
Diane Packard Presiding Presiding Secretary/Treasurer’s Report Kevin G. Cox...
91
2012 Business Meeting North Carolina Health Care Facilities Association Raleigh, NC
Transcript of Diane Packard Presiding Presiding Secretary/Treasurer’s Report Kevin G. Cox...

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Diane PackardPresiding

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Secretary/Treasurer’s Report
Kevin G. Cox

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Nominating Committee Report
Randy Uzzell

2012-2014 Slate of Officers
Chair Cheryl Clapp-Coleman Clapp’s Nursing CenterFirst Vice Chair Kevin Cox Autumn CorporationSecretary/Treasurer Phillip Hill Principle Long Term CareHospital Affiliated Vice Chair Renee Rizzuti Carolinas HealthCare SystemIndependent Owner Vice Chair Jim Martin Tullock Management Company
Multi-Facility Vice Chair John Barber White Oak Management, Inc.Non-Proprietary Vice Chair David Kidder Carolina Adventist Retirement SystemsNational Multi-Facility Vice Chair Steven Jones Kindred Transitional Care & Rehab-RaleighDistrict I Vice Chair Vickie Beaver Choice Health Management ServicesDistrict II Vice Chair Paul Babinski Liberty Healthcare Rehabilitation ServicesDistrict III Vice Chair Denise Clapp-Campbell Clapp's Convalescent Nursing HomeDistrict IV Vice Chair Gary Trullinger Sava Senior CareDistrict V Vice Chair Joan Garvey Liberty Healthcare Rehabilitation ServicesMember-at-Large Chris Bryson UHS-Pruitt CorporationMember-at-Large Mary Beth Turman Principle Long Term Care

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Report From Capitol Hill
Neil Pruitt

AHCA: “Forwarding our Commitment to Quality”
Neil Pruitt, Jr.AHCA Chair

Strategy 1 – Redefining the Consumer Experience
Quality as an expectation Focus on customer service
Strategy 2 – Becoming Part of the Solution New relationships with CMS Proactive political relationships
Strategy 3 – Thinking Differently New payment models Embrace the spectrum of services
AHCA Strategic Plan

Strategy 4 – Promoting Technology Re-launch LTC Trend TrackerSM on a new platform Enable members of all sizes to evaluate and adopt technology
that advances quality and promotes efficiencyStrategy 5 – Being Present
Member participation in grassroots Member participation in quality initiatives
AHCA Strategic Plan

AHCA Board of Governors endorsed establishing a new overarching Quality Cabinet
AHCA Quality Cabinet will coordinate and direct our collective efforts to advance quality of care and quality of life issues
Mary Ousley – former AHCA Chair and 2011 Friend of Quality awardee – will serve as Chair
Howie Groff – Former AHCA BOG Member and NCAL Chair – will serve as Vice Chair
AHCA’s Quality Cabinet will help to guide efforts of AHCA’s: Quality Improvement Committee Clinical Practice Committee Survey/Regulatory Committee Workforce Committee Consumer Experience
New AHCA Quality Cabinet

Strategy 1: Redefining the Consumer Experience
Compiled from opinions of 257,676 employees
Overall Consumer Satisfaction Overall Workforce Satisfaction
Compiled from opinions of 90,576
residents and 140,828 family members
Source: The 2010 National Survey of Consumer & Workforce Satisfaction in Nursing Homes conducted by My InnerView.

Since 2009, nursing facility health survey citations have been on a steady decline and have dropped nearly a full percentage point in two years
Strategy 1: Redefining the Consumer Experience
Every Medicare and Medicaid certified nursing facility in America must be surveyed once every 15 months

• Extends payroll tax cut and physician fee schedule until 12/31/12
• Therapy cap exceptions process continues until 12/31/12
• SNFs are a pay-for through a reduction of bad debt coverage− Dual eligibles reduced over three years
2013 at 88% 2014 at 76% 2015 at 65%
− Non-duals will be reduced this year from 70% to 65%
Conference Committee Action on Payroll Tax Cut and Doc Fix

