
Differential benefits of DAAs in patients with...
56
Differential benefits of DAAs in patients with co-morbidities Marc Bourliere , MD G. Dusheiko, MD Hôpital Saint Joseph UCL Institute for Liver and Health Marseille, France Royal Free Hospital London UK 4 th Workshop on HCV Therapy Advances Paris 12-13 December 2014
Transcript of Differential benefits of DAAs in patients with...

Differential benefits of DAAs in patients with co-morbidities
Marc Bourliere , MD G. Dusheiko, MD Hôpital Saint Joseph UCL Institute for Liver and Health Marseille, France Royal Free Hospital London UK
4th Workshop on HCV Therapy Advances Paris 12-13 December 2014

Disclosures MB and GD
– Board member for : Schering-Plough, Merck, Janssen, Gilead, Boehringer Ingelheim, BMS, Novartis, Roche, Abbott, GSK, Vertex, Idenix
– Speaker for : Roche, Schering-Plough, Merck, Janssen, Gilead, BMS, Abbvie

Populations
• End Stage renal disease patients • Patients with Bleeding disorders • Patients with psychiatric disorders

DAAs Combinations approved by EMA in2014
Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec Jan–Jun Jul–Dec
Telaprevir (G1)
Boceprevir (G1)
Sofosbuvir (G1,3,4,5,6)
Sofosbuvir +
RBV
G2,3, 4
Daclatasvir (G4)
2011 2012 2013 2014
IFN
-free
W
ith IF
N
Simeprevir (G1, 4)
Simeprevir
Sofosbuvir +
G1,4
Sofosbuvir
Daclatasvir +
G1,3,4
Sofosbuvir+ Ledipasvir
FDC* (HARVONI)
RBV
±
G1,3,4

Current access to second-generation DAAs in European region end 2014
*BE and NL: reimbursement approved, will be implemented in Jan 2015 BE: SMV/PR, SOF/PR, SMV-SOF; NL: SMV/PR, SOF/PR, SMV-SOF, DCV IT: SOF and SMV price agreed, pending official publication
SMV/PR
SMV/PR SOF/PR
SMV/PR SOF/PR
SMV-SOF
SOF/LDV SOF+DCV
Special access, pre-NICE
SOF-SMV SOF-DCV SOF-LDV
SOF/PR
SMV, DCV, SOF
SOF-SMV SOF-DCV
* *
*

Populations
• End Stage renal disease patients • Patients with Bleeding disorders • Patients with psychiatric disorders

Patient CA Male aged 62 • Chronic hepatitis C genotype 1b
– Cirrhosis – Past non responder interferon and RBV
• Hepatocellular carcinoma 2010 – October 2010 radiofrequency ablation – Transplant initially excluded alcohol history
• Marked ascites April 2011 – spironolactone

Patient CA
• Past mycetoma: TB
• 2010: – HB 12 WCC 6.4 Platelets 98 – Albumin 25 ALT 185 AST 233 Bilirubin 16 – Creatinine 93 umol/L eGFR 76 ml/min

Course
• April 2011 – Creatinine 114 eGFR 60
• October 2013 – Creatinine 161 eGFR 39 – Urine protein creatinine ratio 1,279 mg/ml
• Cryoglobulins detected • April 2014 HCV RNA 31,562 IU/ml
• Renal biopsy February 2014
– Mixed glomerulopathy with diabetic change – Immune complex glomerulopathy – Subendothelial deposits – Sub epithelial intramembranous mesangial deposits – Mesangiocapillary type glomerulopathy – Hepatitis C cryoglobulin induced

Treatment
• Gliclazide 40 mg daily • Propranolol 10 mg bd • Spironolactone 50 mg /day • Furosemide 20 mg /day
• Abstinent from alcohol since 2010
• Antiviral treatment:
– sofosbuvir 400 mg daclatasvir 60 mg ribavirin 600 bd Sept 2014

