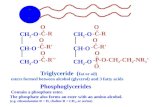
Diabetes and Lipids - Amazon Simple Storage Service · •Does glycemic control matter wrt...
136
Diabetes and Lipids
Transcript of Diabetes and Lipids - Amazon Simple Storage Service · •Does glycemic control matter wrt...

Diabetes and Lipids

Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be
reproduced, copied, stored, or transmitted in any form
or by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information
storage and retrieval systems without prior written
permission of Sea Courses Inc. except where
permitted by law.
Sea Courses is not responsible for any speaker or
participant’s statements, materials, acts or omissions.


•Should we be checking LDL (or other lipid fractions)?
•What is the normal range?•Is there an upper limit to the range?•Is there a lower limit to the range?•What are the targets in people with diabetes? What should the targets be?
•Is the cholesterol hypothesis proven?•Hypothesis or fact?
With respect to (LDL) cholesterol….

Learning objectives:• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Small interfering RNA
• Etc…..

Learning objectives:• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Small interfering RNA
• Etc…..



Slide Source:
Lipids Onlinewww.lipidsonline.org
1.0
0.9
0.8
0.7
0.6
0.5
0
Proportion w
ithout
Majo
r CH
D E
vent
Years Since Randomization
0 1 2 3 4 5 6
Adapted from Pyörälä et al. Diabetes Care 1997;20:614-620.
Diabetes by Hx, simvastatin
Diabetes by Hx, placebo
No diabetes by Hx, simvastatin
No diabetes by Hx, placebo
P=0.002
P=0.0001
Major Coronary Events in 4S Patients with Major Coronary Events in 4S Patients with
or without Diabetes by History (n=202)or without Diabetes by History (n=202)

placebo
Atorva 10
CARDS

TNT: Diabetes Subgroup

With DMThere is no question that treating diabetics
with statins lowers CV risk.

With DMThe resulting lower risk achieved still
exceeds non-diabetics

With DMThere does not seem to be a LDL below
which risk does not continue to drop

Learning objectives:
• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Etc…..

Should every diabetic be treated with a statin?

USA guidelines: how do they compare?

• ≥40 yrs old or
• Macrovascular disease or
• Microvascular disease or
• DM >15 yrs duration and age >30 yrs or
• Warrant therapy based on (other) Canadian
Cardiovascular Society lipid guidelines
2013Who Should Receive Statins?
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association

If on therapy, target
LDL ≤2.0 mmol/L
(77.2 mg/dL)

Slide 21

Slide 22

USA guidelines: how do they compare?

24

25
A New Perspective on LDL-C and Non-HDL-C goals
“The expert panel was unable to find RCT evidence
to support continued use of specific LDL-C and/or
non-HDL-C treatment targets”

Slide Source:
Lipids Onlinewww.lipidsonline.org
1.0
0.9
0.8
0.7
0.6
0.5
0
Proportion w
ithout
Majo
r CH
D E
vent
Years Since Randomization
0 1 2 3 4 5 6
Adapted from Pyörälä et al. Diabetes Care 1997;20:614-620.
Diabetes by Hx, simvastatin
Diabetes by Hx, placebo
No diabetes by Hx, simvastatin
No diabetes by Hx, placebo
P=0.002
P=0.0001
Major Coronary Events in 4S Patients with Major Coronary Events in 4S Patients with
or without Diabetes by History (n=202)or without Diabetes by History (n=202)

CARDS
placebo
Atorva 10

NEJM 350;15 April 8 2004

TNT: Diabetes Subgroup

30
A New Perspective on LDL-C and Non-HDL-C goals
“The expert panel was unable to find RCT evidence
to support continued use of specific LDL-C and/or
non-HDL-C treatment targets”
“… 4 major statin benefit groups were identified for
whom the ASCVD risk reduction clearly outweighs
the risk of adverse events….3) diabetes aged 40-75
years with LDL-C 70-189 mg/dl and without ASCVD”

31
A New Perspective on LDL-C and Non-HDL-C goals
“The expert panel was unable to find RCT evidence
to support continued use of specific LDL-C and/or
non-HDL-C treatment targets”
“… 4 major statin benefit groups were identified for
whom the ASCVD risk reduction clearly outweighs
the risk of adverse events….3) diabetes aged 40-75
years with LDL-C 1.75 – 4.72 mmol/L and without
ASCVD”

