Diagnostic imagingalgorithm cervical soft discneck pain and 85% had radicular pain in a...
5
24ournal of Neurology, Neurosurgery, and Psychiatry 1994;57:724-728 Diagnostic imaging algorithm for cervical soft disc herniation Erik Van de Kelft, Michel van Vyve Abstract MRI with surface coils is currently the preferred method for evaluating degener- ative cervical spine disease. The differen- tiation between soft disc herniation and osteophytic spurs is not always obvious, however, on a 05 Tesla unit. The proce- dure of choice for soft disc herniation, MRI on a 0'5 T superconducting system associated with plain radiography of the cervical spine, in selecting patients for anterior cervical discectomy without interbody fusion (ACD), was evaluated. This prospective study comprised 100 patients with cervical radicular symp- toms, not subsiding after conservative treatment. Plain radiographs were obtained for al patients. Patients without spinal instability, spondylosis, or major osteophytes on plain radiographs and without clinical findings of myelopathy underwent MRI (n = 59) on a 05 Tesla superconducting system. The other 41 patients underwent CT myelography. On MRI, herniation of a cervical soft disc was seen in 55 patients and the localisa- tion corresponded well with the clinical symptoms. CT myelography showed a foraminal herniation in one of four selected patients with negative MRI. Fifty of 55 patients underwent ACD. All herni- ations were confirmed at operation, but in two patients there were important foraminal spurs not seen on MRI. It is concluded that 0-5 T MRI combined with plain radiographs offers an accurate, non-invasive test in the assessment of selected patients with cervical radicu- lopathy. (7 Neurol Neurosurg Psychiatry 1994;57:724-728) Department of Neurosurgery, Universitair Ziekenhuis Antwerpen, Belgium E V de Kelft OLV Middelares Ziekenhuis Sint-Niklaas, Belgium M van Vyve Correspondence to: Dr E Van de Kelft, Dienst Neurochirurgie, Universitair Ziekenhuis Antwerpen, Wilrijkstraat 10, B-2650 Edegem, Belgium. Received 20 January 1993 and in revised form 26 July 1993. Accepted 21 October 1993 MRI with surface coils is currently the pre- ferred method for evaluating degenerative cer- vical spine disease. In prospective and retrospective studies, MRI of the cervical spine has shown a high degree of correlation compared with myelography, CT, CT myel- ography, and surgical findings.' The sensitiv- ity of MRI is considered to be superior in evaluating disc degeneration and ligamenta flava hypertrophy.1-9 Biochemical disc degen- eration, without structural degenerative changes, may be reflected by a low signal intensity in a cervical disc on T2-weighted MRI.9-"1 Inadequate image contrast between bone and soft tissue may, however, diminish specificity of MRI. The differentiation between soft disc herniation and osteophytic spurs is not always obvious. MRI of the cervi- cal spine associated with plain radiographs may be the best alternative in the preoperative neuroradiological assessement of patients sus- pected of a soft disc herniation with no major osteophytic spurs. We prefer anterior cervical discectomy without interbody fusion (ACD) as the surgical procedure for patients with soft disc hernia- tion, without clinical evidence of myelopathy and without advanced spondylosis, instability, or spurs.'2-33 The ACD procedure is ideal to verify the exact location of disc herniations. The purpose of this study was to describe the value of MRI on a 0-5 T superconducting system associated with plain radiography of the cervical spine in selecting patients for ACD. Material and methods PATIENT SELECTION During the period from June 1988 to June 1991, a total of 100 patients with symptoms or signs of cervical radiculopathy, not subsid- ing after a period of conservative treatment, were referred for surgical treatment. Criteria of selection for ACD were: (a) no clinically manifest myelopathy and no prior cervical trauma or surgery; (b) no signs of spondylosis, major osteophytes, or instability on plain radi- ographs (instability was defined as horizontal motion of a segment in excess of 3 5 mm or an angulation of one vertebral body of more than 11 degrees with respect to another); (c) one or more cervical soft disc herniations on MRI (figs IA and 1B, 2, 3).24 Plain radiographs were obtained in the lat- eral, anteroposterior, and 450 oblique views. Flexion and extension radiographs were obtained for all patients to investigate in- stability. MRI EVALUATION After clinical and radiographical selection, 59 patients underwent surface coil MRI of the cervical spine. MRI was performed on a 0 5 T superconducting system (Siemens Magne- tom). The MRI protocol included sagittal Ti- weighted (SE 30) images and sagittal gradient echo images (FLASH sequence GE 29 with 150 flip angle). Additional axial Tl-weighted images were obtained (SE 30 in the prone position and SE 40 with inclination) through the anatomical region of interest as defined by sagittal MRI, with 5 mm sections and disc 724 on February 25, 2020 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. Downloaded from
Transcript of Diagnostic imagingalgorithm cervical soft discneck pain and 85% had radicular pain in a...

