
Diabetes Mellitus Integrated Care Pathway · Diabetes Mellitus Integrated Care Pathway Bristol,...
38
Diabetes Mellitus Integrated Care Pathway Bristol, North Somerset and South Gloucestershire Drug treatment pages 21 st April 2009 (4 th Edition, 2009)
Transcript of Diabetes Mellitus Integrated Care Pathway · Diabetes Mellitus Integrated Care Pathway Bristol,...
Diabetes Mellitus Integrated Care
Pathway
Bristol, North Somerset and South Gloucestershire
Drug treatment pages 21st April 2009
(4th Edition, 2009)
Index (ignore page numbers 21.04.09)1. Diagnosis of diabetes ............................................................................................................ 1
2. Initial assessment and classification 1) in adults .......................................................................................................................3 2) in children and adolescents.....................................................................................4
3. Initial management of type 1 diabetes in adults.............................................................6
4. Initial management of type 2 diabetes .............................................................................7 1) Assessment or risk factors and complications...................................................8 2) Dietary advice ............................................................................................................9 3) Lifestyle and exercise advice............................................................................... 10 4) Structured education for people with diabetes ...............................................11
5. Continuing care of type 1 and type 2 diabetes.............................................................. 13 1) Glycaemic control and monitoring........................................................................ 15
a) Targets...................................................................................................... 15 b) Drug treatment ....................................................................................... 15 c) Monitoring................................................................................................. 19
2) CHD risk factor control and targets .................................................................. 21 d) Management of hypertension................................................................ 22 e) Management of dyslipidaemia ............................................................... 25 f) Anti-platelet agents ................................................................................ 27
6. Suggested specialist referrals ........................................................................................ 28
7. Appendices ................................................................................................................................. 1) Screening for complications
a) Foot assessment form .......................................................................... 29 b) Nephropathy screening ....................................................................... 30
2) Management of complications a) Problematic hypoglycaemia ................................................................... 31 b) Diabetes foot pathway ......................................................................... 34 c) Painful diabetic neuropathy ................................................................ 35 d) Persistent albuminuria or microalbuminuria..................................... 37 e) Erectile dysfunction ............................................................................. 39
3) Special situations a) Diabetes in women
i. From adolescence & throughout potential child-bearing Years ................................................................................................ 41
ii. Pre-pregnancy in women with type 1 or type 2 diabetes .... 42 iii. Confirmed pregnancy in women with type 1 or 2 diabetes 44 iv. Pregnancy in women at risk of gestational diabetes............ 45 v. Post natal care .............................................................................. 46
b) Diabetes in children & young people .................................................. 47 c) Diabetes in the elderly & housebound............................................... 48 d) Managing diabetes at the end of life ................................................ 49 e) Diabetes and steroid treatment ........................................................ 52
4) Treatment a) Starting insulin in type 2 diabetes .................................................... 54 b) Weight management advice ................................................................. 57 c) Weight loss surgery referral.............................................................. 58
8. The Diabetes Teams and other contacts ...................................................................... 59
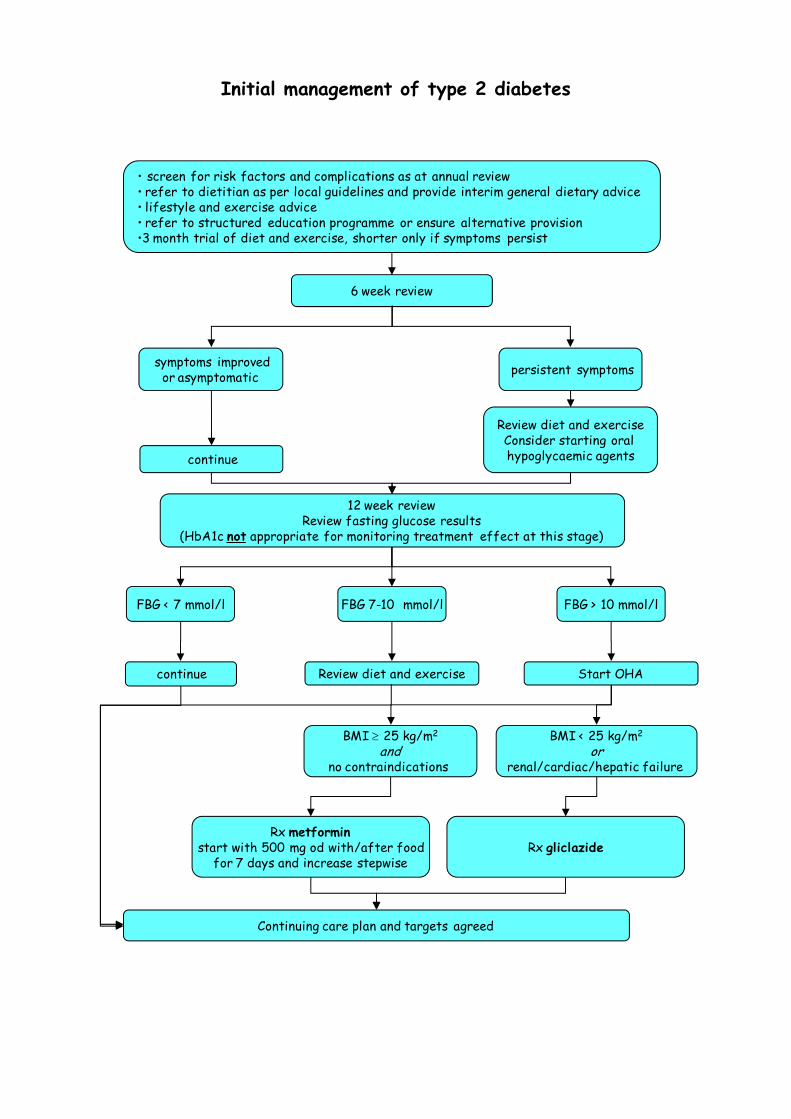
Initial management of type 2 diabetes
symptoms improvedor asymptomatic
6 week review
• screen for risk factors and complications as at annual review • refer to dietitian as per local guidelines and provide interim general dietary advice• lifestyle and exercise advice• refer to structured education programme or ensure alternative provision•3 month trial of diet and exercise, shorter only if symptoms persist
Continuing care plan and targets agreed
Review diet and exerciseConsider starting oral hypoglycaemic agents
persistent symptoms
continue
12 week reviewReview fasting glucose results
(HbA1c not appropriate for monitoring treatment effect at this stage)
FBG < 7 mmol/l FBG 7-10 mmol/l FBG > 10 mmol/l
continue Review diet and exercise Start OHA
BMI ≥ 25 kg/m2
andno contraindications
BMI < 25 kg/m2
orrenal/cardiac/hepatic failure
Rx metforminstart with 500 mg od with/after food
for 7 days and increase stepwiseRx gliclazide
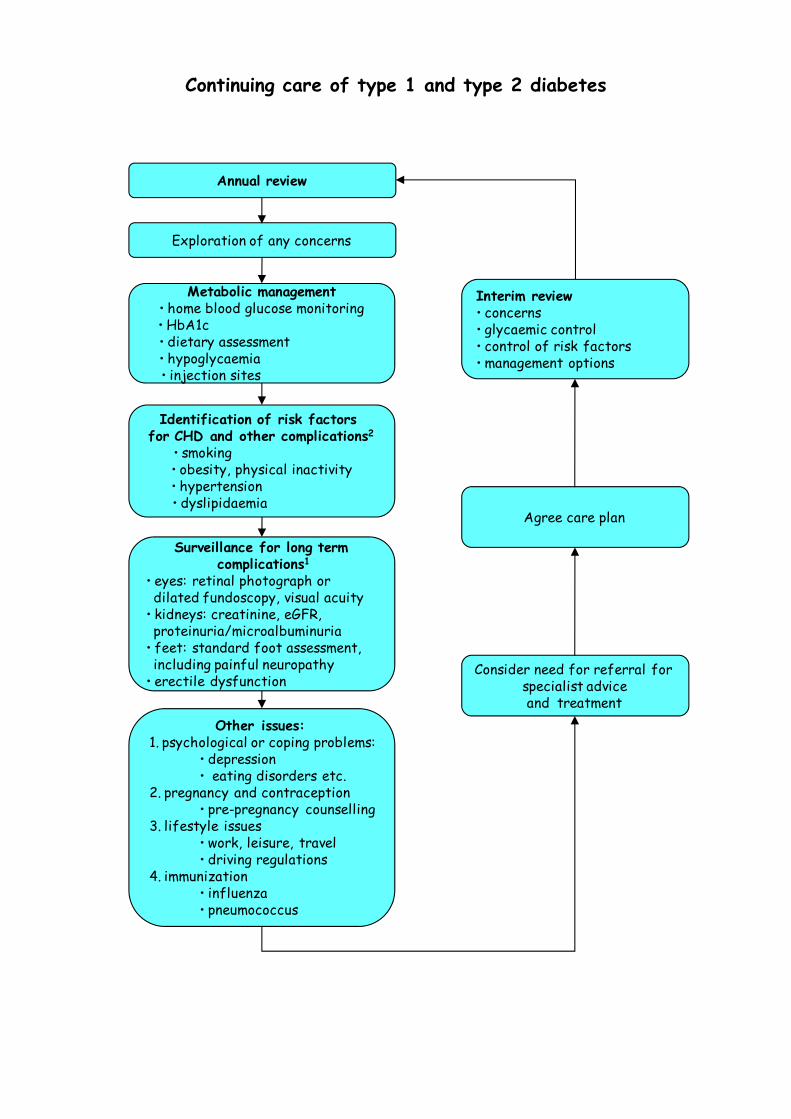
Continuing care of type 1 and type 2 diabetes
Annual review
Exploration of any concerns
Identification of risk factors for CHD and other complications2
• smoking • obesity, physical inactivity• hypertension • dyslipidaemia
Metabolic management• home blood glucose monitoring• HbA1c • dietary assessment • hypoglycaemia • injection sites
Surveillance for long termcomplications1
• eyes: retinal photograph or dilated fundoscopy, visual acuity
• kidneys: creatinine, eGFR, proteinuria/microalbuminuria
• feet: standard foot assessment, including painful neuropathy
• erectile dysfunction
Other issues:1. psychological or coping problems:
• depression • eating disorders etc.
2. pregnancy and contraception• pre-pregnancy counselling
3. lifestyle issues• work, leisure, travel• driving regulations
4. immunization• influenza• pneumococcus
Consider need for referral for specialist adviceand treatment
Agree care plan
Interim review• concerns• glycaemic control• control of risk factors• management options
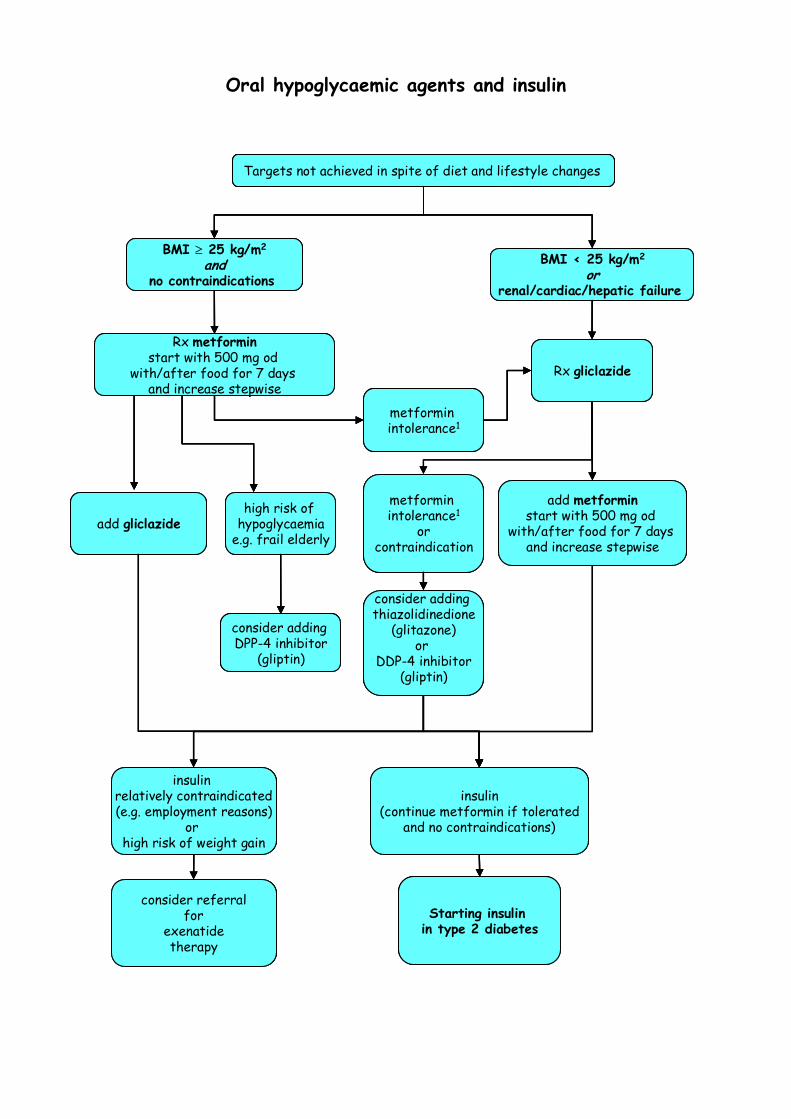
Oral hypoglycaemic agents and insulin
Rx metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
insulin(continue metformin if tolerated
and no contraindications)
BMI ≥ 25 kg/m2
andno contraindications
BMI < 25 kg/m2
orrenal/cardiac/hepatic failure
Rx gliclazide
add gliclazide
add metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
metforminintolerance1
metforminintolerance1
orcontraindication
consider adding thiazolidinedione
(glitazone)or
DDP-4 inhibitor(gliptin)
Targets not achieved in spite of diet and lifestyle changes
high risk of hypoglycaemia
e.g. frail elderly
consider adding DPP-4 inhibitor
(gliptin)
insulin relatively contraindicated(e.g. employment reasons)
or high risk of weight gain
consider referralfor
exenatidetherapy
Starting insulin in type 2 diabetes
Rx metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
insulin(continue metformin if tolerated
and no contraindications)
BMI ≥ 25 kg/m2
andno contraindications
BMI < 25 kg/m2
orrenal/cardiac/hepatic failure
Rx gliclazide
add gliclazide
add metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
metforminintolerance1
metforminintolerance1
orcontraindication
consider adding thiazolidinedione
(glitazone)or
DDP-4 inhibitor(gliptin)
Targets not achieved in spite of diet and lifestyle changes
high risk of hypoglycaemia
e.g. frail elderly
consider adding DPP-4 inhibitor
(gliptin)
insulin relatively contraindicated(e.g. employment reasons)
or high risk of weight gain
consider referralfor
exenatidetherapy
Starting insulin in type 2 diabetes
Rx metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
insulin(continue metformin if tolerated
and no contraindications)
BMI ≥ 25 kg/m2
andno contraindications
BMI < 25 kg/m2
orrenal/cardiac/hepatic failure
Rx gliclazide
add gliclazide
add metforminstart with 500 mg od
with/after food for 7 days and increase stepwise
metforminintolerance1
metforminintolerance1
orcontraindication
consider adding thiazolidinedione
(glitazone)or
DDP-4 inhibitor(gliptin)
Targets not achieved in spite of diet and lifestyle changes
high risk of hypoglycaemia
e.g. frail elderly
consider adding DPP-4 inhibitor
(gliptin)
insulin relatively contraindicated(e.g. employment reasons)
or high risk of weight gain
consider referralfor
exenatidetherapy
Starting insulin in type 2 diabetes
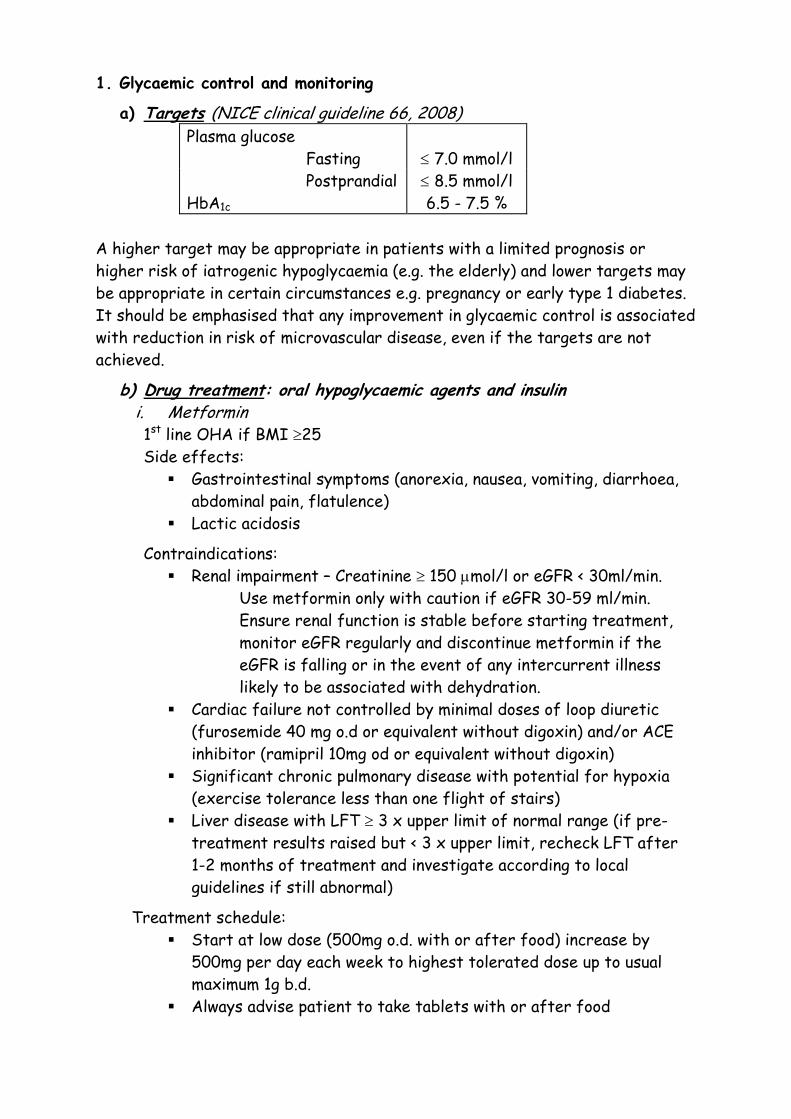
1. Glycaemic control and monitoring
a) Targets (NICE clinical guideline 66, 2008) Plasma glucose Fasting
≤ 7.0 mmol/l
Postprandial ≤ 8.5 mmol/l HbA1c 6.5 - 7.5 %
A higher target may be appropriate in patients with a limited prognosis or higher risk of iatrogenic hypoglycaemia (e.g. the elderly) and lower targets may be appropriate in certain circumstances e.g. pregnancy or early type 1 diabetes. It should be emphasised that any improvement in glycaemic control is associated with reduction in risk of microvascular disease, even if the targets are not achieved.
