Digestive and Liver Disease - COnnecting REpositories · Digestive and Liver Disease 47 (2015) ......
10
Digestive and Liver Disease 47 (2015) 181–190 Contents lists available at ScienceDirect Digestive and Liver Disease jou rnal h om epage: www.elsevier.com/locate/dld Review Article Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome Amedeo Lonardo a,∗ , Stefano Ballestri b , Giulio Marchesini c , Paul Angulo d , Paola Loria a a AUSL Modena and University of Modena and Reggio Emilia, Department of Biomedical, Metabolic and Neural Sciences, Division of Internal Medicine, NOCSAE – Baggiovara, Modena, Italy b AUSL Modena, Department of Internal Medicine, Division of Internal Medicine, Hospital of Pavullo, Pavullo nel Frignano, Italy c “Alma Mater Studiorum” University, Unit of Metabolic Diseases and Clinical Dietetics, Bologna, Italy d University of Kentucky, Division of Digestive Diseases & Nutrition, Section of Hepatology, Medical Center, Lexington, KY, USA a r t i c l e i n f o Article history: Received 30 April 2014 Accepted 21 September 2014 Available online 18 November 2014 Keywords: Dissociation Insulin resistance Natural history Pathogenesis a b s t r a c t The conventional paradigm of nonalcoholic fatty liver disease representing the “hepatic manifestation of the metabolic syndrome” is outdated. We identified and summarized longitudinal studies that, suppor- ting the association of nonalcoholic fatty liver disease with either type 2 diabetes mellitus or metabolic syndrome, suggest that nonalcoholic fatty liver disease precedes the development of both conditions. Online Medical databases were searched, relevant articles were identified, their references were further assessed and tabulated data were checked. Although several cross-sectional studies linked nonalcoholic fatty liver disease to either diabetes and other components of the metabolic syndrome, we focused on 28 longitudinal studies which provided evidence for nonalcoholic fatty liver disease as a risk factor for the future development of diabetes. Moreover, additional 19 longitudinal reported that nonalcoholic fatty liver disease precedes and is a risk factor for the future development of the metabolic syndrome. Finally, molecular and genetic studies are discussed supporting the view that aetiology of steatosis and lipid intra-hepatocytic compartmentation are a major determinant of whether fatty liver is/is not associated with insulin resistance and metabolic syndrome. Data support the novel paradigm of nonalcoholic fatty liver disease as a strong determinant for the development of the metabolic syndrome, which has potentially relevant clinical implications for diag- nosing, preventing and treating metabolic syndrome. © 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. 1. Introduction Steatosis and steatohepatitis, in the absence of competing aeti- ologies such as high alcohol intake, hepatitis C virus (HCV) infection, drugs and other endocrine disorders, are both part of the nonalco- holic fatty liver disease (NAFLD) spectrum [1–3]. NAFLD may either occur in the absence of fatty changes – and is often alluded to either as “cryptogenic” or nonalcoholic steatohepatitis (NASH)-cirrhosis [4,5] – or encompass hepatic and extra-hepatic complications, from hepatocellular carcinoma to atherosclerosis [6]. NAFLD is presently recognized as one the most common causes of altered liver tests, of end-stage liver disease requiring liver transplantation, and is ∗ Corresponding author at: Division of Internal Medicine, NOCSAE – Baggiovara, Via Giardini 1135, 4100 Modena, Italy. Tel.: +39 0593961807; fax: +39 0593961322. E-mail addresses: [email protected], [email protected] (A. Lonardo). frequently associated with the constellation of clinico-laboratory features that comprise the metabolic syndrome [7–9]. The metabolic syndrome is a cluster of cardio-metabolic condi- tions, generally triggered by an expansion of the adipose visceral tissue [10], which include insulin resistance – with or without impaired glucose metabolism and type 2 diabetes (T2D) – athero- genic dyslipidemia [low high density lipoprotein (HDL)-cholesterol and high triglycerides], and high blood pressure [11]. The present definition of metabolic syndrome, at variance with one of its earliest proposals [12], does not include hepatic steatosis despite evidence supporting this association [13]. The existence and the utility of metabolic syndrome as a separate entity has been challenged by some experts [14]. Moreover, it remains controversial whether the presence of the full-blown syndrome really adds to the cardiovas- cular risk dictated by its individual components, particularly T2D [15,16]. Nevertheless, the single traits of the metabolic syndrome tend to aggregate in the same individuals and, more importantly, the presence of each of them often anticipates the appearance of http://dx.doi.org/10.1016/j.dld.2014.09.020 1590-8658/© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. Open access under CC BY-NC-ND license. Open access under CC BY-NC-ND license.
Transcript of Digestive and Liver Disease - COnnecting REpositories · Digestive and Liver Disease 47 (2015) ......

R
Ns
Aa
Nb
c
d
a
ARAA
KDINP
1
odhoa[hro
V
h1
Digestive and Liver Disease 47 (2015) 181–190
Contents lists available at ScienceDirect
Digestive and Liver Disease
jou rna l h om epage: www.elsev ier .com/ locate /d ld
eview Article
onalcoholic fatty liver disease: A precursor of the metabolicyndrome
medeo Lonardoa,∗, Stefano Ballestrib, Giulio Marchesini c, Paul Angulod, Paola Loriaa
AUSL Modena and University of Modena and Reggio Emilia, Department of Biomedical, Metabolic and Neural Sciences, Division of Internal Medicine,OCSAE – Baggiovara, Modena, ItalyAUSL Modena, Department of Internal Medicine, Division of Internal Medicine, Hospital of Pavullo, Pavullo nel Frignano, Italy“Alma Mater Studiorum” University, Unit of Metabolic Diseases and Clinical Dietetics, Bologna, ItalyUniversity of Kentucky, Division of Digestive Diseases & Nutrition, Section of Hepatology, Medical Center, Lexington, KY, USA
r t i c l e i n f o
rticle history:eceived 30 April 2014ccepted 21 September 2014vailable online 18 November 2014
eywords:issociation
nsulin resistanceatural historyathogenesis
a b s t r a c t
The conventional paradigm of nonalcoholic fatty liver disease representing the “hepatic manifestation ofthe metabolic syndrome” is outdated. We identified and summarized longitudinal studies that, suppor-ting the association of nonalcoholic fatty liver disease with either type 2 diabetes mellitus or metabolicsyndrome, suggest that nonalcoholic fatty liver disease precedes the development of both conditions.
Online Medical databases were searched, relevant articles were identified, their references were furtherassessed and tabulated data were checked.
Although several cross-sectional studies linked nonalcoholic fatty liver disease to either diabetes andother components of the metabolic syndrome, we focused on 28 longitudinal studies which providedevidence for nonalcoholic fatty liver disease as a risk factor for the future development of diabetes.Moreover, additional 19 longitudinal reported that nonalcoholic fatty liver disease precedes and is a riskfactor for the future development of the metabolic syndrome.
Finally, molecular and genetic studies are discussed supporting the view that aetiology of steatosis
and lipid intra-hepatocytic compartmentation are a major determinant of whether fatty liver is/is notassociated with insulin resistance and metabolic syndrome.Data support the novel paradigm of nonalcoholic fatty liver disease as a strong determinant for thedevelopment of the metabolic syndrome, which has potentially relevant clinical implications for diag-nosing, preventing and treating metabolic syndrome.© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd.
ND lic
. Introduction
Steatosis and steatohepatitis, in the absence of competing aeti-logies such as high alcohol intake, hepatitis C virus (HCV) infection,rugs and other endocrine disorders, are both part of the nonalco-olic fatty liver disease (NAFLD) spectrum [1–3]. NAFLD may eitherccur in the absence of fatty changes – and is often alluded to eithers “cryptogenic” or nonalcoholic steatohepatitis (NASH)-cirrhosis4,5] – or encompass hepatic and extra-hepatic complications, fromepatocellular carcinoma to atherosclerosis [6]. NAFLD is presently
Open access under CC BY-NC-
ecognized as one the most common causes of altered liver tests,f end-stage liver disease requiring liver transplantation, and is
∗ Corresponding author at: Division of Internal Medicine, NOCSAE – Baggiovara,ia Giardini 1135, 4100 Modena, Italy. Tel.: +39 0593961807; fax: +39 0593961322.
E-mail addresses: [email protected], [email protected] (A. Lonardo).
ttp://dx.doi.org/10.1016/j.dld.2014.09.020590-8658/© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd.
Op
frequently associated with the constellation of clinico-laboratoryfeatures that comprise the metabolic syndrome [7–9].
The metabolic syndrome is a cluster of cardio-metabolic condi-tions, generally triggered by an expansion of the adipose visceraltissue [10], which include insulin resistance – with or withoutimpaired glucose metabolism and type 2 diabetes (T2D) – athero-genic dyslipidemia [low high density lipoprotein (HDL)-cholesteroland high triglycerides], and high blood pressure [11]. The presentdefinition of metabolic syndrome, at variance with one of its earliestproposals [12], does not include hepatic steatosis despite evidencesupporting this association [13]. The existence and the utility ofmetabolic syndrome as a separate entity has been challenged bysome experts [14]. Moreover, it remains controversial whether thepresence of the full-blown syndrome really adds to the cardiovas-
ense.
cular risk dictated by its individual components, particularly T2D[15,16]. Nevertheless, the single traits of the metabolic syndrometend to aggregate in the same individuals and, more importantly,the presence of each of them often anticipates the appearance of
en access under CC BY-NC-ND license.

182 A. Lonardo et al. / Digestive and Liver Disease 47 (2015) 181–190
Table 1Nonalcoholic fatty liver disease and metabolic syndrome – the original spectrum of similarities.
Steatosis Metabolic syndrome
EpidemiologyPrevalence in the general population Up to 25% of adults Epidemic in the elderlyPrevalence grows with age Yes Strongly age-dependentMales more affected Yes (adults, children) Yes
AnthropometryAssociation with central obesity Abdominal adiposity is an independent predictor Visceral fat is correlated with Insulin response and dyslipidemia
Metabolism – Association withHyperinsulinemia Documented Pathogenic mainstayHypertension In drinkers and non-drinkers YesObesity Yes YesHypertriglyceridemia Yes YesLow HDL Cholesterol Circumstantial Evidence Yes
Clinical featuresSystemic disease Yes YesAccelerated atherogenesis Circumstantial Evidence YesResponse to diet and/or exercise In the obese Yes
Experimental pathology
A
ascmm
ibdd(oaNmit
aandcptoadtN
2
i““rgr
ct
Animal Models (rat) Atherogenic diet induces steatosis
dapted from Lonardo [20].
dditional components over time [17]. This, together with the pos-ible progression to organ failure and of the development of someancer types, including primary liver cancer [9,11,18,19], makesetabolic syndrome a relevant condition in clinical practice and aajor public health concern worldwide.In 1999, European researchers [20–22] provided biological, clin-
cal and epidemiological evidence for the theory that NAFLD shoulde regarded as the hepatic manifestation of the metabolic syn-rome (Table 1) [20]. Since then, a “chicken and egg” scientificebate has arisen, concerning the primacy of metabolic syndromeand insulin resistance) over NAFLD or, conversely, of NAFLDver the metabolic syndrome [23]. Moreover, while most studiescknowledge NAFLD to be a risk factor for T2D [24], the notion thatAFLD anticipates the future development of components of theetabolic syndrome other than T2D is far less accepted, although
t has been suggested by few authors [23,25,26] mainly based onheir expert opinion.