24ournal ofNeurology, Neurosurgery, and Psychiatry 1994;57:724-728
Diagnostic imaging algorithm for cervical soft discherniation
Erik Van de Kelft, Michel van Vyve
AbstractMRI with surface coils is currently thepreferred method for evaluating degener-ative cervical spine disease. The differen-tiation between soft disc herniation andosteophytic spurs is not always obvious,however, on a 05 Tesla unit. The proce-dure of choice for soft disc herniation,MRI on a 0'5 T superconducting systemassociated with plain radiography of thecervical spine, in selecting patients foranterior cervical discectomy withoutinterbody fusion (ACD), was evaluated.This prospective study comprised 100patients with cervical radicular symp-toms, not subsiding after conservativetreatment. Plain radiographs wereobtained for al patients. Patients withoutspinal instability, spondylosis, or majorosteophytes on plain radiographs andwithout clinical findings of myelopathyunderwent MRI (n = 59) on a 05 Teslasuperconducting system. The other 41patients underwent CT myelography. OnMRI, herniation of a cervical soft discwas seen in 55 patients and the localisa-tion corresponded well with the clinicalsymptoms. CT myelography showed aforaminal herniation in one of fourselected patients with negative MRI. Fiftyof 55 patients underwent ACD. All herni-ations were confirmed at operation, butin two patients there were importantforaminal spurs not seen on MRI. It isconcluded that 0-5 T MRI combined withplain radiographs offers an accurate,non-invasive test in the assessment ofselected patients with cervical radicu-lopathy.
(7 Neurol Neurosurg Psychiatry 1994;57:724-728)
Department ofNeurosurgery,UniversitairZiekenhuisAntwerpen, BelgiumE V de KelftOLV MiddelaresZiekenhuisSint-Niklaas, BelgiumM van VyveCorrespondence to:Dr E Van de Kelft, DienstNeurochirurgie, UniversitairZiekenhuis Antwerpen,Wilrijkstraat 10, B-2650Edegem, Belgium.Received 20 January 1993and in revised form26 July 1993.Accepted 21 October 1993
MRI with surface coils is currently the pre-ferred method for evaluating degenerative cer-vical spine disease. In prospective andretrospective studies, MRI of the cervicalspine has shown a high degree of correlationcompared with myelography, CT, CT myel-ography, and surgical findings.' The sensitiv-ity of MRI is considered to be superior inevaluating disc degeneration and ligamentaflava hypertrophy.1-9 Biochemical disc degen-eration, without structural degenerativechanges, may be reflected by a low signalintensity in a cervical disc on T2-weightedMRI.9-"1 Inadequate image contrast betweenbone and soft tissue may, however, diminish
specificity of MRI. The differentiationbetween soft disc herniation and osteophyticspurs is not always obvious. MRI of the cervi-cal spine associated with plain radiographsmay be the best alternative in the preoperativeneuroradiological assessement of patients sus-pected of a soft disc herniation with no majorosteophytic spurs.We prefer anterior cervical discectomy
without interbody fusion (ACD) as the surgicalprocedure for patients with soft disc hernia-tion, without clinical evidence of myelopathyand without advanced spondylosis, instability,or spurs.'2-33 The ACD procedure is ideal toverify the exact location of disc herniations.The purpose of this study was to describe
the value ofMRI on a 0-5 T superconductingsystem associated with plain radiography ofthe cervical spine in selecting patients forACD.
