Diabetes Management in the Wards - Home - WSLHD
46
Prescribing Insulin in the Wards N Wah Cheung Dept of Diabetes & Endocrinology
Transcript of Diabetes Management in the Wards - Home - WSLHD

Prescribing Insulin in the Wards
N Wah Cheung Dept of Diabetes & Endocrinology

Why is glucose management important? Insulins and regimens How to chart insulin Supplemental Insulin How to get a diabetes consult Treatment targets and how to adjust insulin Hypos and hyperglycaeima

Diabetes in Hospital 20-40% of inpatients have diabetes Illness, medications, feeds and procedures cause
unstable diabetes or stress hyperglycaemia Increased risk of hypoglycaemia Poor diabetes control affects patient outcomes - impaired wound healing - lower resistance to infection - worse outcomes from AMI - longer LOS - increased mortality

General Principles Identify patients with diabetes: Distinguish T1 from T2 Identify the patients’ usual diabetes medication Ascertain usual level of diabetes control: HbA1c Anticipate problems with BSL control - fasting - infection - medication (eg steroids) Expect that things will change - be proactive rather than reactive Ensure BGLs are measured (minimum fasting and 2 hrs
post meals. Before meals and 0200-0300 also helpful)

Insulin Errors NSW IIMS Reports Jan-Jun 2009
33% of the medical errors that caused death within 48 hours of the error involved insulin Hellman Endo Pract 2004

Current Anti-Diabetes Agents Oral Agents
Metformin Sulphonylureas (eg Gliclazide MR, Glimeperide)
Glitazones (eg Pioglitazone)
α-glucosidase inhibitors (eg Acarbose)
DPP IV inhibitors (eg Sitagliptin, Vildagliptin, Linagliptin, Saxagliptin)
SGLT2 inhibitors (eg Dapagliflozin, Empagliflozin, Ertugliflozin)
Combinations
Non-insulin injectables GLP1 Analogues (eg Exenatide, Dulaglutide, Liraglutide)
Insulin

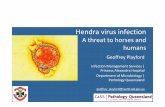
Insulin Pharmacokinetics
Rapid Analogues Novorapid, Humalog, Apidra
Short Acting Actrapid, Humulin R
Intermediate Acting Protaphane, Humulin NPH
Long Acting Levemir, Lantus
Ultra Long Acting Degludec
1 2 3 4 6 8 24 42
Usually given before meals: PRANDIAL or BOLUS
Usually given at bedtime or bd: BASAL

Pre-mixed Insulins Rapid/short acting + intermediate acting
Rapid + Intermediate Rapid + Intermediate 25-30 : 75-70 50 : 50 Eg Novomix 30, Humalog Mix 25
Mixtard 30/70
Humalog Mix 50
Usually given twice daily
Rapid/short acting + ultra long acting Ryzodeg (Aspart + Degludec, 30 : 70)
Usually once or twice daily

Insulin Regimens Basal bolus insulin [preferred in hospital]
NOT sliding scale insulin Insulin infusions [preferred for fasting, mandatory for
T1DM when fasting or DKA]
Bd Premixed insulin- OK if is usual regimen + satisfactory BGs
Basal Insulin only – often with OHAs
Insulin pumps (T1 Diabetes)
Unstable or Stable Patients
Stable Patients
Need Endo team involvement

MN 0600 1200 1800
BSL
Rapid Rapid Rapid Basal
Principles of Basal Bolus Insulin

Basal Bolus Insulin Initiation
Total daily dose 0.5 units/kg/day Reduce to 0.2-0.4 units/kg /day if kidney disease, liver disease, elderly, poor intake, metformin, recurrent hypoglycemia, or other risk factors for hypoglycemia
50% basal + 50% prandial Add supplemental rapid acting insulin TDS ONLY ie at same time as standard prandial insulin May continue Metformin but generally stop other oral agents
If on premixed insulin Adjust from premixed dosage
Adjust from daily dosage If on insulin infusion
Bedtime Long acting Lantus
Rapid acting in 3 divided meal doses Novorapid
If new to insulin
Preferred regimen for unstable patients

Do the following insulin regimens make sense?
i) Protaphane and Novorapid TDS with meals ii) Novorapid TDS with meals and Lantus at
bedtime Mixtard 30/70 TDS iii) Humalog BD iv) Lantus at bedtime with gliclazide BD v) Novomix 30 BD
√
√ √
x
x x √

Subcutaneous Insulin And Blood Glucose Chart

Subcutaneous Insulin Chart The Subcutaneous Insulin Chart is a separate chart
to the National Inpatient Medication Chart. All subcutaneous insulin to be prescribed on SIC IV insulin on iv orders chart Oral anti-hyperglycaemic drugs on the NIMC Glucose monitoring on SIC if patient on insulin, on
BG monitoring chart if not, SAGO chart if not diabetic
https://www.aci.health.nsw.gov.au/resources/endocrine/subcut-insulin/subcut-insulin

