IRCCS San Raffaele Scientific Institute, Università Vita ...

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 7 , N O . 2 3 , 2 0 1 6
ª 2 0 1 6 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 3 . 5 7 3
Diagnosis and Treatment Algorithmfor Blood Flow Obstructions in PatientsWith Left Ventricular Assist Device
Anna Mara Scandroglio, MD,a Friedrich Kaufmann, DIPL ING,b Marina Pieri, MD,a Alexandra Kretzschmar, MD,bMarcus Müller, MD,b Panagiotis Pergantis, MD,c Stephan Dreysse, MD,c Volkmar Falk, MD, PHD,b,d,e
Thomas Krabatsch, MD, PHD,b,d Evgenij V. Potapov, MD, PHDb,d
ABSTRACT
Fro
of
Ca
Be
Th
gra
Sci
da
DC
Ma
BACKGROUND Thrombosis is an uncommon, but severe complication of left ventricular assist devices (LVADs).
OBJECTIVES This study analyzed experience with obstruction of blood flow through the LVAD with the purpose of
developing optimal diagnosis and treatment of LVAD-related thrombosis.
METHODS Between October 2009 and July 2015, a total of 652 LVAD were implanted in 557 patients.
Blood flow abnormalities in patients with LVAD (n ¼ 524) were identified and classified as “high-power” and
“low-flow” events.
RESULTS Three types of late blood flow obstructions were identified: 1) pre-pump via thrombus obstructing the inflow
cannula (26 events; 0.037 events per patient-year); 2) intra-pump (70 events; 0.1 events per patient-year); and 3) post-
pump via thrombosis of the outflow graft or stenosis of the anastomosis to the aorta (4 events; 0.006 events per
patient-year). Pre-pump obstruction was treated by washout maneuver in 9 cases (success rate, 100%), thrombolysis in
9 patients (success rate, 56%), and pump exchange in 9 cases (success rate, 100%); 1 patient died without treatment and
2 were weaned from LVAD. Intra-pump obstruction was treated by thrombolysis (n ¼ 9; success rate, 33%), pump ex-
change (n ¼ 53; success rate, 94%), and removal due to myocardial recovery (n ¼ 3; success rate, 100%); 7 patients died
without treatment and parameters spontaneously normalized in 2 cases. Post-pump obstruction was treated in 2 patients
by stenting (success rate, 100%), and was left untreated in 2 cases.
CONCLUSIONS We identified 3 types of LVAD-related blood flow obstruction, and developed an algorithm for
optimal diagnosis and treatment. (J Am Coll Cardiol 2016;67:2758–68) © 2016 by the American College of
Cardiology Foundation.
T he HeartWare HVAD (HeartWare Interna-tional, Framingham, Massachusetts) is animplantable centrifugal pump that is
designed as a left ventricular assist device (LVAD).Pump thrombosis is a major and severe complication,with a reported incidence of 0.04 to 0.09 events perpatient-year (EPPY) (1–4). Most reports focus on
m the aDepartment of Anesthesia and Intensive Care, IRCCS San Raf
Cardiothoracic and Vascular Surgery, German Heart Center Berlin, Ber
rdiology, German Heart Center Berlin, Berlin, Germany; dDZHK (Germa
rlin, Berlin, Germany; and the eDepartment of Cardiovascular Surgery, Ch
e study was supported by departmental funds of the German Heart Cente
nt from HeartWare and from Berlin Heart; and has received speaker’s fee
entific. All other authors have reported that they have no relationships rel
ta were presented at the annual meeting of the International Society of He
, on April 29, 2016.
nuscript received January 25, 2016; revised manuscript received March 2
pump thrombosis itself, in which the thrombus istrapped between the impeller and the housing. How-ever, blood flow may be disturbed at different levelsof the LVAD system via obstruction of the inflow can-nula caused by large wedge thrombus, by thrombosiswithin the device, and by kinking or stenosis ofthe outflow graft. Different types of blood flow
faele Scientific Institute, Milan, Italy; bDepartment
lin, Germany; cDepartment of Internal Medicine –
n Center for Cardiovascular Research), Partner Site
arité – Universitätsmedizin Berlin, Berlin, Germany.
r Berlin (Germany). Dr. Falk has received a research
s from Edwards Lifesciences, Aesculap, and Boston
evant to the contents of this paper to disclose. These
art and Lung Transplantations 2016, in Washington,
3, 2016, accepted March 24, 2016.

AB BR E V I A T I O N S
AND ACRONYM S
EPPY = events per patient-year
IQR = interquartile range
LVAD = left ventricular assist
device
J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6 Scandroglio et al.J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8 Pre-, Intra-, and Post-Pump Thrombosis
2759
obstruction demonstrate different clinical and tech-nical signs and require specific treatments. The aimof our study was to analyze our experience in therecognition and therapy of various patterns of bloodflow abnormalities in patients supported with theHeartWare HVAD and to develop an algorithm fortheir diagnosis and treatment.
SEE PAGE 2769
METHODS
We retrospectively analyzed data collected from allpatients implanted with a HeartWare HVAD as anLVAD at the Deutsches Herzzentrum Berlin betweenOctober 2009 and July 2015. Under German law,retrospective data analysis of an institution’s owndata does not require ethics committee approval.
Events involving blood flow abnormalities wereidentified using our institutional database and clin-ical and technical files and classified as high-powerand low-flow events, according to the alarms gener-ated from the pump.
