
Diabetic retinopathy
45
CASE DATA Demography: 51 year-old male Chief Complaint: Deterioration of distance and near vision over a period of three months Illness: Spots or dark strings floating in vision (floaters),Blurred vision, impaired color vision Ocular History: Last eye test: A year ago Medical History: Poorly controlled insulin dependent Diabetes Mellitus for the last 10 years Fundus Examination: Blot and dot hemorrhages Few hard exudates in the macular area, Retinal edema Fluorescein
-
Upload
esther-issac -
Category
Health & Medicine
-
view
48 -
download
0
Transcript of Diabetic retinopathy
CASE DATA
Demography: 51 year-old male
Chief Complaint: Deterioration of distance and near vision over a period of three months
Illness: Spots or dark strings floating in vision (floaters),Blurred vision, impaired color vision
Ocular History: Last eye test: A year ago
Medical History: Poorly controlled insulin dependent Diabetes Mellitus for the last 10 years
Fundus Examination: Blot and dot hemorrhages Few hard exudates in the macular area, Retinal edema
Fluorescein Angiography: Extensive leakage supero-temporal to the optic disc

DIABETIC RETINOPATHY

Diabetic Retinopathy refers to the retinal changes seen in patients with Diabetes mellitus
6 MILLIONDiabetics
•STDR•As on April 2015
10 MILLIONDiabetics
•Projected STDR•By 2035

PATHOGENESIS
• Micro vascular occlusion• Micro vascular leakage

LOCATION DISORDERCapillary Occlusion Dilatation Micro aneurysms Abnormal PermeabilityArteriole Narrowing of origin of Terminal arteriesVein Dilatation Beading Reduplication Looping, Kinking Branch vein occlusion Central veins occlusion
RETINAL VASCULAR PATHOLOGY IN DIABETIC RETINOPATHY

MICROVASCULAR LEAKAGE
Degeneration and loss of pericytes
Plasma leakage
Intraretinal hemorrhageHard exudate(Circinate pattern)
Capillary wall weakening
micro aneurysm
Retinal edema
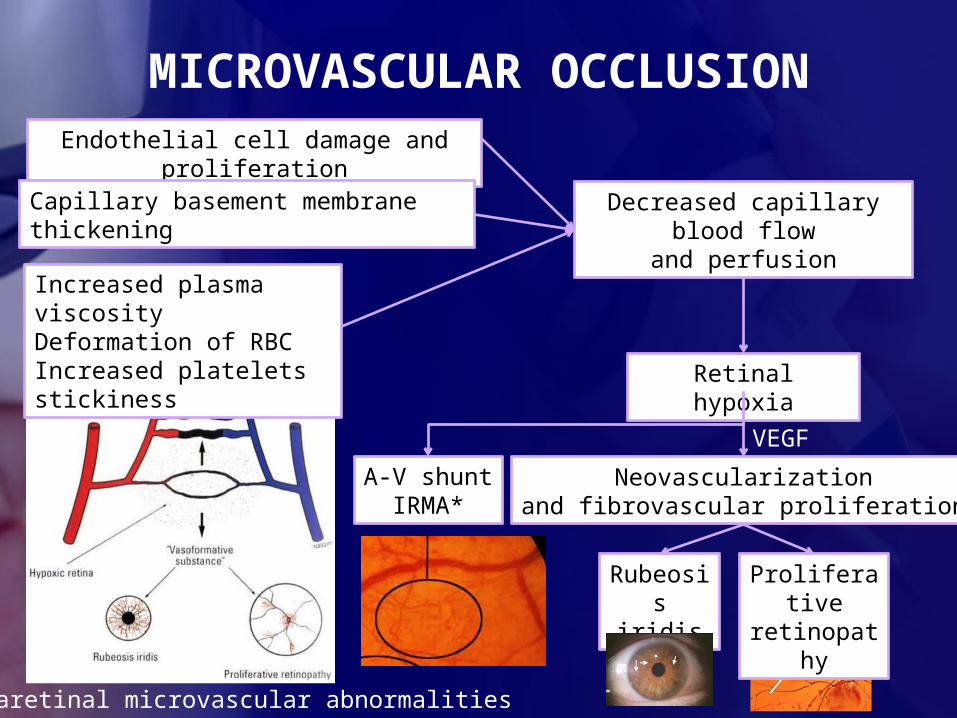
MICROVASCULAR OCCLUSION
Neovascularizationand fibrovascular proliferation
VEGF
Increased plasma viscosityDeformation of RBCIncreased platelets stickiness
Decreased capillary blood flow
and perfusion
Endothelial cell damage and proliferation
Capillary basement membrane thickening
Retinal hypoxia
A-V shuntIRMA*
*intraretinal microvascular abnormalities
Proliferative retinopathy
Rubeosis iridis
ETIOLOGY
Duration of Diabetes
• Sex
Poor metabolic control
• Pregnancy
Hypertension
• Hyperlipidemia
Others-obesity, OCP’s, Anaemia, Smoking