b) Drug treatment: oral hypoglycaemic agents and insulin i. Metformin 1st line OHA if BMI ≥25 Side effects:
Gastrointestinal symptoms (anorexia, nausea, vomiting, diarrhoea, abdominal pain, flatulence)
Lactic acidosis
Contraindications: Renal impairment – Creatinine ≥ 150 µmol/l or eGFR < 30ml/min.
Use metformin only with caution if eGFR 30-59 ml/min. Ensure renal function is stable before starting treatment, monitor eGFR regularly and discontinue metformin if the eGFR is falling or in the event of any intercurrent illness likely to be associated with dehydration.
Cardiac failure not controlled by minimal doses of loop diuretic (furosemide 40 mg o.d or equivalent without digoxin) and/or ACE inhibitor (ramipril 10mg od or equivalent without digoxin)
Significant chronic pulmonary disease with potential for hypoxia (exercise tolerance less than one flight of stairs)
Liver disease with LFT ≥ 3 x upper limit of normal range (if pre-treatment results raised but < 3 x upper limit, recheck LFT after 1-2 months of treatment and investigate according to local guidelines if still abnormal)
Treatment schedule: Start at low dose (500mg o.d. with or after food) increase by
500mg per day each week to highest tolerated dose up to usual maximum 1g b.d.
Always advise patient to take tablets with or after food
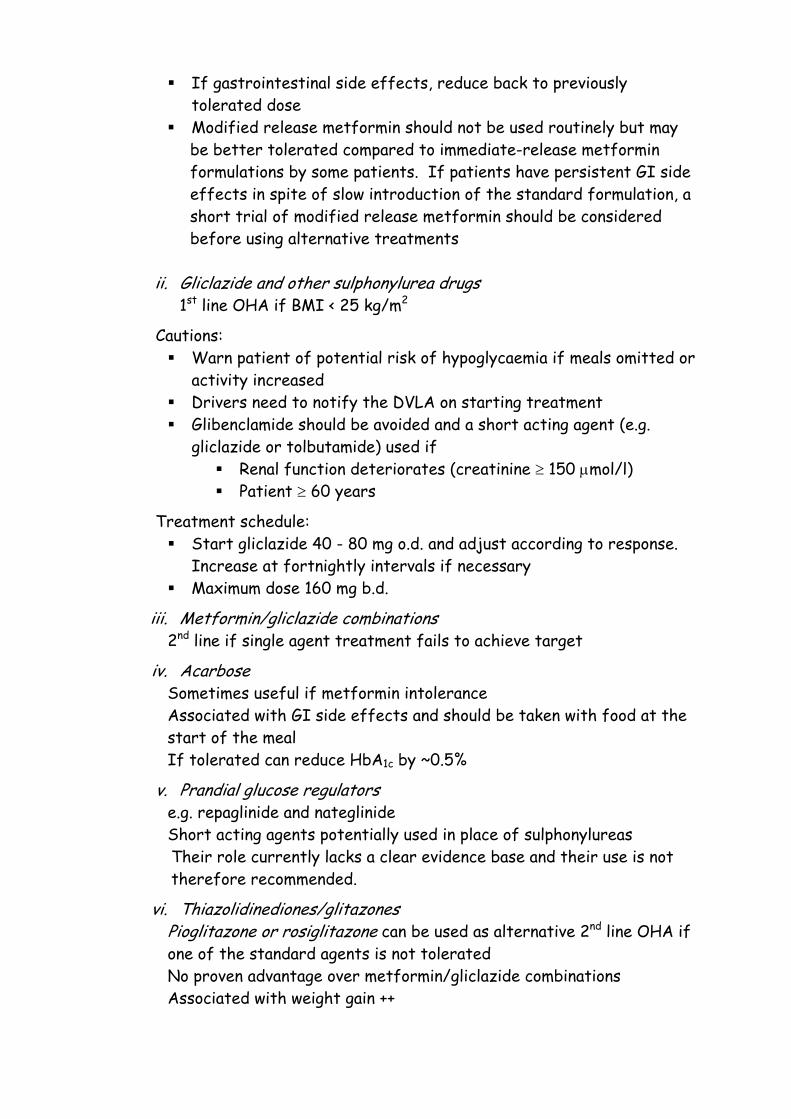
If gastrointestinal side effects, reduce back to previously tolerated dose
Modified release metformin should not be used routinely but may be better tolerated compared to immediate-release metformin formulations by some patients. If patients have persistent GI side effects in spite of slow introduction of the standard formulation, a short trial of modified release metformin should be considered before using alternative treatments
ii. Gliclazide and other sulphonylurea drugs
1st line OHA if BMI < 25 kg/m2
Cautions: Warn patient of potential risk of hypoglycaemia if meals omitted or
activity increased Drivers need to notify the DVLA on starting treatment Glibenclamide should be avoided and a short acting agent (e.g.
gliclazide or tolbutamide) used if Renal function deteriorates (creatinine ≥ 150 µmol/l) Patient ≥ 60 years
Treatment schedule: Start gliclazide 40 - 80 mg o.d. and adjust according to response.
Increase at fortnightly intervals if necessary Maximum dose 160 mg b.d.
iii. Metformin/gliclazide combinations 2nd line if single agent treatment fails to achieve target
iv. Acarbose Sometimes useful if metformin intolerance Associated with GI side effects and should be taken with food at the start of the meal If tolerated can reduce HbA1c by ~0.5%
v. Prandial glucose regulators e.g. repaglinide and nateglinide Short acting agents potentially used in place of sulphonylureas Their role currently lacks a clear evidence base and their use is not therefore recommended.
vi. Thiazolidinediones/glitazones Pioglitazone or rosiglitazone can be used as alternative 2nd line OHA if one of the standard agents is not tolerated No proven advantage over metformin/gliclazide combinations Associated with weight gain ++
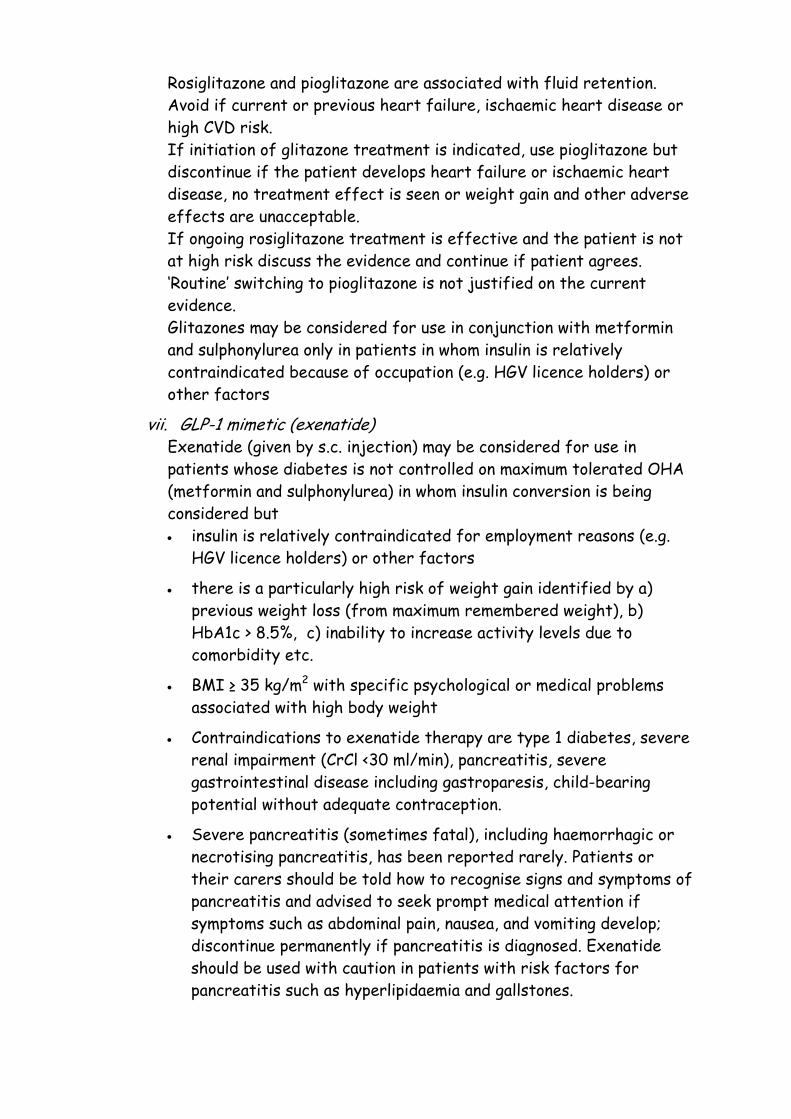
Rosiglitazone and pioglitazone are associated with fluid retention. Avoid if current or previous heart failure, ischaemic heart disease or high CVD risk. If initiation of glitazone treatment is indicated, use pioglitazone but discontinue if the patient develops heart failure or ischaemic heart disease, no treatment effect is seen or weight gain and other adverse effects are unacceptable. If ongoing rosiglitazone treatment is effective and the patient is not at high risk discuss the evidence and continue if patient agrees. ‘Routine’ switching to pioglitazone is not justified on the current evidence. Glitazones may be considered for use in conjunction with metformin and sulphonylurea only in patients in whom insulin is relatively contraindicated because of occupation (e.g. HGV licence holders) or other factors
vii. GLP-1 mimetic (exenatide) Exenatide (given by s.c. injection) may be considered for use in patients whose diabetes is not controlled on maximum tolerated OHA (metformin and sulphonylurea) in whom insulin conversion is being considered but • insulin is relatively contraindicated for employment reasons (e.g.
HGV licence holders) or other factors
• there is a particularly high risk of weight gain identified by a) previous weight loss (from maximum remembered weight), b) HbA1c > 8.5%, c) inability to increase activity levels due to comorbidity etc.
• BMI ≥ 35 kg/m2 with specific psychological or medical problems associated with high body weight
• Contraindications to exenatide therapy are type 1 diabetes, severe renal impairment (CrCl <30 ml/min), pancreatitis, severe gastrointestinal disease including gastroparesis, child-bearing potential without adequate contraception.
• Severe pancreatitis (sometimes fatal), including haemorrhagic or necrotising pancreatitis, has been reported rarely. Patients or their carers should be told how to recognise signs and symptoms of pancreatitis and advised to seek prompt medical attention if symptoms such as abdominal pain, nausea, and vomiting develop; discontinue permanently if pancreatitis is diagnosed. Exenatide should be used with caution in patients with risk factors for pancreatitis such as hyperlipidaemia and gallstones.
Exenatide is an ‘amber light’ drug that is initiated only by the diabetes teams in BNSSG. Patients in whom it is being considered should therefore be referred for consultant review. The drug should be discontinued in the absence of fall of at least 1.0% in HbA1c achieved within 6 months and sustained thereafter.
viii. DPP-4 inhibitors (gliptins) DPP-4 inhibitors (sitagliptin, vildgliptin) may be suitable second-line therapy instead of sulphonylurea if a patient is considered to be at significant risk of iatrogenic hypoglycaemia e.g. frail older people living alone. Their role otherwise currently lacks a clear evidence base. As they are novel agents with potential effects upon multiple tissues and have not yet been widely used, their use in other situations is not recommended.
ix. anti-obesity drugs and obesity surgery Orlistat and sibutramine may be considered as part of a weight-
loss strategy for people with type 2 diabetes and BMI ≥ 28 kg/m2 accordance with NICE guidance. Treatment should generally be discontinued after 12 weeks if patients have been unable to lose at least 5 % of the body weight as measured at the start of drug therapy.