• “The difficulty of giving up the treat to goal paradigm was deliberated extensively over a 3-year period”
• “Use of LDL-C targets may result in
– under-treatment with evidence based statin therapy

33


Mr. M. S., age 58, diabetic
TC: 4.0 mmol/L (155 mg/dl)
HDL: 1.1 mmol/L (42 mg/dl)
LDL: 2.4 (96 mg/dl)
Triglyceride: 2.2 mmol/L (200 mg/dl)
A1c: 6.9%
Are his lipids optimally controlled?
Should you add more statin?
Would more information help?
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Scenario 1

Mr. M. S., age 58, diabetic
TC: 4.0 mmol/L (155 mg/dl)
HDL: 1.1 mmol/L (42 mg/dl)
LDL: 2.4 (96 mg/dl)
Triglyceride: 2.2 mmol/L (200 mg/dl)
A1c: 6.9%
Are his lipids optimally controlled?
Should you add more statin?
Would more information help?
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Scenario 1

Mr. M. S., age 58, diabetic
TC: 4.0 mmol/L (155 mg/dl)
HDL: 1.1 mmol/L (42 mg/dl)
LDL: 2.4 (96 mg/dl)
Triglyceride: 2.2 mmol/L (200 mg/dl)
A1c: 6.9%
Are his lipids optimally controlled?
Should you add more statin?
Would more information help?
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Scenario 1

39

Mr. M. S., age 58, diabetic
TC: 4.0 mmol/L (155 mg/dl)
HDL: 1.1 mmol/L (42 mg/dl)
LDL: 2.4 (96 mg/dl)
Triglyceride: 2.2 mmol/L (200 mg/dl)
A1c: 6.9%
Are his lipids optimally controlled?
Should you add more statin?
Would more information help?
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Scenario 1

41
Mr. M. S., age 58, diabetic
TC: 3.75 mmol/L (150 mg/dl)
HDL: 1.24 mmol/L (49.6 mg/dl)
LDL: 1.7 mmol/L (68 mg/dl)
Triglyceride: 1.55 mmol/L (141 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 20 mg.
Are his lipids optimally controlled?
Scenario 2

42
Mr. M. S., age 58, diabeticMeds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 20 mg. Had an MI 6 mos ago
Are his lipids optimally controlled?
Scenario 3
TC: 3.75 mmol/L (150 mg/dl)
HDL: 1.24 mmol/L (49.6 mg/dl)
LDL: 1.7 mmol/L (68 mg/dl)
Triglyceride: 1.55 mmol/L (141 mg/dl)
A1c: 6.9%

43
Mr. M. S., age 58, diabetic
TC: 2.4 mmol/L (95 mg/dl)
HDL: .9 mmol/L (35 mg/dl)
LDL: 1.0 mmol/L (39 mg/dl)
Triglyceride: 1.1 mmol/L (100 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago
Are his lipids optimally controlled?
Scenario 4

44
Mr. M. S., age 58, diabetic
TC: 2.4 mmol/L (95 mg/dl)
HDL: .9 mmol/L (35 mg/dl)
LDL: 1.0 mmol/L (39 mg/dl)
Triglyceride: 1.1 mmol/L (100 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago
Are his lipids optimally controlled?
Would you decrease the statin?
Scenario 4

45
Mr. M. S., age 58, diabetic
TC: 2.4 mmol/L (95 mg/dl)
HDL: .9 mmol/L (35 mg/dl)
LDL: 1.0 mmol/L (39 mg/dl)
Triglyceride: 1.1 mmol/L (100 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago
Are his lipids optimally controlled?
Would you decrease the statin?
Would LESS information help?
Scenario 4

46
Mr. M. S., age 58, diabetic
TC: 2.4 mmol/L (96mg/dl)
HDL: .9 mmol/L (36 mg/dl)
LDL: 1.0 mmol/L (40mg/dl)
Triglyceride: 1.1 mmol/L (100 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago
Scenario 4
Are his lipids optimally controlled?
Would you decrease the statin?
Would LESS information help?

• “The difficulty of giving up the treat to goal paradigm was deliberated extensively over a 3-year period”
• “Use of LDL-C targets may result in
– under-treatment with evidence based statin therapy

Media, internet, print, etc

Learning objectives:
• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Etc…..


