Diagnosis & Assessment of Alcohol Dependence 2006 RSA Lecture Series Deborah Hasin, Ph.D. Columbia...
39
Diagnosis & Assessment of Alcohol Dependence 2006 RSA Lecture Series Deborah Hasin, Ph.D. Columbia University New York State Psychiatric Institute
-
Upload
keven-checkley -
Category
Documents
-
view
214 -
download
0
Transcript of Diagnosis & Assessment of Alcohol Dependence 2006 RSA Lecture Series Deborah Hasin, Ph.D. Columbia...

Diagnosis & Assessment of Alcohol Dependence
2006 RSA Lecture Series
Deborah Hasin, Ph.D.Columbia University
New York State Psychiatric Institute

Importance to different types of research
• Treatment: inclusion and exclusion criteria for studies of behavioral & pharmacological interventions
• Etiologic: phenotypes in genetic studies, defines case and control groups in other studies
• Epidemiology: defines conditions to determine rates in populations and subgroups
• Policy: determines & documents services needs

Importance of diagnosis and assessment in treatment
• Formulation of treatment plans
• Facilitates communication between clinicians
• Teaching tool
• Justifies third-party payment

DSM-IV/V importance in treatment
• Formulation of treatment plans
• Communication between clinicians with different training or experience
• Justifying 3rd party payment
• Teaching and training

Before “Alcohol Dependence…”
• Ongoing debate over “alcoholism” vs. “alcohol problems”
• 12-step(AA) philosophy vs. social science vs. psychoanalysis
• Little conceptual agreement
• Assessments not standardized

Isn’t “alcoholism” obvious? Don’t you “know one when you see
one?”Not necessarily…
• Concepts of what constitutes an alcohol disorder vary by culture, training, and personal experience
• Non-standardized assessments yield inconsistent coverage
• Variation in concepts and coverage lead to poor reliability (agreement) and validity

What is reliability?
• Reliability: between-rater agreement on presence, absence, or level of a diagnosis• Joint rating design sometimes used• Test-retest more common, informative design
• Reliability coefficients• Kappa (K) most common for binary diagnoses• Intraclass correlation coefficient (ICC) most
common for continuous • Interpretation: > .75 excellent, .60 - .74 good,
.40 - .59 fair, <.40 poor

What is validity?
• This indicates that the condition (diagnosis) being measured is the condition of interest and not something else• No single “validity coefficient” or “gold
standard”
• Validity of diagnosis often indicated by comparison to more authoritative evaluation
• Single biological indicators for alcohol dependence or abuse do not exist
• Usual design compares diagnosis to expert judgment based on longitudinal course, family history, multiple informants, etc.
The need for good reliability and validity
led (in steps) to DSM-IV
• Concern over inconsistent concepts of psychiatric disorders led to specific diagnostic criteria
• Concern over inconsistent and incomplete assessment led to standardized diagnostic interviews

Alcohol Dependence Syndrome(Edwards and Gross, 1976)
• Dependence concept based on close observation of patients
• The concept: a combination of physiological and psychological processes
• Dimensional rather than yes or no
• Bi-axial distinction of core alcohol dependence syndrome from its consequences the basis for dependence/abuse

DSM-IV Alcohol Dependence
Maladaptive drinking leading to clinically significant impairment or distress, shown by 3+ of the following in the same 12-month period:
1. Drinking more or longer than intended2. Persistent desire or unsuccessful efforts to cut
down or stop3. A great deal of time spent on drinking or getting
over its effects4. Important activities given up or reduced because
of drinking5. Continued drinking despite knowledge of a serious
physical or psychological problem6. Tolerance7. Withdrawal, or drinking to avoid or relieve drinking

DSM-IV Alcohol Dependence – Physiological subtype
• Includes tolerance and/or withdrawal• DSM-IV withdrawal criteria: cessation/reduction in
heavy, prolonged use & within several hours to a few days
• 2 or more withdrawal symptoms, including:• Autonomic hyperactivity (sweating or rapid pulse)• Hand tremor• Insomnia• Nausea or vomiting• Transient hallucinations or illusions• Psychomotor agitation• Anxiety• Seizures

DSM-IV Alcohol Abuse
Not dependent, and maladaptive drinking leading to clinically significant impairment or distress, shown by 1 + of the following:
1. Continued use despite social/interpersonal problems
2. Hazardous use (e.g., driving when impaired by alcohol)
3. Frequent drinking leading to failure to function in major roles
4. Legal problems

DSM-III-R, DSM-IV, ICD-10
DSM-III-R Dependence: 3 out of 9 CriteriaAbuse: 1 out of 2 Criteria, no dependence
ICD-10Dependence: 3 out of 6 CriteriaHarmful use: Mental, physical, social harm to
user, no dependence
DSM-IV Dependence: 3 out of 7 CriteriaAbuse: 1 out of 4 Criteria, no dependence