Patients with type 2 diabetes with body mass index ≥ 35 kg/m2 may be suitable for gastric banding or other bariatric surgery in accordance with NICE guidance. Referrals to the service are accepted only from secondary care and patients who are potentially suitable should therefore be referred to the diabetes specialist team in the first instance (see Appendix 4c)
x. Insulin Use if treatment with combined oral hypoglycaemic agents fails to achieve targets. If metformin has previously been tolerated, it should generally be continued in patients with type 2 when starting insulin. See Appendix 4a for guidelines.
References: NICE clinical guideline 66: Management of type 2 diabetes (update) (2008)
(http://www.nice.org.uk/nicemedia/pdf/CG66NICEGuideline.pdf) NICE clinical guideline 43: Obesity (2006)
(http://www.nice.org.uk/nicemedia/pdf/CG43NICEGuideline.pdf )
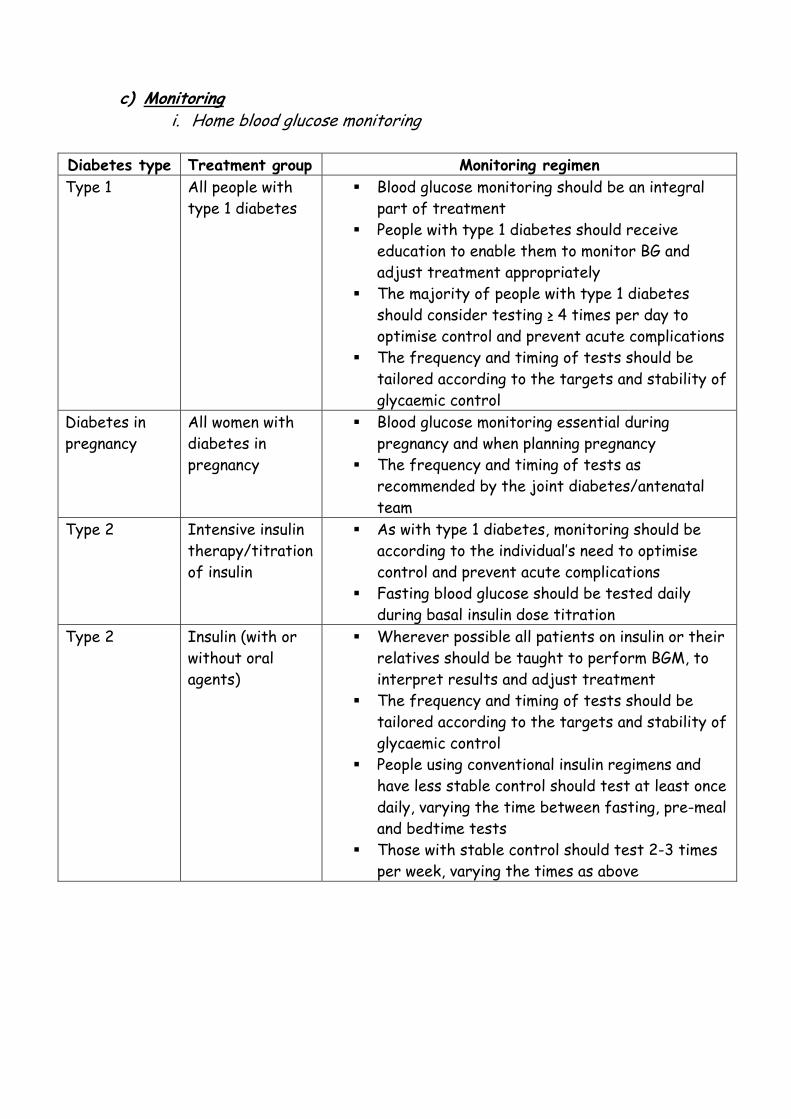
c) Monitoring
i. Home blood glucose monitoring
Diabetes type Treatment group Monitoring regimen Type 1 All people with
type 1 diabetes Blood glucose monitoring should be an integral
part of treatment People with type 1 diabetes should receive
education to enable them to monitor BG and adjust treatment appropriately
The majority of people with type 1 diabetes should consider testing ≥ 4 times per day to optimise control and prevent acute complications
The frequency and timing of tests should be tailored according to the targets and stability of glycaemic control
Diabetes in pregnancy
All women with diabetes in pregnancy
Blood glucose monitoring essential during pregnancy and when planning pregnancy
The frequency and timing of tests as recommended by the joint diabetes/antenatal team
Type 2 Intensive insulin therapy/titration of insulin
As with type 1 diabetes, monitoring should be according to the individual’s need to optimise control and prevent acute complications
Fasting blood glucose should be tested daily during basal insulin dose titration
Type 2 Insulin (with or without oral agents)
Wherever possible all patients on insulin or their relatives should be taught to perform BGM, to interpret results and adjust treatment
The frequency and timing of tests should be tailored according to the targets and stability of glycaemic control
People using conventional insulin regimens and have less stable control should test at least once daily, varying the time between fasting, pre-meal and bedtime tests
Those with stable control should test 2-3 times per week, varying the times as above
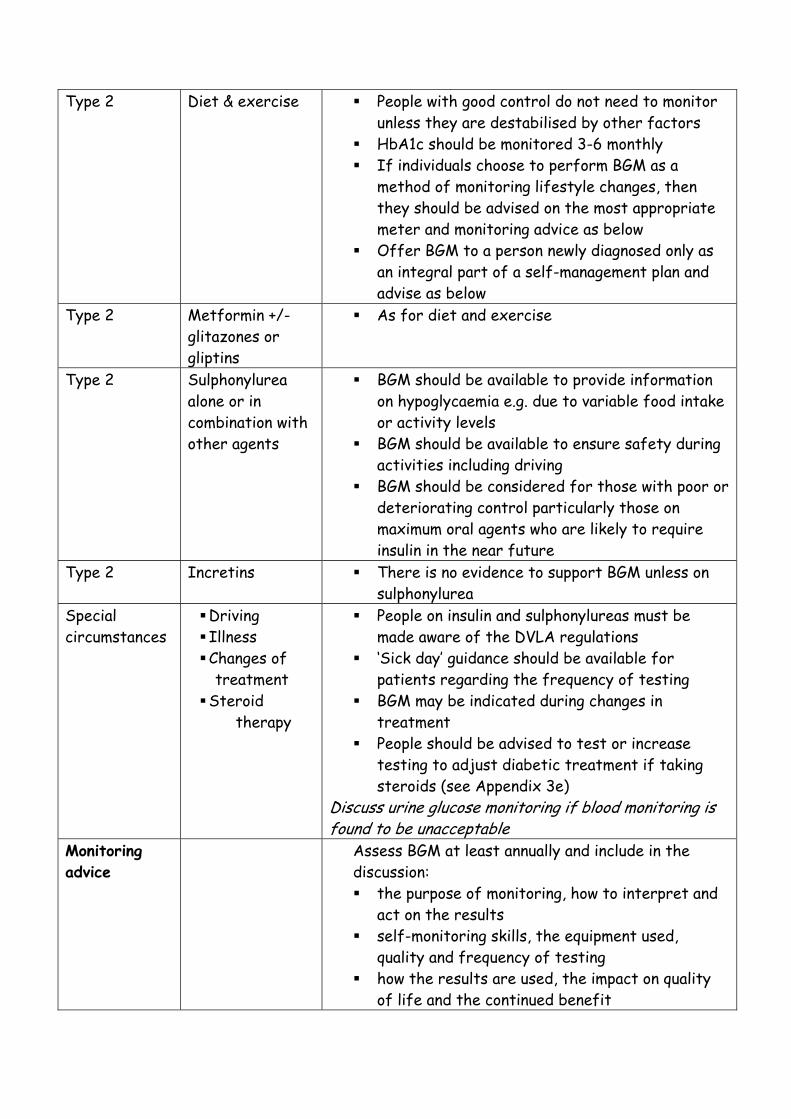
Type 2 Diet & exercise People with good control do not need to monitor
unless they are destabilised by other factors HbA1c should be monitored 3-6 monthly If individuals choose to perform BGM as a
method of monitoring lifestyle changes, then they should be advised on the most appropriate meter and monitoring advice as below
Offer BGM to a person newly diagnosed only as an integral part of a self-management plan and advise as below
Type 2 Metformin +/- glitazones or gliptins
As for diet and exercise
Type 2 Sulphonylurea alone or in combination with other agents
BGM should be available to provide information on hypoglycaemia e.g. due to variable food intake or activity levels
BGM should be available to ensure safety during activities including driving
BGM should be considered for those with poor or deteriorating control particularly those on maximum oral agents who are likely to require insulin in the near future
Type 2 Incretins There is no evidence to support BGM unless on sulphonylurea
Special circumstances
Driving Illness Changes of
treatment Steroid
therapy
People on insulin and sulphonylureas must be made aware of the DVLA regulations
‘Sick day’ guidance should be available for patients regarding the frequency of testing
BGM may be indicated during changes in treatment
People should be advised to test or increase testing to adjust diabetic treatment if taking steroids (see Appendix 3e)
Discuss urine glucose monitoring if blood monitoring is found to be unacceptable
Monitoring advice
Assess BGM at least annually and include in the discussion: the purpose of monitoring, how to interpret and
act on the results self-monitoring skills, the equipment used,
quality and frequency of testing how the results are used, the impact on quality
of life and the continued benefit
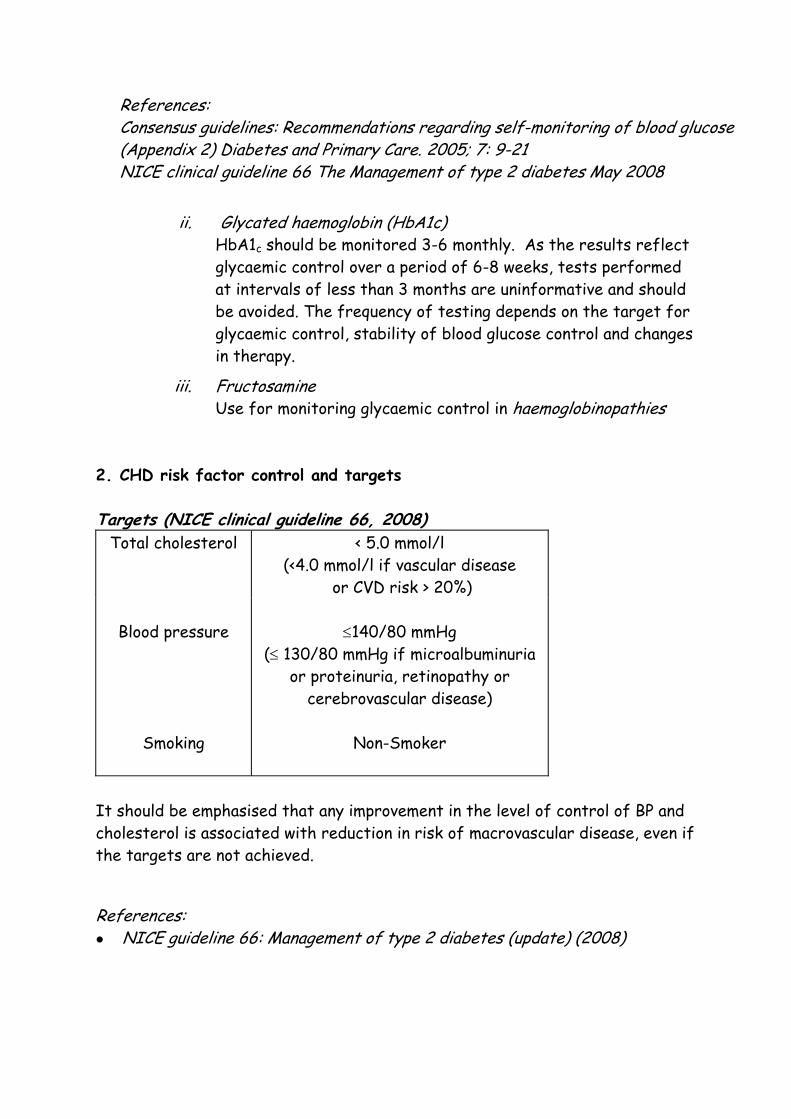
References: Consensus guidelines: Recommendations regarding self-monitoring of blood glucose (Appendix 2) Diabetes and Primary Care. 2005; 7: 9-21 NICE clinical guideline 66 The Management of type 2 diabetes May 2008
ii. Glycated haemoglobin (HbA1c) HbA1c should be monitored 3-6 monthly. As the results reflect glycaemic control over a period of 6-8 weeks, tests performed at intervals of less than 3 months are uninformative and should be avoided. The frequency of testing depends on the target for glycaemic control, stability of blood glucose control and changes in therapy.
iii. Fructosamine Use for monitoring glycaemic control in haemoglobinopathies
2. CHD risk factor control and targets
Targets (NICE clinical guideline 66, 2008) Total cholesterol
< 5.0 mmol/l
(<4.0 mmol/l if vascular disease or CVD risk > 20%)
Blood pressure
Smoking
≤140/80 mmHg
(≤ 130/80 mmHg if microalbuminuria or proteinuria, retinopathy or
cerebrovascular disease)
Non-Smoker
It should be emphasised that any improvement in the level of control of BP and cholesterol is associated with reduction in risk of macrovascular disease, even if the targets are not achieved.