“High power” was defined as a power increase thatgenerated a high-power alarm (alarm thresholdcommonly set at 1 W above mean power consumption)or a power trend increase of more than 0.5 W abovethe 30-day peak values. “Low flow” was defined as adecrease of >2 l/min below patient-specific averagevalue, with a distinction made between persistentimmediate decrease and continuous slow decrease.The alarms triggered by these derangements are“high-power alarm” and “low-flow alarm” and areeasily detected by the patients themselves. Low-flowevents caused by hypovolemia (bleeding or dehydra-tion), hypertension, and arrhythmia were excludedfrom the analysis. All alarm events were managed bythe VAD coordinator.
Anticoagulation was performed as described pre-viously (3), and there were no changes in the anti-coagulation protocol over time. Briefly, in thepostoperative period anticoagulation based on theactivated partial thromboplastin time is targeted to anactivated partial thromboplastin time of 45 to 50 s onday 1, of 50 to 60 on day 2, and of 60 to 70 on day 3. Inthe case of heparin-induced thrombocytopenia typeII, argatroban is administered intravenously with thesame activated partial thromboplastin time target.Aspirin is added 7 to 10 days after surgery if plateletcount and function have returned to nearly normalvalues as monitored by platelet aggregationtests. Clopidogrel can be used in the case of aspirinintolerance or according to specific indications.In all patients, oral anticoagulation is started on
approximately post-operative day 10 afteroral feeding has begun, chest tube and centralvenous catheters have been removed, and norelevant pericardial effusion is present. Thetarget international normalized ratio is set at2.5 to 3.0. In outpatients, the anticoagulationmonitoring and adjustment are based on daily
use of the CoaguChek (Roche Diagnostic, Mannheim,Germany) device and laboratory tests performedduring visits to the outpatient department.For the definition of hemolysis we used a thresholdof 20 mg/dl plasma-free hemoglobin, which is lowerthan reported previously (5) and is used by theInteragency Registry for Mechanically Assisted Cir-culatory Support (6). We measure hemoglobin, totalbilirubin, plasma-free hemoglobin, lactate dehydro-genase, and haptoglobin routinely during everyoutpatient visit and advise the general practitionerswho care for these patients to do so too.
Analysis of actual flow curves, log-files of technicaldata downloaded from the controller, and theacoustic spectra was performed in all patients beforedischarge home, during outpatient visits, and inevery case of blood flow abnormalities, as describedelsewhere (7). Lavare cycle is routinely enabled onfirst day after implantation in all patients; it does notaffect the log-file interpretation because of the pres-ence of a blanking algorithm in the log-file viewer.Acoustic signal analysis has been part of our routinepractice in the past 3 years (7).
The algorithm (Figure 1) was finalized andapproved as an institutional standard operating pro-cedure in October 2015.
DETECTION OF BLOOD FLOW OBSTRUCTIONS. TheHeartWare HVAD log-file analysis permits in-depthanalysis of power and flow trends in real time todistinguish between different kinds of blood flow ob-structions (Central Illustration). The major discrimi-nant is the power consumption. The nextdiscriminator is the pattern of power decrease (e.g.,immediate or slow). Acoustic analysis (7) and hemo-lysis parameters (5,8–14) increase precision of thediagnosis. In-pump blood flow obstructions can berelatively easily identified by the increase of powerconsumption and hemolysis and by acoustic analysis;differentiation between pre-pump and post-pumpflow obstruction (both indicated by low-flow alarmsand low power consumption) is related to the patternof flow decrease. In cases of pre-pump flow obstruc-tion caused by wedge thrombus occluding the inflowcannula, the onset of low flow is acute and withinhours (Figure 2). By contrast, low flow caused bythrombus in the outflow graft, kinking of the graft, or

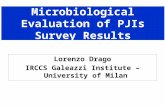
FIGURE 1 Algorithm for the Detection and Treatment of Flow Obstruction in the HeartWare HVAD
Power consumption alarm orenergy 1 Watt above last value
Symptoms of newly occurring heart failure orpersistent low flow values (> 2 l/min below average value)
HemolysisfHb > 20 mg/dl or
LDH > 600 IU/IRe-
evaluation
Acoustic analysis: 3rdharmonic present
Hypovolemia (dehydration/GI bleeding)
Arrhythmia
Hypertension
Log-file analysis
Thrombus inthe pump
Symptoms ofheart failure
High hemolysis values(dark urine)
> 3 days
Thrombolysis
Normalizationof the parameters
Normalization of theacoustic spectrum
Abrupt drop in flowPre-pump thrombus
(inflow)
Slow drop in flowPost-pump thrombus/
stenosis/kinkingSuboptimal
cannula position
3-D echo with “ramp test”, CT angio:- LV and outflow graft visualization with contrast medium- Outflow graft pressure gradient measurement
Thrombusin outflow graft
Stenosis of theanastomis / kinking
Washout withcarotid protection
Stent withcarotid protection Stent
Successful Successful
Pump exchange
Increase targetINR
Oralanticoagulationand discharge
Correctivesurgery
Legend: yes no result/next detection of flow obstruction treatment
Re-evaluation after correction
The figure explains our strategy in managing LVAD pump thrombosis. In the first part, in pink, the steps for the detection of blood flow
obstruction through the system are outlined. In the second part, in blue, the steps for treatment are presented. Arrows indicate positive or
negative answers to single fact or the result of an action. CT ¼ computed tomography; fHb ¼ plasma-free hemoglobin; GI ¼ gastrointestinal;
INR ¼ international normalized ratio; LDH ¼ lactate dehydrogenase; LVAD ¼ left ventricular assist device.
