
“Diagnosis and treatment of latent TB ” Update – Internal Medicine Dr Dick Menzies Montreal...
69
“Diagnosis and treatment of latent TB ” Update – Internal Medicine Dr Dick Menzies Montreal Chest Institute
-
Upload
marylou-rose -
Category
Documents
-
view
223 -
download
0
Transcript of “Diagnosis and treatment of latent TB ” Update – Internal Medicine Dr Dick Menzies Montreal...
“Diagnosis and treatment of latent TB ”Update – Internal Medicine
Dr Dick Menzies
Montreal Chest Institute

Problems with current approach to LTBI management
• TST – Labour intensive, slow, non-specific– Although appears to predict benefit
• Current therapy (INH)– Long duration = poor compliance - less than
50% in most programs, although can be 70%. – Serious side effects - can be fatal– Costs - close follow up necessary = expensive
Overview of Talk• LTBI diagnosis
• The old – Tuberculin skin test
• The new – Interferon gamma release assays
• Treatment of Latent TB• The current standard – 9INH
• Is a TST needed before starting INH therapy?
• Does INH therapy create INH resistance?
• Alternatives – 4RIF and others• The 4RIF trial

Diagnosis - Indications for testing
• Increased risk of developing TB diseaseNew TB infection
Increased risk of reactivation from latent TB
• Increased risk of exposureHealth care workers – at hiring
Other workers with risk of exposure

Tools for diagnosis - TST
• Strengths:– Long history: known test performance– Simple test: can be performed (almost) anywhere– Predictive ability: for benefit of treatment
• Weaknesses:– Specificity: especially if BCG vaccinated– Sensitivity: especially if immune compromise– Predictive ability: <10% develop disease
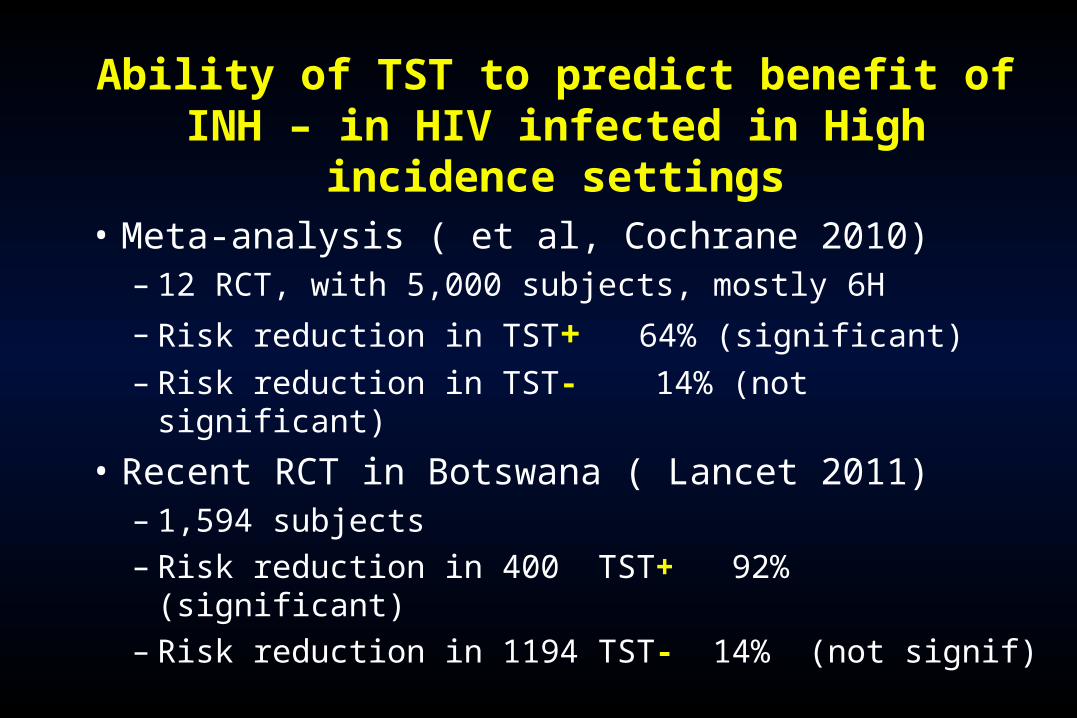
Ability of TST to predict benefit of INH – in HIV infected in High incidence settings
• Meta-analysis ( et al, Cochrane 2010)– 12 RCT, with 5,000 subjects, mostly 6H
– Risk reduction in TST+ 64% (significant)
– Risk reduction in TST- 14% (not significant)
• Recent RCT in Botswana ( Lancet 2011)– 1,594 subjects – Risk reduction in 400 TST+ 92% (significant)– Risk reduction in 1194 TST- 14% (not signif)

Interferon gamma release assays Interferon gamma release assays (IGRA)(IGRA)
• A brief introduction

