
Diabetes Mellitus Fifth Stage-Medicine Dr. Sarbast Fakhradin MBChB, MSc Diabetes Care & Management.
31
Diabetes Mellitus Fifth Stage-Medicine Dr. Sarbast Fakhradin MBChB, MSc Diabetes Care & Management
-
Upload
gabriel-francis -
Category
Documents
-
view
218 -
download
0
Transcript of Diabetes Mellitus Fifth Stage-Medicine Dr. Sarbast Fakhradin MBChB, MSc Diabetes Care & Management.

Diabetes MellitusFifth Stage-Medicine
Dr. Sarbast Fakhradin
MBChB, MSc Diabetes Care & Management
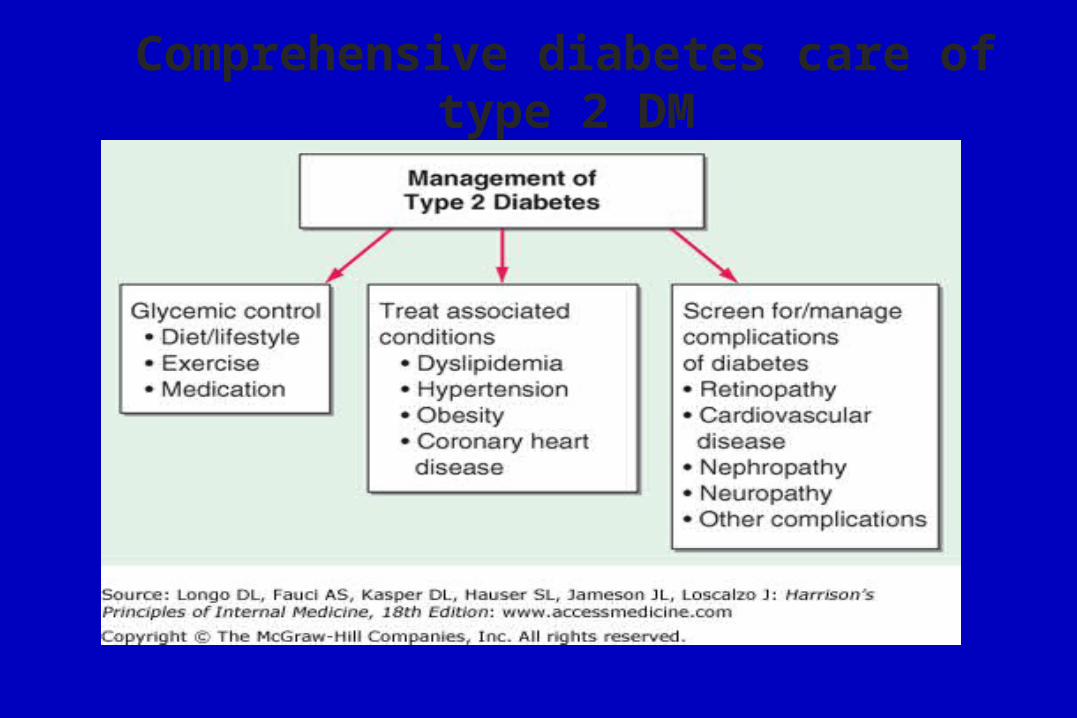
Comprehensive diabetes care of type 2 DM
• Patient education & follow up: DAFNE & DESMOND
– It is essential that people with diabetes understand their
disorder and learn to handle all aspects of their management &
educating patients about diabetes complications.
– Carry a diabetic card stating their name and address.
– Driving
• Patient education & follow up: DAFNE & DESMOND
Blood glucose monitoring;Target Preprandial capillary plasma glucose (70-130 mg/dl)
Target postprandial capillary plasma glucose (< 180 mg/dl)
• A. Treatment with insulin;
• Regular BG monitoring should be performed by all patients to adjust the insulin dose and detect hypoglycaemia
• Daily pre-prandial and bedtime measurements are usually recommended
• Treatment with oral hypoglycemic agents;• BG monitoring is optional in many patients with stable type 2 diabetes.
