Diagnosis and conservative treatment of skeletal
12
Diagnosis and conservative treatment of skeletal Class III malocclusion with anterior crossbite and asymmetric maxillary crowding Linda L. Y. Tseng, a Chris H. Chang, b and W. Eugene Roberts c Hsinchu, Taiwan, Indianapolis, Ind, and Loma Linda, Calif A man, aged 28 years 9 months, came for an orthodontic consultation for a skeletal Class III malocclusion (ANB angle, 3 ) with a modest asymmetric Class II and Class III molar relationship, complicated by an anterior crossbite, a deepbite, and 12 mm of asymmetric maxillary crowding. Despite the severity of the malocclusion (Discrepancy Index, 37), the patient desired noninvasive camouflage treatment. The 3-Ring diagnosis showed that treatment without extractions or orthognathic surgery was a viable approach. Arch length analysis indicated that differential interproximal enamel reduction could resolve the crowding and midline discrepancy, but a miniscrew in the infrazygomatic crest was needed to retract the right buccal segment. The patient accepted the complex, staged treatment plan with the understanding that it would require about 3.5 years. Fixed appliance treatment with passive self-ligating brackets, early light short elastics, bite turbos, interproximal enamel reduction, and infrazygomatic crest retraction opened the vertical dimension of the occlusion, improved the ANB angle by 2 , and achieved excellent alignment, as evidenced by a Cast Radiograph Evaluation score of 28 and a Pink and White dental esthetic score of 3. (Am J Orthod Dentofacial Orthop 2016;149:555-66) A n Angle classification for malocclusion focuses on the occlusal relationship of the first molars, so it can be misleading for many malocclusions. 1 Likewise, anterior crossbites may be deceptive, particu- larly when associated with a prognathic skeletal pattern and a concave face. This unusual case appears to be a modest problem based on the molar discrepancy, but it is a severe malocclusion based on the American Board of Orthodontics Discrepancy Index score of 37, as shown in Supplementary Worksheet 1. Furthermore, the face, anterior crossbite, and ANB angle of 3 are consistent with a skeletal Class III malocclusion. Despite the severity of the problem, the patient insisted on the most conservative treatment possible, so a careful differential diagnosis was critical to determine whether a relatively noninvasive approach was indicated or even possible. Anterior crossbites with a Class III skeletal pattern have a layer of complexity that is not readily diagnosed unless a systematic test is used such as Lin's 3-Ring diagnosis method. 2,3 A careful application of the Discrepancy Index and the 3-Ring method demonstrated that conservative treatment was feasible. However, optimal sagittal alignment of the dentition required a stainless steel miniscrew (OrthoBoneScrew; Newton's A, Hsinchu, Taiwan) in the right infrazygomatic crest to retract the right buccal segment. DIAGNOSIS AND ETIOLOGY A man, aged 28 years 9 months, came for an orthodontic consultation with the following chief concerns: thin upper lip, irregular dentition, and poor smile esthetics (Fig 1). There was no contributing medical or dental history. The clinical examination showed a retrusive upper lip, a deep anterior crossbite of all maxillary incisors, a posterior lingual crossbite of the maxillary right second premolar, and irregular dental attrition of the maxillary right central incisor. Overbite was 7 mm, and overjet was 3 mm. There were 12 mm of asymmetric crowding in the maxillary arch, and asymmetric Class II (right) and Class III (left) buccal segments associated with a midline deviation of the a Lecturer, Beethoven Orthodontic Center, Hsinchu, Taiwan. b Director, Beethoven Orthodontic Center, Hsinchu, Taiwan. c Professor emeritus, School of Dentistry, Indiana University; adjunct professor, School of Mechanical Engineering, Indiana University and Purdue University at Indianapolis, Indianapolis, Ind; visiting professor, Department of Orthodontics, School of Dentistry, Loma Linda University, Loma Linda, Calif. All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest, and none were reported. Address correspondence to: W. Eugene Roberts, Indiana University, School of Dentistry, 1121 W. Michigan St, Indianapolis, IN 46202; e-mail, werobert@iu. edu. Submitted, November 2014; revised and accepted, April 2015. 0889-5406/$36.00 Copyright Ó 2016 by the American Association of Orthodontists. http://dx.doi.org/10.1016/j.ajodo.2015.04.042 555 CASE REPORT
-
Upload
dentalid -
Category
Health & Medicine
-
view
186 -
download
1
Transcript of Diagnosis and conservative treatment of skeletal

CASE REPORT
Diagnosis and conservative treatment of skeletalClass III malocclusion with anterior crossbite andasymmetric maxillary crowding