8Andersen P et al, Lancet 2000
TST vs IGRA: rationale

9
ESAT-6
CFP-10
Cole et al, Nature 1998
GenomicsProteomics

Contains TB specific antigens - ESAT-6, CFP-10, TB7.7 Incubate whole blood 16 hours, then measure IFN-γ
released from sensitized lymphocytes. Using ELISA reader Cost – materials $20, labour $20-25,
From: Pai M, et al.,Lancet Infect Dis 2004
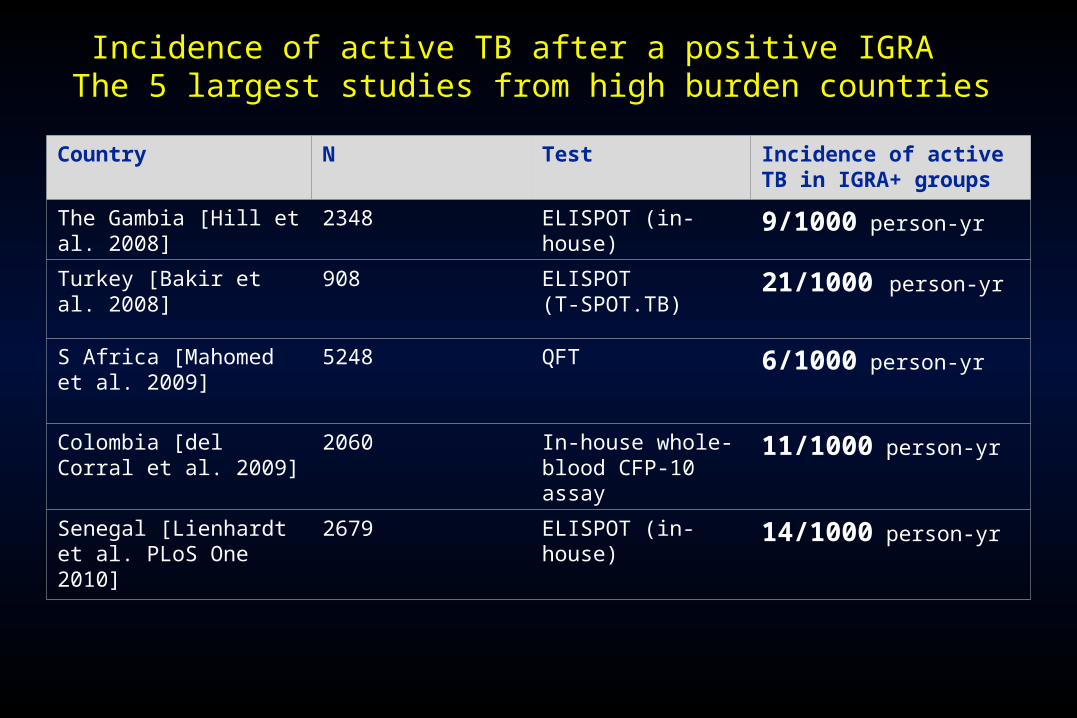
Incidence of active TB after a positive IGRA The 5 largest studies from high burden countries
Country N Test Incidence of active TB in IGRA+ groups
The Gambia [Hill et al. 2008]
2348 ELISPOT (in-house) 9/1000 person-yr
Turkey [Bakir et al. 2008] 908 ELISPOT (T-SPOT.TB)
21/1000 person-yr
S Africa [Mahomed et al. 2009]
5248 QFT 6/1000 person-yr
Colombia [del Corral et al. 2009]
2060 In-house whole-blood CFP-10 assay
11/1000 person-yr
Senegal [Lienhardt et al. PLoS One 2010]
2679 ELISPOT (in-house) 14/1000 person-yr
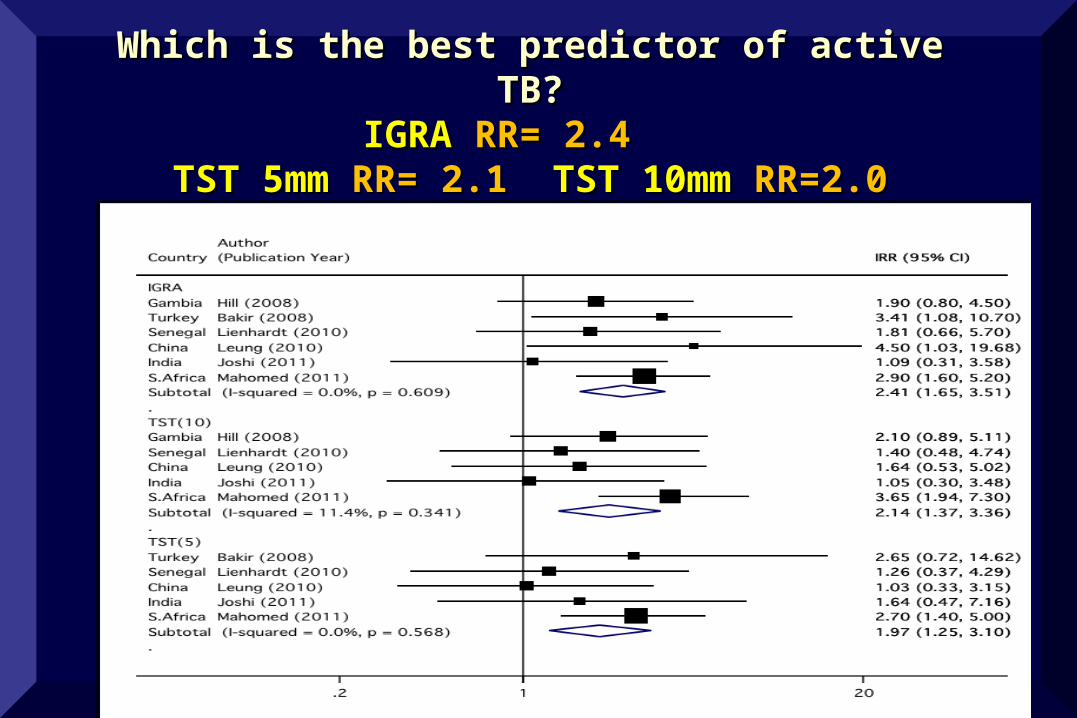
Which is the best predictor of active TB?Which is the best predictor of active TB?IGRA IGRA RR= 2.4 RR= 2.4
TST 5mm TST 5mm RR= 2.1 RR= 2.1 TST 10mm TST 10mm RR=2.0RR=2.0

Summary: IGRASummary: IGRA• Good points:
– Excellent specificity: In all situations and populations. Not affected by BCG.
– Standardization: performed in clinical lab– No Bias – Less chance of bias at reading
• Weak points:– Sensitivity: same as TST, especially if immune
compromised – Costs – more than TST– Long term – predicting active TB – same as TST
• Only 10% get disease– And still not enough experience so unknown problems

Choice of test to diagnose latent TB – Choice of test to diagnose latent TB – Canadian recommendationsCanadian recommendations
1. In general TST remains test of first choice
2. If TST is positive, but person is at low risk of reactivation (student or worker baseline screen):
Perform IGRA – to enhance specificity. If IGRA negative then do not treat
3. If TST negative but high risk (HIV, or immune suppressed).
Perform IGRA – to enhance sensitivity. If IGRA positive then treat

The test is positive – now what?The test is positive – now what?
• Medical evaluation for all – the first time a TST or IGRA is found positive– This includes symptoms, medical history– And a chest x-ray (exclude active TB)

No active TB is found – now No active TB is found – now what?what?
• Decision re treatment – must balance• Risk of TB disease – test size, Chest Xray,
other medical problems• Risk of adverse events• This can be complex. Takes knowledge,
experience, intelligence
• Or it takes….

