
Diabetes and Kidney Disease - Baptist Health South Florida · 2018-03-14 · Diabetes and Kidney...
23
1 Diabetes and Kidney Disease Alessia Fornoni, MD PhD Professor of Medicine Chief, Katz Family Division of Nephrology and Hypertension Director, Peggy and Harold Katz Family Drug Discovery Center University of Miami School of Medicine Disclosures I am vice President and CSO of L&F Health LLC L&F Health LLC and affiliated companies have a patent estate covering some of the topics being presented L&F Health LLC has consulting agreements with and/or has received honoraria from Hoffman La Roche, Genentech, Mesoblast, Bristol Myers Squibb, Abbvie, Jenssen, Boehringer Ingelheim, Astra Zeneca, Pfizer, Mallinkrodt, Chemocentryx, Dimerix, Variant Pharmaceutical. Variant Pharmaceuticals, Inc. has licensed worldwide rights to develop and commercialize hydroxypropyl beta cylodextrin for treatment of kidney disease from L&F Research Objectives •Definition and screening for DKD •2018 Treatment guidelines •New approaches to patients risk stratification Objectives •Definition and screening for DKD •2018 Treatment guidelines •New approaches to patients risk stratification
Transcript of Diabetes and Kidney Disease - Baptist Health South Florida · 2018-03-14 · Diabetes and Kidney...

1
Diabetes and Kidney Disease
Alessia Fornoni, MD PhDProfessor of Medicine
Chief, Katz Family Division of Nephrology and Hypertension
Director, Peggy and Harold Katz Family Drug Discovery Center
University of Miami School of Medicine
DisclosuresI am vice President and CSO of L&F Health LLC
L&F Health LLC and affiliated companies have apatent estate covering some of the topics beingpresented
L&F Health LLC has consulting agreements withand/or has received honoraria from Hoffman LaRoche, Genentech, Mesoblast, Bristol Myers Squibb,Abbvie, Jenssen, Boehringer Ingelheim, Astra Zeneca,Pfizer, Mallinkrodt, Chemocentryx, Dimerix, VariantPharmaceutical.
Variant Pharmaceuticals, Inc. has licensed worldwide rights to develop and commercialize hydroxypropylbeta cylodextrin for treatment of kidney disease from L&F Research
Objectives•Definition and screening for DKD
•2018 Treatment guidelines
•New approaches to patients risk stratification
Objectives•Definition and screening for DKD
•2018 Treatment guidelines
•New approaches to patients risk stratification

2
DKD yearly updates
Page S105: Microvascular complications
Diabetes Care, 2018, Supplement 1 USRDS 2010-2016
DKD remains the most common cause of ESRD
ESRD prevalence (per M) ESRD prevalence by cause 2014
2014
1992
Prevalence of Diabetic Kidney Disease (DKD)
deBoer JAMA 2011; 305: 2532
DKD and yearly risk of death
> 5000 Type 2 Diabetes patients
Yearly risk associated
Adler et al, Kidney International, 2003;63:225
CVD risk protection needs early implementation

3
Kidney disease is among the top causes of death
Murray et al NEJM 2013; 369: 5Copyright ©2004 BMJ Publishing Group Ltd.
Hovind, P. et al. BMJ 2004;328:1105
277 patientsType 1 DMf/u 18 yrs
Natural progression of DKD in T1D
75% ESRD at 20 years
Early Detection and Treatment are EssentialEarly biomarkers are missing
10,290 members of a managed care organization with HTN and T2D (Kayser Permanente)ACR at baseline and with at least 2 additional determinations over time, 7 1/2 years follow up
Vupputuri S et al, Diabetes Res Clin Pr, 91: 246, 2011
30%
12%
Natural progression of DKD in T2D Screening for DKD
yearly follow up, Level of evidence B
ADA recommendations, Diabetes Care, January 2017
At diagnosis if HTN