• Monitoring is most useful in patients taking sulphonylureas, during intercurrent illness and prescription of corticosteroids, and during changes in therapy.
– Lower limbs & feet
– Blood pressure < 130/80
– Smoking & alcohol
– Hypoglycemic episodes.
– Psychological support
– Target Lipid profile: Cholesterol< 200mg/dl,
– LDL < 100 mg/dl,
TG < 150 mg/dl
HDL> 40 mg/dl.

Lifestyle modification• 1. Healthy diet• 2. Regular Exercise: in the form of walking, gardening,
swimming or cycling, approximately 30 minutes daily, as this improves insulin sensitivity and the lipid profile and lowers blood pressure.
• 3. Stop smoking• 4. Reduce/stop alcohol intake• 5. Salt: reduce sodium intake to no more than 6 g daily.
• The glycaemic index (GI) of a carbohydrate-containing food is a measure of the change in blood glucose following its ingestion. Consumption of foods with a low GI is encouraged.
• All the CHO prescribed should be taken in the form of starches and other complex sugars.
• Fiber- rich foods (e.g barley, oats, legumes, beans & lentils) has been associated with improved blood glucose control & lower blood lipids in both normal, diabetic & hyperlipidemic persons.
• Low-calorie and sugar-free drinks are useful for patients with diabetes. These drinks usually contain non-nutritive sweeteners. Many 'diabetic foods' contain sorbitol, are expensive and high in calories, and may cause gastrointestinal side-effects. As a result, these foods are not recommended as part of the diabetic diet.

• Recommended composition of diet for people with diabetes:
• CHO 40-65%
• Fat < 35% ( saturated <10%)
• Protein 10-15%
• Fruit/Vegetable 5 portions daily

Anti-Diabetic Medications • Oral Agents:1. Biguanides (Metformin)
2. Insulin Secretagogues – Sulphonylureas (Gliclazide)
3.Insulin Secretagogues – Non-sulphonylureas (Repaglinide)
4. DPP4 inhibitor (Sitagliptin)
5. α-glucosidase inhibitors (Acarbose)
6. Thiazolidinediones (TZDs) (Pioglitazone)
• Injections:• 1. Insulin
• 2. GLP-1 agonist (Incretin mimetic) Exenatide & Liraglutide
Biguanides (Metformin) First drug of choice for obese patients in whom strict dieting has
failed to control type 2 diabetes.
• Insulin sensitivity and peripheral glucose uptake are increased,
• Impairs glucose absorption by the gut and inhibits hepatic
gluconeogenesis
• It does not increase insulin secretion and seldom causes
hypoglycaemia.
• Metformin is given with food.
Biguanides (Metformin)• Glucose-lowering effect of metformin is synergistic with that of
sulphonylureas.
• Improves lipid profiles & reduces risk of CA.
• SE: Dyspepsia, Risk of lactic acidosis: contraindicated in patients with
impaired renal or hepatic function, drinking alcohol in excess, hypoxia, &
shock.
• Not contraindicated in pregnancy.

SULPHONYLUREAS • Mainly for people with type 2 diabetes who are not overly obese.
• First Generation: Tolbutamide (well tolerated, short acting, useful in
elderly), Chlorpropamide Very long acting (up to 60 hours), avoid in
elderly.
• Second generation: Glibenclamide, Gliclazide, Glimepiride, Glipizide.
• Glibenclamide is prone to induce severe hypoglycaemia (avoid in the
elderly)
• Principally stimulate production of insulin, may reduce glucagon levels.

SULPHONYLUREAS • SUs can cause hypoglycaemia and their use should therefore be closely
monitored in the elderly & in those with nephropathy.
• Several drugs can potentiate their hypoglycaemic effect (e.g. salicylates,
phenylbutazone and antifungal agents)
• SE: Hypoglycemia, increased appetite and weight gain, skin rashes
(hypersensitivity) and G.I. Disturbances, cholestatic Jaundice, blood
dyscrasia. Feature of disulfiram- like reaction occur in some patients
after taking alcohol.