17
http://www.tstin3d.com
THE INTERNET !! (the Online TST/IGRA interpreter)
On-line resource for interpreting TST or IGRA
Incorporates test result, clinical history, & other biologic risk factors to estimate composite risk.
Uses age to estimate risk of hepatotoxicity with INH

Considerations for therapy
• Individual benefit: Primary consideration is the balance of risk of INH therapy vs benefit in terms of likelihood of TB prevention
• Public health benefit: Reduction of transmission through prevention of cases vs cost and feasibility

Risk of active TB disease
• Lifetime risks with Latent TB infection:– Young healthy adult: 5-10%– HIV infected: >50%– Diabetic: 3-4X relative risk = 20-40%– Very young child:
• Age <1: 50% risk in 1 year
• Age 1-2: 20-30% risk in 1 year
• Age 2-5: 15-20% risk

Consequences of active TB
• Mortality:– Undiagnosed Smear positive: 33%/year– Diagnosed and treated: 4% - 7%
• Long term disability following active TB– Surprisingly little data.– US study – average 20% loss of lung function– From Canada – 24% reduction in QALY– Data needed!!

Individual risks of therapy
• Risks of therapy are well known for INH, and INH hepatitis is serious
• Risks of other therapies less well known
Schematic of Risk Benefit Balance for INH LTBI Therapy
Risks of therapy
• Older Age
• Liver Disease
• Alcohol Use
Benefits of therapy
Increased if greater risk of disease:
HIV, diabetes, abnormal Xray, contact, etc

Treatment of hypertension vs LTBI
Hypertension
• Asymptomatic condition
• Very serious complications– Death
– Major disability
• Treatment is for many years– Potential serious side effects
– Requires close monitoring and FU
– Expensive medications
• BUT – no debate about Treating
LTBI
• Asymptomatic condition
• Very serious complications– Death, Major disability
– AND transmission
• Treatment is 9 months– Potential serious side effects
– Requires close monitoring and FU
– Cheap medications
• WHY the debate about Treating

LTBI treatment – what are the options?
• 6-9 months of INH
• 2 months RIF-PZA
• 3-4 months INH-RIF
• 3 months once weekly INH& Rifapentine
• 4 months RIFampin

Duration of INH Therapy and efficacy/effectiveness
Patients with Fibrotic Lesions
Population Duration Reduction in TB
All participants INH 12 mo. 75% INH 6 mo. 65% INH 3 mo. 21%
Completer/compliers INH 12 mo. 93% INH 6 mo. 69% INH 3 mo. 31%
Bull WHO 1982;555-64

How Much Isoniazid Is Needed for the Prevention of Tuberculosis?
• Longer durations of therapy up to 9 months, corresponded to lower TB rates
• No extra increase in protection among those who took >9 months
Comstock GW, 1998

Efficacy of therapy
• INH will reduce risk of disease by 90%– If taken for 9 months– If >80% of doses taken each month

Age Specific Incidence of INH hepatitis
Age Incidence of hepatitis
0-20 < 0.1%
21-34 0.3%
35-49 1.2%
49-64 2.3%
65 + > 5%
From USPHS Surveillance Study - probable cases ONLY, and from Arkansas nursing home residents

Mortality from INH hepatitis
Study Years Age Mortality
(per 100,000) USPHS surveillance 1971-72 < 35
> 35 0 98
IUAT trial 11969-72 35-65 14
CDC surveillance 1972-3 1974-83 1984-8
All All All
54 14 6
Salpeter survey 1983-92 <35
>35 0.6 2.4

Problems with INH
1. Length - 9 months ideal (90% efficacy)– Results in poor compliance - less than 50% in most
programs.
2.Drug induced hepatitis - - Less common now, but deaths still occur.– Also rash, neuropathies
3. Costs - INH is cheap but close follow up is necessary. This is expensive
Is a TST needed before LTBI therapy is given?
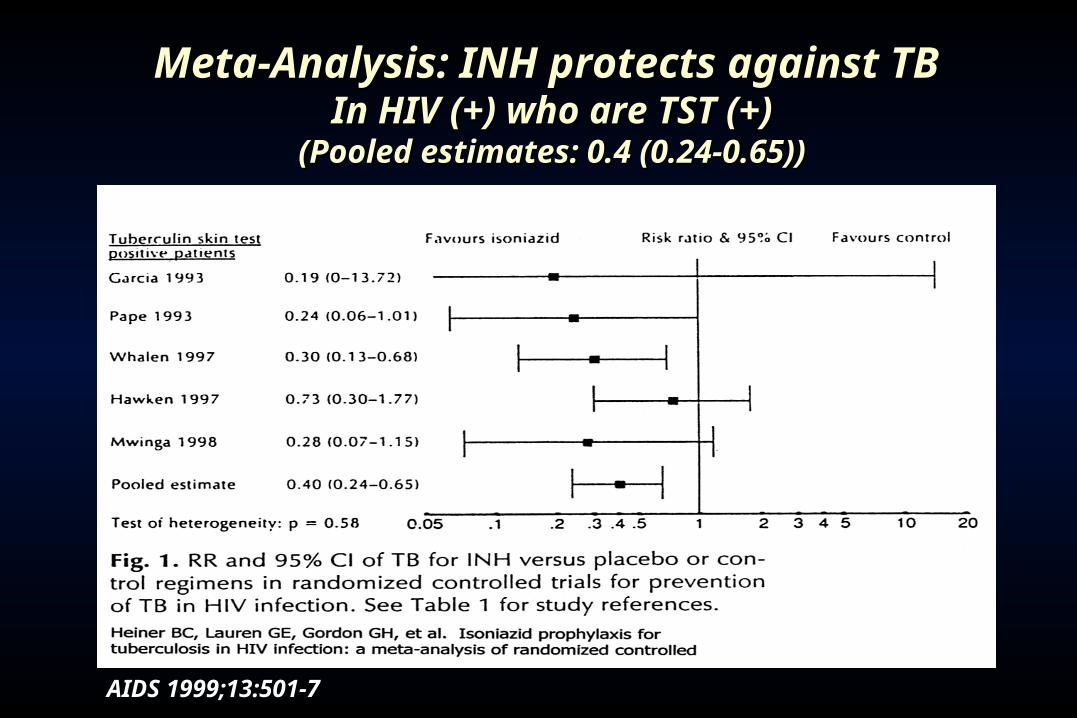
Meta-Analysis: INH protects against TB Meta-Analysis: INH protects against TB In HIV (+) who are TST (+)In HIV (+) who are TST (+)
(Pooled estimates: 0.4 (0.24-0.65))(Pooled estimates: 0.4 (0.24-0.65))
AIDS 1999;13:501-7

