
DIAGNOSIS AND TREATMENT OF JOGGER S HEEL - … AND TREATMENT OF JOGGER S HEEL ... or weight-bearing...
6
Art & science | foot injuries Art & science | acute care February 2015 | Volume 22 | Number 9 EMERGENCY NURSE 18 Art & science | The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON Correspondence [email protected] Laura Horobin is an emergency care practitioner paramedic at the University of Wolverhampton Date of submission November 11 2014 Date of acceptance January 6 2015 Peer review This article has been subject to double-blind review and has been checked using antiplagiarism software Author guideliness rcnpublishing.com/r/ en-author-guidelines DIAGNOSIS AND TREATMENT OF JOGGER’S HEEL Laura Horobin outlines how to identify plantar fasciitis, a common complaint in people who weight bear for long periods, and why the condition should be managed conservatively Research suggests that there is a positive association between plantar heel pain and calcaneal heel spurs, which despite being located in the flexor digitorum brevis can be caused by traction of the plantar aponeurosis (Irving et al 2008). However, most research into plantar heel pain is retrospective and does not specify causation. Thomas et al (2010), for example, found no relationship between heel spurs, which are common in the general population, and the signs and symptoms of plantar fasciitis. Plantar fasciitis is more common in women than men (Schwartz and John 2014). Other intrinsic risk factors include: ■ Flat feet, or pes planus. ■ High-arched feet, or pes cavus. ■ Obesity. ■ Tight Achilles tendon. ■ Weak foot muscles, especially plantar flexor muscles. Extrinsic risk factors include: ■ Inadequate stretching. ■ Poor biomechanics or body alignment. ■ Poorly fitting shoes or those without appropriate midsoles. ■ Prolonged standing. ■ Running long distances quickly. ■ Walking barefoot. ■ Walking on hard surfaces. A case study involving a man diagnosed with plantar fasciitis is discussed in the case study opposite. It is important to differentiate between plantar fasciitis and other possible diagnoses by recognising clinical signs and making appropriate investigations. If patient histories and examination findings are PLANTAR FASCIITIS, also known as ‘flip-flop disease’, jogger’s heel and plantar fasciopathy, is thought to be the most common cause of heel pain (Neufeld and Gerrato 2008). Although the exact aetiology of plantar fasciitis is unknown, overloading during extended periods of walking or weight-bearing can contribute to inflammation and subsequently increase pain (Braddam and Buschbacher 2007). Tatli and Kapasi (2009) suggest that diagnosis of plantar fasciitis is predominantly clinical and that there is little justification for further medical investigation. In 90% of people with plantar fasciitis, acute episodes resolve after between six and eight weeks of conservative treatment, but in 10% plantar fasciitis becomes a chronic condition (Neufold and Gerrato 2008). Early identification and treatment can decrease the risk of long-term problems, such as recurrent pain and reduced mobility leading to an inability to work (Irving et al 2008). Abstract Plantar fasciitis, the most common cause of heel pain, is a self-limiting condition exacerbated by weight bearing after episodes at rest that usually resolves within 12 months after conservative treatment. This article outlines the aetiology of plantar fasciitis and refers to a case study in discussing diagnosis, examination and management. Keywords Plantar fasciitis, foot, heel, inflammation, pain, walking, weight bearing
Transcript of DIAGNOSIS AND TREATMENT OF JOGGER S HEEL - … AND TREATMENT OF JOGGER S HEEL ... or weight-bearing...

Art & science | foot injuriesArt & science | acute care
February 2015 | Volume 22 | Number 9 EMERGENCY NURSE18
Art & science | The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON
Laura Horobin is an emergency care practitioner paramedic at the University of Wolverhampton
Date of submissionNovember 11 2014
Date of acceptanceJanuary 6 2015
Peer reviewThis article has been subject to double-blind review and has been checked using antiplagiarism software
Author guidelinessrcnpublishing.com/r/en-author-guidelines
DIAGNOSIS AND TREATMENT OF JOGGER’S HEEL
Laura Horobin outlines how to identify plantar fasciitis, a common complaint in people who weight bear for long periods, and why the condition should be managed conservatively
Research suggests that there is a positive association between plantar heel pain and calcaneal heel spurs, which despite being located in the flexor digitorum brevis can be caused by traction of the plantar aponeurosis (Irving et al 2008). However, most research into plantar heel pain is retrospective and does not specify causation. Thomas et al (2010), for example, found no relationship between heel spurs, which are common in the general population, and the signs and symptoms of plantar fasciitis.