Linda L. Y. Tseng,a Chris H. Chang,b and W. Eugene Robertsc
Hsinchu, Taiwan, Indianapolis, Ind, and Loma Linda, Calif
aLectubDireccProfeSchooIndianSchooAll auPotenAddreDentiedu.Subm0889-Copyrhttp:/
A man, aged 28 years 9 months, came for an orthodontic consultation for a skeletal Class III malocclusion(ANB angle,�3�) with a modest asymmetric Class II and Class III molar relationship, complicated by an anteriorcrossbite, a deepbite, and 12 mm of asymmetric maxillary crowding. Despite the severity of the malocclusion(Discrepancy Index, 37), the patient desired noninvasive camouflage treatment. The 3-Ring diagnosis showedthat treatment without extractions or orthognathic surgery was a viable approach. Arch length analysis indicatedthat differential interproximal enamel reduction could resolve the crowding and midline discrepancy, but aminiscrew in the infrazygomatic crest was needed to retract the right buccal segment. The patient acceptedthe complex, staged treatment plan with the understanding that it would require about 3.5 years. Fixed appliancetreatment with passive self-ligating brackets, early light short elastics, bite turbos, interproximal enamelreduction, and infrazygomatic crest retraction opened the vertical dimension of the occlusion, improved theANB angle by 2�, and achieved excellent alignment, as evidenced by a Cast Radiograph Evaluation score of28 and a Pink and White dental esthetic score of 3. (Am J Orthod Dentofacial Orthop 2016;149:555-66)
An Angle classification for malocclusion focuseson the occlusal relationship of the first molars,so it can be misleading for many malocclusions.1
Likewise, anterior crossbites may be deceptive, particu-larly when associated with a prognathic skeletal patternand a concave face. This unusual case appears to be amodest problem based on the molar discrepancy, but itis a severe malocclusion based on the American Boardof Orthodontics Discrepancy Index score of 37, as shownin Supplementary Worksheet 1. Furthermore, the face,anterior crossbite, and ANB angle of �3� are consistentwith a skeletal Class III malocclusion. Despite the severityof the problem, the patient insisted on the mostconservative treatment possible, so a careful differential
rer, Beethoven Orthodontic Center, Hsinchu, Taiwan.tor, Beethoven Orthodontic Center, Hsinchu, Taiwan.ssor emeritus, School of Dentistry, Indiana University; adjunct professor,l of Mechanical Engineering, Indiana University and Purdue University atapolis, Indianapolis, Ind; visiting professor, Department of Orthodontics,l of Dentistry, Loma Linda University, Loma Linda, Calif.thors have completed and submitted the ICMJE Form for Disclosure oftial Conflicts of Interest, and none were reported.ss correspondence to: W. Eugene Roberts, Indiana University, School ofstry, 1121 W. Michigan St, Indianapolis, IN 46202; e-mail, werobert@iu.
itted, November 2014; revised and accepted, April 2015.5406/$36.00ight � 2016 by the American Association of Orthodontists./dx.doi.org/10.1016/j.ajodo.2015.04.042
diagnosis was critical to determine whether a relativelynoninvasive approach was indicated or even possible.
Anterior crossbites with a Class III skeletal patternhave a layer of complexity that is not readily diagnosedunless a systematic test is used such as Lin's 3-Ringdiagnosis method.2,3 A careful application of theDiscrepancy Index and the 3-Ring method demonstratedthat conservative treatment was feasible. However,optimal sagittal alignment of the dentition required astainless steel miniscrew (OrthoBoneScrew; Newton'sA, Hsinchu, Taiwan) in the right infrazygomatic crestto retract the right buccal segment.
DIAGNOSIS AND ETIOLOGY
A man, aged 28 years 9 months, came for anorthodontic consultation with the following chiefconcerns: thin upper lip, irregular dentition, and poorsmile esthetics (Fig 1). There was no contributingmedical or dental history. The clinical examinationshowed a retrusive upper lip, a deep anterior crossbiteof all maxillary incisors, a posterior lingual crossbite ofthe maxillary right second premolar, and irregular dentalattrition of the maxillary right central incisor. Overbitewas 7 mm, and overjet was �3 mm. There were12 mm of asymmetric crowding in the maxillary arch,and asymmetric Class II (right) and Class III (left) buccalsegments associated with a midline deviation of the
555

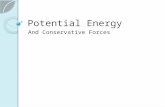
Fig 1. Pretreatment facial and intraoral photographs.
556 Tseng, Chang, and Roberts
maxilla that was 3 mm to the right (Fig 2). The radio-graphic and cephalometric surveys before treatmentare shown (Fig 3). The cephalometric measurementsare summarized in Table I. A severely worn facet onthe maxillary right central incisor required coordinatedorthodontic alignment and restorative care (Fig 4).