Scandroglio et al. J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6
Pre-, Intra-, and Post-Pump Thrombosis J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8
2760

CENTRAL ILLUSTRATION Pre-, Intra-, and Post-Pump Thrombosis: Blood Flow Obstructions in PatientsSupported With HeartWare HVAD
Scandroglio, A.M. et al. J Am Coll Cardiol. 2016;67(23):2758–68.
Pump flow could be disturbed at different levels of the left ventricular assist device system. Numbers indicate the site of thrombus apposition and identify
the types of pump thrombosis. Number 1, pre-pump thrombosis. Number 2, intra-pump thrombosis. Number 3, post-pump thrombosis at the level of
outflow graft and aortic anastomosis.
J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6 Scandroglio et al.J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8 Pre-, Intra-, and Post-Pump Thrombosis
2761

FIGURE 2 Pattern of Flow Decrease in Cases of Pre-Pump Flow Obstruction
Screen shot of left ventricular assist device log-file analysis, pertaining to pump power and flow trends. The onset of low flow, caused by wedge
thrombus occluding the inflow cannula, is acute within hours. Arrow indicates exactly the abrupt onset of low flow. Courtesy of HeartWare.
Scandroglio et al. J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6
Pre-, Intra-, and Post-Pump Thrombosis J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8
2762
anastomotic stenosis develops slowly over days orweeks (Figure 3). This pattern of decrease of powerconsumption is the main discriminator in ouralgorithm.
The theoretical possibility that inflow cannulamigration with gradually increased obstruction couldcause a slow decrease of power consumption andmimic post-pump blood flow obstruction wasconsidered, but never happened in our experience.Two mixed alterations were recognized: occlusivethrombus causing low flow progresses into the pumpbetween the rotor and housing in which the frictionincrease causes elevation of power consumption; andprimary pump thrombosis with outflow graft throm-botic involvement in which high-power consumptionwould decrease to nearly normal values. In both sit-uations “normalization” of power consumption couldbe misleading, despite minimal real blood flow. Inmixed alterations, the hemodynamic status, anunloaded and ejecting left ventricle, and hemolysisguide the diagnosis, and the log-file analysis wouldindicate the primary event.
STATISTICAL ANALYSES. Overall survival was esti-mated by Kaplan-Meier analysis. Data were censoredat end of follow-up. Duration of support is reportedas median (interquartile range [IQR]). Time zero fordeath after pump thrombosis was the date of pumpthrombosis. Cox proportional hazards analysis withdevice thrombosis as a time-dependent covariate wasused to calculate survival for patients without throm-bosis. For patients with multiple device placements
Kaplan-Meier curves start at the first device placementonly. Patients’ baseline characteristics were comparedby analysis of variance or Kruskal-Wallis test in thecase of continuous variables or chi-square test in thecase of categorical variables. Data were analyzedusing R software, version 3.03 (R Foundation forStatistical Computing, Vienna, Austria).
TREATMENT OF BLOOD FLOW OBSTRUCTION. Treat-ment depended on the diagnosis of the type ofblood flow obstruction based on clinical status,hemodynamic values, echocardiographic evaluationincluding “ramp test” (15), level of hemolysis, andend organ function.
The treatment was defined as successful when itled to restoration of normal blood flow from leftventricle to aorta as measured by normalization ofpower consumption and/or parameters of hemolysisand acoustic signals.
Thrombolysis as “soft lysis” was performed withtirofiban (Aggrastat, Merck & Co., West Point, Penn-sylvania) as an initial dose of 1.6 mg/kg/min in 30 minand continuous infusion of 0.4 mg/kg/min (bothreduced by approximately 50% in the case of severerenal impairment) for at least 48 h and maximum of72 h. Hemolysis parameters were monitored twicedaily, including lactate dehydrogenase, plasma-free hemoglobin, hemoglobin, haptoglobin, totalbilirubin, and hemoglobinuria, as well as the acous-tics of the pump. In addition to continuous infusion, astarting dose of 25 mg/kg as a bolus is providedif international normalized ratio at presentation is <3.

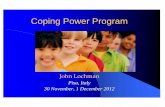
FIGURE 4 Kaplan-Meier Curve of the Overall Survival
0 6 12 18 24 30 36 42 48 54 60 66 72 78Time [Months]
0.0
0.2
0.4
0.6
0.8
1.0Su
rviv
al P
roba
bilit
y
524 321 247 189 154 121 97 64 55 44 27 8
Kaplan-Meier curve of survival of the whole population for 1, 2, and 3 years is shown.
Patients at risk and confidence bounds are indicated below the curve. Patients who were
weaned or transplanted are also included. Survival of patients with multiple device
placements starts at the time of first placement only.
FIGURE 3 Pattern of Flow Decrease in Cases of Post-Pump Flow Obstruction
Screen shot of left ventricular assist device log-file analysis, pertaining to pump power and flow trends. The onset of low flow, caused by
thrombus in the outflow graft, its kinking, or anastomotic stenosis, develops slowly within days or weeks. Arrows mark the trend of low flow.
Courtesy of HeartWare.
