Differential diagnosis of oral and maxillofacial lesions
62
-
Upload
ahmed-adawy -
Category
Health & Medicine
-
view
66 -
download
4
Transcript of Differential diagnosis of oral and maxillofacial lesions


Dr. Ahmed M. Adawy Professor Emeritus, Dep. Oral & Maxillofacial Surg.
Former Dean, Faculty of Dental MedicineAl-Azhar University

A wide variety of lesions from the soft tissues; mucosaand submucosal structures, or hard tissues; bone andodontogenic structures may arise in the orofacial region.Diagnosing such lesions is necessary for the propermanagement of patients. Clinical diagnosis is thecognitive process of applying logic and knowledge, in aseries of step-by-step decisions, to create a list ofpossible diagnoses. A thorough history and a completeoral examination are required. Radiographicexamination, laboratory investigation, and, if indicated,surgical procedure to obtain a biopsy specimen forpathologic examination are also helpful

Oral lesions usually manifest as one of the following: (1)
change in colour; (2) swelling; (3) ulcers; (4) vesiculo-bullous
or (5) surface textural changes [1,2]. The word swelling denotes
any enlargement or protuberance over the body surface [3] . The
swellings may be classified as a sessile or pedunculated based
on the type of junction of the lesion with underlying tissue.
Anatomically, the swellings may also be classified as central
and peripheral lesions. The term exophytic lesions represent
any pathological growth that projects above the normal
contours of the oral surface epithelium [4]. Ulcerations, are loss
of epithelium. Whereas, vesiculo-bullous indicate loculated
fluid in or under the mucosa

"Chief Complaint." is a poor name for what we want the
patient to tell us. To some patients it is not a "complaint",
but to most, they come with a "problem". The primary
task is to seek out and understand the patient's problem. To
do this you must, first, listen carefully to what the patient
says. Second, analyze and interpret the problem. Most of
our patients, however, did not seek medical advice unless
they have pain and/or swellings. Further, many of the
orofacial lesions are completely asymptomatic and are
discovered accidentally during regular chick-up or
periodic radiographic examination

The patient should be questioned for the following:
1. How long has the lesion been present?. The duration of
the lesion may provide valuable clues to its nature. For
instance, a lesion that has been present for several years
may be congenital.
2. Has the lesion changed in size?. If so, at what rate and
to what magnitude?. A rapidly growing lesion is more
likely to be aggressive, whereas a slow-growing lesion
may indicates a more benign process

3. Has the lesion changed in character ?. For example, if a
lesion presented as an ulcer, but the patient says that it
began as a vesicle, a more thorough search for other signs
or symptoms of a vesiculo-bullous or viral disease may be
indicated.
4.What symptoms are associated with the lesion? (e.g.,
pain, abnormal sensations, anesthesia, a feeling of
swelling, bad taste or smell, dysphagia, swelling or
tenderness of adjacent lymph nodes)

If painful, what is the character of the pain?. What
exacerbates and what diminishes the pain?. Pain is most
often associated with lesions that contain an inflammatory
component. Cancer, although referred as a painful lesion,
often is not. Numbness in the distribution of one of the
sensory nerves may indicates an inflammatory or
malignant process. Dysphagia indicates that the muscles
of deglutition are involved

Swelling may be one of the common symptoms associated
with oral lesions, which indicates nothing more than
expansile process that can result from a variety causes.
Slow-growing masses (duration of months to years) are
usually benign. Whereas, rapidly growing masses ( hrs to
days) are usually inflammatory. In general, tender lymph
nodes indicate an inflammation

5. Are there any associated constitutional symptoms
(e.g. fever, nausea, anorexia)? For example, systemic viral
illnesses e.g., measles [5] can cause oral manifestations
along with the systemic illness. Interesting to note that
lymphoma and leukemia are usually accompanied with
low grade fever [6]

6. Is there any historic reason for the lesion (e.g., trauma
to the area, a recent toothache)?. Frequently, lesions in and
around the oral cavity are caused by habits, hard or hot
foods, and recent trauma. Ill-fitting prosthetic device,
cheek biting, sharp teeth, and other habits are common
causes of oral lesions. Additionally, the dentition should
always examined very carefully when a lesion is found,
because many of such lesions have some relationship to
the teeth