4
Definition of DKDDIABETES with:
Abnormal urine albumin excretion >30 mg/24 hours>30 mg/g creatinine (preferred)>20 µg/min
and/ordiabetic glomerular lesions
and/orloss of glomerular filtration rate (CKD-EPI
preferred)ADA recommendations, Diabetes Care, January 2018
ACR & Progression to ESKD
Babazono Diabetes Care 2009; 32: 1518
White: FBlack: M
Proteinuria and GFR: risk factors for ESRD
Shahinfar S et al, Kidney Int: S48-S51, RENAAL Baseline Characteristics
Albuminuria and kidney failure risk
Tangri N et al, JAMA. 2016 Jan 12;315(2):164-74
Risk calculator: kidneyfailurerisk.com
Chronic Kidney Disease Prognosis Consortium721357 participants30 countries

5
Risk stratification
KDIGO 2012, Kidney International, Issue 1, 2013
1
1
1
1
1
2
2
2
2
3 3
3
3
3
4
44 4
Numbers indicate the suggested number of visits/year
Is testing for albuminuria enough?
Albuminuria and DKD progression in T1D: DCCT/EDIC >20 years follow up
Molitich et al, Diabetes Care, 2010; 33:1536-43, DCCT-EDIC f/u
11.4%Severe albuminuria was a strong predictor of risk of developing sustained eGFR <60 ml/min/1.73 m2
Screening with AER alone would have missed 24% of cases of sustained impaired eGFR
Normoalbuminuric DKD progression in T2D
Ravi Retnakaran et al. Diabetes 2006;55:1832-1839, UKPDS 74
5102 UKPDS patients with T2DNormal albuminuria and creatinine at baseline
51% NA

6
Normoalbuminuric DKDPrevalence of low GFR and normoalbuminuria
MacIsaac Kidney Int 2014; 86: 50 MacIsaac, Kidney Int 2014; 86: 50
Natural history of albuminuria
Nephrology referral and biopsy
Worsening proteinuria despite treatmentLoss of eGFR> 1cc/min/1.73m2/monthActive urine sedimentAbsence of retinopathy
>30% reduction in eGFR after initiation of ACEi/ARBRefractory hypertension
eGFR<30 cc/min/1.73m2 at diagnosis
biopsy
CKD care and referral for renal replacement strateg ies
ADA recommendations, Diabetes Care, January 2018NKF QDOQI guidelines for diabetes, AJKD 2014
ADA
QDOQI
Gonzalez Suarez ML, Thomas DB, Barisoni L, Fornoni A., World J Diabetes, 2013
Often the diagnosis
In clinically indicated kidney biopsies differs
from DKD
Protocol kidney biopsies
are needed to understand the
disease
Limitation of clinically indicated kidney biopsies

7
TYPICAL DIABETIC NEPHROPATHY (C2) – 30 %
NEAR NORMAL HISTOLOGY
(C1) – 30 %
NON-SPECIFIC FINDINGS
(C3) – 40 %
(a) Both normal and totally destroyedglomeruli
(b) Severe arteriolohyalinosis
(c) Tubulointerstitialfibrosis
Fioretto et al. Diabetologia 1998;41:233-236
Albuminuria and T2D: pathologic heterogeneity
Change in GFR (%) in patients with T2D and albuminuria
-20
-10
0
+10
∆ %
GF
R/y
ear C3
C1
C2
Nosadini et al. Diabetes 2000;49:476-484
* p<0.05, C2 vs C1 ja C3
*
(n=33, 4 year follow-up)
GBM thickening can predict decline in kidney function in T1D with NA
Caramori M L et al. JASN 2013;24:1175-1181Pagtalunan ME et al, JCI, 99: 342-348, 1997Meyer TW et al, Diabetologia, 42:1341-1344
Podocytopathy in early DKD in T2D