References: NICE guideline 66: Management of type 2 diabetes (update) (2008)
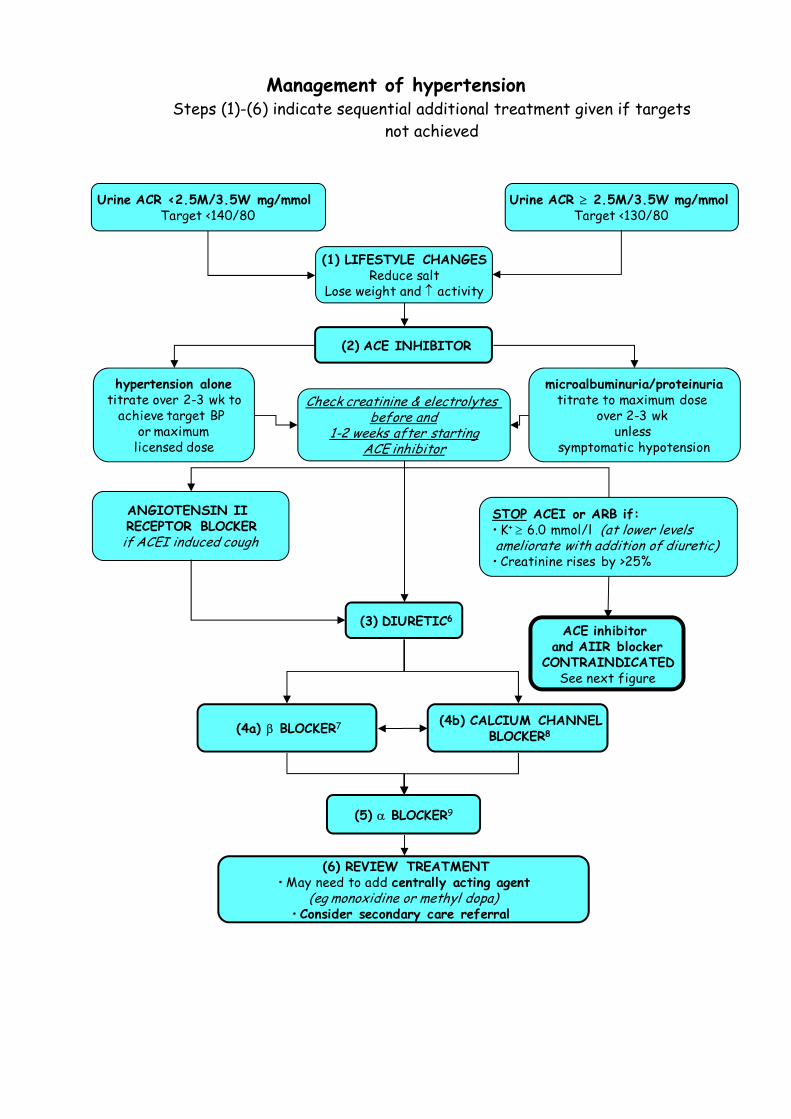
Management of hypertension Steps (1)-(6) indicate sequential additional treatment given if targets
not achieved
Check creatinine & electrolytes before and
1-2 weeks after startingACE inhibitor
Urine ACR <2.5M/3.5W mg/mmolTarget <140/80
Urine ACR ≥ 2.5M/3.5W mg/mmolTarget <130/80
(1) LIFESTYLE CHANGESReduce salt
Lose weight and ↑ activity
(2) ACE INHIBITOR
hypertension alonetitrate over 2-3 wk to
achieve target BP or maximum
licensed dose
microalbuminuria/proteinuriatitrate to maximum dose
over 2-3 wk unless
symptomatic hypotension
STOP ACEI or ARB if:• K+ ≥ 6.0 mmol/l (at lower levelsameliorate with addition of diuretic)• Creatinine rises by >25%
ANGIOTENSIN II RECEPTOR BLOCKER
if ACEI induced cough
(3) DIURETIC6
(4a) β BLOCKER7 (4b) CALCIUM CHANNELBLOCKER8
(5) α BLOCKER9
(6) REVIEW TREATMENT• May need to add centrally acting agent
(eg monoxidine or methyl dopa)• Consider secondary care referral
ACE inhibitor and AIIR blocker
CONTRAINDICATEDSee next figure
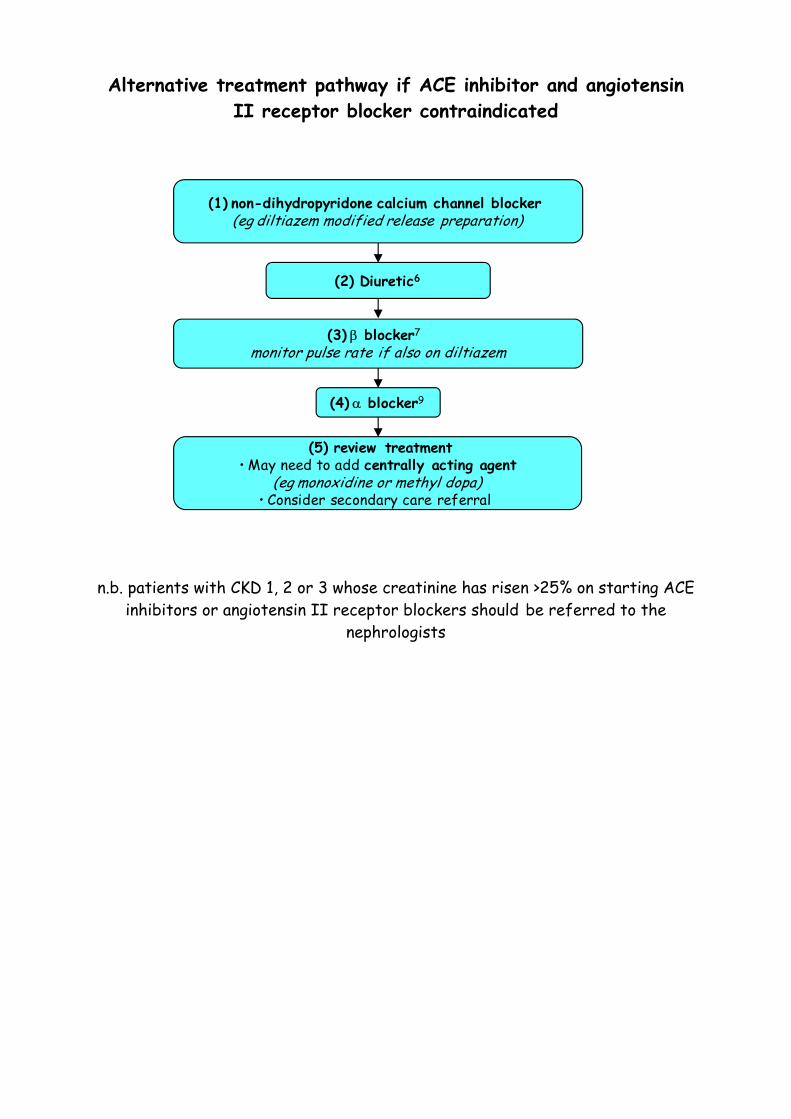
Alternative treatment pathway if ACE inhibitor and angiotensin II receptor blocker contraindicated
n.b. patients with CKD 1, 2 or 3 whose creatinine has risen >25% on starting ACE inhibitors or angiotensin II receptor blockers should be referred to the
nephrologists
(2) Diuretic6
(3) β blocker7
monitor pulse rate if also on diltiazem
(1) non-dihydropyridone calcium channel blocker (eg diltiazem modified release preparation)
(4) α blocker9
(5) review treatment• May need to add centrally acting agent
(eg monoxidine or methyl dopa)• Consider secondary care referral
Notes:
1. Salt intake should be reduced in all patients (patient advice is available on the websites of NHS direct and and the Food Standards Agency: http://www.nhs.uk/Livewell/Goodfood/Pages/salt.aspx http://www.eatwell.gov.uk/healthydiet/fss/salt/ )
2. Patients with ACR ≥ 3 mg/mmol should be started on an ACEI irrespective of blood pressure in line with guidelines for the management of proteinuria or persistent microalbuminuria
3. Check eGFR and potassium before and 1-2 weeks after commencing ACEI or ARB.
• Stop ACEI/ARB if potassium > 6.0 mmol/l with no modifiable cause. • Stop ACEI/ARB if eGFR falls >25% unless modifiable cause • If eGFR falls >5% but less than 25%, recheck eGFR in 1-2 weeks • Refer to nephrologists if eGFR falls >15% in patients with CKD 3 or
CKD 1 & 2
4. Consider stopping ACEI or ARB 1 week prior to elective surgery or during intercurrent illness (especially if fluid depleted) to reduce risk of acute kidney injury
5. Antihypertensive medication should be reviewed in all women planning pregnancy. If clinically acceptable ACEI and ARB should be stopped in all women planning pregnancy and replaced with alternative antihypertensive medication eg methyl dopa or nifedipine
6. Diuretics: bendroflumethiazide 2.5 mg od (maximum effect after 4-6 wk). Use furosemide 40 mg bd if the patient has oedema or GFR <60 ml/min/1.73m2
7. β blockers: Atenolol 50 mg od (avoid in critical limb ischaemia)
8. Calcium channel blockers: Long acting dihydropyridone CCB (e.g. amlodipine, nifedipine, felodipine) or non-dihydropyridone CCB (e.g. diltiazem modified release preparation or verapamil). Long acting dihydropyridone CCB and β blockers may be combined. Caution should be used if prescribing diltiazem and β blockers. Verapamil should not be prescribed with β blockers
9. α blockers: e.g. doxazosin 1 mg od for one wk → 2 mg od for one wk → 4 mg od for one wk. Increase dose further if target not achieved (max 16 mg od)
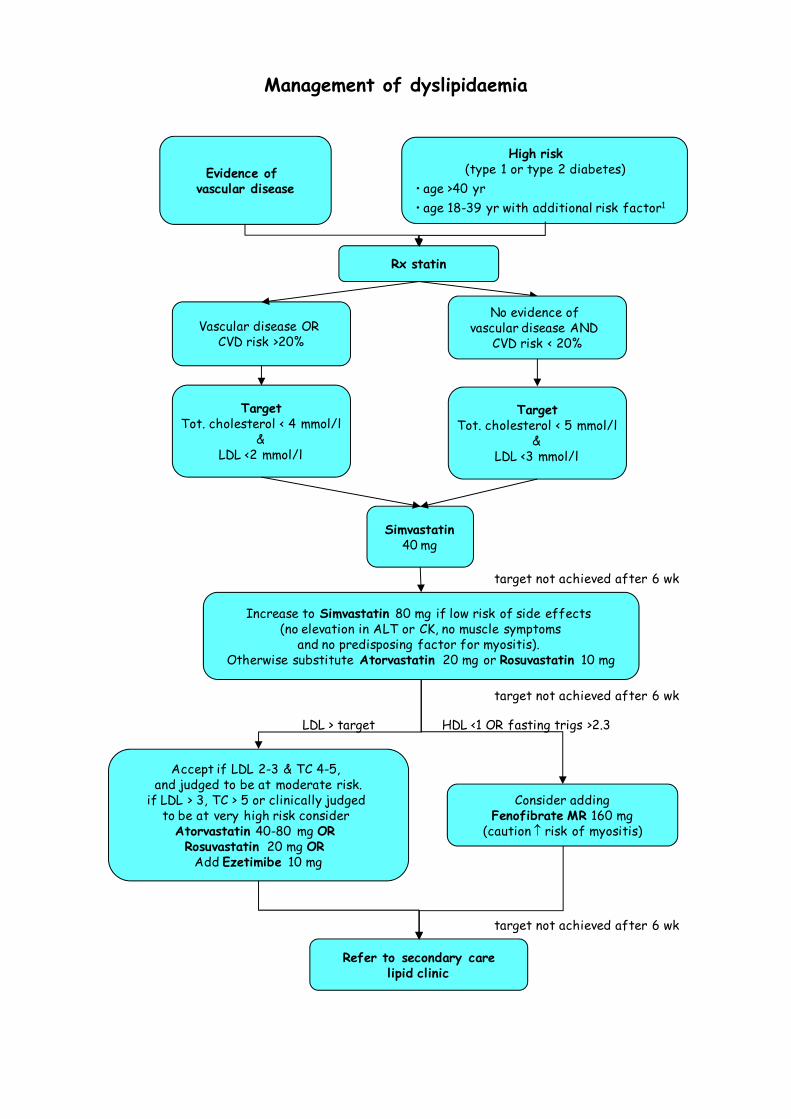
Management of dyslipidaemia
Rx statin
Evidence of vascular disease
Simvastatin40 mg
High risk(type 1 or type 2 diabetes)
• age >40 yr • age 18-39 yr with additional risk factor1
TargetTot. cholesterol < 4 mmol/l
&LDL <2 mmol/l
Increase to Simvastatin 80 mg if low risk of side effects (no elevation in ALT or CK, no muscle symptoms
and no predisposing factor for myositis). Otherwise substitute Atorvastatin 20 mg or Rosuvastatin 10 mg
Accept if LDL 2-3 & TC 4-5, and judged to be at moderate risk.
if LDL > 3, TC > 5 or clinically judged to be at very high risk consider
Atorvastatin 40-80 mg OR Rosuvastatin 20 mg OR
Add Ezetimibe 10 mg
Consider addingFenofibrate MR 160 mg
(caution ↑ risk of myositis)
Refer to secondary carelipid clinic
target not achieved after 6 wk
LDL > target HDL <1 OR fasting trigs >2.3
target not achieved after 6 wk
TargetTot. cholesterol < 5 mmol/l
&LDL <3 mmol/l
Vascular disease OR CVD risk >20%
No evidence of vascular disease AND
CVD risk < 20%
target not achieved after 6 wk
Notes:
1. Additional risk factor:
One or more of the following:
– Evidence of microvascular complications (retinopathy and/or microalbuminuria)
– hypertension on treatment,
– family history of premature cardiovascular disease,
– metabolic syndrome
– HbA1c ≥ 9.0%
– total cholesterol ≥ 6.0 mmol/l
2. Women who are considering pregnancy should stop statins prior to conception as there is a suggestion that statins may affect CNS and limb formation if taken during 1st trimester.
References:
NICE clinical guideline 66. The management of Type 2 diabetes (update) (May 2008)
NICE clinical guideline 67. Cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease (May 2008).
Anti-platelet agents National guidance on the use of antiplatelet agents for primary prevention of cardiovascular disease in people with diabetes is currently under review. The most recent NICE recommendations are to treat any person with type 1 or type 2 diabetes who meets any of the following criteria:
• Age ≥ 50
or
• Age < 50 and significant other cardiovascular risk factors
o hypertension on treatment,
o family history of premature cardiovascular disease,
o metabolic syndrome
o smoking
o microalbuminuria
o existing cardiovascular disease (MI or angina, stroke or TIA, or PVD) Start treatment after systolic blood pressure has been reduced to ≤145 mmHg.
Blood pressure should be kept at 145 mmHg or lower while aspirin is being taken as anti-platelet therapy.
Prescribe dispersible aspirin 75 mg od unless contraindicated (see below)
Consider use of combined dipyridamole/aspirin for 24 months in patients who have experienced a vascular event whilst on aspirin.
Contraindications to anti-platelet agents Aspirin allergy defined by anaphylaxis - rash or wheeze directly
attributable to aspirin ingestion. Consider use of clopidogrel for secondary prevention
Previous cerebral haemorrhage (ever)
Active peptic ulceration. In previous peptic ulcer disease, aspirin can be started in conjunction with a proton pump inhibitor
Bleeding tendency
Active hepatic disease
Concomitant warfarin therapy, unless indicated and carefully monitored
Uncontrolled hypertension (systolic BP ≥145 mmHg)
References: NICE clinical guideline 66: Management of type 2 diabetes (update) (2008) NICE clinical guideline 37: Type 1 diabetes (July 2004)
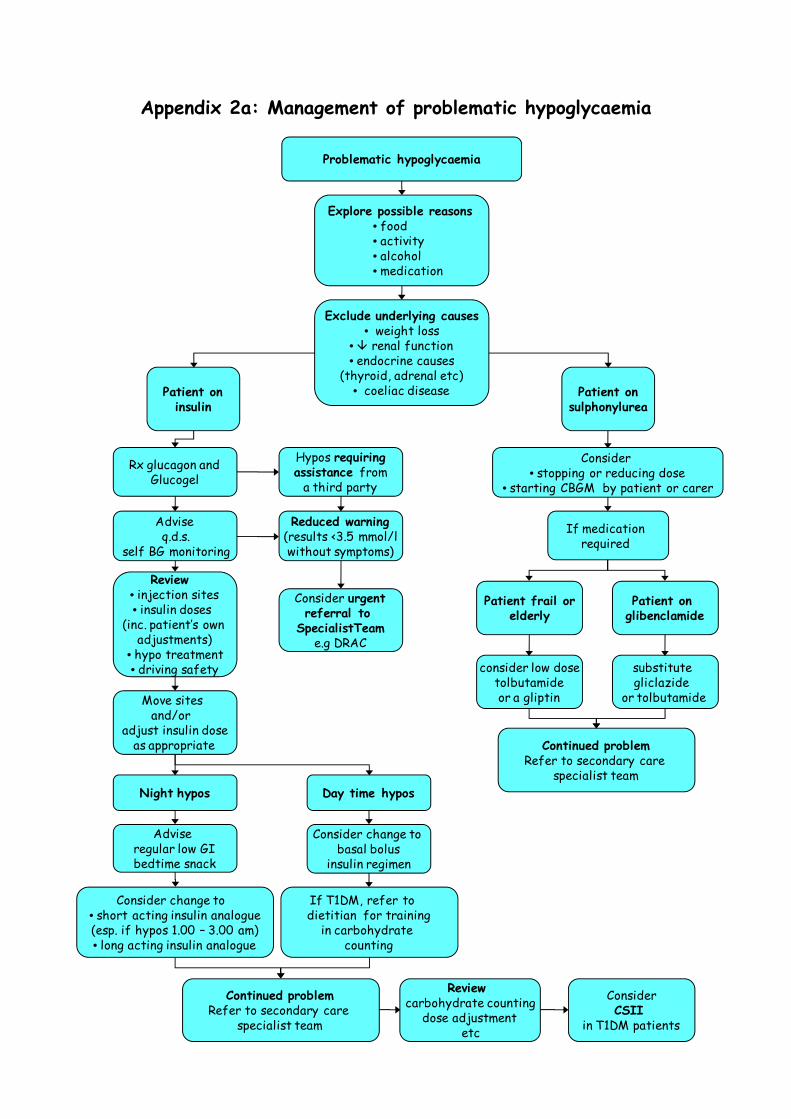
Appendix 2a: Management of problematic hypoglycaemia
Problematic hypoglycaemia
Explore possible reasons• food• activity• alcohol• medication
Exclude underlying causes• weight loss
• renal function• endocrine causes
(thyroid, adrenal etc)• coeliac diseasePatient on
insulinPatient on
sulphonylurea
Adviseq.d.s.