TYPESDiabetic retinopathy
Non-Proliferative
Proliferative
Maculopathy
Advanced diabetic eye disease

NPDR
MildModerat
esevere
Very severe
ETDRS CLASSIFICATION(Modified Airlie House Classification)

FEATURES OF NPDR


Splinter
haemorrhage
Dot & Blot haemorrhage
s

Cotton wool spots
Hard exudates

Hard exudates
Cotton wool spots
↑↑
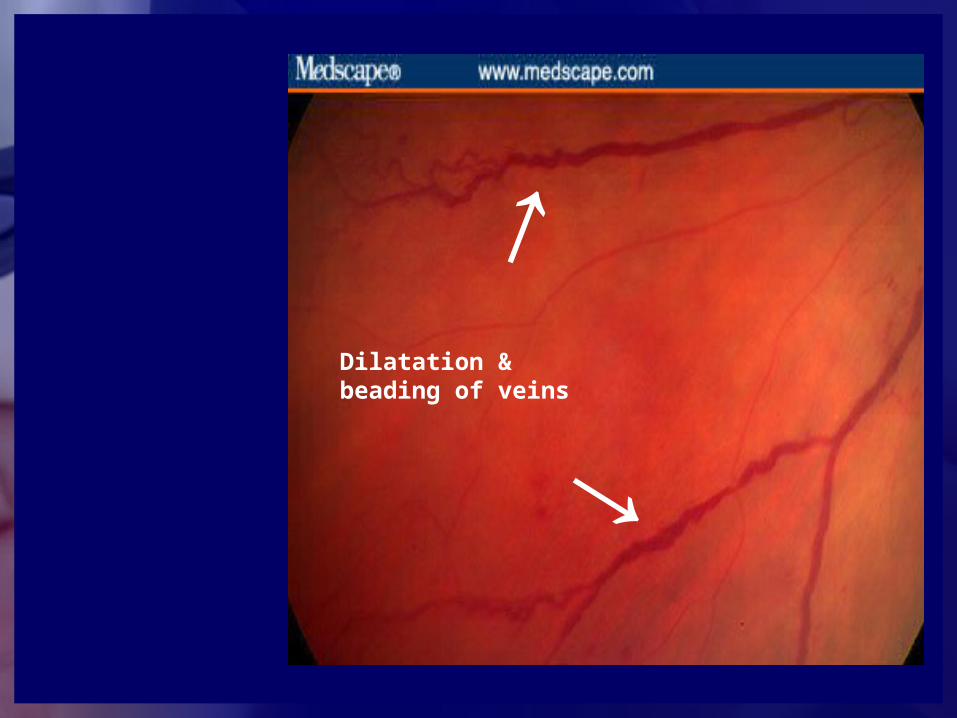
Dilatation & beading of veins

Intraretinal microvascular abnormalities

Microaneurys
ms


Neova
scul
arizat
ion
of d
isc
↑

New vessels of the disc (advanced)