• Occasionally chlorpropamide can induce (SIADH).
Meglitinides - prandial glucose regulators
• Repaglinide, Nateglinide
• Stimulates insulin release (rapid and short acting)
• Better control of postprandial hyperglycaemia
• Take before meals.
• It is less likely to cause hypoglycaemia than sulphonylureas.
Alpha-glucosidase inhibitors (Acarbose)
• Carbohydrate digestion in the small intestine is slowed down by
selectively inhibiting disaccharidases
• Glucose is not absorbed into the bloodstream so quickly.
• SE: Bloating, flatulence, diarrhoea and abdominal pain, especially
upon initial treatment.
Thiazolidinediones (pioglitazone) • Bind and activate peroxisome proliferator-activated receptor-γ
(PPARγ agonists).
• Reduced insulin resistance and decreased insulin levels
• insulin concentrations are not increased & hypoglycemia is not a
problem.
• Fat redistribute from the abdominal stores and into subcutaneous
depots. However, body weight and total body fat are increased.
• Pioglitazone may reduce myocardial infarctions and strokes
(improvement in endothelial function), but increase the risk of HF?
Thiazolidinediones (pioglitazone) • SE: sodium and fluid retention, which is aggravated if they are
combined with insulin, upper limb fractures.
• TZDs must be avoided in patients with cardiac failure, hepatic
impairment or severe renal insufficiency.
• Increase LDL (non-atherogenic form?), increased HDL, lowered