self BG monitoring
Hypos requiringassistance from
a third party
Review • injection sites• insulin doses
(inc. patient’s own adjustments)
• hypo treatment• driving safety
Reduced warning(results <3.5 mmol/lwithout symptoms)
Consider urgentreferral to
SpecialistTeame.g DRAC
Move sites and/or
adjust insulin doseas appropriate
Rx glucagon andGlucogel
Night hypos
Advise regular low GIbedtime snack
Consider change to • short acting insulin analogue(esp. if hypos 1.00 – 3.00 am)• long acting insulin analogue
Day time hypos
Consider change to basal bolus
insulin regimen
If T1DM, refer to dietitian for training
in carbohydrate counting
Continued problemRefer to secondary care
specialist team
Review carbohydrate counting
dose adjustmentetc
ConsiderCSII
in T1DM patients
substitute gliclazide
or tolbutamide
Patient on glibenclamide
Consider • stopping or reducing dose
• starting CBGM by patient or carer
Patient frail orelderly
consider low dosetolbutamideor a gliptin
If medication required
Continued problemRefer to secondary care
specialist team
Notes: Blood glucose levels of < 4 mmol/L should be treated as hypos whether or not accompanied by symptoms. 1. Possible reasons to be considered • Changes in food intake – reduced carbohydrate, delayed or missed meals or snacks.
Varying carbohydrate intake at meals may also cause hypos. • Physical activity – this can include activity such as housework, ironing, shopping and
gardening as well as exercise. Hypos may be delayed following intensive exercise • Medication/ insulin – incorrect or too much. Oral hypoglycaemic agents (eg
gliclazide, glibenclamide) can cause hypos • Alcohol - the effects can often be delayed until the following day, particularly if
large amounts of alcohol are consumed. Advise bedtime snack and blood glucose monitoring following day
2. Potential underlying causes • Renal impairment • Weight loss • Endocrine disorders (eg hypothyroidism, Addison’s disease) • Coeliac disease • Pregnancy • Injection sites (especially if the patient has moved sites) • Cessation/reduction of steroids without reduction in diabetes medication
3. Symptoms • Usual symptoms include sweating, trembling, weakness/fatigue, hunger,
palpitations, speech problems • Recurrent hypos will cause a change/reduction in hypo symptoms.
4. Immediate advice • Advise patients to test BG levels if possible in event of further hypos, and to
ingest 20g of quick acting carbohydrate – eg Lucozade, glucose tablets. Once blood glucose levels are above 4mmol/l to have a snack containing approx 15-20g of longer acting carbohydrate.
• Further information/patient information sheet is available at www.avondiabetes.nhs.uk
5. Assessment and management • Identify the BG level at which the patient’s warning symptoms occur – if
significant reduction in warning or symptoms occur only when BG less than 3.5mmol/l, refer to the diabetes specialist team: the Diabetes Rapid Access Clinic (DRAC) at NBT, the DSNs at UHBristol or the diabetes team at Weston General Hospital
• Encourage patient to test BG levels pre-meals, bed and around the time that hypos most commonly occur
• Explore timing of medication and food. Ensure insulin or sulphonylurea is being taken at recommended times in relation to meals
• Identify patterns in hypos, advise adjustment in insulin/medication accordingly • Review injection sites – lipohypertrophy can cause erratic absorption of insulin. If
patient advised to move sites reduce insulin by 10-20% initially. • Recheck HbA1c. HbA1c < 6.5% in insulin treated patients or HbA1c <6% on
sulphonylureas is suggestive of significant hypoglycaemia.
6. Hypo unawareness • If the patient experiences no symptoms until blood glucose is <3.5mmol/l, he/she
is considered to have hypo unawareness • Unawareness is potentially dangerous, especially if driving or operating machinery • Often the patient has no adrenergic symptoms, and therefore presents with
confusion or other neurological problems • Patients with hypo unawareness should be referred for specialist team review
complete avoidance of low BG levels for around 3 months can help restore warning symptoms. This requires intensive multiprofessional input
7. Indications for referral to secondary care • Hypo unawareness • Any unconscious episodes of hypoglycaemia • More than 3 hypos per week • Consider referral of any patient having hypos requiring assistance from a third
party
8. Driving and Hypoglycaemia • Patients with hypoglycaemia unawareness should be advised not to drive until
warnings return • Always check blood glucose levels before driving, and every 2 hours during the
journey • Do not drive if feeling hypoglycaemic or if blood glucose less than 4 mmol/l • Do not resume driving until 45 minutes after blood glucose has returned to normal.
It takes up to 45 minutes for the brain to fully recover. • If blood glucose ≤ 5mmol/l snack before driving • Ensure the patient knows to have a blood glucose meter and fast acting
carbohydrate in the car Ref: ‘A guide to insulin treated diabetes and driving’ http://www.dvla.gov.uk/media/pdf/medical/aagv1.pdf
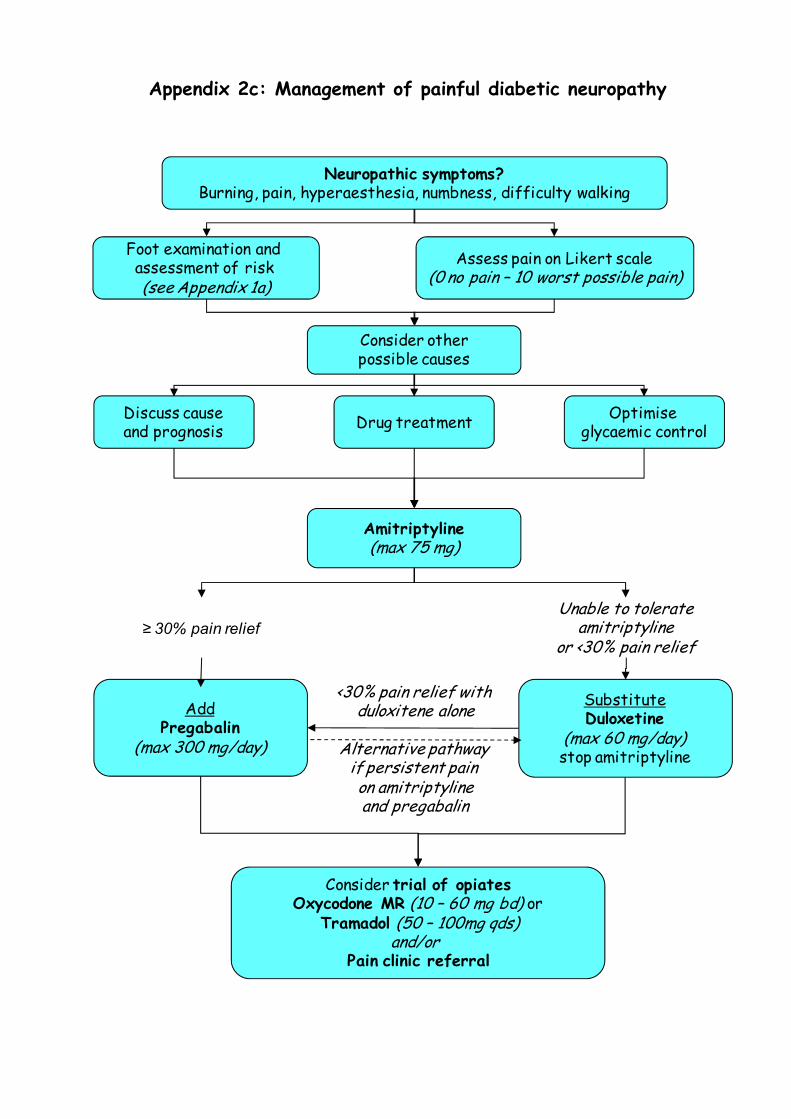
Appendix 2c: Management of painful diabetic neuropathy
Assess pain on Likert scale(0 no pain – 10 worst possible pain)
Foot examination and assessment of risk (see Appendix 1a)
Discuss causeand prognosis
AddPregabalin
(max 300 mg/day)
≥ 30% pain relief
Neuropathic symptoms?Burning, pain, hyperaesthesia, numbness, difficulty walking
Optimise glycaemic controlDrug treatment
Amitriptyline(max 75 mg)
SubstituteDuloxetine
(max 60 mg/day)stop amitriptyline
Consider trial of opiatesOxycodone MR (10 – 60 mg bd) or
Tramadol (50 – 100mg qds)and/or
Pain clinic referral
Consider otherpossible causes
Unable to tolerateamitriptyline
or <30% pain relief
<30% pain relief with duloxitene alone
Alternative pathway if persistent pain on amitriptylineand pregabalin
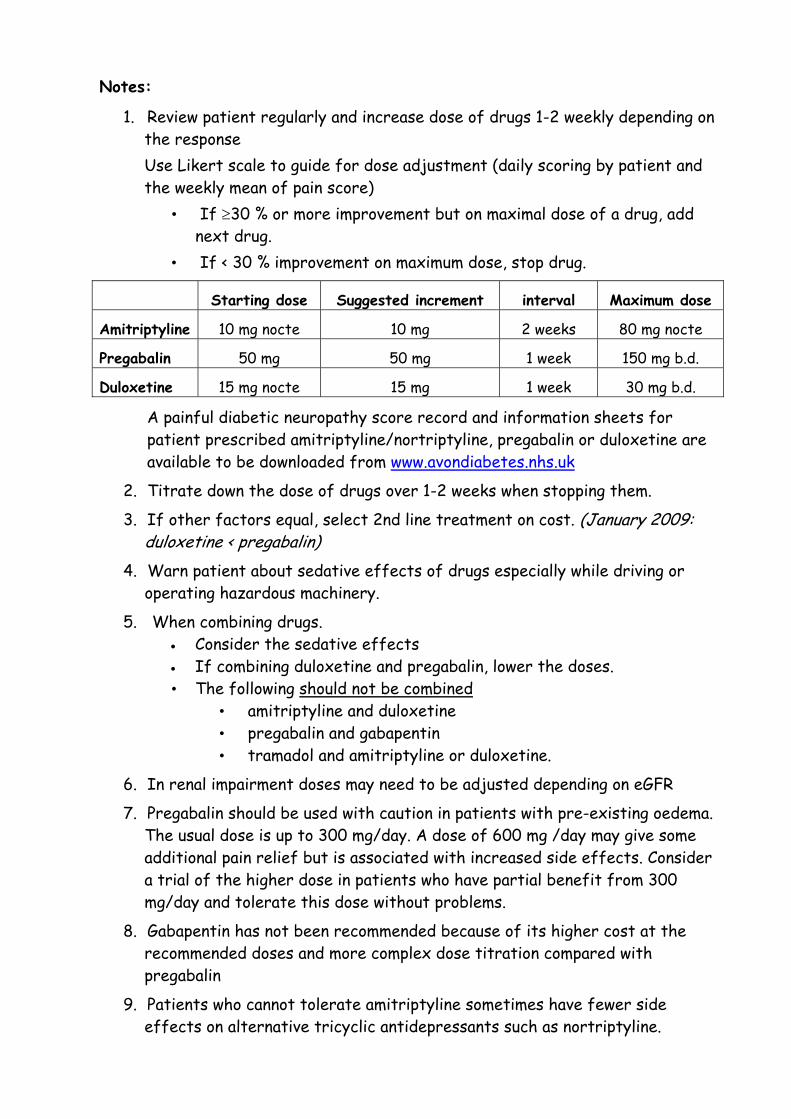
Notes:
1. Review patient regularly and increase dose of drugs 1-2 weekly depending on the response Use Likert scale to guide for dose adjustment (daily scoring by patient and the weekly mean of pain score)
• If ≥30 % or more improvement but on maximal dose of a drug, add next drug.
• If < 30 % improvement on maximum dose, stop drug.
Starting dose Suggested increment interval Maximum dose
Amitriptyline 10 mg nocte 10 mg 2 weeks 80 mg nocte
Pregabalin 50 mg 50 mg 1 week 150 mg b.d.
Duloxetine 15 mg nocte 15 mg 1 week 30 mg b.d.
A painful diabetic neuropathy score record and information sheets for patient prescribed amitriptyline/nortriptyline, pregabalin or duloxetine are available to be downloaded from www.avondiabetes.nhs.uk
2. Titrate down the dose of drugs over 1-2 weeks when stopping them.
3. If other factors equal, select 2nd line treatment on cost. (January 2009: duloxetine < pregabalin)
4. Warn patient about sedative effects of drugs especially while driving or operating hazardous machinery.
5. When combining drugs. • Consider the sedative effects • If combining duloxetine and pregabalin, lower the doses. • The following should not be combined
• amitriptyline and duloxetine • pregabalin and gabapentin • tramadol and amitriptyline or duloxetine.
6. In renal impairment doses may need to be adjusted depending on eGFR
7. Pregabalin should be used with caution in patients with pre-existing oedema. The usual dose is up to 300 mg/day. A dose of 600 mg /day may give some additional pain relief but is associated with increased side effects. Consider a trial of the higher dose in patients who have partial benefit from 300 mg/day and tolerate this dose without problems.
8. Gabapentin has not been recommended because of its higher cost at the recommended doses and more complex dose titration compared with pregabalin
9. Patients who cannot tolerate amitriptyline sometimes have fewer side effects on alternative tricyclic antidepressants such as nortriptyline.