J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6 Scandroglio et al.J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8 Pre-, Intra-, and Post-Pump Thrombosis
2763
For occlusive thrombus of the inflow cannula, werecently developed a noninvasive technique to “washout” the thrombus (16), a procedure that is performedwith direct carotid artery protection to minimize therisk of cerebral thromboembolism. The washout ma-neuver involves stopping and restarting the pump,while in both carotid arteries filters are introduced tocapture thrombus released from the pump, and toprevent it traveling to the brain during the procedure.We used the filter-based cerebral protection systemSentinel Claret (Claret Medical, Santa Rosa, Califor-nia), with endovascular positioning through the rightradial or brachial artery (16) performed in a hybridoperating room.
Surgical treatment included surgical pump ex-change as previously reported (17,18). All explantedpumps were disassembled and visually inspected forthrombus formation. In the case of outflow graftthrombosis or stenosis of the anastomosis with theaorta, the graftwas stented. The graftwas visualized byangiography and the stenosis confirmed by measure-ment of a pressure gradient across the graft. Stentingis performed under angiographicmonitoring (19–22).
RESULTS
Since 2009, a total of 652 HeartWare HVAD pumpsHVADs have been implanted in 557 patients. Of these,524 patients had left ventricular, 5 right ventricular,and 28 biventricular support. The present analysis isbased on the 586 pumps implanted as LVADs in
524 patients. The median duration of support for apatient was 293 days (IQR: 41 to 742 days) and foreach pump 262 days (IQR: 32 to 597 days). Overallsurvival was 81.3% at 30 days, and 61.9%, 50.1%,and 44.3% at 1, 2, and 3 years, respectively (Figure 4).Forty-three patients received heart transplantationand 12 were weaned from the device followingmyocardial recovery.
Survival after event for patients who experiencedthrombosis of the device was 69.7% at 30 days, and

TABLE 1 Patient Data at Baseline
Pre-Pump(n ¼ 26)
Intra-pump(n ¼ 70)
Post-Pump(n ¼ 4) p Value
Age, yrs 58 � 13 52 � 13 48 � 12 0.01
Male 18 (69) 60 (86) 3 (75) 0.26
Body mass index, kg/m2 27 � 6 28 � 7 31 � 6 0.34
Body surface area, m2 1.9 � 0.4 2 � 0.6 2 � 0.1 0.34
Etiology of cardiomyopathy 0.12
Ischemic 12 (46) 47 (67) 0
Dilatative idiopathic 10 (38) 16 (23) 4 (100)
Post-infective 2 (8) 4 (5.8) 0
Corrected congenital heart disease 1 (4) 1 (1.4) 0
Sarcoidosis 1 (4) 0 0
Post-partum 0 1 (1.4) 0
Post-cardiotomic (nonischemic) 0 1 (1.4) 0
INTERMACS 0.58
1 1 (4) 13 (19) 1 (25)
2 8 (31) 25 (36) 1 (25)
3 13 (50) 27 (39) 2 (50)
4 3 (11) 5 (6) 0
Not available 1 (4) 0 0
Duration of support, days 313 (85–463) 345 (50–621) 644 (278–934) 0.44
International normalized ratio 2 � 0.9 2.5 � 1 3.2 � 1 0.02
Activated partial thromboplastin time, s 56 � 19 54 � 20 50 � 10 0.7
Patients with anticoagulation belowtarget range
6 (23) 16 (23) 1 (25) 0.09
Values are mean � SD, n (%), or median (interquartile range).
INTERMACS ¼ Interagency Registry for Mechanically Assisted Circulatory Support.
Scandroglio et al. J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6
Pre-, Intra-, and Post-Pump Thrombosis J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8
2764
49.4%, 37.2%, and 31% at 1, 2, and 3 years, respec-tively. Survival for patients without thrombosis was81.4% at 30 days and 62.3%, 53.7%, and 48,5% at 1, 2,and 3 years, respectively.
During the past 6 years, 100 events of bloodflow abnormalities were recorded (0.143 EPPY):70 high-power episodes (70%), and 30 low-flowevents (30%). Over this period, with growing knowl-edge of the problem, 3 types of blood flow obstructionwere identified (as shown in the Central Illustration).Most events were diagnosed as intra-pump throm-bosis, 26 events were diagnosed as pre-pump, and 4as post-pump thrombosis. In all investigated explan-ted pumps, thrombosis was confirmed by visual in-spection; the exchanged pump could not be analyzedin only a single case. By the nature of the treatment,thrombosis could not be proven visually after back-wash and lysis procedures. Indirectly, thrombosiswas confirmed after backwash maneuver in 3 caseswhere post-procedural arterial angiography provedthrombus in peripheral arteries (femoral and poplitealartery).
Patients’ characteristics and data at the time of thethrombotic event are shown (Table 1). Hemolysis pa-rameters at the time of presentation are shown for eachtype of blood flow obstruction (Table 2). Forty-eight
hours after treatments, parameters diagnostic forintravascular hemolysis were significantly decreased.
Of the 145 nonsintered pumps (without sinteredtitanium microspheres covering one-half of thelength of the inflow cannula) implanted from August2009 to June 2011, a total of 31 developed thromboticevents (0.14 EPPY) with no difference in thrombosisrate compared with sintered pumps. In particular pre-pump thrombosis could be identified in 5 of the pol-ished pumps (3.4%) compared with 21 events insintered pumps (4%). However, intra-pump throm-bosis was recognized in 26 (17.9%) of nonsintered and44 (9.9%) of sintered pumps. Different therapeuticapproaches were followed according to the supposedlevel of flow obstruction (Table 3).
