
Diagnostic_Dossier_December_2014_HE
4
54 | December 2014 Healthcare EXECUTIVE W orldwide sepsis is a major cause of morbidity and mortality. The ACCP/SCCM defined sepsis as systemic inflammatory response caused by infection. In simple words, “sepsis arises when the body’s response to an infection damages its own tissues and organs.” It can lead to complications like shock, multi-organ failure, and death, particularly if not identified early. Mortality occurs in one-third to one-half of all sepsis patients. In developing countries, sepsis accounts for 60-80 percent of all deaths. Every few seconds, someone in the world dies of sepsis. Sepsis is a consequence of infection that is difficult to predict, diagnose, and treat. Patients who develop sepsis have an increased risk of complications and death and face higher healthcare costs with longer treatment. Challenges in Diagnosis of Sepsis However, the major challenge remains as how to prove that there is infection? Culture best identifies it but in only about 30 percent of patients with sepsis. Moreover, false positivity of cultures further complicates the situation. Clinical signs of sepsis, such as fever, tachycardia, and leucocytosis, are DIAGNOSTIC DOSSIER Procalcitonin in Sepsis: Utility or Futility? Procalcitonin (PCT) is an extensively well studied and sensitive sepsis biomarker, efficient in guiding clinicians with antibiotic decision, writes Dr. Sutirtha Chakraborty Figure 1 Available evidence concerning PCT in different infections derived from observational and randomized-controlled intervention studies (Ref: Scheutz et al. BMC Medicine 2011) non-specific and overlap with signs of systemic inflammatory response syndromes (SIRS) of non-infectious origin making detection of sepsis a clinical challenge. Thus, delay in diagnosis and treatment of sepsis is responsible for increased mortality. Clinical utility of Procalcitonin To prove the presence of bacterial infection, serum biomarkers like Procalcitonin (PCT) are considered useful. It is the prohormone of calcitonin, released into the circulation of patients in response to bacterial infection. PCT is an extensively well studied sepsis biomarker for clinical use. A major advantage of PCT compared to other biomarkers, is its early and rapid increase in response to bacterial infections and sepsis. Among all sepsis markers, only PCT has achieved universal use throughout developed Europe in the last decade. High PCT concentrations are commonly found in bacterial infection, in contrast to much lower levels in viral infection. PCT levels also show a trend with the clinical severity of sepsis, severe sepsis and septic shock. Although PCT is virtually undetectable (less than 0.1 ng/ml) in healthy individuals, elevated serum PCT concentrations are not always specific for bacterial sepsis. Many studies have linked elevated PCT to SIRS, localized bacterial infection, autoimmune disease, burns, severe trauma, surgery, pancreatitis, as well as viral, parasitic, and fungal infections. In spite of these challenges, PCT has some other obvious clinical advantages like: 1) Improved accuracy of early clinical sepsis diagnosis 2) Can be used to assess the effectiveness of sepsis treatment
-
Upload
drsutirtha-chakrabortymdfacb -
Category
Documents
-
view
128 -
download
1
Transcript of Diagnostic_Dossier_December_2014_HE
54 | December 2014 Healthcare EXECUTIVE
Worldwide sepsis is a major cause of morbidity and
mortality. The ACCP/SCCM defined sepsis as systemic inflammatory response caused by infection. In simple words, “sepsis arises when the body’s response to an infection damages its own tissues and organs.” It can lead to complications like shock, multi-organ failure, and death, particularly if not identified early. Mortality occurs in one-third to one-half of all sepsis patients. In developing countries, sepsis accounts for 60-80 percent of all deaths. Every few seconds, someone in the world dies of sepsis.
Sepsis is a consequence of infection that is difficult to predict, diagnose, and treat. Patients who develop sepsis have an increased risk of complications and death and face higher healthcare costs with longer treatment.
Challenges in Diagnosis of Sepsis
However, the major challenge remains as how to prove that there is infection? Culture best identifies it but in only about 30 percent of patients with sepsis. Moreover, false positivity of cultures further complicates the situation. Clinical signs of sepsis, such as fever, tachycardia, and leucocytosis, are
DIAGNOSTIC DOSSIER
Procalcitonin in Sepsis:Utility or Futility?