In our systematic review of the literature, we discuss all avail-ble data supporting the view that NAFLD, rather than being
mere “manifestation of the metabolic syndrome” is indeed aecessary precursor of the future development of metabolic syn-rome in humans. To this end, further to identifying all relevantross-sectional studies, we specifically address the evidence fromrospective studies showing that NAFLD is an independent risk fac-or for the future development of both T2D and other componentsf the metabolic syndrome. Methodological limitations of such datare briefly analysed. Finally, we discuss how some examples ofissociation of NAFLD from metabolic syndrome – seemingly con-radicting our thesis – eventually confirm the general paradigm ofAFLD being a precursor of the metabolic syndrome.
. Research strategy
The PubMed data base was manually searched for the follow-ng terms: “Metabolic syndrome”; “Type 2 Diabetes”; “Obesity”;Dyslipidemia” “Hyperlipidemia”; “Insulin resistance”; “Predictor”;Fatty liver”; “Follow-up”; “Association” and “Dissociation”. Theesearch was updated at the 28th of April 2014. Further biblio-raphic updates were performed whenever needed during the
evision process.All of the identified articles and their references were furtherhecked in duplicate in order to identify appropriate articles. Per-inent studies were identified as a result of the agreement two
Hypertensive animals have hyperinsulinemia and hypertriglyceridemia
investigators, who also tabulated the methods and chief findingsof the selected material.
The accuracy of the tabulated data was independently per-formed by all authors.
3. Association of NAFLD with other conditions
3.1. Type 2 diabetes
Many cross-sectional studies demonstrate that NAFLD is asso-ciated with insulin resistance/pre-diabetes/T2D [27–39]. Despitea variable follow-up range, data appear consistent in disclosingthat the “NAFLD pathway” to T2D follows a route characterizedby insulin resistance developing at various anatomic sites, notablyincluding hepatic insulin resistance. Interestingly, the NAFLD-T2D association occurs irrespective of potential confounders andparticularly obesity and moderate alcohol drinking, suggestingthat NAFLD may closely mirror the development of fatty pan-creas disease [40] and thus reflect tissue lipotoxicity. Moreover, aquantitative relationship links fasting plasma glucose with NAFLDprevalence: the higher the former, the higher the latter [29].However, widely acknowledged predictors of T2D in non-NAFLDpopulations (such as high fasting glucose and low HDL-cholesteroland adiponectin, mirroring insulin resistance) and low physicalactivity also predict T2D in NAFLD suggesting that NAFLD prob-ably amplifies the physiological determinants of T2D. Finally, mostfindings appear to be confirmed irrespective of ethnicity (e.g.T2D-prone Asians vs. Caucasians) and of the diagnostic techniquefollowed to capture NAFLD, spanning from the most invasive oraccurate tests (liver histology, magnetic resonance imaging) to themost insensitive (liver tests), via the most widely performed ultra-sonography scanning.
However, the above studies [27–39] are cross-sectional. Accord-ingly, they do not rule out the possibility that primarily impairedgluco-regulation may eventually result in the development ofNAFLD. In order to clarify this issue, in Supplementary Table S-1the studies showing NAFLD as a risk factor for the future devel-opment of T2D were summarized. Eleven out of 12 studies wereconducted in Far East, most of them from Korea. With such a
limitation, they confirm that NAFLD is an independent risk factorfor the development of T2D, although confirmation from Westerncountries appears necessary. Moreover, the diagnostic techniqueused to detect NAFLD may lead to different results. For instance,
A. Lonardo et al. / Digestive and Liver Disease 47 (2015) 181–190 183
Table 2Nonalcoholic fatty liver disease and metabolic syndrome – the expanded spectrum of similarities.
NAFLD Metabolic syndrome
Increasing serum uric acid levels Are associated with increased prevalence and histologicalseverity of NAFLD [66–68]
Are associated with increased prevalence and incidence ofmetabolic syndrome [69–82]
High fructose consumption Is associated with increased prevalence of NAFLD andincreased NASH severity [83,84] owing to enhancedlipogenesis, hepatic fibrosis, inflammation, endoplasmicreticulum stress and lipoapoptosis [85]
Increases the risk of developing metabolic syndrome andits components [86–88]
TSH Clinical/subclinical hypothyroidism and elevated TSH,though in the normal range, are associated with increasedprevalence and histological severity of NAFLD [89–92]
There is a close dose-dependent relationship betweenincreasing TSH and incident/prevalent metabolicsyndrome in various ethnicities and across differentage-groups [93–97]
Bile acids Participate in the pathogenesis of NAFLD throughregulating hepatic nutrients and energy homeostasis;stimulating GLP-1 secretion in the small intestine andenergy expenditure in brown adipose tissue and skeletalmuscle [98]. UDCA’s role in NASH management, however,remains controversial [99,100]
Are powerful regulators of metabolism and induceincreased thermogenesis, protect from diet inducedobesity, hepatic lipid accumulation, and increased plasmatriglyceride and glucose levels via activation of Bile acidsreceptors (FXR and TGR5) [101–103]
Increased physical exercise Protects from NAFLD, independent of weight loss[104–108] and improves histological steatosis [109]
Protects from the development of and cures establishedmetabolic syndrome [110–116]
Light to moderate alcohol consumption Is associated with a reduced prevalence of NAFLD andNASH [3,117–120]
Seemingly protects from the development of at least somecomponents of the metabolic syndrome. Conversely, heavydrinking increases the risk of metabolic syndrome[121–132]
Caffeine Seemingly protects from NAFLD and liver fibrosis[133–136] without decreasing the risk of NASH [134,135].Beneficial liver outcomes are mediated by antioxidant,antifibrogenic, antinflammatory, insulin sensitizing,lipolytic, cyto, and genoprotective activity [137–142]
Reported to be a protective factor from metabolicsyndrome, maybe through a lipolytic effects of caffeine onadipocytes [143–145].
Smoking Risk factor for the development of NAFLD and its fibroticprogression [146–148]
Positively and reversibly associated in a dose-dependentmanner with the risk of metabolic syndrome [149]
Altered sleep physiology Shorter sleep duration and severe obesity-relatedobstructive sleep apnoea are independently associatedwith development and histological severity of NAFLD[150–152]
Altered sleeping time duration and continuity areassociated with increased risk for the metabolic syndrome[150,153–156]
Brown adipose tissue Subjects maintaining active brown adipose tissue areprotected from NAFLD [157]
The presence of brown adipose tissue is inversely relatedto BMI. Brown adipose tissue activity plays a role inconstitutional leanness without affecting glucosemetabolism [158–161]
Intestinal microbiota May promote NASH by several mechanisms includingimproved energetic efficiency; increased gut permeabilityand production of lipopolysaccharides with activation ofthe innate immune system; altered bile acids pool;reduced bioavailability of dietary choline and increasedendogenous ethanol production [162–172]
Plays a significant role in the development of metabolicsyndrome via increased energy harvesting, metabolicendotoxinemia; control of lipid and glucose metabolismvia the composition of bile-acid pools and the modulationof FXR and TGR5 signalling; modulation of intestinalmicrobial composition by innate immune system;“brain-gut enteric microbiota axis” [170,173–188]
Vitamin D deficiency Is associated with NAFLD development and the severity ofhepatic histological changes [189–192]
May increase the risk for metabolic syndrome, type 2diabetes, insulin resistance, obesity, hypertension and
L on-lika d stim
talasHai
3
v[lst
amt
ist of abbreviations: BMI, body mass index; FXR, farnesoid X receptor; GLP-1, glucagtitis; TGR5, membrane-type G-protein-coupled receptor for bile acids; TSH, thyroi
he less specific gamma-glutamyltransferase (GGT) values moreccurately predict the development of T2D than aminotransferaseevels. Similarly, the ultrasonographic severity of NAFLD is associ-ted with increasing risks of T2D and, notably, NASH (more thanimple steatosis) appears to be more closely associated with T2D.owever, such a conclusion was challenged by a subsequent meta-nalysis by Musso et al. showing that the risk of developing T2D isncreased to a similar extent in both steatosis and NASH [41].
.2. Other components of metabolic syndrome
Data reporting NAFLD as a risk factor for either some indi-idual components of metabolic syndrome [arterial hypertension42,43] and dyslipidemia [44]] or the full-blown syndrome areess established than NAFLD progression to T2D. Many cross-ectional studies support the view that NAFLD is associated withhe metabolic syndrome [13,22,45–64].
Data universally confirm the strong NAFLD-metabolic syndromessociation in humans. In addition, although each component ofetabolic syndrome [including serum uric acid, not included in
he diagnostic criteria but clearly a component of the syndrome
cardiometabolic outcomes [193–198]
e peptide-1; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcholic steatohep-ulating hormone; UDCA, ursodeoxycholic acid.
from a pathophysiological point of view [8]] is independently asso-ciated with NAFLD, a few features (visceral obesity, dyslipidemiaand insulin resistance/T2D) are more closely related to NAFLD.The association of NAFLD with the metabolic syndrome appearsto be stronger in lean than in obese individuals, especially inwomen. NAFLD specifically anticipates the presence of metabolicdisorders and independently predicts insulin resistance, identify-ing those individuals with insulin resistance who may be missed bymetabolic syndrome criteria in certain populations. The frequencyof metabolic syndrome significantly increases with quintiles of ALTand GGT, even within the normal range of these enzymes [51].Moreover, T2D and hypertriglyceridemia are more commonly asso-ciated with raised hepato-biliary enzymes, and particularly GGT[65], an association which appears to be independently mediatedby insulin resistance. In turn, the presence of metabolic syndromeis associated with the development of fibrosis or NASH.