TREATMENT OBJECTIVES
In the maxilla (all 3 planes), the objective was tomaintain the anteroposterior, vertical, and transverserelationships.
In the mandible (all 3 planes), the objectives wereto maintain the anteroposterior and transverse relation-ships and to rotate the vertical segment clockwise toimprove the ANB angle.
April 2016 � Vol 149 � Issue 4 American
For the maxillary dentition, the objectives were to(1) protract the incisors and retract the molarsanteroposteriorly, (2) slightly increase the vertical, and(3) slightly increase the intermolar width.
For the mandibular dentition, the objectives were to(1) retract anteroposteriorly; (2) intrude the incisors verti-cally, and (3)maintain intermolar and intercaninewidths.
For the facial esthetics, the objectives were to(1) increase the upper lip protrusion and (2) increasethe vertical dimension of the occlusion to achieve anorthognathic profile.
TREATMENT ALTERNATIVES
After a careful evaluation of the patient's problems,we proposed 3 tentative treatment plans. Treatment
Journal of Orthodontics and Dentofacial Orthopedics

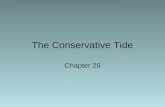
Fig 2. Pretreatment study models.
Fig 3. Pretreatment panoramic radiograph, lateral cephalometric radiograph, and cephalometrictracing, showing a protruded lower lip and crowding of the maxillary arch.
Tseng, Chang, and Roberts 557
American Journal of Orthodontics and Dentofacial Orthopedics April 2016 � Vol 149 � Issue 4

Table I. Cephalometric measurements
Pretreatment Posttreatment DifferenceSkeletalSNA (�) 81 81 0SNB (�) 84 82 2ANB (�) �3 �1 2SN-MP (�) 28 29 1FMA (�) 23 24 1
DentalU1 to NA (mm) 3 7 4U1 to SN (�) 102 114.5 12.5L1 to NB (mm) 3 3 0L1 TO MP (�) 88 91.5 3.5
FacialE-line to UL (mm) �5 �4 1E-line to LL (mm) �0.5 �2 1.5
U1, Maxillary incisor; L1, mandibular incisor; UL, upper lip; LL,lower lip.
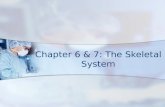
Fig 4. A severely worn facet along the incisal surface ofthe maxillary right central incisor had dentin exposure.
558 Tseng, Chang, and Roberts
plan A was extraction of the maxillary second premolarsand the mandibular first premolars. Treatment plan Bwas insertion of 2 miniscrews in the buccal shelf of themandible to retract the entire arch. Treatment plan Cwas nonextraction camouflage treatment using ClassIII elastics to retract the mandibular labial segmentand protract the maxillary labial segment. The patientchose the most conservative option: treatment plan C.However, this relatively noninvasive approach requiredextensive interproximal reduction of the anteriormaxillary arch and an orthodontic bone screw in theinfrazygomatic crest to retract the right buccal segment.The patient was informed that this conservativeapproach would require 3 to 4 years of treatment,primarily because of the sequence of proceduresnecessary to resolve 12 mm of asymmetric crowding inthe maxillary arch, without extracting any teeth. Heaccepted this treatment limitation.
The final plan included the following: (1) no extrac-tions or orthognathic surgery; (2) Damon Q brackets(Ormco, Glendora, Calif): standard torque passive
April 2016 � Vol 149 � Issue 4 American
self-ligating brackets bonded upside-down on themaxillary canines, lateral incisors, and centralincisors to resist the flaring effect of Class III elastics;(3) open-coil springs between the maxillary right firstmolar and first premolar, and between the maxillaryright canine and central incisor for opening space torelieve crowding; (4) bite turbos on the mandibularcanines initially and then on the mandibular centralincisors as the bite opened; (5) Class III early light shortelastics to assist with anterior crossbite correction and toopen the vertical dimension of the occlusion; (6) anOrthoBoneScrew in the right infrazygomatic crest toretract the right buccal segment; and (7) restoration ofthe maxillary right central incisor with a porcelain veneeror composite resin.