You have to think of your patient demographically, as part
of an age, sex, racial and occupational group, while you
consider their problem. Many diseases and conditions are
found in specific age, sex, race and occupational clusters.
For example, oral squamous cell carcinomas are more
common in males aged between 51 to 70 years, mainly
due to smoking habit. The most frequent sites are lower
lip vermilion, tongue, and gingiva/alveolar ridge. There
was a strong association between outdoor occupation,
mainly farmers, and white skin color with lip squamous
cell carcinoma [7]

An accurate health history, and, if needed, consultationwith medical specialists are mandatory for two basicreasons: The first reason is that a patients with certainmedical conditions, such as congenital heart defects,coagulopathies, and hypertension, may require specialprecautions when any surgical treatment is required. Thesecond reason is that the lesion under investigation may bean oral manifestation of a systemic disease. For instance,multiple lytic lesions and loss of lamina dura bone suggestthe possibility of hyperparathyroidism [8]. A patient withmultiple radiolucencies of the jaws or other bones mayalso have multiple myeloma [9]

It is very helpful to draw the lesion in the patient’s chart [10].
This allows follow-up the course of the lesion over time and
determines whether it is resolving or changing in nature

Lesions may arise from any tissue within the oral cavity,
including mucosal epithelium, submucosal connective
tissue, muscle, tendon, nerve, bone, blood vessels, and
salivary glands. The exact anatomic location of the lesion
should aid in this determination. For example, if a mass is
present on the dorsum of the tongue, an epithelial,
connective tissue, or muscle origin for the mass should be
considered. Similarly, a swelling on the floor of the
mouth, salivary gland etiology has to be included in
differential diagnosis

The lesion should be described as one of the several types of medical terminology [11]:Macule: circumscribed area of color change without elevation
Nodule: large palpable mass, elevated above the epithelial surface
Papule: small palpable mass, elevated above the epithelial surface
Ulcer: loss of epithelium
Erosion: superficial ulcer
Bulla: loculated fluid in or under the epithelium of skin or mucosa
Vesicle: small loculation of fluid in or under the epithelium
Pustule: cloudy or white vesicle, the color of which results from the presence of pus

The clinical characters such as consistency of the lesion(soft/hard), color and pigmentation of the lesion, shape ofthe swelling, base of the growth, location of the lesion(anterior/posterior jaw; labial/buccal mucosa) areimportant parameters in decision making. The obtainedinformation should be analyzed step by step for successfuldiagnosis of the lesion.
Site
Size
Shape
Shade
Surface

Certain locations correspond to certain diseases. Some
lesions occur in certain locations but don't occur in others.
For example, the peripheral ossifying fibroma is seen only
on the gingiva because it is of periodontal ligament origin.
Thus, a lesion located on the lip could not be a peripheral
ossifying fibroma. Meanwhile, lesions of salivary gland
etiology should be excluded form gingival swilling,
simply because salivary glands are not present their.
Another reason location is important, is that certain lesions
occur more frequently in some areas than others. For
example, dentigerous cysts, and ameloblastomas are
commonly seen in the angle and ramus of the mandible

The presence multiple lesions is an important
diagnostic sign. When multiple areas of ulceration are
found within the oral cavity, the possibility of a vesiculo-
bullous disease is suggested. It is unusual to find multiple
areas of carcinoma in the mouth. Likewise, multiple
osteolytic lesions should raise the possibility of multiple
myeloma, metastatic malignancy, and metabolic
abnormality (i.e., hyperparathyroidism)

Accurate recordings of these two basic physical
characteristics should be made for future reference.
Accurate measurements allow to follow the changes in
the size of the lesion. Rapidly growing lesions with a
history of resolution and remission are usually
inflammatory ones. It is not typical for any true
neoplasm to remit or regress, although some will have
periods of biological inactivity. Measurement of the
lesion is also used in the T staging of oral squamous
cell carcinoma and salivary gland malignancies

The color or colors are an important consideration. A
bluish swelling that blanches by pressure may indicate a
vascular lesion, whereas a bluish lesion that does not
blanch may indicate a mucus-containing lesion. A
pigmented lesion of the oral mucosa may carry more
importance than a lesion of normal color. An erythematous
lesion may be more ominous than a white lesion. Some
lesions may have more than one color, and this should be
noted in detail. Frequently, inflammation is superimposed
on areas of the lesion because of mechanical trauma or
ulceration, which gives a varied picture from one time to
the next