Material and methodsPATIENT SELECTIONDuring the period from June 1988 to June1991, a total of 100 patients with symptomsor signs of cervical radiculopathy, not subsid-ing after a period of conservative treatment,were referred for surgical treatment. Criteriaof selection for ACD were: (a) no clinicallymanifest myelopathy and no prior cervicaltrauma or surgery; (b) no signs of spondylosis,major osteophytes, or instability on plain radi-ographs (instability was defined as horizontalmotion of a segment in excess of 3 5 mm oran angulation of one vertebral body of morethan 11 degrees with respect to another); (c)one or more cervical soft disc herniations onMRI (figs IA and 1B, 2, 3).24
Plain radiographs were obtained in the lat-eral, anteroposterior, and 450 oblique views.Flexion and extension radiographs wereobtained for all patients to investigate in-stability.
MRI EVALUATIONAfter clinical and radiographical selection, 59patients underwent surface coil MRI of thecervical spine. MRI was performed on a 0 5 Tsuperconducting system (Siemens Magne-tom). The MRI protocol included sagittal Ti-weighted (SE 30) images and sagittal gradientecho images (FLASH sequence GE 29 with150 flip angle). Additional axial Tl-weightedimages were obtained (SE 30 in the proneposition and SE 40 with inclination) throughthe anatomical region of interest as defined bysagittal MRI, with 5 mm sections and disc
724 on F
ebruary 25, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. Dow
nloaded from

Diagnostic imaging algorithm for cervical soft disc herniation
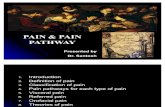
Figure 1 (A) MidsagittalTl-weighted MRI imageshowing proved posteriorsoft disc herniation at C5-C6 in a patient with C6radiculopathy to the right.Plain radiographs werenormal. (B) MidsagittalT2-weighted MRI of thesame patient showingimportant impression onthe dural sac; this patienthad no signs or symptomsof cervical myelopathy.
angled. The primary criterion for the interpre-tation of clinically significant lesions was theeffacement of the subarachnoid space in thevicinity of the clinically affected nerve root onparaxial images.
SURGICAL PROCEDUREFifty ACD procedures were carried out on 50patients within one month after MRI. Therewere 28 men and 22 women. The ages rangedfrom 29 to 54 (mean 36) years. All patientswere operated on under general anaesthesiaand with cervical traction. The anterior cervicalspine was approached in the standard fashionfrom the left side. Fluoroscopy was used tolocate the level and an operating microscopewas employed routinely. The disc space wascleared of all disc material with abrasion ofthe adjacent vertebral end plates. The poste-rior part of the annulus fibrosus and minorposterior osteophytes ("transverse bar") wereremoved. The posterior third of the postero-lateral ridge was routinely removed as theextruded disc fragment, if lateralised, isalways found behind it. Finally, the posteriorlongitudinal ligament was excised to expose
the dural sac and the proximal part of the rootsleeve. The foramina were explored routinelyby a blunt hook. Minor osteophytes lateral tothe uncinate process were removed with a fineangled curette. Patients did not wear cervicalcollars after surgery.
OUTCOME ANALYSISThe outcome was measured by the func-tional-economic outcome rating scaledescribed by Prolo et al (table 1), which con-sists of two subscales: the economic and thefunctional.25 This scale was initially developedfor lumbar spine surgery, but may be appliedfor cervical radiculopathy as well, providingthat no spinal cord symptoms are present.Outcome scores were assigned by the physi-cian (EVdeK) on the basis of clinical follow
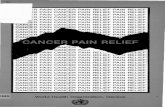
Figure 2 Axial Tl-weighted MRI of the samepatient as in fig 1 showingeffacement of thesubarachnoid space at theright due to a soft discherniation (arrow).
Figure 3 Axial Tl-weighted MRI of a patient with aleft-sided C7 radiculopathy due to a soft disc herniationC6-C7 on the left. Note theforaminal migration of the disc(arrow).
|e||||E|||||||iEiSF
725 on F
ebruary 25, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. Dow
nloaded from

Van de Kelft, van Vyve
Table I Functional-economic outcome rating scale
Economic status:El Complete invalidE2 No gainful occupation including ability to do
housework or continue retirement activitiesE3 Able to work but not at previous occupationE4 Working at previous occupation part time or limited
statusE5 Able to work at previous occupation with no restriction
of any kindFunctional status:
Fl Total incapacity (or worse than before operation)F2 Mild-to-moderate level of neck and/or irradiating arm
painF3 Low level of pain and able to perform all activities
except sportsF4 No pain, but patient has had one or more recurrences
of neck or irradiating painF5 Complete recovery, no recurrent episodes of neck pain,
able to perform all previous sports activities
up at least one year after surgery. The sub-scale scores were summed to obtain an overallscore. Total scores of 5 or less were consid-ered poor; scores 6 to 7 were considered mod-erate; and scores 8 to 10 were considered tobe good outcomes.