TREATMENT PROGRESS
The 0.022-in slot Damon Q standard torquebrackets were bonded on the mandibular arch. Bite tur-bos were bonded on the lingual surfaces of mandibularcanines to open the bite and facilitate anterior crossbitecorrection (Fig 5). One month later, the maxillary archwas bonded with standard torque brackets, but thoseon the 6 maxillary anterior teeth (canine to canine)were bonded upside-down to deliver negative torque(Table II). Initially, there was inadequate space tobond the maxillary right second premolar and thelateral incisor, so open-coil springs were placed onthe archwire, and those teeth were bonded withupside-down, standard torque brackets as soon asadequate space was available. The lengths of theactive nickel-titanium springs were extended approxi-mately 2 mm to activate space opening. The maxillaryright central incisor was severely worn, with dentinexposure. The amount of lost tooth structure wasestimated to be about 2 mm in the axial dimension,so the bracket position for the maxillary left centralincisor was 6 mm from the incisor edge, and the corre-sponding distance for the maxillary right central incisorwas only 4 mm (Fig 6). The goal was to achieve optimalgingival alignment and then restore the maxillary rightcentral incisor tooth structure as needed. The initialarchwires were 0.014-in copper-nickel-titanium. ClassIII early light short elastics (Quail, 3/16-in, 2 oz; Ormco)were placed from the mandibular first premolars to themaxillary first molars, and bite turbos were bonded onthe lingual surfaces of the mandibular central incisors(Fig 7). The stepwise opening of the bite with bite tur-bos was for patient comfort. The patient was instructedto wear the 2-oz early light short elastics full time andto replace them with new ones at least 4 times per day,preferably after meals or snacks. By the fifth month of
Journal of Orthodontics and Dentofacial Orthopedics

Fig 5. Bite turbos on the lingual sides of the mandibular canines were used to disarticulate the occlu-sion (open the bite). Bite turbos for themandibular incisors weremadewith a BTMold (Newton's A) for a5-mm bite ramp bonder (maxillary). The mold (bonder) is filled with composite resin, positioned againstthe lingual surface of the tooth, and then cured with light (mandibular).
Table II. DamonQ torque brackets are available inhigh, standard, and low torque for both arches
Torque
Maxillary arch (�) Mandibular arch (�)
U1 U2 U3 L1 L2 L3High 22 13 11 11 11 13Standard 15 6 7 �3 �3 7Low 2 �5 �9 �11 �11 0Standard upside-down �15 �6 �7
For the maxillary arch (U1, U2, and U3), the bracket can be placedupside-down to deliver superlow torque.U, Maxillary; L, mandibular.
Fig 6. A, Two open-coil springs were inserted on the rightside to create space for the maxillary second premolarand lateral incisor. B, Standard torque brackets werebonded upside-down from canine to canine in the upperarch in the maxillary anterior segment. Note that thebracket position for the maxillary right central incisor(arrow) is at the same level as the adjacent central incisorrelative to the gingival margin.
Tseng, Chang, and Roberts 559
treatment, the anterior crossbite was corrected (Fig 8),the bite turbos were removed, and the mandibulararchwire was changed to 0.014 3 0.025-in copper-nickel-titanium. In the seventh month, the maxillaryarchwire was changed to 0.014 3 0.025-in copper-nickel-titanium. Drop-in hooks (Ormco) were fittedinto the vertical slots of the maxillary canine bracketsto secure the Class II elastics (Fox, 1/4-in, 3.5 oz;Ormco), which accomplished anteroposterior correctionwhile promoting development of the smile arc. Thechange from Class III to Class II elastics at 7 months(Fig 7) was necessary because of the opening of thebite and the 2� improvement in the ANB angle.
In the eighth month, the open-coil springs werereactivated with a light-cured resin ball or a crimpablestop (Fig 9,A andB). In the tenthmonth, the mandibularanterior teeth were too lingually inclined, so the archwirewas changed to a 0.016 3 0.025-in nickel-titanium,pretorqued with 20� of lingual root torque. In the 15thmonth of active treatment, the maxillary archwire wasreplaced by a 0.017 3 0.025-in beta-titanium alloy(Ormco). By 18 months, there was still inadequate spaceto align the maxillary right second premolar (Fig 9, C),and additional coil spring activation was indicated. Inthe 21st month, OrthoBoneScrews were inserted at theright infrazygomatic crest, and an elastomeric chain
American Journal of Orthodontics and Dentofacial Orthoped
was attached to retract the maxillary right canine(Fig 10). Three months later (at 24 months of treatment),no significant space opening to align the maxillary rightsecond premolar had been achieved. In the 25th monthof the treatment, interproximal reduction was performedon the 4 maxillary incisors and along the mesial aspect ofthe maxillary right first molar (Fig 11). Then 5 teeth—maxillary right canine to maxillary lateral incisor—weretied togetherwith a power tube. In the 27thmonth, space
ics April 2016 � Vol 149 � Issue 4

Fig 7. A, Attachment of Class III early light short elastics (arrow) between the maxillary right first molarand the mandibular right first premolar (Quail, 3/16 in, 2 oz). B, Attachment of Class III early light shortelastics (arrow) between themaxillary left first molar and themandibular left first premolar. Note that themaxillary left central incisor bites on the bite turbo.C, Bite turbos (arrow) bonded at the lingual surfacesof the mandibular anterior teeth prevent bracket interference while correcting the crossbite.
