Diagnostic Approach to Pleural Effusion
15
Diagnostic Approach to Pleural Effusion Garrett Waagmeester 4/25/2014
description
Diagnostic Approach to Pleural Effusion. Garrett Waagmeester 4/25/2014. Normal Pleural Physiology. Total pleural fluid volume: 0.2-0.3 mL /kg Fluid produced by systemic vessels of the parietal pleura, primarily less dependent capillaries, based on: Permeability of the pleural vessels - PowerPoint PPT Presentation
Transcript of Diagnostic Approach to Pleural Effusion

Diagnostic Approach to Pleural Effusion
Garrett Waagmeester4/25/2014

Total pleural fluid volume: 0.2-0.3 mL/kg Fluid produced by systemic vessels of the parietal
pleura, primarily less dependent capillaries, based on:◦ Permeability of the pleural vessels◦Hydrostatic and oncotic gradients
Fluid removed by pleural lymphatics in dependent portions of parietal pleura
Rate of production at homeostasis: 0.1 mL/kg/h
Normal Pleural Physiology
Theodore et al, 2010; Suratt, 2003; Noppen et al, 2000

Low in protein: <100 mg/dL Slightly alkaline compared to
serum: pH = 7.60-7.64 Hypocellular compared to
serum◦ 1000-2000 WBC/μL
75% macrophages (IR 64-81%)* 23% lymphocytes (IR 16-31%)*
* Median values; IR= interquartile range
Normal Pleural Fluid Composition
Suratt, 2003; Noppen et al., 2000

1. Increased pulmonary capillary pressure (CHF)
2. Increased pulmonary capillary permeability (PNA)
3. Decreased intrapleural pressure (Atelectasis)
4. Decreased plasma oncotic pressure (Hypoalbuminemia)5. Increased pleural membrane permeability and obstructed lymphatic
flow (pleural malignancy, infection)
6. Diaphragmatic defects (hepatic hydrothorax)
7. Thoracic Duct Rupture (chylothorax)
Mechanisms of Pleural Effusion
Porcel and Light, 2006

Symptoms Dyspnea ◦ Often disproportionate to
hypoxemia Cough Pleuritic Chest Pain
Physical Exam Decreased breath sounds Dullness to percussion Decreased tactile fremitus Egophony (EA) May find rales or pleuritic
friction rub
Symptoms and Exam Findings

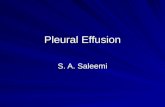
>50-75 mL of fluid on lateral radiograph to blunt costophrenic angle
>175-200 mL of fluid on P/A view to blunt lateral costophrenic angle
Clinically significant pleural effusion: >10mm fluid present on lateral decubitus radiograph (or U/S)
Chest Radiography

Delayed thoracentesis in parapneumonic effusion associated with:◦ Longer hospital stay◦ Greater healthcare cost
Initial pleural fluid analysis:◦ Protein◦ LDH◦ Cell count with differential◦ Gram stain/culture◦ Glucose◦ Cytology◦ pH
Diagnostic Workup
Heffner et al, 1995; Light, 2002

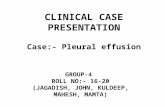
Light, 2002

Transudate versus Exudate?
Light, 2002

Transudative Effusion Exudative EffusionIncreased hydrostatic pressure• Congestive Heart Failure• Constrictive Pericarditis• Pulmonary Embolism*
Reduced oncotic pressure• Nephrotic syndrome• Malnutrition
Transdiagphragmatic leakage• Cirrhosis with ascites*• Peritoneal dialysis• Urinothorax*
Decreased intrapleural pressure•Atelectasis
* Predominantly unilateral
Lymphocytic predominance• Tuberculous/Fungal pleuritis *• Malignant disease (30-35%)*• Sarcoidosis
Neutrophilic predominance• Parapneumonic effusion*• Empyema*• Rheumatoid disease• Pulmonary infarction*
Neutrophilic or lymphocytic•Postcardiac injury (Dressler’s) syndrome•Pulmonary embolism*• Connective tissue disease
Eosinophilic predominance• Trauma• Asbestos• Drug-induced pleural disease
RBC count >100,000• Malignancy*• Trauma• Pulmonary infarction*
Other• Chylothorax/Pseudochylothorax
Transudate versus Exudate? DDx
Suratt, 2003; Ansari and Idell, 1998; Light, 2006