IMProved Reduction of Outcomes: Vytorin Efficacy International Trial
A Multicenter, Double-Blind, Randomized Study to
Establish the Clinical Benefit and Safety of Vytorin
(Ezetimibe/Simvastatin Tablet) vs Simvastatin
Monotherapy in High-Risk Subjects Presenting
With Acute Coronary Syndrome

53
Patients stabilized post ACS ≤ 10 days:
LDL-C 1.3-3.2 mmol/L (1.3–2.6 mmol/L if prior lipid-lowering Rx)
Standard Medical & Interventional Therapy
Ezetimibe / Simvastatin
10 / 40 mg
Simvastatin
40 mg
Follow-up Visit Day 30, every 4 months
Duration: Minimum 2 ½-year follow-up (at least 5250 events)
Primary Endpoint: CV death, MI, hospital admission for UA,
coronary revascularization (≥ 30 days after randomization), or stroke
N=18,144
Uptitrated to
Simva 80 mg
if LDL-C > 2.05
(adapted per
FDA label 2011)
Study Design
Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12
90% power to detect
~9% difference

54
LDL-C and Lipid ChangesM
ean
LD
L-C
(m
mol/
L)
1.0
1.25
1.5
1.75
2.0
2.25
2.5
QE R 1 4 8 12 16 24 36 48 60 72 84 96
Time since randomization (months)Number at risk:
1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 1.81 3.75 1.55 1.24 3.8 mg/dl
EZ/Simva 1.38 3.25 1.36 1.26 3.3 mg/dl
Δ in mmol/L -0.43 -0.50 -0.19 +0.2 -0.5mg/dl

55
LDL-C and Lipid ChangesM
ean
LD
L-C
(m
mol/
L)
1.0
1.25
1.5
1.75
2.0
2.25
2.5
QE R 1 4 8 12 16 24 36 48 60 72 84 96
Time since randomization (months)Number at risk:
1 Yr Mean LDL-C TC TG HDL hsCRP
Simva 70 145 1.55 1.24 3.8 mg/dl
EZ/Simva 53 126 1.36 1.26 3.3 mg/dl
Δ in mg/dl -17 -19 -0.19 +0.2 -0.5mg/dl

56
Simva — 22.2%
1704 events
EZ/Simva — 20.4%
1544 events
HR 0.90 CI (0.84, 0.97)
p=0.003
NNT= 56
CV Death, Non-fatal MI, or Non-fatal Stroke
7-year event rates

Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015

Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015Unpublished
Cannon CP, et al. N Engl J Med. 2015;372:2387-2397. Supplementary Appendix.

Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015
Cannon CP, et al. N Engl J Med. 2015;372:2387-2397. Supplementary Appendix.


LDL Receptor Function and Life Cycle
61 61
For illustration purposes only

The Role of PCSK9 in the Regulation of LDL Receptor Expression
62
For illustration purposes only

Impact of PCSK9 inhibitors on LDL Receptor Expression
63 63
For illustration purposes only

-8.5% (2.9)
-13.5%(3.2)
-8.6%(2.9)
-14.0%(4.2)
-7.4%(2.8)
-14.7%(3.8)
-69.7%(2.4)
-66.4%(2.9) -68.4%
(2.5)
-68.1%(4.2)
-69.2%(2.7)
-66.9%(3.0)
-80%
-70%
-60%
-50%
-40%
-30%
-20%
-10%
0%
Pooled Results: % Change from Baseline in LDL-C at
Week 8/12 by Baseline LDL-C, non-HDL-C and Apo B
64
LS
me
an
(S
E)
% c
ha
ng
e in
LD
L-C
Le
ve
l
at
we
ek
8/1
2 L
OC
F
Baseline LDL-C
subgroup
Baseline non-HDL-C
subgroup
≤3.36 mmol/L <4.3 mmol/L ≥4.3 mmol/L>3.36 mmol/L
n=43 n=66 n=32 n=49 n=26n=38 n=77 n=27
Baseline Apo B
subgroup
<1.1 g/L ≥1.1 g/L
n=46 n=28n=59 n=44
Placebo
Alirocumab
150 mg Q2W
≤130 mg/dL <166 mg/dL ≥166 mg/dL>130 mg/dL <110 mg/dL ≥110 mg/dL
Cut-offs for LDL-C (3.36 mmol/L, 130 mg/dL) and non-HDL-C (4.3 mmol/L, 166 mg/dL) based on thresholds for starting therapy in patients at, respectively, moderate/moderately high cardiovascular (CV) risk in the most
recent US cholesterol management (ATP III) guidelines1 and intermediate CV risk in the 2012 Canadian dyslipidemia guidelines2. Cut-off for Apo B (1.1 g/L, 110 mg/dL) based on value derived by regression analysis
from consensus target LDL-C and non-HDL-C values3 and threshold for initiatiing therapy in intermediate-risk patients in the 2012 Canadian guidelines2. 1. Grundy et al. Circulation. 2004;110:227-239. 2. Anderson et al.
Can J Cardiol. 2013;29151-167. 3. Soran et al. Ann Clin Biochem 2011;48[Pt6]:566-571. Data pooled from mITT population of studies 1003 (NCT01266876), 11565 (NCT01288443), and 11566 (NCT01288469).




