Digest Rectal
8
Case Report The Problematic Issue of Kufs Disease Di ag no sis as Per formed on Rectal Biopsies: A Case Report G. Pasquinelli Dipartimento di Patologia Sperimentale, Sezione di Patologia Clinica, Universita ' di Bologna, Ospedale S. Orsola-Malpighi, Bologna, Italy; and Servizio di Anatomia Patologica, Ospedale ‘‘Casa Sollievo della So¡erenza,’’ IRCCS, San Giovanni Rotondo, Foggia, Italy G. Cenacchi Dipartimento Clinico di Scienze Radiologiche e Istocitopatologiche, Universita ' di Bologna, Ospedale S. Orsola-Malpighi, Bologna, Italy E. Le Piane C. Russo U. Aguglia Centro Regionale per lo Studio delle Epilessie, Ospedali ‘‘Riuniti,’’ Reggio Calabria, Italy Kufs disease, the late-onset form of a group of neurodegenerative disorders, known as the neuronal ceroid-lipofuscinoses, is characterized by intraneuronal =extraneuronal accumulation of proteins that are visible as fingerprint inclusions and granular osmiophilic deposits (GRODs) at the ultrastructural level. A problematic case of Kufs disease in a 53-year-old female affected by progressive gait disturbances, myoclonus, epilepsy, and profound dementia is presented. Laboratory, biochemical, and molecular genetic tests were unremarkable. A magnetic resonance imaging of the bra in reve aled a mod era te atr oph y over bot h hemisp her es with no white matter changes. Ultrastructural examination of rectal mucosa bio psie s sho wed fin ger pri nt incl usio ns in per ivas cul ar smo oth musc le cells. Pathological examination of autoptic tissues showed numerous intraneuronal PAS-positive, diastase-resistant inclusions corresponding to GRODs at the ultrastructural examination, but no fin ger print inc lus ion s. Cer ebellum,skeletal , and car diac muscles, skin, and liver were unaffected. The present case illustrates the diagnostic difficulties encountered while examining Kufs disease pathological samples. Main problematic issues include (1) specificity and diagnostic value of fingerprint inclusions when found exclusively in per ivascular smooth musc le cells; (2) safe dist inc tio n of GRODs from lipofuscin inclusions in cerebral tissue; and (3) reliability in using extraneural tissues and, in particular, rectal mucosa biopsies for diagnostic purposes. Keywords fingerp rint inclusions, GRODs, Kufs disease, NCL, rectal mucosa, ultrastru cture The neu ronal ceroid^l ip ofuscinoses (NCL s) collecti vely constitu te the most common ty pe of autosomal rec essive inherited neuro- deg enerat ive diseases in childhood [1]. However, a rare, late adult onset form, namely Kufs disease, is also described [1]. Cli nic all y, the se neuro- deg ene rat ive dis ord ers are ch ar acte rized by progressive cognitive decline, blindness, and myoclonic epilepsy, while the rare Kufs disease is dominated by dementia. All forms of NCLs are charac ter ized by int raneuronal accumulation of proteins [1], which can be seen as aut ofluoresc ent , diastase-resistant per iodic acid^Schiff (PAS ), and Sudan black B- po si ti ve cyto pl asmic li po pi gmen t granules at light microscopy. With electron microscopy it is po ss ible to di st ingu ish 5 di st inct pa tterns of osmi op hilic li po pi gmen ts: li po fuscin, fi ng er pr int dep osi ts, curvilinear bodies, gra nular osmiop hilic dep osi ts (GR ODs ), andmicrotubu lar par allel arr ays [2] . On the bases of the age of onset, clinical symptoms, and the ultr astruc ture of the storage material, Dyken identi fied 4 main for ms of NCL s: infa ntile, late inf antile, juvenile, and adult [3]. Recent advances in both gen eti cs an d bio che mis try hav e led to the ide nti fic ati on of 8 distinct NCL subtypes: CLN 1^8 [4]. A detailed view of Dyken’ s cl as si fi cation an d curren tl y used genetic classification of NCLs can be found in Boldrini et al . [2]. Kufs diseas e CLN 4 is th e most elusive of th e gr ou p because, to da te, no loci for this NCL subt yp e hav e been identi fied and con seq uen tly the dia gno sis of th e su sp icious clinical cases still relies on the morphological examination of affected tissues and the careful exclusion