
Imaging Degenerative Diseases of the Brain Cathleen Kouvolo.
Upload
mohamed-zaitounCategory
view
5.048download
0
C.N.S.Degenerative & White Matter
Diseases

Mohamed Zaitoun
Assistant Lecturer-Diagnostic Radiology Department , Zagazig University Hospitals
EgyptFINR (Fellowship of Interventional
Neuroradiology)[email protected]


Knowing as much as possible about your enemy precedes successful battle
and learning about the disease process precedes successful management

Degenerative & White Matter Diseases(i) White Matter Disease(ii) Gray Matter Disease
(i) White Matter Disease :-The typical MRI appearance of white matter injury is T2
prolongation of the affected white matter , less likely tumefactive demyelination may be mass like , enhance & look very similar to a tumor
-The key imaging finding of demyelinating disease is minimal mass effect relative to the lesion size
-A frequent pattern of white matter disease consisting of scattered foci of T2 prolongation in the subcortical , deep & periventricular white matter is seen very commonly , especially in older adults , this pattern is most likely due to chronic microvascular ischemia

-In younger patients, a similar pattern can be seen in chronic migraine headaches , as sequelae of prior infectious or inflammatory disease & with demyelination
-Two types :a) Demyelinating diseaseb) Dysmyelinating disease

a) Demyelinating disease : -Acquired disease in which normal myelin is destroyed1-Idiopathic / Autoimmune / Inflammatory : Multiple
Sclerosis2-Post-Viral White Matter Disease : ADEM3-Toxin Related4-Vascular White Matter Disease5-Infectious (Viral) White Matter Disease

1-Multiple Sclerosis :a) Incidenceb) Clinical Picturec) Radiographic Featuresd) Tumefactive MSe) McDonald criteria for MSf) Variantsg) Differential Diagnosis

a) Incidence :-Presentation is usually between adolescence
and the sixth decade with a peak at approximately 35 years of age
-More in females (60 %)-Most common chronic demyelinating disease ,
it often leads to severe disability

b) Clinical Picture :-Monocular visual loss (optic neuritis) , gait difficulties
and sensory disturbances are most common-There are 2 main clinical presentations :1-Relapsing remitting : Most commonPartial or complete resolution of each acute attack2-Progressive :No resolution or incomplete resolution between acute
attacks*Primary progressive : slow onset without discrete
exacerbations*Secondary progressive : similar to relapsing remitting
but with less complete resolution between attacks leading to progressive disability
-The diagnosis is based on a composite of clinical and laboratory data (evoked potentials , CSF oligoclonal bands) but not imaging studies , MRI aids in monitoring treatment

c) Radiographic Features :1-CT :-CT features are usually non specific and significant
change may be seen on MRI with an essentially normal CT scan
-Features that may be present include :a) Plaques can be homogeneously hypoattenuatingb) Brain atrophy may be evident in with long standing
chronic MSc) Some plaques may show contrast enhancement in
the active phase

2-MRI :1-MR Appearance of Plaques2-Distribution of Plaques3-Typical Findings4-Other Findings5-Spine

1-MR Appearance of Plaques :*T1 :-Lesions are typically iso to hypointense (chronic)-Lesions that are dark on T1 are called black holes & are
associated with more severe demyelination & axonal loss*T2 :-Lesions are typically hyperintense-Plaques are most commonly multiple , to support the
diagnosis of MS at least three plaques of >5 mm should be present
-Average size range : 0.5 to 3 cm-Oblong elliptical T2 bright structures at callososeptal
interface (located on the inferior surface of the corpus callosum when the septum pellucidum abuts it)

Multiple focal hyperintense lesions are seen at the callososeptal interface (arrows)

LEFT : Single lesion on T2WI , RIGHT : Two new lesions at 3 month follow-up

*FLAIR :-Lesions are typically hyperintense-when arranged perpendicular to lateral
ventricles extending radially outward (best seen on parasagittal image) , they are termed Dawson fingers

Multiple well-defined ring-like hyperintense lesions are also seen along the periventricular white matter (Dawson's fingers) (arrow) with their long axis perpendicular to the corpus callosum

Dawson’s fingers in MS , parasagittal FLAIR shows numerous foci of T2 prolongation (arrows) within the corpus callosum that points towards the ventricle
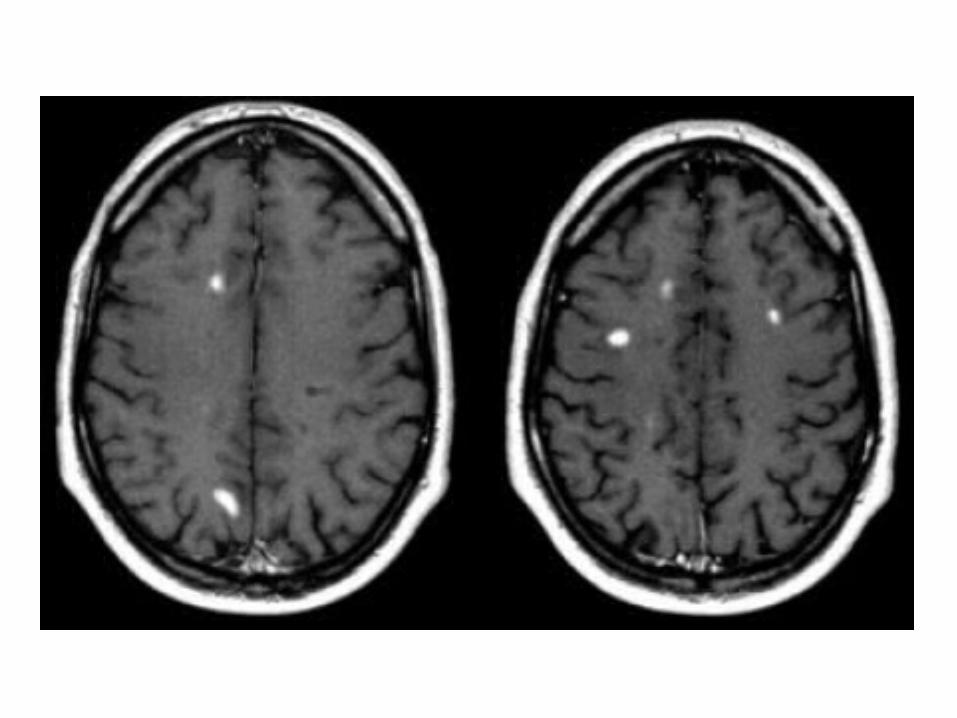
*T1+C :-Contrast enhancement may be homogeneous ,
ringlike or patchy-Enhancement is often incomplete around the
periphery (open ring sign)-Inactive plaques do not enhance*DWI :-Active plaques may demonstrate restricted
diffusion
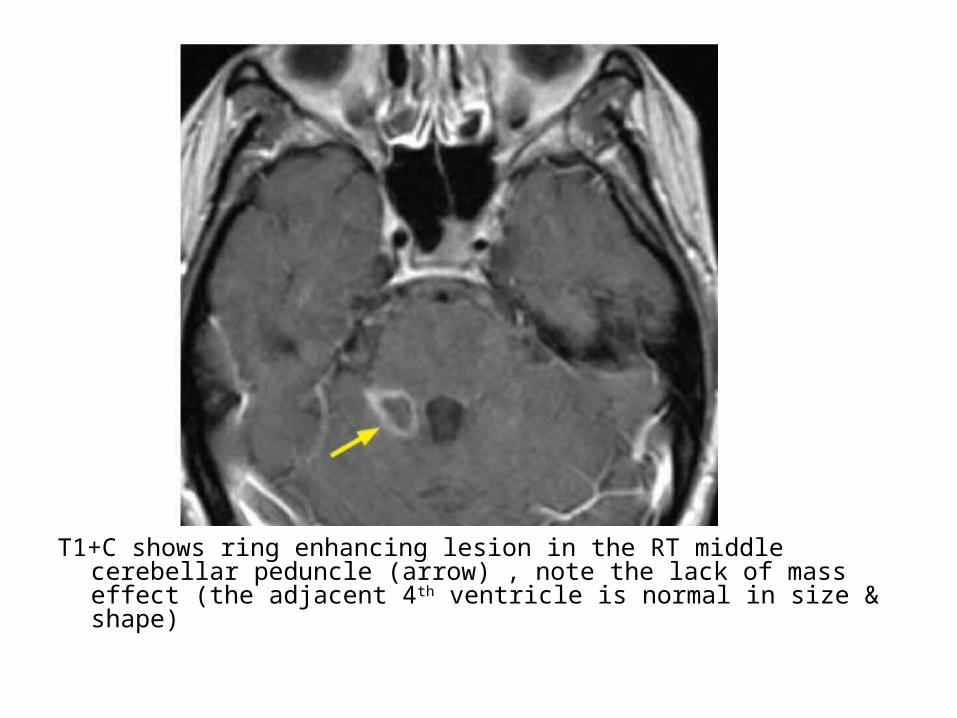
T1+C shows ring enhancing lesion in the RT middle cerebellar peduncle (arrow) , note the lack of mass effect (the adjacent 4th ventricle is normal in size & shape)

T1+C shows incomplete ring enhancement

2-Distribution of Plaques :1-Supratentorial :-Bilateral periventricular , 85%-Corpus Callosum , 70 %-Scattered in WM-GM (uncommon)2-Brain stem3-Cerebellum4-Spinal Cord , 50 %5-Optic Nerve , Chiasm
3-Typical Findings :a) Juxtacortical lesionsb) Temporal lobe involvementc) Multiple lesions adjacent to the ventriclesd) Ovoid lesions perpendicular to the ventriclese) Multiple lesions in brainstem and cerebellumf) Enhancement

a) Juxtacortical lesions :-These are adjacent to the cortex and must
touch the cortex-In small vessel disease these Juxtacortical
U-fibers are not involved and on T2 and FLAIR there will be a dark band between the WML and the (also bright) cortex

LEFT : involvement of U-fibers in MS , RIGHT : U-fibers are not involved in patient with hypertension


b) Temporal lobe involvementc) Multiple periventricular lesionsd) Ovoid lesions perpendicular to the ventricles :-These ovoid lesions are also called Dawson fingers-They represent areas of demyelination along the
small cerebral veins that run perpendicular to the ventricles
e) Multiple lesions in brainstem and cerebellum


f) Enhancement :-This enhancement will be present for about one
month after the occurrence of a lesion-The simultaneous demonstration of enhancing and
non-enhancing lesions in MS is the radiological counterpart of the clinical dissemination in time and space
-The edema will regress and finally only the center will remain as a hyperintense lesion on T2

4-Other Findings :a) Cortical central atrophy , 20%-80% with chronic
MSb) Atrophy of corpus callosum , 40% with chronic
MSc) Hypointense thalamus and putamen on T2
(increased Ferritin)d) Mass effect of very large plaques (>3 cm) may
mimic tumors (uncommon)e) MRS changes with chronic MS are decrease
NAA , increase choline , increase lipids & increase lactate

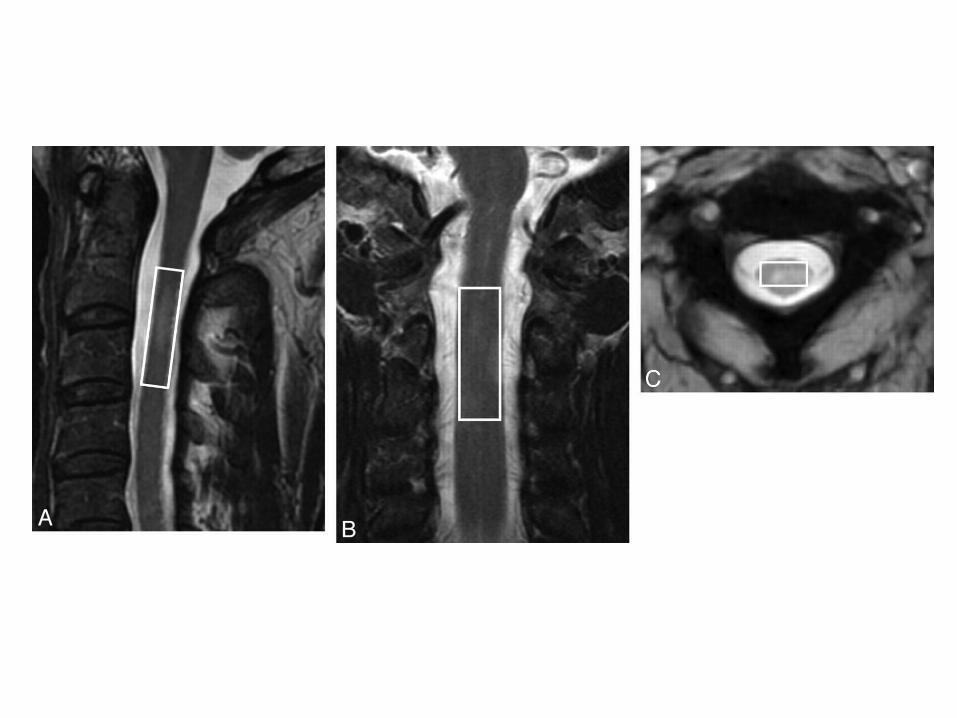
5-Spine :-Typical spinal cord lesions in MS are relatively
small, peripherally located and multiple-They are most often found in the cervical cord
and are usually less than 2 vertebral segments in length
-A spinal cord lesion together with a lesion in the cerebellum or brainstem is very suggestive of MS
-Isolated spinal cord involvement is seen in up to 20 % of cases of MS


d) Tumefactive MS :-Tumefactive MS is a variant of Multiple Sclerosis-It presents as a large intra-parenchymal lesion (> 2 cm)
with usually less mass effect than would be expected for its size
-After the administration of gadolinium, there may be some peripheral enhancement often with an incomplete ring with absence of cortical involvement, these lesions can be distinguished from gliomas or intraparenchymal abscesses which typically have a closed-ring enhancement
-Differential diagnosis of rapidly progressive neurological deficit with ring-enhancing lesions include brain abscess, primary brain neoplasm or brain metastasis, acute disseminated encephalomyelitis (ADEM) and tumefactive MS
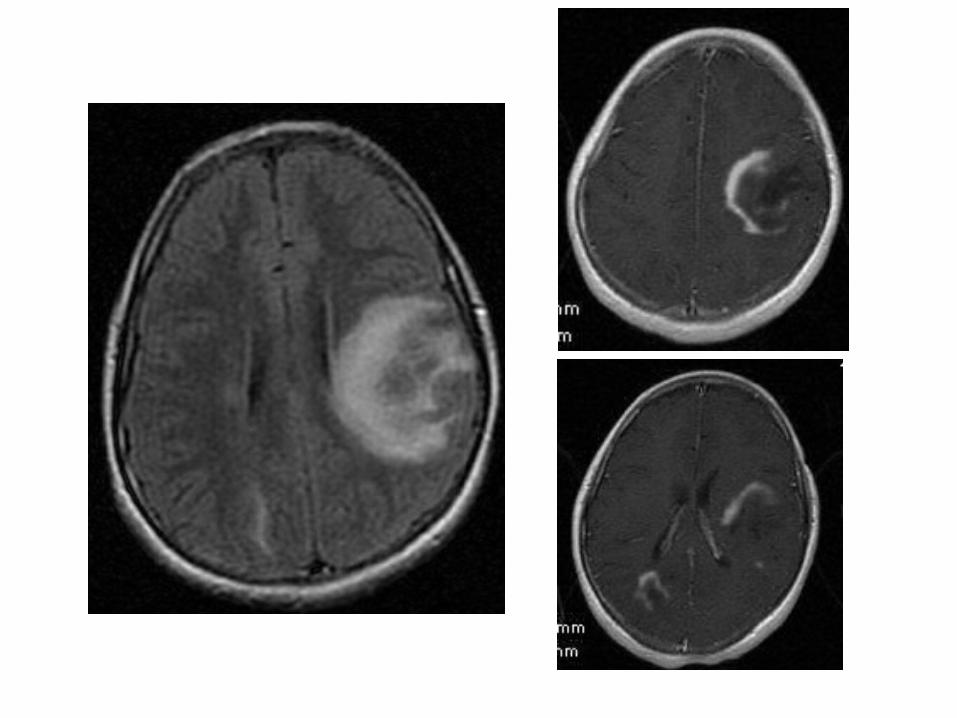

