Diffuse Pulmonary Arteriovenous Malformation in a Child with Polysplenia Syndrome
6
DIFFUSE PULMONARY ARTERIOVENOUS MALFORMATION IN A CHILD WITH POLYSPLENIA SYNDROME Sudesh Kapur, MD, Jonathan Rome, MD, and Roma S. Chandra, MD Departments of Anatomic Pathology and Cardiology, Children's National Medical Center, Department of Pediatrics and Pathology, George Washington University School of Medicine, Washington, DC, USA Pulmonaly arteriovenous malfmmation (PAVM) is usually seen as a well-circumscribed cystic mass. In this communication we describe a diffuse arteriovenous malfmmation in a 5-month-old infant. The lesion was seen only at the microscopic he1 and was associated with abdominal heterotaxy, atrial situs solitus, polysphia, interrupted in fm'or vena cava, atrial septal defect, and atrioventricular canal. This uncommon association may be within the spectrum of polyspbnia syndrome. Keywords diffuse pulmonary arteriovenous malformation, polysplenia Pulmonary arteriovenous malformation is extremely rare in children [ 1-61. These lesions have been called pulmonary arteriovenous malforma- tion (PAVM), pulmonary arteriovenous fistula, pulmonary arteriovenous aneurysm, pulmonary angioma, cavernous hemangioma, and pulmonary hamartoma. Most occur singly, but some multiple lesions have also been observed. They may be isolated lesions or may be seen with more generalized angiodysplasia such as Osler-Weber-Rendu disease. We report a case of diffuse pulmonary arteriovenous malformation in a 5-month-old child with abdom- inal heterotaxy, polysplenia, and atrial septal defect. The unusual clinical setting and diffuse nature of the lesion form the basis of this report. The histopathologic changes of the P A W are described. CASE REPORT An asymptomatic,acyanoticmale infantwas evaluated for a heart murmur at 2 months of age. Two-dimensional echocardiography demonstrated a b Received 6 June 1994;accepted 6 June 1994. Address correspondence to Sudesh Kapur, M.D., Department of Anatomic Pathology, Children's Hospital, 11 1 Michigan Avenue, N.W., Washington, DC 20010. Pediutn'cPathology &? Lubmatq Medicine, 15r463-468, 1995 Copyright 0 1995 Taylor €9 Francis 1077-1042/95$10.00+ .OO 463 Fetal Pediatr Pathol Downloaded from informahealthcare.com by University of Adelaide on 11/17/14 For personal use only.
Transcript of Diffuse Pulmonary Arteriovenous Malformation in a Child with Polysplenia Syndrome

DIFFUSE PULMONARY ARTERIOVENOUS MALFORMATION IN A CHILD WITH POLYSPLENIA SYNDROME
Sudesh Kapur, MD, Jonathan Rome, MD, and Roma S. Chandra, MD Departments of Anatomic Pathology and Cardiology, Children's National Medical Center, Department of Pediatrics and Pathology, George Washington University School of Medicine, Washington, DC, USA
Pulmonaly arteriovenous malfmmation (PAVM) is usually seen as a well-circumscribed cystic mass. In this communication we describe a diffuse arteriovenous malfmmation in a 5-month-old infant. The lesion was seen only at the microscopic h e 1 and was associated with abdominal heterotaxy, atrial situs solitus, polysphia, interrupted in fm'or vena cava, atrial septal defect, and atrioventricular canal. This uncommon association may be within the spectrum of polyspbnia syndrome.
Keywords diffuse pulmonary arteriovenous malformation, polysplenia
Pulmonary arteriovenous malformation is extremely rare in children [ 1-61. These lesions have been called pulmonary arteriovenous malforma- tion (PAVM), pulmonary arteriovenous fistula, pulmonary arteriovenous aneurysm, pulmonary angioma, cavernous hemangioma, and pulmonary hamartoma. Most occur singly, but some multiple lesions have also been observed. They may be isolated lesions or may be seen with more generalized angiodysplasia such as Osler-Weber-Rendu disease. We report a case of diffuse pulmonary arteriovenous malformation in a 5-month-old child with abdom- inal heterotaxy, polysplenia, and atrial septal defect. The unusual clinical setting and diffuse nature of the lesion form the basis of this report. The histopathologic changes of the P A W are described.
CASE REPORT
An asymptomatic, acyanotic male infantwas evaluated for a heart murmur at 2 months of age. Two-dimensional echocardiography demonstrated a b
Received 6 June 1994; accepted 6 June 1994. Address correspondence to Sudesh Kapur, M.D., Department of Anatomic Pathology, Children's
Hospital, 11 1 Michigan Avenue, N.W., Washington, DC 20010.
Pediutn'c Pathology &? Lubmatq Medicine, 15r463-468, 1995 Copyright 0 1995 Taylor €9 Francis 1077-1042/95$10.00+ .OO 463
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.