i.e., MACE

Adverse events were NOT more common if LDL was VERY lowUnpublished data

Learning objectives:
• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Etc…..

71



1.42
1.81
2.58
2.07
2.58
3.37

Learning objectives:
• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Etc…..








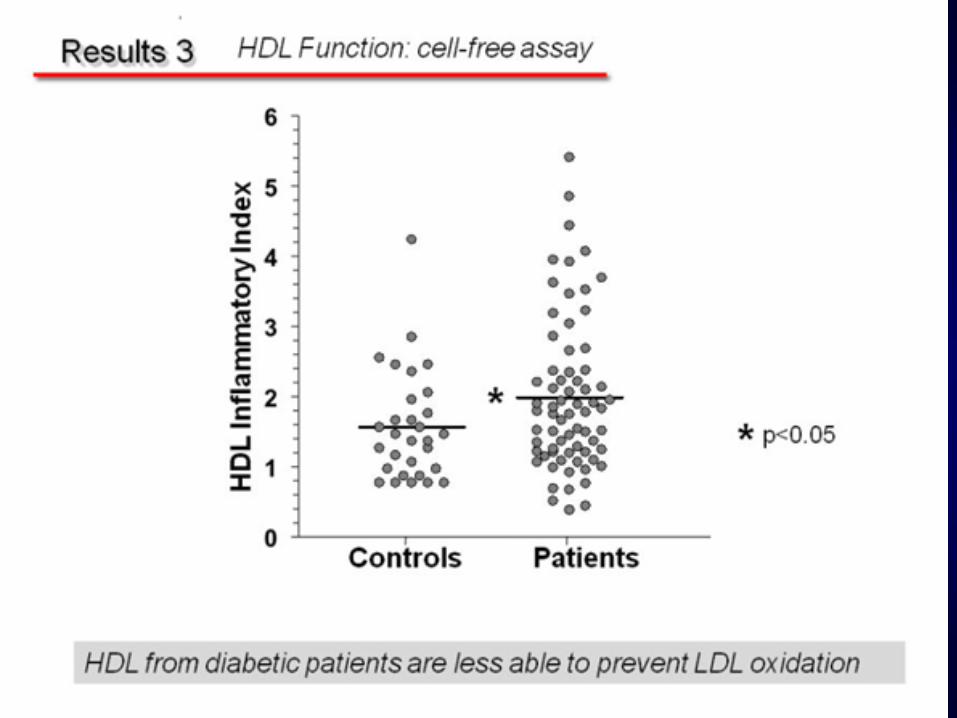
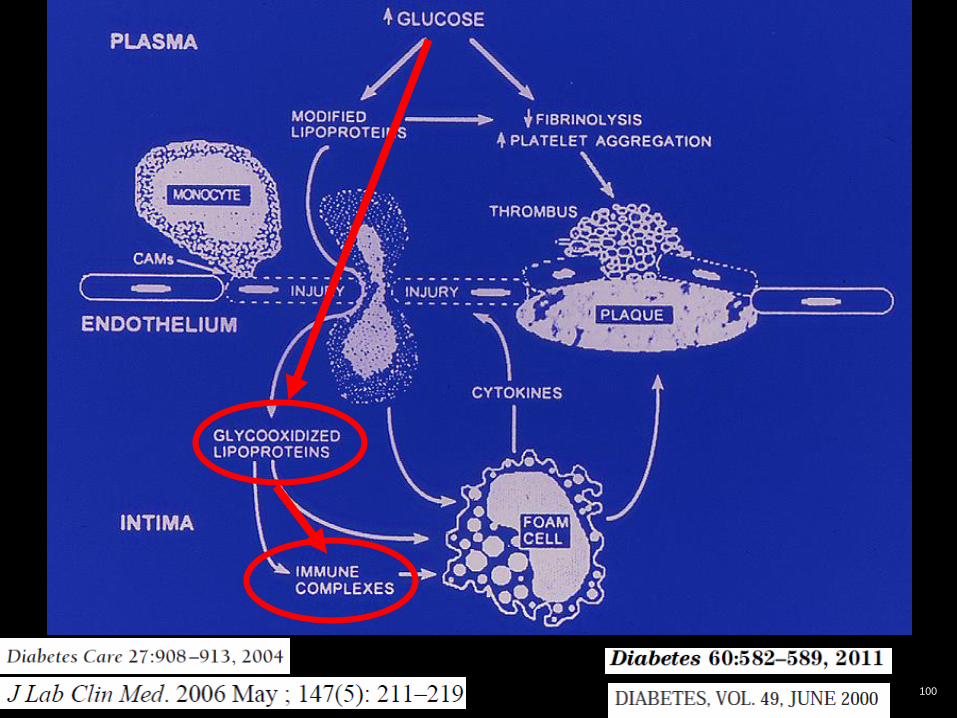
Does glycemic control affect
the function of lipids?
If it does, then should the degree of
glycemic control affect our
recommendations for treating the
lipids?