PRE-PUMP THROMBOSIS. Low-flow events furtheridentified as pre-pump obstruction because of wedgedthrombus obstructing the inflow cannula occurred in26 (26%) cases (0.037 EPPY). Median support durationuntil first event was 313 days (IQR: 85 to 463 days).
Pre-pump obstruction was treated by a washoutmaneuver in 9 patients (all successful), thrombolysisin 9 patients (5 successful; success rate, 56%), andpump exchange in 9 patients (all successful). Onepatient died and 2 were weaned from LVAD. Somepatients received multiple treatment attempts. Onepatient was excluded from the analysis because oferroneous diagnosis and consequently inappropriatetreatment.
INTRA-PUMP THROMBOSIS. High blood flow epi-sodes identified as caused by a thrombus between theimpeller and pump housing occurred in 70 cases(0.10 EPPY). Median support duration until first eventof thrombosis was 345 days (IQR: 50 to 621 days).Acoustic analysis was positive in all cases (100%).Intra-pump obstruction was treated by thrombolysisin 9 patients (3 successful; success rate, 33%), pumpexchange in 53 cases (49 successful; success rate,94%), and removal for myocardial recovery (3 cases;success rate, 100%). Seven patients died (too sick forsurgery or refused surgery) and in 2 cases the pa-rameters spontaneously normalized.
POST-PUMP THROMBOSIS. Post-pump obstructionby thrombus inside the outflow graft or secondary tostenosis of the aortic anastomosis occurred in 4 pa-tients (4%; 0.006 EPPY). Median support durationuntil first event was 644 days (IQR: 278 to 934 days).Post-pump obstruction was treated by stenting(2 cases; success rate, 100%) or left untreated (2 cases).
Based on this experience we developed an algo-rithm (Figure 1) for the diagnosis and treatment ofblood flow abnormalities during support with theLVAD.

TABLE 2 Hemolysis Parameters at the Time of Clinical Presentation Before Treatment
and 48 H After Treatment Presented According to the Type of Flow Obstruction
Pre-Pump(n ¼ 26)
Intra-pump(n ¼ 70)
Post-Pump(n ¼ 4) p Value
Lactate dehydrogenase,before
516 (359–910) 1,495 (1,007–2,548) 426 (299–541) <0.001
Lactate dehydrogenase,after
394 (328 –488) 724 (541–912) 357 (278–437) <0.001
p value 0.023 0.001 0.039
Free hemoglobin, before 13 (7–23) 31 (83–249) 6 (4–8) <0.001
Free hemoglobin, after 5 (4–5) 4 (5–9) 5 (5–6) 0.379
p value <0.001 <0.001 <0.001
Haptoglobin, before 0 (0–18) 0 (0–0) 103 (63–135) 0.031
Haptoglobin, after 32 (0–75) 0 (0–36) 96 (119–142) 0.223
p value 0.50 1.0 1.0
Values are median (interquartile range). A p value was calculated to assess if the variables were statisticallydifferent among the 3 groups presented (pre-, intra-, and post-pump). Furthermore, a p value was calculated toassess if lactate dehydrogenase, free hemoglobin, and haptoglobin values were different before and aftertreatment within each group with statistical significance.
J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6 Scandroglio et al.J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8 Pre-, Intra-, and Post-Pump Thrombosis
2765
DISCUSSION
LVAD thrombosis is an important topic because of theincreasing number of patients supported worldwideand the increasing duration of mechanical circulatorysupport. The clinical presentation may vary fromslightly increased hemolysis or minimal changes inpump values and acoustic profile in an ambulatorypatient to acute hemodynamic collapse, massive he-molysis with multiorgan failure, or critical thrombo-embolic complications (7).
Among 100 events of flow abnormalities in 586HeartWare HVAD implanted as LVAD, most werecaused by an intra-pump thrombosis (70%), just overa quarter by pre-pump obstruction (26%) attributed towedge thrombus partially or totally occluding theinflow cannula, and only a few by outflow graftinvolvement (4%). The inferior survival rate of ourpatients compared with rates reported in the pastmay be explained by the elevated number of high-riskpatients treated at our institution. In the last 2 yearsthe number of patients who received LVAD implan-tation following acute extracorporeal life supportdoubled from 10% to 20%. Moreover, the institutionalpolicy was to preferably use HeartWare HVAD inhigh-risk cases (e.g., on ECLS [extracorporeal lifesupport], redo surgery, cachexia, biventricular assistdevice support, congenital heart disease) because ofits small size, and simple, fast implantation comparedwith HeartMate II.
Earlier reports (1–3), including 1 from our team,showed pump thrombosis of between 0.04 EPPY (1)and 0.09 EPPY (3). However, in our previous report,we considered only cases with visually confirmedpump thrombus (3). In the present study, patientswith successful thrombolysis and those not treatedwere also included in the calculation, leading to aslightly higher incidence of intra-pump thrombosis ofup to 0.10 EPPY.Wedge thrombus formation as a causefor pre-pump flow obstruction may be partially attrib-uted to the pump design, but we observed a more sig-nificant decrease in intra-pump thrombosis after theintroduction of the sintered inflow cannula. Sinteringprobably reduces the development of fibrin layersalong the inflow cannula (fibrin that could be mobi-lized, ingested, and then jammed in the hydrodynamicfield) consequently reducing rates of intra-pumpthrombosis. However, the process of sintering part ofthe device did not influence the therapy of pumpthrombosis over time. Also, in our opinion post-pumpflow obstruction is independent of pump design.