REGULAR DOSE
Chart insulin dose daily
“Units” preprinted
BG Monitoring
Order BG Monitoring


Mrs Annie Smith 53 year old woman admitted with cellulitis Type 2 diabetes 74 kgs Medications: Novorapid 8 units tds Lantus 16 units nocte Metformin 1g bd
No allergies
Chart the regular insulin for her
Annie Smith MRN 0950099 DOB 15/6/1965 12 John St, Westmead 2145


What do we do with unexpected high readings?
Sliding Scale Insulin
Adjust usual insulin and add
Supplemental Insulin

Used in addition to regular subcutaneous insulin to correct and prevent hyperglycaemia.
Not to be used alone.
The MO must prescribe the type of insulin and the Administration Time (Usually given before meals)
Supplemental Scale

Supplemental Scale Use Rapid Acting (Novorapid, Humalog, Apidra)
Standard Insulin Resistant BSLs 10.1-12mmol/l 2 Units 4 Units BSLs 12.1-18mmol/l 4 6 BSL 18.1-20mmol/l 6 8 >20 mmol/l Call RMO
in addition to usual sc insulin ideally before meals.

Mrs Annie Smith You review her recent BGs and they have
intermittently been in the mid teens.
Concerned about possibility of high BGs this evening, you chart a supplemental scale
Chart supplemental insulin for her


Diabetes Consult

Diabetes Consult

Diabetes Consult


Resources Inpatient Diabetes Management Service (surgical patients): Diabetes Registrar Others: Endocrine Registrar Consult early, not on the day of discharge Diabetes Educators - BSL monitoring - insulin administration - general education & support Subcutaneous Insulin Chart My Health Learning Thinksulin

My Health learning

Thinksulin

Treatment targets A high BGL is not normal for a person with diabetes “Normal” glucose 4 - 8 mmol/L
In hospital Aim for BGL <10 mmol/L Do not aim to get BG below 5 mmol/L As a general target aim for 5-10 mmol/L. Not hypo until <4 mmol/L
Patients on oral agents may require insulin in hospital Patients on b.d. insulin may require basal bolus insulin

Adjusting insulin doses - 1
Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 12.4
12 9.8 15.2

Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 13.4
12 8 12 20 10.8 15.2
16

Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 13.4
12 8 12 20 10.8 15.2 13.3 12.8 8.9 9.2
16 12 13

Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 13.4
12 8 12 20 10.8 15.2 13.3 12.8 8.9 9.2
16 8 12 24 12 13
16

Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 13.4
12 8 12 20 10.8 15.2 13.3 12.8 8.9 9.2
16 8 12 24 12 13 10.1 9.5 7.6 8.0
16 8.2 4.1

Novorapidac breakfast
Novorapid ac lunch
Novorapid ac dinner
Lantus bedtime
fasting pc breakfast
ac lunch
pc lunch
ac dinner
pc dinner
8 8 8 16 10 12.1 9.5 8 8.6 13.4
12 8 12 20 10.8 15.2 13.3 12.8 8.9 9.2
16 8 12 24 12 13 10.1 9.5 7.6 8.0
16 8 12 24 8.2 4.1
14

The fasting patient
Diet alone or on small doses of anti-hyperglycaemia tablets may require no specific treatment
Patients on large doses of oral agents or insulin Brief procedures (eg gastroscopy, D&C): schedule first in
morning – may require no specific treatment Longer procedures or later in day – insulin/dextrose infusion Prolonged NBM (eg abdominal surgery): generally maintain
insulin/dextrose infusion

Annie Smith MRN 0950099 DOB 15/6/1965 12 John St, Westmead 2145
Chart Annie’s iv insulin


Upon Discharge Revert back to pre-admission diabetes
medication and doses if patient was previously well controlled and returned to pre-morbid state.
Needs follow-up if control previously poor and/or changed treatment to be continued.
Insulin doses usually need reducing if tight control established in hospital.

Mrs Annie Smith Patient now ready for discharge She has been on Novorapid 12 units mane, 8 units midi, 14 units nocte
(before meals) Lantus 20 units bedtime
Because she will be more active on discharge, you decide to
reduce her Novorapid by 2 units for each dose. She will be using a flexpen.
Write her discharge script, and an external prescription
Annie Smith MRN 0950099 DOB 15/6/1965 12 John St, Westmead 2145


Hypoglycaemia

Sudden severe hyperglycaemia (eg >20) Immediate management Type 1 diabetes: check for ketones Can prescribe supplemental insulin But Is there a pattern of high BGL?
- if so, fix the regular treatment
Why has it occurred? Possible reasons: - missed dose - sugar intake - infection

SGLT-2 Inhibitors and Surgery Recent reports of DKA As precaution, cease 3 days prior to surgery Ensure insulin dextrose infusion for surgery Check ketones pre-op post-op If ketones ≥1.5, check VBGs (HCO3 and pH) Resume SGLT-2 inhibitor only when eating
normally again In meantime need alternative means of
controlling hyperglycaemia