AIDS 1999;13:501-7
Meta-Analysis: INH does not protect against TB – In Meta-Analysis: INH does not protect against TB – In HIV (+) who are TST (-)HIV (+) who are TST (-)
(Pooled estimates: 0.84 (0.54-1.30))(Pooled estimates: 0.84 (0.54-1.30))

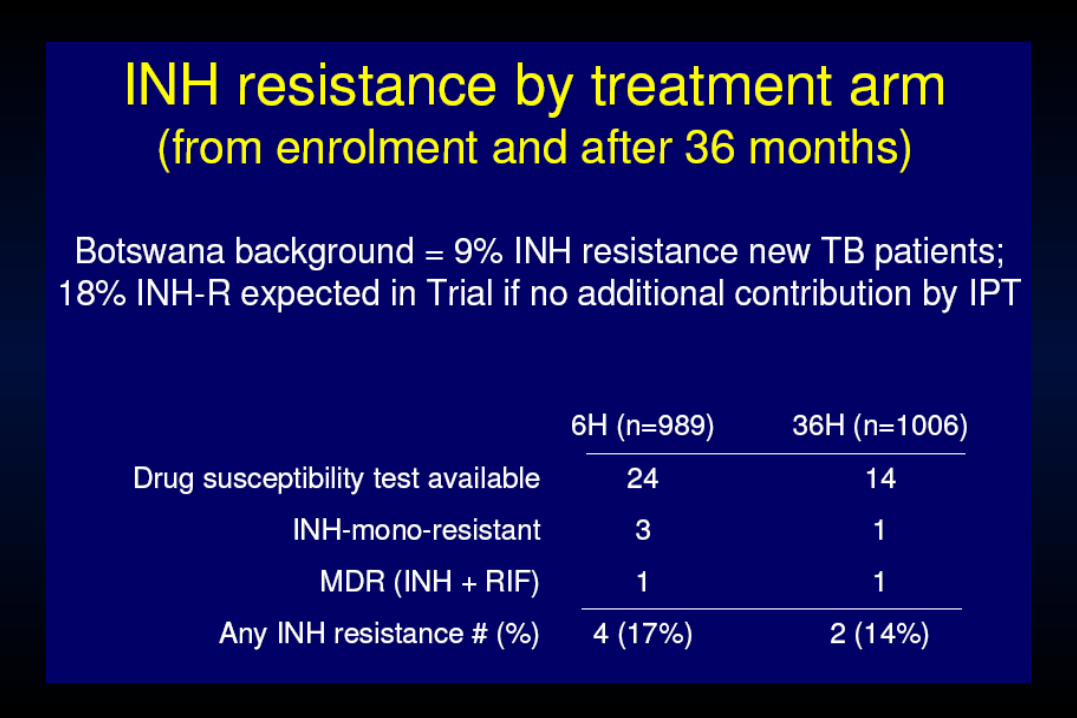
Does INH treatment of LTBI create INH resistance?

INH treatment and INH resistance
• This was assessed in a large cohort of SE Asian refugees who were screened and treated after arrival in the US.– No difference in rates of INH Resistant TB in persons
who took INH, vs those who took nothing
• Meta-analysis (Godfrey-Fausett et al)– Reviewed placebo controlled RCT of INH– Small, but non-significant increase

LTBI treatment – what are the options?
• 6-9 months of INH
• 2 months RIF-PZA
• 3-4 months INH-RIF
• 3 months once weekly INH& Rifapentine
• 4 months RIFampin

Experimental Study of Short-Course Preventive Therapy in Mice – the start of 2RIF-PZA
Lecour HF, et.al. Am Rev Respir Dis 1989:140:1189-93