Hypodense lesion seen over the right fronto-parietal-temporal area surrounded by vasogenic edema and causing midline shift to the left side , this lesion shows peripheral enhancement post IV contrast
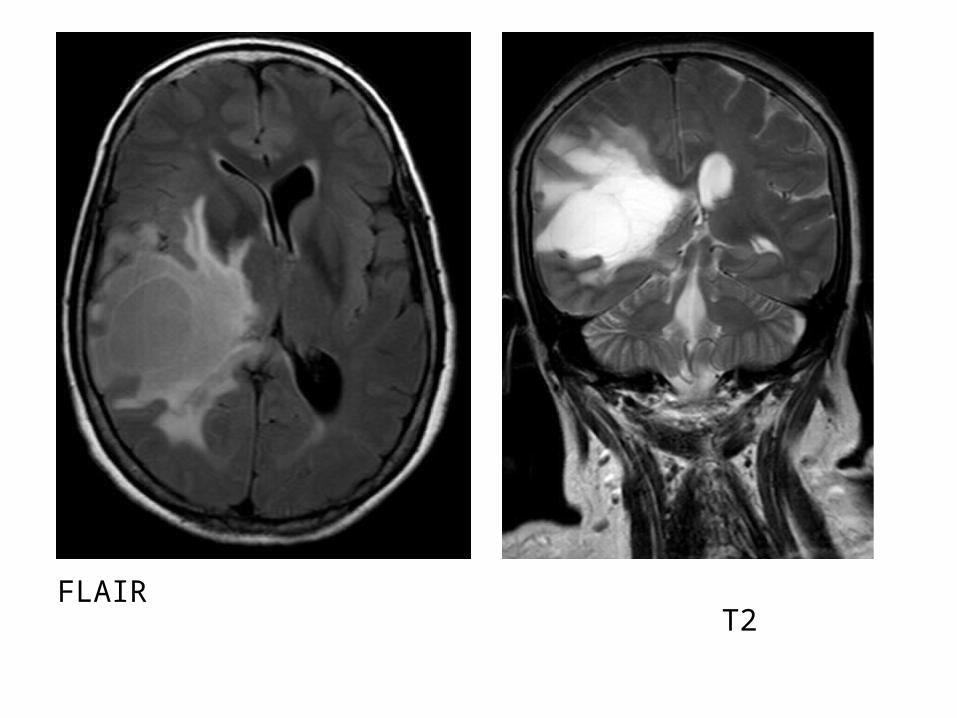
FLAIR T2

T1+C

e) McDonald criteria for MS :-The diagnosis of MS requires elimination of more
likely diagnoses and demonstration of dissemination of lesions in space and time
-In order to make the diagnosis of MS there must be lesions separated in Space (different areas in CNS) & in Time (new lesions across scans)
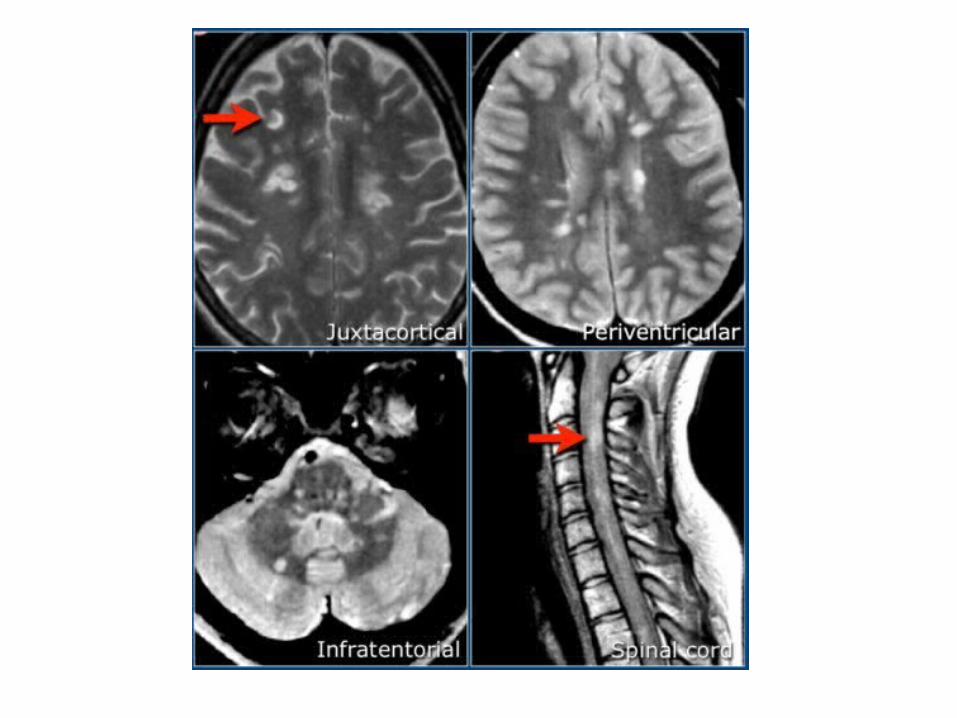
-Dissemination in Space (DIS) is : -≥ 1 T2 lesion in at least two out of four areas of the
CNS : periventricular, Juxtacortical , infratentorial or spinal cord
-Gadolinium enhancement of lesions is not required for DIS

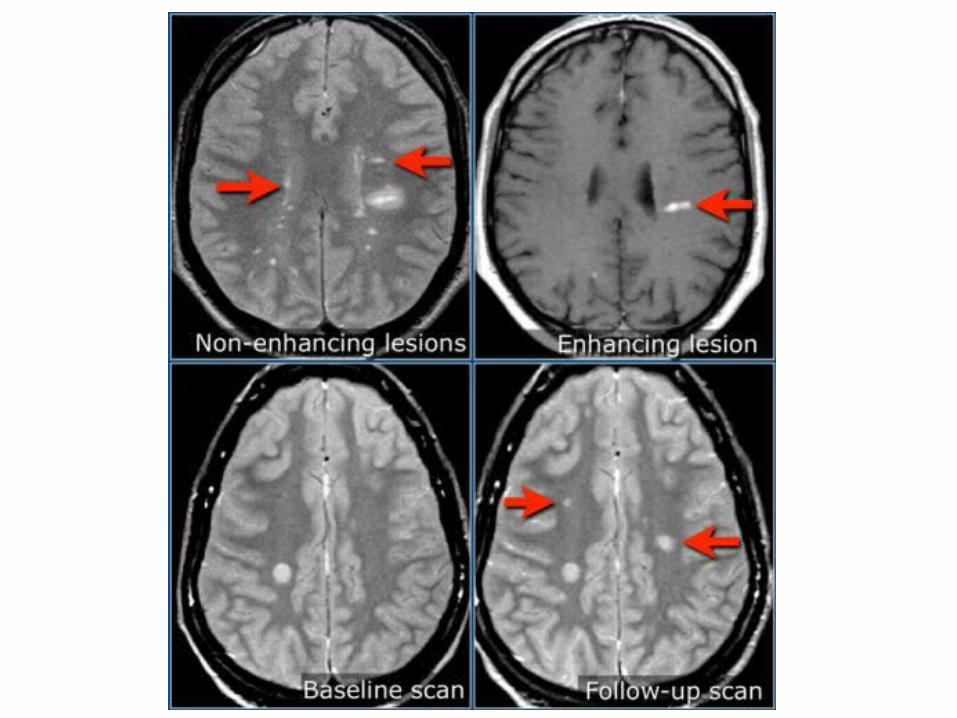
-Dissemination in Time is : -Simultaneous presence of asymptomatic
gadolinium-enhancing and non-enhancing lesions at any time , or
-A new T2 and/or gadolinium-enhancing lesion(s) on follow-up MRI with reference to a baseline scan irrespective of the timing of the baseline MRI , or
-Await a second clinical attack


f) Variants :1-Concentric (Balo) Sclerosis :-Is a very rare variant of MS with pathognomonic alternating
concentric bands of normal & abnormal myelin -It is seen more often in younger patients*T1 : lesions are typically irregular concentric areas of iso and
low signal*T2 : lesions are typically irregular concentric areas alternating
iso/hypointense and hyperintense signal *T1+C : lesions typically show concentric rings of enhancement
and it is implied that the enhancing portions depict active demyelination

(a) T2 show a large right occipitoparietal lesion with alternating concentric hyperintense and isointense rings , there is a small oval lesion on the left , (b) T1+C shows marked and synchronous contrast enhancement of the hyperintense rings seen on the T2
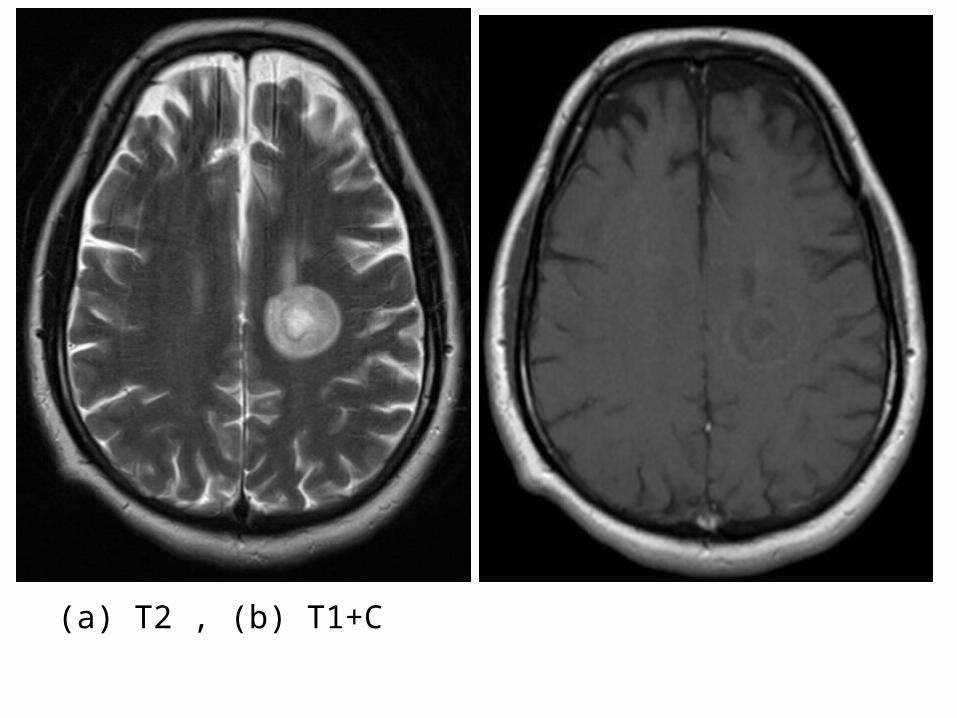
(a) T2 , (b) T1+C
2-Marburg Variant :-Marburg variant of MS is a fulminant
manifestation of MS leading to death within months
3-Devic’s Disease (NMO) :-See later
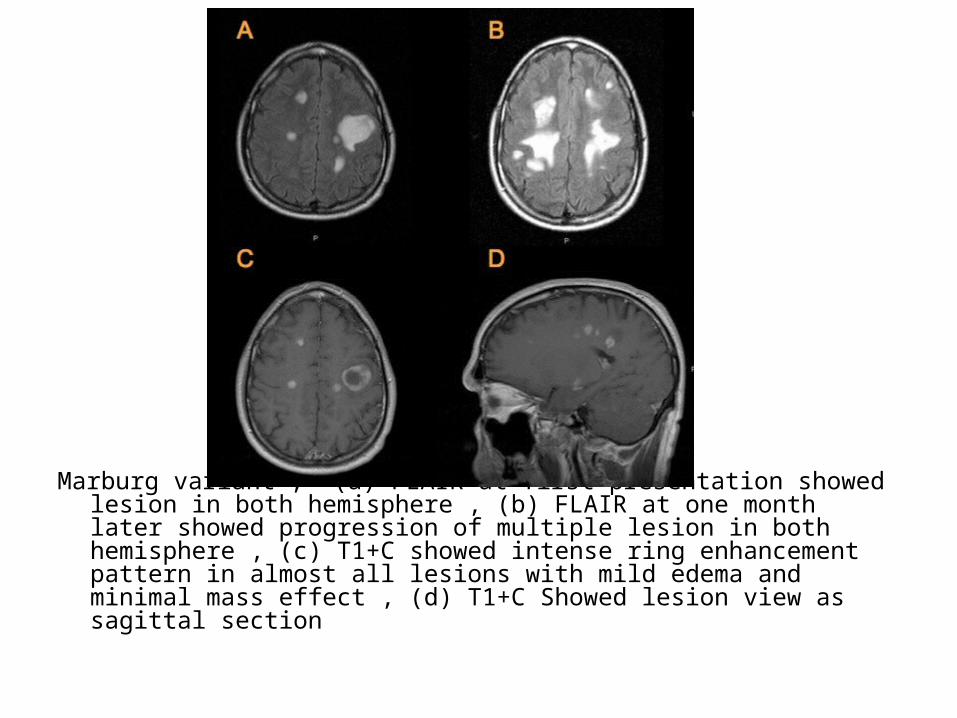
Marburg variant , (a) FLAIR at first presentation showed lesion in both hemisphere , (b) FLAIR at one month later showed progression of multiple lesion in both hemisphere , (c) T1+C showed intense ring enhancement pattern in almost all lesions with mild edema and minimal mass effect , (d) T1+C Showed lesion view as sagittal section
g) Differential Diagnosis :1-Normal Features Mimicking MS2-Vascular3-Other Demyelinating Conditions4-Infection5-Tumor

1-Normal Features Mimicking MS :a) Prominent Perivascular (Virchow-Robin)
spaces:-Peripheral spaces perpendicular to ventricles
but CSF signal on all sequences -May be very large especially in basal ganglia