of other possible alternatives. Histo patho logical diagnosis of Kufs diseas e is b ased on th e intraneurona l pres ence of PAS and Suda n B-posi tive lipo pigme nt inclu sions , which ultra struc- tur all y correspon d to uni que fin ger pri nt inc lus ion s and=or to, more subtle , GRODs [5]. In the repo rte d Receiv ed 5 Octobe r 20 03; accept ed 31Octo ber 20 03. Add ress corr espondence to Giana ndr ea Pasquinelli, Dip artime nt o di Patologia Sperimentale, Sezione di Patologia Clinica,Universita ' di Bologna, Ospeda le S.Orsola-M alpighi,Padiglione11 , via Ma ssare nti 9, 40138 - Bologna, Italy. E-mail: [email protected] .it Ultrastructural Pathology, 28:43–48, 2004 Copyright # Taylor & Francis Inc. ISSN: 0191-3123 print/1521-0758 online DOI: 10.1080/019131 20490275231 43
-
Upload
areef-muarif -
Category
Documents
-
view
223 -
download
0
Transcript of Digest Rectal

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 1/8
Case Report
The Problematic Issue of Kufs Disease Diagnosis asPerformed on Rectal Biopsies: A Case Report
G. Pasquinelli
Dipartimento di Patologia Sperimentale, Sezione diPatologia Clinica, Universita ' di Bologna,Ospedale S. Orsola-Malpighi, Bologna, Italy; and Serviziodi Anatomia Patologica, Ospedale ‘‘Casa Sollievo dellaSo¡erenza,’’ IRCCS, San Giovanni Rotondo, Foggia, Italy
G. Cenacchi
Dipartimento Clinico di ScienzeRadiologiche e Istocitopatologiche, Universita ' di Bologna,Ospedale S. Orsola-Malpighi, Bologna, Italy
E. Le PianeC. RussoU. Aguglia
Centro Regionale per lo Studio delle Epilessie, Ospedali‘‘Riuniti,’’ Reggio Calabria, Italy
Kufs disease, the late-onset form of a group of neurodegenerativedisorders, known as the neuronal ceroid-lipofuscinoses, ischaracterized by intraneuronal =extraneuronal accumulation ofproteins that are visible as fingerprint inclusions and granularosmiophilic deposits (GRODs) at the ultrastructural level. Aproblematic case of Kufs disease in a 53-year-old female affected byprogressive gait disturbances, myoclonus, epilepsy, and profounddementia is presented. Laboratory, biochemical, and moleculargenetic tests were unremarkable. A magnetic resonance imaging of
the brain revealeda moderate atrophy over both hemispheres with nowhite matter changes. Ultrastructural examination of rectal mucosabiopsies showed fingerprint inclusions in perivascular smooth musclecells. Pathological examination of autoptic tissues showed numerousintraneuronal PAS-positive, diastase-resistant inclusionscorresponding to GRODs at the ultrastructural examination, but nofingerprint inclusions. Cerebellum, skeletal, and cardiacmuscles, skin,and liver were unaffected. The present case illustrates the diagnosticdifficulties encountered while examining Kufs disease pathologicalsamples. Main problematic issues include (1) specificity anddiagnostic value of fingerprint inclusions when found exclusively inperivascular smooth muscle cells; (2) safe distinction of GRODs fromlipofuscin inclusions in cerebral tissue; and (3) reliability in usingextraneural tissues and, in particular, rectal mucosa biopsies fordiagnostic purposes.
Keywords fingerprint inclusions, GRODs, Kufs disease, NCL, rectal mucosa, ultrastructure
The neuronal ceroid̂ lipofuscinoses (NCLs)collectively constitute the most common type ofautosomal recessive inherited neuro-degenerativediseases in childhood [1]. However, a rare, late adultonset form, namely Kufs disease, is also described [1].Clinically, these neuro-degenerative disorders arecharacterized by progressive cognitive decline,blindness, and myoclonic epilepsy, while the rare Kufsdisease is dominated by dementia. All forms of NCLsare characterized by intraneuronal accumulation ofproteins [1], which can be seen as autofluorescent,diastase-resistant periodic acid^Schiff (PAS), andSudan black B-positive cytoplasmic lipopigmentgranules at light microscopy. With electron microscopyit is possible to distinguish 5 distinct patterns of
osmiophilic lipopigments: lipofuscin, fingerprintdeposits, curvilinear bodies, granular osmiophilicdeposits (GRODs), andmicrotubular parallel arrays [2].