Reliability and validity evidence
Although developed in patient samples:
• DSM-III-R, DSM-IV and ICD-10 alcohol dependence highly reliable in general population, medical and other populations in the U.S. and elsewhere
• Dependence valid in many designs
• Reliability and validity less consistent for abuse
• Abuse criteria themselves fairly reliable• When diagnosed “hierarchically” as required in
DSM-IV, reliability is lower

How diagnostic criteria ascertained in different types of
assessments
• Fully structured: close-ended questions read to participants exactly as worded. Usually more than one question (“item”) per diagnostic criterion.
• Semi-structured: initial questions provided, but interviewer expected to ask additional questions to clarify responses
• Unstructured: interviewers ask their own questions to determine diagnostic criteria

Structured Clinical Interview for DSM-IV (SCID)
Williams et al., Arch Gen Psychiatry 1992
• Designed for clinicians, often administered by
research assistants
• Reliance on clinical judgment for many ratings
• Reliability of alcohol abuse/dependence:
excellent, validity good (Kranzler et al., 1996)
• Used mainly in clinical studies to determine inclusion,
exclusion criteria
• Semi-structured: initial questions included, interviewer then
adds own probes if more information needed
• Major Axis I disorders, SCID-II for Axis II disorders

Psychiatric Research Interview for
Substance & Mental Disorder (PRISM)
Hasin et al., Am J Psychiatry 1996; 2006• Mainly clinical studies where differentiating primary and substance-induced psychiatric disorders important
• Semi-structured
• Major Axis I disorders, Antisocial and Borderline PD
• Designed for clinicians or research assistants
• Specified guidelines provided for most ratings
• Test-retest reliability of DSM-IV alcohol dependence excellent, alcohol abuse fair (non-hierarchical, excellent)

National Epidemiologic Survey on Alcohol and Related Conditions
(NESARC) 2001-2002• National sample• N= 43,093• NIAAA & NIDA
sponsored• Household, group
residents• Oversampled
Blacks, Hispanics, adults 18-24 yrs
• DSM-IV diagnoses

Alcohol Use Disorders and Associated Disabilities Interview
Schedule (AUDADIS)
Grant et al., Drug Alcohol Depend 1995; 2003
• Used mainly in large-scale epidemiologic studies
• Fully structured
• Designed for lay interviewers
• Major Axis I disorders, Axis II disorders
• Test-retest reliability of DSM-IV alcohol abuse/dependence excellent
• Validity excellent via psychiatrist re-appraisal and other designs

Semi-Structured Assessment for the Genetics of Alcoholism (SSAGA)
Bucholz et al., J Stud Alcohol 1994; 2006
• Mainly used in genetics studies
• Semi-structured
• Major Axis I disorders, Antisocial PD
• Designed for non-clinicians with supervision from an editor
• Test-retest reliability of DSM-IV alcohol dependence excellent, alcohol abuse fair to very good

National Comorbidity Study – Replication
(NCS-R) 2001-2002
• National sample
• N= 9,282
• NIMH sponsored
• Household participants 18+yrs
• DSM-IV diagnoses
• WHO-CIDI
The Composite International Diagnostic Interview (CIDI)
• Used mainly in epidemiologic and clinical studies
• Fully structured, designed for lay interviewers
• Early versions such as CIDI-SAM (substance abuse module) similar to other interviews
• Recent versions (NCS-R, WMH Survey) skipped dependence questions in respondents with no abuse symptoms
• Agreement with SCID for alcohol dependence fair

NESARC findings, current dependence
with and without abuse – alcoholHasin et al., Arch Gen Psychiatry, 2004
Proportion of Sample
Total Dependence with
abuse
Dependence without abuse
% alcohol dependence
cases missed
All women 1.23 1.05 46.1
African American 1.23 1.16 48.5
Hispanic .087 1.07 55.2
All men 3.80 1.55 29.0
African American 2.90 2.19 43.0
Hispanic 3.57 2.33 39.5

NESARC findings, lifetime dependence
with and without abuse – alcoholHasin et al., Arch Gen Psychiatry, 2005
Proportion of Sample
Total Dependence with
abuse
Dependence without
abuse
% alcohol dependence
cases missed
All women 6.11 1.71 29.1
African American 3.60 1.43 24.8
Hispanic 4.17 1.71 29.1
All men 15.44 1.74 10.1
African American 10.66 2.04 16.1
Hispanic 10.52 2.50 19.2

Designs for Validity Research
• Longitudinal – course stays “true” over time, and/or is consistent with theoretical prediction
• Multi-method comparison – methods agree because they measure a consistent underlying construct
• Construct – Conditions associated (or not) with external variables in theoretically predicted patterns
• Factor/latent class analysis – criteria cluster in theoretically predicted patterns

Longitudinal course:
Dependence and Abuse distinctly different
• Hasin et al. National Am J Psychiatry 1990
• Hasin et al. Community heavy J Subst Abuse 1997
drinkers
• Grant et al. National J Subst Abuse 2001
• Schuckit et al. UCSD male Am J Psychiatry 2000
volunteers
• Schuckit et al. COGA Am J Psychiatry 2001

