Diarrhea Julie Anne Ting. Objectives To review the common causes of acute diarrhea in childhood. To...
27
Diarrhea Julie Anne Ting
-
Upload
jonathan-goodwin -
Category
Documents
-
view
219 -
download
1
Transcript of Diarrhea Julie Anne Ting. Objectives To review the common causes of acute diarrhea in childhood. To...
DiarrheaJulie Anne Ting
ObjectivesTo review the common causes of acute diarrhea in childhood.
To review the current approach to outpatient management of acute diarrheal illness.
To review bloody diarrhea and its etiology.
To discuss the causes of chronic diarrhea.
Case
Julie is a 2 year-old girl seen in your office for a 4 day history of diarrhea. She initially had fever and 2 episodes of vomiting but this has since resolved. Her father has been giving her flat coke.
What else would you like to know?
Hx (1)
HPI
diarrhea: quantity and quality
associated GI symptoms: vomiting, abdominal pain, tenesmus, dysuria
constitutional symptoms
intake and output
travel history, sick contacts
Hx (2)
PMHx (incl. immunosuppressive illnesses, chronic diarrheal illness)
Family Hx (incl. IBD, celiac)
Rx (incl. recent Abx use)
Allergies (incl. food intolerances)
Immunizations (incl. Rotarix)
Red Flags on Hx
< 3m.o. with fever for >2d
<3m.o. with diarrhea for >2d
hematochezia or melena
bloody or green bilious vomit
diarrhea >10d
progressively worsening abdominal pain
lethargy, decreased urine output
What are important things not to miss on
P/E?
P/E
General appearance: toxic vs. non-toxic
Vitals
Growth parameters
Hydration status
Abdominal exam: bowel sounds, masses, tenderness, guarding, rebound, (DRE)
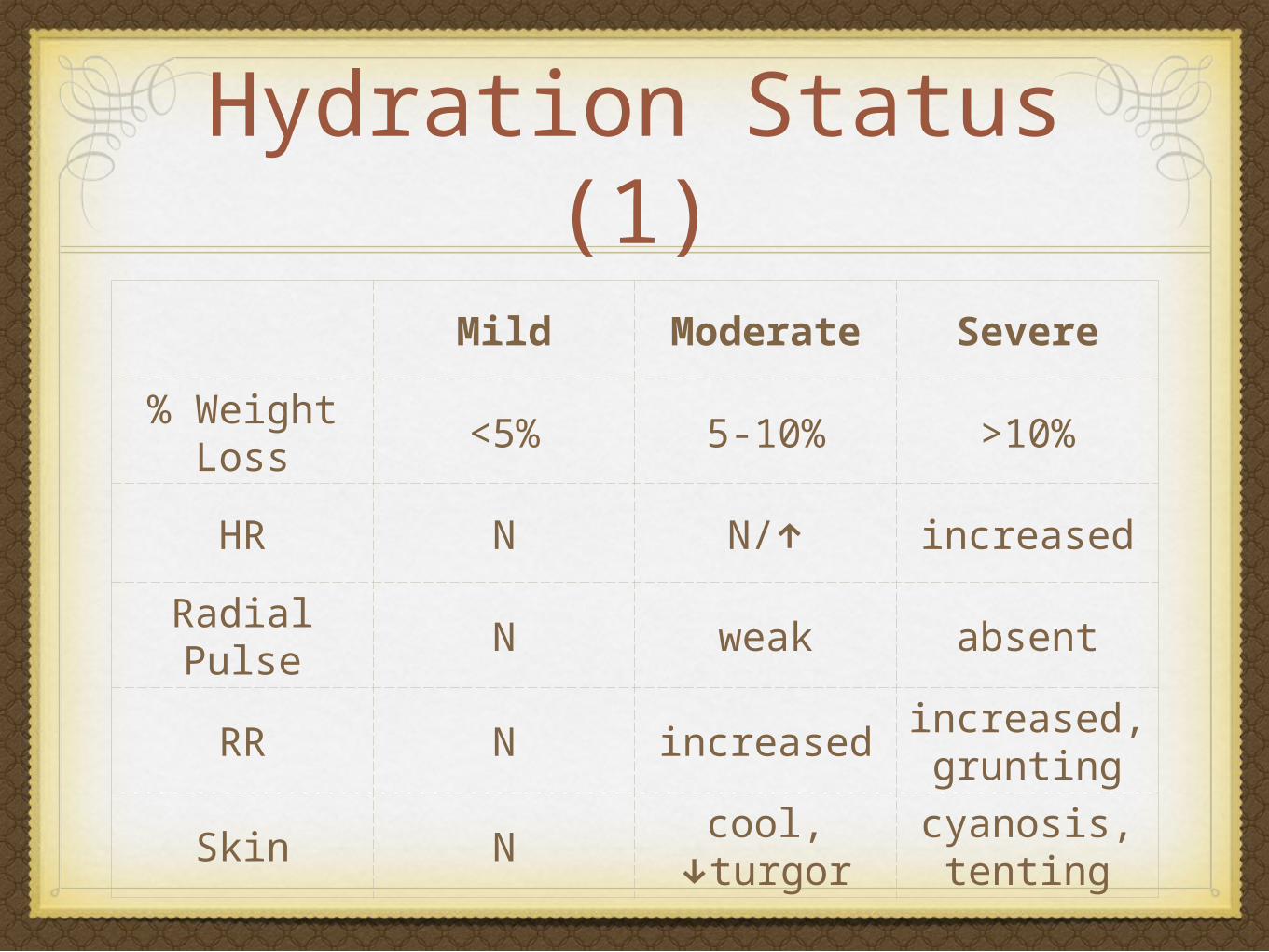
Hydration Status (1)
Mild Moderate Severe
% Weight Loss
<5% 5-10% >10%
HR N N/↑ increased
Radial Pulse N weak absent
RR N increasedincreased, grunting
Skin Ncool,
↓turgorcyanosis, tenting
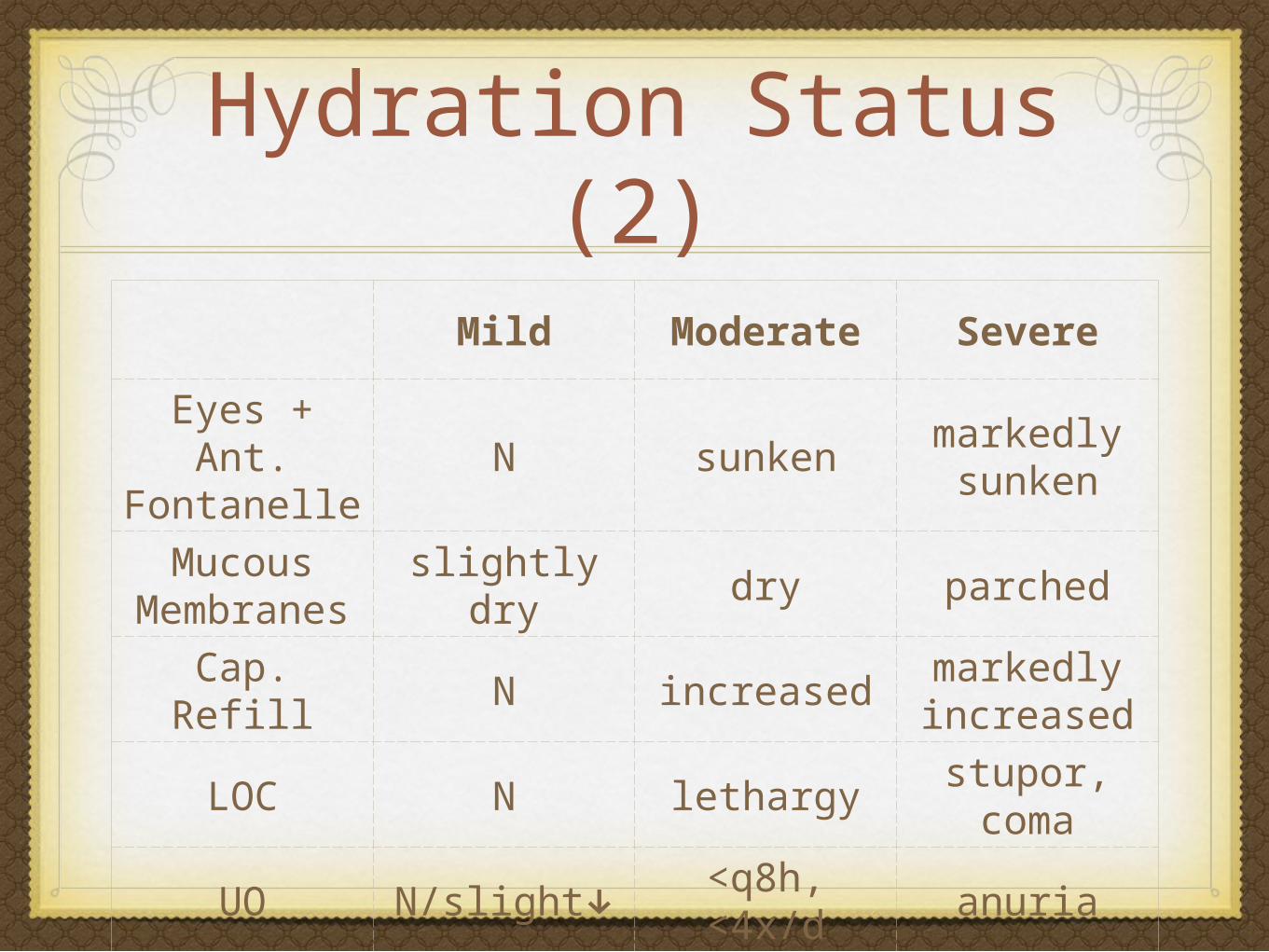
Hydration Status (2)
Mild Moderate Severe
Eyes + Ant. Fontanelle
N sunkenmarkedly sunken
Mucous Membranes
slightly dry dry parched
Cap. Refill N increasedmarkedly increased
LOC N lethargystupor, coma
UO N/slight↓ <q8h, <4x/d
anuria
Julie’s Story
Julie just returned from a family trip to the Caribbean. She has bloody diarrhea.