Plantar fasciitis is more common in women than men (Schwartz and John 2014). Other intrinsic risk factors include:■ Flat feet, or pes planus.■ High-arched feet, or pes cavus.■ Obesity.■ Tight Achilles tendon.■ Weak foot muscles, especially plantar
flexor muscles.Extrinsic risk factors include:■ Inadequate stretching.■ Poor biomechanics or body alignment.■ Poorly fitting shoes or those without
appropriate midsoles.■ Prolonged standing.■ Running long distances quickly.■ Walking barefoot.■ Walking on hard surfaces.A case study involving a man diagnosed with plantar fasciitis is discussed in the case study opposite.
It is important to differentiate between plantar fasciitis and other possible diagnoses by recognising clinical signs and making appropriate investigations. If patient histories and examination findings are
PLANTAR FASCIITIS, also known as ‘flip-flop disease’, jogger’s heel and plantar fasciopathy, is thought to be the most common cause of heel pain (Neufeld and Gerrato 2008). Although the exact aetiology of plantar fasciitis is unknown, overloading during extended periods of walking or weight-bearing can contribute to inflammation and subsequently increase pain (Braddam and Buschbacher 2007).
Tatli and Kapasi (2009) suggest that diagnosis of plantar fasciitis is predominantly clinical and that there is little justification for further medical investigation. In 90% of people with plantar fasciitis, acute episodes resolve after between six and eight weeks of conservative treatment, but in 10% plantar fasciitis becomes a chronic condition (Neufold and Gerrato 2008). Early identification and treatment can decrease the risk of long-term problems, such as recurrent pain and reduced mobility leading to an inability to work (Irving et al 2008).
AbstractPlantar fasciitis, the most common cause of heel pain, is a self-limiting condition exacerbated by weight bearing after episodes at rest that usually resolves within 12 months after conservative treatment. This article outlines the aetiology of plantar fasciitis and refers to a case study in discussing diagnosis, examination and management.
KeywordsPlantar fasciitis, foot, heel, inflammation, pain, walking, weight bearing

EMERGENCY NURSE February 2015| Volume 22 | Number 9 19
Alam
y

Art & science | acute care
February 2015 | Volume 22 | Number 9 EMERGENCY NURSE20
Art & science | foot injuries
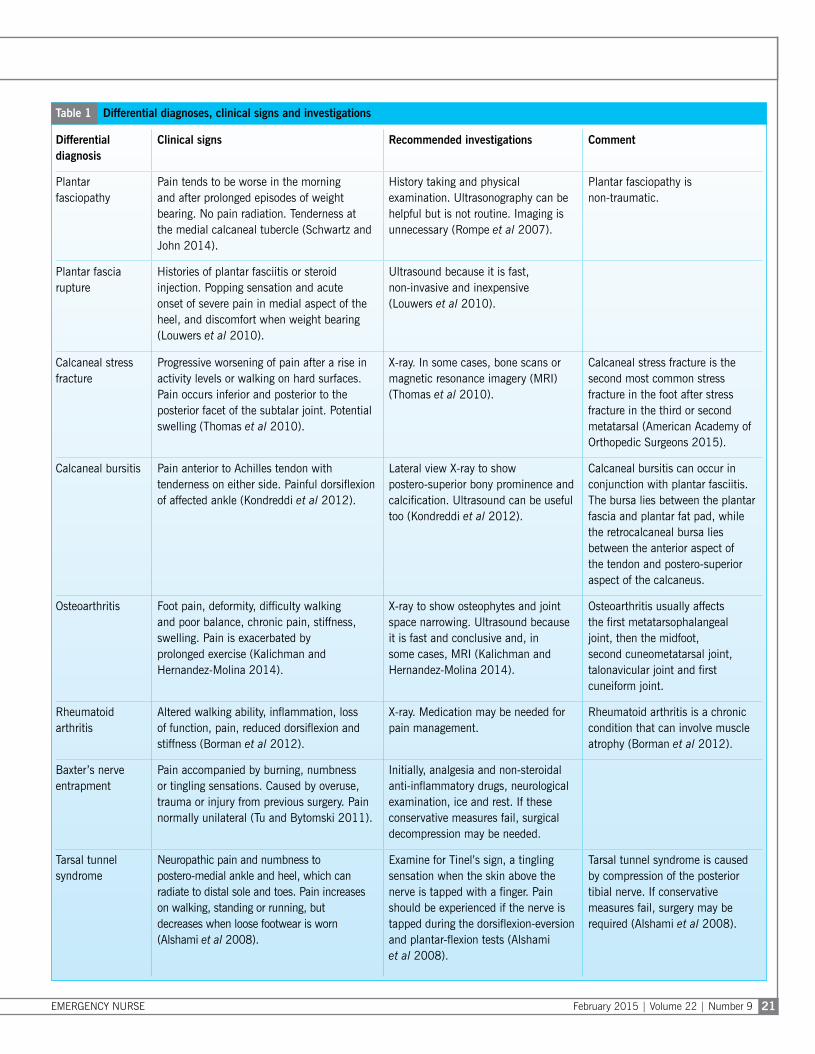