The main interest of the analysis is focused on thetreatment of pump thrombosis. Because multiplestrategies are available, we first localize where the
flow is disturbed and then decide on the appropriatetreatment on the basis of consequences of theabnormal flow in the patient.
PRE-PUMP THROMBOSIS. The leading symptom ofpre-pump thrombosis is hemodynamic instability (ifthe myocardial function has not recovered); thereforeemergency treatment is necessary. For fresh wedgethrombus occluding the inflow cannula, but not pro-truding into the pump between impeller and housingconfirmed by absence of third harmonics, pump stopunder protection of the carotid arteries (23,24) offersthe possibility of less invasive treatment. In ourexperience this was completely successful. The timeframe for successful washout is a matter of hours;later lysis is a viable option, but the success rate waslower (56%). The 4 patients in whom lysis failed thenunderwent washout maneuver (n ¼ 2) and pump ex-change (n ¼ 2).
In the past, pump exchange was performed for pre-pump flow obstruction. For the past 3 years, however,we have regarded the washout maneuver as firstchoice. For 1 year it has been routinely performed witha cerebral protection system. Therefore, our overalltreatment results are influenced by the introductionof the washout maneuver in our clinical practice.
INTRA-PUMP THROMBOSIS. Because early interven-tion is key for success, pump exchange is the defini-tive treatment for intra-pump thrombosis, andthrombolysis plays a secondary role in managing thiscomplication. Technically, an increase of power con-sumption and detection of the third harmonic are thefirst signs of LVAD thrombosis. Clinically, hemolysisas a consequence of the unbalanced impeller withsubsequent friction and destruction of all bloodcomponents is the leading symptom of intra-pump

TABLE 3 Treatment of Blood Flow Abnormalities and Success Rate According to the Obstruction Type
ObstructionSite
Lysis, n(SuccessRate*)
PumpExchange,
n (Success Rate)
WashoutManeuver,
n (Success Rate)
SpontaneousNormalization,n (Success Rate)
Stenting OutflowGraft, n
(Success Rate)Weaning,
n (Success Rate)No
Treatment,† n
Treatments SuccessRate, n (%)
No. of SuccessfulTreatments/
No. of Treatments
HospitalDischarge,
n (%)
Pre-pump(n ¼ 26)
5/9 (56) 9/9 (100) 9/9 (100) 0 NA 2/2 (100) 1 23/27‡ (85) 23/26 (89)
Intra-pump(n ¼ 70)
3/9 (33) 49/53 (94) NA 2/2 (100) NA 3/3 (100) 7 54/64‡ (84) 42/70 (60)
Post-pump(n ¼ 4)
0 0 NA 0 2/2 (100%) 0 2 2/2 (100) 2/4 (50)
Values are n (%). Gastrointestinal bleeding after lysis was recorded in 1 patient with known angiodysplasia. Recurrence of thrombosis after successful lysis was observed in 4 patients. *Success is defined asrestoration of normal blood flow. †With consequent death of the patient. ‡There were multiple treatment attempts.
NA ¼ not applicable.
Scandroglio et al. J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6
Pre-, Intra-, and Post-Pump Thrombosis J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8
2766
thrombosis (5,8–14). However, hemolysis may takehours or days before laboratory or clinical signsappear, and the best threshold for defining hemolysisin LVADs remains to be defined. In the case oflow hemolysis when the event started <3 days before,thrombolysis should be attempted. If hemolysis pro-gresses despite thrombolysis, pump exchange shouldbe performed immediately. Hemoglobinuria withdark urine, although not the defining symptom ofhemolysis, nevertheless may indicate it is occurringeven before the results of routine laboratory test areready, and can therefore trigger the decision forpump exchange. Early pump exchange may preventimminent renal failure. At our institution the sunshould not go down or rise up over dark urine.
In our experience thrombolysis is successful ifstarted immediately after the first signs of intra-pumpthrombosis (power increase or acoustic signals orhemolysis) appear. However, the success rate is stillinferior to that of pump exchange. Two of the 9 pa-tients treated presented with another episode ofhigh-power consumption and underwent surgicalpump exchange in the long-term follow-up (after 2and 6 months, respectively). From the literature,Stulak et al. (25) concluded that attempts to treatpump thrombosis medically have a low success rateand a high risk of hemorrhagic stroke and death.After differentiation into pre-pump, intra-pump,and post-pump blood flow obstructions, thrombol-ysis seems in our experience to be justified inintra-pump thrombosis only. We cannot exclude alower success rate of “soft lysis” based on anti-platelet drugs compared with lysis with r-TPA(recombinant tissue plasminogen activator) (26), butsoft lysis is safe and permits a staged approach notprecluding surgical pump exchange. However,recently published data demonstrate high rate ofintracranial bleeding complications (21%) in patientstreated with thrombolytic agents. Additionally, this
treatment is contraindicated in the case of earlypump thrombosis (surgery <6 months) or after arecent bleeding episode during support (25–27).
Two weaned patients had been previously evalu-ated as having myocardial recovery and intra-pumpthrombosis occurred coincidentally just days beforescheduled pump explantation. It is not our strategy toperform “acute weaning” for pump thrombosis.