Again, association in cross-sectional studies does not provide
evidence as to which condition comes first. In order to address thisissue, studies supporting the view that NAFLD precedes the devel-opment of metabolic syndrome are summarized in SupplementaryTable S-2.
1 d Live
rsatototfisFdt(
4r
ultnsht[dc
wd[crBic[tntttoacasgm
tpdisoclgog
84 A. Lonardo et al. / Digestive an
Collectively, they suggest that NAFLD, either diagnosed via sur-ogate indices or by ultrasonography, antedates the presence ofeveral components of metabolic syndrome, not only of T2D. Thisssociation is largely regulated by the presence of insulin resis-ance. However, in 13 out of 15 such studies, NAFLD was diagnosedn surrogate laboratory indices, on ultrasonographic findings inwo and in none by the gold standard liver biopsy technique. More-ver, the diagnostic criteria tended to be heterogeneous and givenhat enlarged waist circumference is both a main pathogenic keyor NAFLD and is central for the diagnosis of metabolic syndrome, its virtually impossible to rule out the possibility that visceral obe-ity links the development of both NAFLD and metabolic syndrome.inally, no specific traits of the metabolic syndrome (dysglicemia,yslipidemia, high blood pressure and central obesity) are manda-ory for the development of the full-blown metabolic syndromeSupplementary Table S-2).
. Does NAFLD precede metabolic syndrome? Insulinesistance as a major player
Compared to our “historical” perception (Table 1), presentnderstanding of the epidemiological, clinical and pathogenic simi-
arities between NAFLD and the metabolic syndrome has expandedo a substantial extent. Accordingly, it presently embraces a largeumber of risk/protective factors and biological mediators, i.e.,erum uric acid, fructose, TSH, bile acids, physical exercise, alco-ol, caffeine, smoking, altered sleep physiology, brown adiposeissue, intestinal microbiota and vitamin D deficiency (Table 2)66–198]. Associations of these factors with NAFLD may mirrorifferent pathophysiological mechanisms underlying the naturalourse leading from NAFLD to metabolic syndrome.
Phylogenetically evolved to promote survival, insulin resistanceill lead to the deleterious manifestations of the metabolic syn-rome whenever inappropriately activated by unhealthy lifestyles199]. Clinically, insulin resistance is defined as the criticalonnector linking stress, visceral adiposity, and decreased cardio-espiratory fitness with increased cardiovascular disease [14].iologically, elevated fasting glucose will result from hepatic
nsulin resistance, whereas increased free fatty acids (FFA) con-entrations are the expression of peripheral insulin resistance200]. At molecular level, insulin resistance invariably results fromhe interaction of cell membrane receptors with either excessutrients or inflammatory cytokines. Such an interaction willrigger JNK and IKK, protein kinase C, S6K, mTOR, and ERK. Allhese pathways are involved in the amplification of inflamma-ion, phosphorylation of insulin receptor substrates 1 and 2, stressf endoplasmic reticulum, production of reactive oxygen speciesnd mitochondrial dysfunction [201]. Once triggered, this viciousircle of systemic metabolic dysfunction of insulin and leptinction tends to self-perpetuate [202]. Impaired intracellular insulinignalling will eventually result in perturbed Glut-4-mediatedlucose uptake with preserved/potentiated MAP kinase-mediateditogenesis/cell survival pathways [200].First proposed, as early as 1988, as the underlying factor in
he metabolic syndrome [203], insulin resistance undoubtedlylays a major role in the pathophysiology of the metabolic syn-rome [204]. The expansion of visceral adipose tissue will result
n the liver being overflowed with FFA, thus leading to steato-is. A fatty liver, in turn, is the prerequisite for the developmentf highly atherogenic dyslipoproteinemia featuring low HDL-holesterol, hypertriglyceridemia and increased small and dense
ow-density lipoprotein (LDL) particles, as well as for fasting hyper-lycemia, which stimulates the pancreas to compensatory insulinver-secretion. Collectively, increased FFA concentrations, hyper-lycemia and hyper-insulinemia may directly (or indirectly viar Disease 47 (2015) 181–190
sympathetic over-activation) promote arterial hypertension andectopic deposition of fat in extra-adipose tissues. More importantly,the described metabolic derangements are intimately associatedwith increased production of fibrinogen, PAI-1, TNF-alpha, IL-6 anddecreased adiponectin levels. A subclinical pro-inflammatory pro-atherogenic state will ensue, which is a major biological feature ofinsulin resistance and a typical hallmark of the metabolic syndrome[204].
While most individuals with NAFLD have insulin resistance[13,205], only a minority of those with NAFLD exhibit the full-blown metabolic syndrome [206]. This finding most likely resultsfrom fatty liver being a precursor [207] and a necessary prerequisiteto the development of progressive metabolic disease [23,208–210].Adipose tissue is the only physiologic reservoir of fatty acids, andthe accumulation of fat in the extra-adipose tissues may be tissue-damaging and eventually lead to organ dysfunction (a conceptalluded to as “lipotoxicity”). Data from a mouse model support theview of fatty liver being a protective mechanism which preventsprogressive liver damage in NAFLD [211] suggesting that esterifica-tion into triglycerides might well be a mechanism which detoxifieshistologically damaging FFA in the liver. Further evidence for theconcept that fatty liver is an adaptive phenomenon derives from itsoccurrence in animal species other than humans suggesting thatsteatosis is evolutionarily “useful” [212–215].
Characterization of the role of PKC� is probably the most excitingprogress in our understanding of the molecular pathogenesis of theconnection linking liver steatosis with hepatic insulin resistance.In obese humans, fatty substrates such as diacylglycerol accountfor 64% of the variability of insulin sensitivity via the activationof PKC� [216], which impairs insulin signalling as shown in ratsusing antisense oligonucleotides [217]. Of outstanding interest, theintracellular compartmentation of diacylglycerol dictates whetheror not PKC� will translocate to the plasma membrane so promotinghepatic insulin resistance [218]. Stated otherwise, various classes oflipids (such as mono-, di- and tri-acylglycerol) sequestered withinlipid droplets/Endoplasmic reticulum fraction are deemed to beinnocuous as far as the development of hepatic insulin resistanceis concerned in the CGI-58 knockdown mouse model [219].
In humans, however, most cases of NAFLD are stronglyassociated with insulin resistance. In agreement, diacylglycerolacyltransferase 2 (DGAT2), the enzyme catalysing the final stepin the biosynthesis of triglycerides, may link glycemia and triglyc-eridemia [220]. These data are fully consistent with the view thatthe development of a fatty liver occurs upstream in the chain ofmetabolic events eventually leading to the development of themetabolic syndrome [210] and help understand the mechanisticreason why subjects with NAFLD were 1.6 times more likely todevelop T2D than NAFLD-free persons in a recent 3-year follow-up Japanese study [221]. Of clinical interest, a growing numberof components of the metabolic syndrome are associated with anincreased risk of hepatic fibrosis in the individual patient [222]thus enabling the identification of those who should undergo liverbiopsy [223]. In particular, data have shown that a vicious cir-cle links T2D and liver disease, with NAFLD contributing to thefuture development of T2D and the latter triggering progressiveliver injury [40]. Fatty pancreas develops in the setting of metabolicsyndrome, carrying amazing similarities to NAFLD in terms of organinflammation, end-stage organ failure, susceptibility to cancer andpost-surgical complications [224].
Lipid droplets display a unique protein repertoire includingAdipophilin and TIP47 which, further to fatty adipocytes, areexpressed in lipid droplets of hepatic stellate cells. Perilipin, once
deemed to be characteristic of lipid droplets in the adipocytes andsteroidogenic cells, is expressed de novo in liver cells of steatoticliver in humans [225]. The finding that the distribution of perilipinis predominantly perivenous in the liver lobule [225] may suggest
A. Lonardo et al. / Digestive and Liver Disease 47 (2015) 181–190 185
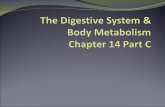
Fig. 1. Primacy of nonalcoholic fatty liver disease over metabolic syndrome. Based on epidemiological and biological data discussed in the text, the cartoon schematicallyi etabos a pao lets inb
anpoi
ideri
ad
5m
scrruos[hc(Oac
an
llustrates the theory of nonalcoholic fatty liver disease being the precursor of myndrome, uric acid is definitely a trait of the metabolic syndrome constellation fromf nonalcoholic fatty liver disease, as discussed in Table 2. The key-role of lipid dropased on recently published data [218,219].
specific role of this protein in the four-step model of histoge-etic events originally proposed by Wanless to account for NASHathogenesis and its progression to cirrhosis via hepatic venularbstruction [226]. Perilipin has been confirmed by following stud-es as one of the most prominent upregulated genes in NAFLD [227].
In summary, alterations in the regulation of lipid droplets phys-ology and metabolism influence the risk of developing metaboliciseases such as T2D and NAFLD [227]. Fig. 1 illustrates the hypoth-sis that NAFLD is a precursor of the metabolic syndrome via insulinesistance resulting from PKC� activation which conceivably occursn most cases of NAFLD in humans.
If the “general rule” is that steatosis and insulin resistance aressociated, are there any examples of such two conditions beingissociated from each other?
. Dissociation of NAFLD from insulin resistance and theetabolic syndrome
The first clinical evidence for conditions where high-gradeteatosis occurs without insulin resistance or low-grade liver fatontent is nonetheless associated with insulin resistance waseported in 2006. This conclusion was reached by comparing insulinesistance (assessed by HOMA-IR) and steatosis grade in three nat-rally occurring different conditions displaying a variable extentf steatosis: familial hypobetalipoprotenemia (FHBL), NAFLD andteatosis (evaluated histologically) associated with HCV infection228]. In 2010 Amaro et al. measuring insulin resistance with theyperinsulinemic-euglycemic clamp procedure coupled with glu-ose tracer infusion and liver fat content with magnetic resonanceMR) spectroscopy, confirmed the results in FHBL individuals [229].f interest, circumstantial evidence suggests that FHBL is associ-ted with progressive liver disease only in those patients featuring
omponents of the metabolic syndrome [230].Consistent with the potential occurrence of steatosis dissoci-ted from insulin resistance, Kantartzis et al. reported that singleucleotide polymorphisms in the diacylglycerol acyltransferase 2
lic syndrome. Although not included in current diagnostic criteria of metabolicthophysiological point of view and a determinant of development and progression
potentially protecting fatty liver from developing insulin resistance is highlighted
(DGAT2) gene accounted for variability in liver fat content ratherthan for insulin resistance. These results confirm and extendto humans the finding that DGAT2 mediates the dissociationbetween fatty liver and insulin resistance [231]. The same groupof researchers reported that the patatin-like phospholipase 3 gene(PNPLA3) is a key factor in determining whether fatty liver is associ-ated or not with metabolic derangements such as insulin resistance[232].