FFA, lowered triglycerides.
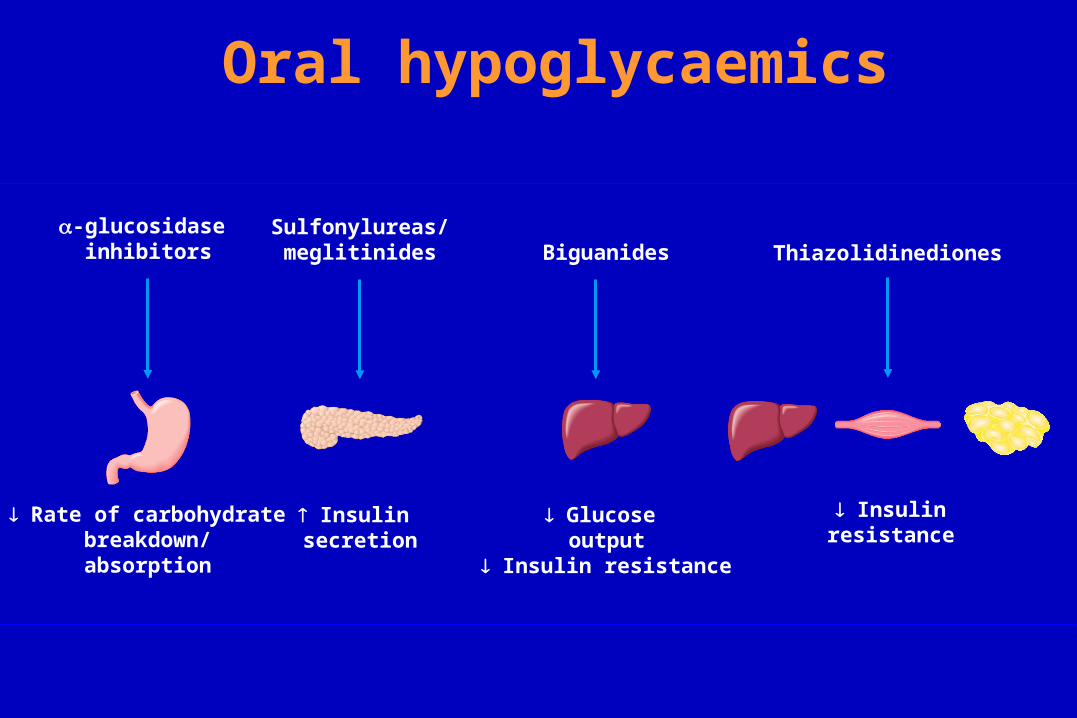
Oral hypoglycaemics
Glucose output
Insulin resistance
Biguanides
Insulin secretion
Sulfonylureas/meglitinides
Rate of carbohydrate breakdown/absorption
-glucosidase inhibitors
Insulin resistance
Thiazolidinediones
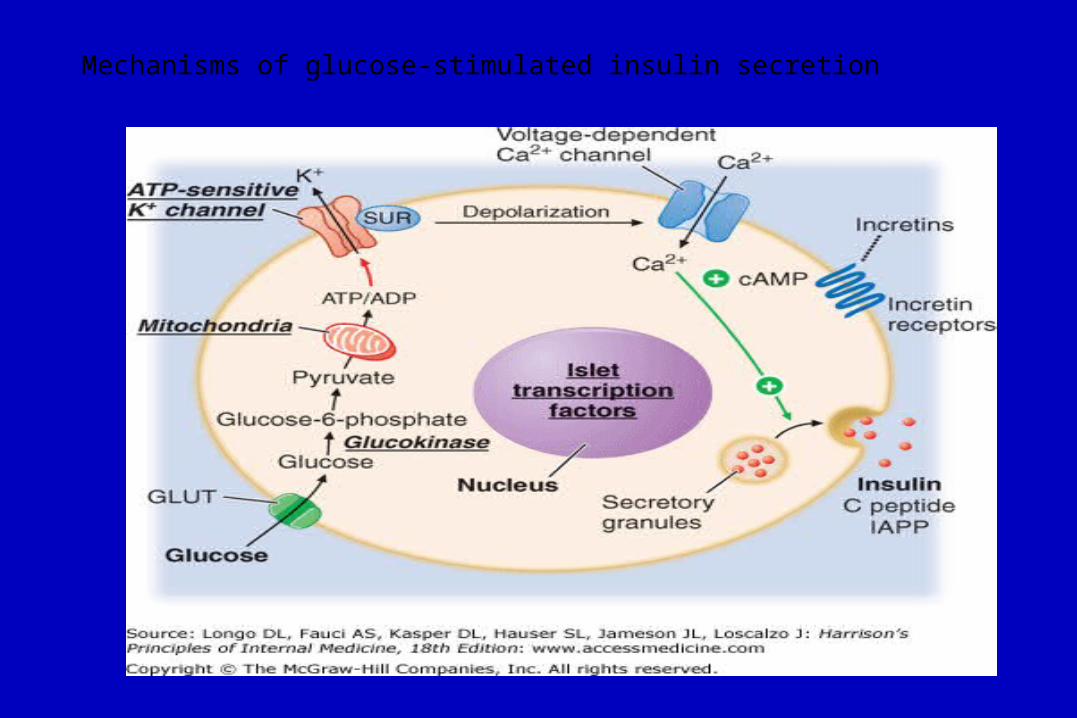
Mechanisms of glucose-stimulated insulin secretion
Incretin-based therapies
•The secretion of insulin in response to a rise in blood glucose is
greater when glucose is given by mouth than by intravenous infusion.
In part this is caused by secretion of gut hormones, or incretins
(Glucagon-like peptide (GLP-1), which potentiate glucose-induced
insulin secretion.
•GLP-1 suppresses glucagon secretion, delays gastric emptying,
reduces appetite and encourages weight loss.

Incretin-based therapies (Cont.)
•They improve postprandial glucose excursions and early satiety
•GLP-1 is rapidly degraded by the enzyme, dipeptidyl peptidase 4,
inhibitors of this enzyme can be used to prolong its biological effect.
•The DPP-4 inhibitors or gliptins (sitagliptin, vildagliptin and
saxagliptin) are oral agents which act in this manner.
Incretin-based therapies (Cont.)
•Exenatide & Liraglutide (SC injection) are Synthetic GLP-1
receptor antagonists with longer therapeutic action. They induce
weight loss in most patients. SE: pancreatitis & GI disturbance.