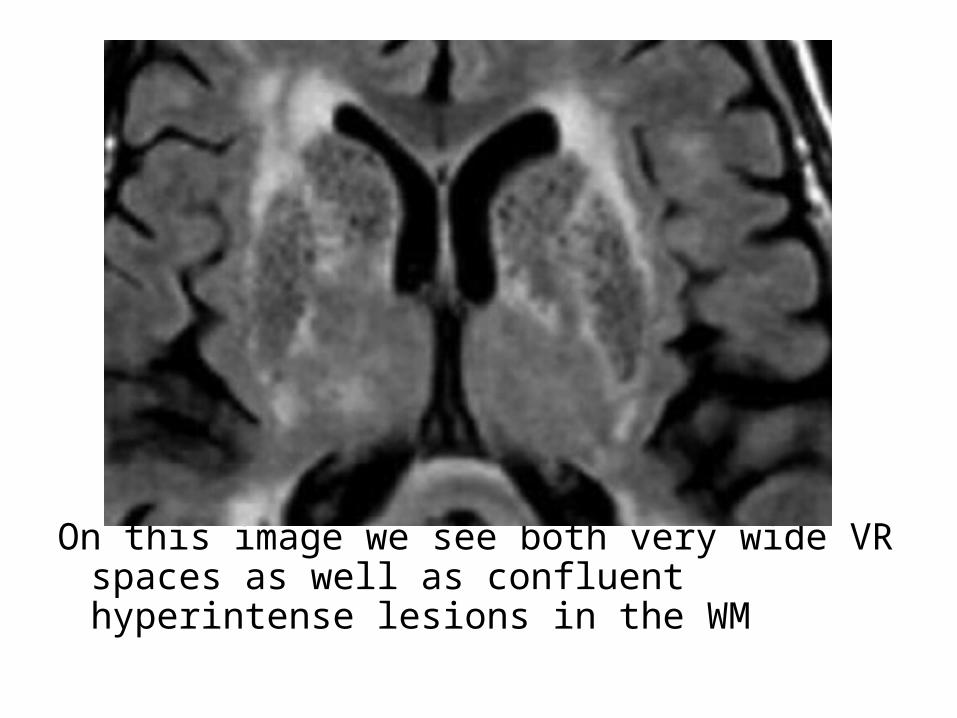
On this image we see both very wide VR spaces as well as confluent hyperintense lesions in the WM

b) Age Related Lesions :-Small peripheral high T2 signal lesions , not all due
to small vessel ischemia-In normal ageing we can see :1-Periventricular caps and bands2-Mild atrophy with widening of sulci and ventricles3-Punctate and sometimes even confluent lesions
in the deep white matter (Fazekas I and II)

Normal aging: Widening of sulci , periventricular caps (arrow) and bands and some punctate WMLs in the deep white matter

2-Vascular :a) Small Vessel Ischemia :-Usually deep and subcortical white matter (not
juxtaventricular, not Juxtacortical and not located in the corpus callosum)
-Discrete or confluent-Commoner if hypertension &/or diabetes-In a patient with vasculitis or ischemia the spinal
cord is usually normal while in a MS patient in more than 90% of the cases it will be abnormal


b) Infarct :-Solitary abnormality with little mass effect
involving white matter & adjacent cortex may be to distinguish from solitary plaque MS , acute infarct will have high signal on DWI & low signal ADC

3-Other Demyelinating Conditions :a) ADEM :-More common in children , typically following a
recent (1-2 weeks prior) viral infection or vaccination
-Involves corpus callosum monophasic in contradistinction to multiple sclerosis which is polyphasic
-ADEM usually fewer larger lesions than MS

-Less likely to be periventricular-Thalamic involvement is rare in MS but not
uncommon in ADEM-More often also affects grey matter , mass
effect unusual-Involvement of the calloso-septal interface is
unusual

b) Central Pontine (Osmotic) Myelinolysis :-MRI low T1 , high T2 signal in central pons with
sparing of periphery , pons swollen-Clinically most usually follows intravenous fluid
correction of chronic hyponatremiac) Post Chemotherapy or Radiotherapyd) Other Toxins :-Alcohol , organic solvents
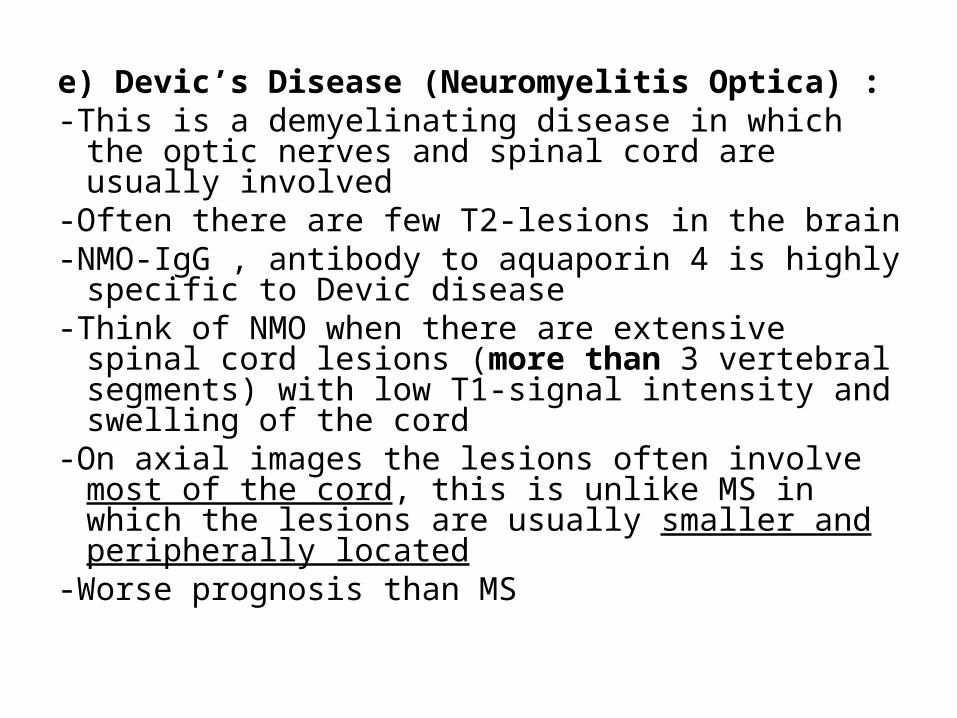
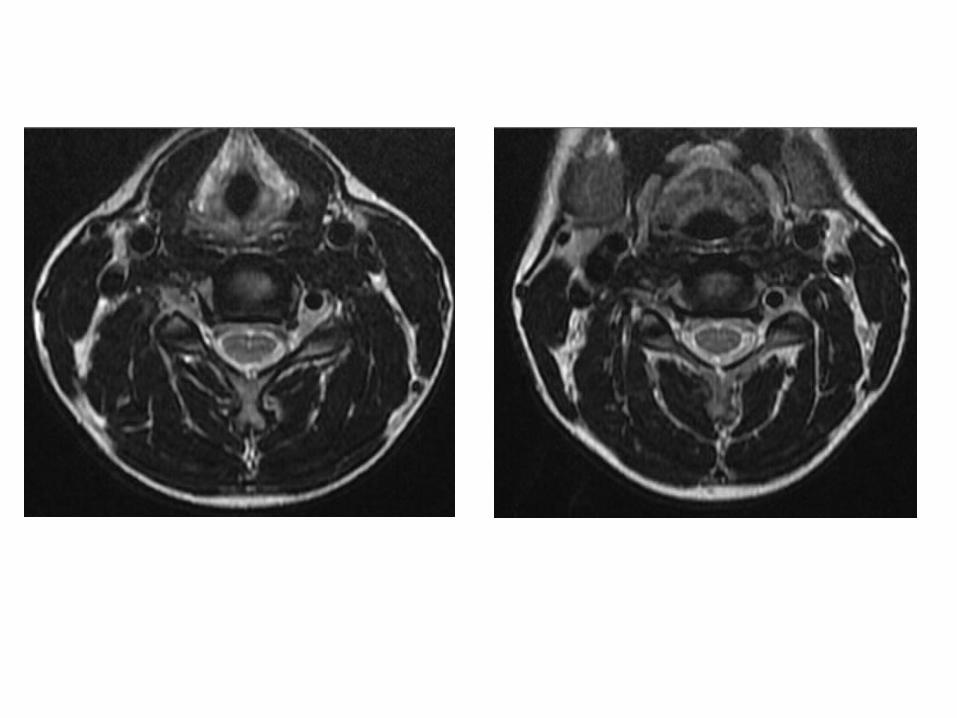
e) Devic’s Disease (Neuromyelitis Optica) :-This is a demyelinating disease in which the optic
nerves and spinal cord are usually involved-Often there are few T2-lesions in the brain-NMO-IgG , antibody to aquaporin 4 is highly
specific to Devic disease -Think of NMO when there are extensive spinal cord
lesions (more than 3 vertebral segments) with low T1-signal intensity and swelling of the cord
-On axial images the lesions often involve most of the cord, this is unlike MS in which the lesions are usually smaller and peripherally located
-Worse prognosis than MS

Devic’s disease , neuritis optica (arrows) , sagittal T2 shows a longitudinally extensive cord lesion with marked swelling

4-Infection :a) Encephalitis :-Viral , HIV and PMLb) Lyme Disease :-White matter lesions resemble MS but
abnormalities also in basal ganglia & brainstem
5-Tumor :a) Glioma :-Large solitary MS plaque may closely mimic
intrinsic tumorb) Multifocal Glioma
2-Acute Disseminated Encephalomyelitis (ADEM) :a) Etiologyb) Incidencec) Locationd) Radiographic Featurese) The Hurst Variant

a) Etiology :-Monophasic acute inflammation and demyelination of
white matter typically following a recent (1-2 weeks prior) viral infection or vaccination
-Grey matter , especially that of the basal ganglia is also often involved
b) Incidence :-Typically , ADEM presents in children or adolescents-The majority of patients will make a full recovery but a
minority will have permanent neurologic sequelae

c) Location :-Lesions are usually bilateral but asymmetrical-Involvement of cerebral cortex , sub cortical
grey matter especially the thalami and the brainstem is not very common but if present are helpful in distinguishing from multiple sclerosis
-Compared to multiple sclerosis , involvement of the calloso-septal interface is unusual
-Similar to MS , ADEM may involve the brain , brainstem or spinal cord

d) Radiographic Features :Imaging findings can be identical to MS1-CT :-The lesions are usually indistinct regions of low
density within the white matter and may demonstrate ring enhancement
2-MRI :*T1 :-Iso to hypointense
*T2 :-Demonstrates regions of high signal with surrounding edema
typically situated in subcortical locations , the thalami and brainstem can also be involved
*T1+C :-Punctate , ring or arc enhancement (open ring sign) is often
demonstrated along the leading edge of inflammation , absence of enhancement does not exclude the diagnosis
*Diffusion :-Restricted diffusion is not seen centrally (usually seen in
cerebral abscesses) but at the advancing rim of demyelination

Deep white matter hyperintensity foci in the left occipital and right parietal lobes in FLAIR sequences

Hyperintense foci in the deep white matter, bilaterally and somewhat symmetrical in FLAIR sequences

Hyperintense asymmetrical bilateral foci in the deep white matter evidenced in the FLAIR sequence in brain and others in the cervical cord , hyperintense on T2
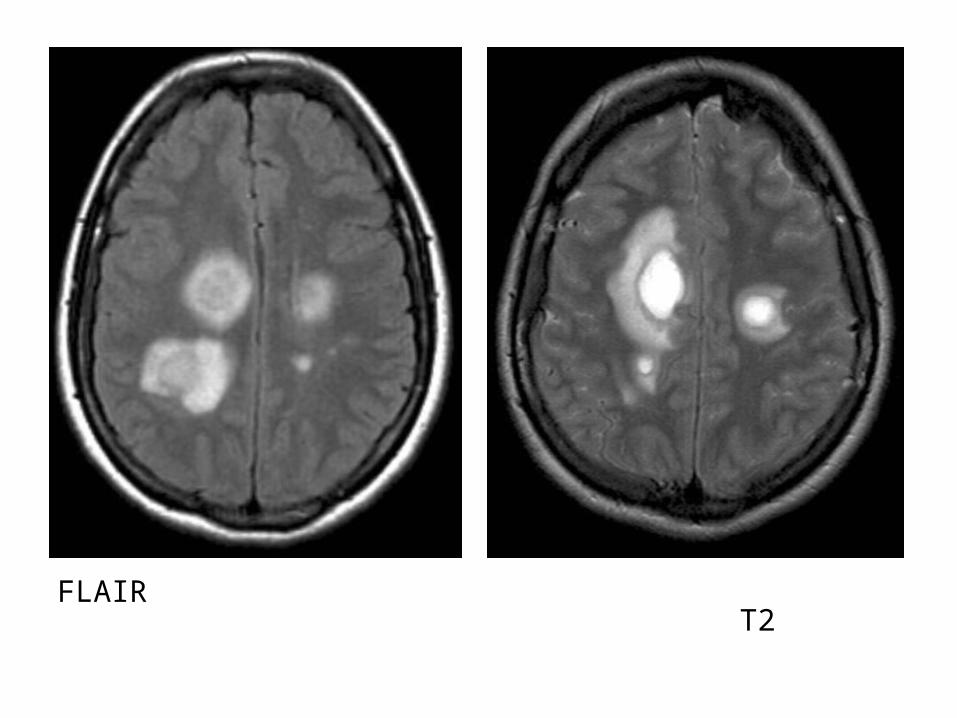
FLAIR T2
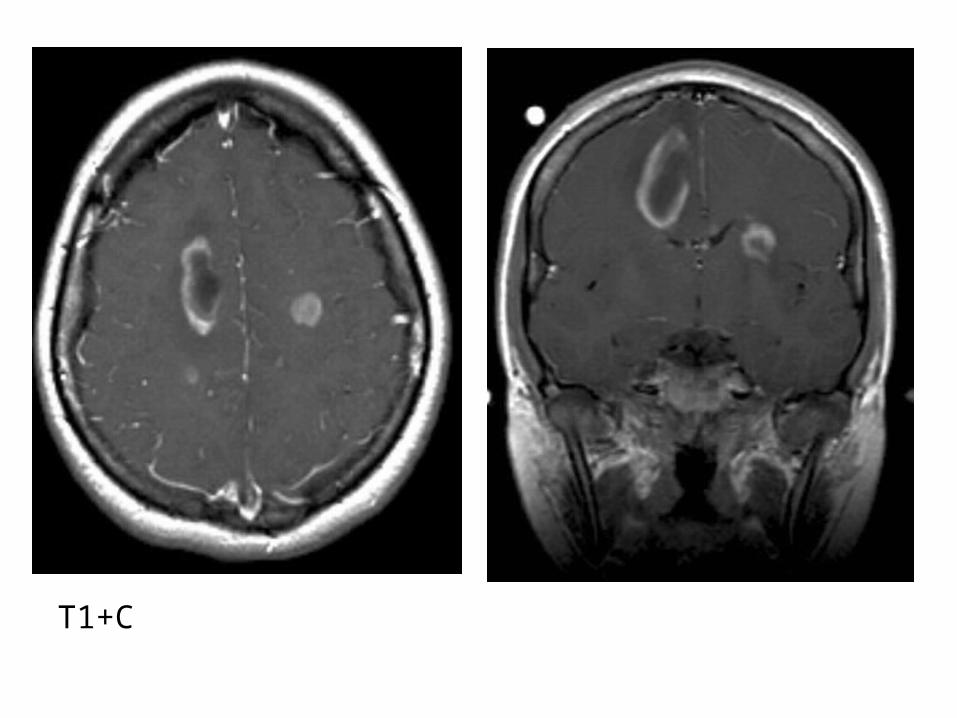
T1+C