• AHCA and its Finance Committee will work on budget neutral options to present to policymakers in an effort to limit the impact of the bad debt
• AHCA to produce state-by-state data for state affiliates to help them fend off additional cuts from Medicaid
• Any action will take place at the end of the year so Members of Congress will need to be educated on these options in advance
Bad Debt Opportunities

• Challenges− Reduce Medicare bad debt payments− Penalty for hospital readmissions− Threat to market basket− Lower provider tax rate− Blended FMAP rate formula
• Opportunities− Site neutral bill− AHCA’s hospital readmission proposal
President’s Budget

Some at CMS, on The Hill and most advocacy groups view the sector as an obstacle to improving quality
Strategy 2: Becoming Part of the Solution
CMS has rejected our notion that we are the cost and quality solution: “analysis of recent quality measure data related to
rehospitalizations, for example, which appears in the March 2011 Report to Congress suggests that quality of care within SNFs has not been improving….We (CMS) do not agree …that shifting patients…to a SNF setting is necessarily more beneficial to the patient…” (SNF PPS Final Rule, August 2011).

Proving our commitment to improving quality demands that we have better ways to measure our progress
Developing better outcome measures that can validate our claims and document our quality efforts is essential
AHCA will lead the quality issue by adopting significant quality efforts and programs
Strategy 2: Becoming Part of the Solution

Beginning in fiscal year 2012, CMS will rank hospitals based on 30-day readmission rate for the top three diagnoses causing the majority of readmissions:
Heart attack Heart failure Pneumonia
Source: Sections 1151 and 3025 of the Patient Protection and Affordable Care Act
Hospitals that fail to meet CMS’ rehospitalization standards will have a percentage of total Medicare payments withheld:
2013: up to 1% 2014: up to 2% 2015: up to 3%
Strategy 3: Thinking Differently
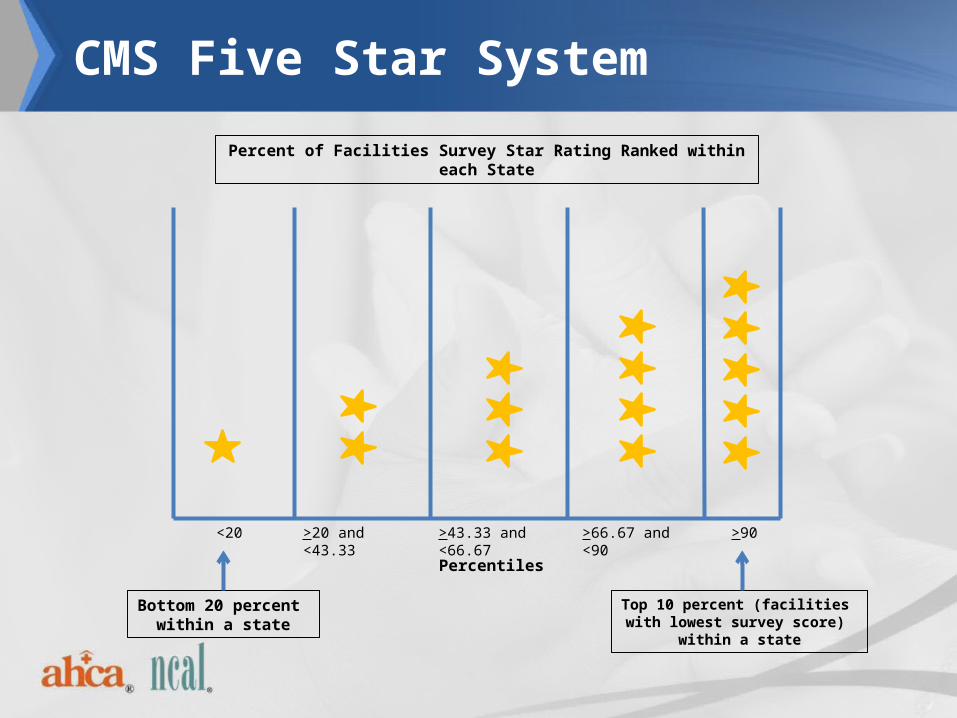
Percent of Facilities Survey Star Rating Ranked within each State
Top 10 percent (facilities with lowest survey score)
within a state
Bottom 20 percent within a state
>90>66.67 and <90>43.33 and <66.67>20 and <43.33<20
Percentiles
CMS Five Star System