ResultsCLINICAL FINDINGSAll patients complained of arm, shoulder, orneck pain and 85% had radicular pain in adermatomal distribution. Fifty five per cent ofpatients had a sensory or reflex loss compati-ble with the location of the disc. Eighteenpatients had clinical signs of myelopathy orthey mentioned previous cervical trauma orsurgery (fig 4).
PLAIN RADIOGRAPHSEighty two patients without myelopathy,previous neck surgery, or trauma as well as 18patients with these clinical findings had plainradiographs taken of the cervical spine (fig 4).Twenty three were found to have spinalinstability, spondylosis, or major osteophyticspurs.
Table 2 Outcome ofpatients after operation as measuredby thefunctional-economic outcome rating scale
Economic (%) Functional (%) Total (%)
El (0) F1 (0) 2 (0)E2 (2) F2 (4) 3 (2)E3 (8) F3 (18) 4 (2)E4 (32) F4 (40) 5 (2)E5 (58) F5 (38) 6 (4)
7 (8)8 (16)9 (34)
10 (32)
MRI EVALUATIONMRI showed 56 herniated discs in 55 out of59 selected patients. In four patients, MRIwas normal. One patient had two herniatedcervical discs. Twenty two discs were at C5-C6, 17 at C6-C7, 10 at C4-C5, five at C3-C4, and two at C7-T1. One herniation wasmedial, 27 were lateralised to the right, 28 tothe left. In four patients, migration of discfragments without rupture of the posteriorlongitudinal ligament was seen. In anotherthree patients, migration of disc fragmentswith rupture of the posterior longitudinal liga-ment were found. All migrated disc fragmentswere lateralised; three to the left and four tothe right.
In all patients, the presence of a cervicalsoft disc herniation was confirmed during theoperation. In 47 of 50 operated cervical softdisc herniations, the operative findings corre-lated exactly with the preoperative MRI(94%). All lateralised disc herniations werevisualised when the posterolateral part of theuncinate process was removed. In one patient,we found rupture of the posterior longitudinalligament, by contrast with the MRI findings.In two other patients we found an importantlateral spur at the level of the herniation, com-pared with MRI on which it was interpretedas disc material. No major osteophytes wereseen during the operation. CT myelographyshowed a lateral foraminal herniation in oneof four selected patients with negative MRI.
Cervical radiculopathy (n = 100)
MyelopathyPrior neck surgery/trauma
No (n = 82) Yes (n = 18)
Plain radiography:anteroposterior,lateral, oblique
SpondylosisMajor spursInstability
No(n = 59)
MRI(soft discherniation)
Yes No-(n = 55) (n = 4)
Yes(n =23)
CTmyelography
t
OUTCOME AS MEASURED BY THE FUNCTIONALECONOMIC OUTCOME RATING SCALEThe mean economic outcome score of allpatients was 4-5. The mean functional out-come score was 4 1 (table 2). Although all 50patients initially noted symptomatic improve-ment postoperatively, two patients reportedresidual symptoms after a one year follow upwith a functional outcome rate of F2. Fourpatients suffered temporary interscapular orneck pain. The overall satisfactory improve-ment was evident in 95% of this series afterone year. No patient developed myelopathy orother radiculopathy. The total functional-economic outcome rating scale score of thisseries was 8 1, with 6% poor, 12% moderate,and 82% good results.
DiscussionFor the past decade, the gold standard in eval-uating patients with cervical radiculopathy has
Figure 4 Diagnosticimaging algorythm forcervical soft discherniation.