ambiguous, differentials such as bony injury and Achilles tendonitis, should be excluded. Differential diagnoses are extensive and can include fat-pat atrophy, osteomyelitis, bone cyst, Ewing’s sarcoma and Paget’s disease. A selection of differential diagnoses, clinical signs and related investigations are shown in Table 1.
DiagnosisAetiology The plantar fascia is made up of pearly white fibres arranged longitudinally between the medial tuberosity of the calcaneus, where the fibres are thin, and the centre of the calcaneus, where they are thicker and divide into five bands that surround local tendons (Tatli and Kapasi 2009). As a result of ageing and secondary to risk factors, such as prolonged weight-bearing activities, the plantar fascia develops signs of degenerative change. The fascia not only provides support to the foot, but also acts as a shock absorber to the foot and leg. As it stretches it allows the foot to accommodate irregularities on walking surfaces. The application of ice to the
fascia should initiate vasoconstriction and reduce inflammation (Foye 2013).
Signs and symptoms To diagnose plantar fasciitis accurately, it is vital to take accurate patient histories, consider the risk factors listed in Table 1 and complete thorough physical examinations (Goff and Crawford 2011).
According to Roxas (2005), weight gain, occupational-related activity, poor biomechanics and inadequate footwear contribute to plantar fasciitis. Typically, people with plantar fasciitis experience more pain when first putting a foot to the floor, for example after prolonged periods of rest or weight bearing. Other characteristic symptoms include no history of trauma, tenderness over midfoot tissues, no radiation of pain and limping. Poor support footwear can also contribute to development of plantar fasciitis (Tatli and Kapasi 2009), while Cutts et al (2012) state that it is caused by repetitive microtrauma due to lifestyle or exercise.
Examination In examining patients with suspected plantar fasciitis, practitioners should look, feel and move the affected limbs. If plantar fasciitis is present, the limb will be neurovascularly intact. There should be no obvious abnormalities or deformities compared with the unaffected limb, no oedema or skin changes, and no bony tenderness over tibia, fibula, malleoli, tarsals, metatarsals and metacarpophalangeal joints and digits. However, palpation of the medial calcaneal tubercle region should elicit a sharp stabbing pain. Meanwhile, passive ankle and first toe dorsiflexion, in which the toes are moved towards the shin, should cause some discomfort in the proximal plantar fascia, which might predispose tightening of the Achilles tendon.