With Dr. Lisha Ruparel
Procalcitonin (PCT) is an extensively well studied and sensitive sepsis biomarker, efficient in guiding clinicians with antibiotic decision, writes Dr. Sutirtha Chakraborty
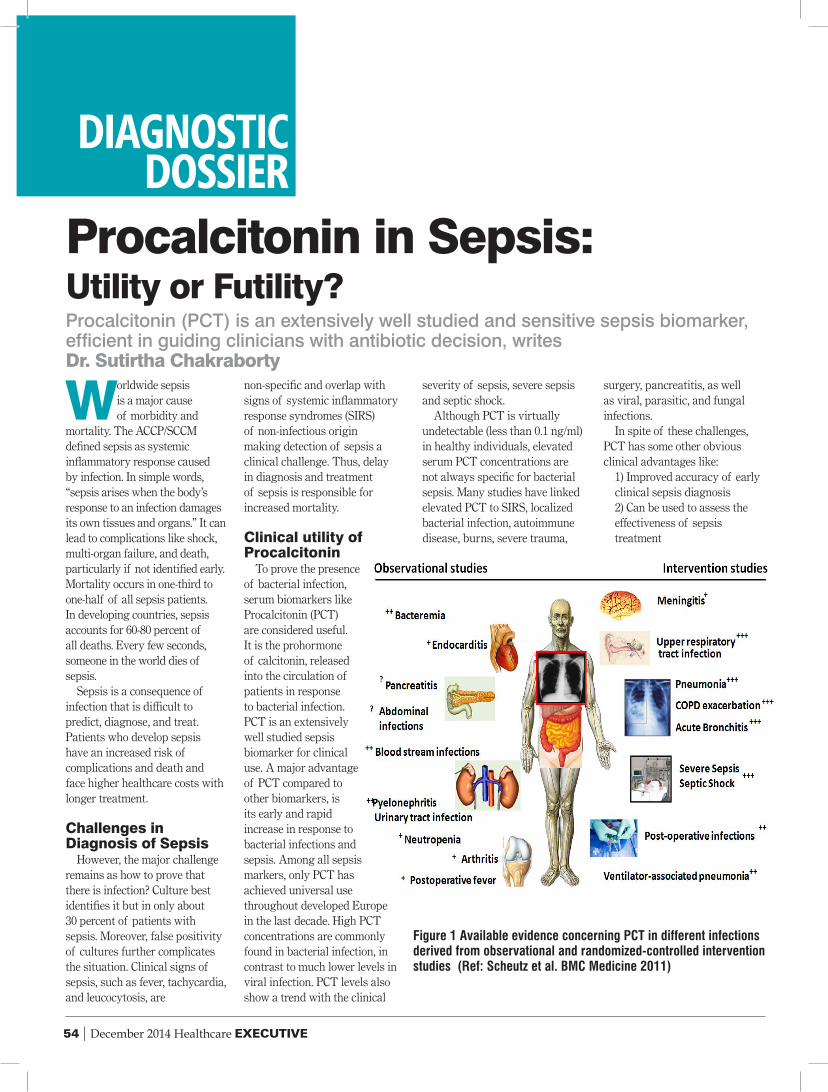
Figure 1 Available evidence concerning PCT in different infections derived from observational and randomized-controlled intervention studies (Ref: Scheutz et al. BMC Medicine 2011)
non-specific and overlap with signs of systemic inflammatory response syndromes (SIRS) of non-infectious origin making detection of sepsis a clinical challenge. Thus, delay in diagnosis and treatment of sepsis is responsible for increased mortality.
Clinical utility of Procalcitonin
To prove the presence of bacterial infection, serum biomarkers like Procalcitonin (PCT) are considered useful. It is the prohormone of calcitonin, released into the circulation of patients in response to bacterial infection. PCT is an extensively well studied sepsis biomarker for clinical use. A major advantage of PCT compared to other biomarkers, is its early and rapid increase in response to bacterial infections and sepsis. Among all sepsis markers, only PCT has achieved universal use throughout developed Europe in the last decade. High PCT concentrations are commonly found in bacterial infection, in contrast to much lower levels in viral infection. PCT levels also show a trend with the clinical
severity of sepsis, severe sepsis and septic shock.
Although PCT is virtually undetectable (less than 0.1 ng/ml) in healthy individuals, elevated serum PCT concentrations are not always specific for bacterial sepsis. Many studies have linked elevated PCT to SIRS, localized bacterial infection, autoimmune disease, burns, severe trauma,
surgery, pancreatitis, as well as viral, parasitic, and fungal infections.