726 on F
ebruary 25, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. Dow
nloaded from

Diagnostic imaging algorithm for cervical soft disc herniation
been CT myelography.627 Limitations exist,however, and are similar to those with plainCT. Moreover, CT myelography allows a lim-ited view of the spine, usually covering onlythree to four cervical levels. The procedure isinvasive and more costly as it requires a mini-mum stay of 24 hours in the hospital. MRIoffers several advantages over CT myelogra-phy in screening for operable cervical spinelesions.' MRI is able to survey the entirecervical spine without ionising radiation andis a non-invasive, outpatient examination,whereas CT myelography requires cervical orlumbar puncture and intrathecal contrastmaterial, with the possibility of delayedadverse reactions.28 Furthermore, MRI pro-vides useful information on pathology, allow-ing a non-invasive evaluation after surgicalprocedures and enabling a better understand-ing of surgical consequences.29
Several disadvantages have retarded the useof MRI as a screening method for degenera-tive disease of the cervical spine. Theseinclude the inability to obtain sections lessthan 3 to 5 mm thick (at least on our system),resulting in a partial volume averaging andsuboptimal differentiation between osteo-phytes and disc material. Herniated discsextending into the obliquely oriented lateralroot canals are not as reliably identified whenspurs are prominent as on intrathecal contrastCT with 1-5 mm thick sections. Poor resolu-tion between osteophytes, CSF, ligaments,and dura, all of which have similar low signalintensity, limits the specificity of MRI. Gd-DTPA enhanced TI-weighted imagesenhance soft tissue details in the neuralforamina, allowing improved detection offoraminal encroachment. Gd-DTPA was notused in our patients as our goal was to establisha non-invasive screening sequence. As such,we prospectively analysed MRI in combina-tion with plain films to exclude those patientswith major osteophytes or spondylotic degen-eration. We are well aware of the fact thatselection of different optimal screening exami-nations for patients with radiculopathy is anoption compromised by inexact correlationbetween clinical findings and anatomicallesions. Other series report 22-7% of patientswith cervical soft disc herniation presentingwith myelopathy rather than radiculopathy.These patients were not selected for MRI inour study, but underwent CT myelography,most patients presenting with myelopathyhave cervical spondylosis for which CT myel-ography seems to be more specific than MRI.1Patients with bony canal stenosis often pre-sent with radiculopathy. These patients wereassessed by CT myelography in our study. 'On sagittal or axial images, disc herniations
are seen as focal protrusions of disc materialbehind the uncinate process, which may com-press the thecal sac and spinal cord, oftenwithout myelopathy. The sequestered discs,seen in eight patients on MRI were all con-firmed during surgery. The dislodgement ofthose disc fragments into the right or left halfof the anterior epidural space and the highincidence of lateralised disc herniations, may
be explained by a sagittally aligned collagenseptum dividing the space between the poste-rior part of the disc and the posterior longitu-dinal ligament into two parts.30
Herniated disc material usually has a highsignal intensity on T2-weighted images com-pared with the vertebral body and the spinalcord, both fat-containing structures with alow signal intensity on these MRI sequences(fig 1B). The intervertebral portion of the discoften degenerates, thereby producing lowersignal intensity on T2-weighted images.Occasionally, the intervertebral portion of thedisc has normal signal intensity, even thoughthe disc is herniated.' This was not found inour study. The T2-weighted pulse sequence isknown to be poor in distinguishing betweenthe ligamentous structures lining the spinalcanal, and the dural sac. Therefore in somepatients an apparent discrepancy existsbetween the T2-weighted gradient echo imagewhich shows an anterior dural impression,and the Tl-weighted section which does not(fig 1A and B).MRI was able to detect at least one soft
herniated disc in 91% of all selected patients.In one patient, the MRI was not able to dis-close a disc herniation, that was shown laterby CT-myelography.
