
Didactic: Hysteroscopy from A-Z - · PDF fileDidactic: Hysteroscopy from A-Z PROGRAM CHAIR...
65
Sponsored by AAGL Advancing Minimally Invasive Gynecology Worldwide Didactic: Hysteroscopy from A-Z PROGRAM CHAIR Sony S. Singh, MD PROGRAM CHAIR Isabel C. Green, MD Linda D. Bradley, MD Neeraj Mehra, MD Scott G. Chudnoff, MD, MS James M. Shwayder, MD, JD Amy L. Garcia, MD GLOBAL CONGRESS ON MINIMALLY INVASIVE GYNECOLOGY NOV. 17-21, 2014 | Vancouver, British Columbia 43rd AAGL
Transcript of Didactic: Hysteroscopy from A-Z - · PDF fileDidactic: Hysteroscopy from A-Z PROGRAM CHAIR...

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Didactic: Hysteroscopy from A-Z
PROGRAM CHAIR
Sony S. Singh, MD
PROGRAM CHAIR
Isabel C. Green, MD
Linda D. Bradley, MDNeeraj Mehra, MD
Scott G. Chudnoff, MD, MSJames M. Shwayder, MD, JD
Amy L. Garcia, MD
GLOBAL CONGRESSON MINIMALLY INVASIVE GYNECOLOGYNOV. 17-21, 2014 | Vancouver, British Columbia
43rd AAGL

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 2 OR or Office: Set Up for Success L.D. Bradley ................................................................................................................................................... 4 Visualization Tips and Tricks for Hysteroscopy N. Mehra ..................................................................................................................................................... 14 Managing Pain and Anxiety for Office or Outpatient Procedures S.G. Chudnoff .............................................................................................................................................. 18 Working With the Awake Patient – Tips and Tricks for Diagnostic and Operative Hysteroscopy S.S. Singh ..................................................................................................................................................... 26 An Alternative to Hysteroscopy – Transvaginal Ultrasound in the Evaluation of Abnormal Bleeding J.M. Shwayder ............................................................................................................................................. 34 Beyond Diagnostics – Office Sterilization, Ablation and Resection A.L. Garcia ................................................................................................................................................... 53 Prepare for the Worst Case Scenario before It Happens – Complications in Office Procedures I.C. Green .................................................................................................................................................... 57 Cultural and Linguistics Competency ......................................................................................................... 62

HSC-‐706 Didactic: Hysteroscopy from A-‐Z
Sony S. Singh, Chair
Isabel C. Green, Co-‐Chair
Faculty: Linda D. Bradley, Scott G. Chudnoff, Amy L. Garcia, Neeraj Mehra, James M. Shwayder This workshop has something for everyone practicing hysteroscopy. It is designed for the doctor ready to push the envelope in outpatient or office procedures, for those considering making the switch, or for those eager to refine their hysteroscopy and sonogram skills. After receiving instruction from expert faculty, the participant should leave the workshop prepared to start an office practice, armed with the tools to improve the quality, safety, and efficiency of hysteroscopy and ultrasound procedures. Learning Objectives: At the conclusion of this course, the clinician will be able to: 1) Identify the appropriate patients and equipment for office hysteroscopic procedures; 2) describe and execute techniques of office hysteroscopy, including diagnostics, polypectomy and excision of synechiae; 3) describe the benefits of and approach to office sonogram in the evaluation of abnormal uterine bleeding; 4) recognize and manage rare procedural emergencies of office hysteroscopic procedures; and 5) describe the various options for pain control for patients undergoing hysteroscopy without general anesthesia.
Course Outline 7:00 Welcome, Introductions and Course Overview S.S. Singh
7:05 OR or Office: Set Up for Success L.D. Bradley
7:30 Visualization Tips and Tricks for Hysteroscopy N. Mehra
8:00 Managing Pain and Anxiety for Office or Outpatient Procedures S.G. Chudnoff
8:30 Working With the Awake Patient – Tips and Tricks for Diagnostic and Operative Hysteroscopy S.S. Singh
9:00 Questions & Answers All Faculty
9:15 Break
9:30 An Alternative to Hysteroscopy – Transvaginal Ultrasound in the Evaluation of Abnormal Bleeding J.M. Shwayder
10:00 Beyond Diagnostics – Office Sterilization, Ablation and Resection A.L. Garcia
10:30 Prepare for the Worst Case Scenario before It Happens – Complications in Office Procedures I.C. Green
10:50 Questions & Answers All Faculty
11:00 Adjourn
Page 1

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor* Kimberly A. Kho* Frank D. Loffer, Medical Director, AAGL* Linda Michels, Executive Director, AAGL* M. Jonathon Solnik* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: Blue Endo, Intuitive Surgical, SurgiQuest Other: Royalties: CooperSurgical William M. Burke* Rosanne M. Kho* Ted T.M. Lee Consultant: Ethicon Endo-‐Surgery Javier F. Magrina* Ceana H. Nezhat Consultant: Karl Storz Other: Medical Advisor: Plasma Surgical Other: Scientific Advisory Board: SurgiQuest Kevin J.E. Stepp Consultant: CONMED Corporation, Teleflex Other: Stock Ownership: Titan Medical Robert K. Zurawin Consultant: Bayer Healthcare Corp., CONMED Corporation, Ethicon Endo-‐Surgery, Hologic, Intuitive Surgical FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Linda D. Bradley Consultant: Bayer Healthcare Corp., Boston Scientific Corp. Inc., Endoceutics, Hologic, Smith & Nephew Endoscopy Grants/Research: Bayer Healthcare Corp. Speakers Bureau: Bayer Healthcare Corp., Smith & Nephew Endoscopy Scott G. Chudnoff* Amy L. Garcia Consultant: Bayer Healthcare Corp., Boston Scientific Corp. Inc., Ethicon Women’s Health & Urology, Gynesonics, IOGYN, Karl Storz, Minerva Surgical Speakers Bureau: Ethicon Endo-‐Surgery Grants/Research: Hologic Isabel C. Green* Neeraj Mehra Consultant: Actavis Pharmaceutical, Bayer Healthcare Corp., Ethicon Endo-‐Surgery James M. Shwayder Page 2

Other: Royalties: Cook Women’s Health Sony S. Singh Grants/Research: Abbott Laboratories, Bayer Healthcare Corp. Speakers Bureau: Actavis, Abbott Laboratories, Bayer Healthcare Corp. Asterisk (*) denotes no financial relationships to disclose.
Page 3

OR or Office: Set Up for Success for Hysteroscopy
Linda D. Bradley MDProfessor of SurgeryVice Chair Obstetrics & GynecologyDirector, Center for Menstrual Disorders, Fibroids, and Hysteroscopic ServicesCleveland Clinic
Disclosures
Consultant: Bayer Healthcare Corp., Boston Scientific Corp. Inc., Endoceutics, Hologic, Smith & Nephew Endoscopy
Grants/Research: Bayer Healthcare Corp.
Speakers Bureau: Bayer Healthcare Corp.,Smith &Nephew Endoscopy
At the end of this lecture you will be able to:
• Identify the necessary equipment needed for office hysteroscopy
• Be knowledgeable about operative hysteroscopy equipment needed to perform ambulatory procedures
• List items on the safety check list that should not be forgotten
Objectives
Avoiding Patient Complaints in Office Hysteroscopy
• Experienced Knowledgeable Physician
• Explain Procedure
• Maintain Dialogue
• Avoid Grasping Cervix
• Consider Paracervical Block
• Little or No Dilation
• Video Control
• Insert Scope Under Direct Vision
• Avoid Overdistention
• Short Procedures (<5 Minutes)
Everyone Needs Education
• Physician– Manual of operations
– Periodic safety drills
• Staff– Periodic in-service training
– Physician training
– Vendor training
• Patient– Brochures
– Videotape
– Answer all questions pre and post procedure
Office: Time Out
• Identify patient
• Pregnancy test results
• Visualize cervix to exclude cervicitis
• Palpate cervix to exclude pelvic inflammatory disease
• Allergies– Soap
– Anesthesia
• Right procedure– IUD removal
– Hysteroscopic sterilization
– Diagnostic
– Brief operative procedure
Page 4

Don’t Play Peek a Boo Medicine
• Informed Consent
• See and examine the patient before the hysteroscopy
• Order appropriate laboratory testing as part of work up
• Promptly return phone calls and exam the if patient has questions
Predisposing Factors Predisposing Factors
Hysteroscopic ComplicationsHysteroscopic Complications
• Contraindications ignored
• Improper surgical technique
• Improper use of equipment
• Incorrectly chosen patient
• Contraindications ignored
• Improper surgical technique
• Improper use of equipment
• Incorrectly chosen patient
Setup
Diagnostic Office HysteroscopyDiagnostic Office Hysteroscopy
• Sterile drapes, gauze, and gloves
• Syringe, needles, and needle extender
• Povidone-iodine solution
• Local anesthetic
• Hysteroflator and insufflation tubing
• Needle holder, forceps, and suture
• Open sided speculum
• Tenaculum, polyp & ring forceps
• Sound, graduated dilator
• Emergency kit for vasovagal reaction
• Saline and IV tubing
• Buttock draping
• Sterile drapes, gauze, and gloves
• Syringe, needles, and needle extender
• Povidone-iodine solution
• Local anesthetic
• Hysteroflator and insufflation tubing
• Needle holder, forceps, and suture
• Open sided speculum
• Tenaculum, polyp & ring forceps
• Sound, graduated dilator
• Emergency kit for vasovagal reaction
• Saline and IV tubing
• Buttock draping
Procedural Cascade With Fluid
Diagnostic HysteroscopyDiagnostic Hysteroscopy
• Bimanual exam for position of cervix and fundus
• Light source “on”
• Normal saline or LR connected to inflow port
• Inflow is purged with liquid distention medium
• Cervix on traction with tenaculum if needed
• Endocervix engaged with hysteroscope
• Keep, “black hole” kept in center of field
• Uterine cavity entered and strategically assessed
• Endocervical canal explored on withdrawal from cavity
• Hysteroscope and tenaculum removed
• Cervix and tenaculum sites assessed for bleeding
• Bimanual exam for position of cervix and fundus
• Light source “on”
• Normal saline or LR connected to inflow port
• Inflow is purged with liquid distention medium
• Cervix on traction with tenaculum if needed
• Endocervix engaged with hysteroscope
• Keep, “black hole” kept in center of field
• Uterine cavity entered and strategically assessed
• Endocervical canal explored on withdrawal from cavity
• Hysteroscope and tenaculum removed
• Cervix and tenaculum sites assessed for bleeding
• Bimanual exam for position of cervix and fundus
• Light source “on”
• Hysteroflator set to 100 mm Hg and 40-60 cc/min
• Cervix on traction with tenaculum
• Endocervix engaged with hysteroscope
• For 30o scope, “black hole” kept at 6 o’clock
• Uterine cavity entered and strategically assessed
• Flow increased up to 100 cc/min for better distention
• Endocervical canal explored on withdrawal from cavity
• Hysteroscope and tenaculum removed
• Cervix and tenaculum sites assessed for bleeding
• Bimanual exam for position of cervix and fundus
• Light source “on”
• Hysteroflator set to 100 mm Hg and 40-60 cc/min
• Cervix on traction with tenaculum
• Endocervix engaged with hysteroscope
• For 30o scope, “black hole” kept at 6 o’clock
• Uterine cavity entered and strategically assessed
• Flow increased up to 100 cc/min for better distention
• Endocervical canal explored on withdrawal from cavity
• Hysteroscope and tenaculum removed
• Cervix and tenaculum sites assessed for bleeding
Procedural Cascade Using Carbon DioxideProcedural Cascade Using Carbon Dioxide
Diagnostic HysteroscopyDiagnostic Hysteroscopy
• Benefits– Refractory index of 1.0
– Cleared by breathing
– Very soluble in blood, low embolic potential
– Not combustible
– Simplicity in cleaning instruments
• Disadvantages
– Need for hysteroflator
– Easy escape from cervix
– Blood and mucus obscure the view
– Shoulder and thoracic discomfort
Carbon Dioxide as Distention MediumCarbon Dioxide as Distention Medium
Diagnostic HysteroscopyDiagnostic Hysteroscopy
Page 5

• Maximum flow at 100 cc/min
• Maximum pressure <100 mm Hg
• Maximum flow at 100 cc/min
• Maximum pressure <100 mm Hg
Carbon Dioxide Insufflator(High pressure with low flow rate)
Carbon Dioxide Insufflator(High pressure with low flow rate)
Not a laparoscopic insufflator!Not a laparoscopic insufflator!
Diagnostic HysteroscopyDiagnostic Hysteroscopy
Equipment for Office Hysteroscopy
• Rigid or Flexible Hysteroscope
• Hysteroinsufflator CO2 or
• Fluid– may use 60 cc syringe for instillation
• Printer
• Video Monitor
• Lighting
• Camera
Page 6

Betocchi System
Office HysteroscopyFlexible vs Rigid Telescopes
• Advantages– Available in 3.1mm and 4.9mm– Tapered Insertion Section
–Facilitates Insertion– Flexible Tip
– Increased Patient Comfort– Gas or Low Viscosity Liquids– Tenaculum/Cervical Dilation Rarely Necessary with 3.1mm Scope– Potential For:
–Reasonable Biopsy–5 French with 4.9mm Scope
–Increased Patient Comfort
Managing Distention Media
Distention Media
Purpose
Distention Media
Purpose
• Create cavity by overcoming myometrial resistance
• Create sufficient pressure to prevent bleeding
• Create cavity by overcoming myometrial resistance
• Create sufficient pressure to prevent bleeding
What Else Do I Want to Know On the Day of Hysteroscopic Surgery?
• Last menstrual period
• Herpes prodrome?
• Did she remember to take Cytotec?
• Does she plan on having children?
• Surgical Time Out?– Right patient?– Right procedure?– Instruments needed
all present?– Informed consent
and complications reviewed with patient
• Anesthesiologist
Operative Hysteroscopy:Technical Considerations
• Operate during early proliferative phase or with endometrial thinning
• Attempt resection of Type 0 and 1 fibroids only
• Always advance the electrode towards yourself
• Visualize all landmarks throughout the case
• Restrict resection to endometrial surfaces– if deep intramural lesion noted--be patient!! Often once the
pseudocapsule is breached, the uterus will contract and expel the myoma into the field
– intermittently decrease intra uterine pressure to prevent “disappearing phenomenon”
• Beware of progressive myometrial eversion
• End resection at capsular level
• Uterine decompression ---and wait--reinspect
General Principles of Operative Hysteroscopic Myomectomy
• Deflate the endometrium as you resect
• Uterine massage
• Reinspect endometrial cavity 2-3 minutes after removing hysteroscope
• Endometrial suppression not needed, try to schedule post-menses or early proliferative phase
• Sharp curettage can be performed if copious endometrial debris, blood, or copious endometrium
• Consider post op office hysteroscopy in patients desiring fertility within 7-10 days– Consider estrogen therapy to aid in re-epithealization of
endometrium in patients desiring fertility– Or placement of a 30 mL intrauterine foley catheter
Page 7
Intrauterine Surgical TechniquesIntrauterine Surgical Techniques
• Resectoscopic Myomectomy– consider oral, vaginal misoprostol or laminaria in
nulliparous, multiple C/S, menopausal, or those with prior cone biopsies, since cervix must be dilated to 22F-31 F with hysteroscope
– use concomitant laparoscopy if concerned about perforation
– use of dilute solution of pitressin intracervically (to decrease absorption of fluid and facilitate cervical dilation) 20u/100ml saline
Intrauterine Surgical Techniques
• Know your landmarks
• Movement– Move wrists– Move your hysteroscope
• Vary the intrauterine pressure
• Open and close outflow valve when needed
• Remove clots and debris when poor visualization occurs
Operative Hysteroscopy: Toolkit
• Ovum forceps
• Polyp forceps
• Ring forceps
• Myoma (Corson) graspers
• Suction curette
• Sharp curette
• Cutting loop
Intra-operative safety precautions
• Flat– Do not use Trendlenberg
• Position legs in Allen stirrup’s or Candy cane
• Collect fluids with drapes/pouches
Fluid Pumps: Use Them!!!Fluid balance is an important issue during hysteroscopy!
But it's really difficult to track!
…especially the amount on the floor.
Page 8