Finally, PNPLA3 gene polymorphisms have recently been associ-ated with those NAFLD cases occurring in the absence of metabolicsyndrome [233], indirectly suggesting that genetic conditionswhich promote the development of fatty changes in the liver mayoccur independently of insulin resistance.
A detailed survey of those studies demonstrating a dissocia-tion of fatty liver and T2D in both experimental conditions andhumans has recently been published by Sun et al. [234]. Collec-tively, findings from both genetically engineered animal modelsand humans with genetic conditions confirm the view that the aeti-ology of steatosis is a major determinant of whether steatosis isassociated (such as seen in most cases of NAFLD observed in clin-ical practice) or dissociated from insulin resistance and featuresof the metabolic syndrome (such as seen in NAFLD occurring incarriers of PNPLA3 gene polymorphisms and in FHBL individuals)[228,233,234]. As schematically depicted in Fig. 1, compartmenta-tion of intrahepatocytic lipids may potentially account for the endresult of NAFLD being either associated or dissociated from insulinresistance [218,219] and therefore from the risk of developingthe metabolic syndrome. Once fully characterized in humans, thesub-cellular mechanisms of dissociation of steatosis from insulinresistance may become a preferential target for the prevention andmanagement of insulin resistance and the metabolic syndrome.
6. Conclusions
A systematic review of the literature shows that the presence ofNAFLD is intimately linked with the metabolic syndrome, including

1 d Live
Toriasabi
topaps
CN
A
Laa
A
t
R
86 A. Lonardo et al. / Digestive an
2D. Moreover, NAFLD is a strong determinant for the future devel-pment of the metabolic syndrome. This is likely to occur as aesult of its being a key factor associated with insulin resistancen naturally occurring conditions in humans. Exceptions to such
theory are found in some genetic polymorphisms where theteatosis-insulin resistance-metabolic syndrome triad is dissoci-ted in humans. The molecular biology of events dictating NAFLDeing associated with or dissociated from insulin resistance is
ncreasingly being elucidated.On these grounds, the diagnostic importance of NAFLD as a cri-
erion for the presence, as well as for risk of future developmentf metabolic syndrome, needs to be emphasized. From a thera-eutic point of view, those pathogenic-based interventions aimedt reversing NAFLD are likely to be a rational approach in therevention and treatment of hepatic insulin resistance, metabolicyndrome and related complications.
onflict of interestone declared.
cknowledgement
This article is devoted to the memory of late Professor Paolaoria, M.D. The authors are grateful to Dr Leon Adams for invaluabledvice and thank Elisa Gibertini for kind assistance as a graphicrtist.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at http://dx.doi.org/10.1016/j.dld.2014.09.020.
eferences
[1] Angulo P. Non-alcoholic fatty liver disease. New England Journal of Medicine2002;346:1221–31.
[2] Marchesini G, Marzocchi R. Metabolic syndrome and NASH. Clinics in LiverDisease 2007;11:105–17.
[3] Nascimbeni F, Pais R, Bellentani S, et al. From NAFLD in clinical practice toanswers from guidelines. Journal of Hepatology 2013;59:859–71.
[4] Caldwell SH, Crespo DM. The spectrum expanded: cryptogenic cirrhosis andthe natural history of non-alcoholic fatty liver disease. Journal of Hepatology2004;40:578–84.
[5] van der Poorten D, Samer CF, Ramezani-Moghadam M, et al. Hepatic fat loss inadvanced non-alcoholic steatohepatitis: are alterations in serum adiponectinthe cause? Hepatology 2013;57:2180–8.
[6] Lonardo A, Sookoian S, Chonchol M, et al. Cardiovascular and systemicrisk in non-alcoholic fatty liver disease – atherosclerosis as a major playerin the natural course of NAFLD. Current Pharmaceutical Design 2013;19:5177–92.
[7] Skelly MM, James PD, Ryder SD. Findings on liver biopsy to investigate abnor-mal liver function tests in the absence of diagnostic serology. Journal ofHepatology 2001;35:195–9.
[8] Lonardo A, Caldwell SH, Loria P. Clinical physiology of NAFLD: a criticaloverview of pathogenesis and treatment. Expert Review of Endocrinology& Metabolism 2010;5:403–23.
[9] Wong RJ, Cheung R, Ahmed A. Non-alcoholic steatohepatitis is the mostrapidly growing indication for liver transplantation in patients with hepa-tocellular carcinoma in the US. Hepatology 2014;59:2188–95.
[10] Palaniappan L, Carnethon MR, Wang Y, et al. Predictors of the incidentmetabolic syndrome in adults: the Insulin Resistance Atherosclerosis Study.Diabetes Care 2004;27:788–93.
[11] Eckel RH. The metabolic syndrome. Lancet 2010;375:181–3.[12] Haller H. Epidemiology and associated risk factors of hyperlipoproteine-
mia. Zeitschrift fur Die Gesamte Innere Medizin und Ihre Grenzgebiete1977;32:124–8.
[13] Musso G, Gambino R, Bo S, et al. Should non-alcoholic fatty liver disease beincluded in the definition of metabolic syndrome? A cross-sectional compar-ison with Adult Treatment Panel III criteria in nonobese nondiabetic subjects.Diabetes Care 2008;31:562–8.
[14] Ferrannini E. Metabolic syndrome: a solution in search of a problem. Journalof Clinical Endocrinology and Metabolism 2007;92:396–8.
[15] Mottillo S, Filion KB, Genest J, et al. The metabolic syndrome and cardiovas-cular risk a systematic review and meta-analysis. Journal of the AmericanCollege of Cardiology 2010;56:1113–32.
r Disease 47 (2015) 181–190
[16] Rachas A, Raffaitin C, Barberger-Gateau P, et al. Clinical usefulness of themetabolic syndrome for the risk of coronary heart disease does not exceed thesum of its individual components in older men and women. The Three-City(3C) Study. Heart 2012;98:650–5.
[17] Kawada T. Predictors of the development of metabolic syndrome in maleworkers: a 3-year follow-up study. Journal of Occupational and Environmen-tal Medicine 2012;54:292–5.
[18] Galassi A, Reynolds K, He J. Metabolic syndrome and risk of cardiovasculardisease: a meta-analysis. American Journal of Medicine 2006;119:812–9.
[19] Welzel TM, Graubard BI, Zeuzem S, et al. Metabolic syndrome increases therisk of primary liver cancer in the United States: a study in the SEER-Medicaredatabase. Hepatology 2011;54:463–71.
[20] Lonardo A. Fatty liver and non-alcoholic steatohepatitis. Where do we standand where are we going? Digestive Diseases 1999;17:80–9.
[21] Marchesini G, Brizi M, Morselli-Labate AM, et al. Association of non-alcoholicfatty liver disease with insulin resistance. American Journal of Medicine1999;107:450–5.
[22] Cortez-Pinto H, Camilo ME, Baptista A, et al. Non-alcoholic fatty liver: anotherfeature of the metabolic syndrome? Clinical Nutrition 1999;18:353–8.
[23] Vanni E, Bugianesi E, Kotronen A, et al. From the metabolic syndrome to NAFLDor vice versa? Digestive and Liver Disease 2010;42:320–30.
[24] Anstee QM, Targher G, Day CP. Progression of NAFLD to diabetes mellitus,cardiovascular disease or cirrhosis. Nature Reviews Gastroenterology & Hep-atology 2013;10:330–44.
[25] Machado MV, Cortez-Pinto H. Management of fatty liver disease withthe metabolic syndrome. Expert Review of Gastroenterology & Hepatology2014;8:487–500.
[26] Yki-Järvinen H. Non-alcoholic fatty liver disease as a cause and a consequenceof metabolic syndrome. The Lancet Diabetes & Endocrinology 2014;2:901–10.
[27] Lonardo A, Trande P. Are there any sex differences in fatty liver? A study ofglucose metabolism and body fat distribution. Journal of Gastroenterologyand Hepatology 2000;15:775–82.
[28] Marchesini G, Brizi M, Bianchi G, et al. Non-alcoholic fatty liver disease: afeature of the metabolic syndrome. Diabetes 2001;50:1844–50.
[29] Jimba S, Nakagami T, Takahashi M, et al. Prevalence of non-alcoholic fatty liverdisease and its association with impaired glucose metabolism in Japaneseadults. Diabetic Medicine 2005;22:1141–5.
[30] Wong VW, Hui AY, Tsang SW, et al. Prevalence of undiagnosed diabetes andpostchallenge hyperglycaemia in Chinese patients with non-alcoholic fattyliver disease. Alimentary Pharmacology and Therapeutics 2006;24:1215–22.
[31] Gastaldelli A, Kozakova M, Højlund K, et al. Fatty liver is associated withinsulin resistance, risk of coronary heart disease, and early atherosclerosisin a large European population. Hepatology 2009;49:1537–44.
[32] Speliotes EK, Massaro JM, Hoffmann U, et al. Fatty liver is associated withdyslipidemia and dysglycemia independent of visceral fat: the FraminghamHeart Study. Hepatology 2010;51:1979–87.
[33] Kim SH, Lee JW, Hwang HJ. Associations between combinations of body massindex plus non-alcoholic fatty liver disease and diabetes mellitus amongKorean adults. Asia Pacific Journal of Clinical Nutrition 2011;20:14–20.
[34] Bedogni G, Gastaldelli A, Manco M, et al. Relationship between fatty liver andglucose metabolism: a cross-sectional study in 571 obese children. Nutrition,Metabolism and Cardiovascular Diseases 2012;22:120–6.
[35] Ortiz-Lopez C, Lomonaco R, Orsak B, et al. Prevalence of prediabetes and dia-betes and metabolic profile of patients with non-alcoholic fatty liver disease(NAFLD). Diabetes Care 2012;35:873–8.
[36] Porter SA, Pedley A, Massaro JM, et al. Aminotransferase levels are associ-ated with cardiometabolic risk above and beyond visceral fat and insulinresistance: the Framingham Heart Study. Arteriosclerosis, Thrombosis, andVascular Biology 2013;33:139–46.
[37] Lazo M, Hernaez R, Eberhardt MS, et al. Prevalence of non-alcoholic fatty liverdisease in the United States: the Third National Health and Nutrition Exam-ination Survey, 1988–1994. American Journal of Epidemiology 2013;178:38–45.