Fig 8. In the fifth month of treatment, the anterior cross-bite was corrected, so the anterior bite turbos wereremoved. At the same appointment, the mandibular arch-wire was changed to a 0.014 3 0.025-in copper-nickel-titanium wire.
Fig 9. A, The open-coil spring was reactivated by addinga light-cured resin ball. B, The open-coil spring was reac-tivated by installing a crimpable stop mesial to the maxil-lary first molar. C, At 18 months of treatment, there wasstill inadequate space to align the maxillary right secondpremolar.
Fig 10. At 21 months, an OrthoBoneScrew (Newton's A)was placed in the right infrazygomatic crest, and a powerchain was attached from the maxillary right canine to theOrthoBoneScrew to retract the right buccal segment asthe space was opened for the maxillary right second pre-molar. At 24 months, no space was gained to align themaxillary right second premolar.
560 Tseng, Chang, and Roberts
opened on the mesial side of the right second premolar.In the 28th month, a button was bonded to the rightsecond premolar, and an elastomeric chain was usedfor buccal traction to align it; in the 32nd month,
April 2016 � Vol 149 � Issue 4 American
it was engaged on a 0.014-in nickel-titanium archwire(Fig 12). At 38 months of treatment, it was finallyaligned. Two weeks before the completion of activetreatment, the maxillary archwire was sectioned distallyto the canines, and box elastics (Fox 1/4 in, 3.5 oz)were used to improve the occlusal contacts. After42 months (3.5 years as projected) of active treatment,all appliances were removed, and 2 retainers weredelivered: a maxillary clear overlay and a maxillaryanterior 2-2 fixed.
TREATMENT RESULTS
In the maxilla (all 3 planes), the anteroposterior,vertical, and transverse relationships were maintained.
In the mandible (all 3 planes), the anteroposterior andtransverse relationships were maintained, and clockwiserotation increased the vertical dimensions of theocclusion and the ANB angle.
In the maxillary dentition, the following results wereobtained: (1) anteroposteriorly, the incisors were flared
Journal of Orthodontics and Dentofacial Orthopedics

Fig 12. A, After 30 months, a button was bonded on thebuccal surface of the maxillary right second premolar,and an elastic chain was attached. It was activated byattaching the opposite end to the infrazygomatic crestminiscrew. B, At 36 months, a bracket was bonded onthe buccal surface of the maxillary right second premolar,and it was engaged on a 0.014-in copper-nickel-titaniumarchwire. C, At 38 months, the maxillary right secondpremolar was aligned, and a 0.017 3 0.025-in betatitanium alloy archwire was engaged.
Fig 11. A, At 25 months, space was opened between the maxillary central incisors with an abrasivestrip.B, A tapered diamond bur was used to reduce themesial surfaces of themaxillary central incisors.C, The mesial surface of the maxillary right first molar was reduced in a similar manner.
Tseng, Chang, and Roberts 561
(102� to 114.5�); (2) the molars were retracted andextruded vertically; and (3) the intermolar and interca-nine widths were maintained.
In the mandibular dentition, the anteroposterior andthe intermolar and intercanine widths were maintained,and vertically, the incisors were intruded and the molarswere extruded.
For the facial esthetics, a facial profile with normalconvexity was obtained.
Retention
A fixed retainer was bonded on all maxillary incisors.A clear overlay retainer was delivered for the maxillaryarch, and the patient was instructed to wear it fulltime for the first 6 months and only at night thereafter.Instructions were provided for oral hygiene and mainte-nance of the retainers.
American Journal of Orthodontics and Dentofacial Orthoped
Final evaluation of treatment
The facial profile was improved primarily byincreasing the relative prominence of the upper lip andincreasing the vertical dimension of occlusion (Fig 13).Both arches were well aligned and optimally interdigi-tated in a near-ideal Class I occlusion, with coincidentdental midlines (Fig 14). Comparing the pretreatmentand posttreatment cephalometric tracings shows thatthe SN to mandibular plane angle increased by 1�
because of the clockwise rotation of the mandible(Fig 15). The axial inclination of the maxillary incisorsto SN increased from 102� to 114.5� (Table I). Themandibular incisors were intruded, but all molars wereextruded (Fig 16). The Cast Radiograph Evaluation scorewas 28 points, as shown in Supplementary Worksheet 2.Most of the points deducted were for lack of occlusalcontacts (8 points). Dental esthetics were excellent asdocumented by the Pink and White dental esthetic indexof 3, shown in Supplementary Worksheet 3. Althoughthe conservative plan required 3.5 years of activetreatment, the patient was pleased with the results.