464 S. KAPUR ET AL.
dominal situs ambiguous, atrial situs solitus, transitional atrioventricular canal with cleft mitral valve, and interruption of the inferior vena cava with azygous continuation. Functioning splenic tissue was demonstrated by nu- clear medicine scan. Polysplenia type of heterotaxia syndrome was diagnosed. At 5 months of age, the child presentedwith respiratory distress and hypoxemia. Chest radiography demonstrated cardiomegaly, hyperinflation, prominent pulmonary vascular markings, and no pneumonia. At cardiac catheterization severe pulmonary venous desaturation present in room air ( P W saturation = 66%), persisted with 0.94 F102 ( P W saturation = 83%). The Qp/Q ratio was 1 .0 with bidirectional intracardiac shunting. Normal pulmonary arterial and venous pressures were present with means of 13 and 7 mm Hg, respec- tively. Pulmonary arteriography demonstrated large central pulmonary arter- ies, dilated peripheral vessels with abnormal tapering, absence of background haze, and rapid filling of pulmonary veins. An open lung biopsy showed no pathologic changes. Subsequently, the arterial septal defect was closed. Post- operatively, severe atrial desaturation persisted and the infant expired.
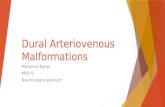
Significant findings noted at autopsy included abdominal heterotaxywith right-sided spleen and stomach, midline liver, malrotation of the bowel with absent ligament of Treitz, midline cecum, and right-sided descending colon. The spleen consisted of one major spleen with a large cleft and three smaller spleens attached with a stalk of fibrofatty tissue to a short pancreas mostly limited to the duodenal loop. The heart was in normal position with a d-loop and normally related great vessels. A patch closing the primum atrial septal defect was noted. The anterior cusp of the mitral valve was cleft. The inferior vena cava was interrupted above the renal veins and drained into the superior vena cava through a dilated azygous vein. The hepatic veins drained into the right atrium. Both lungs had two lobes with bilateral hyparterial bronchi. Lung parenchyma showed focal hemorrhages and congestion without any grossly visible lesions. The main pulmonary artery was injected with barium- gelatin mixture, which immediately drained back from the left upper pulmo- nary vein. Pulmonary veins were markedly dilated but drained normally to the left atrium. Pulmonary angiogram showed multiple corkscrew tortuous vessels forming the background in all the lobes (Figure 1 ) .
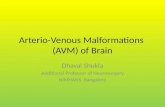
Sections of the lungs showed dilated elastic pulmonary arteries accompa- nying the bronchi. Multiple angiomatoid lesions composed of thin-walled vascular channels with a single layer of elastica were seen in the parenchyma filled with barium (Figure 2). The pulmonary veins in the fibrous septa were somewhat thickened, tortuous, dilated, and filled with barium. An occasional dilated vein showed an anomalous connection to the angiomatoid vascular channels in the vicinity of a bronchus. These vascular lesions were seen in both lungs, most prominently in the left and right upper lobes, and spared the lingula. The alveoli and the bronchi at all levels were unremarkable.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.

DIFFUSE PULMONARY ARTERIOVENOUS MALFORMATION 465
Figure 1. Postmortem angiogram of the left lung showing dilated pulmonaly artery and its branches with excessive background filling by many tortuous corkscrew vessels.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.

466 S. KAPUR ET AL.
Figure 2. A section of the lung showing a typical angiomatoid lesion composed of multiple thin-walled vascular channels filled with barium. H&E section, ~ 5 1 , reproduced at 79%.
DISCUSSION
We describe a 5-month-old child for whom a diagnosis of PAVM was made at autopsy by postmortem injection of barium-gelatin mixture. Macroscopic examination of the lungs at autopsy and a lung biopsy failed to detect the lesion. The spectrum of P A W extends from multiple microscopic lesions to a large multicystic lesion. Multicystic P A W is most often subpleural and is seen as a single circumscribed lesion composed of dilated venous and arterial channels. Thrombosis and calcification may be present.
In children, however, the PAVM tends to be more generalized, at micro- scopic level, and has been designated dispersed telangiectatic type [ 3-61. Cooley and McNamara [ 71 were the first to describe a microscopic PAVM.
Pulmonary capillary hemangiomatosis is another diffuse type of vascular malformation seen in the lungs [8, 91. This lesion is histologically quite different and is characterized by nodules and sheets of back-to-back capillar- ies along both sides of the alveolar walls. Pulmonary veins show intimal thickening and most of these patients present with pulmonary hypertension or pulmonary veno-occlusive disease clinically. Pulmonary hypertension with PAVM has been described but is rare [lo].
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.