New vessels elsewhere

• Macular ischemia• Retinal capillary non-perfusion• Progressive NPDR
• Macular edema• Increased retinal vascular
permeability• Seen in both NPDR and PDR• Focal or diffuse or mixed• Cause of visual loss in DR
DIABETIC MACULOPATHY
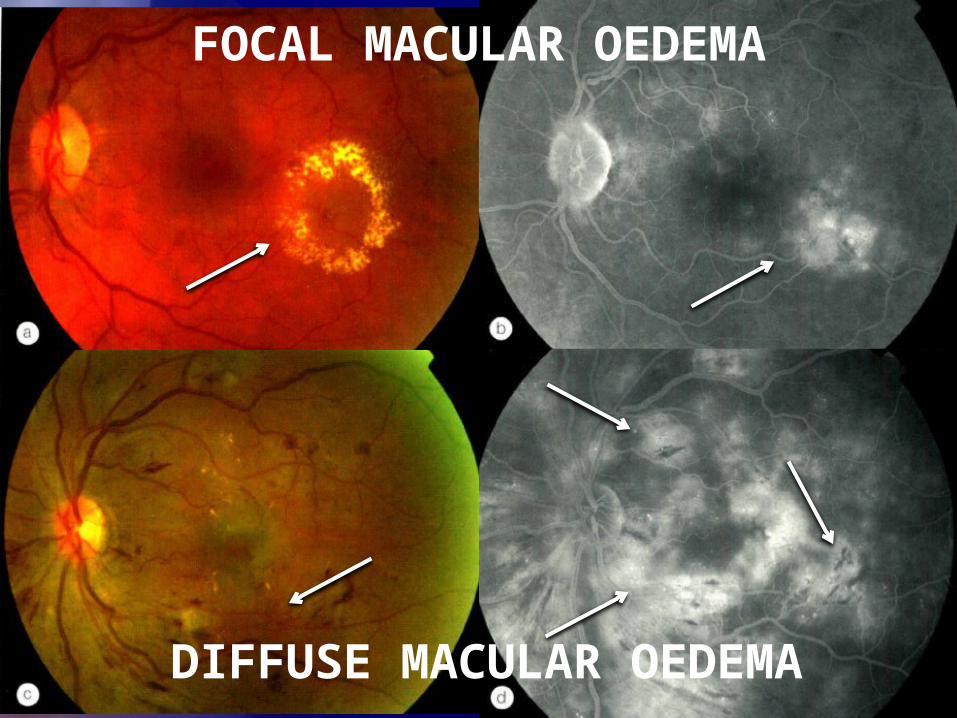
FOCAL MACULAR OEDEMA
DIFFUSE MACULAR OEDEMA

MACULAR ISCHEMIA

CLINICALLY SIGNIFICANT MACULAR OEDEMA (CSME)
Retinal oedema within 500 microns
of centre fovea
Hard exudates within 500 microns of fovea
if as with adjacent retinal thickening
Retinal oedema > 1 disc diameter, any part
is within 1 disc diameter of centre of
fovea

OCT CLASSIFICATION OF DIABETIC MACULAR OEDEMA
• Sponge like thickening of retinal layers due to accumulation of fluid.
• Large cystoid space involving variable depth of retina with intervening septa.
• Serous detachment of retina.• Tractional detachment of fovea.• Taut posterior hyaloid membrane.

VISION IN DR


ADVANCED DIABETIC EYE DISEASE
End result of uncontrolled proliferative Diabetic retinopathy.COMPLICATIONS:
Vitreous haemorrhage
Tractional retinal detachment

Neovascular glaucoma
Rubeosis iridis

INVESTIGATIONS
Blood sugar
OCT
Haemogram
24hr urine
retentionRFT
urine
Lipid profile
HbA1C
FFA

MANAGEMENT
SCREENING
MEDICAL THERAPY
PHOTOCOAGULATION


Prevention Treat underlying conditions
Control blood sugar – HbA1c < 7Control blood pressure – SBP < 130 mmHgControl lipid profile – TG, LDLCorrect anemiaControl diabetic nephropathy
Pregnancy makes DR worsen
MEDICAL THERAPY