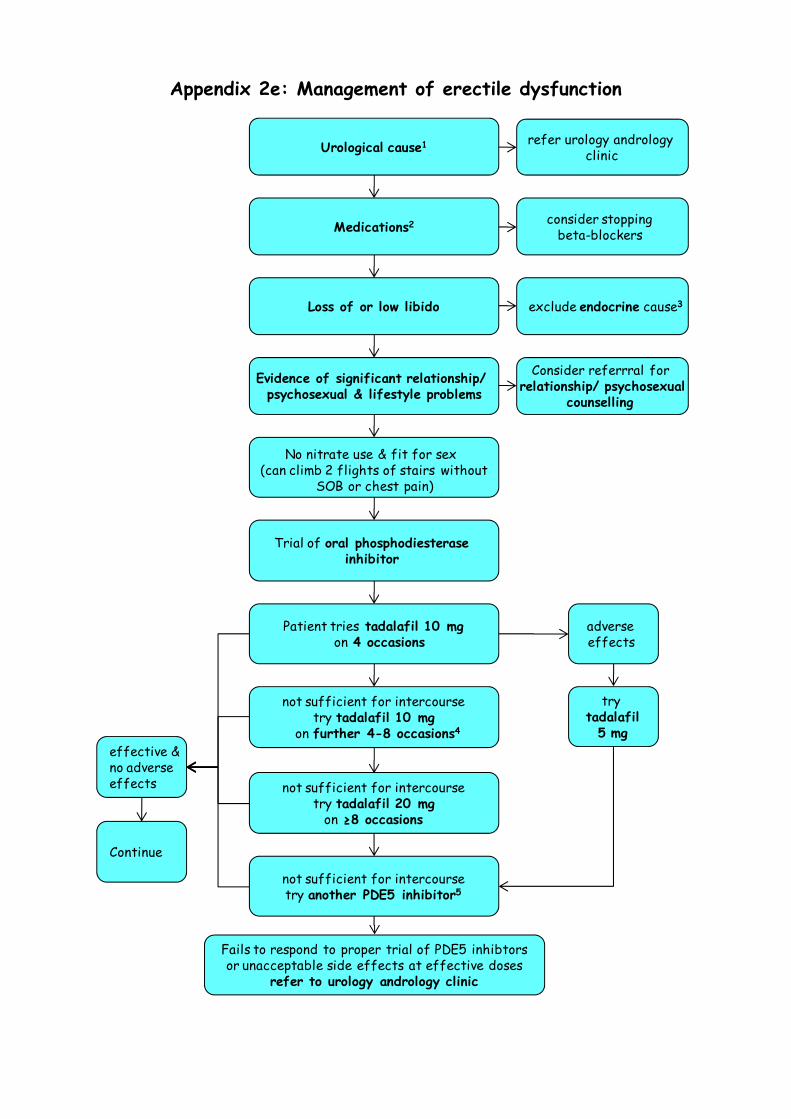
Appendix 2e: Management of erectile dysfunction
Evidence of significant relationship/ psychosexual & lifestyle problems
Consider referrral for relationship/ psychosexual
counselling
No nitrate use & fit for sex (can climb 2 flights of stairs without
SOB or chest pain)
Trial of oral phosphodiesterase inhibitor
consider stopping beta-blockers Medications2
exclude endocrine cause3Loss of or low libido
Urological cause1 refer urology andrology clinic
effective & no adverse effects
Continue
not sufficient for intercoursetry tadalafil 20 mg
on ≥8 occasions
not sufficient for intercoursetry another PDE5 inhibitor5
Patient tries tadalafil 10 mgon 4 occasions
adverse effects
not sufficient for intercoursetry tadalafil 10 mg
on further 4-8 occasions4
try tadalafil
5 mg
Fails to respond to proper trial of PDE5 inhibtorsor unacceptable side effects at effective doses
refer to urology andrology clinic
Notes:
• Erectile dysfunction is usually multifactorial • Organic cause likely if: gradual onset, present in all situations (inc waking
& self stimulation), lack of tumescence, normal ejaculation, risk factors. • Psychogenic cause likely if: sudden onset, early collapse of erection,
normal spontaneous/ waking/ self stimulated erections, premature or absent ejaculation.
Identify treatable causes if possible Notes:
1. Urological causes: e.g. curved penis (Peyronie’s disease), pelvic injury, pelvic/prostatic surgery or radiation treatment.
2. Many drugs can theoretically cause ED but medication changes rarely result in improvement apart from stopping β blockers.
3. Check testosterone, SHBG, LH, FSH, prolactin and thyroid function. Refer for endocrine opinion if appropriate.
4. Effective erections occur after a mean of 8-12 doses of oral phosphodiesterase inhibitors. If any appears ineffective, patient should try the drug on at least 8 occasions at the maximum or maximum tolerated dose before abandoning.
5. Other PDE5 inhibitors: sildenafil (Viagra) 25-100mg or vardenafil (Levitra) 5-20mg. Start at sildenafil 50 mg or vardenafil 10 mg and titrate to response and adverse effects as above. If either appears ineffective, try on at least 8 occasions before abandoning.
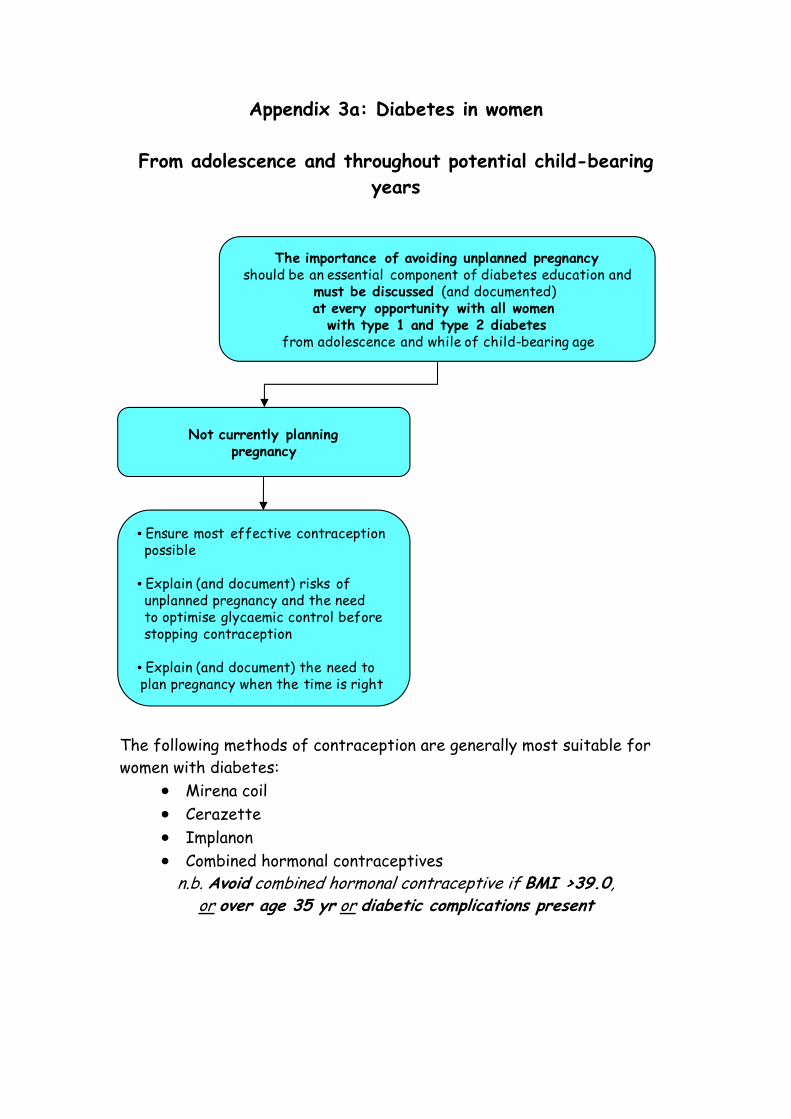
Appendix 3a: Diabetes in women
From adolescence and throughout potential child-bearing years
The following methods of contraception are generally most suitable for women with diabetes:
• Mirena coil • Cerazette • Implanon • Combined hormonal contraceptives
n.b. Avoid combined hormonal contraceptive if BMI >39.0, or over age 35 yr or diabetic complications present
The importance of avoiding unplanned pregnancyshould be an essential component of diabetes education and
must be discussed (and documented) at every opportunity with all women
with type 1 and type 2 diabetesfrom adolescence and while of child-bearing age
Not currently planningpregnancy
• Ensure most effective contraceptionpossible
• Explain (and document) risks of unplanned pregnancy and the need to optimise glycaemic control beforestopping contraception
• Explain (and document) the need to plan pregnancy when the time is right
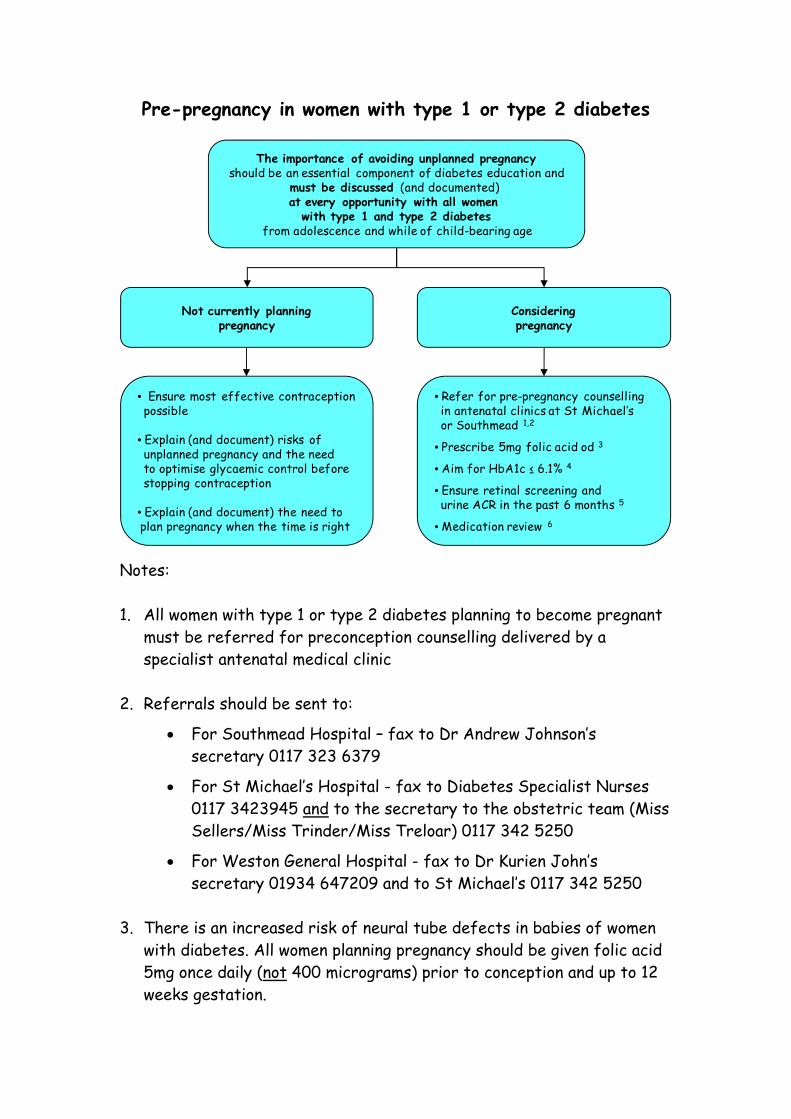
Pre-pregnancy in women with type 1 or type 2 diabetes
The importance of avoiding unplanned pregnancyshould be an essential component of diabetes education and
must be discussed (and documented) at every opportunity with all women
with type 1 and type 2 diabetesfrom adolescence and while of child-bearing age
Not currently planningpregnancy
• Ensure most effective contraceptionpossible
• Explain (and document) risks of unplanned pregnancy and the need to optimise glycaemic control beforestopping contraception
• Explain (and document) the need to plan pregnancy when the time is right
Consideringpregnancy
• Refer for pre-pregnancy counsellingin antenatal clinics at St Michael’s or Southmead 1,2
• Prescribe 5mg folic acid od 3
• Aim for HbA1c ≤ 6.1% 4
• Ensure retinal screening and urine ACR in the past 6 months 5
• Medication review 6
Notes: 1. All women with type 1 or type 2 diabetes planning to become pregnant
must be referred for preconception counselling delivered by a specialist antenatal medical clinic
2. Referrals should be sent to:
• For Southmead Hospital – fax to Dr Andrew Johnson’s secretary 0117 323 6379
• For St Michael’s Hospital - fax to Diabetes Specialist Nurses 0117 3423945 and to the secretary to the obstetric team (Miss Sellers/Miss Trinder/Miss Treloar) 0117 342 5250
• For Weston General Hospital - fax to Dr Kurien John’s secretary 01934 647209 and to St Michael’s 0117 342 5250
3. There is an increased risk of neural tube defects in babies of women
with diabetes. All women planning pregnancy should be given folic acid 5mg once daily (not 400 micrograms) prior to conception and up to 12 weeks gestation.
4. Advise women to aim for an HbA1c below 6.1%, if safe.
Inform women that any reduction in HbA1c may reduce risks. Advise women with HbA1c above 10% to avoid pregnancy.
5. Diabetic retinopathy can worsen in pregnancy, therefore all women
must have retinal assessment by digital imaging with mydriasis using tropicamide within the 6 months prior to conceiving
6. Medication review:
• Oral hypoglycaemic agents may need to be stopped and insulin started if required. However, NICE guidance allows the use of metformin (and exceptionally, with informed consent, glibenclamide) in pregnancy under specialist antenatal care.
• Angiotensin-converting enzyme inhibitors and angiotensin-II receptor antagonists should be stopped and alternative antihypertensives started (methyldopa)
• Statins should be stopped Reference: NICE clinical guideline 63: Diabetes in Pregnancy (July 2008) http://www.nice.org.uk/nicemedia/pdf/CG063NICEGuideline.pdf
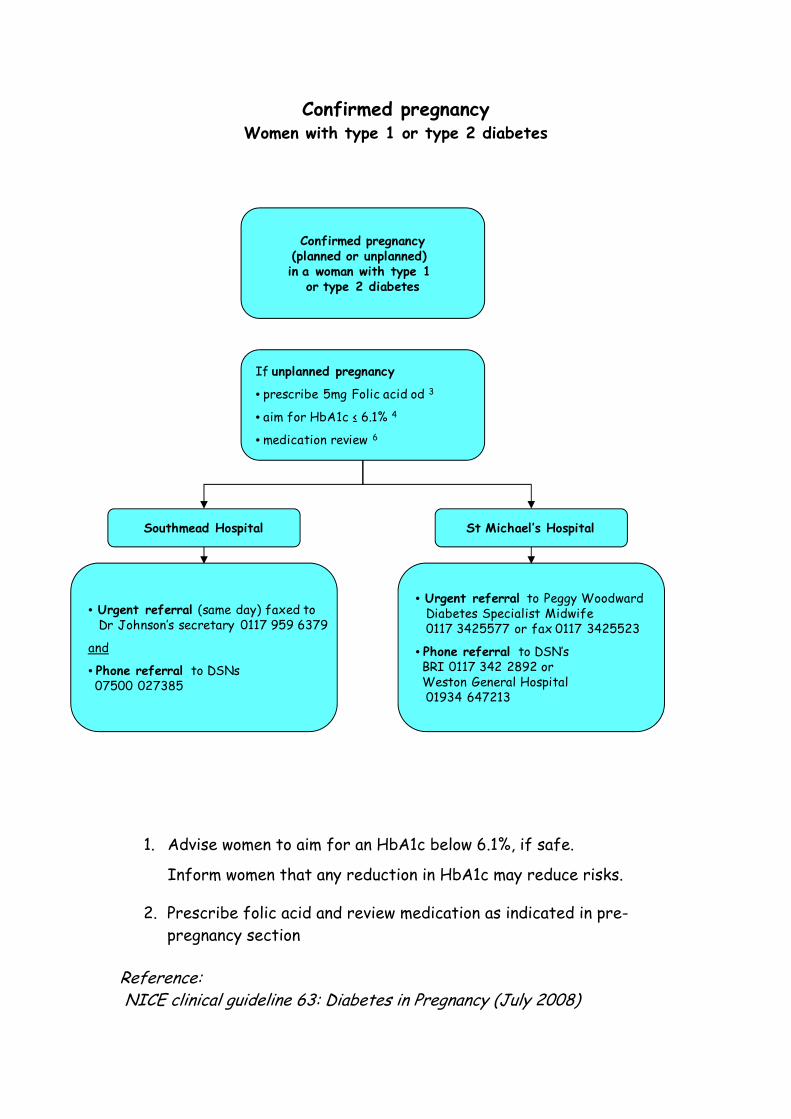
Confirmed pregnancy Women with type 1 or type 2 diabetes
1. Advise women to aim for an HbA1c below 6.1%, if safe.
Inform women that any reduction in HbA1c may reduce risks.