POST-PUMP THROMBOSIS. We observed differentpatterns of the drop in power consumption and thecalculated flow when blood flow obstruction occurredat the level of the aortic anastomosis inside theoutflow graft. Computed tomography scan is a valu-able tool for visualization of thrombosis of theoutflow graft; however, neither case of anastomosisstenosis was recognized by computed tomography.Fluoroscopy, including ventriculography and injec-tion of contrast into the proximal part of the outflowgraft, is an excellent diagnostic tool and allowsconcomitant treatment (19–22).
In cases of low flow, we recommend that the pa-tient be investigated in a hybrid operation room. Thefirst step should be fluoroscopy and direct visualiza-tion of the LV with contrast medium. If pre-pumpobstruction is detected, a washout maneuver undercarotid protection should be attempted, with standbyfor surgical pump exchange. In successful cases, anangiogram should then be immediately performed todetect the location of the thrombus after the ma-neuver. If femoral occlusion is detected, embolec-tomy is performed. If there is no pre-pumpobstruction, visualization of the outflow tract bycatheterization of the tract with injection of contrastshould be performed. Kinking of the outflow tract canbe treated by stenting alone, and thrombosis of theoutflow tract by stenting with a covered stent whileusing cerebral endovascular protection (23,24). Asignificant stenosis of the aortic anastomosis may not

PERSPECTIVES
COMPETENCY IN PATIENT CARE AND PROCEDURAL
SKILLS: Thrombosis of mechanical LVAD may obstruct the
inflow cannula, pump chamber, or outflow graft and aortic
anastomosis. The approach to management and clinical out-
comes depend on the location of thrombus and device type.
TRANSLATIONAL OUTLOOK: Further studies are needed
to elucidate the hemostatic, hydraulic, and surface-dependent
interactions that distinguish pre-pump, intra-pump, and
post-pump thrombosis in patients receiving long-term
mechanical circulatory support.
J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6 Scandroglio et al.J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8 Pre-, Intra-, and Post-Pump Thrombosis
2767
be clearly visualized with contrast. In this case pres-sure should be measured along the outflow graft andin the aorta as the next step. A pressure drop betweenthe outflow graft and aorta indicates stenosis. Pres-sure measurement may be also useful for measuringsuccess after stenting.
Two of our patients were successfully treatedwith stenting; the others were too critical to undergotreatment, and died within a few days (1 was judgedunsuitable for surgery and stenting was not consid-ered; in 1 case the pressure drop was not documented).
Echocardiography may rule out other causes ofhemolysis, such as aortic insufficiency. Echo mea-surement of blood velocity through the outflow graftis feasible and the detection of abnormalities shouldprompt fluoroscopic assessment of the graft.
We were able to restore normal blood flow inalmost all of our patients, in some after 2 or moredifferent attempts. The exceptions were a few pa-tients for whom surgery was not suitable or whodeclined further treatment. Our overall success ratewas 84.9% (79 of 93 attempts). In some patients,despite restoration of blood flow and release of he-molysis, multiorgan failure caused by severe hemo-lysis or hemodynamic collapse was not reversible andthe patients died. Therefore early detection of bloodflow obstruction, localization of the thrombus/stenosis site, and rapid restoration of blood flow andresolution of hemolysis are crucial.
STUDY LIMITATIONS. There are several limitations tothis retrospective analysis. This is a single centerstudy with a small team implanting and managingthese devices, and a multicentered collaborativeapproach would lend greater weight to the results.Furthermore, the detection and management algo-rithm has evolved through the course of the study asthe center learned “best practice.” Therefore duringthe past 6 years our diagnosis and treatment havechanged with growing experience. In earlier days,some cases of pre-pump thrombosis were treated bypump exchange, whereas now we attempt thewashout maneuver first. Similarly, it is probable that
some post-pump thrombosis was not recognized andwas treated by pump exchange.
CONCLUSIONS
Blood flow abnormalities are not rare in patientssupported with the HeartWare HVAD. In most casesthis complication can be successfully treated usingan algorithmic approach. Our treatment strategy isbased on grade of hemolysis and hemodynamic sta-tus. Severe hemolysis as indicated by dark urine oranuria, or hemodynamic instability, triggers emer-gency surgery. In our opinion, the best treatment foreach condition was primary washout maneuver withcarotid protection for pre-pump obstruction, pumpexchange for intra-pump obstruction, and stenting ofthe outflow graft for post-pump obstruction.
ACKNOWLEDGMENTS The authors thank Julia Steinfor the statistical analysis, and Anne Gale for editorialassistance.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Anna Mara Scandroglio, Department of Anesthesiaand Intensive Care, IRCCS San Raffaele ScientificInstitute, Via Olgettina 60, 20132 Milan, Italy. E-mail:[email protected].
RE F E RENCE S
1. Najjar SS, Slaughter MS, Pagani FD, et al. Ananalysis of pump thrombus events in patients inthe HeartWare ADVANCE bridge to transplant andcontinued access protocol trial. J Heart LungTransplant 2014;33:23–34.
2. Aaronson KD, Slaighter MS, Miller LW,et al. Use of an intrapericardial, continuous-flow, centrifugal pump in patients awaitingheart transplantation. Circulation 2012;125:3191–200.
3. Soltani S, Kaufmann F, Vierecke J, et al.Design changes in continuous-flow left ventric-ular assist devices and life-threatening pumpmalfunctions. Eur J Cardiothorac Surg 2015;47:984–9.
4. Birati EY, Rame JE. Diagnosis and managementof LVAD thrombosis. Curr Treat Options Car-diovasc Med 2015;17:361.
5. Stepanenko A, Krabatsch T, Hennig E, et al.Retrospective hemolysis comparison between
patients with centrifugal biventricular assist andleft ventricular assist devices. ASAIO J 2011;57:382–7.