8
Podocytopathy in DKD in T1D
White K E et al. Diabetes 2002;51:3083-3089
Podocyte detachment occurs in T1D correlates with AER and loss of GFR
Toyoda M et al, Diabetes, 2007, 56: 2155
Fraction of peripheral GBM covered by intact foot processes
Objectives•Definition and screening for DKD
•2017 Treatment guidelines
•New approaches to patients risk stratification
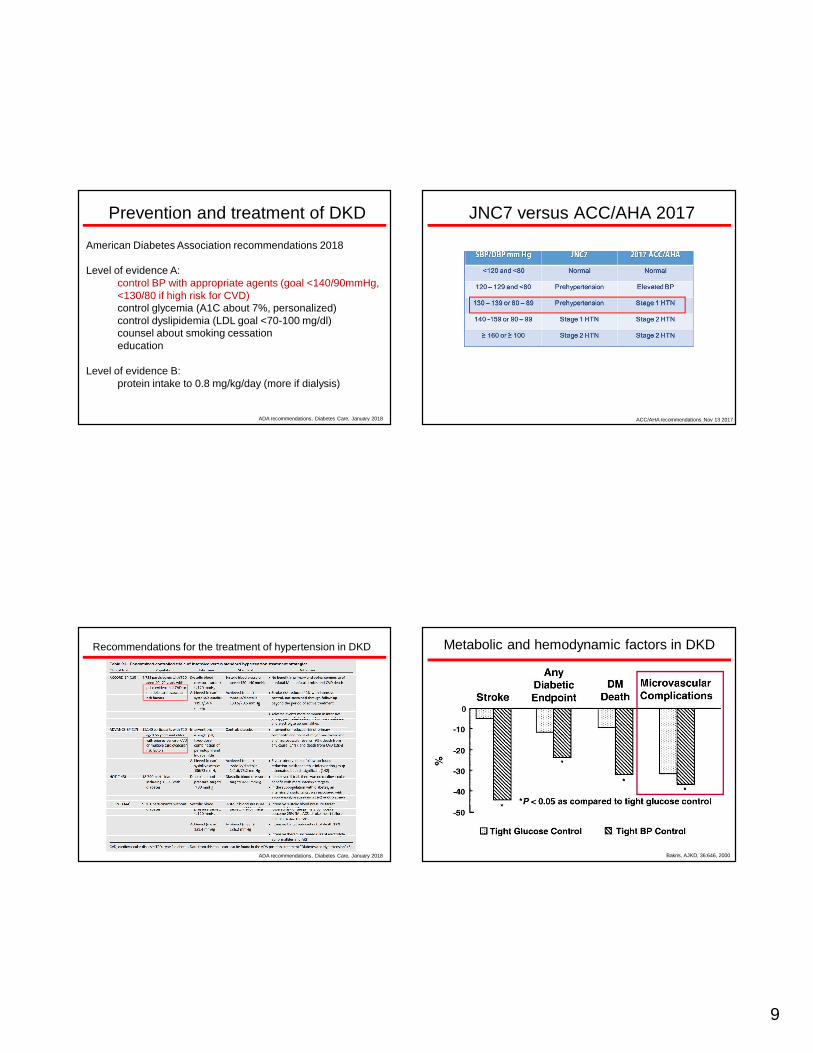
Prevention and treatment of DKD
American Diabetes Association recommendations 2018
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2018
9
Prevention and treatment of DKD
American Diabetes Association recommendations 2018
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2018
JNC7 versus ACC/AHA 2017
ACC/AHA recommendations Nov 13 2017
Recommendations for the treatment of hypertension in DKD
ADA recommendations, Diabetes Care, January 2018
Metabolic and hemodynamic factors in DKD
Bakris, AJKD, 36:646, 2000

10
Bakris GL, AJKD, 36:646, 2000
Role of BP in DKD Role of ACEi to treat DKD
The Collaborative Study Group, NEJM, 329:1456, 1993
Type I DM (207 captopril and 202 placebo)
Proteinuria>500 mg/24 h
Creat <2.5 mg/dl
Significant effect of captopril on blood pressure
0
10
20
30
40
50
%
1 2 3 4
Risk reduction of 51% P=0.006
Captopril 25mg x 3
Time (year)
Placebo
Captopril
% o
f patient
s with e
ndpoints
* dialysis, transplant, death
Role of ARB to treat DKD
IDNT trial, NEJM 345:851, 2001
1715 pt type 2 DM + HTN
Irb 300 mg vs amlo 10 mg vs placebo
End points:
doubling creatinine
ESRD
death
F/u 2.6 years
-3.3 mmHg mean BP in tx vs placebo
Placebo
Irbesartan 150 mg
Irbesartan 300 mg
20
15
10
5
0
0 3 6 12 18 22 24
Inc
idenc
e o
f diabetic
nephro
path
y (%
)
P<0.001
P=NS
Time (months)
IRMA-2. Parving et al. N Engl J Med 2001;345:870-8
ACEi vs CCB in primary prevention of DKD with mild hypertension
BENEDICT, NEJM, 251:1941, 2004
1204 patients, type 2 DM
Primary end point: persistent MA

