FUra effectiveness. Inhibition of DPDactivity has been shown to potentiate the effect of FUra both in vitroand in vivo (6, 15-18, 35-37). However, in light of the severe toxicity
in patients with DPD deficiency, caution, including DPD determination, should be used prior to administration of these DPD inhibitors inconjunction with FUra chemotherapy.
In summary, the DPD assay described in the present report is asensitive, accurate, and precise method that can be used in DPDscreening in cancer patients. DPD activity in the general populationfollows a normal distribution with no significant differences in sex,age, or race. Additional DPD-deficient patients have been identified,
suggesting that this pharmacogenetic syndrome is not rare. In considering the frequent use of FUra in cancer patients, severe FUra toxicity
4 Z. Lu, R. Zhang, and R. B. Diasio, unpublished data.
in DPD-deficient patients, and the potential value of the measurement
of DPD activity in improving FUra chemotherapy, we suggest that themeasurement of DPD activity could be routinely conducted in cancerpatients prior to or during FUra treatment. Further studies screeningthe frequency of DPD deficiency in the cancer patient population,prospectively determining the relationship between DPD activity andFUra effectiveness and/or toxicity, and the molecular basis for DPDdeficiency are currently under investigation in our laboratory.
ACKNOWLEDGMENTS
We thank H. Xiao and T. K. Krayer for their excellent technical assistance,Dr. T. Liu for assistance in statistical analysis, and the following medicaloncologists for their interest and collaboration in studies with cancer patients:Drs. J. Barton, G. Bjarnason, J. Carpenter, I. Gore, B. Greidcr, W. Haefeli, R.K. Hall, R. Hart, J. Herman, J. Jolivet, A. F. LoBuglio, R. Marsh, T. Miller, A.Miserez, F. M. Muggia, H. M. Rciman, S. M. Sugarman, S. J. Vukelja, L.
Weiselberg, and R. Wheeler.
REFERENCES
1. Chahncr, B. A., and Myers, C. E. Clinical pharmacology of cancer chemotherapy. In:V. T. De Vita, S. Hellman, and S. A. Rosenberg (eds.). Cancer—Principles and Practiceof Oncology, Ed. 3. pp. 349-395. Philadelphia: J. B. Lippincoll Company. 1989.
2. Grem, J. L. Fluorinated pyrimidines. In: B. A. Chabner and J. M. Collins (eds.).Cancer Chemotherapy: Principles and Practice, pp. 180-224. Philadelphia: J. B.
Lippincott Company. 1990.3. Diasio, R. B., and Harris, B. E. Clinical pharmacology of 5-fluorouracil. Clin. Phar-
macokinet., 16: 215-237, 1989.4. Daher. G. C., Harris, B. E., and Diasio, R. B. Metabolism of pyrimidine analogues and
their nucleosides. Pharmacol. Ther., 48: 189-222, 1990.5. Heggie, G. D., Sommadossi, J-P., Cross, D. S., Huster, W. J., and Diasio, R. B.
Clinical pharmacokinctics of 5-fluorouracil and its metabolites in plasma, urine, andbile. Cancer Res., 47: 2203-2206, 1987.
6. ligo. M., Araki, E., Nakajima, Y. Hoshi. A., and de Clercq, E. Enhancing effect ofbromovinyldeoxyuridine on antitumor activity of 5-fluorouracil against adenocarci-
noma 755 in mice: increased therapeutic index and correlation with increased plasma5-fluorouracil level. Biochem. Pharmacol.. 37: 1609-1613, 1988.
7. Harris. B. E., Song, R., Soong, S-j., and Diasio, R. B. Relationship between dihy-dropyrimidine dehydrogenase activity and plasma 5-fluorouracil levels with evidence
for circadian variation of enzyme activity and plasma drug levels in cancer patientsreceiving 5-fluorouracil by protracted continuous infusion. Cancer Res., 50: 197-201,
1990.8. Fleming, R. A., Milano, G., Thyss, A., Etienne. M-C., Renée,N., Schneider, M., and
Dcmard, F. Correlation between dihydropyrimidine dehydrogenase activity in peripheral mononuclear cells and systemic clearance of fluorouracil in cancer patients.Cancer Res., 52: 2899-29(12, 1992.