•Incretin-based therapies are most useful in obese patients and can be
used in combination with other oral anti-diabetic agents.
Insulin• Insulin are either bovine or porcine, human insulin produced by
recombinant DNA technology & protein engineering technique.
• In most countries, the insulin concentration in available formulations has
been standardised at 100 U/mL.
• Plastic Syringe or pen injector.
• Insulin is usually given by the SC route, IV or IM routes.
• Rotation of injection sites is recommended to reduce insulin injection
site damage.

Insulin (Cont.)• It is removed mainly by the liver and also the kidneys; plasma
insulin concentrations are elevated in patients with liver disease or
renal failure.
• Absorption from the abdomen is faster than from thighs or upper
arms and may be preferred for short- acting preparation.
• Insulin absorption may be influenced by insulin formulation,
injection site, depth and volume of injection, skin temperature
(warming), local massage and exercise.
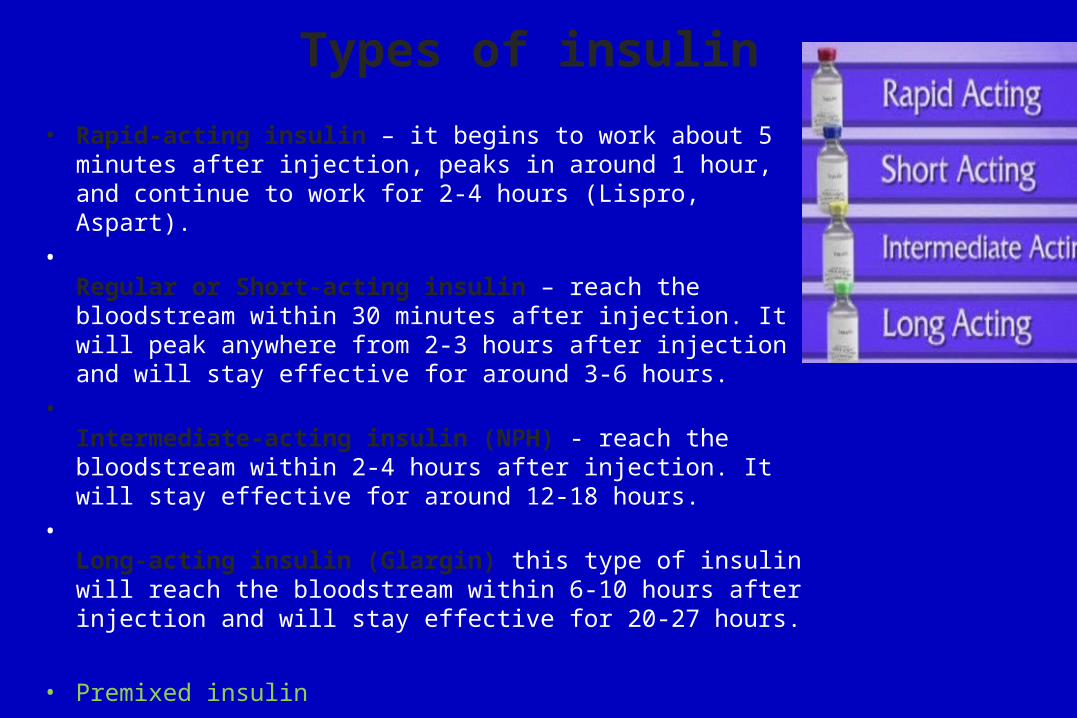
Types of insulin
• Rapid-acting insulin – it begins to work about 5 minutes after injection, peaks in around 1 hour, and continue to work for 2-4 hours (Lispro, Aspart).
•Regular or Short-acting insulin – reach the bloodstream within 30 minutes after injection. It will peak anywhere from 2-3 hours after injection and will stay effective for around 3-6 hours.
•Intermediate-acting insulin (NPH) - reach the bloodstream within 2-4 hours after injection. It will stay effective for around 12-18 hours.
•Long-acting insulin (Glargin) this type of insulin will reach the bloodstream within 6-10 hours after injection and will stay effective for 20-27 hours.