International Study of 12INH vs 2RIF-PZA in HIV Infected patients - OUTCOMES
Regimen 2 RIF/PZA 12 INH RR (CI)
No. enrolled 791 790
Confirmed TB 19 26 0.7 (.4,1.2)
Conf/Probable TB 28 29 0.95 (.6,1.2)
Death 139 159 0.9 (.7,1.1)
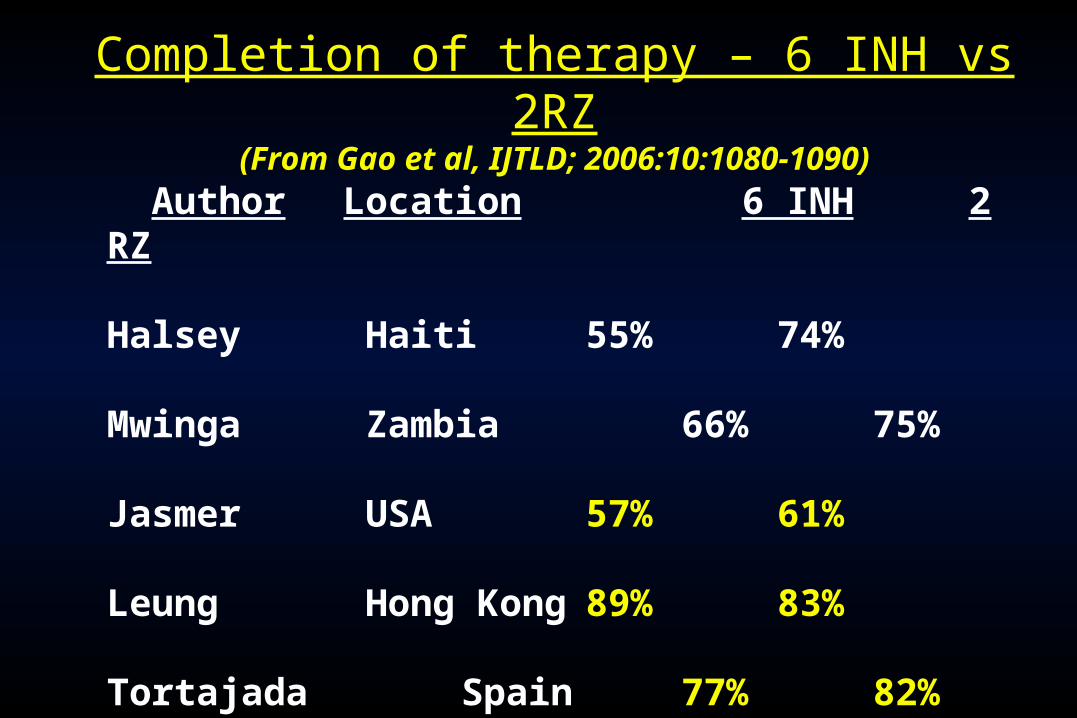
Completion of therapy – 6 INH vs 2RZ(From Gao et al, IJTLD; 2006:10:1080-1090)
Author Location 6 INH 2 RZ
Halsey Haiti 55% 74%
Mwinga Zambia 66% 75%
Jasmer USA 57% 61%
Leung Hong Kong 89% 83%
Tortajada Spain 77% 82%
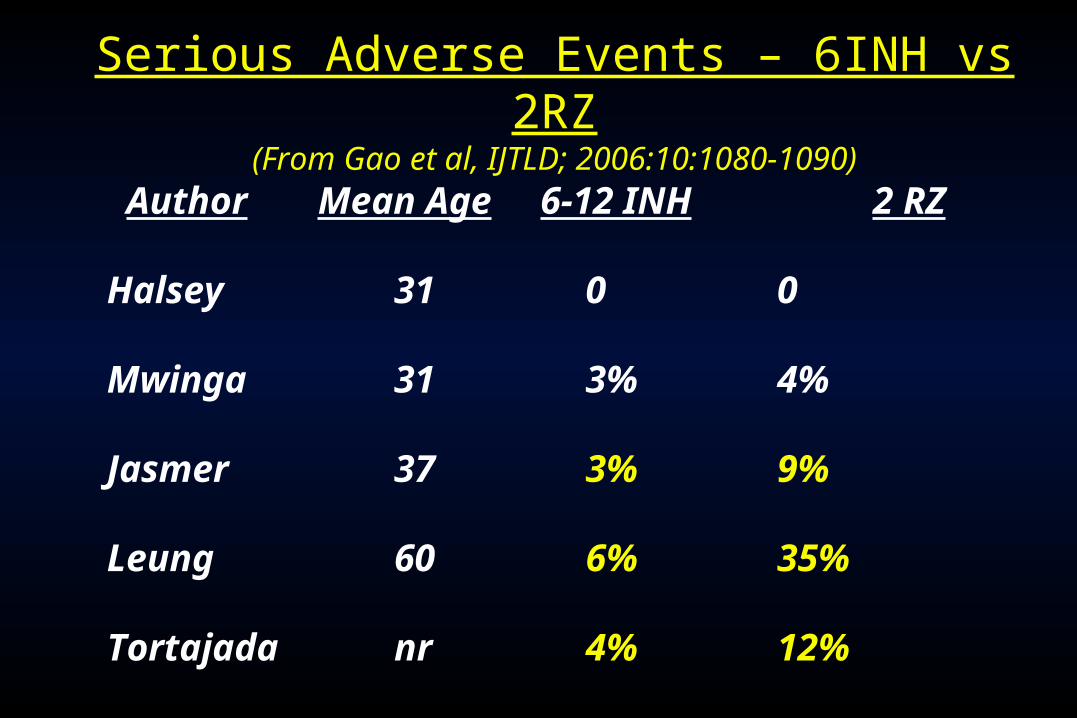
Serious Adverse Events – 6INH vs 2RZ(From Gao et al, IJTLD; 2006:10:1080-1090)
Author Mean Age 6-12 INH 2 RZ
Halsey 31 0 0
Mwinga 31 3% 4%
Jasmer 37 3% 9%
Leung 60 6% 35%
Tortajada nr 4% 12%

2 months Rifampin and PZA
• In 1989 – 2 mos RIF&PZA – effective in mice
• 1990-2000 – several trials – all in HIV infected
• 2000 – Strong recommendations – to use this
• 2000-2001 – Reports of severe hepatitis
• 2001 – recommendation withdrawn
• DO NOT USE 2 RIF-PZA
LTBI treatment – what are the options?
• 6-9 months of INH
• 2 months RIF-PZA
• 3-4 months INH-RIF
• 3 months once weekly INH& Rifapentine
• 4 months RIFampin

3-4 mos Rifampin-INH vs 6-12 mos INH 3-4 mos Rifampin-INH vs 6-12 mos INH A meta-analysis of 5 RCT’s A meta-analysis of 5 RCT’s
Occurrence of active TBOccurrence of active TB(Ena & Valls, Clin Inf Dis; 2005; 40: 670-676)(Ena & Valls, Clin Inf Dis; 2005; 40: 670-676)
(+0.1%)
41/97239/954Pooled estimates
(+0.3%)9/5567/536Whalen (Uganda – HIV)
(+0.1%)
3/823/83Rivero (Spain – HIV)
(- 3.3%)2/694/64Martinez (Spain - HIV)
(+1.0%)1/980/98Martinez (Spain – HIV)
(+1.1%)26/16725/173Hong Kong (silicotics)
(Diff. %)INH/RIF INH

3-4 mos Rifampin-INH vs 6-12 mos INH 3-4 mos Rifampin-INH vs 6-12 mos INH A meta-analysis of 5 RCT’s A meta-analysis of 5 RCT’s Serious Adverse EventsSerious Adverse Events
(Ena & Valls, Clin Inf Dis; 2005; 40: 670-676)(Ena & Valls, Clin Inf Dis; 2005; 40: 670-676)
(+0.1%)48/97246/954Pooled estimates
(+1.7%)13/5563/536Whalen (Uganda – HIV)
(+11%)15/826/83Rivero (Spain – HIV)
(- 16%)5/6915/64Martinez (Spain - HIV)
(- 2.0%)7/989/98Martinez (Spain – HIV)
(- 2.7%)8/16713/173Hong Kong (silicotics)
(Diff. %)INH/RIF INH