CA course
• September 2014 – Creatinine 207 – GFR Tc-99m DTPA eGFR 27 ml/min – Calculated Cockroft and Gault 39 ml/mn
• October 2014 HCV RNA not detected. – Continued sofosbuvir 400 mg/day
• November 2014 – Creatinine 255 eGFR 23 – HCV RNA undetectable
• Ribavirin stopped 27 November
• Admitted hyperkalemia • December 2014
– Creatinine 215 eGFR 28

HCV and cryoglobulinaemia • Cirrhosis, membranous glomerulonephritis, mixed essential
cryoglobulinaemia and vasculitis associated chronic hepatitis C. • HCV continuous stimulus for production of circulating immune
complexes which may form cryoprecipiates • Complement:
– cold-insoluble immune complex -mediated vasculitis – involving small blood vessels different tissues including skin, kidney, peripheral, and
central nervous system.
• B-cell clonal selection may arise as a result of antigen stimulation – May lead to malignant B-cell proliferation.
• Optimal treatment relies on reducing HCV RNA as the driver of the process?

Almehmi et al American Journal of kidney diseases 54: 7070 2009

Almehmi et al American Journal of kidney diseases 54: 7070 2009

Frequency of CD19+ B cells lower in HCV-infected patients with mixed essential cryoglobulinaemia
Holtz et al, Hepatology Volume 56 pages 1602-1610, 14 OCT 2012

B cell homeostasis in chronic hepatitis C virus–related mixed cryoglobulinemia is maintained through naïve B cell apoptosis
Holtz et al, Hepatology Volume 56 pages 1602-1610, 14 OCT 2012
B cell numbers paradoxically reduced in HCV-infected patients with MC HCV patients Increased sensitivity of naıve B cells to apoptosis: reduction in size of naıve B cell subset.

Discussion
• Use (and continued use) of sofosbuvir in patients with impaired renal function
• Worsening of renal function in patients with rapid decline in HCV RNA? – ? B cell surge with reduction in HCV RNA? – Rituximab use
• ? Contraindicated past TB

Sofosbuvir
Prodrug
uridine monophosphate
Metabolism GS-461203
uridine – triphosphate 1. Hydrolysis of the carboxyl ester moiety 2. Phosphoramidate cleavage 3. Phosphorylation by pyrimidine nucleotide biosynthesis pathway Dephosphorylation GS331007
80%, 14%, and 2.5% recovered in urine, faeces, and expired air Urine: recovered: GS331007 (78%) 3.5% as sofosbuvir.
uridine triphosphate
Hepatocyte

Sofosbuvir GS331007 Mild eGFR ≥ 50 and < 80
Moderate eGFR ≥ 30 and < 50
Severe (eGFR <
30
ESRD
Plasma half life
0.48-0.75 hrs 7.2 - 11.8 hrs
Cmax ng/ml 603 1378
AUC ng/ml 539 9369
Sofosbuvir AUC
61% 107% 171% 28% pre 60% post
GS331007 55% 88% 451%
Sofosbuvir pharmacokinetics in renal impairment

SOF + RBV in Patients with Severe Renal Impairment
Study Rationale: Prior studies in renally impaired patients without HCV demonstrated higher exposures of SOF and GS-3310071
Phase 2b, efficacy, PK, and safety of SOF + RBV in patients with HCV GT 1 and GT 3 with eGFR < 30 mL/min (Stage 4 CKD)
The cause of renal disease was not defined for participation; medical history of patients included HCV, diabetes, hypertension, and lupus nephritis
SVR12
Week 0 24
SOF 20 0 mg QD + RBV Part 1 Severe renal n=20 SOF 40 0 mg QD + RBV
SOF 20 0 mg QD + RBV
SOF 40 0 mg QD + RBV
0 24 0 24 0 24
SVR12
SVR12
SVR12
Part 2 ESRD
on dialysis
n=20
1. Cornpropst M, et al. EASL 2012, Poster 1101. Gane, AASLD, 2014, Poster #966 ClinicalTrials.gov NCT 01958281