Patients with the condition should have a good range of movement, including inversion, eversion, plantar flexion and dorsiflexion, as well as strong equal pedal pulses bilaterally, full sensation in the affected limb and normal gait (Schwartz and John 2014). Active or passive dorsiflexion of the ankle and foot stretches the plantar fascia. This exacerbates pain during acute episodes, which is diagnostically helpful (Ogden et al 2001). The plantar fascia itself is involved in maintaining walking stability and can break after only a minimal amount of strain, such as an increased amount of walking on a daily basis.
If findings from history taking and physical examination do not indicate plantar fasciitis, differential diagnoses should be considered (Goff and Crawford 2011). Imaging is not necessary to diagnose plantar fasciitis but can be valuable to help distinguish it from other conditions.
Case studyAn unaccompanied 59-year-old man presented at a walk-in centre. He was limping on his right foot and seemed to be in some discomfort, but otherwise appeared well. History taking revealed that he was a manual labourer who spent a lot of his working life on his feet. Over the previous week he had experienced pain in the arch of his right foot first thing in the morning, although it had eased slightly by the time he got to work. Throughout his work shifts the pain would return to the extent that he had to rest his foot periodically and the severity of pain had increased each day. The man was of average weight, and had no history of trauma to his ankle or foot.
Examination of the patient’s right foot and comparison with the left revealed an increase in pain to the right calcaneum on palpation with maximum tenderness over the soft tissue. The patient experienced pain during manipulation of the plantar surface of the right foot and pain increased on dorsiflexion, but there
was no bony tenderness nor evidence of trauma.
The patient described the pain as recent and intermittent, rather than chronic and severe, which suggested plantar fasciitis. His history was also typical of plantar fasciitis with no contraindications, such as ulcers or gastritis. No X-ray was required.
The emergency care practitioner on call advised the patient to take non-steroidal anti-inflammatory drugs, such as ibuprofen, and paracetamol to control the pain, although he was advised that he could be prescribed dexamethasone if the pain continued or increased in severity over the next six months. The practitioner also discussed ongoing management of the condition, including massage and the use of orthoses in his shoes to reduce inflammation and pain on his return to work. She also advised the patient to rest before returning to work and undertake a series of stretching exercises, and to return to the walk-in centre if the pain returned.
EMERGENCY NURSE February 2015 | Volume 22 | Number 9 21
Differential diagnosis
Clinical signs Recommended investigations Comment
Plantar fasciopathy
Pain tends to be worse in the morning and after prolonged episodes of weight bearing. No pain radiation. Tenderness at the medial calcaneal tubercle (Schwartz and John 2014).
History taking and physical examination. Ultrasonography can be helpful but is not routine. Imaging is unnecessary (Rompe et al 2007).
Plantar fasciopathy is non-traumatic.
Plantar fascia rupture
Histories of plantar fasciitis or steroid injection. Popping sensation and acute onset of severe pain in medial aspect of the heel, and discomfort when weight bearing (Louwers et al 2010).
Ultrasound because it is fast, non-invasive and inexpensive (Louwers et al 2010).
Calcaneal stress fracture
Progressive worsening of pain after a rise in activity levels or walking on hard surfaces. Pain occurs inferior and posterior to the posterior facet of the subtalar joint. Potential swelling (Thomas et al 2010).
X-ray. In some cases, bone scans or magnetic resonance imagery (MRI) (Thomas et al 2010).
Calcaneal stress fracture is the second most common stress fracture in the foot after stress fracture in the third or second metatarsal (American Academy of Orthopedic Surgeons 2015).
Calcaneal bursitis Pain anterior to Achilles tendon with tenderness on either side. Painful dorsiflexion of affected ankle (Kondreddi et al 2012).
Lateral view X-ray to show postero-superior bony prominence and calcification. Ultrasound can be useful too (Kondreddi et al 2012).
Calcaneal bursitis can occur in conjunction with plantar fasciitis. The bursa lies between the plantar fascia and plantar fat pad, while the retrocalcaneal bursa lies between the anterior aspect of the tendon and postero-superior aspect of the calcaneus.