DISCUSSION
Conservative treatment of a Class III skeletalmalocclusion is popular with patients but challengingfor orthodontists. There are 4 principal factorscontributing to successful conservative management:accurate diagnosis, advanced fixed appliances, customauxiliaries, and interproximal enamel reduction.2,3
After determining the complexity of a malocclusionwith the Discrepancy Index, a realistic diagnosis andtreatment plan are facilitated by 2 stepwise differentialtests: the 3-Ring diagnosis system (Fig 17) and theExtraction Decision Table (Table III).
A skeletal Class III malocclusion is often confusedwith pseudo-Class III problems, which typically have afunctional shift or an anterior crossbite with Class Ibuccal segments.4 Lin5 reported that the prevalence ofskeletal Class III malocclusion is about 1.65% in Taiwan,
ics April 2016 � Vol 149 � Issue 4

Fig 13. Posttreatment facial and intraoral photographs.
562 Tseng, Chang, and Roberts
but pseudo-Class III problems (Class I with anteriorcrossbite) are found in approximately 2.31% of children9 to 15 years of age. The 3-Ring diagnosis method(Fig 17) was developed to help predict the prognosisfor anterior crossbite correction.6 The clinical datashowed that 90% of anterior crossbite corrections werestable if the following diagnostic criteria were met:(1) an acceptable facial profile in centric relation;(2) the canines and molars in or near a Class Irelationship; and (3) an evident functional shift.
Good candidates for conservative (camouflage)treatment have an orthognathic profile (acceptable facialbalance) in centric relation, buccal segments that areapproximately Class I, and a functional shift.7 Therewere other favorable indicators: a marginally low to
April 2016 � Vol 149 � Issue 4 American
average mandibular plane angle and no open bite.Orthodontic camouflage to treat a Class III malocclusionmay result in increased axial inclination of the maxillaryincisors and decreased axial inclination of the mandibularincisors, particularly if there is an underlying Class IIIskeletal discrepancy.8 If it is necessary to retract themandibular incisors, an axial inclination of at least 88� isdesirable.9
The Extraction Decision Table of Chang10 (Table III)was used to assess the necessity for extractions. The 2factors favoring extraction were the protrusive profileand crowding greater than 7 mm in the maxillary arch.However, maxillary extractions would have complicatedthe correction of the anterior crossbite and might resultin a midface deficiency. Furthermore, the patient was
Journal of Orthodontics and Dentofacial Orthopedics

Fig 14. Posttreatment study models (casts).
Fig 15. Posttreatment panoramic radiograph, lateral cephalometric radiograph, and cephalometrictracing, showing the improved profile and the parallel alignment of all tooth roots.
Tseng, Chang, and Roberts 563
American Journal of Orthodontics and Dentofacial Orthopedics April 2016 � Vol 149 � Issue 4

Fig 16. Initial (black) and final (red) cephalometric tracings are superimposed on the anterior cranialbase (left), and on the stable skeletal structures of the maxilla (upper right), and the mandible (lowerright).
564 Tseng, Chang, and Roberts
strongly opposed to extractions, so the nonextractionoption was selected, with the understanding thatextensive interproximal reduction and infrazygomaticcrest anchorage were necessary.
Passive self-ligating brackets with light wiresfacilitate the conservative correction of Class IIImalocclusions.7 The bracket is a tube-like appliancecapable of delivering a continuous light force, similarto the multiloop edgewise archwire effect.7,11,12 If apatient meets the 3 criteria of the 3-Ring diagnosis,straight wires and Class III elastics are usually sufficientto correct the malocclusion.2 For our patient, Class IIIearly light short elastics were used initially with biteturbos but were then replaced by Class II elastics assoon as the bite opened and the anterior crossbite wascorrected. These are common mechanics for patientswith an anterior crossbite and Class I buccal segments.If it is necessary to manage an asymmetry or retractthe entire mandibular arch, bilateral buccal shelfOrthoBoneScrews are indicated.7,12,13
Proper torque control with passive self-ligatingbrackets and light nickel-titanium wires can be chal-lenging.14 For this patient, the dental axial inclinationswere managed with low-torque brackets (Table II), pre-torqued archwires, and temporary skeletal anchoragedevices to retract the right buccal segment. Controlling
April 2016 � Vol 149 � Issue 4 American
torque with the selection of brackets is particularlyeffective with passive self-ligating brackets15,16
(Table II). Low torque was used on the maxillary incisorsto compensate for the side effects of the Class III elastics:flaring of the maxillary incisors and excessive retractionof the mandibular incisors.17 If low-torque brackets areinsufficient for controlling axial inclinations, bondingstandard-torque brackets upside-down is a viablealternative.15-17 If a rectangular archwire fails togenerate adequate root torque, a 20� pretorquedarchwire such as 0.016 3 0.025 in or 0.019 3 0.025in is recommended. Since this patient had standard-torque brackets bonded on the mandibular teeth, a0.016 3 0.025-in nickel-titanium archwire with 20� oftorque was inserted 10 months into treatment to correctthe axial inclinations in the anterior segment.17
This problem could have been prevented by usinghigher-torque brackets in the mandibular anteriorsegment initially (Table II).