9. Goldberg, J. A., Ken, D. J., Willmott, N., McKillop, J. H., and McArdle, C. S.Pharmacokinetics and pharmacodynamics of locoregional 5-fluorouracil (5-FU) inadvanced colorectal liver métastases.Br. J. Cancer, 57: 186-189, 1988.
10. Daher, G. C., Harris, B. E., Zhang. R., Willard, E. M., Soong, S-j., and Diasio. R. B.
The role of dihydropyrimidine dehydrogenase (DPD) and thymidine phosphorylase(dThdPase) in the circadian variation of plasma drug levels of 5-fluorouracil (FUra)and 5-fluorodeoxyuridine (FdUrd) following infusion of FUra or FdUrd. Annu. Rev.Chronopharmacol., 7: 227-230, 1990.
11. Harris, B. E., Song, R., He, Y-J., Soong, S-j., and Diasio, R. B. Circadian rhythm of
rat liver dihydropyrimidine dehydrogenase, possible relevance to fluoropyrimidinechemotherapy. Biochem. Pharmacol., 37: 4759-4762, 1988.
12. Harris, B. E., Song, R., Soong. S-j., and Diasio, R. B. Circadian variation of 5-fluorouracil catabolism in isolated perfused liver. Cancer Res., 49: 6610-6614, 1989.
13. Daher, G. C.. Zhang, R., Soong, S-j.. and Diasio, R. B. Circadian variation offluoropyrimidine catabolic enzymes in rat liver: possible relevance to 5-fluorodcoxy-uridine chemotherapy. Drug Metab. Dispos., 19: 285-287, 1991.
14. Zhang. R.. Lu. Z.. Liu. T.. Soong, S-j.. and Diasio. R. B. Relationship betweencircadian-dependent toxicity of 5-fluorodeoxyuridine and circadian rhythms of pyrimidine enzymes: possible relevance to fluoropyrimidine chemotherapy. CancerRes., 53: 2816-2822, 1993.
15. Martin, D. S.. Nayak. P., Sawyer, R. C., Stolfi, R. L., Young, C. W.. Woodcock, T., andSpiegelman. S. Enhancement of 5-fluorouracil chemotherapy with emphasis on theuse of excess thymidine. Cancer Bull. (Houst.), 30: 219-224, 1978.
16. Wasternack, C. Degradation of pyrimidines and pyrimidine analogs—pathways andmutual influences. Pharmacol. Ther., 8: 629-665. 1980.
17. Daher, G. C., Naguib, F. N. M., el Kouni, M. H., Zhang, R., Soong, S-j., and Diasio,
R. B. Inhibition of fluoropyrimidine catabolism by benzyloxybenzyluracil. Possiblerelevance to regional chemotherapy. Biochem. Pharmacol.. •¿�//:1887-1893. 1991.
18. Porter, D. J. T.. Chestnut, W. G., Taylor, L. C. E., Merrill, B. M., and Spector, T.Inactivation of dihydropyrimidine dehydrogenase by 5-iodouracil. J. Biol. Chem.,266: 19988-19994, 1991.
19. Diasio, R. B., Beavers, T. L., and Carpenter, J. T. Familial deficiency of dihydropyrimidine dehydrogenase. J. Clin. Invest., HI: 47-51, 1988.
20. Harris, B. E., Carpenter, J. T.. and Diasio, R. B. Severe 5-fluorouracil toxicity
secondary to dihydropyrimidine dehydrogenase deficiency: a potentially more common pharmacogenetic syndrome. Cancer (Phila.), 68: 499-501, 1991.
5437
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

DPD ACTIVITY AND FUra CHEMOTHERAPY
21. Lyss, A. P., Lilenbaum, R. C., Harries, B. E., and Diasio, R. B. Severe 5-fluorouraciltoxicity in a patient with decreased dihydropyrimidine dehydrogenase activity. CancerInvest., ;;.' 239-240, 1993.
22. Tuchman, M., Stoeckeler, J. S., Kiang. D. T., O'Dea, R. F., Rammaraine, M. L., and
\lnMU. B. L. Familial pyrimidinemia and pyrimidinuria associated with severe fluo-rouracil toxicity. N. Engl. J. Med., 313: 245-249, 1985.
23. Fleming, R. A., Milano, G. A., Gaspard, M. H., Bargnoux, P. J., Thyss, A., Plagne, R.,Renée,N., Schneider, M., and Demard, F. Dihydropyrimidine dehydrogenase activityin cancer patients. Eur. J. Cancer, 29A: 740-744, 1993.