[38] Li X, Xia M, Ma H, et al. Liver fat content, evaluated through semi-quantitativeultrasound measurement, is associated with impaired glucose profiles: acommunity-based study in Chinese. PLOS ONE 2013;8:e65210.
[39] Ou HY, Wang CY, Yang YC, et al. The association between non-alcoholic fattypancreas disease and diabetes. PLOS ONE 2013;8:e62561.
[40] Loria P, Lonardo A, Anania F. Liver and diabetes. A vicious circle. HepatologyResearch 2013;43:51–64.
[41] Musso G, Gambino R, Cassader M, et al. Meta-analysis: natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasivetests for liver disease severity. Annals of Medicine 2011;43:617–49.
[42] Ikai E, Noborizaka Y, Tsuritani I, et al. Serum gamma-glutamyl transpep-tidase levels and hypertension in non-drinkers: a possible role of fattyliver in the pathogenesis of obesity related hypertension. Obesity Research1993;1:469–74.
[43] Donati G, Stagni B, Piscaglia F, et al. Increased prevalence of fatty liver inarterial hypertensive patients with normal liver enzymes: role of insulinresistance. Gut 2004;53:1020–3.
[44] Lonardo A, Bellini M, Tartoni P, et al. The bright liver syndrome. Prevalence
and determinants of a “bright” liver echopattern. Italian Journal of Gastroen-terology and Hepatology 1997;29:351–6.[45] Knobler H, Schattner A, Zhornicki T, et al. Fatty liver – an additional andtreatable feature of the insulin resistance syndrome. QJM 1999 Feb;92:73–9.

d Live
A. Lonardo et al. / Digestive an[46] Marchesini G, Avagnina S, Barantani EG, et al. Aminotransferase andgamma-glutamyltranspeptidase levels in obesity are associated with insulinresistance and the metabolic syndrome. Journal of Endocrinological Investi-gation 2005;28:333–9.
[47] Fan JG, Zhu J, Li XJ, et al. Fatty liver and the metabolic syndromeamong Shanghai adults. Journal of Gastroenterology and Hepatology2005;20:1825–32.
[48] Kotronen A, Westerbacka J, Bergholm R, et al. Liver fat in the metabolic syn-drome. Journal of Clinical Endocrinology and Metabolism 2007;92:3490–7.
[49] Kawamoto R, Kohara K, Tabara Y, et al. Serum gamma-glutamyl transferaselevels are associated with metabolic syndrome in community-dwelling indi-viduals. Journal of Atherosclerosis and Thrombosis 2009;16:355–62.
[50] Anty R, Iannelli A, Patouraux S, et al. A new composite model includingmetabolic syndrome, alanine aminotransferase and cytokeratin-18 for thediagnosis of non-alcoholic steatohepatitis in morbidly obese patients. Ali-mentary Pharmacology and Therapeutics 2010;32:1315–22.
[51] Xia MF, Yan HM, Lin HD, et al. Elevation of liver enzymes within the normallimits and metabolic syndrome. Clinical and Experimental Pharmacology andPhysiology 2011;38:373–9.
[52] Boursier J, Chaigneau J, Roullier V, et al. Steatosis degree, measured bymorphometry, is linked to other liver lesions and metabolic syndrome com-ponents in patients with NAFLD. European Journal of Gastroenterology andHepatology 2011;23:974–81.
[53] Hu X, Huang Y, Bao Z, et al. Prevalence and factors associated with non-alcoholic fatty liver disease in Shanghai work-units. BMC Gastroenterology2012;12:123.
[54] Pickhardt PJ, Jee Y, O’Connor SD, et al. Visceral adiposity and hepatic steatosisat abdominal CT: association with the metabolic syndrome. American Journalof Roentgenology 2012;198:1100–7.
[55] Castro-Martínez MG, Banderas-Lares DZ, Ramírez-Martínez JC, et al. Preva-lence of non-alcoholic fatty liver disease in subjects with metabolic syndrome.Cirugia y Cirujanos 2012;80:128–33.
[56] Kwon YM, Oh SW, Hwang SS, et al. Association of nonalcoholic fatty liver dis-ease with components of metabolic syndrome according to body mass indexin Korean adults. American Journal of Gastroenterology 2012;107:1852–8.
[57] Sinn DH, Gwak GY, Park HN, et al. Ultrasonographically detected non-alcoholic fatty liver disease is an independent predictor for identifyingpatients with insulin resistance in non-obese, non-diabetic middle-agedAsian adults. American Journal of Gastroenterology 2012;107:561–7.
[58] Younossi ZM, Stepanova M, Negro F, et al. Non-alcoholic fatty liver disease inlean individuals in the United States. Medicine 2012;91:319–27.
[59] Yousefzadeh G, Shokoohi M, Yeganeh M, et al. Role of gamma-glutamyltransferase (GGT) in diagnosis of impaired glucose tolerance and metabolicsyndrome: a prospective cohort research from the Kerman CoronaryArtery Disease Risk Study (KERCADRS). Diabetology & Metabolic Syndrome2012;6:190–4.
[60] Soresi M, Noto D, Cefalù AB, et al. Non-alcoholic fatty liver and metabolic syn-drome in Italy: results from a multicentric study of the Italian Arteriosclerosissociety. Acta Diabetologica 2013;50:241–9.
[61] Smits MM, Ioannou GN, Boyko EJ, et al. Non-alcoholic fatty liver disease asan independent manifestation of the metabolic syndrome: results of a USnational survey in three ethnic groups. Journal of Gastroenterology and Hep-atology 2013;28:664–70.
[62] Eraslan S, Kizilgul M, Uzunlulu M, et al. Frequency of metabolic syndromeand 25-hydroxyvitamin D3 levels in patients with non-alcoholic fatty liverdisease. Minerva Medica 2013;104:447–53.
[63] Juárez-Rojas JG, Medina-Urrutia AX, Jorge-Galarza E, et al. Fatty liver increasesthe association of metabolic syndrome with diabetes and atherosclerosis.Diabetes Care 2013;36:1726–8.
[64] Tao L, Li X, Zhu H, et al. Association between �-glutamyl transferase andmetabolic syndrome: a cross-sectional study of an adult population in Bei-jing. International Journal of Environmental Research and Public Health2013;10:5523–40.
[65] Fraser A, Harris R, Sattar N, et al. Alanine aminotransferase, gamma-glutamyltransferase, and incident diabetes: the British Women’s Heart andHealth Study and meta-analysis. Diabetes Care 2009;32:741–50.
[66] Lonardo A, Loria P, Leonardi F, et al. Policentrica Steatosi Epatica Non Alcolica.Fasting insulin and uric acid levels but not indices of iron metabolism areindependent predictors of non-alcoholic fatty liver disease. A case–controlstudy. Digestive and Liver Disease 2002;34:204–11.
[67] Petta S, Cammà C, Cabibi D, et al. Hyperuricemia is associated with histologicalliver damage in patients with non-alcoholic fatty liver disease. AlimentaryPharmacology and Therapeutics 2011;34:757–66.
[68] Keenan T, Blaha MJ, Nasir K, et al. Relation of uric acid to serum levels ofhigh-sensitivity C-reactive protein, triglycerides, and high-density lipopro-tein cholesterol and to hepatic steatosis. American Journal of Cardiology2012;110:1787–92.
[69] Ryu S, Song J, Choi BY, et al. Incidence and risk factors for metabolic syn-drome in Korean male workers, ages 30 to 39. Annals of Epidemiology2007;17:245–52.
[70] Sui X, Church TS, Meriwether RA, et al. Uric acid and the development of
metabolic syndrome in women and men. Metabolism: Clinical and Experi-mental 2008;57:845–52.[71] Lee JM, Kim HC, Cho HM, et al. Association between serum uric acid leveland metabolic syndrome. Journal of Preventive Medicine and Public Health2012;45:181–7.
r Disease 47 (2015) 181–190 187
[72] Zhang Q, Zhang C, Song X, et al. A longitudinal cohort based association studybetween uric acid level and metabolic syndrome in Chinese Han urban malepopulation. BMC Public Health 2012;12:419.
[73] Wang JY, Chen YL, Hsu CH, et al. Predictive value of serum uric acid levelsfor the diagnosis of metabolic syndrome in adolescents. Journal of Pediatrics2012;161, 753–6.e2.
[74] Lu W, Song K, Wang Y, et al. Relationship between serum uric acid andmetabolic syndrome: an analysis by structural equation modeling. Journalof Clinical Lipidology 2012;6:159–67.
[75] Yang T, Chu CH, Bai CH, et al. Uric acid level as a risk marker for metabolicsyndrome: a Chinese cohort study. Atherosclerosis 2012;220:525–31.
[76] Zhang Z, Bian L, Choi Y. Serum uric acid: a marker of metabolic syndrome andsubclinical atherosclerosis in Korean men. Angiology 2012;63:420–8.
[77] Goncalves JP, Oliveira A, Severo M, et al. Cross-sectional and longitudinalassociations between serum uric acid and metabolic syndrome. Endocrine2012;4:450–7.
[78] Hara S, Tsuji H, Ohmoto Y, et al. High serum uric acid level and low urine pH aspredictors of metabolic syndrome: a retrospective cohort study in a Japaneseurban population. Metabolism: Clinical and Experimental 2012;61:281–8.
[79] Zhang ML, Gao YX, Wang X, et al. Serum uric acid and appropriate cut-offvalue for prediction of metabolic syndrome among Chinese adults. Journal ofClinical Biochemistry and Nutrition 2013;52:38–42.
[80] Osgood K, Krakoff J, Thearle M. Serum uric acid predicts both current andfuture components of the metabolic syndrome. Metabolic Syndrome andRelated Disorders 2013;11:157–62.
[81] Ziaee A, Esmailzadehha N, Ghorbani A, et al. Association between uric acidand metabolic syndrome in Qazvin Metabolic Diseases Study (QMDS), Iran.Global Journal of Health Science 2012;5:155–65.
[82] Cohen E, Krause I, Fraser A, et al. Hyperuricemia and metabolic syndrome:lessons from a large cohort from Israel. Israel Medical Association Journal2012;14:676–80.
[83] Ouyang X, Cirillo P, Sautin Y, et al. Fructose consumption as a risk factor fornon-alcoholic fatty liver disease. Journal of Hepatology 2008;48:993–9.
[84] Abdelmalek MF, Suzuki A, Guy C, et al. Increased fructose consumption is asso-ciated with fibrosis severity in patients with non-alcoholic fatty liver disease.Hepatology 2010;51:1961–71.