Safety, efficacy and phramokinetics of Sofosbuvir in ESKD
• 10 patients with ESKD (eGFR < 30 ml/mn) and HCV (GT-1, 7GT-1a, 2 GT-1b and7 GT-3) without cirrhosis. 7/10 were naive ,were treated with SOF 200 mg/j and RBV 200 mg/j.
• Efficacy : – HCV RNA undetectable at w2, W4.
– SVR 12 = SVR 24 = 40 % – No relation between AUC and SVR 12
• Safety : – 20 % AE (anemia) – 4 dose reduction and 1 RBV stopped – No SOF discontinuation
➜ Despite favorable pharmacokinetics and good tolerance, efficacy is poor due to partly difficulty of managing ribavirin ?
Gane EJ et al. AASLD 2014: abstr. 966
Pharmacokinetics of sofosbuvir and his metabolite : GS-331007
SOF GS-331007
AUC appears to be equivalent for sofosbuvir and X4 for GS-331007 compared to patients with normal eGFR but without clinical impact so far.

Gane, AASLD, 2014, Poster #966

Sofosbuvir in renal impairment • Case series: • 4 male genotype 1
– 2 on dialysis – 1 Liver transplant fibrosing cholestatic hepatitis – 1 post renal transplant
• Dose: 400 mg alternate days + simeprevir 150 mg or RBV
• Three/four SVR • Treatment appeared “safe and feasible”
Bhamidimarri et al AASLD 2014

Sofosbuvir and ribavirin: Early efficacy and safety in renal transplant patients
• HCV RNA undetectable in all patient at week 8 – follow-up after the end of treatment in 3 patients – All achieve end of treatment response with no relapse so far
17 renal transplant patients with eGFR > 30 ml/mn treated by sofosbuvir 400 mg/j plus ribavirin 200 et 800 mg/j for24 weeks
➜ SOF-RBV is potent on-treatment in renal transplant patient , however calcineurin inhibitors dosage should be adapted in half of the patient and anemia is frequent requring treatment
Huard G et al. AASLD 2014; abstr. 701
Adverse events Number (%)
Anemia requiring treatment 8 (47,1 %)
Calcineurin inhibitors dose modification 8 (47,1 %)
Other serious adverse events – Pruritus – Myalgia
1 (5,9 %) 1 (5,9 %)
Premature discontinuation: anemia (1), pruritus (1), myalgia (1), patient wish (1)
4 (23,5 %) 3/4 relapses
Viral kinetics

ABT-450/, ombitasvir with or without dasabuvir in subject with renal impairment
• Phase I multicenter, single dose non fasting open label, 2 period study of 3D and 2D in patients with renal impairement compzred to subject with normal renal function.
• 24 subjects without HCV were compared according to renal function in 4 groups according to creatinine clearance: ≥ 90 ml/mn, between 60 – 89ml /mm, between 30-59 ml/mm and between 15-29 ml/mm.
➜ None of the changes in drug exposures were clinically relevant and they do not require dose adjustment. ➜ Clinical studies in HCV infected patients with renal insufficiency are planned in light of these
pharmacokinetic results
Compared with subjects with normal Renal function
Mild renal Impairment
Moderate renal impairment
Severe renal impairment
AUC ombitasvir comparable comparable comparable
AUC ABT-450 et dasabuvir 20 % 37 % 50 %
AUC ritonavir 42 % 80 % 114 %
– None of the changes in drug exposures were clinically relevant – Change in DAA exposure are not clinically relevant for safety
Khatri A et al.AASLD 2014: abstr. 238,