6. Interagency Registry for Mechanically AssistedCirculatory Support, National Heart Lung and BloodInstitute. Adverse event definitions. Available at:https://www.uab.edu/medicine/intermacs/appendices-4-0/appendix-a-4-0. Accessed April 12, 2016.
7. Kaufmann F, Hörmandinger C, Stepanenko A,et al. Acoustic spectral analysis for determining

Scandroglio et al. J A C C V O L . 6 7 , N O . 2 3 , 2 0 1 6
Pre-, Intra-, and Post-Pump Thrombosis J U N E 1 4 , 2 0 1 6 : 2 7 5 8 – 6 8
2768
pump thrombosis in rotary blood pumps. ASAIO J2014;60:502–7.
8. Bartoli CR, Ghotra AS, Pachika AR, et al. He-matologic markers better predict left ventricularassist device thrombosis than echocardiographicor pump parameters. Thorac Cardiovasc Surg2014;62:414–8.
9. Katz JN, Jensen BC, Chang PP, et al.A multicenter analysis of clinical hemolysis in pa-tients supported with durable, long-term leftventricular assist device therapy. J Heart LungTransplant 2015;34:701–9.
10. Baumann Kreuziger LM, Kim B,Wieselthaler GM. Antithrombotic therapy for leftventricular assist devices in adults: a systematicreview. J Thromb Haemost 2015;13:946–55.
11. Heilmann C, Geisen U, Benk C, et al. Haemol-ysis in patients with ventricular assist devices:major differences between systems. Eur J Car-diothorac Surg 2009;36:580–4.
12. Wieselthaler GM, O Driscoll G, Jansz P, et al.Initial clinical experience with a novel left ven-tricular assist device with a magnetically levitatedrotor in a multi-institutional trial. J Heart LungTransplant 2010;29:1218–25.
13. Jabbar AA, Yau R, Frazier OH, Delgado R 3rd.Direct thrombolytic therapy for thrombosis of acentrifugal flow left ventricular assist device.ASAIO J 2013;59:530–2.
14. Feldman D, Pamboukian S, Teuteberg JJ, et al.The 2013 International Society for Heart andLung Transplantation Guidelines for Mechanical
Circulatory Support: Executive Summary. J HeartLung Transplant 2013;32:157–87.
15. Uriel N, Morrison KA, Garan AR, et al. Devel-opment of a novel echocardiographiy ramp testfor speed optimization and diagnosis of devicethrombosis in continuous-flow left ventricularassist devices. The Columbia Ramp Study. J AmColl Cardiol 2012;60:1764–75.
16. Potapov E, Krabatsch T, Buz S, Falk V,Kempfert J. Cerebral protection system appliedduring washout of thrombus occluding inflowcannula of HeartWare HVAD left ventricular assistdevices. J Heart Lung Transplant 2015;34:1640–1.
17. Potapov EV, Krabatsch T, Hübler M, Hetzer R.Subcostal approach for replacement of failingcirculatory pumps. J Thorac Cardiovasc Surg 2012;144:1272.
18. Potapov E, Stepanenko A, Kaufmann F, et al.Thrombosis and cable damage in the HeartWarePump: clinical decisions and surgical technique.ASAIO J 2013;59:37–40.
19. Abraham J, Remick JD, Caulfield T, et al. Leftventricular assist device outflow cannula obstruc-tion treated with percutaneous endovascularstenting. Circ Heart Fail 2015;8:229–30.
20. Pham DT, Kapur NK, Dermody M, Halin N.Stenting of an outflow graft obstruction afterimplantation of a continuous-flow, axial-flow leftventricular assist device. J Thorac Cardiovasc Surg2015;150:e11–2.
21. Cheng RK, Aboulhosn J, Nsair A. Percutaneousangioplasty of stenotic outflow graft anastomosis
of HeartMate II. J Am Coll Cardiol Intv 2014;7:700–3.
22. Pieri M, Scandroglio AM, Kukucka M, et al.Heart failure after five years on left ventricularassist device: diagnosis and treatment of out-flowgraft obstruction. ASAIO J 2016. [e-pub ahead ofprint].
23. Naber CK, Ghanem A, Abizaid AA, et al. First-in-man use of a novel embolic protection devicefor patients undergoing transcatheter aortic valveimplantation. EuroIntervention 2012;8:43–50.
24. Lansky AJ, Schofer J, Tchetche D, et al.A prospective randomized evaluation of the Tri-Guard HDH embolic DEFLECTion device duringtranscatheter aortic valve implantation: results fromthe DEFLECT III trial. Eur Heart J 2015;36:2070–8.
25. Stulak JM, Dunlay SM, Sharma S, et al. Treat-ment of device thrombus on the HeartWare HVAD:success and outcomes depend significantly on theinitial treatment strategy. J Heart Lung Transplant2015;34:1535–41.
26. Jorde UP, Aaronson KD, Najjar SS, et al.Identification and management of pump thrombusin the HeartWare left ventricular assist devicesystem. J Am Coll Cardiol HF 2015;3:849–56.
27. Stewart GC, Givertz MM, Mehra MR. Pumpthrombosis redux. J Heart Lung Transplant 2015;34:1511–4.
KEY WORDS algorithm, complication, leftventricular assist device, mechanicalcirculatory support, thrombosis