Normal mucosal color in elevated lesions indicates the
pathology is submucosal in origin. Most commonly,
normal color lesions may be due to one of several forms of
underlying pathosis, e.g. hyperplasia, neoplasia, fluid
accumulation, or cyst formation

In general, the white color of a lesion is due to 1) a thickening of
the epithelium (which may be the result of hyperkeratosis,
acanthosis, or edema of the epithelial cells), 2) a whitish
pseudomembane composed of surface debris or fungal colonies
covering the epithelium, or 3) decreased vascularity or various
deposits affecting the underlying connective tissue [12]

The red color of a lesion is usually indicative of :
1) an inflammatory lesion of variable etiology (e.g. reactive,
allergic, or infectious) accompanied by hyperemia,
2) an atrophy of the epithelium allowing easier visualization of
the vascular component of the underlying connective tissue, or
3) a lesion featuring proliferation of blood vessels [12]

In most instances, blue/purple discoloration of oral mucosa is
produced by blood-containing vascular lesions, or mucus-
containing salivary gland lesions. In contrast, a brown/gray/black
discoloration usually ensues from accumulation of either
exogenous stain or melanin [12]

The surface of the lesion may be smooth lobulated, or
irregular. If ulceration is present, the characteristics of the
ulcer base should be recorded. Ulcer beds can be smooth;
full of granulation tissue: covered with a slough,
membrane, or scab; or fungating, such as is seen with
some malignancies

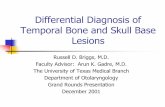
Schematic view of surface and base characteristics
of exophytic lesions [13]

Nodular lesion with
smooth surface
Dome-shaped lesion
With smooth surface

Papillary growth
Verrucous lesions
Surface

A sessile lesion with ulcerated
smooth surface
Pedunculated lesion with
granular surface

The sharpness of the boundaries of the lesion is an
important sign. If a mass is present, is it fixed to
surrounding deeper tissues or is it freely movable?. The
determination of the boundaries will aid in establishing
whether the mass is fixed to bone, arising from the bone
and extending into soft tissues, or of an infiltrating nature.
The same applies to an ulceration; however, a description
of the boundaries should include a physical description of
the margins. The margin of an ulcer may be flat, rolled,
raised, or everted

The consistency of lesions is described as soft, as in the
case of a lipoma; firm, which is the consistency of a
fibroma; or hard, as in the case of an osteoma or tori.
Indurated simply means firm or hard
Lipoma Fibroma Osteoma

Fluctuation is the term given to a wavelike motion felt on
palpating a mass or cavity with nonrigid walls, which
contains fluid. This is a valuable physical sign, because it
usually indicates fluid within the mass. It can be elicited
by palpating with two or more fingers in a rhythmic
fashion, such that as one finger exerts pressure, the other
finger feels the impulse transmitted through the fluid-filled
cavity

Palpation of a mass may reveal a pulsatile quality, which
indicates a large vascular component. This is especially
important in bony lesions. A thrill is the name given to the
palpable vibration accompanying a vascular murmur or
pulsation. If a thrill is palpable, auscultation with a
stethoscope may reveal a bruit, or audible murmur.
Lesions with palpable thrills or audible bruits should be
referred to a specialist for treatment, because life-
threatening hemorrhage can arise when biopsy is
attempted

Inspection and palpation of the areas around the lesion,
including the regional lymph nodes, is mandatory. The
presence of neck swellings is not an uncommon finding,
especially in patients with oral infections or malignancies.
Lymphatic drainage from oral cavity sites is mainly to
submental and submandibular lymph nodes, although
other regional lymph nodes may be involved.
Lymphadenopathy secondary to infection is generally
characterized by both mobile and tender nodes. Patients
with oral cancer typically present with non-tender node
enlargement, with firm or hard lymph nodes on palpation
and fixation [14]

Anatomic location of cervico-facial lymph nodes

Radiographs are useful as diagnostic adjuncts to the
clinical examination and history of lesions within or
adjacent to bone. Compared to the adjacent bone, the
radiodensity of the lesion could be uniformly radiolucent,
radiolucent with patchy opacities within (mixed) and
radiopaque [15]. Radiolucency is a result of resorption of
mineralized tissue or decrease in thickness where as
radiopacity is due to an increase in mineralization,
increase in thickness, superimposition on some other
structures or a result of calcification in soft tissues