Daclatasvir: dose adjustment not required in subjects with renal impairment
CI = confidence interval; CrCL = creatinine clearance; AE = adverse events. Garimella T, et al. HCV/HIV Clinical Pharmacology Workshop. Poster 2014 P_43
• Compared with a normal creatinine clearance (CrCL; 90 mL/min), AUCinf estimated to increase 1.3-, 1.6- and 1.8-fold for subjects with CrCL values of 60, 30 and 15 mL/min, respectively
– Similar estimated increases in the AUCinf of unbound free DCV were also observed – Increased DCV exposure was within the exposures observed in the population PK and exposure-safety assessment, which has not shown a correlation between higher exposures
and adverse events (AEs) • DCV was generally well-tolerated in subjects with normal renal function or renal impairment of varying degree • DCV can be administered in subjects with renal impairment without dose modification
1.000
10.000
100.000
0 40 80 120 160
Individual AUCinf Fitted regression line 90% CIs
DC
V AU
Cin
f ng●
h/m
L
Creatinine clearance (mL/min)
100
1.000
10.000
0 40 80 120 160
DC
V C
max
ng/
mL
Creatinine clearance (mL/min)
Fitted regression line
Individual Cmax
90% CIs

Simeprevir: dose adjustment not required in subjects with renal impairment
• For subjects with severe renal impairment, simeprevir Cmin, Cmax, and AUC24h were about 71%, 34% and 62% higher, respectively, compared with matched healthy subjects
• No relevant differences in tmax were observed between the groups
Parameter
LS meansa
LS means ratio 90% CI Renal impaired
(test)
Healthy controls
(reference)
Cmin, ng/mL 985.5 577.5 1.71 0.65, 4.50
Cmax, ng/mL 3459 2588 1.34 0.66, 2.72
AUC24h, ng.h/mL 51710 32010 1.62 0.73, 3.59
Mediana Treatment difference median 90% CI
tmax, h 6.0 6.0 0.0 0.0, 2.0
AUC24h, area under the plasma-time curve; CI, confidence interval; Cmax, maximum plasma concentration; Cmin, minimum plasma concentration; tmax, time to reach Cmax aN: 8 for reference (healthy controls) and N: 8 for test (renal impaired)
For subjects with severe renal impairment, SMV Cmin, Cmax and AUC24h were about 71%, 34% and 62% higher, respectively, compared with matched healthy controls – For tmax, no relevant differences were observed between the groups

Populations
• End Stage renal disease patients • Patients with Bleeding disorders • Patients with psychiatric disorders

Safety and Efficacy of LDV/SOF + RBV in HCV GT 1 Patients with Bleeding Disorders
AEs were generally mild
Grade 3/4 laboratory abnormalities were infrequent and consistent with RBV safety profile
No safety concerns were associated with underlying bleeding disorders
14 GT 1 treatment-naïve and -experienced patients with hereditary bleeding disorders received LDV/SOF + RBV for 12 weeks 1 patient (7%) was cirrhotic
Primary Endpoint
100% of patients achieved SVR12 and demonstrated a similar safety profile to the general HCV patient population
Stedman CA, et al. APASL 2014. Poster #734; Data on file – Gilead Sciences EAME – (HCV1300047)
14/14

Populations
• End Stage renal disease patients • Patients with Bleeding disorders • Patients with psychiatric disorders

Simeprevir+ Sofosbuvir for GT-1 patients in special population: INSPIRE-C study
• Psychiatric population ( major depression, suicidal ideation ,bipolar , schizophrenia and psychosis)
• 60 patients ( schizophrenia 33%, major depression 25%, bipolar (33%), suicide attempt 8.3%)
• All patient except 2 complete treatment
Basu P et al AASLD 2014
SIM+SOF+RBV
SOF+RBV
SIM+SOF+ VITD
Duration of therapy 12 24 12
Mean age 53 58 58
Schizophrenia Major depression Bipolar Suicide attempt
8 8` 5 2
7 8 4 1
8 9 4 2
Prior IVDU on Methadone
15 12
13 8
15 8
GT-1a GT-1b
0 20
20 0
3 17
F0-F2 F3-F4
14 6
2 18
15 5