Focal or Grid • CSME in both NPDR
and PDRPanretinal
• PDR
PHOTOCOAGULATION
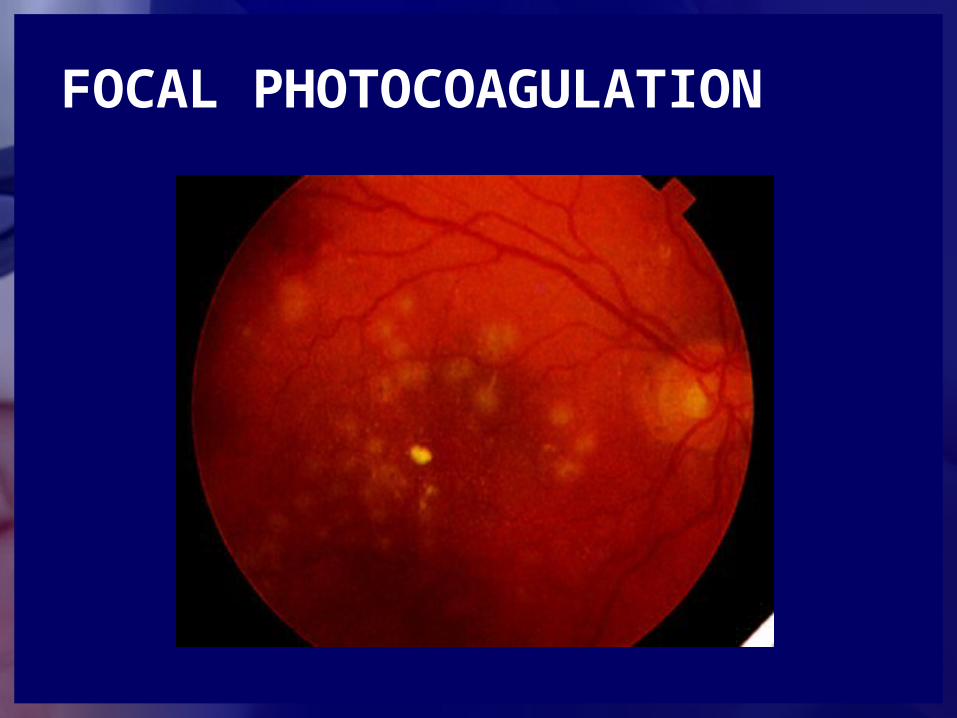
FOCAL PHOTOCOAGULATION

GRID PHOTOCOAGULATION

PANRETINAL PHOTOCOAGULATION (PRP)

• Indications for pars plana vitrectomy (PPV) in DR• Severe persistent vitreous hemorrhage• Progressive tractional RD (threatening or
involving macula)• Combined tractional and rhegmatogenous
RD• Premacular subhyaloid hemorrhage• Recurrent vitreous hemorrhage after laser
PRP
SURGICAL MANAGEMENT

• Pars plana vitrectomy (PPV)• Membrane peeling (MP)• Endolaser (EL)• Fluid gas exchange (FGX)
• SF6
• C3F8
VITREORETINAL SURGERIES

CHANCES OF GOING BLIND
AGE(yrs)
FUNDUS LESION
% OF BLIND PATIENTS
<29 Retinal microaneurysms
Intraretinal hemorrhages+ Hard
exudates
0
4
30-59 Retinal microaneurysms
Intraretinal hemorrhages+ Hard
exudates
12
24
(within 5yrs of onset of disease)

Hypertensive retinopathyRadiation retinopathyCentral retinal vein
occlusion (CRVO)Branch retinal vein
occlusion (BRVO)Ocular ischemic syndromeHIV-related retinopathy
DIFFERENTIAL DIAGNOSIS

THANK YOU















![The Guide - Diabetic Retinopathy - Vision Lossvisionloss.org.au/wp-content/uploads/2016/05/The... · the guide [diabetic retinopathy] What is Diabetic Retinopathy? Diabetic Retinopathy](https://static.fdocuments.in/doc/165x107/5e3ed00bf9c32e41ea6578a8/the-guide-diabetic-retinopathy-vision-the-guide-diabetic-retinopathy-what.jpg)