Multi-Method Comparison Dependence: Excellent Abuse hierarchical: Low Abuse non-hierarchical: Better*
• Rounsaville et al. Clinical Addiction 1993
• Schuckit et al. COGA Addiction 1994
• Hasin et al. Community * Addiction 1996
• Grant National Alch Clin Exp Res 1996
• Hasin et al. WHO Int’l Drug Alch Depend 1997
• Pull et al. WHO Int’l * Drug Alch Depend 1997
• Cottler et al. WHO Int’l * Drug Alch Depend 1997

Construct Validation: DependenceDrinkers from a community and
national sample
Dependence Community NLAES
Treatment 10.1 11.1
Suicidality 2.0 3.2
Blackouts 6.0 9.8
Average ethanol 1.9 2.6
Family History 1.4 2.9
Hasin et al., Alcohol Clin Exp Res, 1997; Hasin and Paykin, 1999

Construct Validation: AbuseCommunity Heavy Drinkers and NLAES
drinkers
Abuse Community NLAES
Treatment -- 2.3
Suicidality -- --
Blackouts 2.4 4.8
Ethanol -- 1.7
Family History -- 1.9
Hasin et al., Alcohol Clin Exp Res 1997; Hasin and Paykin, 1999

Factor analyses:
Dependence and Abuse
• Harford, Muthen U.S. national, NLSY 2 factors
• Muthen et al. U.S. national, NHIS 2 factors
• Proudfoot et al. Australian, National 1 factor
• Saha et al. U.S. NESARC 1 factor

DSM-V issues concerning dependence
• Alcohol dependence is a highly reliable, valid alcohol diagnosis, however:
• Should a severity indicator of dependence be added, as has been used in small-sample/low-frequency genetics studies (Hasin et al., 2002; Heath et al., 2001)?
• Should drinking level be added as a criterion or as an extra requirement, e.g., Project COMBINE? (Anton et al., 2006)
• Can biological endophenotypes be identified that would aid in the diagnosis, e.g., the COGA study? (Hesselbrock et al., 2001; Edenberg et al., 2004)
• Can the relationship of substance and psychiatric disorders be specified better than the current primary/substance-induced differentiation?

DSM-V issues concerning abuse
• Alcohol abuse is less clear
• Keep abuse as it is now?
• Diagnose it independently from dependence?
• Add a severity indicator?
• Combine abuse and dependence criteria?
• Rename?
• Drop category entirely?

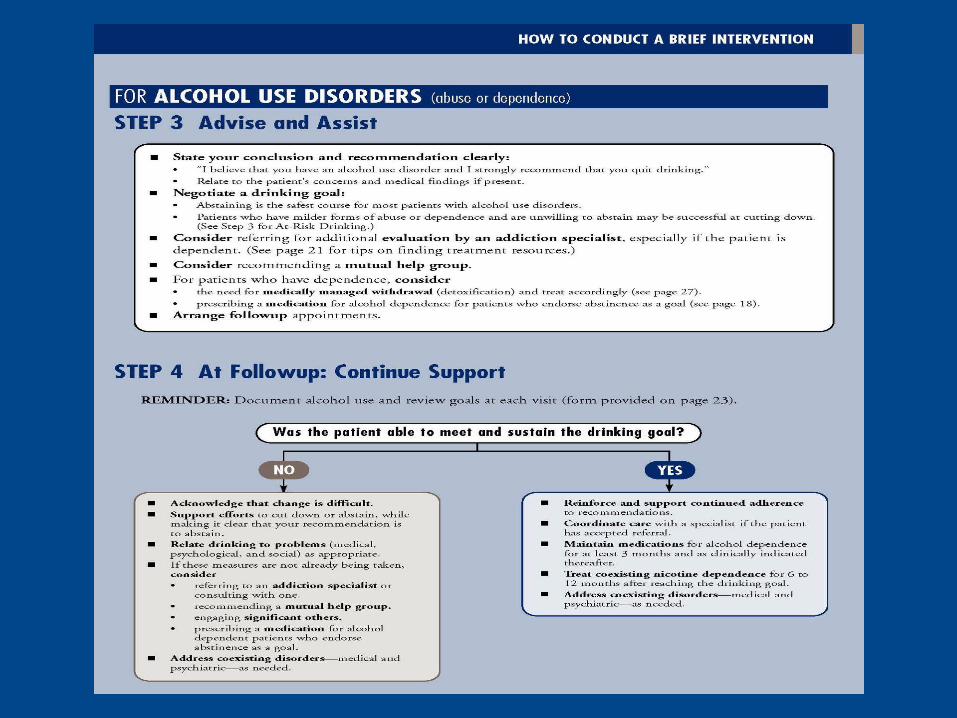
Clinical assessment and diagnosis
• NIAAA Clinician’s Guide• http://pubs.niaaa.nih.gov/publications/
Practitioner/CliniciansGuide2005/guide.pdf



Acknowledgements
• K05 AA014223, R01 AA008159, AA008910, DA008409 DA010919 DA018652
• New York State Psychiatric Institute
• Presentation: Valerie Richmond, M.A.
• Contact: [email protected]