Correction of a deepbite can be achieved by molarextrusion, incisor intrusion, or both. This patient'sdeepbite was corrected with anterior bite turbos, whichintruded the mandibular incisors and allowed theposterior segments to extrude (Fig 16). The advantagesof anterior bite turbos at the beginning of treatmentwere to serve as vertical stops for the deep overbite, to
Journal of Orthodontics and Dentofacial Orthopedics

Fig 17. The Class III diagnosis system developed by Lin6
has simplified the complicated diagnostic procedure forassessing anterior crossbite.
Table III. The Extraction Decision Table of Chang,10
summarizing the aids for determining an extractionor nonextraction treatment plan
Extraction Nonextraction1. Profile Protrusive Straight2. Mandibular angle High Low3. Bite Open Deep4. Anterior inclination Flaring Flat5. Crowding .7 mm None6. Decayed or missing teeth Present ?7. Patient perception OK No
Tseng, Chang, and Roberts 565
unlock the posterior interdigitation, and to allow themalocclusion greater freedom for 3-dimensional toothmovement.15-17 Bite turbos for Class III treatment haveadditional advantages: (1) protect the enamel fromattrition, (2) prevent accidental bracket debonding,(3) improve the effect of light wires for 3-dimensionaltooth movement such as correction of posteriorcrossbites, (4) improve the response to early light shortelastics, and (5) help correct mandibular plane angleproblems.15 For deep anterior crossbites, a stepwiseopening of the bite with bite turbos is more comfortablefor the patient (Figs 5 and 7).
American Journal of Orthodontics and Dentofacial Orthoped
For our patient, the anterior crossbite and deepbitewere corrected simultaneously in about 5 months usingClass III elastics as the principal active mechanics.15-17
Starting with 2-oz early light short elastics during theleveling phase enhanced treatment efficiency by helpingto level the arches and achieve correction in the sagittalplane.14,15 The side effects of Class III elastics are labialtipping of the maxillary incisors, extrusion of themaxillary molars, and distal tipping of the mandibularmolars.15-17 Since these effects were consideredfavorable for our patient, Class III elastics were usedrather than inserting bone screws into the buccal shelfof the mandible.12
At 21 months, an OrthoBoneScrew was placed at theright infrazygomatic crest to provide anchorage to retractthe canine, prevent incisor flaring, and retract themolars.However, these mechanics failed to open adequate spacefor alignment of the maxillary right second premolar(Fig 10). So, interproximal reduction was performedwith an air rotor and abrasive finishing strips in theanterior segment of the maxillary arch to reduce theblack triangles, gain space for alignment of themaxillary right second premolar, improve toothproportions, and establish more ideal interproximalcontacts (Fig 11).18,19
The Pink and White esthetic score evaluates anteriormaxillary esthetics by analyzing clinical photographs.Refer to the scoring form in Supplementary Worksheet3. The form includes 2 esthetic assessments: Pink is agingival evaluation, and White is a score of dentalmicroesthetics. The column on the right lists 6 variablesthat are scored from 0 to 2 for each assessment. Theactual Pink and White score is marked with red circlesfor the 6 variables in the areas highlighted in blue.20
The deficiencies scored were blunted mesial and distalgingiva papillae, creating small dark triangles betweenthe incisors; inadequate incisal curve (smile line); andan apparent deviation from the ideal incisal rootangulation. Three points or fewer on the Pink and Whitescore is considered an excellent result, particularly forpatients with incisal abrasion.