Proposed recommendations to revise Five Star rating system Expand domains of measures used
Hospitalization Rehab Satisfaction
Expand measures within existing domain Add turnover and retention
Change weights for each domain
Use targets/benchmarks to assign star rating rather than percentile ranking
AHCA Proposed Five Star

LTC Trend Tracker provides members with the ability to benchmark their quality, clinical and financial data
Domains - Staffing, Rehospitalization, Survey Findings, Medicare Cost Report, Medicare Utilization, Retention and Turnover, Resident Characteristics, Five Star Ratings, Five Star Staffing
Participants – 581 organizations; 4,061 facilitiesUtilization – 1,300 reports per month (Jan. through
Aug. 2011) up from 800 reports per month in 2010
Strategy 4: Promoting Technology

LTC Trend Tracker Growth Multi and Single Organizations 2010 – 2011
Multi Single Total0
100
200
300
400
500
600
700
175213
388
235
346
581
20102011

AHCA Board of Governors Adopted Three Quality Principles:
I. Improvement in four clinical measures which are meaningful, measurable,
and moveable:
1. 30-Day Hospital Readmission
2. Customer Satisfaction (Post-Acute and LTC)
3. Staff Turnover
4. Antipsychotic Rx Reduction
II. Development of a Therapy Outcome Measurement System
III. Promote Proactive Payment Models (January retreat)
AHCA will not be successful without the full support of our
members
Strategy 5: Being Present

October 2011 Public Education
MOTION: To formally replace the term “nursing home” with “skilled nursing care,” augmented by centers where appropriate, to describe our profession.

Breaking the Nursing Home Paradigm

State-of-the-Art Rehab Suite
Aquatic Therapy Pool

Private Suites

Restaurant-StyleDining Rooms
Sitting Rooms

Spa
Movie Theater

Coffee Shop
Internet Cafe

“The system should not overpay for certain patients, which creates incentives for nursing homes to spiff up their buildings and set staffing levels to entice profitable patients. I encourage CMS to continue taking steps to address these issues.”
- Stark
Breaking The “Nursing Home” Paradigm

Thank You!

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
CON Construction Rules
Kristi Huff

Certificate of Need• House Select Committee on Certificate Of Need Process and Related
Hospital Issues• Committee Charge:
– To study House Bill 743 and House Bill 812;– The legal requirements and process governing DHHS determinations on
applications for CON including an analysis of exceptions granted under policy AC-3;– Issues related to publicly owned hospitals including the appropriate role of State-
owned hospitals;– Whether a hospital operating under a Certificate of Public Advantage (COPA)
should be required to comply with the same rules, policies and limitations to each county in which it operates;
– The extent to which a publicly owned hospital should engage in business with an entity having a COPA or operating under an exemption under the CON laws of the state;
– Any other matter reasonably related to the above.

Certificate of Need (continued)
• 3 public hearings across the state: Fletcher, Mt. Holly, and Wilmington
• Topics of discussion include:– Appeals process– Raising monetary thresholds in the law for diagnostic
centers, major medical equipment, renovations, expedited reviews
– SHCC Appointments made by Governor and legislature– Whether State Ethics Act should apply to the SHCC– Transparency in the CON process


Construction Rules Review
• Governor’s Executive Order 70: identify rules that are burdensome, duplicative, or impose unnecessary costs
• Nursing Home Physical Plan Rules review – meeting with Construction Section and DHSR leadership
Construction Rules Review (continued)
• Areas likely to be changed:– Exempt certain small projects from a plan review
(and fee)– Eliminate references to a “nurse’s station” or
nursing unit in the rule– Bath/shower rooms – for every 120 beds– Soiled utility/soiled linen rooms– Handrails – maximum opening between handrails
of 12 feet

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Payment For Services
John BarberSam Clark

What’s Up With Our Medicaid Rates?
• There has been some confusion and uncertainty surrounding nursing home rates.
• The state is currently working on a State Plan Amendment that will address multiple rate changes.
• NCHCFA will review the SPA before it is sent to CMS for approval.