[85] Basaranoglu M, Basaranoglu G, Sabuncu T, et al. Fructose as a key player inthe development of fatty liver disease. World Journal of Gastroenterology2013;19:1166–72.
[86] Dhingra R, Sullivan L, Jacques PF, et al. Soft drink consumption and riskof developing cardiometabolic risk factors and the metabolic syndrome inmiddle-aged adults in the community. Circulation 2007;116:480–8.
[87] Perez-Pozo SE, Schold J, Nakagawa T, et al. Excessive fructose intake inducesthe features of metabolic syndrome in healthy adult men: role of uric acid inthe hypertensive response. International Journal of Obesity 2010;34:454–61.
[88] Khitan Z, Kim DH. Fructose: a key factor in the development ofmetabolic syndrome and hypertension. Journal of Nutrition and Metabolism2013;2013:682673.
[89] Liangpunsakul S, Chalasani N. Is hypothyroidism a risk factor for non-alcoholic steatohepatitis? Journal of Clinical Gastroenterology 2003;37:340–3.
[90] Ittermann T, Haring R, Wallaschofski H, et al. Inverse association betweenserum free thyroxine levels and hepatic steatosis: results from the Study ofHealth in Pomerania. Thyroid 2012;22:568–74.
[91] Chung GE, Kim D, Kim W, et al. Non-alcoholic fatty liver disease across thespectrum of hypothyroidism. Journal of Hepatology 2012;57:150–6.
[92] Carulli L, Ballestri S, Lonardo A, et al. Is non-alcoholic steatohepatitis associ-ated with a high-though-normal thyroid stimulating hormone level and lowercholesterol levels? Internal and Emergency Medicine 2013;8:297–305.
[93] Park HT, Cho GJ, Ahn KH, et al. Thyroid stimulating hormone is associatedwith metabolic syndrome in euthyroid postmenopausal women. Maturitas2009;62:301–5.
[94] Ruhla S, Weickert MO, Arafat AM, et al. A high normal TSH is associated withthe metabolic syndrome. Clinical Endocrinology 2010;72:696–701.
[95] Lai Y, Wang J, Jiang F, et al. The relationship between serum thyrotropin andcomponents of metabolic syndrome. Endocrine Journal 2011;58:23–30.
[96] Heima NE, Eekhoff EM, Oosterwerff MM, et al. Thyroid function and themetabolic syndrome in older persons: a population-based study. Euro-pean Journal of Endocrinology/European Federation of Endocrine Societies2012;168:59–65.
[97] Waring AC, Rodondi N, Harrison S, et al. Thyroid function and prevalent andincident metabolic syndrome in older adults: the Health, Ageing and BodyComposition Study. Clinical Endocrinology 2012;76:911.
[98] Trauner M, Claudel T, Fickert P, et al. Bile acids as regulators of hepatic lipidand glucose metabolism. Digestive Diseases 2010;28:220–4.
[99] Liechti F, Dufour JF. Treatment of NASH with ursodeoxycholic acid:cons. Clinics and Research in Hepatology and Gastroenterology 2012;36:S46–52.
[100] Ratziu V. Treatment of NASH with ursodeoxycholic acid: pro. Clinics andResearch in Hepatology and Gastroenterology 2012;36:S41–5.
[101] Liaset B, Hao Q, Jørgensen H, et al. Nutritional regulation of bile acid
metabolism is associated with improved pathological characteristics of themetabolic syndrome. Journal of Biological Chemistry 2011;286:28382–95.[102] Watanabe M, Morimoto K, Houten SM, et al. Bile acid binding resin improvesmetabolic control through the induction of energy expenditure. PLoS ONE2012;7:e38286.

1 d Live
88 A. Lonardo et al. / Digestive an[103] Porez G, Prawitt J, Gross B, et al. Bile acid receptors as targets for the treat-ment of dyslipidemia and cardiovascular disease. Journal of Lipid Research2012;53:1723–37.
[104] Johnson NA, George J. Fitness versus fatness: moving beyond weight loss innon-alcoholic fatty liver disease. Hepatology 2010;52:370–81.
[105] Hallsworth K, Fattakhova G, Hollingsworth KG, et al. Resistance exercisereduces liver fat and its mediators in non-alcoholic fatty liver disease inde-pendent of weight loss. Gut 2011;60:1278–83.
[106] Bae JC, Suh S, Park SE, et al. Regular exercise is associated with a reductionin the risk of NAFLD and decreased liver enzymes in individuals with NAFLDindependent of obesity in Korean adults. PLoS ONE 2012;7:e46819.
[107] Keating SE, Hackett DA, George J, et al. Exercise and non-alcoholic fattyliver disease: a systematic review and meta-analysis. Journal of Hepatology2012;57:157–66.
[108] Gerber L, Otgonsuren M, Mishra A, et al. Non-alcoholic fatty liver disease(NAFLD) is associated with low level of physical activity: a population-basedstudy. Alimentary Pharmacology and Therapeutics 2012;36:772–81.
[109] Thoma C, Day CP, Trenell MI. Lifestyle interventions for the treatment ofnon-alcoholic fatty liver disease in adults: a systematic review. Journal ofHepatology 2012;56:255–66.
[110] Murer M, Schmied C, Battegay E, et al. Physical activity behaviour in patientswith metabolic syndrome. Swiss Medical Weekly 2012;142:w13691.
[111] Yamaoka K, Tango T. Effects of lifestyle modification on metabolic syn-drome: a systematic review and meta-analysis. BMC Medicine 2012;10:138.
[112] Hagnäs MP, Cederberg H, Mikkola I, et al. Reduction in metabolic syndromeamong obese young men is associated with exercise-induced body composi-tion changes during military service. Diabetes Research and Clinical Practice2012;98:312–9.
[113] Kim JW, Kim DY. Effects of aerobic exercise training on serum sex hor-mone binding globulin, body fat index, and metabolic syndrome factors inobese postmenopausal women. Metabolic Syndrome and Related Disorders2012;10:452–7.
[114] Nanri A, Tomita K, Matsushita Y, et al. Effect of six months lifestyle interven-tion in Japanese men with metabolic syndrome: randomized controlled trial.Journal of Occupational Health 2012;54:215–22.
[115] Gardner AW, Parker DE, Krishnan S, et al. Metabolic syndrome and dailyambulation in children, adolescents, and young adults. Medicine and Sciencein Sports and Exercise 2013;45:163–9.
[116] Kim J, Tanabe K, Yoshizawa Y, et al. Lifestyle-based physical activity inter-vention for one year improves metabolic syndrome in overweight maleemployees. Tohoku Journal of Experimental Medicine 2013;229:11–7.
[117] Dunn W, Xu R, Schwimmer JB. Modest wine drinking and decreasedprevalence of suspected non-alcoholic fatty liver disease. Hepatology2008;47:1947–54.
[118] Moriya A, Iwasaki Y, Ohguchi S, et al. Alcohol consumption appears to pro-tect against non-alcoholic fatty liver disease. Alimentary Pharmacology andTherapeutics 2011;33:378–88.
[119] Dunn W, Sanyal AJ, Brunt EM, et al. Modest alcohol consumption is associatedwith decreased prevalence of steatohepatitis in patients with non-alcoholicfatty liver disease (NAFLD). Journal of Hepatology 2012;57:384–91.
[120] Hamaguchi M, Kojima T, Ohbora A, et al. Protective effect of alcohol con-sumption for fatty liver but not metabolic syndrome. World Journal ofGastroenterology 2012;18:156–67.
[121] Carnethon MR, Loria CM, Hill JO, et al. Risk factors for the metabolic syn-drome: the Coronary Artery Risk Development in Young Adults (CARDIA)study, 1985–2001. Diabetes Care 2004;27:2707–15.
[122] Wilsgaard T, Jacobsen BK. Lifestyle factors and incident metabolic syn-drome. The Tromsø study 1979–2001. Diabetes Research and Clinical Practice2007;78:217e24.
[123] Baik I, Shin C. Prospective study of alcohol consumption and metabolic syn-drome. American Journal of Clinical Nutrition 2008;87:1455–63.
[124] Alkerwi A, Boutsen M, Vaillant M, et al. Alcohol consumption and theprevalence of metabolic syndrome: a meta-analysis of observational studies.Atherosclerosis 2009;204:624–35.
[125] Baliunas DO, Taylor BJ, Irving H, et al. Alcohol as a risk factor fortype 2 diabetes: a systematic review and meta-analysis. Diabetes Care2009;32:2123–32.
[126] Wakabayashi I. Cross-sectional relationship between alcohol consumptionand prevalence of metabolic syndrome in Japanese men and women. Journalof Atherosclerosis and Thrombosis 2010;17:695–704.
[127] Lee KW, Park BJ, Kang HT, et al. Alcohol-drinking patterns and metabolicsyndrome risk: the 2007 Korean national health and nutrition examinationsurvey. Alcohol 2011;45:499–505.
[128] Sayon-Orea C, Martinez-Gonzalez MA, Bes-Rastrollo M. Alcohol consump-tion and body weight: a systematic review. Nutrition Reviews 2011;69:419–31.
[129] Kim BJ, Kim BS, Kang JH. Alcohol consumption and incidence of metabolicsyndrome in Korean men. A 3-year follow-up study. Circulation Journal2012;76:2363–71.
[130] Chen CC, Lin WY, Li CI, et al. The association of alcohol consumption with
metabolic syndrome and its individual components: the Taichung communityhealth study. Nutrition Research 2012;32:24–9.[131] Barrio-Lopez MT, Bes-Rastrollo M, Sayon-Orea C, et al. Different types of alco-holic beverages and incidence of metabolic syndrome and its components ina Mediterranean cohort. Clinical Nutrition 2013;32:797–804.
r Disease 47 (2015) 181–190
[132] Stoutenberg M, Lee DC, Sui X, et al. Prospective study of alcohol consumptionand the incidence of the metabolic syndrome in US men. British Journal ofNutrition 2013;110:901–10.
[133] Birerdinc A, Stepanova M, Pawloski L, et al. Caffeine is protective in patientswith non-alcoholic fatty liver disease. Alimentary Pharmacology and Thera-peutics 2012;35:76–82.
[134] Molloy JW, Calcagno CJ, Williams CD, et al. Association of coffee and caf-feine consumption with fatty liver disease, non-alcoholic steatohepatitis, anddegree of hepatic fibrosis. Hepatology 2012;55:429–36.
[135] Anty R, Marjoux S, Iannelli A, et al. Regular coffee but not espresso drink-ing is protective against fibrosis in a cohort mainly composed of morbidlyobese European women with NAFLD undergoing bariatric surgery. Journal ofHepatology 2012;57:1090–6.