In spite of these challenges, PCT has some other obvious clinical advantages like:
1) Improved accuracy of early clinical sepsis diagnosis2) Can be used to assess the effectiveness of sepsis
treatment
Healthcare EXECUTIVE December 2014| 55
3) Role in antibiotic stewardship. For respiratory tract
infection in ICU patients with baterial sepsis and post-operative infections, randomized-controlled studies have shown the efficacy of using PCT algorithms to guide antibiotic decisions. PCT guided antibiotic therapy leads to significant reduction of the length of antibiotic therapy. However in order to judiciously use it for assessment of therapeutic effectiveness and antibiotic stewardship, serial measurements of PCT are needed. Surviving sepsis campaign: international guidelines (2012) suggest that PCT measurements can be used for the sepsis diagnosis and to discontinue antibiotic therapy
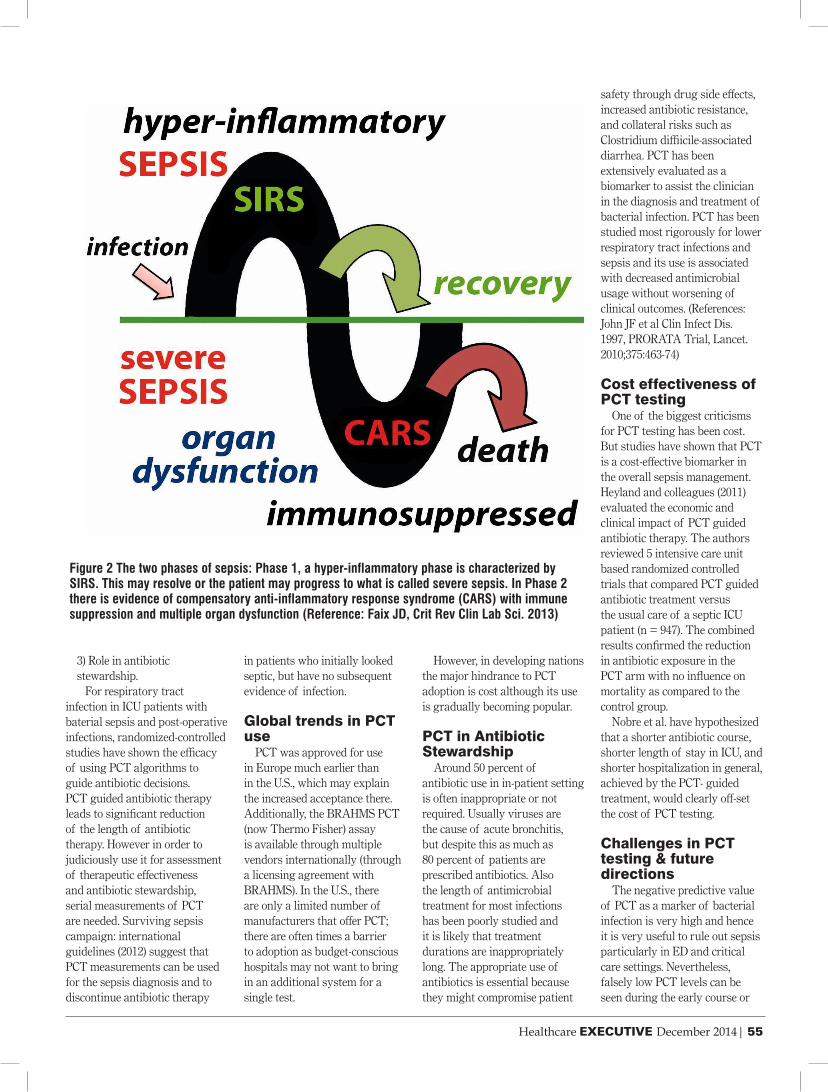
Figure 2 The two phases of sepsis: Phase 1, a hyper-inflammatory phase is characterized by SIRS. This may resolve or the patient may progress to what is called severe sepsis. In Phase 2 there is evidence of compensatory anti-inflammatory response syndrome (CARS) with immune suppression and multiple organ dysfunction (Reference: Faix JD, Crit Rev Clin Lab Sci. 2013)
in patients who initially looked septic, but have no subsequent evidence of infection.
Global trends in PCT use
PCT was approved for use in Europe much earlier than in the U.S., which may explain the increased acceptance there. Additionally, the BRAHMS PCT (now Thermo Fisher) assay is available through multiple vendors internationally (through a licensing agreement with BRAHMS). In the U.S., there are only a limited number of manufacturers that offer PCT; there are often times a barrier to adoption as budget-conscious hospitals may not want to bring in an additional system for a single test.
However, in developing nations the major hindrance to PCT adoption is cost although its use is gradually becoming popular.