Osteoarthritis Foot pain, deformity, difficulty walking and poor balance, chronic pain, stiffness, swelling. Pain is exacerbated by prolonged exercise (Kalichman and Hernandez-Molina 2014).
X-ray to show osteophytes and joint space narrowing. Ultrasound because it is fast and conclusive and, in some cases, MRI (Kalichman and Hernandez-Molina 2014).
Osteoarthritis usually affects the first metatarsophalangeal joint, then the midfoot, second cuneometatarsal joint, talonavicular joint and first cuneiform joint.
Rheumatoid arthritis
Altered walking ability, inflammation, loss of function, pain, reduced dorsiflexion and stiffness (Borman et al 2012).
X-ray. Medication may be needed for pain management.
Rheumatoid arthritis is a chronic condition that can involve muscle atrophy (Borman et al 2012).
Baxter’s nerve entrapment
Pain accompanied by burning, numbness or tingling sensations. Caused by overuse, trauma or injury from previous surgery. Pain normally unilateral (Tu and Bytomski 2011).
Initially, analgesia and non-steroidal anti-inflammatory drugs, neurological examination, ice and rest. If these conservative measures fail, surgical decompression may be needed.
Tarsal tunnel syndrome
Neuropathic pain and numbness to postero-medial ankle and heel, which can radiate to distal sole and toes. Pain increases on walking, standing or running, but decreases when loose footwear is worn (Alshami et al 2008).
Examine for Tinel’s sign, a tingling sensation when the skin above the nerve is tapped with a finger. Pain should be experienced if the nerve is tapped during the dorsiflexion-eversion and plantar-flexion tests (Alshami et al 2008).
Tarsal tunnel syndrome is caused by compression of the posterior tibial nerve. If conservative measures fail, surgery may be required (Alshami et al 2008).
Table 1 Differential diagnoses, clinical signs and investigations

Art & science | acute care
February 2015 | Volume 22 | Number 9 EMERGENCY NURSE22
Art & science | foot injuries
ManagementOrthoses Landorf et al (2006) claim that orthoses, or shoe inserts that correct abnormalities in the foot, can reduce pain in 90% of patients, but report little relief for those with persistent or severe symptoms (Neufold and Gerrato 2008).
Steroids Alternative treatment includes steroid injections, which Crawford et al (1999) suggest decrease pain for up to one month with pain returning at around three months. Steroid injections can be painful and should not be made regularly, however, so it is important to try all conservative measures, such as ice, stretching exercises and pain relief, before considering corticosteroids (Lee and Ahmad 2007, National Institute for Health and Care Excellence (NICE) 2014).
McMillan et al (2012) undertook a randomised controlled trial to establish if dexamethasone, a corticosteroid, is effective after use of lidocaine, a tibial nerve block. The effect of corticosteroid on a group of participants was measured against that of a placebo, namely normal saline, on a group of the same size. Results show that dexamethasone is safe and effective for short-term treatment of plantar fasciitis, provides better pain relief at four weeks than the placebo, and reduces inflammation and swelling over several months.
Although the McMillan et al (2012) conclude that treatment with a corticosteroid reduces inflammation and pain, further studies involving larger sample
sizes are needed to differentiate the effects of corticosteroid administration from that of placebo. A larger trial could involve initial administration of corticosteroid or placebo, second doses at four weeks and review at eight weeks to determine if pain continues to reduce, and further review at 12 months to see if inflammation has resolved. According to NICE (2014), there is no literature on the efficacy of second corticosteroid injections. It should be noted that Tatli and Kapasi (2009), and Toomey (2009), recommend limiting the number of corticosteroid injections to two to avoid plantar fascia rupture.
Soundwaves Ultrasonic ‘shockwaves’ have been administered to patients with musculoskeletal disorders for 15 years to reduce the severity and number of episodes of pain. Focal shockwaves stimulate tissues while radial shockwaves cause disintegration of fibroses and increases blood circulation to treated locations (Greve et al 2009).