On the bases of the age of onset, clinical symptoms,and the ultrastructure of the storage material, Dykenidentified 4 main forms of NCLs: infantile, late infantile, juvenile, and adult [3]. Recent advances in bothgenetics and biochemistry have led to the identificationof 8 distinct NCL subtypes: CLN 1^8 [4]. A detailedview of Dyken’s classification and currently usedgenetic classification of NCLs can be found in Boldriniet al. [2]. Kufs disease CLN 4 is the most elusive ofthe group because, to date, no loci for this NCL subtypehave been identified and consequently the diagnosis ofthe suspicious clinical cases still relies on themorphological examination of affected tissues and thecareful exclusion of other possible alternatives.
Histopathological diagnosis of Kufs disease is basedon the intraneuronal presence of PAS and SudanB-positive lipopigment inclusions, which ultrastruc-turally correspond to unique fingerprint inclusionsand =or to, more subtle, GRODs [5]. In the reported
Received 5 October 20 03; accepted 31October 2003.
Address correspondence to Gianandrea Pasquinelli, Dipartimento diPatologia Sperimentale, Sezione di Patologia Clinica, Universita ' di Bologna,Ospedale S.Orsola-Malpighi,Padiglione11, via Massarenti 9, 40138 - Bologna,Italy. E-mail: [email protected]
Ultrastructural Pathology, 28:43–48, 2004Copyright # Taylor & Francis Inc.ISSN: 0191-3123 print/1521-0758 onlineDOI: 10.1080/01913120490275231
43

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 2/8
cases, the lipopigment inclusions have been describedin the cytoplasm of neurons and, to a lesser extent,of other cell types including smooth muscle cells,Schwann cells, and eccrine sweat gland epithelial cells[1, 5, 6].
Extraneural tissues have been proposed as analterative to brain biopsy to facilitate diagnostic tissuecollection in a number of neurodegenerative lysosomaland peroxisomal disorders [7]. Rectal biopsy is simpleto perform, scarcely traumatic, and cost-effective. Apartfrom the epithelial and endocrine components, therectal biopsy includes numerous cytotypes, e.g.,inflammatory cells, vascular cells, smooth muscle cells,Schwann cells, and ganglion cells, which canaccumulate specific lipopigment inclusions. In a reviewon the diagnostic value of extracerebral biopsy inlysosomal and peroxisomal disorders, the diagnosticcontribution of rectal biopsy to Kufs disease has beenrated as essential [7].
Here we report a problematic case of Kufs disease
with clinical, histological, and ultrastructural docu-mentation serving as a teaching case to illustrate themany diagnostic traps that can be encountered whileexamining cerebral and extracerebral tissues, and inparticular rectal mucosa, for diagnostic purposes.
CASE REPORTM.L. was a 53-year-old right-handed woman from
Philippines. She had no personal antecedents ofneurological disease or drug intake. The familial historycould not be recorded. Three years earlier, at the age of50 years, she began to present behavioral disturbances,
loss of memory, and unsteady gait associated withcontinuous jerking of arms and legs, which were worseon action. Sensation was normal, as were the tendon jerks, and the plantar responses were flexor. Gait wasataxic and disturbed by myoclonus.
Cognitive examination was grossly abnormal. Ocularexamination disclosed bilateral macular dystrophy.Results of general physical examination were normal.Both cognitive impairment and jerks increased in thenext years and pharmacoresistant partial motor seizuresdeveloped. Routine hematological and biochemicalinvestigations, as well as serum blood gases, ammonia,vitamins E and B12, folate, very-long-chain fatty acids,arylsulfatase A, b-galactosidase, and b-hexosaminidase
A and B, were all normal. Urinalysis was normal, even ifurinary sediment dolichol estimation was notperformed. Cerebral spinal fluid examination revealed anormal glucose and protein concentration; oligoclonalbanding was absent. Furthermore, testing for thepresence of the 14-3-3 protein was negative.
On molecular genetic investigation, we also ruledout mutations of the genes causing dentato-rubro-pallidoluysian atrophy, Huntington chorea, Friedreichataxia, spino-cerebellar atrophy (SCA) type 1, 2, 3, 6,and 7, myoclonus epilepsy, and ragged-red fiberssyndrome, and all known mutations of the prion proteingene on chromosome 20 related to Creutzfeldt Jacobdisease. The genotype of the apoliprotein E alleles in
this patient was e3^e4. MRI study revealed moderateatrophy over both hemispheres, with no definitewhite matter abnormalities. Electroencephalographicrecordings showed diffuse background slowingassociated with spikes and sharp-wave complexesinvolving both hemispheres. Intermittent photicstimulation never elicited a photoparoxysmal or
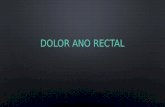
FIG. 1 Rectal mucosa. Perivascular smooth musclecell showing fingerprint inclusions (arrows).TEM. Original magnification, 6,000.