PCT in Antibiotic Stewardship
Around 50 percent of antibiotic use in in-patient setting is often inappropriate or not required. Usually viruses are the cause of acute bronchitis, but despite this as much as 80 percent of patients are prescribed antibiotics. Also the length of antimicrobial treatment for most infections has been poorly studied and it is likely that treatment durations are inappropriately long. The appropriate use of antibiotics is essential because they might compromise patient
safety through drug side effects, increased antibiotic resistance, and collateral risks such as Clostridium diffiicile-associated diarrhea. PCT has been extensively evaluated as a biomarker to assist the clinician in the diagnosis and treatment of bacterial infection. PCT has been studied most rigorously for lower respiratory tract infections and sepsis and its use is associated with decreased antimicrobial usage without worsening of clinical outcomes. (References: John JF et al Clin Infect Dis. 1997, PRORATA Trial, Lancet. 2010;375:463-74)
Cost effectiveness of PCT testing
One of the biggest criticisms for PCT testing has been cost. But studies have shown that PCT is a cost-effective biomarker in the overall sepsis management. Heyland and colleagues (2011) evaluated the economic and clinical impact of PCT guided antibiotic therapy. The authors reviewed 5 intensive care unit based randomized controlled trials that compared PCT guided antibiotic treatment versus the usual care of a septic ICU patient (n = 947). The combined results confirmed the reduction in antibiotic exposure in the PCT arm with no influence on mortality as compared to the control group.
Nobre et al. have hypothesized that a shorter antibiotic course, shorter length of stay in ICU, and shorter hospitalization in general, achieved by the PCT- guided treatment, would clearly off-set the cost of PCT testing.
Challenges in PCT testing & future directions
The negative predictive value of PCT as a marker of bacterial infection is very high and hence it is very useful to rule out sepsis particularly in ED and critical care settings. Nevertheless, falsely low PCT levels can be seen during the early course or

56 | December 2014 Healthcare EXECUTIVE
localized state of an infection. PCT can identify bacterial sepsis and risk stratifies the clinical course but it cannot identify the causative organism or its antibiotic sensitivity/resistance pattern. The future needs highly sensitive PCT assays, so that subtle changes of PCT at very low concentrations can be monitored, increasing the sensitivity of the test and thus the safety of patients. Major clinical decisions regarding antibiotic stewardship are taken in the PCT range of 0.25 – 0.50 ng/mL. Thus accuracy and reproducibility at such low range of the analyte is of great clinical importance. PCT has the ability to be the “Troponin of Bacterial Sepsis” provided such “high sensitive” assays can be developed by the IVD industry.
Key Principles of PCT Interpretation Interpret in the clinical context of the patient
Patients with septic shock
should not have antibiotics withheld based on normal PCT. Patients with mild elevations in PCT who exhibit no signs or symptoms of infection may be closely monitored with serial measurements.
Serial measurements are preferred and provide more useful information
Patients very early in the onset of infection may have a normal PCT value. Patients who have persistently normal PCT levels are unlikely to have bacterial infection. Patients with other inflammatory events such as major surgery who have steadily decreasing PCT levels often do not need antibiotics.
Consider the dynamics of the disease
PCT needs to be clinically used taking into consideration the dynamics of the infective process. Patients with rising PCT suggest that there is a lack of control of the infection. Also
patients with severe infections (bacteremic pneumonia) will generally take longer time for PCT levels to normalize.
Be aware of conditions which may affect PCT levels
PCT rise is triggered by non-infective conditions like severe stress, trauma, heat stroke etc. Thus PCT should not be requested in the first 48 hours of a major surgery. Similarly PCT should not be used in neonates in the first 72 hours of birth.
Conclusions
Like any biomarker, PCT is not perfect and has some significant limitations. Moreover, it is an expensive biomarker with costs significantly higher than CRP, blood counts etc. Hence, it cannot be recommended as the single definitive test for sepsis diagnosis, but rather it must be interpreted in context of medical history, physical examination, microbiological assessment
and other relevant laboratory parameters. Nevertheless, PCT use has the evidence base of several high quality large clinical trials making it one of the strongest contenders of the sepsis biomarker arena.
Dr. Sutirtha Chakraborty, Chief Consultant, Department of Clinical Biochemistry, Peerless Hospital & B. K. Roy Research Center, Kolkata.
E: [email protected]; P: +91 080-26633486/487 HOSMAC India Pvt. Ltd.,
# 4/60, 32nd ‘C’ Cross,“1st Floor”, 4th Block - Jayanagar, Bangalore-560
011, Karnataka
HOSMAC Communication
Marketing Communications
Branding Promotion
Media Presence
Let us talk about you. We make people talk about you.



