Slide Source:
Lipids Onlinewww.lipidsonline.org
LDL
LDL
Cockerill GW et al. Arterioscler Thromb Vasc Biol 1995;15:1987-1994.
Endothelium
Vessel Lumen
Monocyte
Modified LDL
Macrophage
MCP-1AdhesionMolecules
Cytokines
Inhibition of Adhesion Molecules
Intima
Foam Cell
HDL and “Anti-Atherosclerosis”

Slide Source:
Lipids Onlinewww.lipidsonline.org
LDL
LDL
Cockerill GW et al. Arterioscler Thromb Vasc Biol 1995;15:1987-1994.
Endothelium
Vessel Lumen
Monocyte
Modified LDL
Macrophage
MCP-1AdhesionMolecules
Cytokines
Inhibition of Adhesion Molecules
Intima
HDL InhibitOxidation
of LDL
HDL Inhibits Chemotaxis and inhibits Adhesion Molecule Expression
Foam Cell
HDL Promote Cholesterol Efflux
HDL and “Anti-Atherosclerosis”

86

87

88

89
90

91
Presented at ADA San Diego
2011

92

93

94

95
Mean A1c 7.6%

96

97

98

99
100

Glycated LDL and HDL
•Glycemic control may play a role in how atherogenic the lipoproteins may be
•Guidelines don’t specifically recommend it, but if you have someone with an A1c of 6.5% vs A1c of 8.5%, you might choose to be more aggressive treating the lipids of the latter.
•Some Type 1’s have HDL of 2 or more. If their A1c is 10%, do we care? Is the HDL doing anything? At what point are we assured?

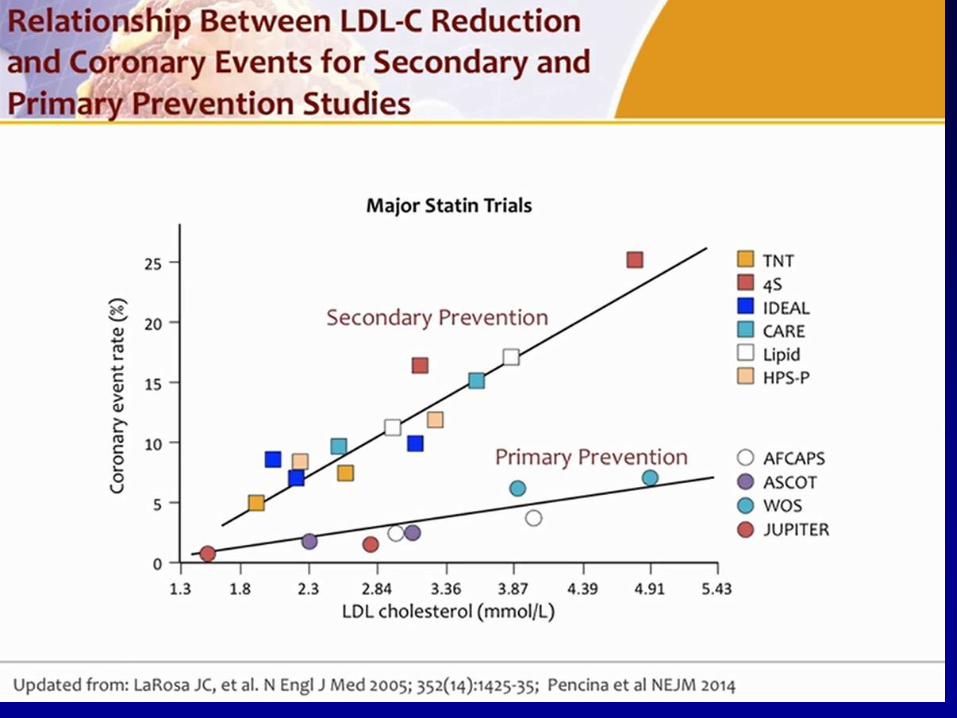
Summary and conclusions• Statins lower CV risk in essentially all diabetics.
– The use of statins should be guided by perceived CV risk, as per guidelines (which guidelines???)
– Lifetime risk should also be considered
• Correct LDL first
• In people in whom you cannot decide, measuring an apoB, non-HDL might provide further information