Diffusion

e) The Hurst Variant :-The Hurst Variant (acute hemorrhagic
leukoencephalitis) is a rapidly fulminant form of ADEM that leads to death within days
-MRI shows multifocal T2 prolongation and associated white matter hemorrhage which may appear as confluent hematomas

Confluent hyperintense foci in deep white matter and cerebellar hemispheres evidenced in the FLAIR (a,b) , hemorrhagic foci in the left parietal hemisphere and cerebellum shown in GRE* sequence (c)

3-Toxin Related :-Causes :a) Central Pontine Myelinolysisb) Radiation Therapy & Chemotherapyc) Alcoholismd) Paraneoplastic Syndromes

a) Central Pontine Myelinolysis : (CPM) (Osmotic Demyelination)
1-Etiology2-Clinical Picture3-Radiographic Features4-Differential Diagnosis

1-Etiology :-This disease entity is characterized by symmetrical
noninflammatory demyelination of the pons-The exact mechanism of which is unknown , osmotic shifts
due to rapid correction in patients with hyponatremia have been implicated
-CPM is also seen in chronic alcoholics and malnourished patients and in patients undergoing liver transplantation
-Despite the name extrapontine structures can also be affected: basal ganglia, midbrain and subcortical white matter , it is then known as extrapontine myelinolysis (EPM)
2-Clinical Picture :-Clinically CPM presents in a biphasic pattern-The first phase is usually attributable not to the
demyelination but rather to the inciting electrolyte abnormality with patients being acutely encephalopathic
-Following rapid reversal of this abnormality the patient transiently improves before progressing onto the classic CPM features 2-3 days later
-These consist of :a) Spastic quadriparesisb) Pseudobulbar palsyc) Changes in levels of consciousnessd) Coma or death-Extrapontine lesions are common in putamina
and thalami
3-Radiographic Features :a) CT :-May demonstrate low attenuation crossing the
midline in the lower pons , no mass effect , no enhancement

CT shows large central hypoattenuating focus in the central pons

b) MRI :-May be negative initially on patient presentation
but lesions become apparent on follow-up scans*T1 :-Mildly or moderately hypointense*T2 :-Diffuse central pontine hyperintensity , sparing the
periphery and corticospinal tracts (symmetric trident shaped or bat wing shaped area of increased signal intensity in the central pons)

*T1+C :-No enhancement*PD & FLAIR :-Hyperintense*DWI :-The earliest change is seen on DWI with
restriction in the lower pons , this is seen within 24 hours of the onset of quadriplegia

FLAIR shows the classic trident-shaped pontine signal intensity abnormality
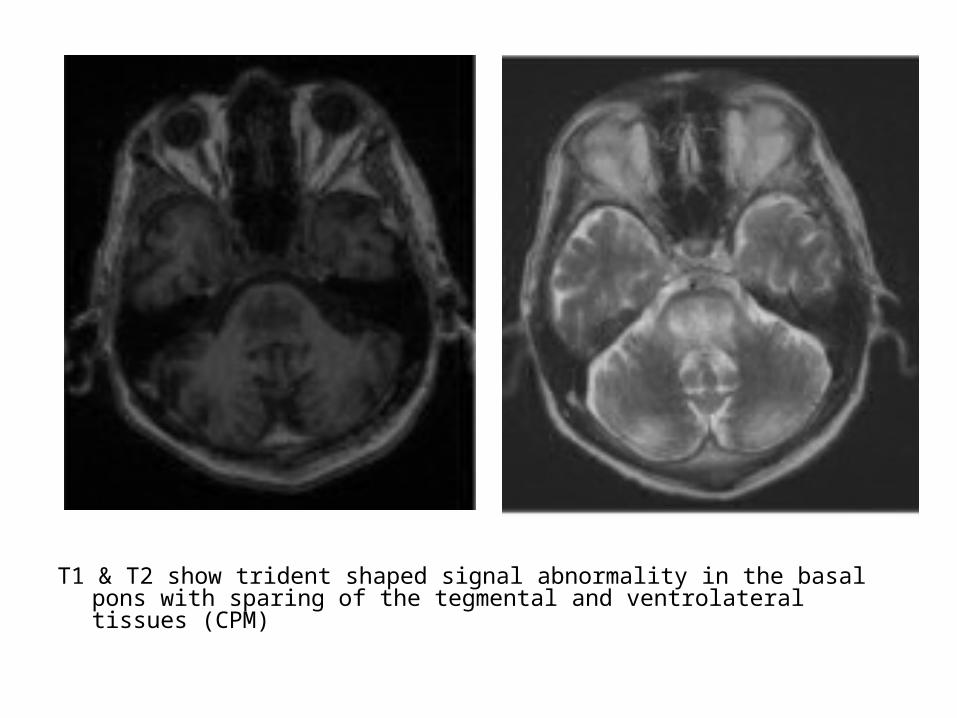
T1 & T2 show trident shaped signal abnormality in the basal pons with sparing of the tegmental and ventrolateral tissues (CPM)

T1 T2


Coronal FLAIR shows increased signal in the hippocampi , lateral putamen and thalami bilaterally (EPM)

CPM with EPM
4-Differential Diagnosis :a) Demyelination including multiple sclerosis b) Infarction from basilar perforators can be
central although usually brainstem infracts stop at the midline
c) Pontine neoplasms including astrocytomas
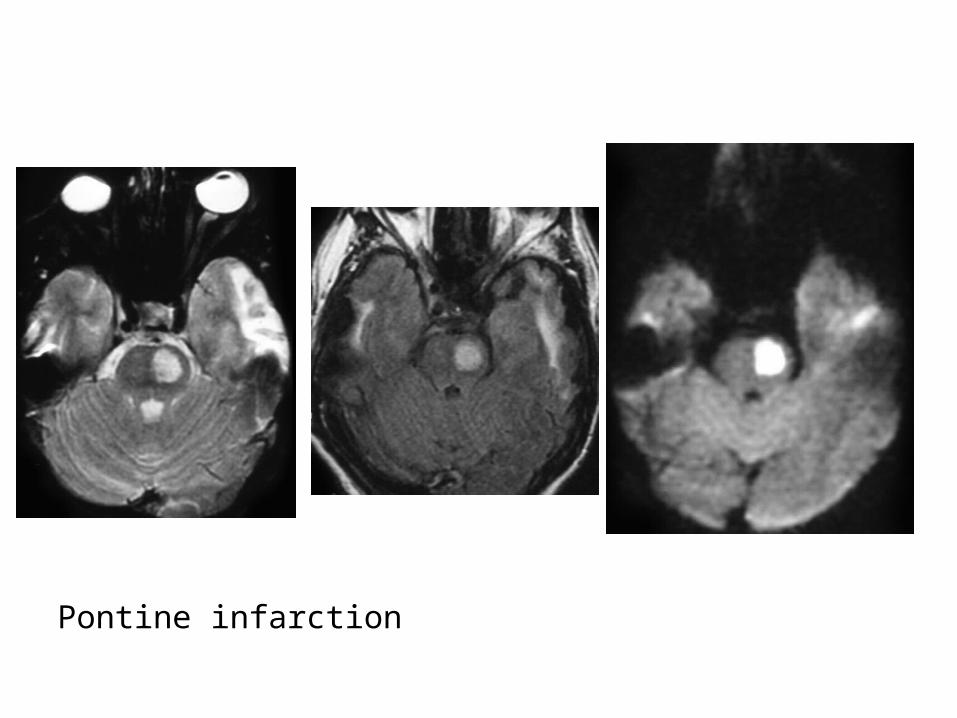
Pontine infarction
b) Radiation / Chemotherapy Induced CNS Abnormalities :
1-Causes2-Types

1-Causes :-Cyclosporine causes posterior confluent WM
hyperintensity , patients often present with blindness
-Fluorouracil (5-FU) , methotrexate (systemic)-Intrathecal methotrexate-Radiation and chemotherapy potentiate each
other's toxic effects , intrathecal methotrexate and whole brain radiation lead to diffuse deep WM T2 hyperintensity
2-Types :a) Acute Changes :-Occur during or immediately after course of radiation , resolve after
therapy ends-Changes usually represent mild edema & inflammationb) Chronic Changes :-Occurrence :*6 to 8 months after nonfractionated therapy : proton beam ,
stereotactic therapy*2 years after fractionated conventional radiation-May be permanent-Pathology : occlusion of small vessels , focal demyelination ,
proliferation of glial elements & mononuclear cells and atrophy-Radiographic Features :CT : HypodenseT2 : Hyperintense
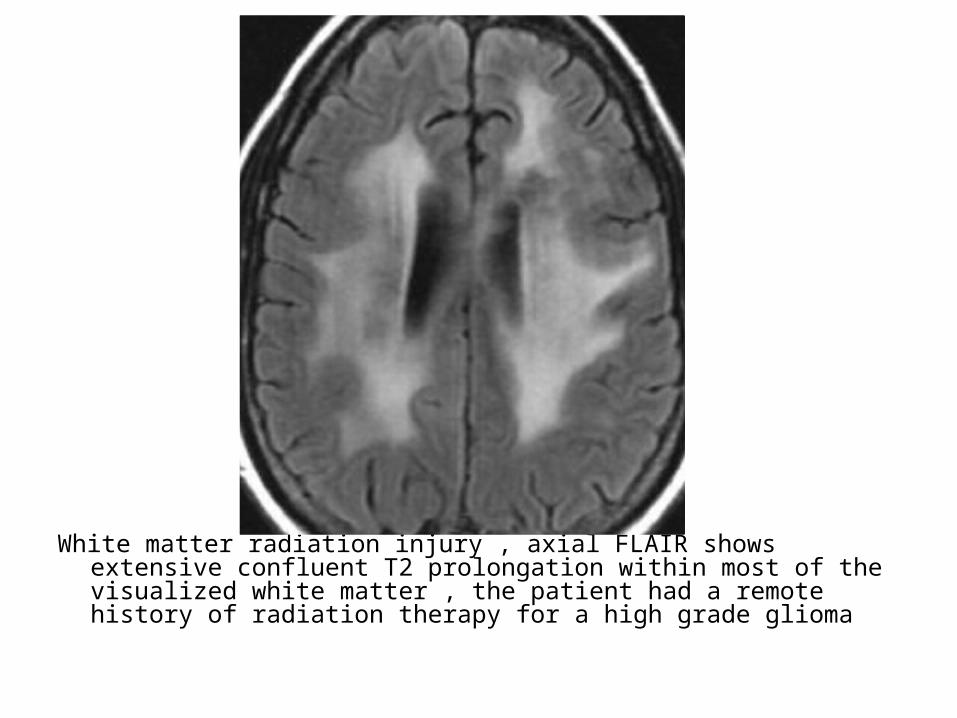
White matter radiation injury , axial FLAIR shows extensive confluent T2 prolongation within most of the visualized white matter , the patient had a remote history of radiation therapy for a high grade glioma

WM changes after treatment with radiation and temozolamide
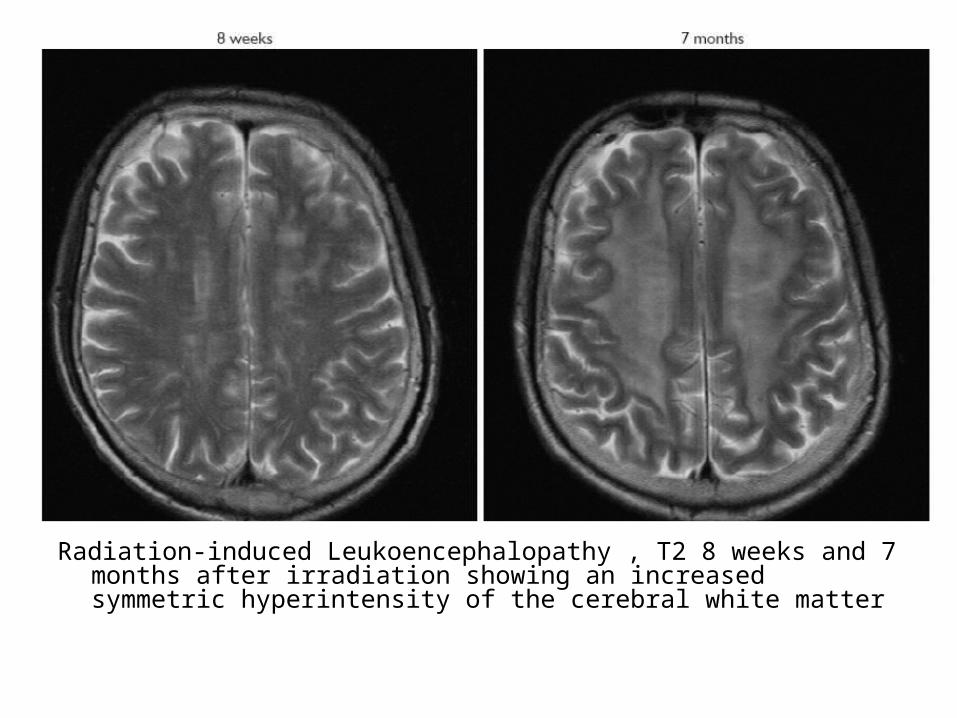
Radiation-induced Leukoencephalopathy , T2 8 weeks and 7 months after irradiation showing an increased symmetric hyperintensity of the cerebral white matter
c) The Late Delayed Phase :-Months to years after radiation-It can present as white matter injury or a focal
radiation necrosis-Mass effect , edema & enhancement are
common -Radiation necrosis should be considered in the
differential of a ring enhancing mass in a patient with history of prior radiation

Radiation necrosis , ring enhancing lesion

c) Alcoholism :1-Marchiafave-Bignami :-Is a fulminant demyelinating disease of the corpus
callosum seen in male alcoholics2-Wernicke Encephalopathy :-Is an acute syndrome of ataxia , confusion & occulomotor
dysfunction which may be caused either by alcoholism (due to thiamine deficiency) or generalized metabolic disturbances such as bariatric surgery
-On imaging, there is T2 prolongation &possible enhancement within the mamillary bodies & medial thalamus m the non-alcoholic form may also affect the cortex

Marchiafava-Bignami , (a) FLAIR shows T2 hyperintensity confined to corpus callosum with restricted diffusion on Dw images (b)

Marchiafava-Bignami

Wernicke Encephalopathy , FLAIR shows marked hyperintensity of the tectal region (white arrows) , periaqueductal area (black arrowheads) and mamillary bodies (white arrowheads)