What’s Up With Our Medicaid Rates?
Provider Assessment Increase• The provider assessment, currently assessed at an
overall rate of approximately 5.5%, will be increased to 6%.
• The increase will be approximately $1 per non-Medicare day.
• The effective date of this change will be January 1, 2012.
• Medicaid rates will be increased to repay the provider the Medicaid portion of the assessment.

What’s Up With Our Medicaid Rates?
Case-Mix Adjustments • The frozen case-mix will be unfrozen and the rates
effective April 1, 2012 will be adjusted for acuity using the December 31, 2011 snapshot date.
• Quarterly CMI adjustments will resume beginning on July 1, 2012.

What’s Up With Our Medicaid Rates?
Rate Reduction• The current 3.51% rate reduction will be adjusted to
an amount needed to achieve a 2.17% average reduction for the state fiscal year (July 1, 2011-June 30,2012).
• This will be effective January 1, 2012.• The rate reduction will be adjusted again effective
July 1, 2012 to ensure that the annual reduction in SFY 2013 will be 2.17% plus the impact of any other adjustments approved by the legislature.

Fair Rental Value
• Aging of facilities• April Updates
– Cost per square foot $142 increased to $147– Most location factors will increase

Medicare Bad Debt• The final agreement on Medicare "doc fix" legislation will
reduce Medicare reimbursement for uncollectible bad debt, but not as much as in the bill originally passed by the House last fall.
• Section 3201 - Reducing Bad Debt Payments – This provision would phase down the bad debt reimbursements to 65 percent beginning in FY2013 for providers who are currently being reimbursed at 70 percent, while phasing in the reduction to 65 percent over three years for those who are reimbursed at 100 percent of their bad debt. (88%, 76%, 65%)
• Effective for cost reports beginning on or after 10/1/12.• The legislation also extends the therapy caps exceptions
process through December 31, 2012.

National Issues
• Mike Cheek with AHCA will be addressing more of the national issues during the Tuesday morning session.

HMS Credit Balance Reviews
• HMS has completed their first round of reviews.• Most of the findings have involved
– Resident monthly liability in the month moving from Medicare to Medicaid
– Medicare Part C Co-insurance paid by Medicaid for dual eligible residents
• NCHCFA recently met with the State and HMS on the outstanding issues.
• HMS is getting ready to start round two.

Medicaid RACs
• Medicare RACs have been around for several years, but have been concentrating on hospital issues.
• States are required to contract with Medicaid RACs.
• NC is preparing an RFP.• Can’t review items that have already been
reviewed.

Cost Report Audits and the MDS Reviews
• The audits of the 2009 cost reports have been called off.
• The MDS reviews continue.– MDS reviews of snapshot dates not used for setting rates
are purely educational. Rates are not adjusted.– After the M&S audit was completed, they choose multiple
REHAB RUGs from the CMI report, asked to see the Start of therapy, END of therapy dates and the log showing they were treated. These are strictly information gathering audits that DMA has asked them to do. It is not reflected on the report she gives to center and she says she has no idea of what the purpose of the audits are. She has just been told to gather the data.

Medicaid Cost Report Transition
• The Medicaid cost report as you have known it is no more.
• NCHCFA and other interested parties are currently working with DMA.
• Moving forward, nursing homes will– Use the Medicare cost report, 9/30 year end not required– File supplemental schedules to account for certain
Medicaid specific items– More information to come

Ask-the-Contractor Teleconference
Palmetto GBA had to cancel the February 9, 2012, J11 Part A Ask-the-Contractor Teleconference (ACT). The rescheduled date and time for this ACT is Wednesday, February 22, 2012, from 2 p.m. to 3 p.m. ET.
Conference Call Information • Teleconference Number: (866) 449-7848 • Confirmation Code: 52721579

Keeping Up-to-Date
• Providers should be receiving electronic notices from CMS, Palmetto GBA and Medicaid electronically.
• Our weekly newsletter, UPDATE, in the next several issues will list how to sign up for these important items.