Populations
• End Stage renal disease patients • Patients with Bleeding disorders • Patients with psychiatric disorders • Gt-1 cirrhotic PI-failure patients

GT-1 PI-Failure what are the current options
• SOF+ PR 12 weeks • SOF + DCV 24 weeks • SOF + SIM ± RBV 12 weeks • SOF/LDV ± RBV 12 weeks

GT-1 PI-Failure what are the current options
• SOF+ PR 12 weeks • SOF + DCV 24 weeks • SOF + SIM ± RBV 12 weeks • SOF/LDV ± RBV 12 weeks

Sofosbuvir in «real life »
• Treatment regimen were done according to guidelines
➜ Demographics, clinical virological and safety data were collected
AASLD 2014 – Jensen DM et al., abstr. 45 ; Dieterich D et al., abstr. 46,
Cohort (Nb patients treated)
SOF/Peg/RBV SOF/RBV SOF/SMV SOF/SMV/RBV
Target (2 063) 384 667 784 228
Trio (995) 384 227 320
Trio cohort 1 211 patients included in 231 centers in USA
Target cohort 2 330 patients included
In 53 centers in USA , Canada and Germany
Treatment regimen

Sofosbuvir in «real life »
TARGET (n = 2 063)
TRIO (n = 995)
Age mean (range) 57,6 (20-83) 57 (17-86)
Male 1 300 (63,7 %) 565 (59 %)
Teatment failure 1 077 (52,2 %) 407 (43 %)
– PI failure (TVR/BOC) 193 (17,9 %) 82 (20 %)
Cirrhosis 999 (48,4 %) 291 (30 %)
– prior decompensation 375 (43,1 %) -
Liver transplantation 227 (11 %) -
HCC 211 (10,2 %) -
HIV 47 (2,3 %) -
Genotypes 1a-1b - 1 - 462 (48 %) – 179 (19 %) – 62 (6 %)
Genotype 2 - 212 (22 %)
Genotype 3 - 7 (1 %)
36
Baseline characteristics
AASLD 2014 – Jensen DM et al., abstr. 45 ; Dieterich D et al., abstr. 46,

TRIO : Real life data from USA : Sofosbuvir + PEG/RBV
SVR 12 in treatment –experienced GT-1 patients
ITT Per protocol
Failure to PEG IFN/RBV + Protease inhibitors
0
20
40
60
80
100
40 n =
%
73 %
36 37 33
67 % 78 % 73 %
SOF + PEG/RBV SOF + PEG/RBV
Failure to PEG IFN/RBV
Dieterich D et al. AASLD 2014, Abs. 46

GT-1 PI-Failure what are the current options
• SOF+ PR 12 weeks • SOF + DCV 24 weeks • SOF + SIM ± RBV 12 weeks • SOF/LDV ± RBV 12 weeks

SOF + DCV ± RBV in PI failures : AI444-040 – study design
Randomised, open-label, parallel group Phase 2 study investigating the safety and efficacy of SOF + DCV ± RBV
SOF: 400 mg QD; DCV: 60 mg QD RBV: 1000–1200 mg/day Sulkowski MS, et al. N Engl J Med 2014;370:211–21
SOF + DCV
0 24 SVR12
n=21
SOF + DCV + RBV n=20
Treatment-experienced (TVR + PR or BOC + PR),
non-cirrhotic HCV genotype 1 patients Week
Primary endpoint: SVR12

SOF + DCV ± RBV: efficacy in PI -failures
*METAVIR score derived from fibrotest (classified according to manufacturers website) Patients with F4 were required to have no evidence of cirrhosis based upon a biopsy Sulkowski MS, et al. N Engl J Med 2014;370:211–21
SOF + DCV
24 weeks
19/20
Without RBV
With RBV
SVR
12 (%
)
21/21
No cirrhotics included*

GT-1 PI-Failure what are the current options
• SOF+ PR 12 weeks • SOF + DCV 24 weeks • SOF + SIM ± RBV 12 weeks • SOF/LDV ± RBV 12 weeks