Tracking Glycine Irrigation Fluid Intraoperatively
• When asked to estimate amount of fluid on the floor, experienced OR nurses had a difficult time, commenting: ”we are totally unable to estimate the amount of fluid on the floor” .
Estimate of Fluid on Floor (cc)
0
200
400
600
800
1000
1200
Trial Number
Actual
Nurse 1
Nurse 2
Nurse 3
Nurse 4
Puddle Vac AKA“Sucky Ducky”
33
Size of Intracavitary Lesion Determines Surgical Time
22.45
14.14
8.18
4.19
1.770.520.07
33.51
0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
80.00
0 1 2 3 4
Diameter (cm)
Sur
gery
tim
e (m
in)
Surgery Time vs. Size*
• As diameter of myoma increases, volume increases cubically (v= 4/3r3 ), increasing operating time
• Surgeons should be aware of this dynamic and plan accordingly for overall procedure time
* Emanuel, MH. (2005). Presentation to Smith & Nephew
Remember Volume
• 4/dr3
• 1 cm =1/2 cubic cm tissue
• 2 cm = 4 cubic cm tissue
• 3 cm = 14 cubic cm tissue
• 4 cm = 33 cubic cm tissue
As you increase the size of the lesion for operative hysteroscopy, the volume of Resected tissue dramatically increases.
This affects length of surgery, amount of fluid used, and ability to complete the surgery.
Cytotec: Use It
• Misoprostol (cytotec)
– Synthetic methyl analogous of PGE2
– Acts on cellular matrix, dissolving collagen, increases hyaluronic acid, increased cervical water by increasing vascularity permeability
– Interleukin-8 is affected, increasing collagenase and thus cervical softening
– Activates smooth muscle contractions
Ribeiro A. Use of Misoprostol Prior to Hysteroscopy in Postmenopausal Women: A Randomized, Placebo-Controlled Clinical Trial. J Minim InvasiveGynecol.2008;15:67-73.
Use Cytotec: It Works
• Options– Cytotec 200-400 mcg by mouth or intra-vaginally at
bedtime prior to procedure
– If very tight cervix suspected, then begin above regimen 2 days before procedure as well as at bedtime prior to procedure
Ribeiro A. Use of Misoprostol Prior to Hysteroscopy in Postmenopausal Women: A Randomized, Placebo-Controlled Clinical Trial. J Minim InvasiveGynecol.2008;15:67-73
Page 9

Consider Vasopressin
• Preparation: 20 u/100 saline = 0.2 u/cc
• Direct intra-cervical stromal injection of 5 mL at 12, 3, 6 and
9 o’clock
– Alert anesthesiologist
– Aspirate before injection
– Administer 5 cc/side = 4 units
– Assess for cardiovascular response before
second injection
MMeeaassuurreemmeenntt pp vvaalluuee
BBLLOOOODD LLOOSSSS << ..0055
IINNTTRRAAVVAASSAATTIIOONN << ..0055
OOPPEERRAATTIINNGG TTIIMMEE << ..0055
MMeeaassuurreemmeenntt pp vvaalluuee
BBLLOOOODD LLOOSSSS << ..0055
IINNTTRRAAVVAASSAATTIIOONN << ..0055
OOPPEERRAATTIINNGG TTIIMMEE << ..0055
Intracervical VasopressinEffects During Operative HysteroscopyAdapted from Phillips D et al. Obstet Gynecol. 1996; 88:761-766.
N=106
Intracervical VasopressinEffects During Operative HysteroscopyAdapted from Phillips D et al. Obstet Gynecol. 1996; 88:761-766.
N=106
Operative HysteroscopyOperative Hysteroscopy
Hysteroscopic Instrumentation
• Telescope
• Sheath System– Hysteroscope
–Diagnostic
–Operative
– Resectoscope
GYNECARE VERSAPOINT Bipolar Electrodes: Utilizing Saline
Spring Twizzle Ball
Bipolar Loop Resecting 0-Degree Vaporizing
Chips: The Most Frustrating Part of the Procedure
• Removal under direct visualization with wire loop
• Polyp forceps
• Corson graspers
• Suction curette
• Consider morcellators
• Care must be taken to prevent perforation when done blindly
Page 10
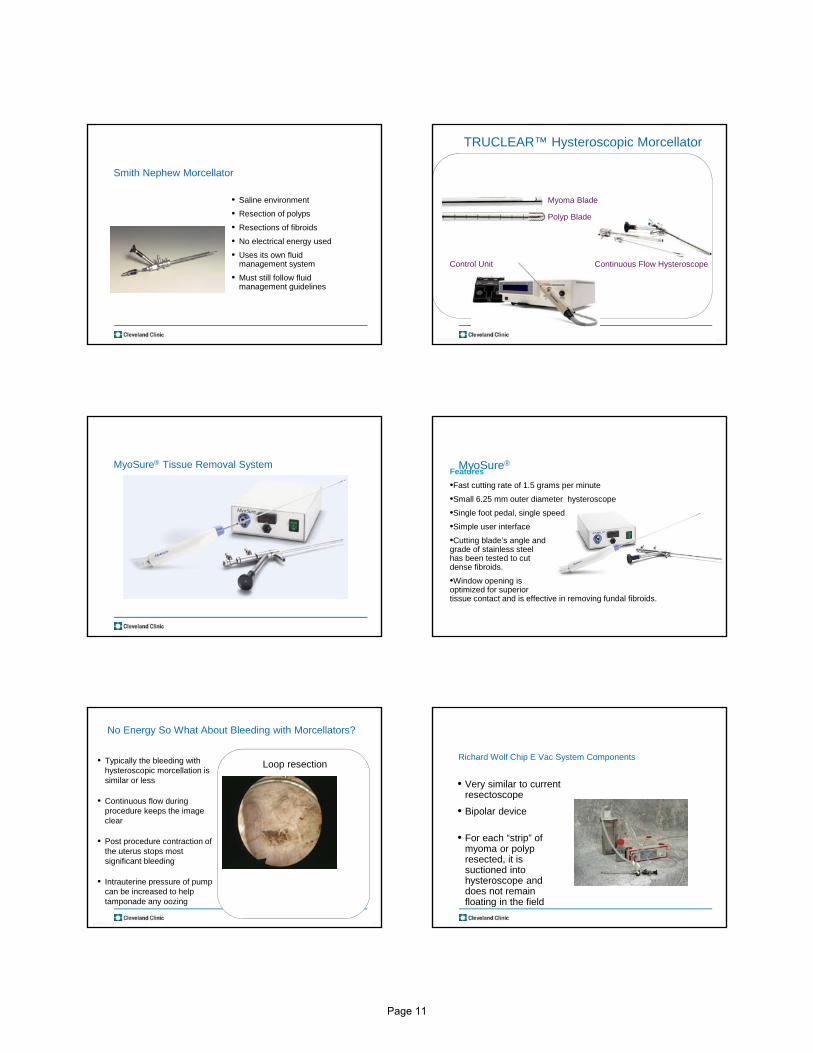
Smith Nephew Morcellator
• Saline environment
• Resection of polyps
• Resections of fibroids
• No electrical energy used
• Uses its own fluid management system
• Must still follow fluid management guidelines
4410/6/2014
TRUCLEAR™ Hysteroscopic Morcellator
Control Unit Continuous Flow Hysteroscope
Myoma Blade
Polyp Blade
MyoSure® Tissue Removal System MyoSure®Features
•Fast cutting rate of 1.5 grams per minute
•Small 6.25 mm outer diameter hysteroscope
•Single foot pedal, single speed
•Simple user interface
•Cutting blade’s angle and grade of stainless steel has been tested to cut dense fibroids.
•Window opening is optimized for superiortissue contact and is effective in removing fundal fibroids.
4710/6/2014
No Energy So What About Bleeding with Morcellators?
• Typically the bleeding with hysteroscopic morcellation is similar or less
• Continuous flow during procedure keeps the image clear
• Post procedure contraction of the uterus stops most significant bleeding
• Intrauterine pressure of pump can be increased to help tamponade any oozing
Loop resectionRichard Wolf Chip E Vac System Components
• Very similar to current resectoscope
• Bipolar device
• For each “strip” of myoma or polyp resected, it is suctioned into hysteroscope and does not remain floating in the field
Page 11

Components of Richard Wolf Chip E-Vac System
Intra Operative Surgical Techniques for Polypectomy
• If blind procedure is performed, look with hysteroscope to determine that full resection is completed
• Resect to the endometrium
• Remove and send all portions of polyp for pathology
• Determine if other pathology is present
• Final inspection to determine that full resection occurred
– Check the endocervix and endometrial canal…don’t miss co-existing lesions
Fluid Guidelines
• If using Glycine or Sorbitol solutions– Halt procedure when deficit is 1000 mL and order stat sodium
and potassium level.
– If normal proceed and completely stop procedure with total deficit of 1500 mL, recheck electrolytes and consider empiric diuresis with Lasix 20 mg IV
–Monitor clinical symptoms if Na < 132
• If Normal Saline is used, more latitude– Halt procedure when deficit is 2,500 -3000 mL
– Diuresis with Lasix, assess for pulmonary edema
Don’t Play Peek a boo or Telephone Medicine
• See and examine the patient
• Order appropriate laboratory and imaging tests
• Don’t hope the problem away
• Re-assess until the problem has resolved
Informed Consent
• Fluid Overload
• Thermal injury
• Infertility
• Adhesions
• Bleeding
• Infection
• Uterine perforation
• Symptomatic hyponatremia
• Early termination
• Incomplete resection
• Hematometria
• Conversion:– Laparoscopy– Laparotomy
• Hysterectomy
• Death
Page 12

Discharge instructionsDischarge instructions
• Expect serous discharge 1-2 weeks
• bloody discharge 7-21 days
• cramping 24-48 hours
• no intercourse for one week
• call if persistent pain or fever
Summary
• Excellent pre-operative evaluation is essential to determine, size, number and location of fibroids
• Excellent hysteroscopic skills with attention to fluid management is necessary
• Superb clinical outcome and minimal complications noted with operative hysteroscopy in appropriately selected patients
References
• Ribeiro A. Use of Misoprostol Prior to Hysteroscopy in Postmenopausal Women: A Randomized, Placebo-Controlled Clinical Trial. J Minim Invasive Gynecol.2008;15:67-73
Page 13

Focusing in on the Problem:Visualization in Hysteroscopy
Focusing in on the Problem:Visualization in HysteroscopyNeeraj Mehra, MD, FRCSC
Department of Obstetrics & Gynecology
University of British Columbia
AAGL Global Congress: Hysteroscopy Course
November 18, 2014
DisclosureDisclosure
Consultant: Actavis Pharmaceutical, Bayer Healthcare Corp., Ethicon Endo-Surgery
Learning ObjectivesLearning Objectives
1.Understand the importance of good visualization at endoscopy
2.Identify common reasons for poor visualization at laparoscopic and hysteroscopic surgery
3.Develop specific strategies to improve visualization at laparoscopy and hysteroscopy
THEN NOW
Why is visualization important?
Why is visualization important?
1.Suboptimal view slows procedural progress
2.Increased frustration with repeated attempts to resolve the situation
3.Poor visualization increases potential for adverse events
Visualization Problems in Hysteroscopy
Visualization Problems in Hysteroscopy
1. Focus & Lighting
2. Zoom
3. Blood
4. Distention
5. Bubbles
Page 14