Radiolucent
Mixed radiolucent/ radiopaque
Radiopaque

Interpretation of radiographs has been made on a clinical
basis constituted by the following criteria: (1) location (2)
periphery and shape (3) internal structure (4) effect on
surrounding structures and (5) periosteal reactions [16].
The radiographic appearance frequently gives clues to the
true nature of a lesion. For example, the periphery or the
boundary of lesion constitute a broad classification as ill-
defined, well-defined with corticated margins and well-
defined with sclerotic margins

An illdefined (diffuse, irregular, moth-eaten, ragged)
periphery is suggestive of a lesion enlarging by invading
the surrounding bone. A well-defined (circumscribed)
periphery with corticated margins is suggestive of a lesion
enlarged by expansion. A well-defined periphery with a
sclerotic radiopaque margin is suggestive of an extremely
slow-growing lesion enlarged by expansion. Slow
growing lesions often cause expansion with cortical
bowing, while cortical destruction denotes aggressive
inflammatory or neoplastic lesions

Well-defined Ill-defined

Mixed radiolucent radiopaque lesions can be due to
inflammation, metabolic anomalies, fibro-osseous
conditions, or less commonly, malignant processes. [17]
The examples include, “cotton wool” appearance of
fibrous dysplasia and Paget’s disease, “orange-peel”
appearance or “ground glass” appearance of fibrous
dysplasia, “sunburst” appearance of central hemangioma,
and “wind-driven snow” appearance of Pindborg tumor

Mixed radiopaque-radiolucent lesion
exhibiting cotton – wool appearance

Orange peel opacity

Ground glass appearance

Sunburst pattern of trabeculations

Wind-driven snow appearance

Some benign lesions like ameloblastoma occurs in manyforms such as unilocular radiolucency resembling a cyst,soap-bubble pattern , or a multicystic appearance. Otherexamples with similar pattern are central giant cellgranuloma, central hemangioma, and odontogenickeratocystic tumor. “Honeycomb” or “solid pattern” areseen in tumors that have not undergone cystic degeneration
Multilocular lesion

The punched-out periphery is a characteristic feature of
multiple myeloma seen only when tumor destruction
extends to the surface of the bone and there is often no
new bone laid down

When lesions within the soft tissues are proximal to bone,
radiographs may elucidate whether the lesion is causing an
osseous reaction, eroding into the bone or invading the
bony cortex

Several oral lesions may be manifestations of systemic
diseases. For instance, multiple lyric lesions and loss of
lamina dura bone suggest the possibility of
hyperparathyroidism. Serum levels of calcium,
phosphorus, and alkaline phosphatase should identify this
metabolic abnormality. A patient with multiple
radiolucencies of the jaws or other bones may also have
multiple myeloma. Serum protein analysis can be useful
for identifying this disease process

Differential diagnosis is the art or process of
differentiating between two or more conditions / diseases
which share similar signs and symptoms. Differential
diagnosis should be approached on the basis of exclusion.
All lesions that cannot be excluded represent the initial
differential diagnosis and are the basis for ordering tests
and procedures to narrow the diagnosis. Attempts should
be done to come to timely diagnosis via more logical
routes such as decision trees rather than test-and error
methods. A decision tree is a flowchart that organizes
features of lesions so that the clinician can make a series
of orderly decisions to reach a logical conclusion

Decision tree of oral and maxillofacial lesions

The first decision to make when using the decision tree is
whether the lesion is a surface lesion, soft tissue
enlargement, or that of bony origin. Surface lesions consist
of lesions that involve the epithelium and superficial
connective tissue of mucosa and skin. They do not exceed
2-3 mm in thickness. Surface lesions are divided into three
categories based on their clinical appearance: white,
pigmented, and vesicular-ulcerated-erythematous. Soft
tissue enlargements are swellings or masses that are
divided into two categories: reactive and tumors. If a soft
tissue enlargement appears to be a tumor, the clinician
must next determine if the enlargement is benign or
malignant