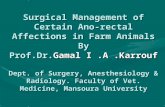
FIG. 2 Rectal mucosa. At high magnificationcurvilinear profiles (arrowheads) and fingerprints (arrows) are visible. TEM.Original magnification, 40,000.
44 G. Pasquinelli et al.

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 3/8
photomyoclonic response. Electrical stimulation ofeither median nerve failed to produce a large cortical
somatosensory evoked potential.In 2 different instances the patient underwent
rectoscopy for collecting multiple fragments of rectalmucosa suited for ultrastructural investigation. Sixmonths after our first examination, the patient becamebedridden and months later died because of pulmonaryinfection. A pathological examination was made. Atautopsy, mild cerebral atrophy was found andmultiorgan tissue sampling was performed.
MATERIALS AND METHODSFresh rectal endoscopic biopsies were immediately
fixed in 2.5% buffered glutaraldehyde, postfixed in 1%
osmium tetroxide, and routinely processed for electronmicroscopy. Thin sections were stained with uranyl
acetate and lead citrate and viewed with a Philips 410transmission electron microscope.
Autoptic samples were collected from the fronto-parietal cortex, cerebellum, cardiac and skeletalmuscles, skin, and liver. The samples were routinellyfixed in 10% buffered formalin and processed forlight microscopy. Paraffin-embedded sections werestained with hematoxylin and eosin as well as with PASand PAS =D. Fragments from the frontoparietal cortexand skin were additionally fixed in glutaraldehyde andprocessed for electron microscopy. For immuno-histochemistry, frontoparietal cortex paraffin sectionswere stained with anti-protein tau (Ab-3, 1:200,NeoMarkers, Fremont CA, USA) and anti-ubiquitin
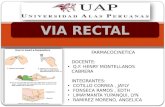
FIG. 3 Autoptic frontoparietal cortex. PAS-positive diastase-resistant intraneuronal inclusions. PAS =D. Original magnification, 40.
Kufs Disease Diagnosis on Rectal Biopsy 45

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 4/8
(Abi-1, 1:100, NeoMarkers, Fremont CA, USA)polyclonal antibodies followed by routine ABCmethod. Immunostains were performed by usingappropriate controls.
RESULTSIn rectal mucosa biopsies we studied epithelial cells,inflammatory cells, Schwann cells, peripheral nerveendings, endothelial cells, and smooth muscle cells. Inone tissue bioptic series, the samples contained onlysurface elements thus limiting the examination to therather not diagnostic elements, e.g., epithelial andinflammatory cells. Although extensively searched, noganglion cells could be identified in all the screenedbiopsies. Several fingerprint inclusions were located inthe cytoplasm of perivascular smooth muscle cells(Figure 1); no other cytotypes were found to beinvolved. At high magnification, the inclusions showedthe typical association of curvilinear profiles andfingerprint structures (Figure 2). The latter werecomposed of stacks of paired, straight or curving,lamellae separated from the adjacent pair by a narrowclear space. No GRODs were seen. Theseultrastructural findings were consistent with thediagnosis of Kufs disease.
Histopathological study of frontoparietal cortextaken at autopsy showed loss of neurons, astrocytosis,and corpora amilacea; numerous intraneuronalPAS-positive, diastase-resistant inclusions were alsofound (Figure 3); these inclusions corresponded toGRODs at the ultrastructural examination (Figure 4).Putative GRODs with a higher lipidic content were also
seen (Figure 5). No fingerprint inclusions were found.Immunohistochemical detection of protein tau and
ubiquitine was negative. In the cerebellum no loss ofPurkinje cells was found (Figure 6); the skeletal,cardiac muscles were unaffected; the skin did not revealany cytoplasmic accumulation of lipopigment in theeccrine sweat gland epithelial cells and fibroblasts bothat light and electron microscopy level; the liver showedmoderate to severe steatosis.