Focus
• Adjust focus BEFORE introducing hysteroscope
• May become off focus even when set initially. Consider focus adjustment when other visualization methods are ineffective
Lighting
• White balance to reduce glare and adjust color tone
• Consider damage to fiberoptic cable or light source
• Light transmission is a function of number of fibers, size of the cable and power of light source
Focus & LightingFocus & LightingVisualization TipVisualization Tip
Make the Circle
Adjust the Zoom
Incorrect Correct
Visualization Problems in Hysteroscopy:
ZOOM
Visualization Problems in Hysteroscopy:
ZOOM
Visualization Problems in Hysteroscopy: POOR DISTENSION
Visualization Problems in Hysteroscopy: POOR DISTENSION
Possible Reasons for Poor Distension
Low inflow of distention media
Excess suction
Over dilated cervix
Perforation
How to correct?
Raise height of bagPressure cuff / Squeeze
Fluid Management System
Turn down suction(but NOT OFF)
Extra tenaculum on cervix
Consider Stopping
Visualization Problems in Hysteroscopy:
BLOOD
Visualization Problems in Hysteroscopy:
BLOOD
Visualization Problems in Hysteroscopy:
BLOOD
Visualization Problems in Hysteroscopy:
BLOOD
Page 15
Suction blocked at internal os
No Flow
= Poor vision
Scope too far
Turbulent Flow
= Poor vision
Suction past internal os
Laminar Flow
= Vision Clear!
Visualization Problems in Hysteroscopy:
BLOOD
Visualization Problems in Hysteroscopy:
BLOOD
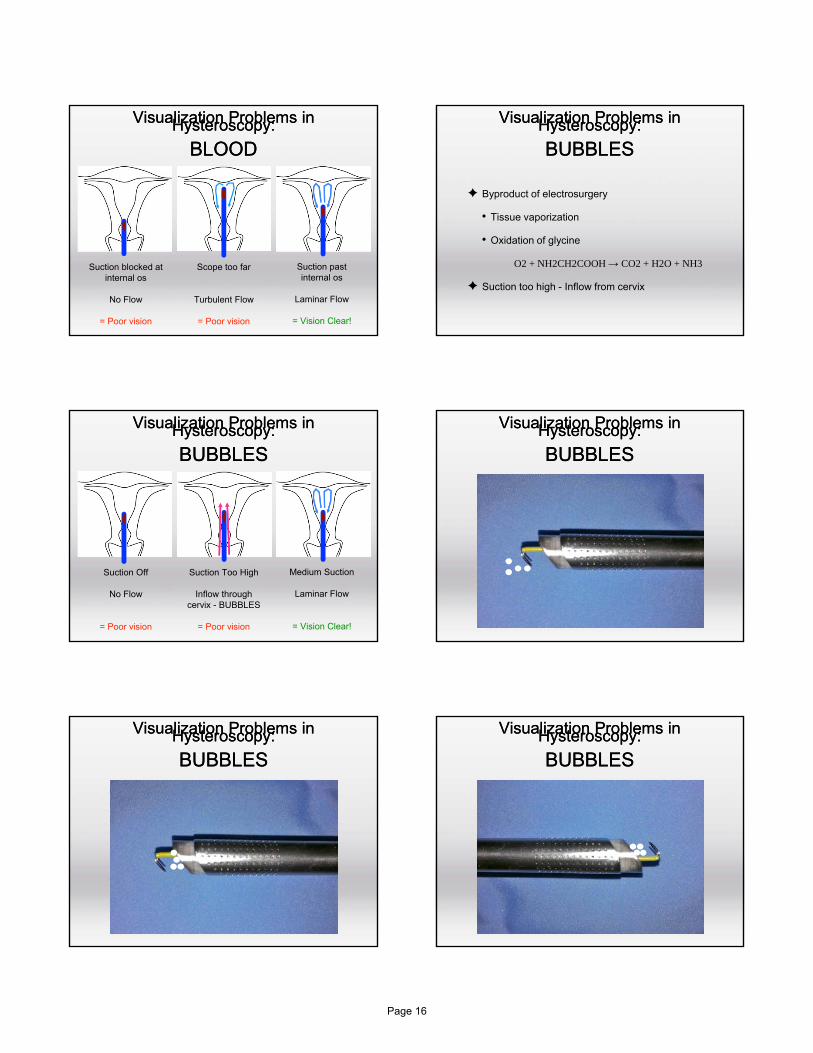
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
✦ Byproduct of electrosurgery
• Tissue vaporization
• Oxidation of glycine
O2 + NH2CH2COOH → CO2 + H2O + NH3
✦ Suction too high - Inflow from cervix
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Suction Off
No Flow
= Poor vision
Medium Suction
Laminar Flow
= Vision Clear!
Suction Too High
Inflow through cervix - BUBBLES
= Poor vision
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES
Page 16

Visualization Problems in Hysteroscopy:
BUBBLES
Visualization Problems in Hysteroscopy:
BUBBLES CONCLUSIONSVisualization at Hysteroscopy
CONCLUSIONSVisualization at Hysteroscopy
1. Focus and White Balance before starting
2. Make the Circle - Adjust the Zoom
3. Ensure adequate distention
• Adjust inflow & suction
4. Clear the blood - get past the cervix
5. Clear the bubbles under the hood
Thank YouThank You
Page 17
Managing Pain and Anxiety for Office or Outpatient Procedures
Scott Chudnoff, MD, MSAssociate Professor – Einstein Medical SchoolDirector of Gynecology – Montefiore Medical
Center
Disclosure
I have no financial relationships to disclose.
Objectives
• After conclusion of this lecture, the participant will be able to:
– To explain the association of pain and anxiety
– To recognize the sources of pain and anxiety for procedures in the office setting
– To describe various techniques to reduce the associated pain and anxiety with outpatient hysteroscopic procedures
The Pitfalls of Office Procedures
Fear of Pain
• One of the biggest obstacles to office procedures is physician fear of pain
– Many patients also concerned regarding potential for pain
6
Page 18

Anxiety
Procedural Factors
Analgesia / Anesthesia
Perceived Pain
How Painful Is Hysteroscopy?
VAN DEN BOSCH T, VERGUTS J, DAEMEN A, et al. Pain experienced during transvaginal ultrasound, saline contrast sonohysterography, hysteroscopy and office sampling: a comparative study. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2008;31:346‐51.
ANXIETYAssociation with Pain
The Story of Aron Rolston Pain and Anxiety Association
Perceived Pain
Painful Stimulus
Anxiety
KOKANALI MK, CAVKAYTAR S, GUZEL AI, et al. Impact of preprocedural anxiety levels on pain perception in patients undergoing office hysteroscopy. Journal of the Chinese Medical Association : JCMA 2014;77:477‐81.CARWILE JL, FELDMAN S, JOHNSON NR. Use of a Simple Visual Distraction to Reduce Pain and Anxiety in Patients Undergoing Colposcopy. Journal of lower genital tract disease 2014.BASER E, TOGRUL C, OZGU E, ESERCAN A, CAGLAR M, GUNGOR T. Effect of pre‐procedural state‐trait anxiety on pain perception and discomfort in women undergoing colposcopy for cervical cytological abnormalities. Asian Pacific journal of cancer prevention : APJCP 2013;14:4053‐6.KOLA S, WALSH JC. Determinants of pre‐procedural state anxiety and negative affect in first‐time colposcopy patients: implications for intervention. European journal of cancer care 2012;21:469‐76.
Page 19
DECREASING ANXIETY
Distraction
Music
ANGIOLI R, DE CICCO NARDONE C, PLOTTI F, et al. Use of music to reduce anxiety during office hysteroscopy: prospective randomized trial. Journal of minimally invasive gynecology 2014;21:454‐9.
Waiting
CARTA G, PALERMO P, MARINANGELI F, et al. Waiting time and pain during office hysteroscopy. Journal of minimally invasive gynecology 2012;19:360‐4.
Setting
Temperature Modesty
• Lock the door when starting the procedure
• Cover the patient
PROCEDURAL FACTORS
Page 20

Where is the pain
• Anytime there if physical manipulation there may be pain– Insertion of the speculum– Tenaculum– Injection of cervix / paracervix– Dilation– Hysteroscope insertion
• External Os• Internal Os
– Vasovagal
– Uterine distention
Case Selection / Technique
Vaginoscopy
COOPER NA, SMITH P, KHAN KS, CLARK TJ. Vaginoscopic approach to outpatient hysteroscopy: a systematic review of the effect on pain. BJOG : an international journal of obstetrics and gynaecology 2010;117:532‐9.
Misoprostol Cervical Preparation
Menopause
Dose (mcg) / Route / Timing Prior (hrs)
Variable Assessed Pain Difference P‐Value
Atay V, et al PRE 400 / Vaginal / 4 Cervical Dilation Reduced 0.05
Valente, et al PRE 400 / Vaginal / 6 Entire Procedure No Difference 0.72
Da Costa, et al POST 200 / Vaginal / 8 Hysteroscope in OSClamping CervixEndometrial Biopsy
Reduce (VAS 7 : 5)No DifferenceNo Difference
0.020.740.19
Singh, et al PRE / POST
400 / Vaginal / 4‐6 Pain At End Reduced 0.03
Waddell, et al PRE / POST
400 / Vaginal / 12‐24 Cervical Dilation Reduced*(sub group only Post)
0.004
BenChetrit , et al PRE Oral Entire Procedure No difference 0.60
DA COSTA AR, PINTO‐NETO AM, AMORIM M, PAIVA LH, SCAVUZZI A, SCHETTINI J. Use of misoprostol prior to hysteroscopy in postmenopausal women: a randomized, placebo‐controlled clinical trial. Journal of minimally invasive gynecology 2008;15:67‐73.SINGH N, GHOSH B, NAHA M, MITTAL S. Vaginal misoprostol for cervical priming prior to diagnostic hysteroscopy‐‐efficacy, safety and patient satisfaction: a randomized controlled trial. Archives of gynecology and obstetrics 2009;279:37‐40.VALENTE EP, DE AMORIM MM, COSTA AA, DE MIRANDA DV. Vaginal misoprostol prior to diagnostic hysteroscopy in patients of reproductive age: a randomized clinical trial. Journal of minimally invasive gynecology 2008;15:452‐8.WADDELL G, DESINDES S, TAKSER L, BEAUCHEMIN MC, BESSETTE P. Cervical ripening using vaginal misoprostol before hysteroscopy: a double‐blind randomized trial. Journal of minimally invasive gynecology 2008;15:739‐44.BEN‐CHETRIT A, ELDAR‐GEVA T, LINDENBERG T, et al. Mifepristone does not induce cervical softening in non‐pregnant women. Hum Reprod 2004;19:2372‐6.
COOPER NA, SMITH P, KHAN KS, CLARK TJ. Does cervical preparation before outpatient hysteroscopy reduce women's pain experience? A systematic review. BJOG : an international journal of obstetrics and gynaecology 2011;118:1292‐301.
Scope SizeMenopause
Sheath Size (mm) Pain Difference P‐Value
Giordia, et al POST 3.5 vs. 5 Reduced <0.01
Campo, et al PRE / POST
3.5 vs. 5 Reduced 0.72
DE Angelis, et al POST 3.3 vs. 5 Reduced 0.020.740.19
Rullo, et al PRE / POST
3 vs. 5 No Difference 0.03
1. CAMPO R, MOLINAS CR, ROMBAUTS L, et al. Prospective multicentre randomized controlled trial to evaluate factors influencing the success rate of office diagnostic hysteroscopy. Hum Reprod 2005;20:258‐63.2. DE ANGELIS C, SANTORO G, RE ME, NOFRONI I. Office hysteroscopy and compliance: mini‐hysteroscopy versus traditional hysteroscopy in a randomized trial. Hum Reprod 2003;18:2441‐5.3. GIORDA G, SCARABELLI C, FRANCESCHI S, CAMPAGNUTTA E. Feasibility and pain control in outpatient hysteroscopy in postmenopausal women: arandomized trial. Acta obstetricia et gynecologica Scandinavica 2000;79:593‐7.4. RULLO S, SORRENTI G, MARZIALI M, ERMINI B, SESTI F, PICCIONE E. Office hysteroscopy: comparison of 2.7‐ and 4‐mm hysteroscopes for acceptability, feasibility and diagnostic accuracy. The Journal of reproductive medicine 2005;50:45‐8.
Page 21
Fluid Temperature
Increase Comfort
Increase Fluid Intravasation
ALMEIDA ZM, PONTES R, COSTA HDE L. [Evaluation of pain in diagnostic hysteroscopy by vaginoscopy using normal saline at body temperature as distension medium: a randomized controlled trial]. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia 2008;30:25‐30.
DE FREITAS FONSECA M, ANDRADE CM, JR., DE MELLO MJ, CRISPI CP. Effect of temperature on fluidity of irrigation fluids. British journal of anaesthesia 2011;106:51‐6.
ANALGESIA / ANESTHESIA
Approaches
• PO / IM Meds– NSAID’s / Cox 2 inhibitors– Opiates– Anxiolytics
• Blocks– Topical– Injectable
• Regional• Conscious Sedation• General Anesthesia
NSAID’s / COX 2 Inhibitors
NAGELE F, LOCKWOOD G, MAGOS AL. Randomised placebo controlled trial of mefenamic acid for premedication at outpatient hysteroscopy: a pilot study. British journal of obstetrics and gynaecology 1997;104:842‐4.TAM WH, YUEN PM. Use of diclofenac as an analgesic in outpatient hysteroscopy: a randomized, double‐blind, placebo‐controlled study. Fertility and sterility 2001;76:1070‐2.ISSAT T, BETA J, NOWICKA MA, MACIEJEWSKI T, JAKIMIUK AJ. A randomized, single blind, placebo‐controlled trial for the pain reduction during the outpatient hysteroscopy after ketoprofen or intravaginal misoprostol. Journal of minimally invasive gynecology 2014;21:921‐7.
NSAID’s
• Need to give before procedure
– 15 minute
• Some will give 2 doses
– 1 the night before
– 2nd prior to procedure
Cochrane Review
AHMAD G, O'FLYNN H, ATTARBASHI S, DUFFY JM, WATSON A. Pain relief for outpatient hysteroscopy. The Cochrane database of systematic reviews 2010:CD007710.
Page 22

FLORIS S, PIRAS B, ORRU M, et al. Efficacy of intravenous tramadol treatment for reducing pain during office diagnostic hysteroscopy. Fertility and sterility 2007;87:147‐51.LIN YH, HWANG JL, HUANG LW, CHEN HJ. Use of sublingual buprenorphine for pain relief in office hysteroscopy. Journal of minimally invasive gynecology 2005;12:347‐50.
? Pain Control
Decreased Compliance
Increase complications
Conscious Sedation
• Need to know local and state regulations
• Need to be prepared for airway, respiratory and cardiac support
• Is generally unnecessary for office hysteroscopy
Depth of Sedation
Patient Response Minimal Sedation(Anxiolysis)
Moderate Sedationand Analgesia (Conscious Sedation)
Deep Sedation / Analgesia
General Anesthesia
Responsiveness Normal Response to verbal stimulation
Purposeful response to verbal or tactile stimulation
Purposeful response after repeated or painful stimulation
Unarousable even with painful stimulus
Airway Unaffected No intervention required
Intervention may be required
Intervention often required
Spontaneous Ventilation
Unaffected Adequate Maybe inadequate Often inadequate
Cardiovascular function Unaffected Usually maintained Usually maintained May be impared
Developed by the ASA
• Can easily slip from a lighter sedation to heavier sedation • Represents a continuum
• Doesn’t matter the route of administration included
Different Local Blocks
COOPER NA, KHAN KS, CLARK TJ. Local anaesthesia for pain control during outpatient hysteroscopy: systematic review and meta‐analysis. BMJ 2010;340:c1130.
Page 23