Summary and conclusions: cont’d
• The addition of Ezetemibe to statin with subsequent lowering of LDL does lower risk more (at least in diabetics)
• Targets are changing (at least in the US) in view of IMPROVE-IT and FOURIER
• PCSK9 inhibitors …..
104

105

106




•Should we be checking LDL (or other lipid fractions)?
•What is the normal range?•Is there an upper limit to the range?•Is there a lower limit to the range?•What are the targets in people with diabetes? What should the targets be?
•Is the cholesterol hypothesis proven?•Hypothesis or fact?
With respect to (LDL) cholesterol….

Learning objectives:• Review the importance of statins to lower CV risk in
diabetes
• To review lipid guidelines (Canadian and American) as they
pertain to diabetes
• Is lower better (at least for diabetes)?
– To review results with Ezetemibe and PCSK9 inhibitors
• Are studies with these drugs going to impact guidelines?
• Does glycemic control matter wrt lipids/targets?
• To review where triglyceride management might fit in
• Is statin intolerance real? Does it matter?
• Do statins cause diabetes? Does it matter?
• Small interfering RNA
• Etc…..

Mr. M. S., age 58, diabetic
TC: 4.22 mmol/L (163 mg/dl)
HDL: .99 mmol/L (38 mg/dl)
LDL: 1.42mmol/L (55 mg/dl)
Triglyceride: 3.98 mmol/L (349 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?

Mr. M. S., age 58, diabetic
TC: 4.22 mmol/L (163 mg/dl)
HDL: .99 mmol/L (38 mg/dl)
LDL: 1.42mmol/L (54 mg/dl)
Triglyceride: 3.98 mmol/L (349 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?

Mr. M. S., age 58, diabetic
TC: 4.22 mmol/L (163 mg/dl)
HDL: .99 mmol/L (38 mg/dl)
LDL: 1.42mmol/L (54 mg/dl)
Triglyceride: 3.98 mmol/L (349 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?

Mr. M. S., age 58, diabetic
TC: 4.22 mmol/L (163 mg/dl)
HDL: .99 mmol/L (38 mg/dl)
LDL: 1.42mmol/L (54 mg/dl)
Triglyceride: 3.98 mmol/L (349 mg/dl)
A1c: 6.9%
Meds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?

Mr. M. S., age 58, diabeticMeds include Metformin 1 gm bid, Ramipril10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?
TC: 4.22 mmol/L (163 mg/dl)
HDL: .99 mmol/L (38 mg/dl)
LDL: 1.42mmol/L (54 mg/dl)
Triglyceride: 3.98 mmol/L (349 mg/dl)
apoB: .94

Mr. M. S., age 58, diabeticMeds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?
TC: 3.52 mmol/L (136 mg/dl)
HDL: .89 mmol/L (34 mg/dl)
LDL: 1.07 mmol/L (41 mg/dl)
Triglyceride: 3.5 mmol/L (310 mg/dl)
apoB .79

Mr. M. S., age 58, diabeticMeds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg
Are his lipids optimally controlled?
Should you add more statin?
Should you add a fibrate?
TC: 3.52 mmol/L (136 mg/dl)
HDL: .89 mmol/L (34 mg/dl)
LDL: 1.07 mmol/L (41 mg/dl)
Triglyceride: 3.5 mmol/L (310 mg/dl)
apoB .79
119