2. Prescribe folic acid and review medication as indicated in pre-pregnancy section
Reference: NICE clinical guideline 63: Diabetes in Pregnancy (July 2008)
If unplanned pregnancy
• prescribe 5mg Folic acid od 3
• aim for HbA1c ≤ 6.1% 4
• medication review 6
Southmead Hospital St Michael’s Hospital
• Urgent referral (same day) faxed toDr Johnson’s secretary 0117 959 6379
and
• Phone referral to DSNs07500 027385
• Urgent referral to Peggy WoodwardDiabetes Specialist Midwife 0117 3425577 or fax 0117 3425523
• Phone referral to DSN’s BRI 0117 342 2892 orWeston General Hospital 01934 647213
Confirmed pregnancy(planned or unplanned) in a woman with type 1
or type 2 diabetes
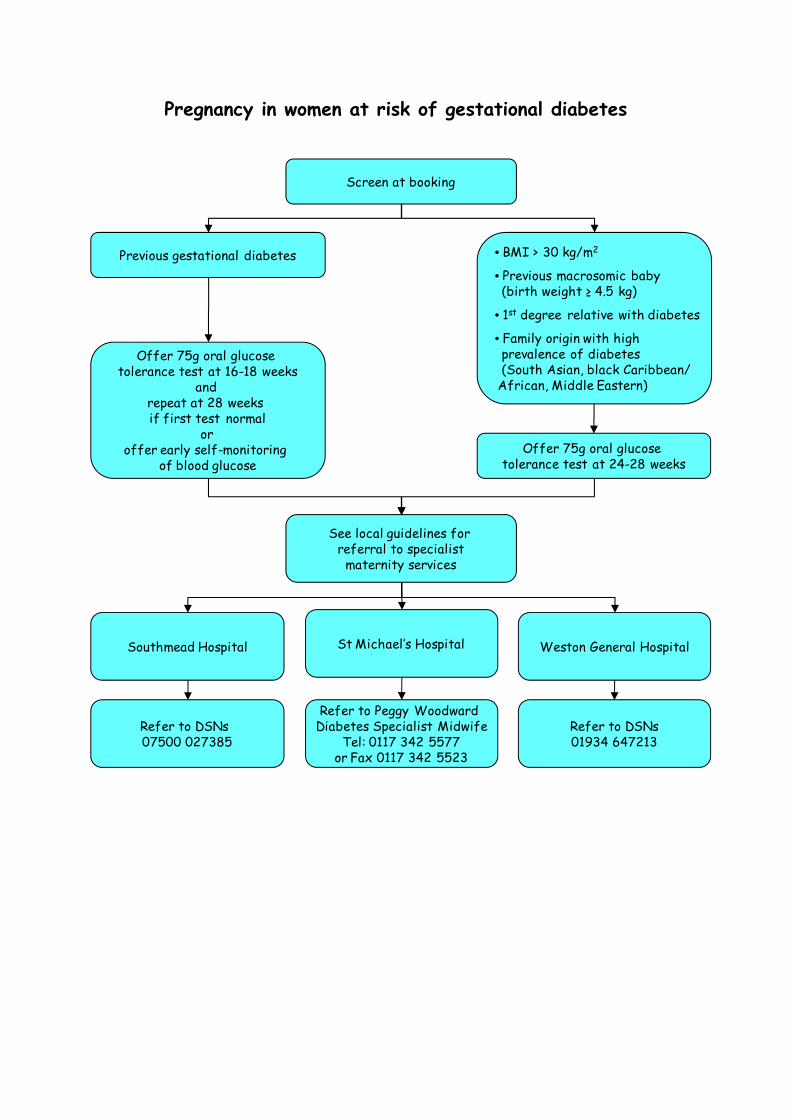
Pregnancy in women at risk of gestational diabetes
Screen at booking
Previous gestational diabetes • BMI > 30 kg/m2
• Previous macrosomic baby (birth weight ≥ 4.5 kg)
• 1st degree relative with diabetes
• Family origin with high prevalence of diabetes(South Asian, black Caribbean/
African, Middle Eastern)
Offer 75g oral glucose tolerance test at 16-18 weeks
and repeat at 28 weeks if first test normal
or offer early self-monitoring
of blood glucose
See local guidelines for referral to specialist
maternity services
Southmead Hospital St Michael’s Hospital Weston General Hospital
Refer to DSNs 07500 027385
Refer to Peggy Woodward Diabetes Specialist Midwife
Tel: 0117 342 5577or Fax 0117 342 5523
Refer to DSNs01934 647213
Offer 75g oral glucose tolerance test at 24-28 weeks
Post natal care
General:
• Breastfeeding - continue to avoid drugs discontinued for safety reasons
• Advise on the importance of contraception and pre-conception care when planning future pregnancies
Gestational diabetes:
• Advise on
o weight control, diet / exercise
o symptoms of hyperglycaemia
o Risks of gestational diabetes and need for screening when planning pregnancy
• FBG at the 6-week postnatal appointment, then annually
Insulin-treated pre-existing diabetes:
• Encourage frequent monitoring as insulin requirements may change
• Risk of hypoglycaemia, especially while breastfeeding
• Food available before / during breastfeeding
• Refer back to routine diabetes care
Type 2 diabetes:
• Resume or continue metformin or insulin while breastfeeding. Other oral hypoglycaemic agents to be avoided
• Refer back to routine diabetes care Ophthalmological follow-up:
• Women with preproliferative diabetic retinopathy diagnosed in pregnancy should be offered ophthalmological follow-up for at least 6 months post partum
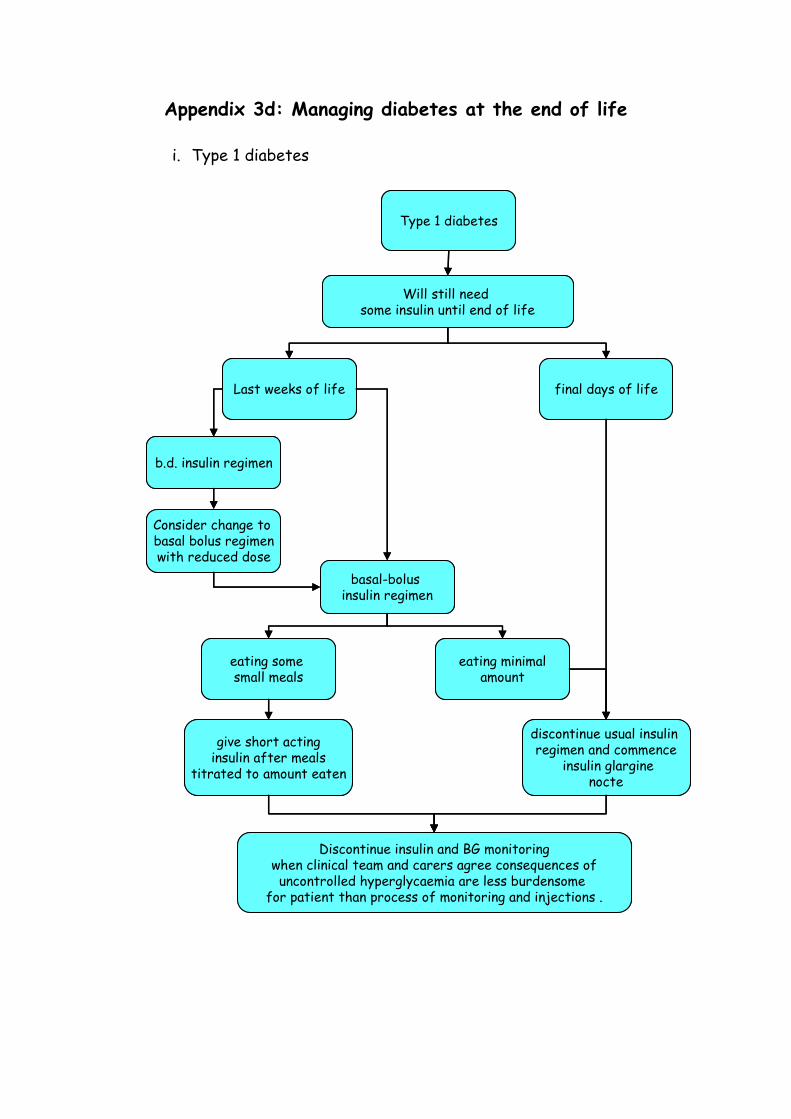
Appendix 3d: Managing diabetes at the end of life
i. Type 1 diabetes
Type 1 diabetes
Last weeks of life
Will still need some insulin until end of life
Consider change to basal bolus regimenwith reduced dose
eating some small meals
eating minimalamount
give short actinginsulin after meals
titrated to amount eaten
discontinue usual insulin regimen and commence
insulin glarginenocte
final days of life
b.d. insulin regimen
basal-bolus insulin regimen
Discontinue insulin and BG monitoringwhen clinical team and carers agree consequences ofuncontrolled hyperglycaemia are less burdensome
for patient than process of monitoring and injections .
Type 1 diabetes
Last weeks of life
Will still need some insulin until end of life
Consider change to basal bolus regimenwith reduced dose
eating some small meals
eating minimalamount
give short actinginsulin after meals
titrated to amount eaten
discontinue usual insulin regimen and commence
insulin glarginenocte
final days of life
b.d. insulin regimen
basal-bolus insulin regimen
Discontinue insulin and BG monitoringwhen clinical team and carers agree consequences ofuncontrolled hyperglycaemia are less burdensome
for patient than process of monitoring and injections .
ii. Type 2 diabetes
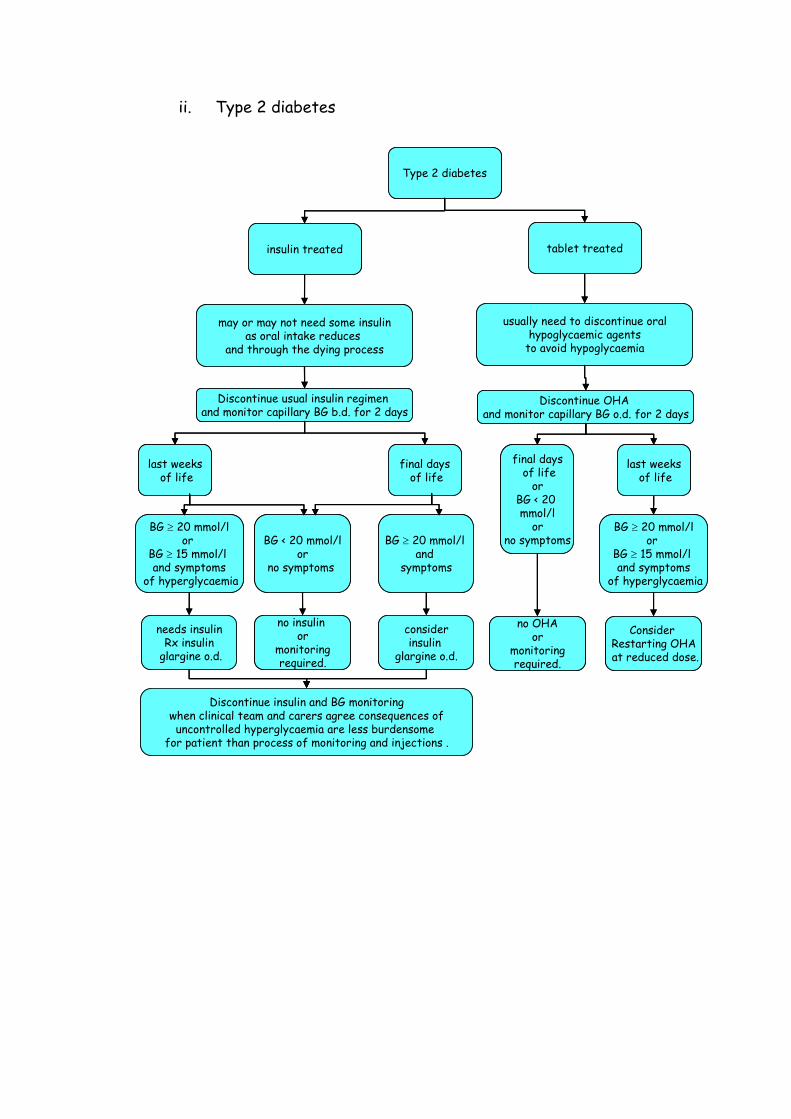
Type 2 diabetes
last weeksof life
may or may not need some insulinas oral intake reduces
and through the dying process
needs insulinRx insulin
glargine o.d.
final daysof life
Discontinue usual insulin regimen and monitor capillary BG b.d. for 2 days
BG ≥ 20 mmol/lor
BG ≥ 15 mmol/land symptoms
of hyperglycaemia
insulin treated tablet treated
BG < 20 mmol/lor
no symptoms
no insulin or
monitoring required.
BG ≥ 20 mmol/land
symptoms
considerinsulin
glargine o.d.
Discontinue insulin and BG monitoringwhen clinical team and carers agree consequences ofuncontrolled hyperglycaemia are less burdensome
for patient than process of monitoring and injections .
Discontinue OHA and monitor capillary BG o.d. for 2 days
usually need to discontinue oralhypoglycaemic agents
to avoid hypoglycaemia
BG ≥ 20 mmol/lor
BG ≥ 15 mmol/land symptoms
of hyperglycaemia
Consider Restarting OHAat reduced dose.
last weeksof life
final daysof life
orBG < 20 mmol/l
orno symptoms
no OHAor
monitoring required.
Type 2 diabetes
last weeksof life
may or may not need some insulinas oral intake reduces
and through the dying process
needs insulinRx insulin
glargine o.d.
final daysof life
Discontinue usual insulin regimen and monitor capillary BG b.d. for 2 days
BG ≥ 20 mmol/lor
BG ≥ 15 mmol/land symptoms
of hyperglycaemia
insulin treated tablet treated
BG < 20 mmol/lor
no symptoms
no insulin or
monitoring required.
BG ≥ 20 mmol/land
symptoms
considerinsulin
glargine o.d.
Discontinue insulin and BG monitoringwhen clinical team and carers agree consequences ofuncontrolled hyperglycaemia are less burdensome
for patient than process of monitoring and injections .
Discontinue OHA and monitor capillary BG o.d. for 2 days
usually need to discontinue oralhypoglycaemic agents
to avoid hypoglycaemia
BG ≥ 20 mmol/lor
BG ≥ 15 mmol/land symptoms
of hyperglycaemia
Consider Restarting OHAat reduced dose.
last weeksof life
final daysof life
orBG < 20 mmol/l
orno symptoms
no OHAor
monitoring required.