DIFFUSE PULMONARY ARTERIOVENOUS MALFORMATION 467
The incidence of P A W in children is low; in a review of 350 cases of PAVM only 17% were seen under the age of 10 years [ll]. One third of the cases are associated with Osler-Weber-Rendu disease [ 11,121. In the present case no evidence of mucocutaneous angiomas was seen.
Clinically the diagnosis may be difficult. In suspected cases with persistent cyanosis diagnosis is made by pulmonary angiogram or by contrast echo- cardiography. Sometimes the diagnosis may be overlooked at autopsy because grossly visible telangiectasia may not be present. Injection of barium-gelatin mixture followed by roentgenography has been found to be very helpful in demonstrating the anomalous connections.
In the present case there was an associated atrial septal defect, abdominal heterotaxy, polysplenia, and short pancreas. Such association is rare. Knight et al. [4] reported three children with diffuse PAVM as seen in the present case; one of the cases had atrial septal defect with abdominal heterotaxy, but there was only one right-sided spleen and the status of lobation pattern of the lungs was not mentioned. Landing [12] has described five different types of malformation complexes with isomerism of the lungs, abnormality of spleen, and congenital heart disease. Polysplenia complex is the most common form. None of these cases and a review of 146 cases described by Peoples et al. [ 131 were found to have PAVM. Papagiannis et al. [ 141 recently described a patient with polysplenia, dextrocardia, left atrial isomerism, and PAVM without any intracardiac shunts. Diagnosis in this case was made by angiography and lung biopsy. The etiology of polysplenia is not known. It is rarely familial and is probably a field defect. The present report adds to the small number of cases of PAVM associated with polysplenia and raises the possibility that P A W may be a component, albeit rare, of the polysplenia syndrome.
REFERENCES 1 . Burke CM, Safai C, Nelson D, W i n T. Pulmonary arteriovenous malformations: A critical update.
2. Dines DE, Seward JB, Bernatz PE. Pulmonary arteriovenous fistula. Mayo Clin Proc 1983;58:176-81. 3. Finn U, Brandrup F. Pulmonary arteriovenous fistulas in children. Acta Paediat Scand 1973;
4. Knight WB, Bush A, Busst CM, Haworth SG, Bowyer JJ, Shinebourne EA. Multiple pulmonary
5. Przybojewski ]Z, Martiz E. Pulmonary arteriovenous fistulas; a case presentation and review of
6. Shumaker HB Jr, Waldhausen ]A. Pulmonary arteriovenous fistulas in children. Ann Surg 1963;158:
7. Cooley DA, McNamara DG. Pulmonary telangiectasia: Report of a case proved by pulmonary biopsy.
8. Tron V, Magee F, Wright JL, Colby T, Churg A. Pulmonary capillary hemangiomatosis. Hum Pathol
9. Wagenvoort CA, Beetstra A, Spijker]. Capillary hemangiomatosis of the lung. Histopathology 1978;2:
Am Rev Respir Dis 1986;134:334-9.
62~422-32.
arteriovenous fistulas in childhood. IntJ Cardiol 1989;23:105-16.
literature. S Afr Med J 1980;57:366-77.
713-20.
J Thorac Surg 1954;27:614-22.
1985;17:1144-50.
401-6.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.

468 S. KAPUR ET AL.
10. Sapru R, Hutchinson DSC, Hall JI. Pulmonary hypertension in patientswith pulmonary arteriovenous
11. Bosher Lfl Jr, Blake DA, Byrd BR. An analysis of the pathologic anatomy of pulmonary arteriovenous
12. Landing BH. Five syndromes (malformation complexes) of pulmonary symmetry, congenital heart
13. Peoples WM, MollerJH, Edwards JE. Polysplenia: A review of 146 cases. Pediat Cardiol 1983;4:129-37. 14. PapagiannisJ, Kanter R, Effman EI., et al. Polysplenia with pulmonary arteriovenous malformations.
fistulae. Br HeartJ 1969;31:559-69.
aneurysms with particular reference to local excision. Surgery 1959;45:91-104.
disease and multiple spleens. Pediatr Pathol 1984;2:125-33.
Pediau Cardiol 1993;14:127-9.
Feta
l Ped
iatr
Pat
hol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
17/1
4Fo
r pe
rson
al u
se o
nly.