LTBI treatment – what are the options?
• 6-9 months of INH
• 2 months RIF-PZA
• 3-4 months INH-RIF
• 3 months once weekly INH& Rifapentine
• 4 months RIFampin

3 months INH & Rifapentine (3HP)
• Large scale trial – just completed
• 96% HIV negative
• US, Canada, Spain and Brazil
• 9 months daily INH vs 3 months INH/RPT once weekly – 12 doses – directly observed
• More than 8,000 enrolled
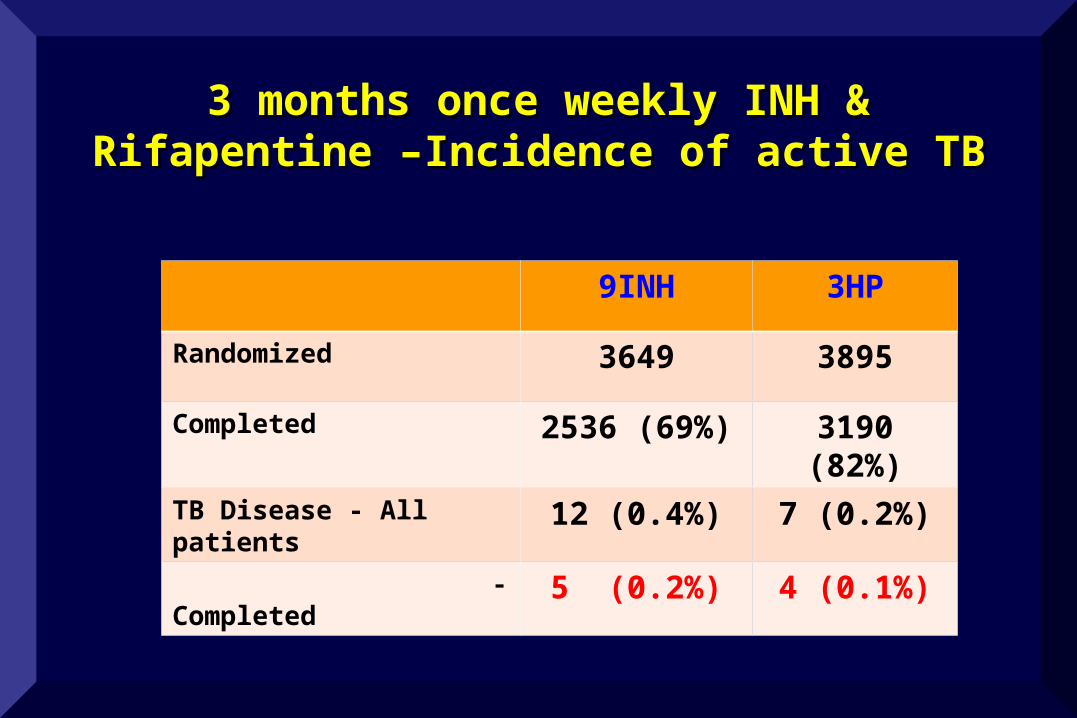
3 months once weekly INH & 3 months once weekly INH & Rifapentine –Incidence of active TBRifapentine –Incidence of active TB
9INH 3HP
Randomized 3649 3895
Completed 2536 (69%) 3190 (82%)
TB Disease - All patients
12 (0.4%) 7 (0.2%)
- Completed
5 (0.2%) 4 (0.1%)

3 months once weekly INH & 3 months once weekly INH & Rifapentine – Adverse eventsRifapentine – Adverse events
9INH 3HP
Randomized 3649 3895
Total- Grade 3-4 AE 7.4% 6.0%
Drugs stopped for AE 3.6% 5.0%
Hepatotoxicity 2.8% 0.5%
Hypersensitivity 0.8% 4.0%

LTBI treatment – what are the options?
• 6-9 months of INH
• 2 months RIF-PZA
• 3-4 months INH-RIF
• 3 months once weekly INH & Rifapentine
• 4 months RIFampin