Wernicke Encephalopathy

4-Vascular White Matter Disease :a) Posterior Reversible Encephalopathy
Syndrome (PRES)b) Cerebral Autosomal Dominant Arteriopathy
with Subcortical Infarcts & Leukoencephalopathy (CADASIL)
c) Vasculitisd) Microangiopathy

a) Posterior Reversible Encephalopathy Syndrome (PRES) :
-Imaging shows symmetric regions of subcortical white matter abnormality, vasogenic edema (hypoattenuation on CT & T2 prolongation on MRI) especially in the posterior circulation (occipital & parietal lobes and posterior fossa), mild mass effect & enhancement can be seen
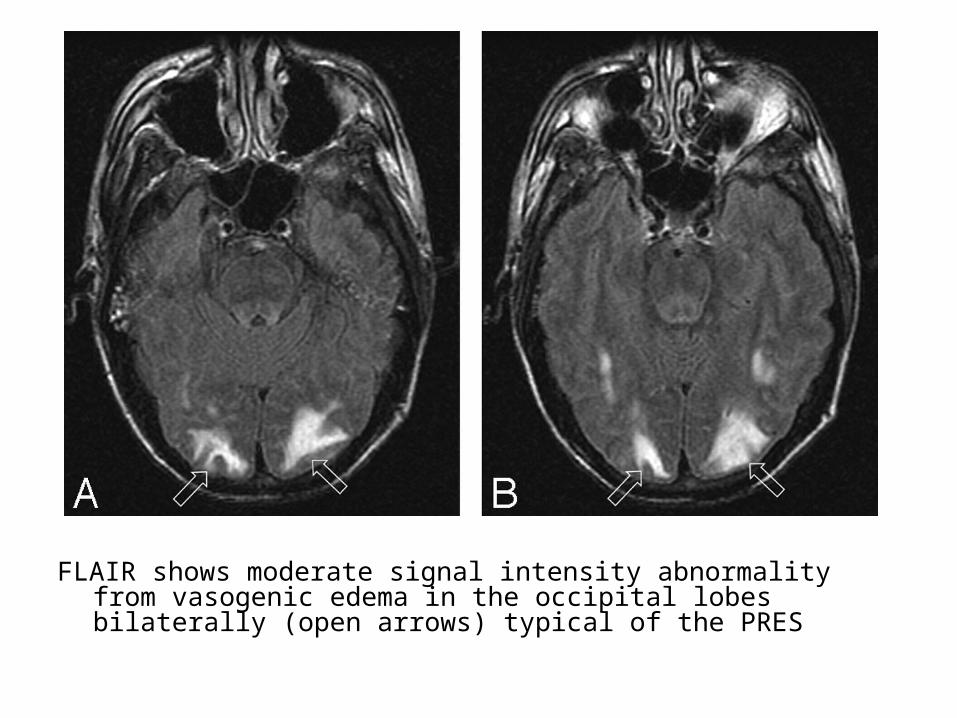
FLAIR shows moderate signal intensity abnormality from vasogenic edema in the occipital lobes bilaterally (open arrows) typical of the PRES
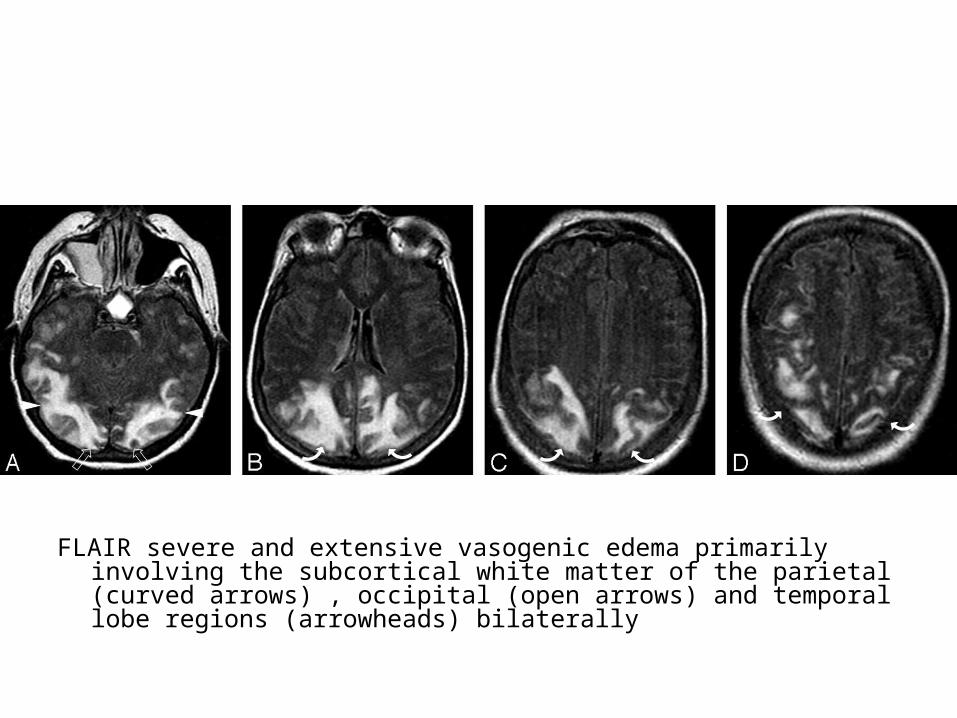
FLAIR severe and extensive vasogenic edema primarily involving the subcortical white matter of the parietal (curved arrows) , occipital (open arrows) and temporal lobe regions (arrowheads) bilaterally

b) Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts & Leukoencephalopathy (CADASIL) :
-CADASIL is an inherited disease characterized by recurrent stroke , migraine , subcortical dementia and pseudobulbar palsy due to small vessel arteriopathy
-The clinical hallmark of CADASIL is recurrent episodes of stroke or TIAs which are nearly always found to be subcortical in the white or basal ganglia on imaging , there is often associated migraine , it may eventually lead to dementia

-MRI shows symmetric foci of T2 prolongation in the subcortical white matter which may become confluent as the disease progresses
-Anterior temporal lobe or paramedian frontal lobe foci of T2 prolongation are highly sensitive & specific for CADASIL , especially with clinical history of migraine
-Although the symmetric subcortical pattern is similar to PRES , the distribution in CADASIL is anterior circulation

Axial FLAIR (A-C) & T2* gradient (D) of CADASIL patients , complete MR imaging spectrum of CADASIL : confluent hyperintensities (A-C) , lacunar infarcts (A, arrow) , subcortical lacunar lesions (B, arrow) and microbleeds (D, arrow)
c) Vasculitis :-CNS vasculitis is a group of vascular inflammatory
disorders that primarily affects the small vessels, in particular the leptomeningeal & small parenchymal vessels
-Etiology : SLE , PAN , giant cell arteritis & Sjogren syndrome
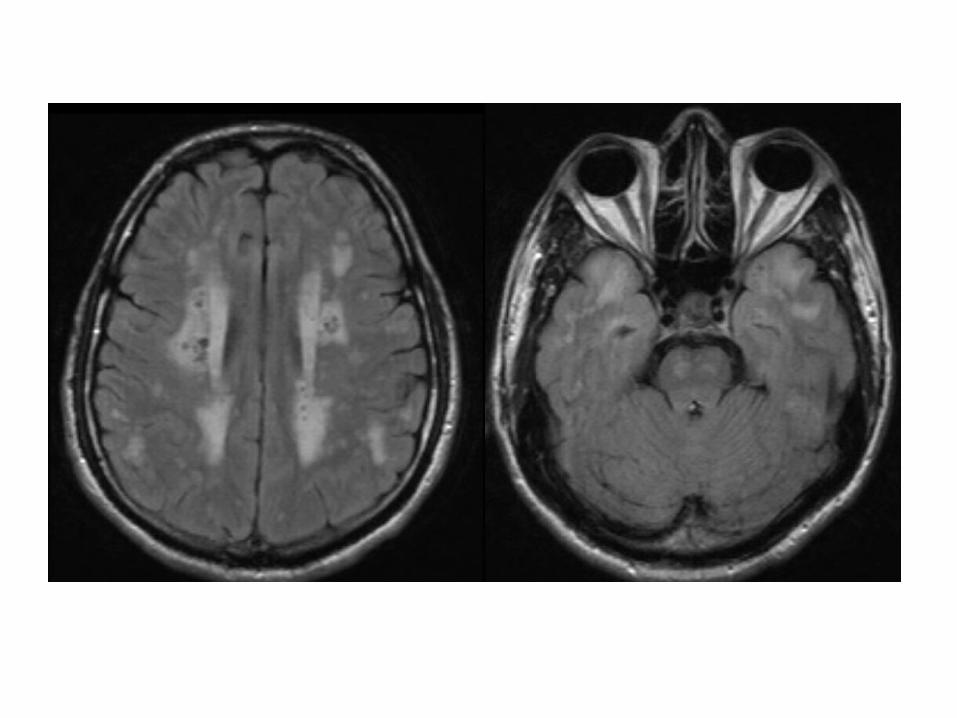
-MRI shows numerous small focal areas of T2 prolongation in subcortical & deep white matter
-Although the appearance may be similar to MS , foci of hemorrhage (best seen on GRE or SWI) may be present in vasculitis which would not be seen in MS
-CTA & catheter angiography are more sensitive and show a beaded irregular appearance to the cerebral vessels

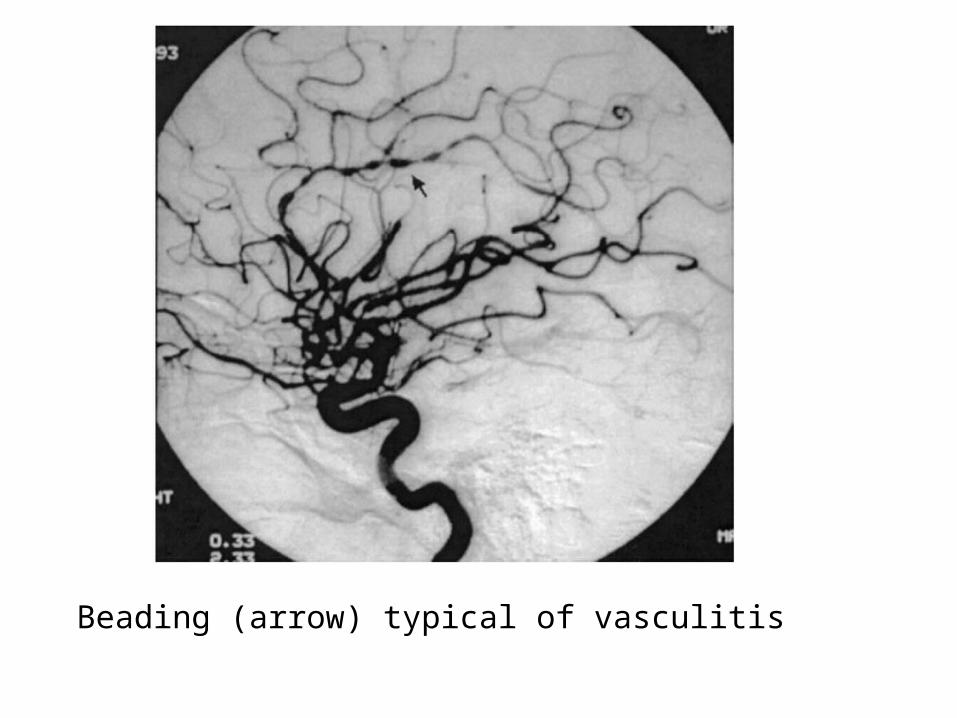
Beading (arrow) typical of vasculitis
d) Microangiopathy :-Microangiopathy describes age-related chronic axonal
loss , gliosis & ischemic changes seen in up to 80 % of elderly individuals
-Never involves the corpus callosum , if involvement of the corpus callosum is present , an alternative diagnosis should be considered , such as MS or neoplasm
-Binswanger disease represents the combination of dementia & severe microangiopathy


5-Infectious (Viral) White Matter Disease :a) Progressive Multifocal Leukoencephalopathy
(PML)b) Subacute Sclerosing Panencephalitis (SSPE)

a) Progressive Multifocal Leukoencephalopathy (PML) :
1-Incidence2-Radiographic Features3-Differential Diagnosis

1-Incidence :-PML is a demyelinating disease of
immunocompromised patients caused by reactivation of JC virus , there is progressive demyelination with lack of inflammatory response
-PML occurs most commonly in AIDS patients (PML is an AIDS defining illness) but can also be seen in patients with malignancy , status post organ transplant or with autoimmune disorders

2-Radiographic Features :1-Asymmetric multifocal white matter lesions that may
become confluent2-No mass effect or enhancement3-The arcuate (subcortical U) fibers are typically involved
, arcuate fibers are myelinated tracts at the gray-white junction that connect cortex to cortex
4-A posterior location has been used as an imaging sign favorable to the diagnosis of PML , particularly when lesions have been observed in the occipital or parietal lobes , posterior centrum semiovale is the most common site
-Approximately 1 in 1000 patients with MS treated with natalizumab (Tysabri) may have superimposed PML and it may be difficult to distinguish between MS & PML , diagnosis is made by PCR for JC virus DNA in CSF

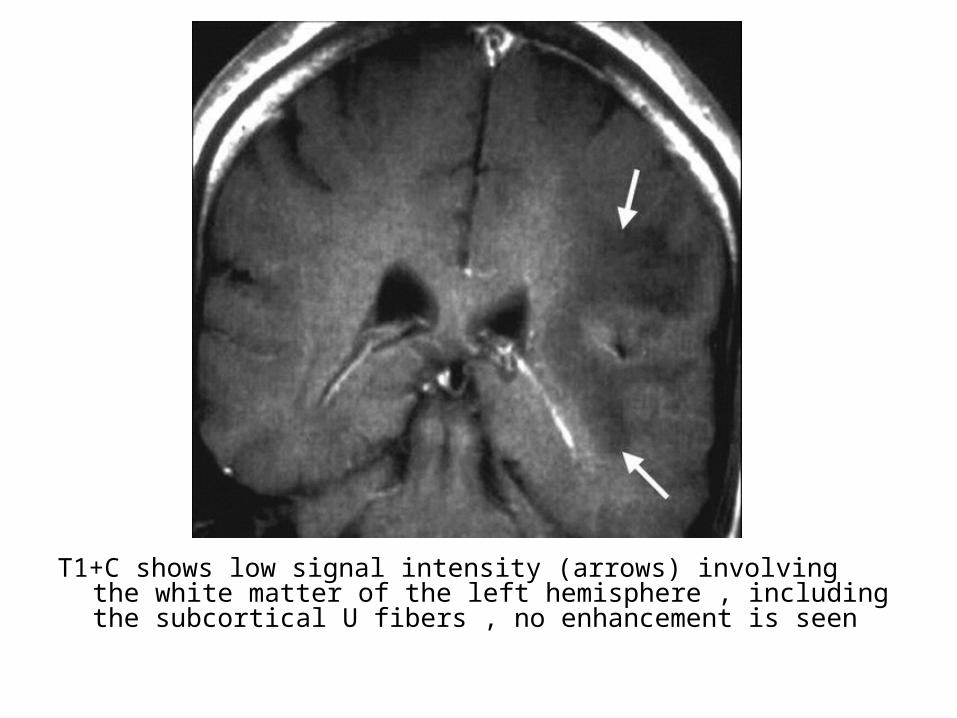
T1+C shows low signal intensity (arrows) involving the white matter of the left hemisphere , including the subcortical U fibers , no enhancement is seen

(a) NECT shows focal area of low attenuation within the white matter of the right hemisphere , the subcortical U fibers are involved and no mass effect is present , T2 shows hyperintensity involving the white matter of the right hemisphere , including the subcortical U fibers , no mass effect is seen , (c) T1+C shows hypointensity and no evidence of associated enhancement

(A) T1 shows low signal intensity lesions , (B) T2 shows hyperintense lesions in the centrum semiovale bilaterally , subcortical white matter and corpus callosum , note the asymmetrical white matter involvement with the left cerebral hemispheric white matter more severely affected