CT has higher sensitivity than CXR or MRI for:◦ Pleural thickening and
loculation◦ Pleural vs. parenchymal disease
Empyema vs. abscess◦ Pulmonary embolism
Helical CT◦Malignancy◦Mediastinal disease
Role for CT scan in Workup?
Porcell and Light, 2006; Davies et al, 2003; Qureshi and Gleeson, 2006; Sahn, 2007

However, there are no trials demonstrating benefits of CT in terms of:◦ Shorter time to diagnosis◦Decreased need for diagnostic procedures (e.g. thoracentesis)◦ Shorter hospital stay/decreased cost
Management guidelines recommend CT scans for complicated cases after failed initial diagnostic workup
Role for CT scan in Workup?
Porcell and Light, 2006; Davies et al, 2003; Qureshi and Gleeson, 2006; Sahn, 2007

Ultrasound◦ Guided thoracentesis◦ Identifies locultated effusion
Needle biopsy of pleura◦ Tuberculous pleuritis and malignancy
Bronchoscopy◦ Bronchial invasion by malignancy or
infiltrate Thoracoscopy◦ Allows for pathologic analysis◦ Option for pleurodesis
Open biopsy
Other Diagnostic Testing
Davies et al, 2003; Light, 2006; Sahn, 2007

Pleural fluid is produced and removed by parietal pleura◦ Multiple mechanisms to
disrupt homeostasis Thoracentesis essential to
diagnosis◦ Light’s criteria: sensitive and
specific for identifying exudative effusions
CT scan can be helpful for complicated cases
Summary

1. Theodore PR, Jablons D. Chapter 18. Thoracic Wall, Pleura, Mediastinum, & Lung. In: Doherty GM. eds. CURRENT Diagnosis & Treatment: Surgery, 13e.New York, NY: McGraw-Hill; 2010. http://accessmedicine.mhmedical.com.liboff.ohsu.edu/content.aspx?bookid=343&Sectionid=39702805. Accessed April 18, 2014.
2. Suratt BT. Chapter 22. Pleural Effusions, Excluding Hemothorax. In:Hanley ME, Welsh CH. eds. CURRENT Diagnosis & Treatment in Pulmonary Medicine. New York, NY: McGraw-Hill; 2003. http://accessmedicine.mhmedical.com.liboff.ohsu.edu/content.aspx?bookid=346&Sectionid=39883273. Accessed April 18, 2014.
3. Noppen M, De Waele M, Li R, Gucht KV, D’Haese J, Gerlo E. Volume and Cellular Content of Normal Pleural Fluid in Humans Examined by Pleural Lavage. Am J Respir Crit Care Med 2000; 162: 1023-1026.
4. Porcel JM, Light RW. Diagnostic Approach to Pleural Effusion in Adults. Am Fam Physician 2006; 73: 1211-1220.
5. Heffner JE, McDonald J, Barbieri C, Klein J. Management of Parapneumonic Effusion: an analysis of physician practice patterns. Arch Surg 1995; 130:433-438.
6. Light RW. Pleural Effusion. NEJM 2002; 346: 1971-1977
7. Ansari T, Idell S. Management of Undiagnosed Persistent Pleural Effusion. Clin Chest Med 1998; 19(2): 407-417.
8. Light RW. The Undiagnosed Pleural Effusion. Clin Chest Med 2006; 27: 309-319.
9. Qureshi NR, Gleeson FV. Imaging of Pleural Disease. Clin Chest Med 2006; 27: 193-213.
10. Davies CWH, Gleeson FV, Davies RJO. BTS Guidelines for the management of pleural infection. Thorax 2003; 58(ii): 18-28.
11. Sahn SA. Diagnosis and Management of Parapneumonic Effusions and Empyema. Clin Infect Disease 2007; 45: 1480-1486.
12. Light RW. Pleural Effusions. Med Clin N Am 2011; 95: 1055-1070
References