• Premixed insulin
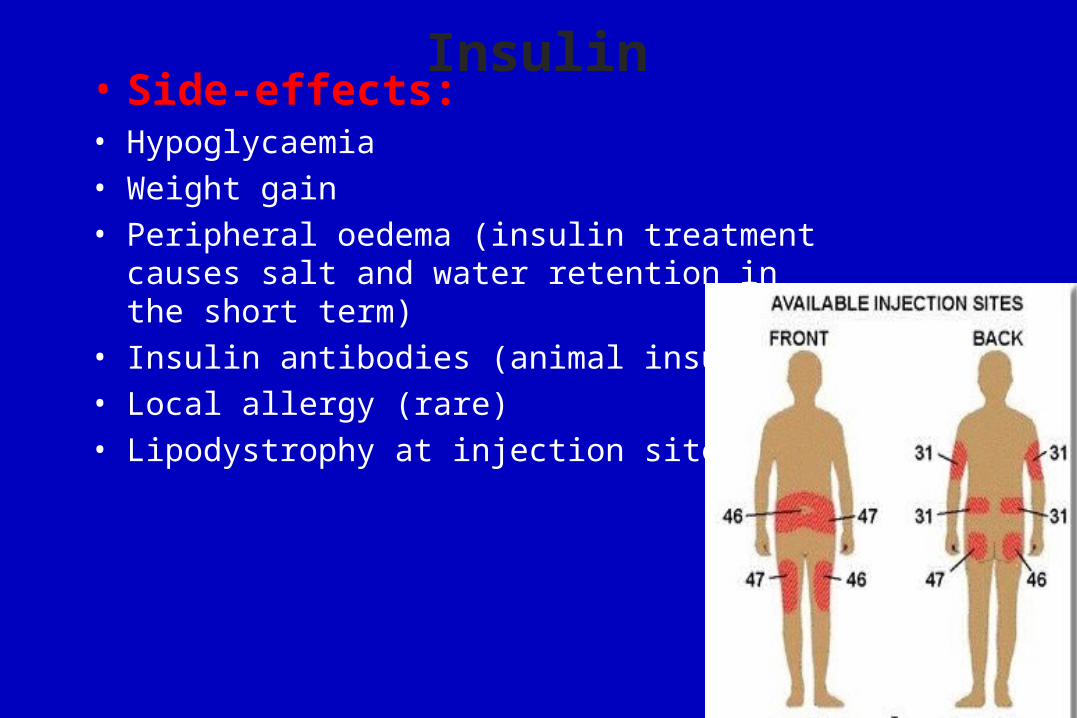
Insulin• Side-effects:• Hypoglycaemia
• Weight gain
• Peripheral oedema (insulin treatment causes salt and water retention in the short term)
• Insulin antibodies (animal insulins)
• Local allergy (rare)
• Lipodystrophy at injection sites
Insulin dosing regimens• Most people require two or more injections of insulin daily.
• Once-daily injections rarely achieve satisfactory glycaemic control & are
reserved either for some elderly patients or for those who retain substantial
endogenous insulin secretion & have a low insulin requirement.
• Twice- daily mixtures of short- and intermediate acting insulin is a commonly
used regimen.
• Basal-Bolus: A regimen of multiple injection of short- acting insulin before the
main meals, with an appropriate dose of single daily intermediate- or long
acting insulin.
• The dose of the insulin preparations is adjusted according to frequent
monitoring of blood glucose levels. Blood glucose monitory should be
intensified during intercurrent illness & other stressful conditions (Sick Day
rule)

• Combined oral anti-diabetic therapy and insulin • In patients with type 2 diabetes who are requiring increasing doses
of oral anti-diabetic drugs, the introduction of a single dose of an intermediate- (e.g. isophane) or long-acting insulin analogue, administered at bedtime, may improve glycaemic control and delay the development of overt pancreatic β-cell failure.
• Insulin Pump• Transplantation• Surgery


Thank YouQuestion?


