In our opinion, clinically significant osteo-phytes adjoining herniated soft discs areunlikely to be missed by both combined plainfilm/MRI screening and the ACD procedure.Herniated discs and minor osteophytes in thelateral root canal are considered to be uncom-mon causes of cervical radiculopathy.3'32 Inour series, however, two patients had a discherniated into the lateral foramen associatedwith a lateral spur. This was not seen on MRIbecause of the low specificity of 05 T MRIfor foraminal structures. The specificity ofMRI for cervical soft disc herniation, withoutspondylosis on plain films, is 96% in ourstudy. This confirms the low specificity ofMRI for foraminal lesions, which might occurmore often than is generally accepted.32 Theabsence of fat in the cervical epidural spaceand its paucity in the neural foraminal canallimit the usefulness of Ti-weightedsequences. Provided that sufficient MRI spa-tial resolution is available, T2-weightedsequences could be fruitful because signalsfrom both the cerebrospinal fluid and flow inthe intraspinal or canalicular venous plexusmay highlight structures that posses a lesserT2-weighted signal, such as the spinal cord,nerve roots, and some adjacent normal orpathological bone and joints. Recently,Yousem et al introduced three dimensionalFourier transform (3DFT) MRI in assessingdegenerative foraminal narrowing in the cervi-cal canal with good results.32 Under these cir-cumstances, MRI, even without theassociation of plain films, may become as spe-cific as CT myelography in showing cervicalroot pathology. Osteophytes are preformed incartilage, however, and evolve within severalweeks to a few months. They may be of sub-stantial size before ossification.3' In a recentstudy, these "cartilaginous caps", described
727 on F
ebruary 25, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. Dow
nloaded from

Van de Keift, van Vyve
during surgery, were not seen on CT myelo-graphy or on MRI.34 A cervical foraminalradiculopathy may exist, even without neuro-radiological evidence.
In conclusion MRI with surface coils per-formed on a 0 5 T superconducting systemcombined with plain films of the cervical spineoffers an accurate, non-invasive test for thepreoperative evaluation of cervical radiculo-pathy without myelopathy. Lateral foraminalhemiations may be missed, however, byclassical 2 DFT imaging modalities. Theproposed strategy: plain radiography plusMRI as a first screening for cervical radiculo-pathy should presently be the optimal pro-cedure and by far the most cost effective. Itmay be the only imaging strategy requiredbefore appropriate treatment is applied.
1 Brown BM, Schwartz RH, Frank E, Blank NK.Preoperative evaluation of cervical radiculopathy andmyelopathy by surface-coil MR imaging. AJNR 1988;151:1205-12.
2 Czervionke LF, Daniels DL. Cervical spine anatomy andpathologic process. Applications of new MR techniques.Rad Clin North Am 1988;26:921-47.
3 Enzmann DR, Rubin JB. Cervical spine: MR imaging witha partial flip angle, gradient-refocused pulse sequence.Part I. General considerations and disc disease.Radiology 1988;166:467-72.
4 Flannigan BD, Lufkin RB, McGlade C, et al. MR imagingof the cervical spine: neurovascular anatomy. AJNR1987;148:785-90.
5 Larsson EM, Holtas S, Croncvist S, Brandt L.Comparison of myelography and magnetic resonanceimaging in cervical spondylosis and disk hemiation. ActaRadiol 1989;30:233-9.
6 Ross JS, Masaryk TJ, Modic MT. Postoperative cervicalspine: MR assessment. J Comput Assist Tomogr 1987;11:955-62.
7 Ross JS, Modic M, Masaryk TJ, Carter J, Marcus TE,Bohlman H. Assessment of extradural degenerativedisease with Gd-DTPA-enhanced MR imaging.Correlation with surgical and pathologic findings. AJNR1989;10: 1243-50.
8 Ross JS, Modic MT, Masaryk TJ. Tears of the annulusfibrosus: assessement with Gd-DTPA-enhanced MRimaging. AJNR 1989;10:1251-5.
9 Schiebler ML, Camerino VJ, Fallon MD, Zlatkin MB,Grenier N, Kressel H. In vivo and ex vivo magnetic reso-nance imaging evaluation of early disc degeneration withhistopathologic correlation. Spine 1991 ;16:635-40.
10 Tertti M, Paajanen H, Laato M, Aho H, Komu M,Kormano M. Disc degeneration in magnetic resonanceimaging. A comparative biochemical, histologic, andradiologic studies in cadaver species. Spine 1991;16:629-34.
11 Viikari-Juntura E, Raininko R, Videman Y, Porkka L.Evaluation of cervical disc degeneration with ultralowfield MRI and discography. An experimental study oncadavers. Spine 1989;14:616-9.
12 Bertalanffy H, Eggert HR. Complications of anteriorcervical discectomy without fusion in 450 consecutivepatients. Acta Neurochir (Wien) 1989;99:41-50.
13 Eriksen EF, Buhl M, Fode K, et al. Treatment of cervicaldisc disease using Cloward's technique. The prognosticvalue of clinical preoperative data in 1106 patients. ActaNeurochir (Wien) 1984;70: 181-97.