Sofosbuvir in «real life »
• Treatment regimen were done according to guidelines
➜ Demographics, clinical virological and safety data were collected
AASLD 2014 – Jensen DM et al., abstr. 45 ; Dieterich D et al., abstr. 46,
Cohort (Nb patients treated)
SOF/Peg/RBV SOF/RBV SOF/SMV SOF/SMV/RBV
Target (2 063) 384 667 784 228
Trio (995) 384 227 320
Trio cohort 1 211 patients included in 231 centers in USA
Target cohort 2 330 patients included
In 53 centers in USA , Canada and Germany
Treatment regimen

TRIO : Real life data from USA : Sofosbuvir + simeprevir
SVR 12 in treatment –experienced GT-1 patients
ITT Per protocol
Failure to PEG IFN/RBV + Protease inhibitors
0
20
40
60
80
100
n =
%
33 75 31 70
82 % 80 %
87 % 86 %
SMV + SOF + RBV SMV + SOF + RBV
Failure to PEG IFN/RBV
Dieterich D et al. AASLD 2014, Abs. 46

Real Life TARGET cohort
• Genotype 1 : SOF + SIM + RBV 12 weeks : • 72 patients failure to triple regimen with PI
We can do it !!
Jensen DM et al. AASLD 2014, Abs. 45
RVS4 : No cirrhosis : 85 % (17/20) Cirrhosis : 79 % (27/34)
SVR4 : available 54/69
SVR 4= 81 % (44/54)
Breakthrough 0 %
(0/54)
Relapse 19 %
(10/54)
Non response 0 %
(0/54)
Lost of follow up 0 %
(0/303)

GT-1 PI-Failure what are the current options
• SOF+ PR 12 weeks • SOF + DCV 24 weeks • SOF + SIM ± RBV 12 weeks • SOF/LDV ± RBV 12 weeks

No cirrhosis cirrhosis
SVR
12
(%)
50/52 12/14 51/51 11/13 35/36 14/14 38/38 13/13
12 Weeks 24 Weeks
LDV/SOF + RBV LDV/SOF + RBV LDV/SOF LDV/SOF
ION-2 : SOF/LDV in GT-1 treatment failures to PI
Afdhal N, et al. N Engl J Med 2014;370: 1483-93
SVR 12 according to fibrosis stage

Sofosbuvir + Ledipasvir in GT-1 with compensated cirrhosis
SVR : 96 % 20 treatment failure: 18 relapse, 1 death, 1 lost of follow up
Bourlière M et al. AASLD 2014, Abs. 82
w 0 w 12 w 36 w 24
SVR 12 LDV/SOF
SVR 12 LDV/SOF
+ RBV
SVR 12 LDV/SOF + RBV
SVR 12 LDV/SOF
118
204
133
58
SVR
12 (%
)
Overall 12 weeks 24 weeks
493/513
SVR 12
n

Sofosbuvir + Ledipasvir in GT-1 with compensated cirrhosis
Bourlière M et al. AASLD 2014, Abs. 82
Réponse Virologique Soutenue
Overall Treatment naive
Treatment failure
Overall SVR 12
Duration 12 weeks
24 weeks
Regimen LDV/SOF
LDV/SOF + RBV
Duration ± RBV
LDV/SOF 12 weeks
LDV/SOF + RBV 12 weeks
LDV/SOF 24 weeks
LDV/SOF + RBV 24 weeks
RVS12, %
96 % 98 % 95 %
95 % 97 % 94 %
98 % 99 % 98 %
95 % 96 % 95 %
97 % 99 % 96 %
92 % 96 % 90 %
96 % 98 % 96 %
98 % 97 % 98 %
100 % 100 % 100 %