BIP: Effects of baseline Triglycerides
on response to treatment
Circulation, 2000;102:21-27
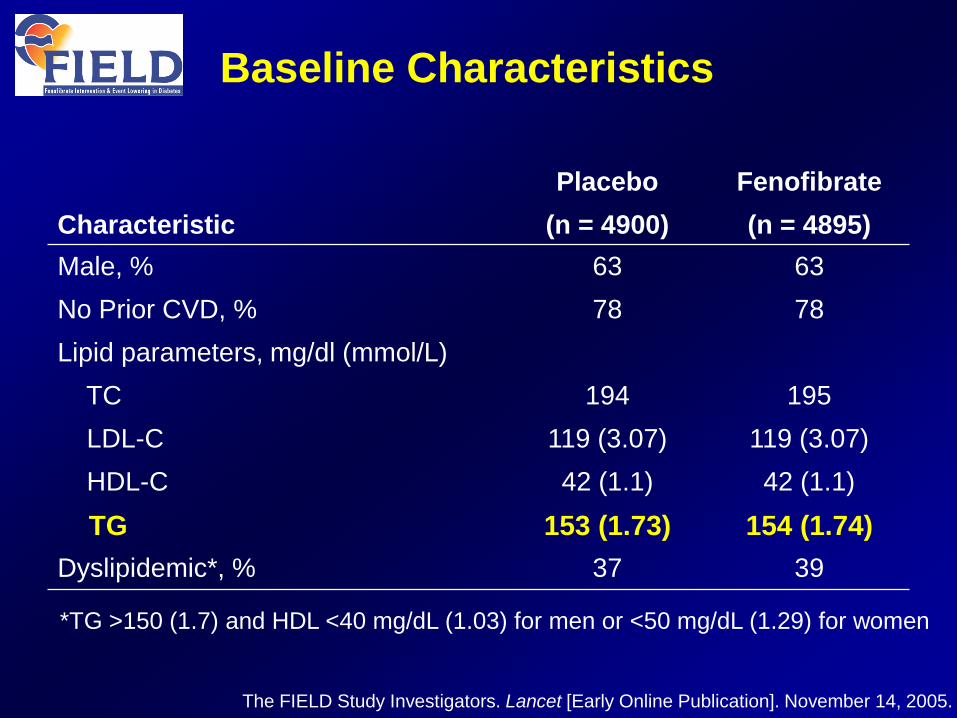
Characteristic
Placebo
(n = 4900)
Fenofibrate
(n = 4895)
Male, % 63 63
No Prior CVD, % 78 78
Lipid parameters, mg/dl (mmol/L)
TC 194 195
LDL-C 119 (3.07) 119 (3.07)
HDL-C 42 (1.1) 42 (1.1)
TG 153 (1.73) 154 (1.74)
Dyslipidemic*, % 37 39
Baseline Characteristics
*TG >150 (1.7) and HDL <40 mg/dL (1.03) for men or <50 mg/dL (1.29) for women
The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.





127



130

131

132

133

Lipid Goals for Individuals at Risk for ASCVD
Lipid parameter Goal (mg/dL)
TC <200
LDL-C <130 (low risk)
<100 (moderate risk)
<100 (high risk)
<70 (very high risk)
<55 (extreme risk)
Non–HDL-C 30 above LDL-C goal; 25 above LDL-C goal (extreme risk individuals)
TG <150
Apo B <90 (individuals at high risk of ASCVD, including those with diabetes)
<80 (individuals at very high risk with established ASCVD or diabetes plus
≥1 additional risk factor)
<70 (individuals at extreme risk)
Abbreviations: apo, apolipoprotein; ASCVD, atherosclerotic cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
AACE/ACE 2017;epub ahead of print; Baigent C, et al. Lancet. 2010;376:1670-1681; Boekholdt SM, et al. J Am Coll Cardiol. 2014;64(5):485-494; Brunzell JD, et al. Diabetes Care. 2008;31:811-822; Cannon CP, et al. N Engl J Med. 2015;372(25):2387-2397; Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22; Jellinger P, Handelsman Y, Rosenblit P, et al. Endocr Practice. 2017;23(4):479-497; Ridker PM, J Am Coll Cardiol. 2005;45:1644-1648; Sever PS, et al. Lancet. 2003;361:1149-1158; Shepherd J, et al. Lancet. 2002;360:1623-1630; Weiner DE, et al. J Am Soc Nephrol. 2004;15(5):1307-1315.