24. Shiotani, T., and Weber, G. Purification and properties of dihydrothymine dehydrogenase from rat liver. J. Biol. Chem., 256.- 219-224, 1981.
25. Fujimoto, S., Matsuda, K., Kikugama, M., Kaneko, M., and Tamak. N. Effect ofvitamin B2 deficiency on rat liver dihydropyrimidine dehydrogenase activity. J. Nutr.Sci. Vitaminol., 37: 89-98. 1991.
26. Podschun, B., Wahler, G., and Schnackerz, K. D. Purification of dihydropyrimidinedehydrogenase from pig liver. Eur. J. Biochem., 185: 219-224, 1989.
27. Naguib, F. N. M., el Kouni, M. H., and Cha, S. Enzymes of uracil catabolism innormal and neoplastic human tissues. Cancer Res., 45: 5405-5412, 1985.
28. Lu, Z., Zhang. R., and Diasio, R. B. Purification and characterization of dihydropyrimidine dehydrogenase from human liver. J. Biol. Chem., 267.' 17102-17109, 1992.
29. Lu, Z., Zhang, R., and Diasio, R. B. Comparison of dihydropyrimidine dehydrogenasefrom human, rat, pig, and cow liver. Biochemical and immunological properties.Biochem. Pharmacol., 46: 945-952, 1993.
30. Sommadossi, J-P., Gewirtz, D. A., Diasio, R. B., Aubert, C., Cano, J. P., and Goldman,I. D. Rapid catabolism of 5-fluorouracil in freshly isolated hepatocytes as analyzed by
high performance liquid chromatography. J. Biol. Chem., 257: 8171-8176, 1982.
31. Bradford, M. A. Rapid sensitive method for the quantitation of microgram qualities ofprotein utilizing the principle of protein-dye binding. Anal. Biochem., 72: 258-254,
1976.32. Towbin, H., Staehelin, T., and Gorden, J. Electrophoretic of proteins from polyacryl-
amide gels to nitrocellulose sheets: procedure and some applications. Proc. Nati.Acad. Sci. USA, 76: 4350-4354, 1979.
33. Milano, G., Etienne, M. C., Casssuto-Viguier, E., Thyss, A., Santini. J., Frenay, M.,
Renée,N., Schneider, M., and Demard, F. Influence of sex and age on fluorouracilclearance. J. Clin. Oncol., 10: 1171-1175.
34. Ho, D. H., Townsend, L., Luma, M. A., and Bodely. G. P. Distribution and inhibitionof dihydrouracil dehydrogenase activities in human tissues using 5-fluorouracil as asubstrate. Anticancer Res., 6: 781-784, 1986.
35. Desgranges, C., Razaka, G., De Clercq, E., Herdewijn, P., Balzarini, J., Drouillet, F.,and Bricaud, H. Effect of (E")-5-(2-bromovinyl)uracil on the catabolism and antitumor
activity of 5-fluorouracil in rats and leukemic mice. Cancer Res.. 46: 1094-1101,
1986.36. Masaaki. I., Araki, E., Nakajima, Y., and De Clercq, E. Enhancing effects of bro-
movinyldeoxyuridine on anlitumor activity of 5-fluorouracil against adenocarcinoma
755 in mice. Increased therapeutic index and correlation with increased plasma5-fluorouracil levels. Biochem. Pharmacol., 37: 1609-1613, 1988.
37. Naguib, F. N. M., el Kouni, M. H., and Cha, S. Structure-activity relationship of
ligands of dihydrouracil dehydrogenase from mouse liver. Biochem. Pharmacol., 3fl:1471-1480, 1989.
5438
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1993;53:5433-5438. Cancer Res Zhihong Lu, Ruiwen Zhang and Robert B. Diasio 5-Fluorouracil ChemotherapyNewly Identified Deficient Patients, and Clinical Implication inBlood Mononuclear Cells and Liver: Population Characteristics, Dihydropyrimidine Dehydrogenase Activity in Human Peripheral
Updated version
http://cancerres.aacrjournals.org/content/53/22/5433
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/53/22/5433To request permission to re-use all or part of this article, use this link
on April 8, 2021. © 1993 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from