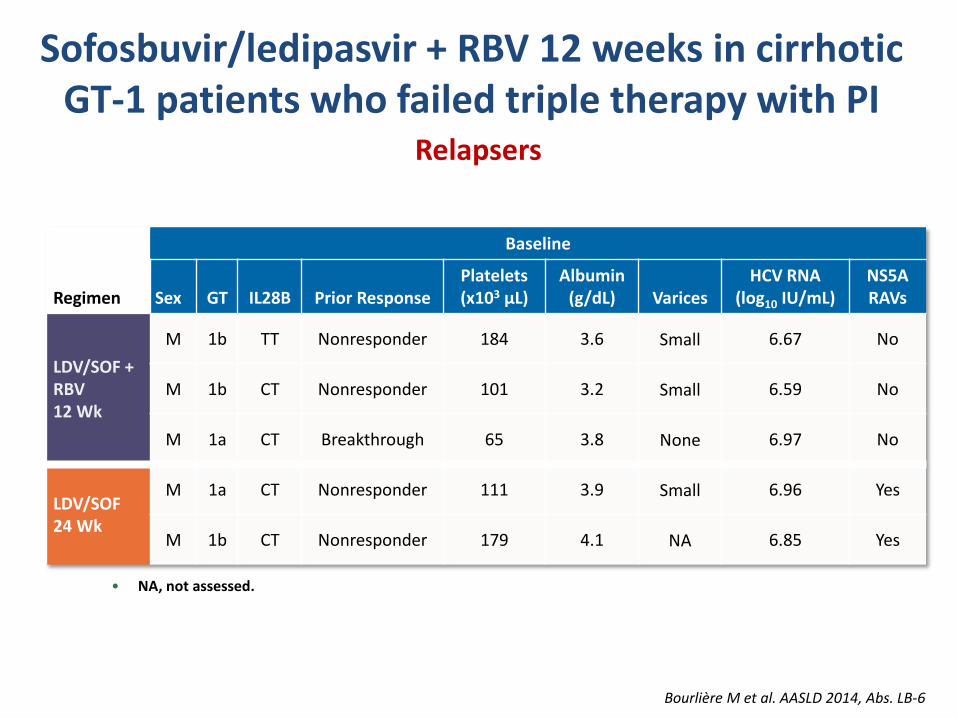
Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy
with PI
• Phase 2 multicenter randomized controlled double blind study • 155 cirrhotic GT-1 patient who failed triple therapy with PI
Sofosbuvir/Ledipasvir + RBV for 12 weeks is the optimal combination in cirrhotic GT-1 patients who failed prior regimen with PR and subsequently failed to triple regimen with PI.
Bourlière M et al. AASLD 2014, Abs. LB-6
12 weeks 36 weeks 24 weeks D0
LDV/SOF + Placebo SVR 12
LDV/SOF + RBV Placebo SVR 12
n = 77
n = 78

Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy
with PI
Placebo 12 weeks → LDV/SOF + RBV
12 weeks (n = 77)
LDV/SOF + Placebo
24 weeks (n = 78)
Overall (n = 155)
Age mean, years (range) 56 (39–74) 57 (23–77) 56 (23–77)
Male, n (%) 58 (75) 56 (72) 114 (74)
Mean BMI, kg/m2 (range) 27,9 (19,6–47,1) 26,3 (19,1–39,8) 27,1 (19,1–47,1)
MELD mean (range) 7 (6-16) 7 (6-12) 7 (6-16)
Esophageal varices, n (%) 16 (21) 25 (32) 41 (26)
Platelets mean (range) 153 (54–316) 141 (59–278) 147 (54–316)
Platelets < 100 x 103/µl 14 (18) 13 (17) 27 (17)
Albumin g/dl mean (range) 3,9 (3,2–4,6) 3,9 (3,0–4,9) 3,9 (3,0–4,9)
Albumin < 35 g/l, n (%) 6 (8) 14 (17) 20 (13)
Bilirubin mg/dl mean (range) 0,8 (0,3–2,5) 0,8 (0,3–1,8) 0,8 (0,3–2,5)
Bourlière M et al. AASLD 2014, Abs. LB-6
Patients characteristics

Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy with PI
Placebo 12 weeks → LDV/SOF + RBV
12 weeks (n = 77)
LDV/SOF + Placebo
24 weeks (n = 78)
Overall (n = 155)
GT, n (%)
1a 48 (62) 50 (64) 98 (63)
1b 28 (36) 27 (35) 55 (36)
HCV RNA mean log10 UI/mL (range) 6,5 (5,3–7,7) 6,5 (3,9–7,5) 6,5 (3,9–7,7)
Prior PI regimen, n (%)
Telaprevir 43 (56) 49 (63) 92 (59)
Boceprevir 30 (39) 27 (35) 57 (37)
Otherrs 4 (5) 2 (3) 6 (4)
NS3/4A RAVS 58 (75) 55 (71) 113 (73)
CUPIC* participation , n (%) 25 (32) 22 (28) 47 (30)
Bourlière M et al.AASLD 2014, Abs. LB-6
Patients characteristics

Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy with PI
75/77 74/77
LDV/SOF 24 weeks
LDV/SOF+RBV 12 weeks
3 relapses 2 relapses
Bourlière M et al. AASLD 2014, Abs. LB-6
Sustained Virological Response
Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy with PI
Bourlière M et al. AASLD 2014, Abs. LB-6
Relapsers
Baseline
Regimen Sex
GT IL28B Prior Response Platelets (x103 μL)
Albumin (g/dL) Varices
HCV RNA (log10 IU/mL)
NS5A RAVs
LDV/SOF + RBV 12 Wk
M 1b TT Nonresponder 184 3.6 Small 6.67 No
M 1b CT Nonresponder 101 3.2 Small 6.59 No
M 1a CT Breakthrough 65 3.8 None 6.97 No
LDV/SOF 24 Wk
M 1a CT Nonresponder 111 3.9 Small 6.96 Yes
M 1b CT Nonresponder 179 4.1 NA 6.85 Yes
• NA, not assessed.

Results: HCV Sequence Analysis
92% SVR 98% SVR
n=127/130
No NS5A RAVs at Baseline With NS5A RAVs at Baseline
• There was no difference in SVR12 rates among patients with or without NS3/4A RAVs at Baseline (96% and 97% respectively)
Bourlière M et al. AASLD 2014, Abs. LB-6

Sofosbuvir/ledipasvir + RBV 12 weeks in cirrhotic GT-1 patients who failed triple therapy with PI
Safety
Bourlière M et al. AASLD 2014, Abs. LB-6
Patients, n (%)
Placebo 12 Weeks → LDV/SOF + RBV 12 Wk
LDV/SOF 24 Wk
Placebo 12 Wk n=77
LDV/SOF+RBV 12 Wk
n=76
Overall Period n=77
First 12 Wk n=78
Overall Period n=78
Overall Safety
AEs 63 (82) 66 (87) 74 (96) 66 (85) 68 (87)
Grade 3-4 AEs 1 (1) 5 (7) 6 (8) 2 (3) 10 (13)
SAEs 1 (1) 3 (4) 4 (5) 3 (4) 8 (10)
Treatment Related SAEs 0 1 (1) 1 (1) 0 0
Treatment D/C due to AEs 1 (1) 0 1 (1) 0 0
Death 0 0 0 0 0
Grade 3-4 lab abnormalities 18 (23) 8 (11) 24 (31) 15 (19) 11 (14)
Hb <10 g/dL 1 (1) 1 (1) 2 (3) 0 1 (1)
Hb <8.5 g/dL 1 (1) 1 (1) 2 (3) 0 0

GT-1 PI-Failure what are the current options
• (1) SOF/LDV ± RBV 12 weeks • (2) SOF + DCV 24 weeks • (3) SOF + SIM ± RBV 12 weeks • (4) SOF+ PR 12 weeks


