[136] Gutiérrez-Grobe Y, Chávez-Tapia N, Sánchez-Valle V, et al. High coffee intakeis associated with lower grade non-alcoholic fatty liver disease: the role ofperipheral antioxidant activity. Annals of Hepatology 2012;11:350–5.
[137] Masterton GS, Hayes PC. Coffee and the liver: a potential treatmentfor liver disease? European Journal of Gastroenterology and Hepatology2010;22:1277–83.
[138] Kalthoff S, Ehmer U, Freiberg N, et al. Coffee induces expression of glu-curonosyltransferases by the aryl hydrocarbon receptor and Nrf2 in liver andstomach. Gastroenterology 2010;139:1699–710.
[139] Yamauchi R, Kobayashi M, Matsuda Y, et al. Coffee and caffeine amelioratehyperglycemia, fatty liver, and inflammatory adipocytokine expression inspontaneously diabetic KK-Ay mice. Journal of Agricultural and Food Chem-istry 2010;58:5597–603.
[140] Matsuda Y, Kobayashi M, Yamauchi R, et al. Coffee and caffeine improveinsulin sensitivity and glucose tolerance in C57BL/6J mice fed a high-fat diet.Bioscience, Biotechnology, and Biochemistry 2011;75:2309–15.
[141] Carrieri MP, Sogni P, Cohen J, et al. HEPAVIH Study Group. Elevated coffeeconsumption and reduced risk of insulin resistance in HIV-HCV coinfectedpatients (HEPAVIH ANRS CO-13). Hepatology 2012;56:2010.
[142] Sugiura C, Nishimatsu S, Moriyama T, et al. Catechins and caffeine inhibit fataccumulation in mice through the improvement of hepatic lipid metabolism.Journal of Obesity 2012;2012:520510.
[143] Hino A, Adachi H, Enomoto M, et al. Habitual coffee but not green teaconsumption is inversely associated with metabolic syndrome: an epidemio-logical study in a general Japanese population. Diabetes Research and ClinicalPractice 2007;76:383–9.
[144] Panchal SK, Wong WY, Kauter K, et al. Caffeine attenuates metabolic syn-drome in diet-induced obese rats. Nutrition 2012;28:1055–62.
[145] Takami H, Nakamoto M, Uemura H, et al. Inverse correlation between coffeeconsumption and prevalence of metabolic syndrome: baseline survey of theJapan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima,Japan. Journal of Epidemiology 2013;23:12–20.
[146] Hamabe A, Uto H, Imamura Y, et al. Impact of cigarette smoking on onset ofnon-alcoholic fatty liver disease over a 10-year period. Journal of Gastroen-terology 2011;46:769–78.
[147] Zein CO, Unalp A, Colvin R, et al. Non-alcoholic steatohepatitis clinicalresearch network. Smoking and severity of hepatic fibrosis in non-alcoholicfatty liver disease. Journal of Hepatology 2011;54:753–9.
[148] Koehler EM, Schouten JN, Hansen BE, et al. Prevalence and risk factors of non-alcoholic fatty liver disease in the elderly: results from the Rotterdam study.Journal of Hepatology 2012;57:1305–11.
[149] Sun K, Liu J, Ning G. Active smoking and risk of metabolic syndrome: a meta-analysis of prospective studies. PLoS ONE 2012;7:e47791.
[150] Hsieh SD, Muto T, Murase T, et al. Association of short sleep duration withobesity, diabetes, fatty liver and behavioral factors in Japanese men. InternalMedicine 2011;50:2499–502.
[151] Aron-Wisnewsky J, Minville C, Tordjman J, et al. Chronic intermittent hypoxiais a major trigger for non-alcoholic fatty liver disease in morbid obese. Journalof Hepatology 2012;56:225–33.
[152] Musso G, Cassader M, Olivetti C, et al. Association of obstructive sleep apnoeawith the presence and severity of non-alcoholic fatty liver disease. A system-atic review and meta-analysis. Obesity Reviews 2013;14:417–31.
[153] Sookoian S, Gemma C, Fernández Gianotti T, et al. Effects of rotating shift workon biomarkers of metabolic syndrome and inflammation. Journal of InternalMedicine 2007;261:285–92.
[154] Donga E, van Dijk M, van Dijk JG, et al. A single night of partial sleep depri-vation induces insulin resistance in multiple metabolic pathways in healthysubjects. Journal of Clinical Endocrinology and Metabolism 2010;95:2963–8.
[155] Choi JK, Kim MY, Kim JK, et al. Association between short sleep duration andhigh incidence of metabolic syndrome in midlife women. Tohoku Journal ofExperimental Medicine 2011;225:187–93.
[156] Arora T, Jiang CQ, Thomas GN, et al. Self-reported long total sleep duration isassociated with metabolic syndrome: the Guangzhou Biobank Cohort Study.Diabetes Care 2011;34:2317–9.
[157] Yilmaz Y, Ones T, Purnak T, et al. Association between the presence of brownadipose tissue and non-alcoholic fatty liver disease in adult humans. Alimen-tary Pharmacology and Therapeutics 2011;34:318–23.
[158] van Marken Lichtenbelt WD, Vanhommerig JW, Smulders NM, et al. Cold-
activated brown adipose tissue in healthy men. New England Journal ofMedicine 2009;360:1500–8.[159] Cypess AM, Lehman S, Williams G, et al. Identification and importance ofbrown adipose tissue in adult humans. New England Journal of Medicine2009;360:1509–17.

d Live
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
A. Lonardo et al. / Digestive an
160] Pasanisi F, Pace L, Fonti R, et al. Evidence of brown fat activity in constitutionalleanness. Journal of Clinical Endocrinology and Metabolism 2013;98:1214–8.
161] Matsen ME, Thaler JP, Wisse BE, et al. In uncontrolled diabetes, thyroid hor-mone and sympathetic activators induce thermogenesis without increasingglucose uptake in brown adipose tissue. American Journal of Physiology:Endocrinology and Metabolism 2013;304:E734–46.
162] Wigg AJ, Roberts-Thomson IC, Dymock RB, et al. The role of small intesti-nal bacterial overgrowth, intestinal permeability, endotoxaemia, and tumournecrosis factor alpha in the pathogenesis of non-alcoholic steatohepatitis. Gut2001;48:206–11.
163] Nair S, Cope K, Risby TH, et al. Obesity and female gender increasebreath ethanol concentration: potential implications for the pathogene-sis of non-alcoholic steatohepatitis. American Journal of Gastroenterology2001;96:1200–4.
164] Thuy S, Ladurner R, Volynets V, et al. Non-alcoholic fatty liver disease inhumans is associated with increased plasma endotoxin and plasminogen acti-vator inhibitor 1 concentrations and with fructose intake. Journal of Nutrition2008;138:1452–5.
165] Miele L, Valenza V, La Torre G, et al. Increased intestinal permeability andtight junction alterations in non-alcoholic fatty liver disease. Hepatology2009;49:1877–87.
166] Harte AL, da Silva NF, Creely SJ, et al. Elevated endotoxin levels in non-alcoholic fatty liver disease. Journal of Inflammation 2010;7:15.
167] Verdam FJ, Rensen SS, Driessen A, et al. Novel evidence for chronic expo-sure to endotoxin in human non-alcoholic steatohepatitis. Journal of ClinicalGastroenterology 2011;45:149–52.
168] Henao-Mejia J, Elinav E, Jin C, et al. Inflammasome-mediated dysbiosis regu-lates progression of NAFLD and obesity. Nature 2012;482:179–85.
169] Machado MV, Cortez-Pinto H. Gut microbiota and non-alcoholic fatty liverdisease. Annals of Hepatology 2012;11:440–9.
170] Tremaroli V, Bäckhed F. Functional interactions between the gut microbiotaand host metabolism. Nature 2012;489:242–9.
171] Zhu L, Baker SS, Gill C, et al. Characterization of gut microbiomes in non-alcoholic steatohepatitis (NASH) patients: a connection between endogenousalcohol and NASH. Hepatology 2013;57:601–9.
172] Aron-Wisnewsky J, Gaborit B, Dutour A, et al. Gut microbiota and non-alcoholic fatty liver disease: new insights. Clinical Microbiology and Infection2013;19:338–48.
173] Ley RE, Bäckhed F, Turnbaugh P, et al. Obesity alters gut microbial ecol-ogy. Proceedings of the National Academy of Sciences of the United Statesof America 2005;102:11070–5.
174] Turnbaugh PJ, Ley RE, Mahowald MA, et al. An obesity-associated gut micro-biome with increased capacity for energy harvest. Nature 2006;444:1027–31.
175] Ley RE, Turnbaugh PJ, Klein S, et al. Microbial ecology: human gut microbesassociated with obesity. Nature 2006;444:1022–3.
176] Turnbaugh PJ, Hamady M, Yatsunenko T, et al. A core gut microbiome in obeseand lean twins. Nature 2009;457:480–4.
177] Schwiertz A, Taras D, Schäfer K, et al. Microbiota and SCFA in lean and over-weight healthy subjects. Obesity 2010;18:190–5.
178] Cani PD, Possemiers S, Van de Wiele T, et al. Changes in gut microbiota controlinflammation in obese mice through a mechanism involving GLP-2-drivenimprovement of gut permeability. Gut 2009;58:1091–103.
179] Furet JP, Kong LC, Tap J, et al. Differential adaptation of human gut microbiotato bariatric surgery-induced weight loss: links with metabolic and low-gradeinflammation markers. Diabetes 2010;59:3049–57.
180] Vijay-Kumar M, Aitken JD, Carvalho FA, et al. Metabolic syndrome and alteredgut microbiota in mice lacking Toll-like receptor 5. Science 2010;328:228–31.
181] Tilg H, Kaser A. Gut microbiome, obesity, and metabolic dysfunction. Journalof Clinical Investigation 2011;121:2126–32.
182] Greenblum S, Turnbaugh PJ, Borenstein E. Metagenomic systems biology ofthe human gut microbiome reveals topological shifts associated with obesityand inflammatory bowel disease. Proceedings of the National Academy ofSciences of the United States of America 2012;109:594–9.
183] Leber B, Tripolt NJ, Blattl D, et al. The influence of probiotic supplemen-tation on gut permeability in patients with metabolic syndrome: an openlabel, randomized pilot study. European Journal of Clinical Nutrition 2012;66:1110–5.
184] Tehrani AB, Nezami BG, Gewirtz A, et al. Obesity and its associated disease: arole for microbiota? Neurogastroenterology and Motility 2012;24:305–11.