Notes: 1. Objectives of care
• To prevent symptomatic hyperglycaemia • To prevent diabetic ketoacidosis (DKA) or hyperosmolar non-ketotic state
(HONK) • To prevent iatrogenic hypoglycaemia • To prevent unnecessarily invasive interventions in the last weeks to days
of life • To recognise that strict glycaemic control and dietary restrictions are
not desirable and aim for blood glucose range 5 – 20 mmol/l.
2. Clinical teams should recognise and communicate with the patient, carers and staff that the patient with diabetes is entering the final weeks or days of their life, so that care and medical management can be planned
3. The consensus clinical guideline to manage diabetes at the end of life is
available on www.avondiabetes.nhs.uk 4. The appropriate clinical guidance should be selected on the patient’s
expected prognosis and diabetes type.
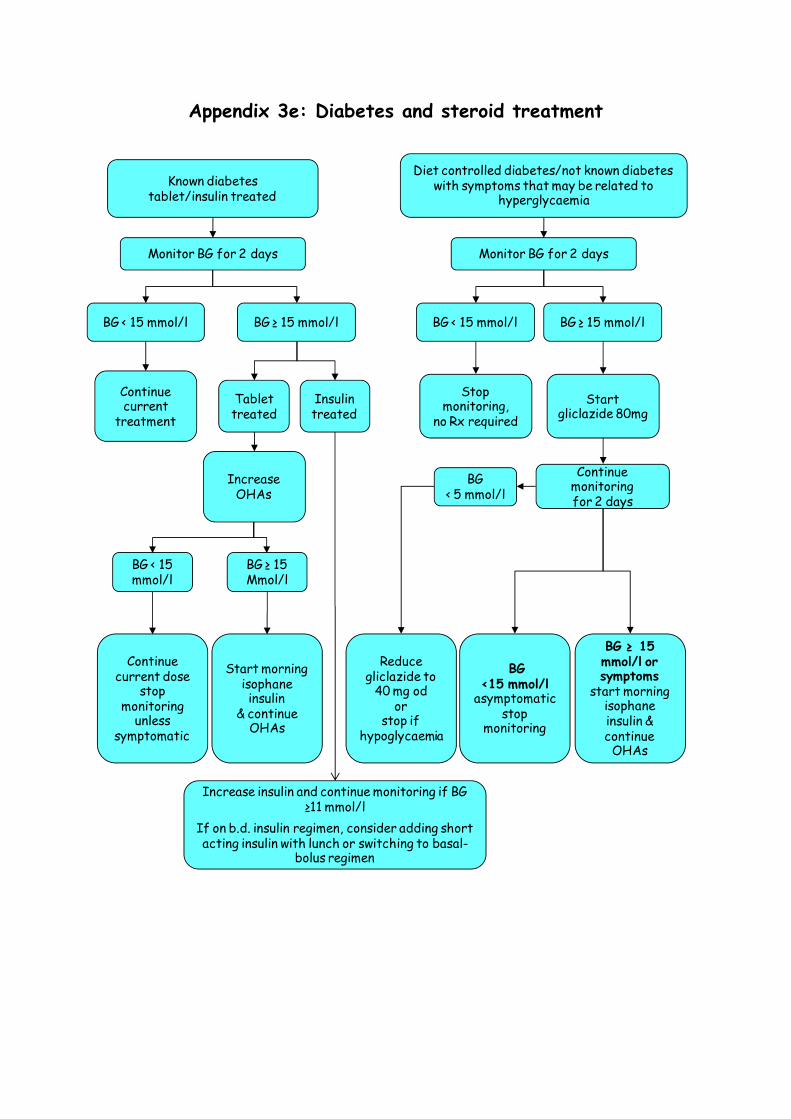
Appendix 3e: Diabetes and steroid treatment
Diet controlled diabetes/not known diabetes with symptoms that may be related to
hyperglycaemia
Monitor BG for 2 days
BG < 15 mmol/l BG ≥ 15 mmol/l
Stop monitoring,
no Rx required Start
gliclazide 80mg
Continue monitoringfor 2 days
BG < 5 mmol/l
Reduce gliclazide to
40 mg odor
stop if hypoglycaemia
BG <15 mmol/l
asymptomatic stop
monitoring
BG ≥ 15mmol/l or symptoms
start morning isophaneinsulin &continue OHAs
Known diabetestablet/insulin treated
Monitor BG for 2 days
BG ≥ 15 mmol/lBG < 15 mmol/l
Tablet treated
Continue current
treatment
Insulin treated
Increase OHAs
BG ≥ 15Mmol/l
BG < 15mmol/l
Continue current dose
stop monitoring
unless symptomatic
Start morning isophaneinsulin
& continue OHAs
Increase insulin and continue monitoring if BG ≥11 mmol/l
If on b.d. insulin regimen, consider adding short acting insulin with lunch or switching to basal-
bolus regimen
Effect of steroids on blood glucose levels
• Steroids induce a state of relative insulin resistance, most patients will not have significantly different FBG but postprandial hyperglycaemia is exaggerated
• BG levels can start to rise within a few days of commencing oral steroids & subside within 48 hours of stopping the medication. Injected steroids may cause BG levels to rise soon after administration & last 3 - 10 days
• Controlling BG levels will improve hyperglycaemic symptoms, reduce the risk of infections and hyperglycaemic emergencies
Managing diabetes and steroid therapy
• Start BG monitoring (BGM) or increase the frequency – check fasting and post-prandial levels for 2 days
• Diet/tablet controlled – if BG ≥ 15mmol/l add gliclazide for people normally controlled on diet alone or with metformin
• If BG remains ≥ 15mmol/l after increasing OHAs, add isophane insulin, initially at breakfast time
• Frail or elderly patients may benefit from other regimens suited to their glucose profile and circumstances contact the community DSN or specialist team for advice if in doubt any of these situations
• Insulin treated – increase insulin if BG ≥ 11mmol/l consider a basal bolus regimen or adding short acting insulin to a bd regimen and adjust as per sick day guidance (www.avondiabetes.nhs.uk)
• Not known to have diabetes but displaying symptoms that may be related to hyperglycaemia, initiate BGM for 2 days and treat as for diabetes if BG ≥ 15mmol/l
General advice
Patients on steroids often have additional causes for the increase in BG level, such as decrease in activity, increased appetite & weight gain
• Follow a healthy eating plan & see a dietitian if indicated
• Refer to DSN for ongoing education and support if indicated
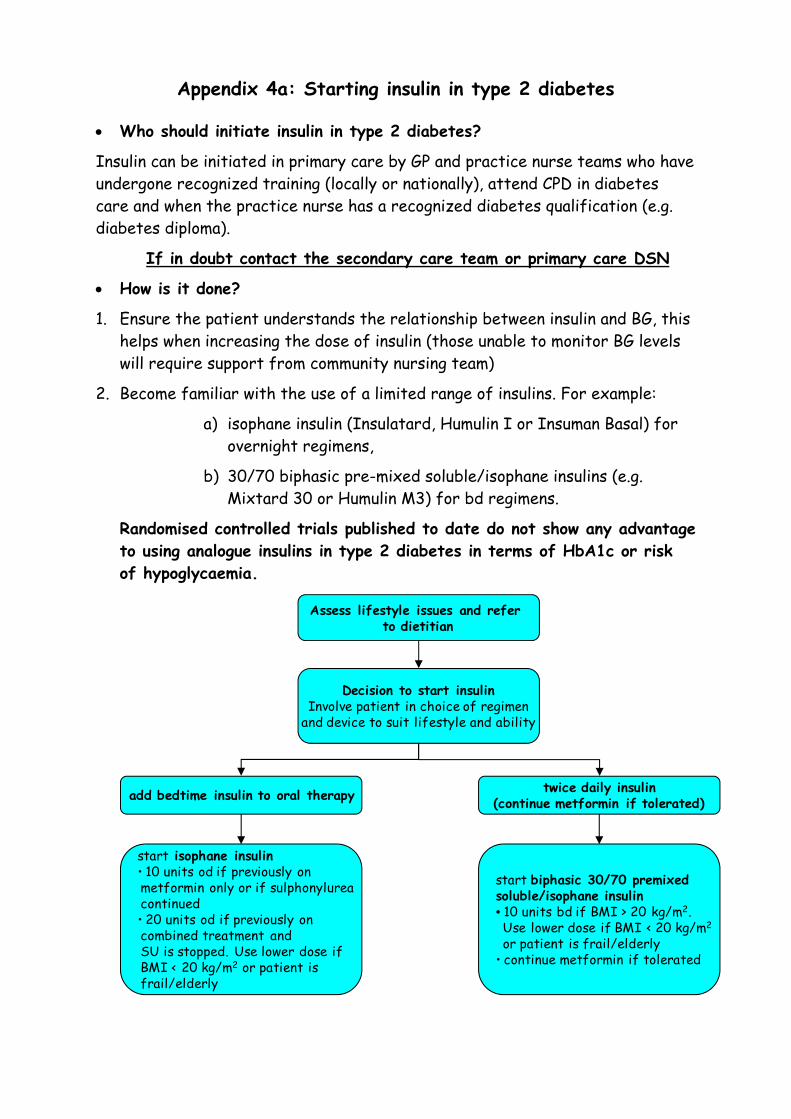
Appendix 4a: Starting insulin in type 2 diabetes • Who should initiate insulin in type 2 diabetes?
Insulin can be initiated in primary care by GP and practice nurse teams who have undergone recognized training (locally or nationally), attend CPD in diabetes care and when the practice nurse has a recognized diabetes qualification (e.g. diabetes diploma).
If in doubt contact the secondary care team or primary care DSN
• How is it done?
1. Ensure the patient understands the relationship between insulin and BG, this helps when increasing the dose of insulin (those unable to monitor BG levels will require support from community nursing team)
2. Become familiar with the use of a limited range of insulins. For example:
a) isophane insulin (Insulatard, Humulin I or Insuman Basal) for overnight regimens,
b) 30/70 biphasic pre-mixed soluble/isophane insulins (e.g. Mixtard 30 or Humulin M3) for bd regimens.
Randomised controlled trials published to date do not show any advantage to using analogue insulins in type 2 diabetes in terms of HbA1c or risk of hypoglycaemia.
twice daily insulin(continue metformin if tolerated)add bedtime insulin to oral therapy
start isophane insulin• 10 units od if previously on metformin only or if sulphonylureacontinued• 20 units od if previously on combined treatment and SU is stopped. Use lower dose if BMI < 20 kg/m2 or patient is frail/elderly
start biphasic 30/70 premixedsoluble/isophane insulin• 10 units bd if BMI > 20 kg/m2. Use lower dose if BMI < 20 kg/m2
or patient is frail/elderly• continue metformin if tolerated
Decision to start insulinInvolve patient in choice of regimen
and device to suit lifestyle and ability
Assess lifestyle issues and refer to dietitian
In general, addition of a single dose of bedtime insulin to oral therapy is only likely to control BG if the patient is asymptomatic and HbA1c <9.5%.
Continue metformin in combination with the insulin if tolerated in order to minimize weight gain. If unable to tolerate metformin, consider switch to modified release or reduced dose.
3. Hypoglycaemia is unlikely because of the nature of type 2 diabetes and the low starting dose – however, patients need to be clear on how to recognize symptoms and what corrective action to take – refer to hypoglycaemia guidelines/patient information sheet available on www.avondiabetes.nhs.uk
4. Implications for DVLA need to be discussed.
5. Telephone support and an emergency contact are needed with regular follow up.
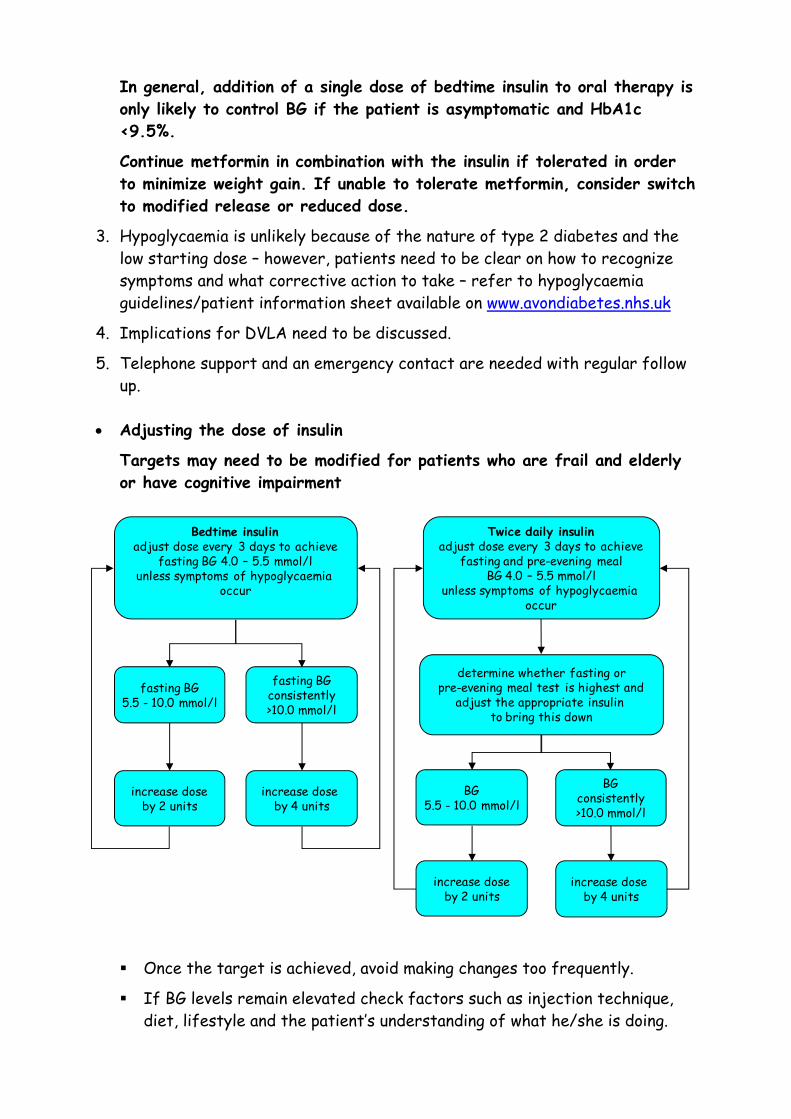
• Adjusting the dose of insulin
Targets may need to be modified for patients who are frail and elderly or have cognitive impairment
Once the target is achieved, avoid making changes too frequently.
If BG levels remain elevated check factors such as injection technique, diet, lifestyle and the patient’s understanding of what he/she is doing.
Bedtime insulinadjust dose every 3 days to achieve
fasting BG 4.0 – 5.5 mmol/lunless symptoms of hypoglycaemia
occur
Twice daily insulinadjust dose every 3 days to achieve
fasting and pre-evening mealBG 4.0 – 5.5 mmol/l
unless symptoms of hypoglycaemia occur
determine whether fasting orpre-evening meal test is highest and
adjust the appropriate insulin to bring this down
fasting BG5.5 - 10.0 mmol/l
fasting BGconsistently>10.0 mmol/l
increase dose by 4 units
increase doseby 2 units
BG5.5 - 10.0 mmol/l
BGconsistently>10.0 mmol/l
increase doseby 2 units
increase dose by 4 units


