T2 shows bilateral hyperintense lesions in the cerebellar white matter (right greater than left)

PML in MS patient on natalizumab

3-Differential Diagnosis : From HIV Encephalitis-In an AIDS patient , the primary differential for white
matter lesions is PML & HIV encephalitis , in contrast to PML , HIV-encephalitis is usually bilateral and symmetric , spares the subcortical white matter and is associated with cerebral atrophy :
*Diffuse bilateral involvement with sparing of subcortical white matter and cerebral atrophy >> HIV encephalitis
*Asymmetric involvement , involvement of subcortical white matter and lack of atrophy >> PML
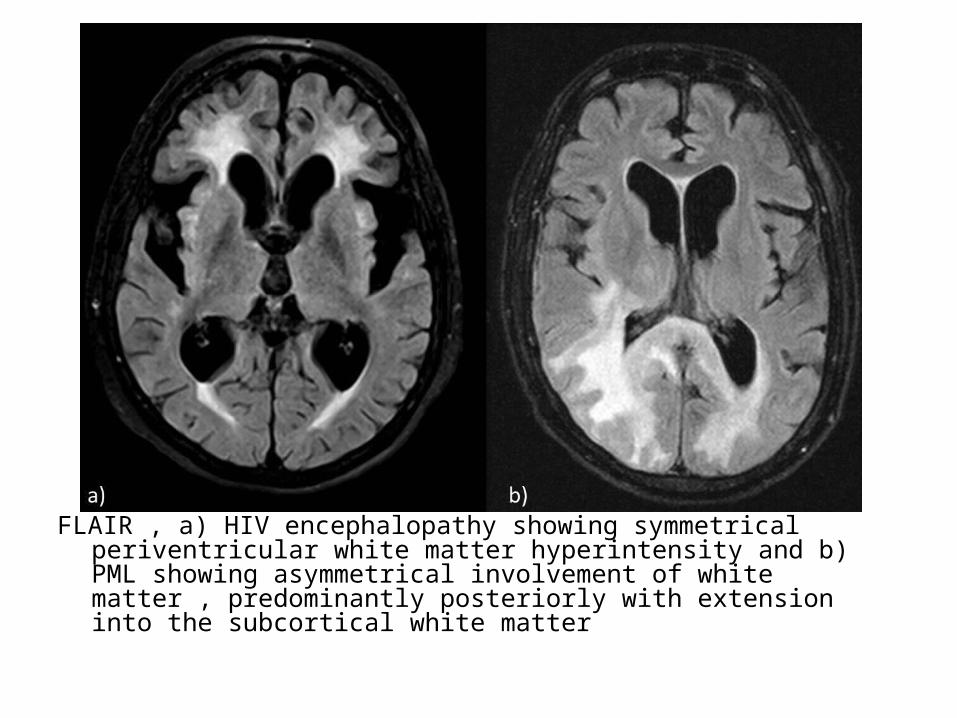
FLAIR , a) HIV encephalopathy showing symmetrical periventricular white matter hyperintensity and b) PML showing asymmetrical involvement of white matter , predominantly posteriorly with extension into the subcortical white matter

b) Subacute Sclerosing Panencephalitis (SSPE) :-SSPE is a demyelinating disease caused by
reactivation of measles virus , usually after a long latent period
-Imaging shows periventricular white matter lesions , but in distinction to the other white matter entities , SSPE lesions tend to have surrounding edema & mass effect
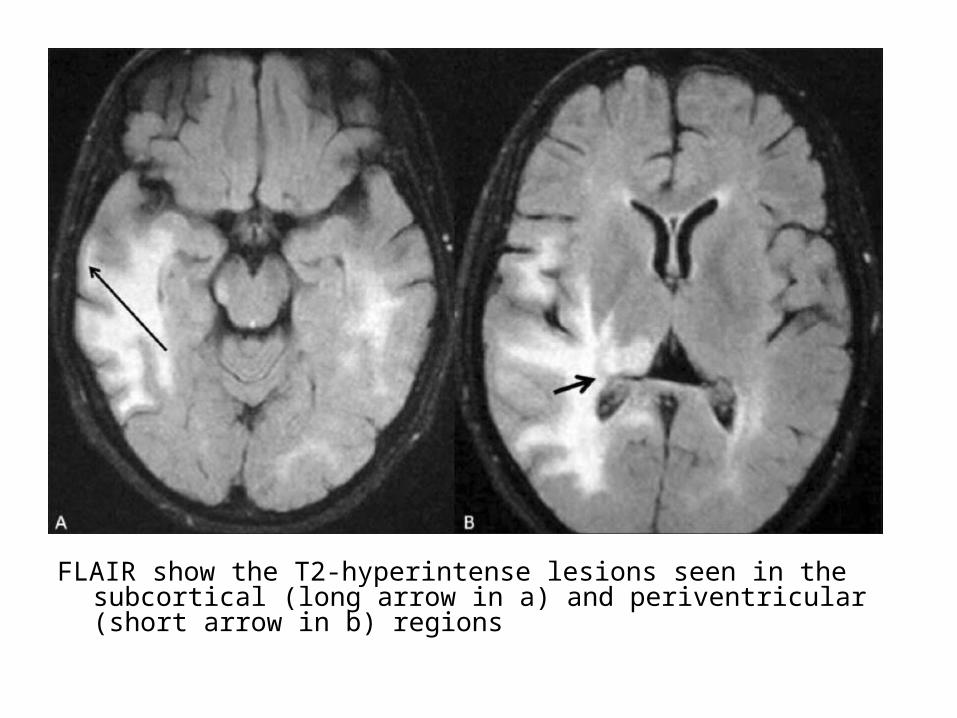
FLAIR show the T2-hyperintense lesions seen in the subcortical (long arrow in a) and periventricular (short arrow in b) regions

b) Dysmyelinating disease : (Leukodystrophies)-Hereditary inborn errors of myelin synthesis ,
maintenance or degradation-MRS shows :Evidence of neuronal loss manifested by a
decrease in the NAA peak and an elevation in the lactate peak
1-Lysosomal Disorders2-Peroxisomal Disorders3-Mitochondrial Disorders4-Aminoacidopathies5-Idiopathic
1-Lysosomal Disorders :a) Metachromatic Leukodystrophy b) Krabbe’s (Globoid) Leukodystrophy

a) Metachromatic Leukodystrophy : (MLD)1-Incidence2-Radiographic Features

1-Incidence :-Most common hereditary leukodystrophy-Infantile form is most common-Age at presentation : <2 years in 80%-Death in childhood

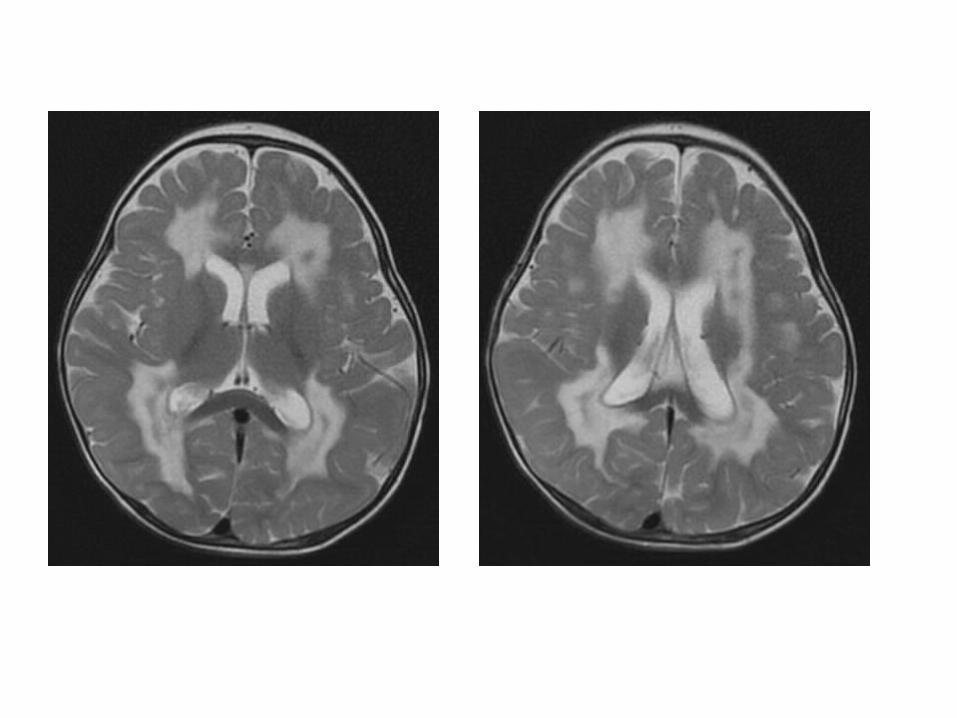
2-Radiographic Features :-Bilateral symmetrical confluent areas of signal change
in periventricular white matter with sparing of subcortical U fibers
-CT : hypodense-T2 : hyperintense (Stripe sign or Tigroid pattern , results
from dark spots or stripes (spared perivascular white matter) within bright demyelinated periventricular white matter on T2
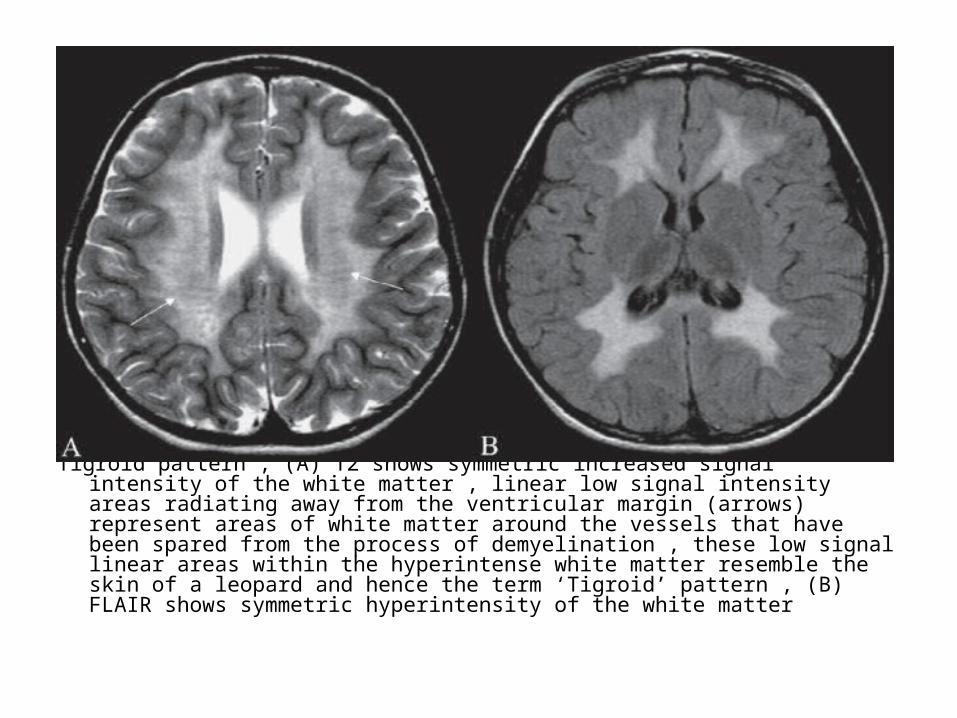
Tigroid pattern , (A) T2 shows symmetric increased signal intensity of the white matter , linear low signal intensity areas radiating away from the ventricular margin (arrows) represent areas of white matter around the vessels that have been spared from the process of demyelination , these low signal linear areas within the hyperintense white matter resemble the skin of a leopard and hence the term ‘Tigroid’ pattern , (B) FLAIR shows symmetric hyperintensity of the white matter


b) Krabbe’s (Globoid) Leukodystrophy :1-Incidence2-Radiographic Features
1-Incidence :-The disorder is present at birth -It is clinically classified into :1-Early infantile form : which presents between 1 to 12
months of age2-Late infantile form (early childhood form) :
presenting between 1-3 yrs of age3-Juvenile variety : manifesting in older children-The early infantile form is most common and the late
onset form is rare

2-Radiographic Features :-The thalami , central white matter and cerebellum
show hyperdensities on CT which are seen on MR as decreased signal intensity on T2 and increased on T1
-MR also shows abnormalities in the periventricular white matter which are non specific and resemble those seen in other dysmyelinating disorders
-T1+C : no contrast enhancement

-N.B. :*The D.D. of CT hyperdensities of basal ganglia
and cerebellum include :1-Alexander's disease2-Fahr's syndrome3-Tuberous sclerosis4-Cockayne's disease5-Sandhoff and Tay Sach's disease

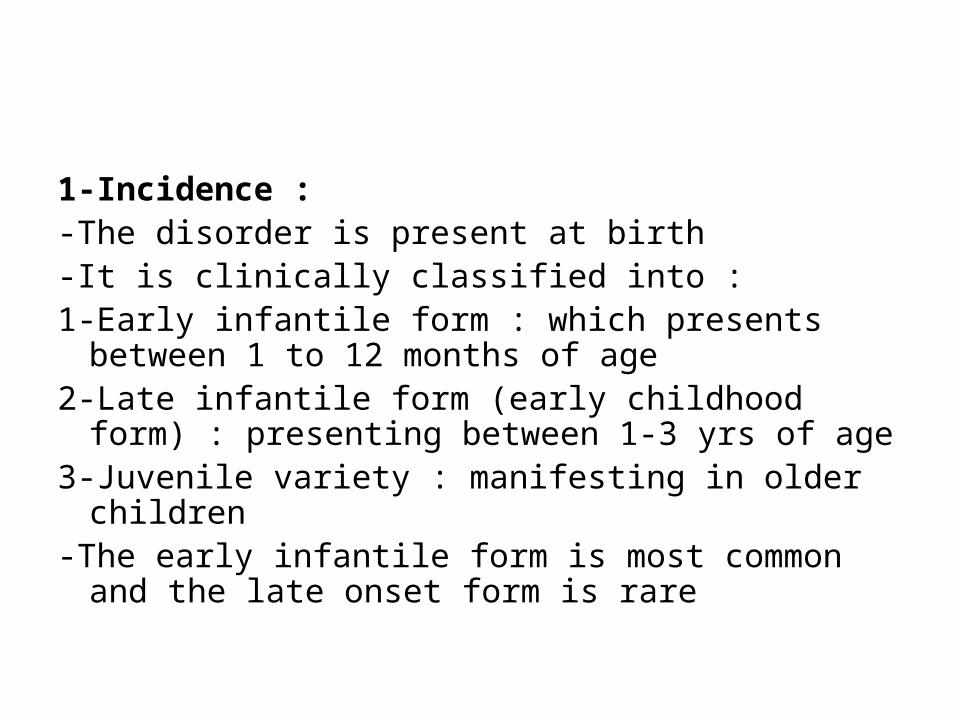
CT without contrast shows bilaterally symmetrical hyperdensities in thalami , basal ganglia & cerebellar white matter with ventricular dilatation & cerebral & cerebellar atrophy