Stretching Evidence suggests that stretching the fascia is the most effective, inexpensive and straightforward way to manage plantar fasciitis. In a clinical trial conducted two years after stretching exercises had begun, Digiovanni et al (2006) showed that the patients concerned experienced less pain and were generally satisfied.
Degeneration of the plantar fascia affects up to 10% of the general population, so the preferred treatment is physiotherapy to suppress existing
Clockwise from above: Achilles tendon stretching, wall push ups with knee held straight and, far right, with leading knee bent, stair stretching and dynamic stretching
Figure 1 Examples of self-physiotherapy exercises for people with plantar fasciitis

EMERGENCY NURSE February 2015 | Volume 22 | Number 9 23
pain and restore function of the fascia to assist gait. Although there are limited reviews of the benefits of self-physiotherapy, Digiovanni et al (2006) found that stretching exercises for plantar fasciitis can reduce pain, while other clinical reviews note that stretching exercises are advantageous for this condition (Thing et al 2012). Nurses should therefore recommend and explain such self-physiotherapy exercises to patients (Figure 1). The exercises may include:■ Achilles tendon and plantar fascia stretching,
in which the patient should loop a towel around one foot and pull it taught for 30 seconds while the knees are kept straight to cause dorsiflexion. The process should be undertaken at least three times with each foot.
■ Wall push ups, in which the patient places both hands against a wall at shoulder height while placing one foot in front of the other and about 30cm from the wall. The patient then bends the front knee while keeping the back knee straight and then lean towards the wall to tighten the gastrocnemous before slowly releasing. The process should be undertaken at least ten times and then repeated a further ten times while the back foot is moved forwards slightly causing the back knee to bend slightly.
■ Stair stretching, in which the patient stands at the bottom of a flight of stairs so that most of the feet
are on the tread but the heels are suspended over the riser. Holding the hand rail for support and, with the legs are slightly apart, the patient should lower the heels below the tread while keeping both knees straight until the gastrocnemius begins to tighten. This position should be held for between 20 and 60 seconds before the patient returns to the start position and repeats five times in the morning and six times in the evening.
■ Dynamic stretching, in which the patient sits on a chair with the arch of the foot resting on a rolling pin or ball and rolls the object so that the ankle moves freely over it. This exercise should continue until some discomfort is felt, and repeated once more in the morning and twice in the evening.
Conclusion Plantar fasciitis is characterised by heel pain exacerbated by weight bearing after episodes at rest (McMillan et al 2012). The condition is self-limiting and usually resolves within 12 months after conservative treatment. It is important to conduct a thorough examination and take a comprehensive history to form an accurate diagnosis, and differential diagnoses should be considered (McPoil et al 2008). Analgesia should be used in conjunction with stretching exercises, which are the most common therapeutic intervention (Greve et al 2009).
ReferencesAlshami A, Souvlis T, Coppieters M (2008) A review of plantar heel pain of neural origin: differential diagnosis and management. Manual Therapy. 13, 2, 103-111.
American Academy of Orthopedic Surgeons (2015) OrthoInfo: Stress Fractures of the Foot and Ankle. tinyurl.com/pn2zooz (Last accessed: December 11 2014.)
Borman P, Ayhan F, Tuncay F et al (2012) Foot problems in a group of patients with rheumatoid arthritis: an unmet need for foot care. Open Rheumatology Journal. 6, 1, 290-295.
Braddam RL, Buschbacher RM (2007) Physical Medicine and Rehabilitation. Third edition. Elsevier, Philadelphia PA.
Crawford F, Atkins D, Young P et al (1999) Steroid injection for heel pain: evidence of short term effectiveness: a randomised control trial. Rheumatology. 38, 10, 974-977.
Cutts S, Obi N, Pasapula C et al (2012) Plantar fasciitis. Annals Royal College of Surgeons. 94, 8, 539-542.
Digiovanni B, Nawoczenski D, Malay P et al (2006) Plantar fascia: specific stretching exercise improves outcomes in patients with chronic plantar fasciitis. A prospective clinical trial with two-year follow up. Journal of Bone and Joint Surgeons. 88, 8, 1775-1748.