The anterior cranial base superimposition (Fig 16)shows that the mandible was rotated posteriorlyapproximately 4 mm, but the Frankfort-mandibularplane angle opened by only 1� because the posteriormandible moved inferiorly. This unusual pattern ofmandibular rotation may indicate a morphologicproblem in the temporomandibular joints. In retrospect,it might have been wise to use a cone-beam computedtomography image prospectively to evaluate the joints.Furthermore, a cone-beam image might be a wiseprecaution for assessing all skeletal malocclusions thatrequire surgery or temporary anchorage devices.
ics April 2016 � Vol 149 � Issue 4

566 Tseng, Chang, and Roberts
CONCLUSIONS
This difficult skeletal malocclusion (ANB angle, �3�;Discrepancy Index, 37) was treated to an excellent result(Cast Radiograph Evaluation, 28) without extractions ororthognathic surgery. A differential diagnosis using 3methods (Discrepancy Index, 3-Ring, and ExtractionDecision Table) showed that the patient's desire forconservative treatment was feasible. A carefullysequenced treatment plan achieved an excellent resultfor this severe malocclusion, but it did require 3.5 yearsof treatment. In retrospect, the treatment time mighthave been decreased by introducing interproximalreduction and infrazygomatic crest anchorage earlierin the sequence, but the necessity for those more-invasive measures was not clear until about 18 monthsinto treatment. Despite 12 mm of asymmetric crowdingin the maxillary arch, the problem was treated to anoptimal result without excessive arch expansion andincisal flaring.21
ACKNOWLEDGMENTS
We thank Paul Head for proofreading this article.
SUPPLEMENTARY DATA
Supplementary data related to this article can be foundat http://dx.doi.org/10.1016/j.ajodo.2015.04.042.
REFERENCES
1. Angle EH. Classification of malocclusion. Dent Cosmos 1899;41:248-64.
2. Lin JJ. The most effective and simplest ways for treating severeClass III without extraction or surgery. Int J Orthod Implantol2014;33:4-18.
3. Yeh HY, Lin JJ, Roberts WE. Conservative adult treatment forsevere Class III openbite malocclusion with bimaxillary crowding.Int J Orthod Implantol 2014;34:12-25.
4. Kelly J, Harvey C. An assessment of the teeth of youths 12-17years:Publication No. (HRA) 74-1644. Washington, DC: NationalCenter for Health Statistics, US Public Health Service; 1977.
April 2016 � Vol 149 � Issue 4 American
5. Lin JJ. Prevalence of malocclusion in Taiwan children age 9-15.Clin Dent 1984;4:227-34.
6. Lin JJ. Creative orthodontics blending the Damon System & TADsto manage difficult malocclusion. 2nd ed. Taipei, Taiwan: YongChieh; 2010. p. 263-71.
7. Lin JJ, Liaw JL, Chang HN, Roberts WE. Class III correction ortho-dontics. Taipei, Taiwan: Yong Chieh; 2013. Published electroni-cally on Apple iBooks as Orthodontics vol. 3: Class III correction.
8. Costa Pinho TM, Ustrell Torrent JM, Correia Pinto JG. Orthodon-tics camouflage in the case of a skeletal Class III malocclusion.World J Orthod 2004;5:213-23.
9. McLaughlin RP, Bennett JC, Trevisi H. Systemized orthodon-tics treatment mechanics. London, United Kingdom: Mosby;2001.
10. Chang CH. Advanced Damon course no.1: extractiondecision-making (table). Beethoven Podcast Encyclopedia inOrthodontics. Hsinshu, Taiwan: Newton's A; 2011.
11. Pollard AP. Capturing the essence of the Damon approach. ClinImpression 2003;12:4-11.
12. Lin JJ. Treatment of severe Class III with buccal shelf mini-screws.News Trends Orthod 2010;18:3-12.
13. Huang S. Non-extraction management of skeletal class IIImalocclusion with facial asymmetry. News Trends Orthod 2010;20:22-31.
14. Kozlowski J. Honing Damon system mechanics for the ultimate inefficiency and excellence. Clin Impressions 2008;16:23-8.
15. Pitts T. Begin with the end in mind: bracket placement and earlyelastics protocols for smile arc protection. Clin Impressions2009;17:4-13.
16. Huang S, Pitts T. Secrets of excellent finishing. News TrendsOrthod 2009;14:6-23.
17. Chang CH. Basic Damon course no. 5: finish bending. BeethovenPodcast Encyclopedia in Orthodontics. Hsinshu, Taiwan: Newton'sA; 2012.
18. Zachrisson BU, Nyoygaard L, Mobarak K. Dental health assessedmore than 10 years after interproximal enamel reduction ofmandibular anterior teeth. Am J Orthod Dentofacial Orthop2007;131:162-9.
19. Hsu YL. Approaching efficient finishing with hard and soft tissuecontouring, part II: hard tissue contouring. News Trends Orthod2008;11:17-9.
20. Su B. IBOI Pink and White esthetic score. Int J Orthod Implantol2012;28:80-5.
21. Liaw JL. Molar retraction in all four quadrants to correct a Class III,crowded malocclusion in a patient with a flat profile. Int J OrthodImplantol 2012;27:20-31.
Journal of Orthodontics and Dentofacial Orthopedics