Topical Anesthesia
• Unlikely to provide significant improvement in pain during procedure.
• May reduce pain associated with tenaculumplacement.
COOPER NA, KHAN KS, CLARK TJ. Local anaesthesia for pain control during outpatient hysteroscopy: systematic review and meta‐analysis. BMJ 2010;340:c1130.DAVIES A, RICHARDSON RE, O'CONNOR H, BASKETT TF, NAGELE F, MAGOS AL. Lignocaine aerosol spray in outpatient hysteroscopy: a randomized double‐blind placebo‐controlled trial. Fertility and sterility 1997;67:1019‐23.
Intrauterine Anesthesia
MERCIER RJ, ZERDEN ML. Intrauterine anesthesia for gynecologic procedures: a systematic review. Obstetrics and gynecology 2012;120:669‐77.
COOPER NA, KHAN KS, CLARK TJ. Local anaesthesia for pain control during outpatient hysteroscopy: systematic review and meta‐analysis. BMJ 2010;340:c1130.
Intrauterine Anesthesia Endometrial Innervation
• Recent evidence about patients with endometriosis and adenomyosis may have increased endometrial innervation
• Presence of pelvic pain history increases the amount of pain likely to be experienced
SARDO AD, FLORIO P, FERNANDEZ LM, et al. The Potential Role of Endometrial Nerve Fibers in the Pathogenesis of Pain During Endometrial Biopsy at Office Hysteroscopy. Reprod Sci 2014.ZHANG X, LU B, HUANG X, XU H, ZHOU C, LIN J. Innervation of endometrium and myometrium in women with painful adenomyosis and uterine fibroids. Fertility and sterility 2010;94:730‐7.
Paracervical / Cervical Block
Courtesy Dr. Mark Glasser
Keys to Paracervical Block
• Time
• Dosage
Page 24

Paracervical Block Cochrane Review
Summative Data – Raw Scores (comp)Total Normal Saline Lidocaine
Mean SD Mean SD Mean SDMean
Difference P‐value
Toradol 2.39 2.44 2.42 2.63 2.35 2.27 .07 .96
Ant Lip Inj 1.77 1.63 2.08 1.76 1.45 1.43 .63 .12
Tenaculum 1.98 2.17 3.00 2.41 0.97 1.28 2.03 <.001
Paracervical 3.53 2.30 4.49 2.38 2.57 1.78 1.92 <.001
Ext Os 2.61 2.52 3.77 2.68 1.46 1.71 2.30 <.001
Int Os 2.95 2.71 4.10 2.77 1.79 2.11 2.30 <.001
EssurePlacement 3.44 2.71 3.74 2.73 3.15 2.69 .60 .33
Menstrual Pain 3.35 2.57 3.45 2.54 3.25 2.62 .20 .68
Post Average 3.76 4.33 4.15 1.90 3.38 5.84 .77 <.001
Post Worst 4.81 2.66 5.84 2.38 3.78 2.54 2.06 <.001
Post Pain 2.23 2.27 2.12 1.90 2.33 2.60 ‐.21 .90
CHUDNOFF S, EINSTEIN M, LEVIE M. Paracervical block efficacy in office hysteroscopic sterilization: a randomized controlled trial. Obstetrics and gynecology 2010;115:26‐34.
References1. Ahmad G, O'Flynn H, Attarbashi S, Duffy JM, Watson A. Pain relief for outpatient hysteroscopy. The Cochrane database of systematic reviews 2010(11):CD007710.2. Almeida ZM, Pontes R, Costa Hde L. [Evaluation of pain in diagnostic hysteroscopy by vaginoscopy using normal saline at body temperature as distension medium: a randomized controlled trial]. Revista brasileira de ginecologia e obstetricia : revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia 2008 Jan;30(1):25‐30.3. Baser E, Togrul C, Ozgu E, Esercan A, Caglar M, Gungor T. Effect of pre‐procedural state‐trait anxiety on pain perception and discomfort in women undergoing colposcopy for cervical cytological abnormalities. Asian Pacific journal of cancer prevention : APJCP 2013;14(7):4053‐6.4. Ben‐Chetrit A, Eldar‐Geva T, Lindenberg T, Farhat M, Shimonovitz S, Zacut D, et al. Mifepristone does not induce cervical softening in non‐pregnant women. Hum Reprod 2004 Oct;19(10):2372‐6.5. Campo R, Molinas CR, Rombauts L, Mestdagh G, Lauwers M, Braekmans P, et al. Prospective multicentre randomized controlled trial to evaluate factors influencing the success rate of office diagnostic hysteroscopy. Hum Reprod 2005 Jan;20(1):258‐63.6. Carwile JL, Feldman S, Johnson NR. Use of a Simple Visual Distraction to Reduce Pain and Anxiety in Patients Undergoing Colposcopy. Journal of lower genital tract disease 2014 Jun 20.7. Cooper KG, Jack SA, Parkin DE, Grant AM. Five‐year follow up of women randomised to medical management or transcervical resection of the endometrium for heavy menstrual loss: clinical and quality of life outcomes. BJOG : an international journal of obstetrics and gynaecology 2001 Dec;108(12):1222‐8.8. Cooper NA, Khan KS, Clark TJ. Local anaesthesia for pain control during outpatient hysteroscopy: systematic review and meta‐analysis. BMJ 2010;340:c1130.9. Cooper NA, Smith P, Khan KS, Clark TJ. Vaginoscopic approach to outpatient hysteroscopy: a systematic review of the effect on pain. BJOG : an international journal of obstetrics and gynaecology 2010 Apr;117(5):532‐9.10. Cooper NA, Smith P, Khan KS, Clark TJ. Does cervical preparation before outpatient hysteroscopy reduce women's pain experience? A systematic review. BJOG : an international journal of obstetrics and gynaecology 2011 Oct;118(11):1292‐301.11. da Costa AR, Pinto‐Neto AM, Amorim M, Paiva LH, Scavuzzi A, Schettini J. Use of misoprostol prior to hysteroscopy in postmenopausal women: a randomized, placebo‐controlled clinical trial. Journal of minimally invasive gynecology 2008 Jan‐Feb;15(1):67‐73.12. Davies A, Richardson RE, O'Connor H, Baskett TF, Nagele F, Magos AL. Lignocaine aerosol spray in outpatient hysteroscopy: a randomized double‐blind placebo‐controlled trial. Fertility and sterility 1997 Jun;67(6):1019‐23.13. De Angelis C, Santoro G, Re ME, Nofroni I. Office hysteroscopy and compliance: mini‐hysteroscopy versus traditional hysteroscopy in a randomized trial. Hum Reprod 2003 Nov;18(11):2441‐5.14. de Freitas Fonseca M, Andrade CM, Jr., de Mello MJ, Crispi CP. Effect of temperature on fluidity of irrigation fluids. British journal of anaesthesia 2011 Jan;106(1):51‐6.15. Dood RL, Gracia CR, Sammel MD, Haynes K, Senapati S, Strom BL. Endometrial cancer after endometrial ablation versus medical management of abnormal uterine bleeding. Journal of minimally invasive gynecology 2014 Feb 28.16. Floris S, Piras B, Orru M, Silvetti E, Tusconi A, Melis F, et al. Efficacy of intravenous tramadol treatment for reducing pain during office diagnostic hysteroscopy. Fertility and sterility 2007 Jan;87(1):147‐51.17. Giorda G, Scarabelli C, Franceschi S, Campagnutta E. Feasibility and pain control in outpatient hysteroscopy in postmenopausal women: a randomized trial. Actaobstetricia et gynecologica Scandinavica 2000 Jul;79(7):593‐7.18. Issat T, Beta J, Nowicka MA, Maciejewski T, Jakimiuk AJ. A randomized, single blind, placebo‐controlled trial for the pain reduction during the outpatient hysteroscopy after ketoprofen or intravaginal misoprostol. Journal of minimally invasive gynecology 2014 Sep‐Oct;21(5):921‐7.19. Kokanali MK, Cavkaytar S, Guzel AI, Topcu HO, Eroglu E, Aksakal O, et al. Impact of preprocedural anxiety levels on pain perception in patients undergoing office hysteroscopy. Journal of the Chinese Medical Association : JCMA 2014 Sep;77(9):477‐81.20. Kola S, Walsh JC. Determinants of pre‐procedural state anxiety and negative affect in first‐time colposcopy patients: implications for intervention. European journal of cancer care 2012 Jul;21(4):469‐76.
References21. Lethaby A, Penninx J, Hickey M, Garry R, Marjoribanks J. Endometrial resection and ablation techniques for heavy menstrual bleeding. The Cochrane database of systematic reviews 2013;8:CD001501.22. Lethaby AE, Cooke I, Rees M. Progesterone or progestogen‐releasing intrauterine systems for heavy menstrual bleeding. The Cochrane database of systematic reviews 2005(4):CD002126.23. Lin YH, Hwang JL, Huang LW, Chen HJ. Use of sublingual buprenorphine for pain relief in office hysteroscopy. Journal of minimally invasive gynecology 2005 Jul‐Aug;12(4):347‐50.24. Marjoribanks J, Lethaby A, Farquhar C. Surgery versus medical therapy for heavy menstrual bleeding. The Cochrane database of systematic reviews 2006(2):CD003855.25. Nagele F, Lockwood G, Magos AL. Randomised placebo controlled trial of mefenamic acid for premedication at outpatient hysteroscopy: a pilot study. British journal of obstetrics and gynaecology 1997 Jul;104(7):842‐4.26. Riley KA, Davies MF, Harkins GJ. Characteristics of patients undergoing hysterectomy for failed endometrial ablation. JSLS : Journal of the Society of Laparoendoscopic Surgeons / Society of Laparoendoscopic Surgeons 2013 Oct‐Dec;17(4):503‐7.27. Rullo S, Sorrenti G, Marziali M, Ermini B, Sesti F, Piccione E. Office hysteroscopy: comparison of 2.7‐ and 4‐mm hysteroscopes for acceptability, feasibility and diagnostic accuracy. The Journal of reproductive medicine 2005 Jan;50(1):45‐8.28. Singh N, Ghosh B, Naha M, Mittal S. Vaginal misoprostol for cervical priming prior to diagnostic hysteroscopy‐‐efficacy, safety and patient satisfaction: a randomized controlled trial. Archives of gynecology and obstetrics 2009 Jan;279(1):37‐40.29. Tam WH, Yuen PM. Use of diclofenac as an analgesic in outpatient hysteroscopy: a randomized, double‐blind, placebo‐controlled study. Fertility and sterility 2001 Nov;76(5):1070‐2.30. Tan YH, Lethaby A. Pre‐operative endometrial thinning agents before endometrial destruction for heavy menstrual bleeding. The Cochrane database of systematic reviews 2013;11:CD010241.31. Valente EP, de Amorim MM, Costa AA, de Miranda DV. Vaginal misoprostol prior to diagnostic hysteroscopy in patients of reproductive age: a randomized clinical trial. Journal of minimally invasive gynecology 2008 Jul‐Aug;15(4):452‐8.32. Van den Bosch T, Verguts J, Daemen A, Gevaert O, Domali E, Claerhout F, et al. Pain experienced during transvaginal ultrasound, saline contrast sonohysterography, hysteroscopy and office sampling: a comparative study. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2008 Mar;31(3):346‐51.33. Waddell G, Desindes S, Takser L, Beauchemin MC, Bessette P. Cervical ripening using vaginal misoprostol before hysteroscopy: a double‐blind randomized trial. Journal of minimally invasive gynecology 2008 Nov‐Dec;15(6):739‐44.
Page 25

Working with the Awake PatientTips and Tricks for Success
Sukhbir Sony Singh MD, FRCSCAssociate ProfessorVice‐Chair, GynecologyDepartment of Obstetrics and GynaecologyUniversity of Ottawa/The Ottawa Hospital
AAGL MIS Fellowship DirectorUniversity of Ottawa
Disclosure
Grants/Research: Abbott Laboratories, Bayer Healthcare Corp.
Speakers Bureau: Actavis, Abbott Laboratories, Bayer Healthcare Corp.
43rd AAGL Global Congress. November 17 – 21, 2014. Vancouver, British Columbia.2
Objectives
• At the conclusion of this presentation, the participant will:
– Identify strategies to determine if patients are eligible for “awake” hysteroscopy
– Recognize factors which may lead to successful hysteroscopy in a clinic/office setting
– apply principles which may improve the patient experience during “awake” hysteroscopy
Introduction
• Outpatient (office/ambulatory) hysteroscopy is a safe and effective method to evaluate the endometrial cavity
• Operative procedures can also be completed safely, including transcervical sterilization and global endometrial ablation
• Can be performed without intraoperative analgesia, using the vaginoscopy approach
Bettochi et al., J Am Assoc Gyn Lap. 2004, Cicinelli et al, Fert Ster 2003, Cooper et al. BJOG 2010
Introduction
• Several advantages over hysteroscopy in the OR, including:
reduced anesthetic risks
faster recovery
improved postoperative pain control
reduced cost
• Many hysteroscopic procedures suitable for outpatient clinic or office setting are currently performed in the operating room
Marsh et al., BJOG 2004, Marsh et al. BJOG 2006
Rationale
• Despite evidence of safety and efficacy, few centers have experience with office/clinic hysteroscopy
• The potential:
– Cost savings to the hospital system
– Patient safety (avoiding GA)
– High surgeon satisfaction
– Timely patient care
Page 26