Foye PM (2013) Physical Medicine and Rehabilitation for Plantar Fasciitis. tinyurl.com/pkbqrdc (Last accessed: January 20 2014.)
Goff J, Crawford R (2011) Diagnosis and treatment of plantar fasciitis. American Family Physician. 84, 6, 676-682.
Greve J, Grecco M, Santos-Silva P (2009) Comparison of radial shockwaves and conventional physiotherapy for treating plantar fasciitis. Clinical Science. 64, 2, 97-103.
Irving DB, Cook JL, Young MA et al (2008) Impact of chronic plantar heel pain on health related quality of life. Podiatry Medical Journal. 98, 1, 283-299.
Kalichman L, Hernandez-Molina G (2014) Midfoot and forefoot osteomylitis. Foot. 24, 3, 128-134.
Kondreddi V, Gopal K, Yalamanchili R (2012) Outcome of endoscopic decompression of retrocalcaneal bursitis. Indian Journal of Orthopaedics. 46, 6, 659-663.
Landorf K, Keenan A, Herbert R (2006) Effectiveness of foot orthoses to treat plantar fasciitis: a randomised control trial. International Medical Journal. 166, 1, 1305-1310.
Lee TG, Ahmed TS (2007) Intralesional autologous blood injection compared to corticosteroids injection for treatment of chronic plantar fasciitis: a prospective randomised, controlled trial. Foot and Ankle International. 28, 9, 984-990.
Louwers M, Pangilinan P, Stabb B (2010) Utility of ultrasound in evaluation of a spontaneous plantar fascia rupture: a case report. American Academy of Physical Medicine and Rehabilitation. 2, 9, 98.
McMillan A, Landorf K, Gilheany M et al (2012) Ultrasound guided corticosteroid injection for plantar fasciitis: randomised control trial. British Medicine Journal. 344, 1, 3260-3268.
McPoil T, Martin R, Cornwall M et al (2008) Heel pain: plantar fasciitis: clinical practice guide. Journal of Orthopaedics and Sports Physical Therapy. 38, 4, 321-327.
National Institute for Health and Care Excellence (2014) Plantar Fasciitis. Scenario: Management. tinyurl.com/qfnc6so (Last accessed: January 13 2015.)
Neufeld S, Gerrato R (2008) Plantar fasciitis: evaluation and treatment. Journal of the American Academy of Orthopaedics. 16, 1, 338-346.
Ogden J, Alvarez R, Levit R et al (2001) Shockwave therapy in musculoskeletal disorders. Clinic of Orthopaedics. 387, 1, 22-40.
Rompe J, Furia J, Weil L et al (2007) Shockwave therapy for chronic plantar fasciopathy. British Medical Bulletin. 82, 1, 183-208.
Roxas M (2005) Plantar fasciitis: diagnosis and therapeutic considerations. Alternative Medical Review. 10, 1, 83-93.
Schwartz NE, John SU (2014) Plantar fasciitis: a concise review. Permanente Journal. 18, 1, 105-107.
Tatli Y, Kapasi S (2009) The real risks of steroid injection for plantar fasciitis with a review of conservative therapies. Musculoskeletal Medicine. 2, 1, 3-9.
Thing J, Maruthappu M, Rogers J (2012) Diagnosis and management of plantar fasciitis in primary care. British Journal of General Practice. 62, 601, 443-444.
Thomas JL, Christensen JC, Kravitz SR et al (2010) The diagnosis and treatment of heel pain: a clinical practise guideline revision 2010. Journal of Foot and Ankle Surgery. 49, 1, 1-19.
Toomey EP (2009) Plantar heel pain. Foot and Ankle Clinics. 14, 2, 229-245.
Tu P, Bytomski J (2011) Diagnosis of heel pain. American Family Physician. 84, 8, 909-916.
Conflict of interestNone declared
Online archiveFor related information, visit our online archive and search using the keywords


