DISCUSSIONThe patient described here had a clinical picture
consistent with Kufs disease. Although extensivelyinvestigated, the laboratory, biochemical, and mol-ecular genetic tests failed to disclose any possiblediagnostic alternative. Postmortem autoptic study ofthe frontoparietal cerebral cortex revealed age-relateddegenerative lesions as well as PAS-positive,diastase-resistant intraneuronal lipopigment inclusions.Ultrastructurally, these inclusions corresponded tocytoplasmic collections of moderately electron-dense,
granular inclusions, which we interpreted as GRODs.According to Carpenter et al. [8], GRODs are difficultto distinguish from conventional lipofuscin on electronmicroscopy. Clues for the GROD nature of theinclusions are uniform matrix granularity, moderateelectron density, and poor lipidic content; however, asFigure 5 demonstrates, a clear-cut distinction betweensuch inclusions is not always possible. Consequently,we believe that the final diagnostic interpretationshould be driven by the clinical and laboratory back-ground as well as by the absence of any possiblediagnostic alternative.
Further, GRODs and fingerprints are not alwaysexpressed in the same tissue; in fact, in our patient thefingerprints were found in the rectal mucosa but not inthe frontoparietal cortex while the reverse was true with
FIG. 4 Autoptic frontoparietal cortex. Collections of granular osmiophilic deposits (GRODs) in theneuronal cytoplasm. TEM. Original magnification, 6,000.
FIG. 5 Autoptic frontoparietal cortex. Detail of putative GRODs associated with neutral lipids. TEM. Original magnification, 18,000.
46 G. Pasquinelli et al.

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 5/8
GRODs. This previouslyunfocusedcharacteristic could,at least in part, explain the plethora of differentlytextured inclusions that have been published in the pastspecific literature (for an example, see [9]). Moreover,
our investigation of extraneural autoptic tissues failedto demonstrate any specific findings; in particular,cutaneous eccrine sweat gland epithelial cells andfibroblasts were unremarkable at both the light andelectron microscopy levels. This confirms previousreports that studies of extracerebral tissues give variableresultswithouta consistent diagnostic pattern [5,6, 10].
In the setting of storage diseases, fingerprintinclusions are believed to be virtually unique to Kufsdisease. Ultrastructurally, the fingerprint inclusions arecomposed by tightly bound lamellae that are set in amoderately electron-dense matrix; the lamellae maypresent various spatial arrangements; whorled(fingerprints), stacked, and prismatic (paracristalline)
profiles are possible in relation to the plane ofsectioning; the matrix frequently contains curvilinearprofiles, also described as C-shaped or worm-likeprofiles [11]. Based on a mandatory, detailed know-
ledge of the morphological criteria for specific storage,nonspecific structures, and artifacts [12], the finger-print inclusions can be accurately differentiated fromconventional lipofuscin bodies, showing coarselygranular, electron-dense material intermixed with large,poorly osmiophilic lipidic globules; multivescicularbodies, showing packed vesicles set in a dense matrix;myelinosomes, containing whorls, stacks of collapsedor reticulated lamellae; and angulated lysosomes ofGaucher-like type, containing sheaves of rigidfilaments and lamellae. The present case showedtypical fingerprint inclusions in perivascular smoothmuscle cells of rectal mucosa, which were consistentwith the diagnosis of Kufs disease.
FIG. 6 Autoptic cerebellar cortex. The Purkinje cell layer appears well preserved. EE. Original magnification, 40.
Kufs Disease Diagnosis on Rectal Biopsy 47

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 6/8
GRODs and fingerprints are believed to be themorphological expression of protein accumulationwithin cytoplasmic lysosomes, with phospholipids,neutral lipids, and metals accounting for the rest of theinclusion content [13]. Mitochondrial ATP synthetasesubunit c (SCMAS) is the major protein component ofsuch inclusions at least in 4 types of NCLs (CNL 2, 3, 5,8) but is not present in infantile NCL (CLN 1), whichhas been demonstrated to accumulate lysosomalprotein saponins (SAP) A&D [14]; subunit c has beenhistochemically documented in CNL 4 and 6 [15];lysosomal protease deficiencies, i.e., palmitoyl proteinthioesterase and pepstatin-insensitive peptidase, weredemonstrated in CLN 1 and CLN 2, respectively [13].Based on this biochemical setting, it can be suggestedthat the lipopigment inclusions reflect a general cellprotease defect or impairment and that theultrastructural morphology of these inclusions mayamount their biochemical composition, i.e., SAPaccumulation corresponding to GRODs and SCMAS
to fingerprint =curvilinear inclusions [1].On the practical ground, it is necessary to screen,
ultrastructurally, a great diversity of cells even whenthe inclusions are thought to be restricted to a maincell component. For this purpose, rectal biopsy issimple, safe, scarcely traumatic, and cost-effective;further, many cytotypes can be examined, includingthe numerous axonal terminals and sustain cells lyingfree in the lamina propria stroma as well as ganglioncells of mioenteric plexi. However, diagnostic diffi-culties exist when (1) the biopsy is not deep enoughto allow the sampling of ganglion and smoothmuscle cells, and this was our experience with thepresent routine endoscopic material; or (2) a singlecytotype presents fingerprint inclusions exclusively. Inour case the fingerprints were located in perivascularsmooth muscle cells only. As previously discussed,these inclusions have sufficiently distinctiveultrastructural characteristics to be identified withconfidence; however, identical structures have beenfound in the smooth muscle cells of human renalarterioles [5], thus raising the possibility thatfingerprints could be a previously unrecognizedfeature of normal smooth muscle cells from humanrectal submucosa arterioles.