Where to do it?
• Royal College of Obstetricians and Gynecologist in the United Kingdom 2010 Guidelines:
– All gynecology units provide a dedicated outpatient hysteroscopy service for AUB
• 90% of the procedures can be performed successfully (Cooper et al. 2010).
• What about practice in North America?
Outpatient Hysteroscopy
PROS
• Save OR Time for major cases
• Avoid General Anesthetic
• Quicker Turn Over potential
• Patient centered care
• Out of Hospital
Cons
• Equipment investment
• Surgical experience– Lack of educational
opportunities
• Perceptions – Painful for patients
– Impairs ability to “good surgery”
The Benefits of Outpatient Hysteroscopy
• The “Gold Standard” for Diagnosis of Uterine Abnormalities
• Easy to do and NO Anesthesia Required
• See and Treat Patient Centered Approach
The “Office” Set Up
• Things have changed…
– Image Quality
– Scope size
– Distension Media
The Space
The Society of Obstetricians and Gynaecologists of Canada (SOGC) | Annual Clinical Meeting | Calgary, Alberta | June 11‐14, 201312
Page 27
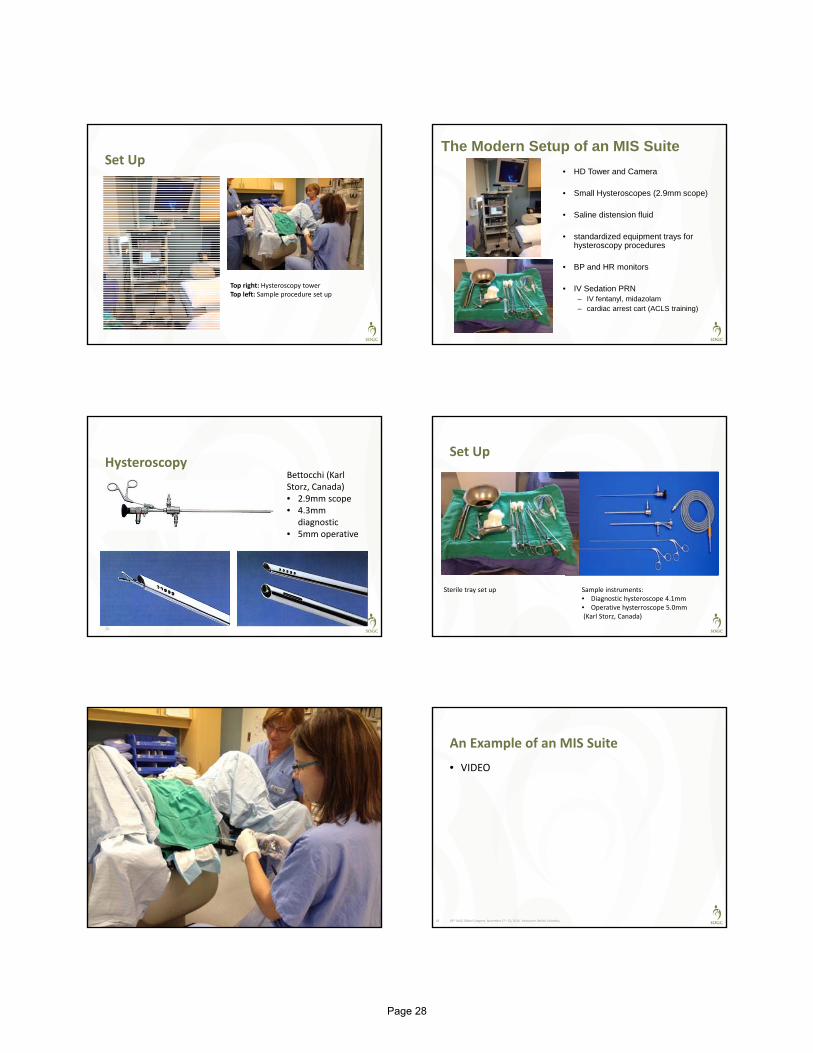
Set Up
Top right: Hysteroscopy towerTop left: Sample procedure set up
The Modern Setup of an MIS Suite
• HD Tower and Camera
• Small Hysteroscopes (2.9mm scope)
• Saline distension fluid
• standardized equipment trays for hysteroscopy procedures
• BP and HR monitors
• IV Sedation PRN – IV fentanyl, midazolam– cardiac arrest cart (ACLS training)
Hysteroscopy
15
Bettocchi (Karl Storz, Canada)• 2.9mm scope• 4.3mm
diagnostic• 5mm operative
Set Up
Sterile tray set up Sample instruments:• Diagnostic hysteroscope 4.1mm• Operative hysterroscope 5.0mm(Karl Storz, Canada)
The Society of Obstetricians and Gynaecologists of Canada (SOGC) | Annual Clinical Meeting | Calgary, Alberta | June 11‐14, 201317
An Example of an MIS Suite
• VIDEO
43rd AAGL Global Congress. November 17 – 21, 2014. Vancouver, British Columbia.18
Page 28

Important Clinical Applications for Office Hysteroscopy
• Retained IUD
• “Failed Hysteroscopy” in the OR/Stenotic Cervix
• Post myomectomy
• Post uterine surgery or complications
• Uterine anomaly or abnormalities
• Primary visit for infertility
Pain Pain
Patient ExperiencePatient
Experience
Surgeon ExperienceSurgeon
Experience
Pain Relief ModalitiesPain Relief Modalities
Equipment Size
Equipment Size
Patient factors
• Anxiety
– Education
– Environment
– Support
• History of Pain
– Dysmennorrhea
– endometriosis
Environment matters
• Reduce anxiety and surrounding stressors
• Lighting, music and “vocal local”
Education Surgeon experience & Instrument Size
• Protective against pain
• Time (duration) of procedure
• Instrument size matters
de Freitas Fonseca et al. JMIG 2014 & Pluchino et al. JMIG 2010 (see references)
Page 29

No Anesthesia Required!
Less pain with: Mini‐hysteroscopes 3.5mm instruments versus 5mm
Skilled surgeon
Surgery in mucosa (polyps, biopsies, lysis of adhesions
Greater Risk of Pain with: Previous C/S
Anxiety & CPP
Menopausal
Longer procedure (>15min)
Hysteroscopy without anesthesia: review of recent literature.Cicinelli E. J Minim Invasive Gynecol. 2010 Nov-Dec;17(6):703-8.University of Bari, Bari, Italy. [email protected]
No Touch technique
• involves introducing the hysteroscope into the vagina, cervix, and into cavity under direct vision,
• without speculum insertion
• without application of a tenaculum
Outcomes:
• Less pain versus traditional speculum/tenaculum
• Speculum is most painful
• Can avoid using any analgesia or anesthesia
Ron Sagev et al. 2006, Garbin et al, 2006, Siristatidis et al, 2010, Cooper et al, 2010
Vaginoscopy
Vaginoscopy.mov
Office Hysteroscopy
Hysteroscopy.mov55 yo for hysterectomy referral
Hysteroscopy Suite
Diagnostic/Operative
(ie. Polypectomy, sterilization)
Procedural•Ablation•Myomectomy•Sterilization
•Preop NSAIDS•If required:Ativan SL, NarcoticParacervical blockIV Sedation
•Preop NSAIDS• IV sedation:
•Midazolam 2mg*•Fetanyl 50‐100mcg*
•Paracervical block
Analgesia Protocols Analgesia Protocols
Diagnostic and Operative
• Preop NSAIDS
• & acetaminophen
• If required:
– Ativan SL,
– PO Narcotic
– Paracervical block
– IV Sedation
Procedural
• Preop NSAIDS
• & acetaminophen
• IV sedation:
– Midazolam 2mg*
– Fetanyl 50‐100mcg*
• Paracervical block
43rd AAGL Global Congress. November 17 – 21, 2014. Vancouver, British Columbia.30
Page 30

Procedural Protocol
• information booklet provided to patients
• NSAID & Acetaminophen PO night before and morning of the procedure
• +/‐ 200 mcg pv misoprostol night or am prior to procedure (physician preference)
• light meal prior to procedure
Office Hysteroscopy works
• Approx 5000 cases by Betocchi (2004)
• NO Anesthetic or analgesia
– Operative hysteroscopy
– Polyps, lysis of adhsions, septums
– Extremely well tolerated
– Only those with larger polyps felt more discomfort (low to moderate pain)
J Am Assoc Gynecol Laparosc. 2004 Feb;11(1):59-61.Operative office hysteroscopy without anesthesia: analysis of 4863 cases performed with mechanical instruments.Bettocchi S, Ceci O, Nappi L, Di Venere R, Masciopinto V, Pansini V, Pinto L, Santoro A, Cormio G
Complications
• Very low rate
– Pain not controlled with methods available (pre‐procedure with cytotec, with procedure)
– Vasovagal response
– Allergic reaction (to local, to meds)
• Clark et al., 2002: systematic review of 25,000
– 3/10,000 rate of serious complications (uterine perforation, pelvic infection, bladder perforation
Complications
• Di Spiezio Sardo et al, 2008
– complication rate of 5.4%
– such as pain, vasovagal, bleeding, shoulder pain, false passage and cervical trauma
• Cicinelli et al (2003)
– 6000 procedures
– 0.17% rate of vasovagal reaction, 2.08% rate of nausea, and 5.75% rate of abdominal cramps.
Personal Experience Shared
The Ottawa Hospital
Table 1: Overview of Procedures Performed at the Ottawa Hospital Hysteroscopy Suite from Nov. 26, 2008 to July 13, 2012
Procedure type # of cases % of total
Diagnostic Hysteroscopy (+/‐ pipelle biopsy)Failed attempts
844**
31%
Operative Hysteroscopy• Polypectomy, lysis of adhesions, septoplasty, removal
retained IUD, directed biopsy
99 37%
Endometrial Ablations* 62 23%
Transcervical Sterilization 21 7.7%
Total # of cases 271**
*All endometrial ablation procedures were performed using the Novasure device (Hologic, California)** total number of procedures performed exceed 271 due to multiple procedures per case
Page 31

Table 2: Indications for Hysteroscopy (possible to have multiple indications)
Indications for hysteroscopy # cases
Abnormal uterine bleedingPostmenopausal bleedingPolypContraception Fertility assessment/recurrent pregnancy loss Thickened endometrial liningAsherman’s/uterine synechiaRetained IUDAssessment post myomectomy Uterine Septum
10536232121191712106
Table 3: Analgesia administered during each procedure type
Diagnostic Hysteroscopy(total = 84)*
Operative Hysteroscopy(total = 99)
Endometrial Ablation(total = 62)
TranscervicalSterilization(total = 21)
Preoperative NSAIDs
61(72%) 78(79%) 62(100%) 16(76%)
Preoperativeacetominophen
8(9.5%) 8(8.1%) 0 6(29%)
Lorazepam 1(1.2%) 8(8.1%) 0 0
IV fentanyl/midazolam
2(2.4%) 5(5.1%) 61(98%) 2(9.5%)
Paracervicalblock**
10(12%) 7(7.1%) 62(100%) 5(24%)
None 12(14%) 7(7.1%) 0 0
Unspecified 8(9.5%0 8(8.1%) 0 3(14%)* some patients had more than one method of analgesia**performed as per surgeon preference – in most cases with xylocaine and epinephrine
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Overalllevelofcare
Cleanlinessoffacilities
Infotohelpyoumanageathome
Provisionofeducationalmaterial
Paincontrolafterprocedure
Paincontrolduringprocedure
Explanationoftests/procedures
Accessibilityofnursingsupport
Comfortlevelinspeakingwithnurse
Professionalismofattendingnurse
OutpatientHysteroscopyPatientSatisfaction
Excellent
VeryGood
Good
Fair/Poor
N/A
The Ottawa Experience
• High Satisfaction
• Low pain experience
• No anesthesia for basic procedures
• IV sedation limited to patient request (mainly ablations at present)
Conclusion
• Outpatient hysteroscopy can be performed in a safe and effective manner
• Patients are highly satisfied with their procedural experience and analgesia control
• Development of new outpatient hysteroscopy clinics in Canada is strongly encouraged
Page 32

Thanks
• Olga Bougie (PGY ‐4)
• Hassan Shenassa (PGY 20)
• Karine Lortie (PGY 10)
• Our Nurses and Team at The Ottawa Hospital
The Society of Obstetricians and Gynaecologists of Canada (SOGC) | Ontario CME| Toronto, Ontario| November 28, 201343
References
• Ahmad G et al. Pain Relief in office gynaecology. European J of Ob & Gyn & Reprod Biol 155 (2011): 3‐13.
• Angioli R et al. Use of Music to Reduce Anxiety during Office Hysteroscopy. JMIG May/June 2014. Vol 21(3).
• Munro & Brooks. Use of Local Anesthesia for Office Diagnostic and Operative Hysteroscopy. JMIG Nov/Dec 2010. Vol 17(6).
• Pluchino N et al. Office vaginoscopic hysteroscopy in infertile women: effects of gynecologist experience, instrument size and distension media. JMIG 2010:17:344‐350.
Page 33

An Alternative to Hysteroscopy-Transvaginal Ultrasound in the
Evaluation of Abnormal Bleeding
James M. Shwayder, M.D., J.D.Professor and Chair
Department of Obstetrics and Gynecology University of Mississippi
Jackson, Mississippi
Disclosure
Other: Royalties: Cook Women’sHealth
Learning Objectives
• Understand the relative value of different methods of evaluating the endometrium in patients with abnormal uterine bleeding
• Be able to better predict the presence of significant pathology in different age groups
• Understand the role of ultrasound and saline infusion sonography in diagnosis and management
• Be able to describe the unique capabilities of ultrasound
Outline
• Causes of AUB amenable to US diagnosis
• Age-based evaluation
• Sonohysterography (3D)
• Sonobiopsy
• Advantages of ultrasound over hysteroscopy
“Age-Related” Evaluation
• Reproductive Age Group
• Perimenopause
• Menopausal Patients
AUB
• Abnormal Uterine Bleeding (AUB)• Heavy menstrual bleeding (AUB/HMB)
• Menorrhagia• Intermenstrual bleeding (AUB/IMB)
• Metrorrhagia• DUB - Eliminated
Page 34