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
President’s Report
J. Craig Souza

2012 Convention & Trade Show
Trade Show SOLD OUT for30th Consecutive Year
“Thank You TRADE MEMBERS!”

2011 Full Registrations 402
2012 Full Registrations 345

Future Meetings
2012 Mid-Year MeetingAugust 14-17, 2012Marriott Grande DunesMyrtle Beach, SC
2013 Mid-Year MeetingAugust 6-9, 2013Marriott Grande DunesMyrtle Beach, SC
2013 Convention and Trade ShowFebruary 10-13, 2013Greensboro, NC
2014 Convention and Trade ShowFebruary 23-26, 2014Greensboro, NC

• Conducted and published by the Department of Social & Behavioral Sciences at the University of California San Francisco.
• Released in October, 2011– Offers calendar year data of the following:
• Facility characteristics• Resident characteristics • Nurse staffing (RNs, LVNs, and NAs) hours per resident day.• Data on facility deficiencies based on state surveyor evaluations.
Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2005-2010

• North Carolina skilled nursing facilities champion quality improvement and have instituted best practices that are working to transform the health care system for the frail and elderly.
• This report reflects that as the level of resident need increases and nursing home residents become more medically complex. North Carolina continues to provide the highest level of care and is scoring better than the national average in almost every category.
Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2005-2010

• AVERAGE SUMMARY SCORE FOR RESIDENT ACUITY USING THE MANAGEMENT MINUTE INDEX
• North Carolina scores decreased from 116.70 in 2005 to 104.46 in 2010 but have consistently remained above the national average. In 2010, the Average Acuity Score for an NC resident was 12.84 points above the national average.
RESIDENT CHARACTERISTICS
2005 2006 2007 2008 2009 2010NC 116.70 114.90 114.90 111.16 107.46 104.46US 102.20 101.60 101.30 99.91 96.74 91.62

FINDINGS - DEFICIENCIES FROM QUALITY OF CARE EVALUATION
FACILITY DEFICIENCIES FROM STATE SURVEYS
2005 2006 2007 2008 2009 2010PERCENT OF FACILITIES WITH NO DEFICIENCIES
79 percent increase.
NC 6.34 6.60 8.21 14.66 14.75 11.35US 5.51 6.03 6.24 6.86 6.63 6.11
PERCENT OF FACILITIES RECEIVING A DEFICIENCY FOR ACTUAL HARM OR JEOPARDY OF RESIDENTS
25 percent decline.
NC 25.61 25.47 20.77 17.07 17.56 19.15US 25.97 27.70 26.57 25.68 24.67 23.36

Percent of Facilities with Deficiencies
FACILITY DEFICIENCIES FROM STATE SURVEYS
2009 2010PHYSICAL RESTRAINTS 60 percent decline from 2005.
NC 8.67 2.84US 10.78 8.79
DIGNITY 29 percent decline from 2005.NC 13.82 13.00US 20.35 20.23
HOUSEKEEPING 39 percent decline from 2005NC 9.60 11.35US 21.15 19.69
SUFFICIENT NURSING STAFF NC 0.47 0.00US 2.84 2.89
PRESSURE SORES 10.21 percent below national average.NC 10.07 9.22US 21.16 19.43
ACCIDENT ENVIRONMENT 19.31 percent below national average.NC 24.59 23.40US 45.43 42.71

Average Full Time Equivalents/HPPD –Staff (12/2011)
USFTE HPPD
NCFTE HPPD
RN 7.43 0.41 7.35 0.40
LPN 14.94 0.83 15.53 0.85
NA 44.32 2.42 43.13 2.42
Total 66.13 3.66 67.20 3.67

Government Performance Results ActRestraints %
Year - NC / Region / Nation2003 – 9.4 9.4 7.7
2011 - 2.5 3.4 2.7Change rate in % 73.4 63.8 64.9