Question: How are different drugs used to treat dyslipidemia? Statins, Fibrates
Statins
• R56. Statin therapy is recommended as the primary pharmacologic agent to achieve target LDL-C goals on the basis of morbidity and mortality outcome trials (Grade A; BEL 1).
• R57. For clinical decision making, mild elevations in blood glucose levels and/or an increased risk of new-onset T2DM associated with intensive statin therapy do not outweigh the benefits of statin therapy for ASCVD risk reduction (Grade A, BEL 1).
• R58. In individuals within high-risk and very high-risk categories, further lowering of LDL-C beyond established targets with statins results in additional ASCVD event reduction and may be considered (Grade A, BEL 1).
• R59. Very high-risk individuals with established coronary, carotid, and peripheral vascular disease, or diabetes, who also have at least 1 additional risk factor, should be treated with statins to target a reduced LDL-C treatment goal of <70 mg/dL (Grade A, BEL 1).
• R60. Extreme risk individuals should be treated with statins or with combination therapy to target an even lower LDL-C treatment goal of <55 mg/dL (Grade A, BEL 1).
Fibrates
• R61. Fibrates should be used to treat severe hypertriglyceridemia (TG >500 mg/dL) (Grade A; BEL 1).
• R62. Fibrates may improve ASCVD outcomes in primary and secondary prevention when TG concentrations are 200 mg/dL and HDL-C concentrations <40 mg/dL (Grade A; BEL 1).
•R55. In individuals at risk for ASCVD, aggressive lipid-modifying therapy is recommended to achieve appropriate LDL-C goals (Grade A, BEL 1).
Re
com
me
nd
ati
on
s a
sso
cia
ted
wit
h t
his
q
ue
stio
n:
Jellinger P, Handelsman Y, Rosenblit P, et al. Endocr Practice. 2017;23(4):479-497.
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol;
TG, triglycerides.
136

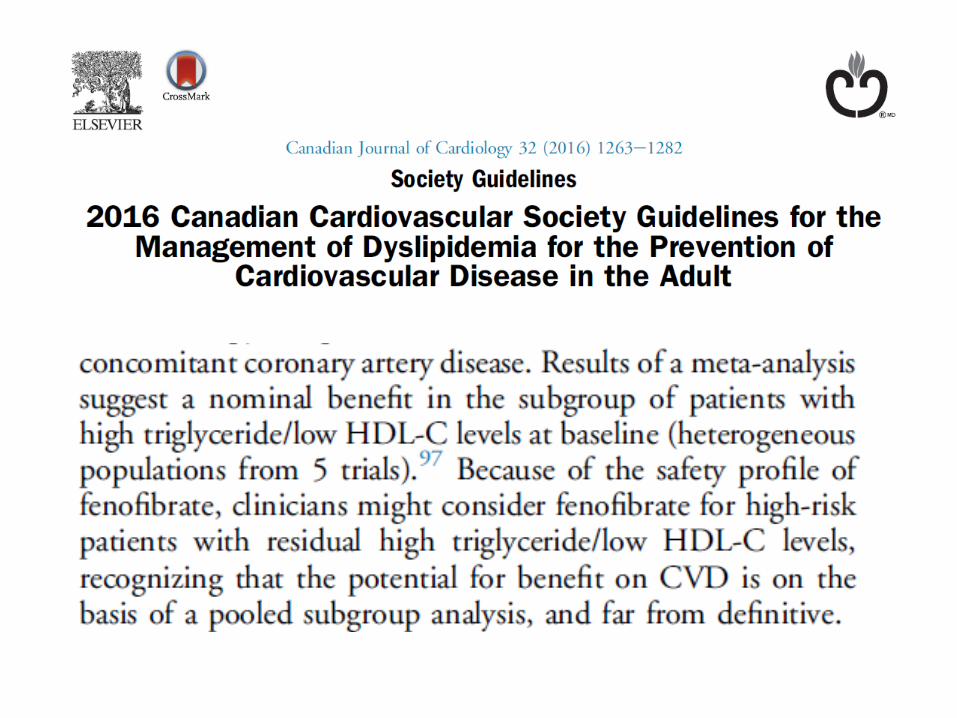
Summary and conclusions: cont’d
• Most guidelines around the world are coming around to the same conclusion, i.e., that in the presence of atherogenic dyslipidemia, there is reasonable evidence that fibrates decrease CV risk
• (Gemfibrozil should not be used with a statin)