11
ARB vs placebo in primary prevention of DKD with normal BP
Bilius R et al, DIRECT, Annals of internal medicine, 2009; 151:11-20
3326/1905 (type 1/type2) patients.
Normotensive with normoalbuminuria
Candesartan versus placebo (significant effect on BP)
4.7 years follow up
Primary end point: development of MA
Secondary: Change in UAER Barnett AH, NEJM, 351:1952, 2004
ACEi or ARB?
Prospective, multicentered, double-blind study250 patients with type 2 DM and DNTelmisartan 80 mg vs enalapril 20 mg.Five year follow-upPrimary end-point: change in iohexol GFRSecondary end-points: creat, UAE, BP
no difference!
ACEi or ARB?
ADA 2017:
Type 1 DM with HTN and albuminuria: ACEiType 2 DM with HTN and microalbuminuria: either ACEi or ARBsType 2 DM with HTN and overt nephropathy: ARBsWhen not tolerated, substitute one for the other
ADA recommendations, Diabetes Care, January 2017
Combination not supported
Is there a role for ACEi/ARB combinationin DKD in type 2 DM? ON TARGET
Mann J et al, ONTARGET trial, The Lancet, 2008, 372: 547-562
25620 patients with CV disease or high risk diabetes Follow up for 5 yearsPrimary renal outcome: dialysis, x2 creat, death
BP -2.4/1.4 mmHg
BP -0.9/0.6 mmHg

12
Aldosterone antagonism in DN
J Hyperten, 2006, 24:2285
Randomized trial59 patients with type 2 DM+ macroalbuminuriaOn ACEi or ARB25-50 mg spironolactone x 1 year
Epstein, M. et al. Clin J Am Soc Nephrol 2006;1:940-951
Figure 3. Percentage change in median UACR from baseline to we ek 12, by quartile of baseline estimated glomerular filtration rate (eGFR) and treatment group
Aldosterone antagonism in DKD
ARTS-DN Japan
Journal of Diabetes and Its Complications 2017 31, 758-765DO
Aldosterone antagonism in DKD:phase 2b with finerenone
ARTS-DN
JAMA 2015, 314:884
Prevention and treatment of DKD
American Diabetes Association recommendations 2017
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2017

13
Kovesdy CP et al, AJKD 2008, 52: 766Cohen RM et al, Diabetes Care. 2003 Jan;26(1):163-7McCarter RJ et al, Diabetes Care. 2004 Jun;27(6):1259-64
A1C: a real measure in CKD?
Falsely elevated A1C:
Uremic toxinsMetabolic acidosis
Falsely decreased A1C:
Decreased 1/2 life RBCsBlood transfusionsEPO treatment
May need to change to glycated fructosamine, glycated albumin, variation of A1C or glycosylation gap (based on A1C and fructosamine)
Intensive treatmentWith A1c 7.2
Standard treatment With A1c 9.1
-64
-54-51
-39
-56-61
-72-80
-70
-60
-50
-40
-30
-20
-10
0Retinopathy Severe DR Laser Rx Microalb Severe
MicroalbAlbuminuria Neuropathy
NEJM 1993; 329:977
DCCT: 1441 patients with type 1 DM
f/u 6.5 years
Insulin 3 x day or pump vs conventional (1 or 2 daily insulin injection)
Primary prevention/secondary prevention
Difference maintained after discontinuation of tx (7 yr follow up)
Role of glycemia in type 1 DM and DKD
Treatment with A1c 7.0
Diet with A1c 7.9
-12
-25-29
-24
-34-40
-35
-30
-25
-20
-15
-10
-5
0Any Diabetes
RelatedEndpoint
MicrovascularEndpoints
Laser Rx Cataract Albuminuria
UKPDS: 3867 type 2 DM
Median age 54
Intensive tx (sulpha or insulin) versus diet
End points: any DM related end-point, diabetes related death and all cause mortality
F/u 10 years (15 years f/u had no difference in diabetes related death)Lancet 1998; 352: 837-853
Role of glycemia in type 2 DM and DKD Role of glycemia in advanced DKD
Ricks et al., Diabetes 61(30): 708–715, 2012