CT+C shows no significant contrast enhancement in the areas of hyperdensity
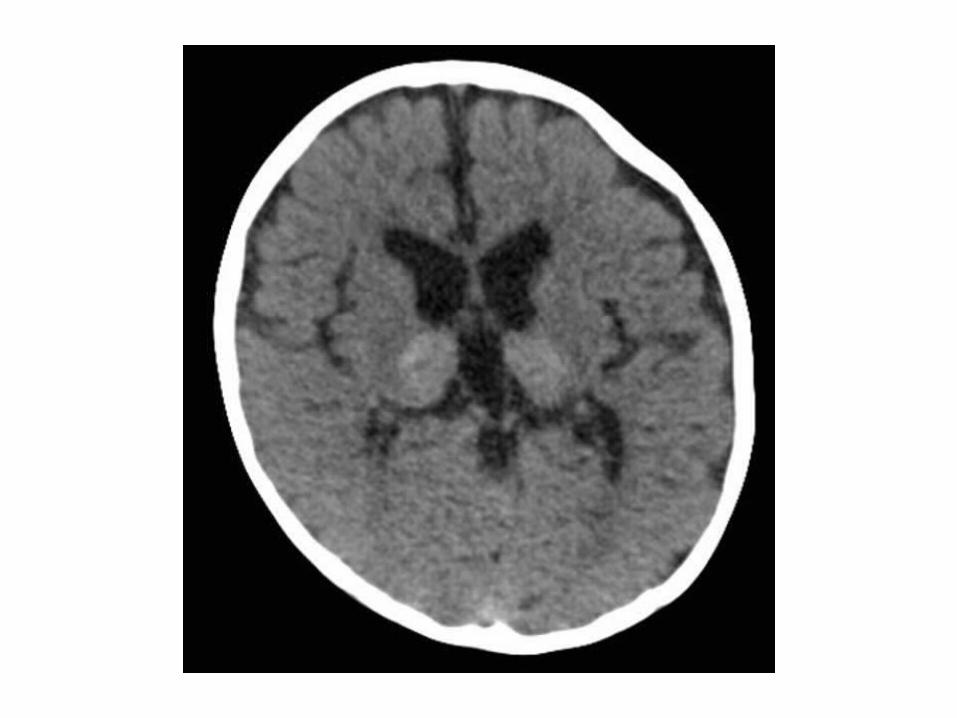
T1 : basal ganglia and thalami are hyperintense
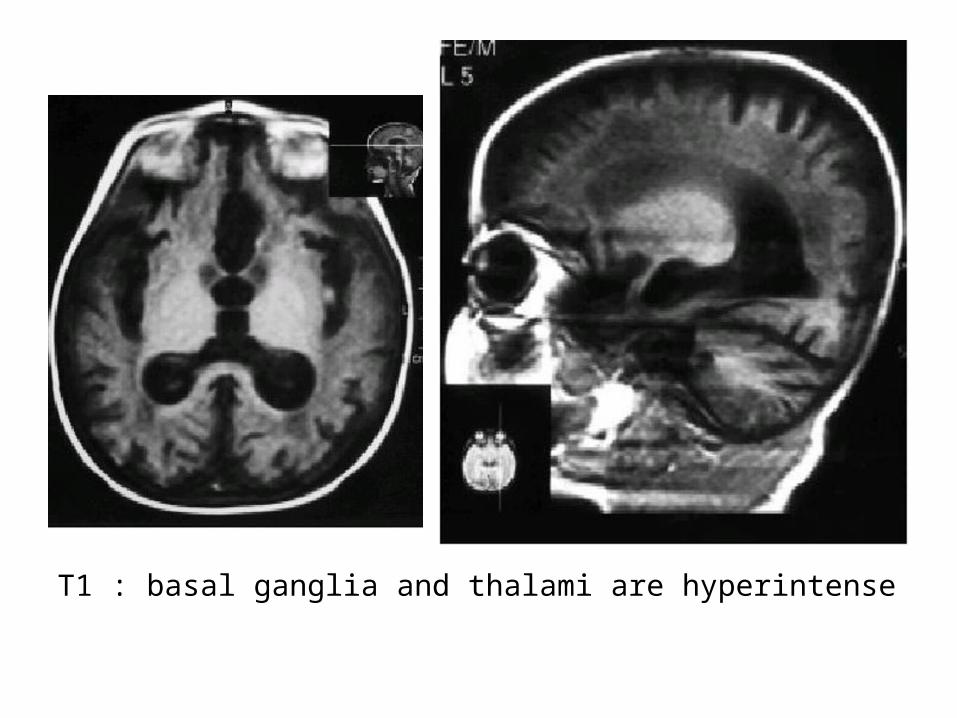
T2 shows hypointensity in both thalami & basal ganglia

FLAIR shows hyperintensity of the periventricular white matter

2-Peroxisomal Disorders :a) Adrenoleukodystrophyb) Zellweger’s (Cerebrohepatorenal) Syndrome
a) Adrenoleukodystrophy : (ALD)1-Incidence2-Radiographic Features
1-Incidence :-One of the x-linked congenital dysmyelinating diseases-Due to its X-linked inheritance it classically affects young males-The cerebral white matter is typically split into three different
zones :1-Central (inner) zone : irreversible gliosis and scarring2-Intermediate zone : active inflammation and breakdown of the
BBB3-Peripheral (outer) zone : leading edge of active demyelination
2-Radiographic Features :a) Distributionb) Signal Intensitiesc) End stage
a) Distribution :-Symmetrical-Disease starts in occipital regions and spreads
anteriorly to involve frontal lobes and across corpus callosum

b) Signal Intensities :1-CT :-Low attenuation ( edema and gliosis )-Enhancement of leading edge ( inflammation )2-MRI :-T1 : hypointense-T2 : hyperintense (central zone) with hypointense
intermediate and peripheral zone-T1+C : Leading edge enhancementc) End stage : atrophy

T1+C

b) Zellweger’s (Cerebrohepatorenal) Syndrome:1-Incidence2-Radiographic Features

1-Incidence :-It results from an abnormality in peroxisomal
metabolism-It is the most severe of the peroxisomal
disorders-It primarily affects the CNS , Hepatic and Renal
systems

2-Radiographic Features :a) CNS :-Ventricular enlargement-Abnormal gyration patterns :*Pachygyria*Polymicrogyriab) Liver : Hepatomegalyc) Kidney : Hyperechoic kidneys
3-Mitochondrial Disorders :a) MELAS syndrome (mitochondrial myopathy ,
encephalopathy , lactic acidosis , strokelike episodes)
b) MERRF syndrome (myoclonic epilepsy with ragged red fibers)
c) Leigh disease

-Mitochondrial Cytopathies (Leigh’s Disease) :1-Incidence2-Radiographic Features
1-Incidence :-Leigh’s Disease is a mitochondrial disease that
results from a disorder in the respiratory chain production of adenosine triphosphate
-More in children-Progressive neurodegenerative disorder and
invariably leads to death in childhood
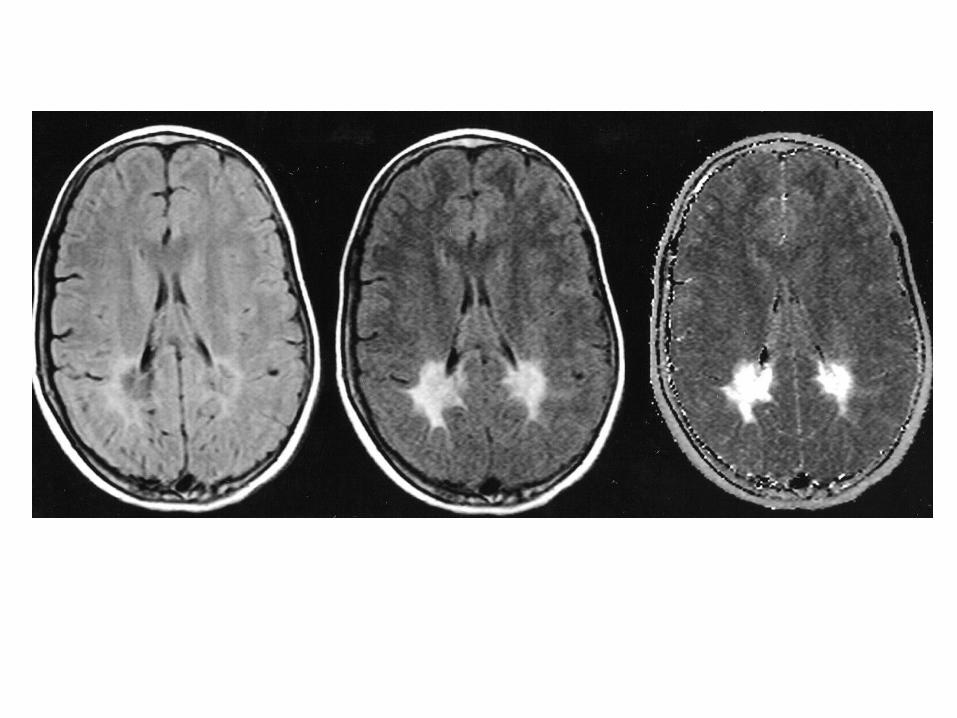
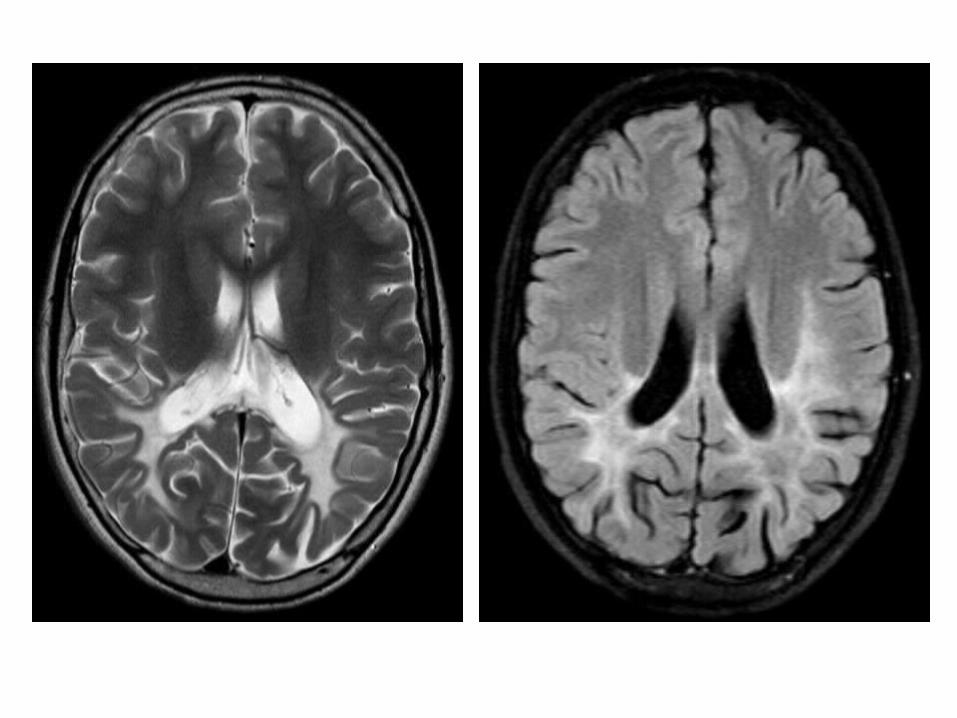
2-Radiographic Features :-MRI :*Symmetric areas of T2 prolongation in the basal
ganglia , periaqueductal region and cerebral peduncles with putaminal involvement being a consistent feature
-MRS :*May reveal the presence of abnormally high
lactate levels in the basal ganglia which together with elevated serum and CSF lactate levels supports the diagnosis
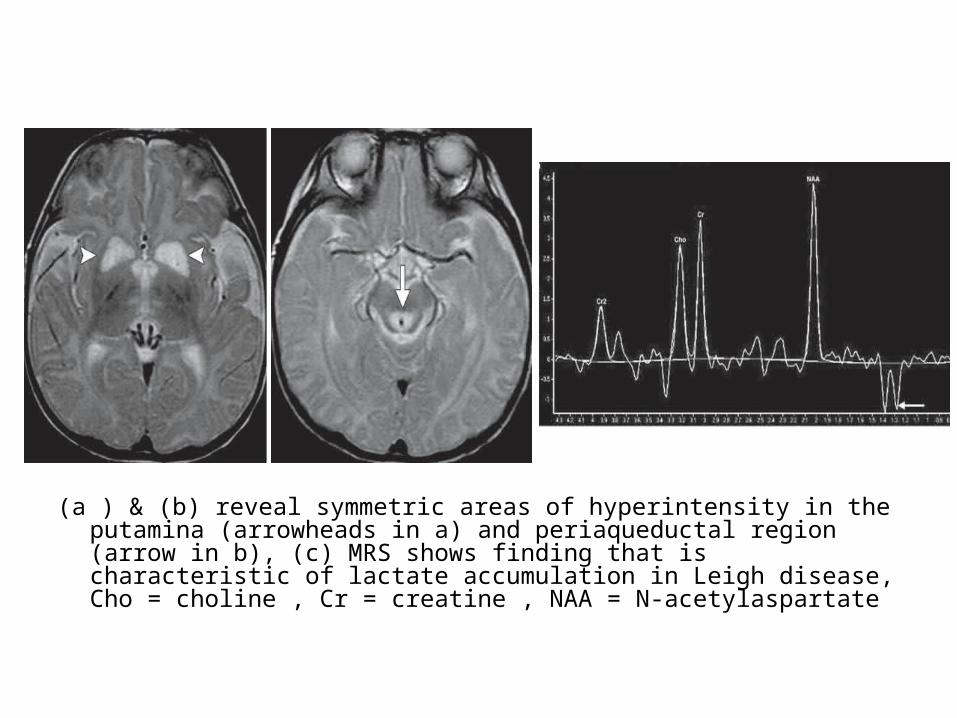
(a ) & (b) reveal symmetric areas of hyperintensity in the putamina (arrowheads in a) and periaqueductal region (arrow in b), (c) MRS shows finding that is characteristic of lactate accumulation in Leigh disease, Cho = choline , Cr = creatine , NAA = N-acetylaspartate
4-Aminoacidopathies :a) Phenylketonuriab) Homocystinuria

5-Idiopathic :a) Alexander's Diseaseb) Cockayne's Diseasec) Pelizaeus-Merzbacher Diseased) Canavan's Disease
-Radiographic Features of Leukodystrophies :1-Macrocephaly :-Canavan’s disease-Alexander’s disease2-Frontal Lobe Predilection :-Alexander’s disease3-Occipital Lobe Predilection :-Adrenoleukodystrophy
4-Contrast Enhancement :-Adrenoleukodystrophy-Alexander's disease5-Hyperdense Basal Ganglia :-Krabbe’s disease6-ischemic Infarctions :-Mitochondrial disorders (MELAS , MERRF)-Homocystinuria

(ii) Gray Matter Disease :1-Senile dementia , Alzheimer's type ( SDAT )2-Pick's disease3-Vascular cortical dementia ( multiinfarct
dementia )4-Parkinson's disease5-Amyotrophic Lateral Sclerosis ( ALS )
1-Senile Dementia , Alzheimer's type ( SDAT ) :a) Incidenceb) Radiographic Features

a) Incidence :-Alzheimer's disease is the most common cause
of dementia and accounts for two thirds of cases of dementia in patients aged 60-70 years

b) Radiographic Features :1-CT2-MRI3-Nuclear Medicine

1-CT :-CT is able to demonstrate the characteristic
patterns of cortical atrophy , however , MRI is more sensitive to these changes and better able to exclude other causes of dementia (e.g. multi-infarct dementia)