GPRAPressure Ulcers - %
Year NC / Region / Nation2003 – 10.1 9.4 8.9
2011 - 8.4 7.8 7.4ChangeRate% 16.8 17.0 16.9
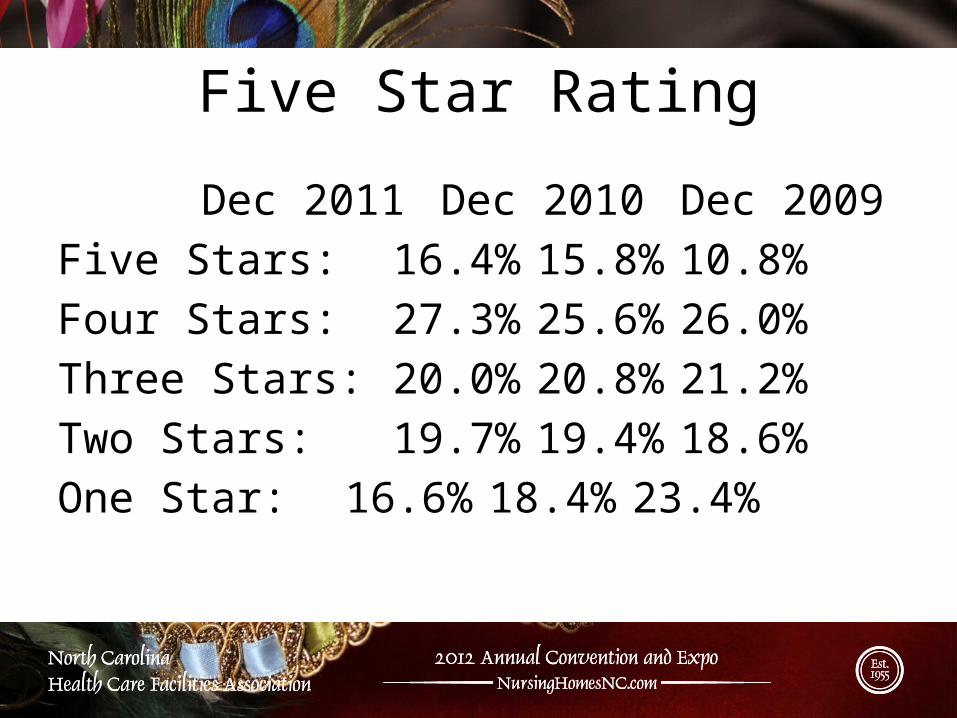
Five Star Rating
Dec 2011 Dec 2010 Dec 2009Five Stars: 16.4% 15.8% 10.8%Four Stars: 27.3% 25.6% 26.0%Three Stars: 20.0% 20.8% 21.2%Two Stars: 19.7% 19.4% 18.6%One Star: 16.6% 18.4% 23.4%


P R E S I D E N T ‘S 2013 BUDGETSkilled Nursing Provisions
“Reduce Medicare Coverage of Bad Debts”…would reduce bad debt payment to 25% for all eligible providers beginning in 2013. Savings: $36 billion over 10 years. “Phase Down the Medicaid Provider Tax Threshold Beginning in 2015”…proposes to limit taxes on health care providers to help finance the State share of Medicaid program costs by phasing down provider tax threshold from 6% to 3.5% beginning in 2014. Savings: $21.8 billion over 10 years. “Apply a Single Blended Matching Rate to Medicaid and CHIP Starting in 2017” …Proposes to replace current FMAP formula with a single matching rate specific to each State that automatically increases if a recession forces enrollment and State costs to rise beginning in 2017. This would result in the State’s share of Medicaid to increase and the federal share to decrease. Savings: $17.9 billion.