She has mild dehydration.
She has non-localizing abdominal pain. There are no signs of peritonitis.

What are possible causes of Julie’s diarrheal illness?
DDx Acute DiarrheaVery Common:
GI infection: virus (usu. non-bloody) > bacteria > parasite
Antibiotic-associated diarrhea
Very Life-Threatening
Systemic infection
Surgical abdomen: intussusception, appendicitis, toxic megacolon
Which of these investigations would you order for Julie?
CBC
BUN, Cr
electrolytes
stool C&S
stool O&P
C. difficile toxin screen
urinalysis
abdominal ultrasound
abdominal CT
Indications for Investigations
Cause other than gastroenteritis is suspected
Severe dehydration
Bloody diarrhea
How would you manage Julie’s
diarrhea?
Rx ChoicesRehydration: ORT (mild-mod) or IVF (severe)
Early refeeding: increases speed of bowel recovery
Antibiotics: consider if bloody diarrhea, systemic illness
Empiric Abx for bloody diarrhea: ciprofloxacin 20mg/kg/d div BID x 5d or ceftriaxone 50mg/kg/d (max 1.5g) x 5d
Zinc supplementation: a first-line Rx in developing countries
Probiotics: some evidence of benefit
Smectite: adsorbent
Oral Rehydration Therapy
Pedialyte (no juice, no pop, no salty chicken noodle soup, no cow’s milk, no plain water)
for mild-moderate (<10%) dehydration
not for patients with protracted vomiting, worsening diarrhea, stupor/coma, or intestinal ileus
Oral Rehydration Therapy
20mL/kg/h over the 1st hour,
then 10mL/kg/h for mild (<5%) dehydration and 15-50mL/kg/h for severe (5-10%) dehydration
reassess in 6-8h
(or if you’re at CHEO, follow the pre-printed handouts)
Does Julie need follow-up?
Hemolytic Uremic syndrome (HUS)
A potential complication of EHEC (esp. O157:H7), also Campylobacter, Shigella, and some viruses
usually starts 3 days after resolution of diarrhea
increased risk if <5y.o. and bloody diarrhea
warn parents to watch out for bruising, oliguria, neurological changes
Rx: dialysis prn
Summary: Approach to Acute Diarrhea
Hydration Status
mild to moderate volume loss (<10%): ORT
severe volume loss (>10%): admit for IVF resuscitation
Toxic vs. Non-Toxic
if suspect severe/systemic illness: cultures, Abx
if suspect surgical abdomen: imaging, consult surgery
Julie Says Thank You for saving
her!
Causes of Chronic Diarrhea
Chronic Diarrhea Without FTT
Toddler’s Diarrhea (Chronic Nonspecific Diarrhea)
cause: excess fluid intake, carbohydrate malabsorption, low dietary fat intake, disordered GI motility, excess fecal bile acids
Rx: 4Fs: fibre, normal fluid intake, 35-40% fat, D/C fruit juice
Infection
Lactose Intolerance
IBS
Chronic Diarrhea with FTT
Intestinal: celiac disease, milk protein allergy, IBD
Pancreatic: CF, Schwachman-Diamond Syndrome
Other: osmotic, endocrine, immunodeficiency, neoplastic, food allergy, laxative abuse








![Review Article ...downloads.hindawi.com/journals/jpr/2012/981424.pdf · patients with diarrhea [47–60], and in 4.6% of patients without diarrhea [55]. Also in developing countries,](https://static.fdocuments.in/doc/165x107/5f782745d395186fef31def1/review-article-patients-with-diarrhea-47a60-and-in-46-of-patients-without.jpg)