14 Espersen JO, Buhl M, Eriksen EF, et al. Treatment of cer-vical disc disease using Cloward's technique. I Generalresults, effect of different operative methods and compli-cations in 1106 patients. Acta Neurochir (Wien)1984;70:97-114.
15 Herkowitz HN, Kurz LT, Overholt DP. Surgical manage-ment of cervical soft disc hemiation. A comparisonbetween the anterior and posterior approach. Spine1990;15: 1026-30.
16 Edger MA, Nundy S. Innervation of the spinal dura mater.Y Neurol Neurosurg Psychiatry 1964;29:530-4.
17 Robertson JT. Anterior cervical discectomy withoutfusion. In: Dunsker SB, ed. Cervical spondylosis. NewYork: Raven Press, 1981:181-1904.
18 Robertson JT, Johnson SD. Anterior cervical discectomywithout fusion: long-term results. Clin Neurosurg 1980;27:440-9.
19 Scoville WB. Types of cervical disc lesions and their surgi-cal approaches. JAMA 1966;196:105-7.
20 Simeone FA, Rothman RH. Cervical disc disease. In:Rothman RH, Simeone FA, eds. The spine. Philadelphia:WB Saunders, 1982:491.
21 Wilson DH, Campbell DD. Anterior cervical discectomywithout bone graft. Y Neurosurg 1977;47:551-5.
22 Wohlert L, Buhl M, Eriksen EF, et al. Treatment ofcervical disc disease using Cloward's technique. IIIEvaluation of cervical spondylotic myelopathy in 138cases. Acta Neurochir (Wien) 1984;70:121-31.
23 Yamamoto I, Ikeda A, Shibuya N, Tsugane R, Sato 0.Clinical long-term results of anterior discectomy withoutinterbody fusion for cervical disc disease. Spine 1991;16:272-9.
24 Burrows E. The sagittal diameter of the spinal canal incervical spondylosis. Clin Radiol 1963;14:77-86.
25 Husag L, Probst C. Microsurgical anterior approach tocervical discs. Review of 60 consecutive cases of discec-tomy without fusion. Acta Neurochir (Wien) 1984;73:229-42.
25 Prolo DJ, Oklund SA, Butcher M. Toward uniformity inevaluating results of lumbar spine operations. A para-digm applied to posterior lumbar interbody fusions.Spine 1986;11:601-6.
26 Landman JA, Hoffman JC Jr, Braun IF, Barrow DL. Valueof computed tomographic myelography in the recogni-tion of cervical herniated disc. AJNR 1984;5:391-5.
27 Sobel DF, Barkovich AJ, Munderloh SH. Metrizamidemyelography and postmyelographic computed tomogra-phy: comparative adequacy in the cervical spine. AJ7NR1984;5:385-90.
28 Van de Kelft E, Bosmans J, Van Vyve M, Parizel PM,Selosse P. Intracerebral hemorrhage after iohexol myelo-graphy. Report of a case and review of the literature.Neurosurgery 1991;28:570-4.
29 Van de Kelft E, Van Vyve M, Selosse P. Postsurgicalfollow-up by MRI of anterior cervical discectomy with-out fusion. Eur J7 Radiol 1992; 15: 196-9.
30 Schellinger D, Manz HJ, Vidic B, et al. Disk fragmentmigration. Radiology 1990;175:831-6.
31 Tsuruda JS, Norman D, Dillon W, Newton TH, MillsDG. Three-dimensional gradient-recalled MR imagingas a screening tool for the diagnosis of cervical radiculo-pathy. AYR 1990;154:375-83.
32 Youssem DM, Atlas SW, Goldberg HI, Grossman RI.Degenerative narrowing of the cervical spine neuralforamina: evaluation with high-resolution 3DFTgradient-echo MR imaging. A3rNR 1991;12:229-37.
33 Sabiston CP, Adams ME, Li DKB. Magnetic resonanceimaging of osteoarthritis: correlation with gross pathol-ogy using an experimental model. J Orthop Res 1987;5:164-72.
34 Houser OW, Onofrio BM, Miller GM, Folger WN, SmithPL, Kallman DA. Cervical neural foraminal stenosis:computerized tomographic myelography diagnosis._J Neurosurg 1993;79:84-8.
728
on February 25, 2020 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.6.724 on 1 June 1994. D
ownloaded from