P R E S I D E N T ‘S 2013 BUDGETSkilled Nursing Provisions
“Encourage Efficient Post-Acute Care” ….gradually realign payments with costs through adjustments to payment rate updates in 2013 through 2022. Savings: $10.16 billion savings by 2017, $56.67 billion over 10 years. “Adjusting SNF Payments to Reduce Unnecessary Hospital Readmissions”…..reduces SNF payments by up to 3% beginning in 2016 for facilities with high rates hospital readmissions. Savings: $1.95 billion by 2022; $460 million by 2017. “Strengthen the Independent Payment Advisory Board (IPAB) to Reduce Long-Term Drivers of Medicare Cost Growth”

HOUSE AND SENATE REACH AGREEMENT ON PAYROLL TAX CUT & SGR
Skilled Nursing Provisions 1. Section 3005 –Outpatient Therapy Caps - (summary)
Extends the therapy cap exceptions process through December, 31, 2012.Adds requirements for physician review of the therapy care plan.Spending caps ($1,880 in 2012) would be extended to hospital outpatient departments.HHS is to collect data to assist in reforming payments for therapy services.MedPAC to recommend improvements to outpatient benefit to reflect the individual needs of patients.
2. Section 3201 –Reducing Bad Debt Payments – (summary)
Phase down bad debt reimbursements from 100% for dual eligibles to 65% beginning in 2013. Reduction of 12% in 2013, 12% in 2014 and 11% in 2015.

NC General Assembly


Jun-03 Jun-04 Jun-05 Jun-06 Jun-07 Jun-08 Jun-09 Jun-10 Jun-11 Jun-120.8500
0.9000
0.9500
1.0000
1.0500
1.1000
6/30/03 through 9/30/11
Med
icai
d C
ase-
Mix
Ind
ex
June 2003 CMI .94September 2011 CMI 1.07
Medicaid Day Weighted CMI
Not used for rates

MDS Reviews
2004-5, 40% 2005-6, 40% 2006-7, 35% 2007-8, 25% 2008-9, 25% 2009-10, 25% 2010-11, 25%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
77%
29%
13%18%
14%11% 10%
% of Facilities Over Adjustment Threshold(facilities subject to rate adjustment)
Review Period and Corresponding Re-RUG Threshold
% o
f Rev
iew
s Ove
r the
Uns
uppo
rted
Thr
esho
ld 2004-5 was the first year of the review process. These reviews were educational in nature and no rates were adjusted.

Average Occupancy
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
US 0.875 0.866 0.867 0.865 0.709 0.851 0.853 0.849 0.834 0.834 0.834
NC 0.917 0.901 0.905 0.892 0.895 0.892 0.888 0.887 0.88 0.871 0.867
53%
57%
63%
68%
73%
78%
83%
88%
93%

Average Medicaid Rate Graph
10/1/2
006
1/1/2
007
4/1/2
007
7/1/2
007
10/1/2
007
1/1/2
008
4/1/2
008
7/1/2
008
10/1/2
008
1/1/2
009
4/1/2
009
7/1/2
009
10/1/2
009
11/1/2
009
1/1/2
010
4/1/2
010
7/1/2
010
10/1/2
010
1/1/2
011
4/1/2
011
7/1/2
011
10/1/2
011
1/1/2
012 (est)
$100
$110
$120
$130
$140
$150
$160
$170
135.28 137.88 139.06
147.84 149.22
156.51 156.90 159.88
155.11
158.85
3.51% reduction7/1/11
2.3% increase1/1/11Rebasing
1/1/08 and 10/1/08
FRV Implemented1/1/2007

Average NC Medicare Rate
Oct-09
Nov-09
Dec-09
Jan-10
Feb-10
Mar-10
Apr-10
May-10
Jun-10Jul-1
0
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11Jul-1
1
Aug-11
Sep-11
Oct-11
Nov-11
$300
$350
$400
$450
$500
$550
417.87
469.22
483.85
424.82

Medicare Average LOS
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
US 38.11 37.2 38.06 38.16 38.09 37.69 37.87 37.86 37.1 37.23 36.89
NC 44.32 44.26 44.15 45.77 44.87 43.36 42.41 41.06 38.01 40.66 39.79
27.5
32.5
37.5
42.5
47.5
Days
NC Continues to have a higher Medicare length of stay than the US.

Medicare Utilization
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
US 0.083 0.091 0.102 0.111 0.119 0.126 0.13 0.131 0.135 0.136 0.137
NC 0.099 0.108 0.119 0.13 0.134 0.142 0.141 0.143 0.144 0.145 0.149
1%
3%
5%
7%
9%
11%
13%
15%
Med
icare
Per
cent
age
NC Continues to have a higherMedicare utilization than the US.