Experimental Study of Short-Course
Preventive Therapy in Mice – what about RIF?
Lecour HF, et.al. Am Rev Respir Dis 1989:140:1189-93
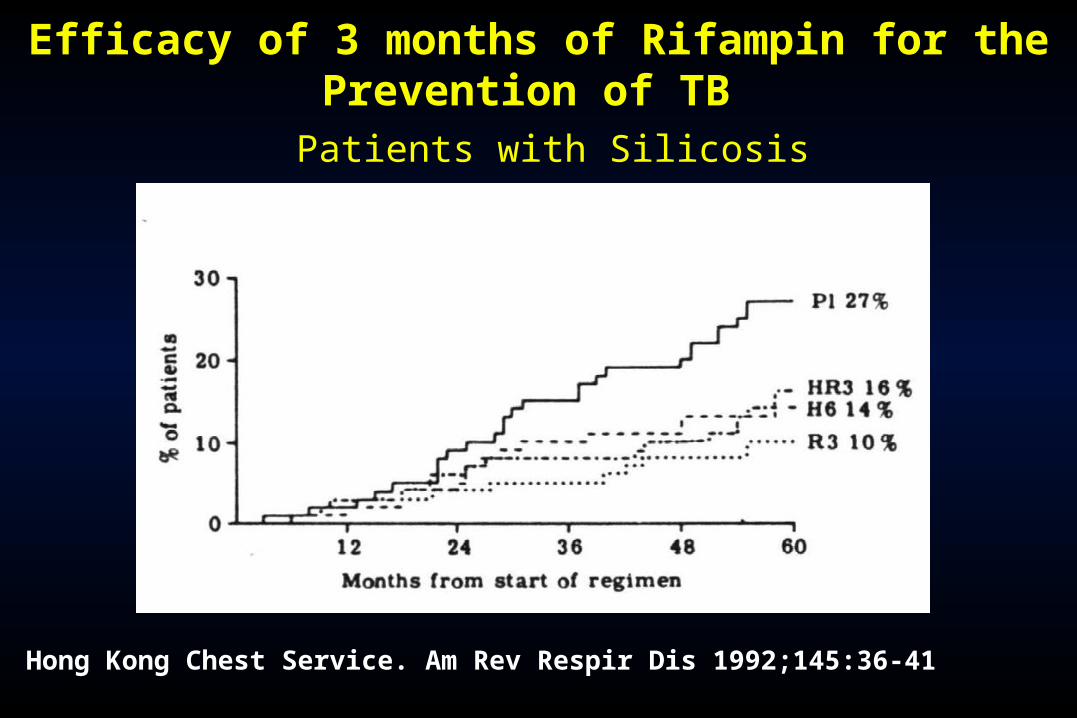
Efficacy of 3 months of Rifampin for the Prevention of TB
Patients with Silicosis
Hong Kong Chest Service. Am Rev Respir Dis 1992;145:36-41
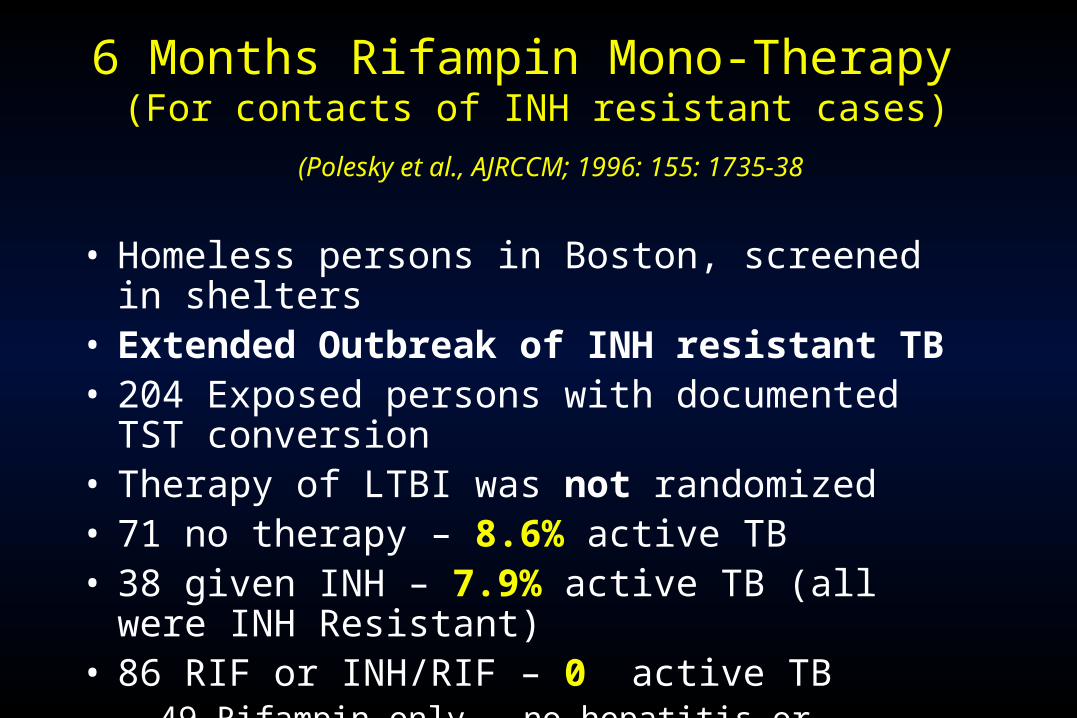
6 Months Rifampin Mono-Therapy (For contacts of INH resistant cases)
(Polesky et al., AJRCCM; 1996: 155: 1735-38
• Homeless persons in Boston, screened in shelters• Extended Outbreak of INH resistant TB• 204 Exposed persons with documented TST conversion• Therapy of LTBI was not randomized• 71 no therapy – 8.6% active TB• 38 given INH – 7.9% active TB (all were INH Resistant)• 86 RIF or INH/RIF – 0 active TB
– 49 Rifampin only – no hepatitis or increased LFT’s

Program Experience with 4RIF and 9INHMaryland 1999-2004
Page et al. Archives Internal Med. 2006: 166; 1863-70
• Patients offered 4 RIF or 9 INH by provider• Concurrent study but non-randomized
4 RIF 9 INH
Number Starting 1,379 770
Completing Therapy 987 (72%) 405 (52%)
Grade 3 to 4 Hepatitis 1 (0.1%) 12 (2%)

Program Experience with 4RIF and 9INHNew Jersey 1999-2004
Lardizabal et al. Chest, 2006: 130;1712-16
4 RIF 9 INH
Number Starting 261 213
Completing Therapy 210 (81%) 113 (53%)
Grade 3 to 4 SAE 8 (3%) 13 (6%)
Hepatitis 0 3
Non-concurrent and non-randomized study
A randomized trial to compare 4 months Rifampin vs 9 months
INH for the treatment of LTBI
Phase 1: Compliance and completion
Completed in 2003
Phase 2 – Adverse events and costsCompleted in 2007
Phase 3: Efficacy and effectiveness

RCT of 9 INH vs. 4 RIF for LTBI
Study design
• Design - open label randomized trial• Positive control = 9INH
– Not placebo as INH of proven benefit

RCT of 4RIF vs 9INH for LTBI
Study Population – Inclusion Criteria
Positive TST, high risk - prescribed LTBI treatment.• Highest risk reactors – Risk of reactivation >1% per year
– Close contact, TST conversion, HIV (+), apical fibronodular disease
• Moderate Risk (risk of 0.5% - 1% per year)– Diabetes, renal failure, immuno-compromise– Casual contacts, TST conversion in 2-5years– Or two of the following three:
• Arrival in the past two years from TB endemic country• Less than 90% ideal body weight• Granulomas, calcified nodes• TST > 15mm

RCT of 4RIF vs 9INH for LTBI
Study Population – Exclusion Criteria
• Exclude as few as possible
• Essential exclusion criteria:– Contacts of INH or RIF resistant (or MDR) index cases– High potential for drug interactions (Certain HIV therapy,
or oral contraceptives)– Known INH or RIF allergy
• All other patients eligible if LTBI therapy prescribed– Regardless of age, or other risk factors for SAE