2-MRI :-The primary role of MRI in the diagnosis of
Alzheimer's disease is the assessment of volume change in characteristic locations which can yield a diagnostic accuracy of up to 87%
-The diagnosis should be made on the basis of features :
a) Mesial temporal lobe atrophyb) Temporoparietal cortical atrophyc) Global Cortical Atrophy

a) Mesial temporal lobe atrophy :-Mesial temporal lobe atrophy can be viewed directly by
assessing for hippocampal and parahippocampal decrease in volume or indirectly by examining enlargement of the parahippocampal fissures , the former is more sensitive and specific but ideally requires actual volumetric calculations
-These measures have been combined in the medial temporal atrophy score which has been shown to be predictive of progression from mild cognitive impairment (MCI) to dementia

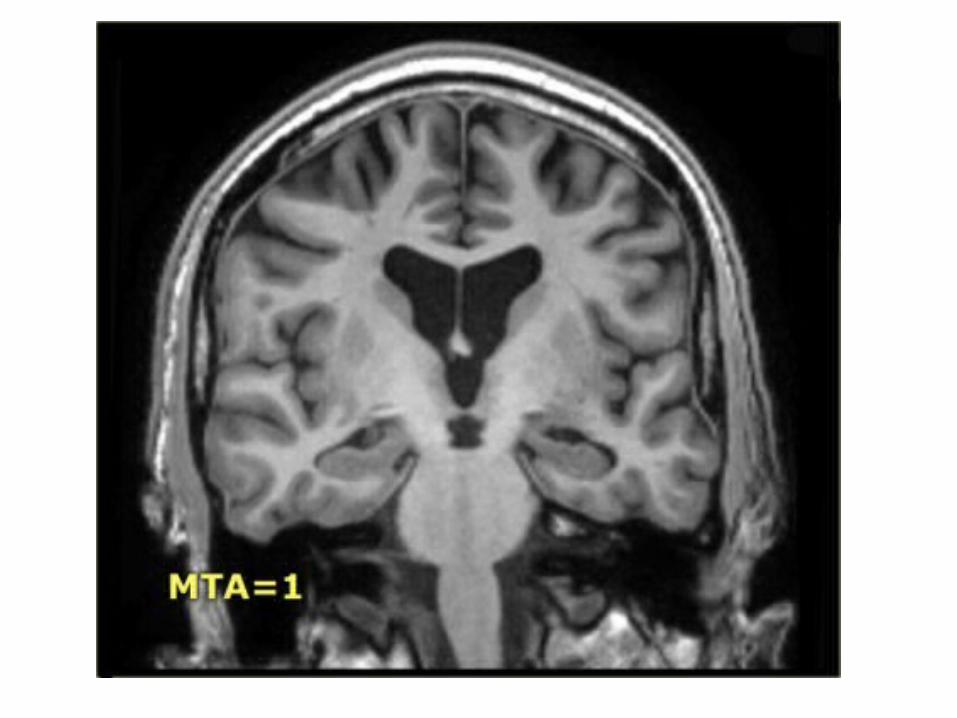
-Medial temporal lobe atrophy (MTA) score :*It is a visual score performed on MRI of the
brain using coronal T1 weighted images through the hippocampus at the level of the anterior pons and assesses three features :
1-Width of the choroid fissure 2-Width of the temporal horn of the lateral
ventricle 3-Height of the hippocampus

*Each is graded from 0 to 4 :0 = No atrophy1 = Only widening of choroid fissure2 = Also widening of temporal horn of lateral
ventricle3 = Moderate loss of hippocampal volume
( decrease in height ) 4 = Severe volume loss of hippocampus


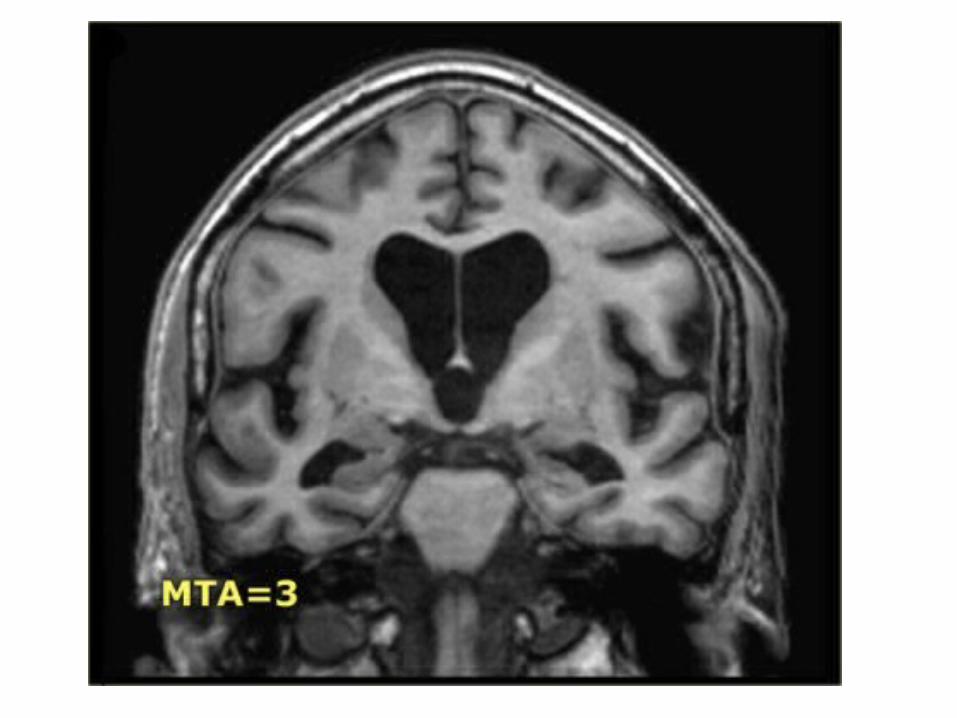

*In a patient younger than 75 years of age , a score of 2 or more is abnormal
*In a patient 75 years or older , a score of 3 or more is abnormal
*Atrophy has been shown to correlate with likelihood of progression from mild cognitive impairment (MCI) to dementia
b) Temporoparietal cortical atrophy :-This is often best seen on the interhemispheric
surface of the parietal lobe by examining the posterior cingulate sulcal and parieto-occipital sulcal size and degree of atrophy of the pre-cuneus and cortical surface of the parietal lobe
-This has also been combined into a scoring system , posterior atrophy score of parietal atrophy (Koedam score)
-The posterior atrophy score (Koedam score) :*To generate this score , the brain must be
viewed in three planes and multiple structure assessed :
1-sagittal plane posterior cingulate sulcus :a) parieto-occipital sulcusb) precuneus gyri

2-Coronal plane :a) posterior cingulate sulcusb) parietal gyri3-Axial plane :a) Posterior cingulate sulcusb) Parietal lobes

*Each is graded from 0 to 3 :Grade 0 = closed sulci , no gyral atrophyGrade 1 = mild sulcal widening , mild gyral
atrophyGrade 2 = substantial sulcal widening ,
substantial gyral atrophyGrade 3 = marked sulcal widening, knife-blade
gyral atrophy
c) Global Cortical Atrophy :-GCA scale is the mean score for cortical atrophy
throughout the complete cerebrum-Cortical atrophy is best scored on FLAIR images0: No cortical atrophy1: Mild atrophy : opening of sulci2: Moderate atrophy : volume loss of gyri3: Severe (end-stage) atrophy: knife blade atrophy

3-Nuclear Medicine :-SPECT and PET are able to detect regional
hypoperfusion / hypometabolism in a bi-parietal and bi-temporal distribution

2-Pick's disease :a) Incidenceb) Radiographic Features

a) Incidence :-Rare cortical dementia that commonly
manifests before age 65 ( presenile onset ) -Typically manifests between the ages of 40 and
60 years with a male predilection

b) Radiographic Features :-Frontotemporal atrophy , frontal horn
enlargement and parietooccipital sparing are typical imaging features

3-Vascular cortical dementia (multiinfarct dementia) :
a) Incidenceb) Typesc) Radiographic features

a) Incidence :-Ischemic dementia is the second most common
form of dementia after SDAT

b) Types :1-Multiinfarct dementia :-Cortical infarctions ( territorial vascular
infarctions )-Enlarged sulci and ventricles-Prominent T2W hyperintensities2-Subcortical dementia ( Binswanger's disease ) :-Periventricular hyperintensity (penetrating
vessel ischemia)- Hypertension is common
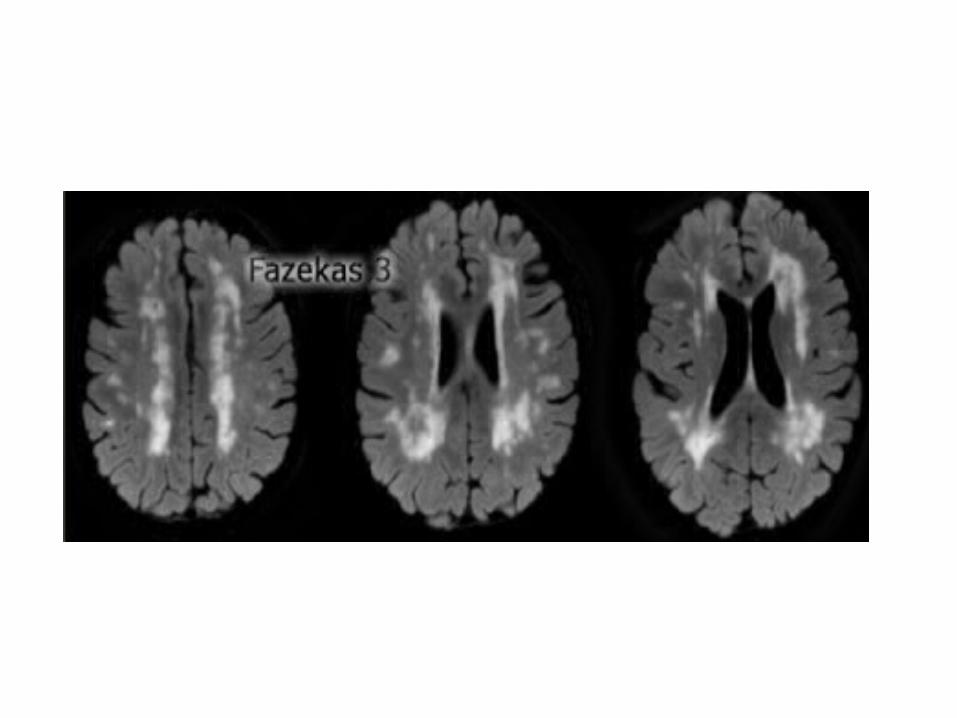
c) Radiographic features :1-Fazekas scale for WM lesions2-Looking for strategic infarcts

1-Fazekas scale for WM lesions :-On MR , white matter hyperintensities (WMH) and
lacunes , both of which are frequently observed in the elderly , are generally viewed as evidence of small vessel disease
-The Fazekas-scale provides an overall impression of the presence of WMH in the entire brain
-It is best scored on transverse FLAIR or T2-weighted images
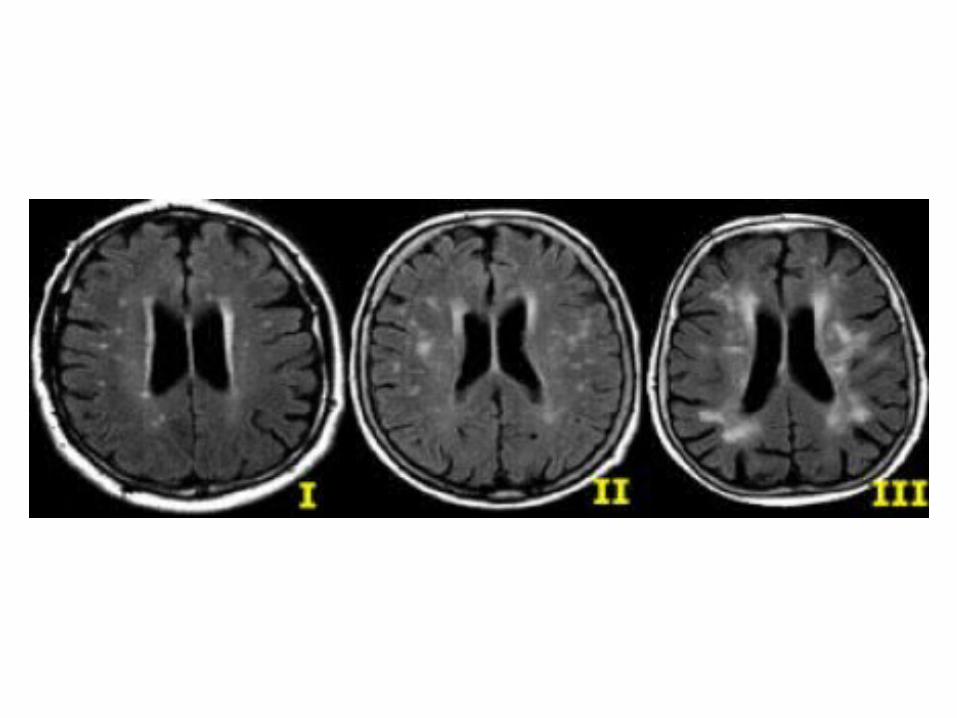
-Score :Fazekas 0 : None or a single punctate WMH
lesionFazekas 1 : Multiple punctate lesionsFazekas 2 : Beginning confluency of lesions
(bridging)Fazekas 3 : Large confluent lesions

-Fazekas 1 is considered normal in the elderly-Fazekas 2 and 3 are pathologic but may be seen
in normally functioning individuals , they are however , at high risk for disability




2-Looking for strategic infarcts :-Strategic infarctions are infarctions in areas
that are crucial for normal cognitive functioning of the brain
-Strategic infarctions are best seen on transverse FAIR and T2W sequences

4-Parkinson's disease :a) Incidenceb) Clinical Picturec) Typesd) Radiographic Features

a) Incidence :-More in elderly patients and is common seen in 2-
4% of all individuals older than 65 years of age
b) Clinical Picture :-Cogwheel rigidity-Bradykinesia-Tremor

c) Types :1-Parkinson's disease2-Secondary parkinsonism :a) Neuroleptic drugsb) Traumac) CO poisoning
3- Parkinson-plus syndrome (patients who respond poorly to antiparkinson medication) :
a) Striatonigral degenerationb) Shy-Drager syndromec) Olivopontocerebellar atrophyd) Progressive supranuclear palsy
d) Radiographic Features :-Iron-induced signal loss in basal ganglia best
seen on T2W spin-echo and gradient-echo images ( black ganglia )
-Location of signal intensity change : *Parkinson : globus pallidus*Parkinson-plus : putamen-Cerebral atrophy in chronic cases

5-Amyotrophic Lateral Sclerosis (ALS) :a) Incidenceb) Radiographic Features

a) Incidence :-Progressive neurodegenerative illness-Unknown etiology but 5%-10% of cases are
familial

b) Radiographic Features :-Abnormal high signal intensity in corticospinal
tracts on PDW/FLAIR images , best seen at level of middle or lower internal capsule
-Low signal intensity within motor cortex



