New Faces in State GovernmentAfter November Election**
• New Governor • New Lieutenant Governor• New Secretary of DHHS• 3 New U.S. House Members
– Reps. Myrick, Miller and Shuler not running• 8 New N.C. Senate Members• 28 New N.C. House Members
**As of February 16, 2012

General Assembly Outlook, 2012-2013Issues on the Horizon
• Medicaid Budget• Managed Care• Certificate of Need Changes (Appeals,
Composition of SHCC, Thresholds)• Mental Health Care• Health Benefits Exchange

Have You Contributed to the PAC?


TOP PACs in N.C. 2009-2010 Election Cycle1. NC ADVOCATES FOR JUSTICE PAC (Trial Lawyers) $530,4002. NC MEDICAL SOCIETY $355,0003. PROGRESS ENERGY EMPLOYEES CAROLINAS PAC $344,5004. BANK OF AMERICA PAC $339,2005. NATIONWIDE CAROLINA POLITICAL PARTICIPATION FUND $302,0006. NC FARM BUREAU PAC $294,5507. NC REALTORS PAC $294,5008. NC HOSPITAL ASSOCIATION $277,2509. EASTERN BAND OF CHEROKEE INDIANS $272,50010. DUKE ENERGY CORPORATION PAC $246,500…..31. NC HEALTH CARE FACILITIES PAC (NCHCFA) $98,500

Who Is FutureCare?
A statewide non-profit leader in
focusing on technology,
innovation and best practices in long-term
care.
FutureCare of North Carolina is a
subsidiary non-profit of the North Carolina Health Care Facilities
Association.

Chris BrysonUHS- Pruitt Corporation
Ken Burgess, ChairPoyner Spruill
Gerald P. CoxAutumn Corporation
Dr. Gordon DeFrieseFormer President and CEO of FutureCare
Cheryl GeddieHaymount Rehabilitation and Nursing Center
Dr. Laura GeraldNC State Health Director
Ted GoinsLutheran Services for the Aging
Polly JohnsonNorth Carolina Foundation for Nursing Excellence
Deborah LekanDuke School of Nursing
Dr. Darlyne MenscerCarolinas Healthcare System
Diane PackardRehab and Health Care Village Green
William A. PullyNC Hospital Association
Robert SeligsonNC Medical Society
Randy UzzellBritthaven
J. Bradley WilsonBCBSNC
Jeff WilsonLong Term Care Management Services
J. Craig Souza, Vice ChairNCHCFA
Samuel Clark, Secretary-TreasurerNCHCFA
Polly Godwin WelshNCHCFA
FutureCare of North Carolina Board of Directors

FutureCare Staff
Cameron GrahamExecutive Director
Mandy RichardsProgram Director
Contact Information Cameron Graham
FutureCare of North Carolina
Mailing Address5109 Bur Oak Circle
Raleigh, North Carolina 27612919.782.3827

Mission
Our mission is to improve the quality of long-term care for all North Carolinians for the elderly
and disabled, with a special focus on skilled nursing care.
Future Care of North Carolina seeks to achieve its goals by
bringing together leaders from across the state from within the
long-term care field: researchers, health care foundations,
policymakers, quality improvement organizations, and
corporations.
In order to achieve this mission, we need your INPUT and SUPPORT!

Goals
• Develop nursing staff to expert level in order to reduce unnecessary emergency room and hospital admissions
• Prepare potential residents and family members to access quality and innovative care
• Increase access to technology and innovative solutions in long-term care
• Educate the citizens of North Carolina (and lead the nation) on best practices in long-term care

Current Programs
1. Medication Error Management Training for Skilled Nursing Staff Using a High-Fidelity Mannequin Simulator
2. Mouth Care Training for Skilled Nursing Staff

NORTH CAROLINA HEALTH CARE FACILITIES ASSOCIATION
AHCA’s Public Education & Communication Campaign

2012 Business MeetingNorth Carolina Health Care Facilities Association
Raleigh, NC
Chair’s Report
Diane Packard


