As illustrated by the present case, the lack of aspecific genetic locus alteration makes the diagnosis ofKufs disease rather difficult; in fact, the value ofultrastructural documentation of GRODs and finger-print inclusions can be narrowed by the paucity ofspecific findings, monotype cell involvement, dis-sociated expression of the specific inclusions in tissues,as well as by the variable results observed in theextraneural tissues. To this respect, we suggest that awell-established diagnosis cannot be achieved whenonly one cytotype is affected by specific inclusions.
REFERENCES1. Haltia M. The neuronal ceroid-lipofuscinoses. J Nueropathol
Exp Neurol . 2003;62:1^13.2. Boldrini R, Biselli R, Santorelli FM, Bosman C. Neuronal ceroid
lipofuscinosis: an ultrastructural, genetic, and clinical studyreport. Ultrastruct Pathol . 2001;25:51^58.
3. Dyken PJ. The neuronal ceroid lipofuscinoses. J Child Neurol .1989;4:165^174.
4. Mole SE. Batten’s disease: eight genes and stillcounting? Lancet . 1999; 354:443^445.
5. Berkovic SF, Carpenter S, Andermann F, Andermann E,Wolfe LS. Kufs’ disease: a critical reappraisal. Brain .1988;111:27^62.
6. Goebel HH, Braak H. Adult neuronal ceroid-lipofuscinosis. ClinNeuropathol . 1989;8:109^119.
7. Ceuterick-de Groote C, Matin JJ. Extracerebral biopsy inlysosomal and peroxisomal disorders: ultrastructural findings.Brain Pathol . 1998;8:121^132.
8. Carpenter S, Karpati G, Wolfe LS, Andermann F. A type of juvenile cerebromacular degeneration characterised by granularosmiophilic deposits. J Neurol Sci . 1973;18:67^87.
9. Zeman W, Siakotos AN. Neuronal ceroid-lipofuscinoses. In:Lysosomes and Storage Diseases . Hers HG, Van Hoof F, eds.New York: Academic Press; 1973;535^542.
10. Carpenter S. Morphological diagnosis and misdiagnosis in
Batten-Kufs disease. Am J Med Gen . 1988;5:85^91.11. Ghadially FN. Ultrastructural Pathology of the Cell and Matrix ,ed 4. London:Butterworth-Heinemann; 1997;752^755.
12. Martin JJ, Ceuterik C. The contribution of pathology to thestudy of storage disorders. Pathol Res Pract .1988;183:375^385.
13. Palmer DN, Fearley IM, Walker JE et al. Mitochondrial ATPsynthetase subunit c storage in the ceroid-lipofuscinoses. Am J Med Gen . 1992;42:561^567.
14. Tyynela Y, Suopanky J, Baumann M, Haltia M. Sphingolipidactivator proteins (SAPs) in neuronal ceroid-lipofuscinosis.Neuropediatrics . 1997;28:49^52.
15. Jolly RD, Bown S, Das AM, Walkley SU. Mitochondrialdysfunction in the neuronal ceroid-lipofuscinosis (Battendisease). Neurochem Int . 2002;40:565^571.
48 G. Pasquinelli et al.

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 7/8

8/13/2019 Digest Rectal
http://slidepdf.com/reader/full/digest-rectal 8/8
Copyright of Ultrastructural Pathology is the property of Taylor & Francis Ltd and its content may not be
copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.