ACOG Practice Bulleting. Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged Women. Number 128, July 2012
PALM-COEINEndometrial EvaluationHistologic Evaluation
• Options
• Endometrial biopsy
• Dilatation and curettage
• Diagnosis best made by tissue biopsy
• Hormonal dysregulation
• Endometritis
• Endometrial hyperplasia
• Diffuse malignancy
Endometrial EvaluationVisual Evaluation
• Options• Hysteroscopy
• Transvaginal sonography (TVS)
• Saline-infusion sonohysterography (SIS)
• 3D Ultrasound/SIS
• Diagnosis best made by visualizing the endometrial cavity for focal anatomic causes
• Polyps
• Submucous myomas
• Focal malignancy ACOG Practice Bulleting. Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged Women. Number 128, July 2012
PALM-COEIN
Age-Based Findings at Hysteroscopy
Age Group (#)Normal Abnormal
% # % #
< 29 14 64% 9 36% 5
30–39 58 45% 36 55% 22
40–49 105 42% 44 58% 61
50–59 43 28% 12 76% 31
> 60 18 33% 6 67% 12
Total 238 45% 107 55% 131
Indman PD, J Reprod Med 1995; 40: 545-548
Age-Based Findings at SIS(filling defects)
Brown and Shwayder, AIUM Annual Meeting 2007
Age (#)Normal Abnormal
% # % #
< 29 38 68.4% 26 31.6% 12
30–39 80 62.5% 50 37.5% 30
40–49 152 68.4% 104 31.6% 48
50–59 43 60.4% 26 39.6% 17
> 60 28 60.7% 17 39.3% 11
Total 341 65.4% 223 34.6% 118
Page 35
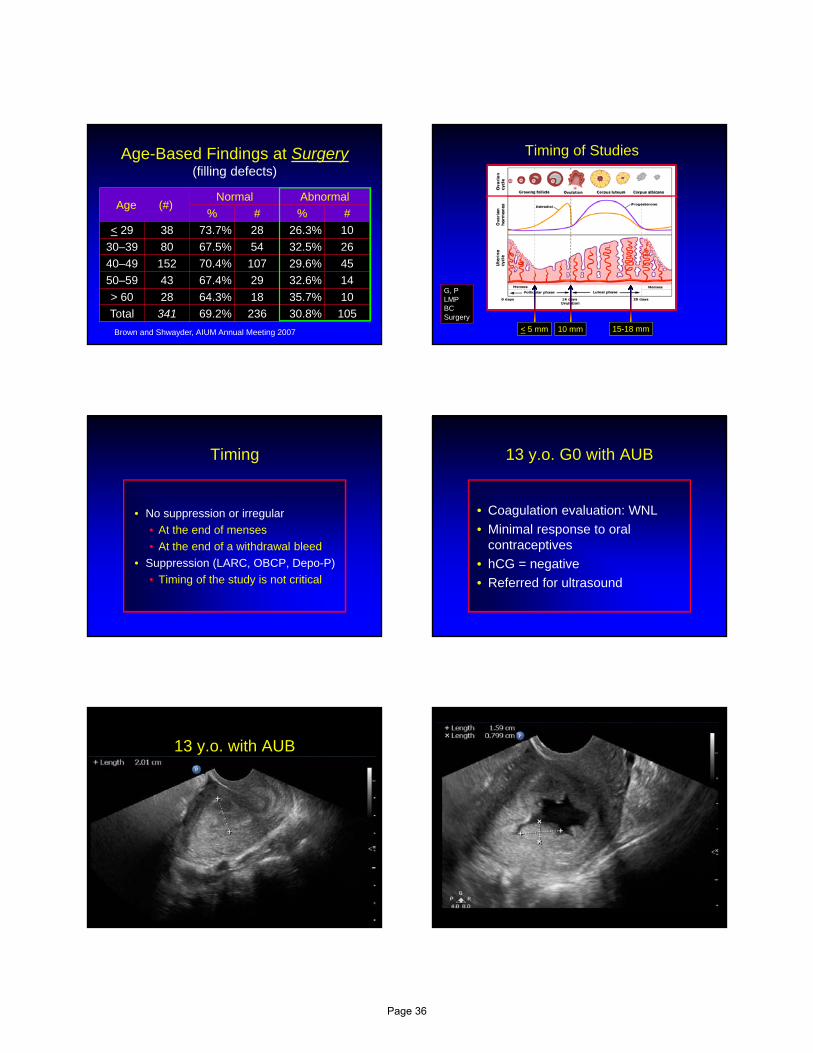
Age-Based Findings at Surgery(filling defects)
Age (#)Normal Abnormal
% # % #
< 29 38 73.7% 28 26.3% 10
30–39 80 67.5% 54 32.5% 26
40–49 152 70.4% 107 29.6% 45
50–59 43 67.4% 29 32.6% 14
> 60 28 64.3% 18 35.7% 10
Total 341 69.2% 236 30.8% 105
Brown and Shwayder, AIUM Annual Meeting 2007 < 5 mm 10 mm 15-18 mm
Timing of Studies
G, PLMPBCSurgery
Timing
• No suppression or irregular
• At the end of menses
• At the end of a withdrawal bleed
• Suppression (LARC, OBCP, Depo-P)
• Timing of the study is not critical
13 y.o. G0 with AUB
• Coagulation evaluation: WNL
• Minimal response to oral contraceptives
• hCG = negative
• Referred for ultrasound
13 y.o. with AUB
Page 36
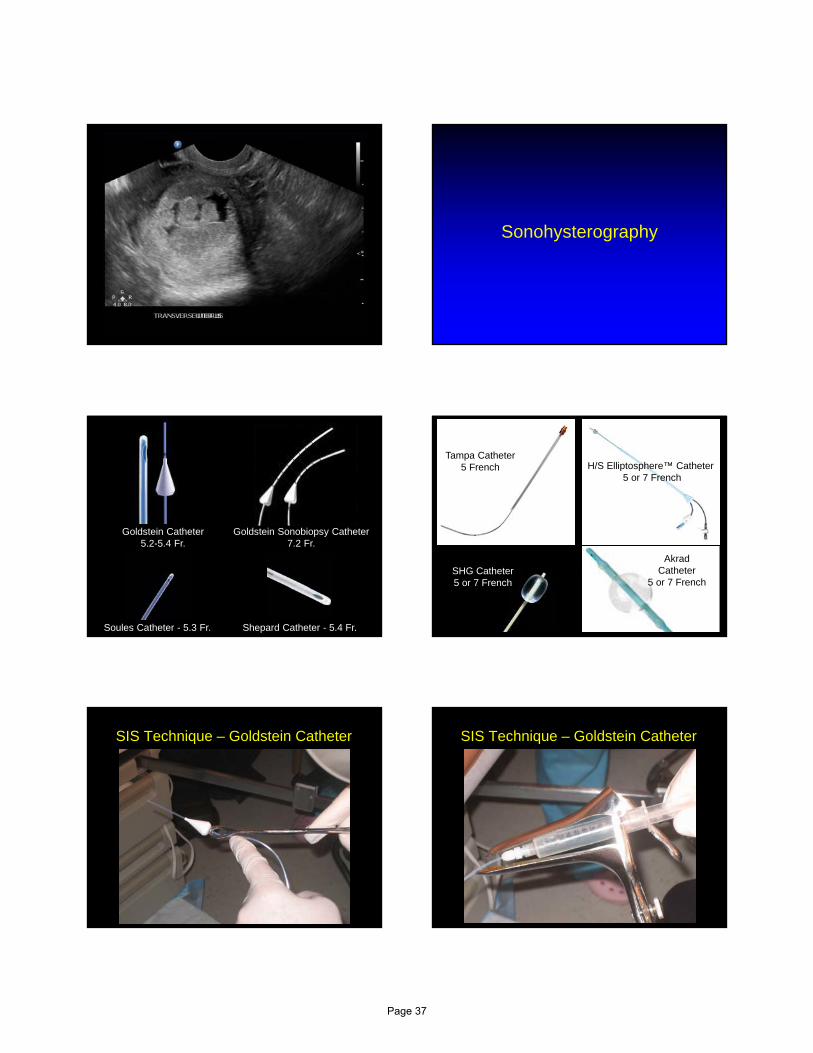
Sonohysterography
Shepard Catheter - 5.4 Fr.Soules Catheter - 5.3 Fr.
Goldstein Catheter5.2-5.4 Fr.
Goldstein Sonobiopsy Catheter7.2 Fr.
SHG Catheter5 or 7 French
Tampa Catheter5 French
Akrad Catheter
5 or 7 French
H/S Elliptosphere™ Catheter5 or 7 French
SIS Technique – Goldstein Catheter SIS Technique – Goldstein Catheter
Page 37
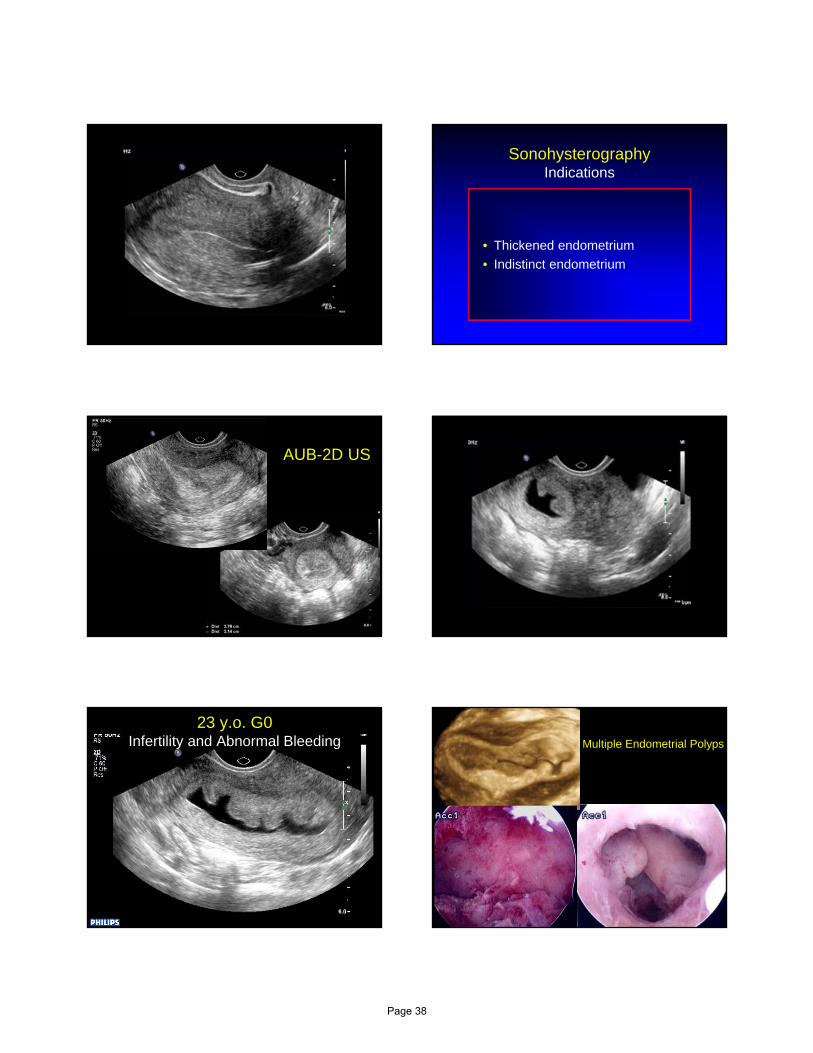
SonohysterographyIndications
• Thickened endometrium
• Indistinct endometrium
AUB-2D US
23 y.o. G0Infertility and Abnormal Bleeding Multiple Endometrial Polyps
Page 38

Indistinct Endometrium 2D SISPolyp
Endometrial Polyp
Endometrial polyp
Perez-Medina et al. J Ultrasound Med 2002; 21: 125-28.
Page 39

SonohysterographyFindings
• Endometrial polyps • Central blood supply or “feeder vessel”
Question
Endometrial polyp
• Is there a risk of malignancy?
Malignancy in Endometrial Polyps
• Asymptomatic 1-2%
• Symptomatic 2-6%
• Increased risk
• Larger size > 19 mm1
• Older age > 55 y.o.2
• Abnormal Doppler RI < 0.53
1Ferrazzi et al. Am J Obstet Gynecol 2009;200:235e1-6.2Hileeto et al. World J Surg Onc 2005;3:8.3Perez-Medina et al. J Ultrasound Med 2002; 21: 125-28.
Sonohysterogram: PolypMultiplaner Display
SonohysterographyEndometrial Polyps and Fibroids 36 y.o. G2P1011
• Presents with complaints of menometrorrhagia for 8 months
• Contraception: None
• HCG: Negative
• Open myomectomy 4/09
• Hysteroscopic myomectomy 10/10
• Cesarean delivery 9/11
Page 40
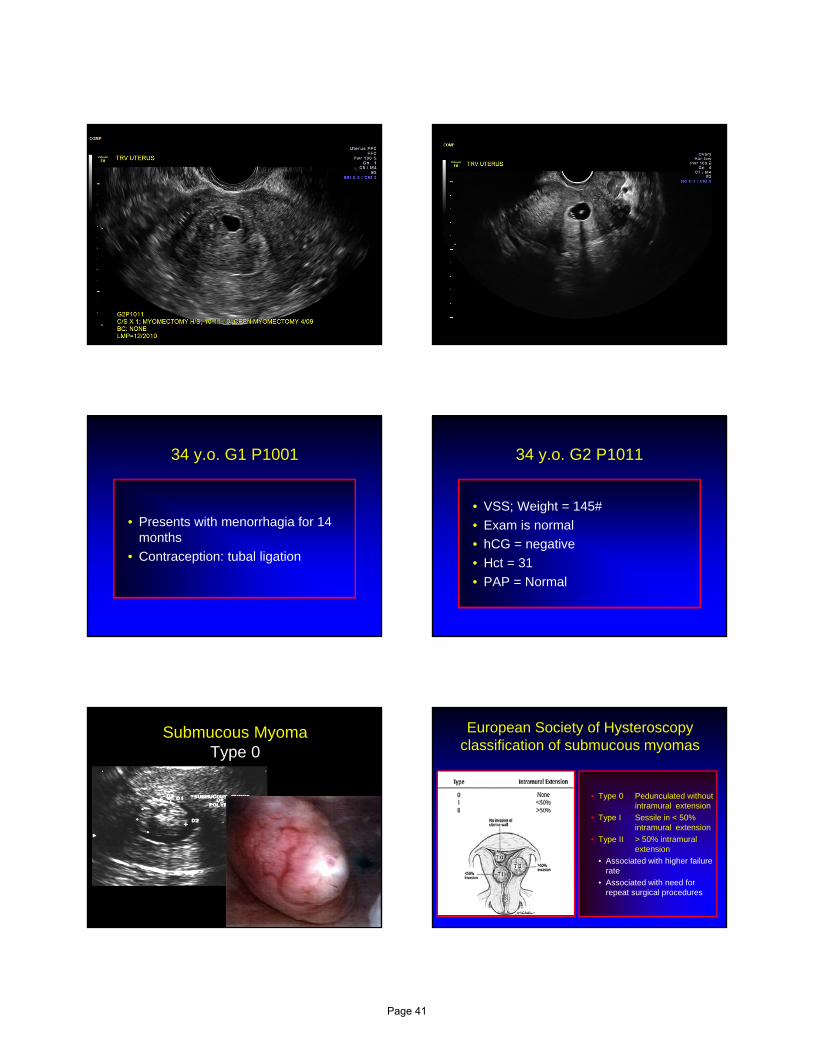
34 y.o. G1 P1001
• Presents with menorrhagia for 14 months
• Contraception: tubal ligation
34 y.o. G2 P1011
• VSS; Weight = 145#
• Exam is normal
• hCG = negative
• Hct = 31
• PAP = Normal
Submucous MyomaType 0
European Society of Hysteroscopy classification of submucous myomas
• Type 0 Pedunculated without intramural extension
• Type I Sessile in < 50% intramural extension
• Type II > 50% intramural extension
• Associated with higher failure rate
• Associated with need for repeat surgical procedures
Page 41
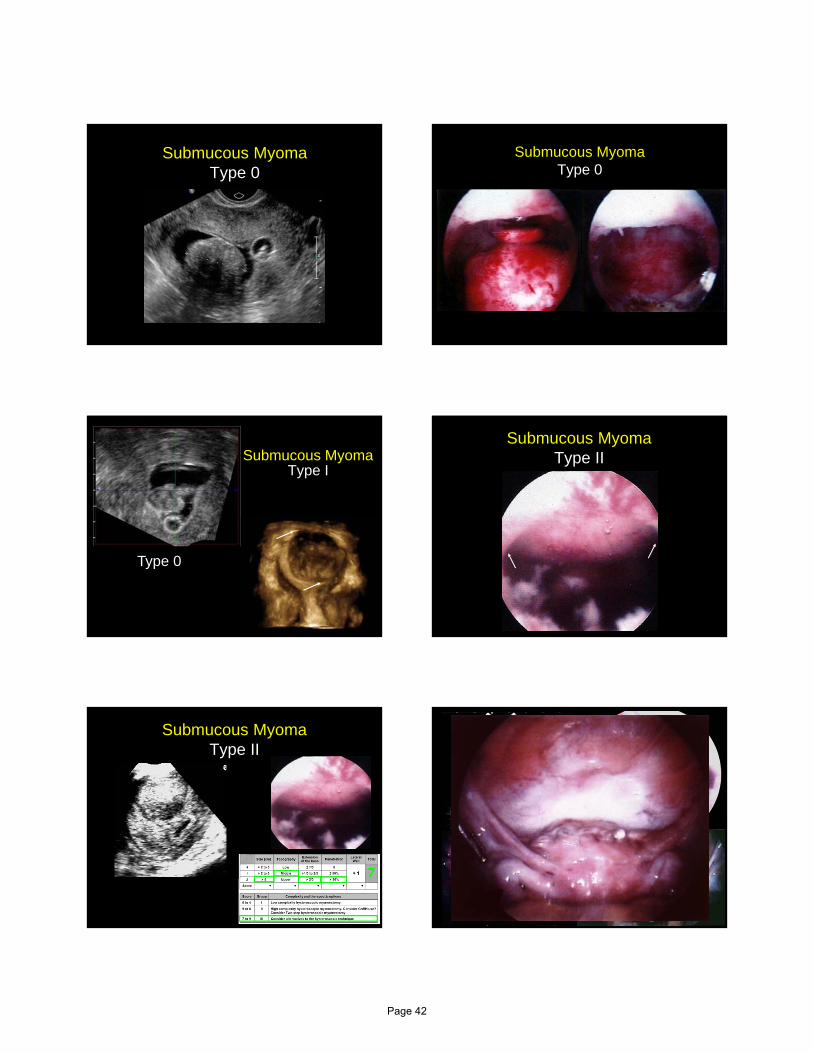
Submucous MyomaType 0
Submucous MyomaType 0
Submucous Myoma Type I
Type 0
Submucous Myoma Type II
Submucous Myoma Type II
77
Page 42