185] Zupancic ML, Cantarel BL, Liu Z, et al. Analysis of the gut microbiota inthe old order Amish and its relation to the metabolic syndrome. PLoS ONE2012;7:e43052.
186] Vrieze A, Van Nood E, Holleman F, et al. Transfer of intestinal microbiotafrom lean donors increases insulin sensitivity in individuals with metabolicsyndrome. Gastroenterology 2012;143:913–6.
187] Parnell JA, Reimer RA. Prebiotic fibres dose-dependently increase satiety hor-mones and alter Bacteroidetes and Firmicutes in lean and obese JCR:LA-cprats. British Journal of Nutrition 2012;107:601–13.
188] Caricilli AM, Saad MJ. The role of gut microbiota on insulin resistance. Nutri-ents 2013;5:829–51.
189] Targher G, Bertolini L, Scala L, et al. Associations between serum 25-
hydroxyvitamin D3 concentrations and liver histology in patients withnon-alcoholic fatty liver disease. Nutrition, Metabolism and CardiovascularDiseases 2007;17:517–24.190] Barchetta I, Carotti S, Labbadia G, et al. Liver vitamin D receptor. CYP2R1, andCYP27A1 expression: relationship with liver histology and vitamin D3 levels
r Disease 47 (2015) 181–190 189
in patients with non-alcoholic steatohepatitis or hepatitis C virus. Hepatology2012;56:2180–7.
[191] Eliades M, Spyrou E, Agrawal N, et al. Meta-analysis: vitamin D and non-alcoholic fatty liver disease. Alimentary Pharmacology and Therapeutics2013;38:246–54.
[192] Adams LA, White SW, Marsh JA, et al. Association between liver-specific genepolymorphisms and their expression levels with non-alcoholic fatty liver dis-ease. Hepatology 2013;57:590–600.
[193] Kayaniyil S, Retnakaran R, Harris SB, et al. Prospective associations of vitaminD with b-cell function and glycemia. Diabetes 2011;60:2947–53.
[194] Ding C, Gao D, Wilding J, et al. Vitamin D signalling in adipose tissue. BritishJournal of Nutrition 2012;108:1915–23.
[195] Maki KC, Fulgoni VL, Keast DR, et al. Vitamin D intake and status are associ-ated with lower prevalence of metabolic syndrome in U.S. adults: NationalHealth and Nutrition Examination Surveys 2003–2006. Metabolic Syndromeand Related Disorders 2012;10:363–72.
[196] Wang C. Role of vitamin D in cardiometabolic diseases. Journal of DiabetesResearch 2013:243934.
[197] Khan H, Kunutsor S, Franco OH, et al. Vitamin D, type 2 diabetes and othermetabolic outcomes: a systematic review and meta-analysis of prospectivestudies. Proceedings of the Nutrition Society 2013;72:89–97.
[198] Kayaniyil S, Harris SB, Retnakaran R, et al. Prospective association of 25(OH)Dwith metabolic syndrome. Clinical Endocrinology 2014;80:502–7.
[199] Tsatsoulis A, Mantzaris MD, Bellou S, et al. Insulin resistance: an adap-tive mechanism becomes maladaptive in the current environment – anevolutionary perspective. Metabolism: Clinical and Experimental 2012;62:622–33.
[200] Leclercq IA, Da Silva Morais A, Schroyen B, et al. Insulin resistance in hepa-tocytes and sinusoidal liver cells: mechanisms and consequences. Journal ofHepatology 2007;47:142–56.
[201] Seki E, Brenner DA, Karin M. A liver full of JNK: signaling in regulation of cellfunction and disease pathogenesis, and clinical approaches. Gastroenterology2012;143:307–20.
[202] Hotamisligil GS. Endoplasmic reticulum stress and the inflammatory basis ofmetabolic disease. Cell 2010;140:900–17.
[203] Reaven GM. Banting lecture 1988: role of insulin resistance in human disease.Diabetes 1988;37:1595–607.
[204] Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet2005;365:1415–28.
[205] Loria P, Lonardo A, Carulli N. Should non-alcoholic fatty liver disease berenamed? Digestive Diseases 2005;23:72–82.
[206] Hamaguchi M, Takeda N, Kojima T, et al. Identification of individuals withnon-alcoholic fatty liver disease by the diagnostic criteria for the metabolicsyndrome. World Journal of Gastroenterology 2012;18:1508–16.
[207] Lonardo A, Bellentani S, Ratziu V, et al. Insulin resistance in non-alcoholicsteatohepatitis: necessary but not sufficient – death of a dogma from analy-sis of therapeutic studies? Expert Review of Gastroenterology & Hepatology2011;5:279–89.
[208] Suzuki A, Angulo P, Lymp J, et al. Chronological development of ele-vated aminotransferases in a non-alcoholic population. Hepatology 2005;41:64–71.
[209] Bugianesi E, McCullough AJ, Marchesini G. Insulin resistance: a metabolicpathway to chronic liver disease. Hepatology 2005;42:987–1000.
[210] Kotronen A, Yki-Järvinen H. Fatty liver: a novel component of themetabolic syndrome. Arteriosclerosis, Thrombosis, and Vascular Biology2008;28:27–38.
[211] Yamaguchi K, Yang L, McCall S, et al. Inhibiting triglyceride synthesis improveshepatic steatosis but exacerbates liver damage and fibrosis in obese mice withnon-alcoholic steatohepatitis. Hepatology 2007;45:1366–74.
[212] Lonardo A, Loria P, Carulli N. Insulin resistance in non-alcoholic fatty liverdisease: a clinical perspective. In: Leuschner U, James O, Dancygier H, edit-ors. Falk symposium 121 steatohepatitis (NASH and ASH). Dordrecht, TheNetherlands: Kluwer; 2001. p. 104–13.
[213] Caldwell SH, Ikura Y, Iezzoni JC, et al. Has natural selection in human popu-lations produced two types of metabolic syndrome (with and without fattyliver)? Journal of Gastroenterology and Hepatology 2007;22:S11–9.
[214] Cohen JC, Horton JD, Hobbs HH. Human fatty liver disease: old questions andnew insights. Science 2011;332:1519–23.
[215] Riva MA, Riva E, Spicci M, et al. The city of “Hepar”: rituals, gastronomy, andpolitics at the origins of the modern names for the liver. Journal of Hepatology2011;55:1132–6.
[216] Kumashiro N, Erion DM, Zhang D, et al. Cellular mechanism of insulinresistance in non-alcoholic fatty liver disease. Proceedings of the NationalAcademy of Sciences of the United States of America 2011;108:16381–5.
[217] Samuel VT, Liu ZX, Wang A, et al. Inhibition of protein kinase Cepsilon pre-vents hepatic insulin resistance in non-alcoholic fatty liver disease. Journal ofClinical Investigation 2007;117:739–45.
[218] Cantley JL, Yoshimura T, Camporez JP, et al. CGI-58 knockdown sequesters dia-cylglycerols in lipid droplets/ER-preventing diacylglycerol-mediated hepaticinsulin resistance. Proceedings of the National Academy of Sciences of theUnited States of America 2013;110:1869–74.
[219] Perry RJ, Samuel VT, Petersen KF, et al. The role of hepatic lipids in hepaticinsulin resistance and type 2 diabetes. Nature 2014;510:84–91.
[220] Zammit VA. Hepatic triacylglycerol synthesis and secretion: DGAT2 asthe link between glycaemia and triglyceridaemia. Biochemical Journal2013;451:1–12.

1 d Live
[233] Shen J, Wong GL, Chan HL, et al. PNPLA3 gene polymorphism accounts forfatty liver in community subjects without metabolic syndrome. Alimentary
90 A. Lonardo et al. / Digestive an
[221] Kasturiratne A, Weerasinghe S, Dassanayake AS, et al. Influence of non-alcoholic fatty liver disease on the development of diabetes mellitus. Journalof Gastroenterology and Hepatology 2013;28:142–7.
[222] Ryan MC, Wilson AM, Slavin J, et al. Associations between liver histology andseverity of the metabolic syndrome in subjects with non-alcoholic fatty liverdisease. Diabetes Care 2005;28:1222–4.
[223] Loria P, Adinolfi LE, Bellentani S, et al. Practice guidelines for the diagnosis andmanagement of non-alcoholic fatty liver disease. A decalogue from the ItalianAssociation for the Study of the Liver (AISF) Expert Committee. Digestive andLiver Disease 2010;42:272–82.
[224] Smits MM, van Geenen EJ. The clinical significance of pancreatic steatosis.Nature Reviews Gastroenterology & Hepatology 2011;8:169–77.
[225] Straub BK, Stoeffel P, Heid H, et al. Differential pattern of lipid droplet-associated proteins and de novo perilipin expression in hepatocytesteatogenesis. Hepatology 2008;47:1936–46.
[226] Wanless IR, Shiota K. The pathogenesis of non-alcoholic steatohepatitis andother fatty liver diseases: a four-step model including the role of lipid release
and hepatic venular obstruction in the progression to cirrhosis. Seminars inLiver Disease 2004;24:99–106.[227] Greenberg AS, Coleman RA, Kraemer FB, et al. The role of lipid droplets inmetabolic disease in rodents and humans. Journal of Clinical Investigation2011;121:2102–10.
r Disease 47 (2015) 181–190
[228] Lonardo A, Lombardini S, Scaglioni F, et al. Hepatic steatosis and insulinresistance: does etiology make a difference? Journal of Hepatology2006;44:190–6.
[229] Amaro A, Fabbrini E, Kars M, et al. Dissociation between intrahepatic triglyc-eride content and insulin resistance in familial hypobetalipoproteinemia.Gastroenterology 2010;139:149–53.
[230] Ballestri S, Lonardo A, Losi L, et al. Do diabetes and obesity promote hepaticfibrosis in familial heterozygous hypobetalipoproteinemia? Internal andEmergency Medicine 2009;4:71–3.
[231] Kantartzis K, Machicao F, Machann J, et al. The DGAT2 gene is a candidate forthe dissociation between fatty liver and insulin resistance in humans. ClinicalScience (London) 2009;116:531–7.
[232] Kantartzis K, Peter A, Machicao F, et al. Dissociation between fatty liver andinsulin resistance in humans carrying a variant of the patatin-like phospho-lipase 3 gene. Diabetes 2009;58:2616–23.
Pharmacology and Therapeutics 2014;39:532–9.[234] Sun Z, Lazar MA. Dissociating fatty liver and diabetes. Trends in Endocrinology
and Metabolism 2013;24:4–12.