RCT of 4RIF vs 9INH for LTBI
Data Gathering in treatment phase – Pragmatic trial
• As little impact on follow-up as possible, i.e. routine follow-up– Follow-up visits will be monthly for first 2 months, or
more often per physician – CBC, liver transaminases at baseline and first follow-
up visit
• Study staff to have as little direct involvement as possible– Minimize ‘study effect’ – Estimate effectiveness under ‘routine’ conditions
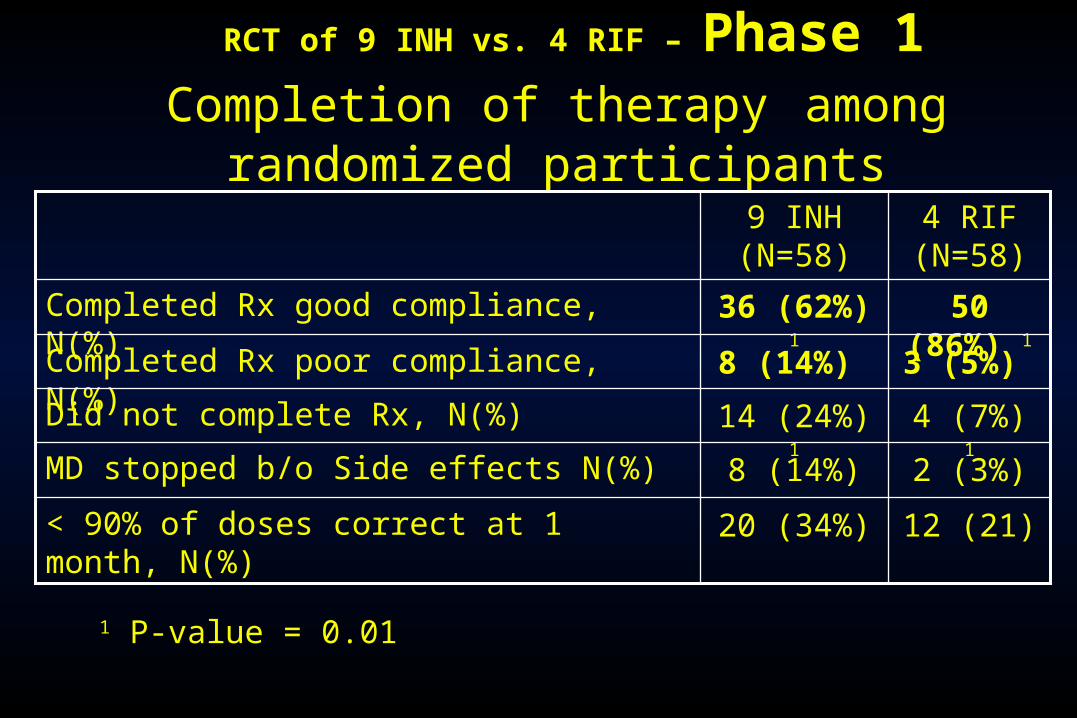
RCT of 9 INH vs. 4 RIF – Phase 1Completion of therapy among randomized participants
3 (5%) 8 (14%) Completed Rx poor compliance, N(%)
2 (3%)8 (14%)MD stopped b/o Side effects N(%)
12 (21)20 (34%) < 90% of doses correct at 1 month, N(%)
4 (7%) 114 (24%) 1Did not complete Rx, N(%)
50 (86%) 136 (62%) 1Completed Rx good compliance, N(%)
4 RIF (N=58)
9 INH (N=58)
1 P-value = 0.01

RCT of 4RIF vs. 9INH for LTBI – Phase 1 Phase 1: Side effects associated with the 2
regimens
27% 114% 1Minor, %
22Major – other, N
04Major – hepatitis, N
4 RIF 9 INH
1 P-value = <0.001

RCT of 4RIF vs. 9INH for LTBI – Phase 2
Completion of Phase 2 Study
4 RIF
(N=420)
9 INH
(N=427)
P-value
Completed Therapy N (%) 339 (81%) 259 (69%) <.0001
Patient Non-compliant (Total)
- Drop-out
- Intolerance
61 (14%)52 (12%)
3 (1%)
117 (27%)82 (20%)
23 (5%)
MD Non-compliant 6 (1%) 12 (3%)

RCT of 4RIF vs. 9INH for LTBI – Phase 2
Serious Drug Related Adverse Events
4 RIF
(N=420)
9 INH
(N=427)
P-value
All Grades – Total (%) * 16 (3.8%) 24 (5.6%) NS
Grade 3 to 4 - Total
- Hepato-toxicity
- Hematologic
- Drug Interaction
- Rash
6 (1.5%)
3 (0.7%)1
1
1
17 (4.0%)
16 (3.8%)1
0
0
.02
.003
-
-
-
Grade 1 to 2 - Total
- Rash
- GI intolerance
- Hematologic
11 (2.0%)
8
1
2
7 (1.6%)
4
2
0
NS
NS
-
-
* Severity, type + relationship to study drug by independent blinded 3-member panel

RCT of 4RIF vs. 9INH for LTBI – Phase 2Therapy Stopped Permanently but Not Related to Study Drug*
4 RIF
(N=420)
9 INH
(N=427)
P-value
Death 0 1
Pregnancy 2 3
* The severity, type and relationship to study drug judged by independent three-member panel blinded to patient allocation.

Serious adverse events significantly less than 9INH• Particularly for grade 3 to 4 hepatitis
• The most important/lethal complication
• Completion significantly better with 4RIF than 9INH• Both in Phase 2 and in Phase 1
• Overall costs lower with 4RIF• Despite high RIF costs in Canada
Conclusions – 4RIF

RCT of 4RIF vs 9INH for LTBI – Phase 3 Objectives of Phase 3
• Primary objective (effectiveness)– Compare incidence of confirmed active TB in all randomized
in the 28 months post-randomization
– “Pragmatic” trial – estimate under programme conditions.
• Secondary objectives– Compare incidence of confirmed active TB in those who took
at least 80% of doses within maximum allowed time (efficacy)
– Compare incidence of confirmed plus clinical active TB in all randomized
– Compare serious adverse events

RCT of 4RIF vs 9INH for LTBI –
Timelines of Phase 3
• Planned enrolment is almost 6,000 persons
• Enrolment to end in 2013
• Last follow-up will end in 2015
• Publication in 2016!!
• Wish me luck – (even just to last that long!!)

Thank - you


