Decision tree for oral mucosal lesions

Benign tumors, typically have a slow growth rate,
measured in months and years. They can be subdivided into
three categories: epithelial, mesenchymal, and salivary
gland tumors. Malignant neoplasms are more likely to be
painful and cause ulceration of the overlying epithelium
than benign lesions. Since malignant neoplasms invade or
infiltrate surrounding muscle, nerve, blood vessels, and
connective tissue, they are fixed or adherent to surrounding
structures during palpation. In general, benign tumors are
surrounded by a fibrous connective tissue capsule, which
may allow the lesion to be moved within the tissue
independent of surrounding structures

Central jaw lesions develop from both odontogenic and
nonodontogenic origins and have varying degrees of
destructive potential. Common benign cystic lesions
include radicular cysts, and follicular cysts. Benign solid
tumors represent a broad spectrum of lesions such as
ameloblastomas, odontomas, ossifying fibromas, and
periapical cemental dysplasia. Malignant tumors that often
involve the jaw bones include squamous cell carcinomas,
osteosarcoma, and metastatic tumors. In addition, vascular
lesions such as hemangioma and arteriovenous
malformations may develop, further expanding the
differential diagnosis

It should be emphasized, however, that the clinical
descriptions of this presentation are general guidelines,
and exceptions occur. Removal of the lesion and
microscopic examination of the tissue is often the only
way to arrive at a definitive diagnosis


1. Van Dis ML. Swellings of the oral cavity. Dermatol Clin; 14: 355, 1996.
2. Spijkervet FK, Vissink A, Raghoebar GM, van der Waal I.
Vesiculobullous lesions of the oral mucosa. Ned Tijdschr Tandheelkd; 108:
223, 2001.
3. Schneider LC, Schneider AE. Diagnosis of oral ulcers. Mt Sinai J Med;
65: 383, 1998.
4. Wood NK, Goaz PW. Differential diagnosis of oral and maxillofacial
lesions, 5th ed. St. Louis: Mosby; pp. 131, 1997.
5. Katz J, Guelmann M, Stavropolous F, Heft M: Gingival and other oral
manifestations in measles virus infection. J Clin Periodontol; 30: 665,
2003.
6.Vanderschueren S, Knockaert D, Adriaenssens T, et al. From prolonged
febrile illness to fever of unknown origin: the challenge continues. Arch
Intern Med; 163: 1033, 2003.
7. Alves AM, Correa MB, da Silva KD, et al. Demographic and Clinical
Profile of Oral Squamous Cell Carcinoma from a Service-Based Population.
Braz. Dent. J; 28: no.3, 2017.
8. Mittal S, Gupta D, Sekhri S, et al. Oral manifestations of parathyroid
disorders and its dental management. J Dent Allied Sci; 3: 34, 2014.

9. Hong K, Lim AA, Wong R, Chan EH, et al. Multiple Myeloma: Concise
Review of the Literature and A Case Report of Mandibular Involvement. Int J
Dentistry Oral Sci; 3: 309, 2016.
10. Ellis III R. Principles of differentia l diagnosis and biopsy in Peterson LJ:
Contemporary Oral and Maxillofacial Surgery 4th ed. Elsevier; pp. 461, 2005.
11.Oral Pathology: Chapter 1 Introduction To Preliminary Diagnosis Of Oral
Lesions by bitz 27, Sep. 2014.
12. Nikitakis NG. Oral soft tissue lesions: A guide to differential diagnosis
Part I: Introduction and changes in color. Braz J Oral Sci. 2: 291, 2003.
13. Mortazavi H, Yaser Safi Y, Baharvand M, et al. Peripheral Exophytic Oral
Lesions: A Clinical Decision Tree. Int J Dent; 2017: 9193831, 2017.
14. Haddad R, Annino D, Tishler RB. Multidisciplinary approach to cancer
treatment: focus on head and neck cancer. Dent Clin North Am; 52: 1, 2008.
15. Whaites E. Dental Radiography and Radiology. 3rd ed. London: Churchill
Livingstone; pp. 287, 2002.
16. White SC, Pharoah MJ. Oral Radiology Principles and Interpretation. 6
ed. Philadelphia: Mosby; pp. 256-428, 2011.
th

17. Khalek A A, Razek A. Imaging appearance of bone tumors of the
maxillofacial region. World J Radiol; 3: 125, 2011.