Submucous Myoma Type I
Lasmar et al. J Minim Invasive Gynecol. 2012;19(5):575-80.
55
34 y.o. G0 with AUB Desires Fertility
MRI and Myomas
• MRI was more sensitive than TVS (80% vs. 40%)1
• MRI valuable when 4 or more myomas were present2
• MRI assists in planning surgical approach and complete removal3
1Levens et al. Am J Obstet Gynecol. 2009;200:537.e1-.e7.2Dueholm et al. Am J Obstet Gynecol. 2002;186:409-15.3Parker WH. Am J Obstet Gynecol. 2012;206(1):31-6.
45 y.o. G4 P2113
• Presents with complaints of menometrorrhagia for 16 months
• Contraception: None
• HCG: Negative
• EMB = Endometrial hyperplasia
Ultrasound-based triage for perimenopausal patients with abnormal uterine bleeding
433 perimenopausal patients with AUB• TVS day 4 - 6
• Endometrium < 5 mm = DUB
• No biopsy required
• Endometrium > 5 mm or indistinct = SIS
• SIS < 3 mm = DUB
• SIS = Focal lesion Hysteroscopy + D&C
• SIS = Globally thickened Endometrial Biopsy
Goldstein et al, Am J Obstet Gynecol. 177: 102-108, 1997. (New York)
Page 43

Ultrasound-based triage for perimenopausal patients with abnormal uterine bleeding
Conclusion
Non-directed office biopsy alone without imaging would have potentially missed the diagnosis of focal lesions such as polyps, submucous myomas, and focal hyperplasia in up to 80 patients (18.5%)
Goldstein et al, Am J Obstet Gynecol. 177: 102-108, 1997. (New York)
Benign Endometrial Masses with Endometrial Thickness < 5 mm
• 206 premenopausal women with AUB
• Endometrial thickness in 200
• 80 had an ET < 5mm
Breitkopf et al. Obstet Gynecol 2004;101:120-125.
Benign Endometrial Masses with Endometrial Thickness < 5 mm
Breitkopf et al. Obstet Gynecol 2004;101:120-125.
SIS findingsET < 5 mm ET > 5 mm
# % # %
Normal 61 76.3 71 59.2
Endometrial polyp 11 13.8 23 19.2
Submucous myoma 5 6.2 22 18.3
Uterine septum 1 1.2 0 0
Focal thickening 0 0 3 2.5
Blood clot 2 2.5 1 0.8
Postmenopausal Bleeding
• 58 y.o G1P1001 with persistent postmenopausal bleeding
• Endometrial biopsy x 3• Tissue insufficient for diagnosis
Endometrial Evaluation
1. Endometrial biopsy
2. Dilatation and curettage
3. Hysteroscopy + D&C
4. Transvaginal sonography
5. Saline-infusion sonohysterography
6. 3D Ultrasound
7. Hysterectomy
AUB
Page 44
Endometrial Carcinoma
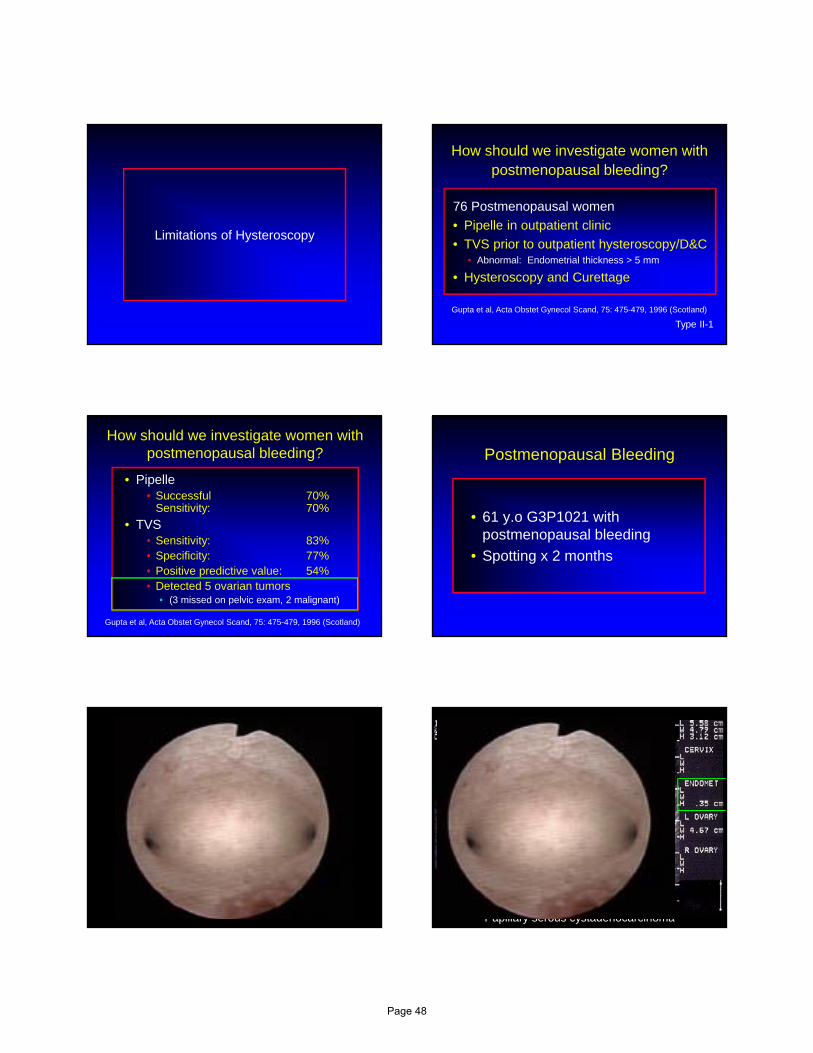
Pipelle endometrial sampling. Sensitivity in the detection of endometrial cancer.
Author Year # Sens JournalZorlu 1994 26 95% Gyn Ob InvestStovall 1991 40 97.5% Obstet GynGuido 1995 65 83% J Reprod MedVan den Bosch 1995 140 44.6% Obstet Gyn
Evidence: II-1
Pipelle endometrial sampling. Sensitivity in the detection of endometrial cancer.
65 Patients with known endometrial cancer• Endometrial biopsy prior to hysterectomy
• Adequate for analysis 63 of 65 97%
• Malignancy detected 54 of 65 83%• Missed: 5 on polyp
3 disease < 5% of surface area
All 11 < 50% of surface area
Guido et al. J Reprod Med 1995; 40: 553-555.
A comparison of Pipelle device and the Vabra aspirator
25 Patients scheduled for hysterectomy• Percent surface area sampled
• Pipelle 4.2% + 0.92%
• Vabra Aspirator 41.6% + 5.7% (p<0.0001)
• Mean number of quadrants sampled (4 ant/4 post)
• Pipelle 2.4 + 0.41
• Vabra aspirator 7.4 + 0.42 (p < 0.0001)
Rodriguez, Yaqub, and King. Am J Obstet Gynecol: 168: 55-59, 1993 (University of Chicago)
Diagnostic OptionsSensitivity
Technique # Polyps & Myomas
Hyperplasia All
Findings
TVS 236 0.39 0.90 0.74
SIS 94 0.96 0.13 0.96
Hysteroscopy 273 0.99 0.27 1.00
Pipelle Biopsy 171 0.10 0.33 0.24
Technique # Polyps & Myomas
Hyperplasia All
Findings
TVS 236 0.39 0.90 0.74
SIS 94 0.96 0.13 0.96
Hysteroscopy 273 0.99 0.27 1.00
Pipelle Biopsy 171 0.10 0.33 0.24
Pasqualotto et al, JAAGL 7: 201, 2000.3.8 mm
Page 45

• Endometrial thickness < 4 mm• Endometrial sampling is not required
• Endometrial thickness > 4 mm or inability to visualize endometrium• Further evaluation• Endometrial biopsy• Hysteroscopy• Sonohysterography
Endometrial Thickness and Postmenopausal Bleeding
ReferenceET
(mm)# # CA
NPV
(%)
Karlsson 1995 < 4 1168 0 100
Ferrazzi 1996< 4
9302 99.8
< 5 4 99.6
Gull 2000 < 4 163 1 99.4
Epstein 2001 < 5 97 0 100
Gull 2003 < 4 394 0 100
Can Ultrasound Replace D&C?
• 394 postmenopausal women referred for PMB (1987-1990)
• Menopausal if > 1 year w/o bleeding
• Ultrasound and D&C
• 10 year follow-up (n = 339)
Gull et al. Am J Obstet Gynecol 2003; 188: 401-08.Göteborg, Sweden
Can Ultrasound Replace D&C?Endometrial Thickness
# CA HyperCA or Hyper
< 4 mm 1780
0%
2
1.1%
2
1.1%
5-7 mm 514
7.8%
0
0%
4
7.8%
> 8 mm 10535
33.3%
3
2.9%
38
36.2%
Unmeasurable 5 0 0 0
TOTAL 33939
11.5%
5
1.5%
44
13%
Recurrent PMB - None
Endometrial Thickness # CA
< 4 mm 134 0
5-7 mm 31 0
> 8 mm 22 0
Unmeasurable 4 0
TOTAL 191 0
Gull et al. Am J Obstet Gynecol 2003; 188: 401-08.Göteborg, Sweden
Recurrent PMB - YesEndometrial Thickness
# CA HyperCA or Hyper
< 4 mm 28 02
7.1%
2
7.1%
5-7 mm 93
33.3%
1
11.1%
4
44.4%
> 8 mm 284
14.3%
5
17.9%
9
32.1%
Unmeasurable 1 0 0 0
TOTAL 667
10.6%
8
12.1%
15
22.7%
Page 46

Sonobiopsy
• Endometrial biopsy performed with catheter used for SIS
• Allows one-step procedure for complete diagnosis
• Assures intracavitary sample
Sonobiopsy
Bernard and Lécuru Goldstein Sonobiopsy Catheter7.2 Fr.
A comparison of Pipelle device and the Vabra aspirator
25 Patients scheduled for hysterectomy• Percent surface area sampled
• Pipelle 4.2% + 0.92%
• Vabra Aspirator 41.6% + 5.7% (p<0.0001)
• Mean number of quadrants sampled (4 ant/4 post)
• Pipelle 2.4 + 0.41
• Vabra aspirator 7.4 + 0.42 (p < 0.0001)
Rodriguez, Yaqub, and King. Am J Obstet Gynecol: 168: 55-59, 1993 (University of Chicago)
Page 47
Limitations of Hysteroscopy
How should we investigate women with postmenopausal bleeding?
76 Postmenopausal women
• Pipelle in outpatient clinic
• TVS prior to outpatient hysteroscopy/D&C• Abnormal: Endometrial thickness > 5 mm
• Hysteroscopy and Curettage
Type II-1
Gupta et al, Acta Obstet Gynecol Scand, 75: 475-479, 1996 (Scotland)
How should we investigate women with postmenopausal bleeding?
• Pipelle• Successful 70%
Sensitivity: 70%
• TVS• Sensitivity: 83%• Specificity: 77%• Positive predictive value: 54%• Detected 5 ovarian tumors
• (3 missed on pelvic exam, 2 malignant)
Gupta et al, Acta Obstet Gynecol Scand, 75: 475-479, 1996 (Scotland)
Postmenopausal Bleeding
• 61 y.o G3P1021 with postmenopausal bleeding
• Spotting x 2 months
Papillary serous cystadenocarcinoma
Page 48
Postmenopausal Bleeding
• 70 y.o G3P1202 with postmenopausal bleeding
Bladder TransverseACOG Practice Bulleting. Diagnosis of Abnormal Uterine Bleeding in
Reproductive-Aged Women. Number 128, July 2012
PALM-COEIN
Page 49

32 y.o. G0 with AUBEnlarged Uterus
• Ultrasound (limited)
• Probable myoma
• Planned for myomectomy
• Referred for complete ultrasound
Adenomyosis
• Incidence• 20-30% of female population
• Up to 70% of hysterectomy specimen
• Symptoms• Pelvic pain
• Dysmenorrhea
• Menorrhagia
• Findings• Inhomogeneous myometrial texture 100%• Globular uterus 95.7%• Small cystic spaces in myometrium 78.7%• Indistinct endometrial stripe 78.7%
• If 2 positive findings• Correct diagnosis by TVUS 84.3%
AdenomyosisUltrasound Diagnosis
Bromley et al. J Ultrasound Med 2000; 19:529–534.
Bromley Criteria
Inhomogeneous myometrium Globularly enlarged uterus
Cystic spaces (> 2 mm) Indistinct endomyometrial border
Page 50
Additional Criteria
Asymmetry Increased myometrial vascularity
Sakhal and Abuhamad. J Ultrasound Med 2012; 31:805–808
Adenomyosis and SIS
Shwayder and Sakhal. J Minim Invasive Gynecol 2014;21: 362-376.
Indistinct border
Indistinct borderCystic spaces
Asymmetry
Shwayder and Sakhal. J Minim Invasive Gynecol 2014;21: 362-376.
Cystic spaces (> 2 mm)
Increased myometrial vascularity
Cystic spaces (> 2 mm)
T2 weighted images
T1 weighted images
Take-home MessageIntracavitary Lesions
• Intracavitary lesions (polyps and submucous myomas) are relatively common in all age groups
• < 29 32.4%• 30-39 39.0%• 40-49 30.6%• 50-59 35.5%• > 60 42.3%
• SIS or hysteroscopy is justifiable in patients of all ages presenting with AUB
Take-home MessagePost-menopausal Bleeding
Endometrial Thickness < 4 mm
• TVS endometrial thickness < 4 mm is a reasonable threshold to avoid initial endometrial biopsy, SIS, or hysteroscopy
• Recurrent abnormal vaginal bleeding requires further evaluation
Page 51

Ultrasound in AUB
• Initial screening to determine if biopsy is necessary• Correlate biopsy findings with ultrasound
findings
• Identify intracavitary lesions• Planning for surgical treatment
• Candidate for more intensive medical/hematologic evaluation
• Adnexal evaluation• Bladder evaluation
Evaluating AUB
Kadir et al. Fertil Steril 2005;84:1352-59.
References
1. ACOG Practice Bulleting. Diagnosis of Abnormal Uterine Bleeding in Reproductive-Aged Women. Number 128, July 2012
2. Indman PD, J Reprod Med 1995; 40: 545-548
3. Brown and Shwayder, AIUM Annual Meeting 2007
4. Ferrazzi et al. Am J Obstet Gynecol 2009;200:235e1-6.
5. Hileeto et al. World J Surg Onc 2005;3:8.
6. Perez-Medina et al. J Ultrasound Med 2002; 21: 125-28. Lasmar et al. J Minim Invasive Gynecol 2012;19(5):575-80.
7. Levens et al. Am J Obstet Gynecol 2009;200:537.e1-.e7.
8. Dueholm et al. Am J Obstet Gynecol 2002;186:409-15.
9. Parker WH. Am J Obstet Gynecol 2012;206(1):31-6.
10. Goldstein et al, Am J Obstet Gynecol 1997;177:102-108.
11. Breitkopf et al. Obstet Gynecol 2004;101:120-125.
12. Zorlu et al. Gynecol Obstet Invest 1994;38:272-275.
References
13. Stovall et al. Obstet Gynecol 1991;77:954-956.
14. Guido et al. J Reprod Med 1995; 40: 553-555.
15. Van den Bosch et al. Obstet Gynecol 1995;85:349-352.
16. Rodriguez, Yaqub, and King. Am J Obstet Gynecol 1993;168:55-59.
17. Pasqualotto et al. JAAGL 2000;7:201-209.
18. Gull et al. Am J Obstet Gynecol 2003;188:401-08.
19. Gupta et al. Acta Obstet Gynecol Scand 1996;75:475-479.
20. Bromley et al. J Ultrasound Med 2000;19:529-534.
21. Sakhal and Abuhamad. J Ultrasound Med 2012; 31:805-808.
22. Shwayder and Sakhal. J Minim Invasive Gynecol 2014;21: 362-376.
23. Kadir et al. Fertil Steril 2005;84:1352-59.
Thank You
Page 52

Beyond Diagnostics –Office Sterilization,
Ablation and Resection Amy Garcia, MD
AAGL/SRS Fellowship-Trained in MIG
Director, Center for Women’s Surgery
Clinical Assistant Professor, University of New MexicoDepartment of Obstetrics and Gynecology
Albuquerque, New Mexico
Disclosure
Consultant: Bayer Healthcare Corp., Boston Scientific Corp. Inc., Ethicon Women’s Health & Urology, Gynesonics, IOGYN, Karl Storz, Minerva Surgical
Speakers Bureau: Ethicon Endo-Surgery
Grants/Research: Hologic
Objectives
Review anesthetic protocol necessary for procedures in the office
Utilize an operative hysteroscope and operative instruments in the office
Discern operative hysteroscopy techniques for in-office procedures
Operative Office Hysteroscopy
Myomectomy Uterine Septoplasty Polypectomy Endometrial Ablation Sterilization Retrieval of IUD Other
In-Office Hysteroscopy--Why
Patient Comfort Patient Financial Burden Lessened
Office co-pay vs. outpatient co-pay/deductible Co-insurance, self-pay
Reduced Risk No general anesthesia EMB vs. D & C See and treat
Immediate Visual Affirmation Patient Convenience Physician Convenience
Injectable Local Anesthesics
Anesthetic ConcentrationOnset (min)
Duration (hours)
Maximal Dose (mg / kg)Maximum Dose
(mL /70 kg)
Lidocaine (Xylocaine®)
1%, 2% <2 1.5-24 mg/kg not to exceed 280 mg
28mL (1%); 14 mL (2%)
Mepivicaine(Carbocaine®)
1% 3-5 0.75-1.54 mg/kg not to exceed 280 mg
28 mL
Prilocaine (Citanest®)
1% <2 >17 mg/kg not to exceed 500 mg
50 mL
Lidocaine with Epinephrine
Lidocaine 0.5%, 1%, 2%Epinephrine1:100,000, 1:200,000
<2 2-6 7 mg/kg not to exceed 500 mg
100 mL (0.5%)50 mL (1%)25 mL (2%)
Bupivicaine (Marcaine®)
0.25% 5-8 2-42.5mg/kg not to exceed 175 mg
50 mL
Etidocaine (Duranest®)
0.25 , 1% 4-6 2-34 mg/kg not to exceed 300 mg
50 mL (0.5%)25 mL (1%)
Page 53

Topical Local Anesthetics
Anesthetic Formulation
Onset Duration Complications
0.5%, Tetracaine, 1:2,000 Epinephrine, 11.8% Cocaine (TAC®)
10-30 min Unknown Rare severe toxicity including seizures and sudden cardiac death
4% Lidocaine, 1:2,000 Epinephrine, 0.5% Tetracaine (LET®)
20-30 min Unknown No severe adverse reactions reported
2.5% Lidocaine, 2.5% Prilocaine (EMLA®)
1 hour 0.5 – 2 hours Contact dermatitis, methemoglobinemia(very rare)
4% Liposomal Lidocaine
0.5 hour 0.5 – 2+ hours No severe adverse reactions reported
Uterine Neuroanatomy
Courtesy Dr. Malcolm Munro
Uterine Neuroanatomy Endometrial Innervation
Uterine Local AnesthesiaSites to Consider
Vagina Topical
Cervix Intracervical Topical
Corpus Paracervical Topical
Courtesy Dr. Malcolm Munro
Pre-procedure Medicaiton
NSAID’s Ibuprofen 1 hour to 48 hours prior to procedure
Ketoralac 30 or 60 mg IM 30 min – 60 min prior to procedure
Narcotic – 1 hour prior
Anxiolytic – 1 hour prior
Consider Anti-nausea Medication – 1 hour prior
Post-Procedure Medication
NSAID Ibuprofen ATC x 24 hours
600 q 6 hrs
Narcotic q 6 hrs ATC x 24 hours
Alternate q 3 hrs with NSAID
Anti-nausea
Page 54

Consideration for IV Sedation
Reduces Anxiety Patient Physician
Reduces Patient Discomfort
Pre-emptive Local Anesthesia
Post-procedure Analgesia
Lengthens Recovery Time
Risk Factors for Polyps
Significance association Age Menopause HTN Obesity
Only AGE keeps statistical significance in univariable analysis
Endometrial Polyps and Hyperplasia
Increased risk of atypical hyperplasia in random directed biopsies
International Journal of Gynecological Pathology 28;522-528. 2010
©2012 All rights reserved. For internal distribution only. CC-3001 13JAN12F
Change Entry Angle
In-Office Endometrial Ablation
Gynesys HTA
HerOption
NovaSure
ThermaChoice
Documentation
Page 55

Reimbursement
In-Patient (21), Out-Patient (22), ASC (24)
58558 Hysteroscopy withPolypectomy, Biopsy, D & C
2014 RVUMedicare
CF 35.8228125%
CF 44.7785
7.75 $ 277.63 $ 347.03
Non-Facility/Office (11)
11.31 $ 405.16 $ 506.44
No Global
With E/M VisitModifier 25
Document HS Separately
2014Reimbursement
In-Patient (21), Out-Patient (22), ASC (24)
58562 Hysteroscopy withRemoval Foreign Body
2014 RVUMedicare
CF 35.8228125%
CF 44.7785
8.42 $ 301.63 $ 377.03
Non-Facility/Office (11)
11.72 $ 419.84 $ 524.80
No Global
With E/M VisitModifier 25
Document HS Separately
2014
Reimbursement
In-Patient (21), Out-Patient (22), ASC (24)
Hysteroscopy with Myomectomy58561
2014 RVUMedicare
CF 35.8228125%
CF 44.7785
15.92 $ 570.30 $ 712.87
Non-Facility/Office (11)
0 $ 0 $ 0
No Global2014
Page 56
Preparing for the Worst Case ScenarioAddressing Office Safety
Isabel Green
Johns Hopkins University
Nov, 2014
Disclosure
I have no financial relationships to disclose.
10/6/2014 2
What we least expect when we least expect it….
Preparing for the Worst Case Scenario
We will discuss….
• Transition from the OR: our crutch
• Emergencies & Management
• Safety in the Commonplace
• Protocols: Role and Execution
Office Emergencies
• The norm: no complications
• Estimated 5% complication rate for office procedures– Vasovagal episode
– Anaphylaxis
– Lidocaine toxicity
– Respiratory depression
– Hemorrhage Lutwak et al BMJ 2013Kaneshiro et al Cochrane Review 2012
Transition from the OR
Leaving the OR Behind…..•Anesthesia team
•Surgical nursing
•Monitors
•Resuscitation equipment
•Rapid responders
•The asleep patient
Page 57

Transition from the OR
Moving procedures creates unique challenges • Nurse and provider inexperience in
managing complications
• Absence of regulatory oversight and guidelines
Office Patient Safety Assessment. National Results Report. Spring 2012. American College of Obstetricians and Gynecologists.
Reaction
Recognition and Management
Accessed: http://www.myconfinedspace.com/
Reaction
• Recognize symptoms
• Call for help
• Initiate treatment
• Assess and reassess
• Monitor recovery VASOVAGAL
VasovagalRecognition
• Neural reflex: vagal tone vasodilation and self-limited hypotension, bradycardia
– Triggers: stress, noxious stimuli, fear
– Prodrome: nausea, pallor, diaphoresis, hyperventilation, visual disturbance
• Common in the young and healthyAiden et al World J Cardiology 2012
VasovagalManagement
• Restore circulation: Supine position, legs raised
• Smelling salts/ stimulation• +/- Volume repletion• +/- Oxygen • Serial vital signs until resolution
• Advanced support as needed (cardiac patient)
• Muscle tensing may help abort episodesCrediet et al Circulation 2002
Page 58

ANAPHYLAXIS
AnaphylaxisRecognition
• Severe allergic reaction/hypersensitivity, IgE
• Trigger rapid evolution then mild with spontaneous resolution or progressive
– Hives, flushing, itching, swollen lips/tongue*– Sensation of choking, stridor, wheezing,
shortness of breath, cough– Nausea, vomiting, abdominal pain– Tachycardia, hypotension, dizziness, syncope
AnaphylaxisManagement
Using epinephrine, halt progression to anaphylactic shock and support resolution
1st line
delay increases mortality risk
adjunct are just that, adjunct
AnaphylaxisManagement
• Remove/stop trigger
• Assess airway, circulation, mentation
• Call for help
• Administer IM epinephrine (1mg/1mL; 0.3 to 0.5)
• Recumbent position
• IV Fluids & Supplemental oxygen
• Reassess and monitor
LIDOCAINE TOXICITY
Lidocaine ToxicityRecognition
• Systemic toxicity due to idiosyncratic response, excessive dosing or intravascular admin– Metallic taste, ringing in ears, tingling lips,
seizures
– Bradycardia, AV Block, ventricular arrhythmias, vasodilation, cardiac arrest
Page 59
Lidocaine ToxicityManagement
• Prevention– Limit dose– Avoid intravascular injection– Educate the patient
• Stop the medication• Assess: vitals, cardiac monitor• Call for help• Support: supplemental oxygen, IV access • Initiate life support algorithm• Fat emulsion
WORST CASE SCENARIO IS RARE…..
Patient Safety Extends Beyond The Rare and Unlikely to the Routine
Accessed: http://siliconkarne.com/tag/europe/
Slices of Safety
Patient SelectionConsent
Procedural Timing – Luteal Phase PregnancyMedication storage and administration
Patient positioningEquipment maintenance and cleaning
Emergency Equipment Training and MaintenanceDocumentation
Patient Follow UpProvider PrivilegingProgram Evaluation
Medical Error
James Reason, 1991Accessed: http://patientsafetyed.duhs.duke.edu/
Protocols
1. Consider patient population & procedures2. Review state laws & hospital guidelines3. Outline procedure criteria & algorithms4. Determine availability of rapid responders5. Assess equipment6. Assign roles7. Build in mock codes8. Schedule life support training & recert
Making a Protocol Reality
Office procedures should have a component of preplanned responsiveness for emergencies
Weiss et al Clin Obstet Gynecol 2012
Page 60

Preplanned Responsiveness
Team simulation– Effective tool for education in life support &
medical emergency management
– Multi-disciplinary simulation effective in error reduction in OB emergencies
Ruesseler Postgrad Med J 2012Didwania J Grad Med Educ 2011
Merien Obstet Gynecol 2010Guise Jt Comm J Qual Patient Saf. 2010
How to Sim
• In the office = high fidelity
• Scheduled and unscheduled
• Observer role for evaluation
• Safe debrief– Review performance
– What worked well
– Identify deficiencies
– Address challenges
Practice Safety
Protocol Design
Simulation
Debrief & Evaluation
Troubleshoot
Safety Expectations in the Office
Patients have the right to expect the same level of safety regardless of where their procedure is performed….
Office Patient Safety Assessment. National Results Report. Spring 2012. American College of Obstetricians and Gynecologists.
Safety Expectations in the Office
Patients have the right to expect the same level of safety regardless of where their procedure is performed….
It is the responsibility of the provider to ensure that a culture of patient safety is ingrained in their office practice ….
Thank you
Page 61

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
Page 62


