14
Regression of MA in type 1 DM
% Risk Reduction Perkins, NEJM, 2003;348:2285
386 patients with persistent MATotal f/u of 4 periods of 2 years eachRegression defined as 50% reduction in UAE from one period to the other
Regression of MA in type 2 DM
% Risk Reduction Araki, Diabetes, 2005;54:2983
216 Japanese patients with type 2 DMF/u 6 years, 3 periods of 2 years eachRegression: 50% reduction MARemission: back to NA
A1C: how low can we get?
ADVANCE trial, NEJM, 358:24, 2008
11140 patients, standard vs intensive (sulfa + other drugs to achieve A1C less than 6.5).Macro: CV death, MI, strokeMicro: development of alb, x 2 creat, ESRD
21% relative reductionin nephropathy
ACCORD, NEJM, 358:24, 2008
10,251 patients, standard vs intensive (mainly insulin and TZDs).1/3 patients had prior CV eventEnd point: CV death, MI, strokeDiscontinued after 3.5 years f/u for high mortality in intensive arm.
A1C: how low can we get?

15
Are all anti-diabetic drugs alike?
Legend: MET=Metformin, GLP1 RA= incretins, SGLT2i= glycosuric a, DPP4-i= incretins, AGi=alpha-gluc inhib, TZD=glytazones, Su= sulphanilurea, GLN= glucosaminog, COLSVL= bile acid, BCR=bromocriptin, PRAM=pramlintide
www.AACE.com Hattersley AT, Thorens B. N Engl J Med 2015;373:974-976
Renal Absorption of Glucose and Glucagon Secretion According to the Presence or Absence of a Sodium-
Coupled Glucose Transporter Type 2 (SGLT2) Inhibito r.Glycemia and DKD: drug class effect
SGLT2 inhibition: is sweet urine the solution?
Wanner C et al. N Engl J Med 2016. DOI: 10.1056/NEJMoa1515920
K–Meier Analysis of Two Key Renal Outcomes.SGLT2 inhibitors and DKD: EMPA-REG
Composite outcomeComposite outcomeComposite outcomeComposite outcome: doubling of the serum creatinine initiation of renal-replacement therapy death from renal disease
46%
Worsening NephropathyWorsening NephropathyWorsening NephropathyWorsening Nephropathy:eGFR<60 ml/min and/or ACR>300 mg/g
39%
Neal et al, et al. N Engl J Med 2017. 377:644-657
K–Meier Analysis of Two Key Renal Outcomes.SGLT2 inhibitors and DKD: CANVAS trial
With better A1C and BP control

16
K–Meier Analysis of Two Key Renal Outcomes.ARB versus SGLT2 inhibitors
Doubling of serum creatinine
ESRD
All cause mortality
0.1 0.4 0.7 1.0 1.4
0.67
0.92
0.77
Hospitalisation for heart failure
0.78
Doubling of serum creatinine
ESRD
All cause mortality
0.1 0.4 0.7 1.0 1.4
0.56
0.68
Hospitalisation for heart failure
0.65
0.45
IDNT EMPA-REG
Courtesy of Dr Per-Henrik Groop % Risk Reduction
SGLT2 inhibitors and TG feedback
Cherney D et al, CirculationAHA 2013
No difference in incident albuminuria!
Other effects?
DN: the gut to kidney connection
Muskiet et al, Nature Review, 10:88-103, 2014
K–Meier Analysis of Two Key Renal Outcomes.Liraglutide and DKD: LEADER trialTime to first renal event: ACR>300, x2 creat, ESRD, renal death
The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI: confidence interval; ESRD: end-stage renal disease; HR: hazard ratio.
Mann J et al, NEJM 2017, 377:839-848, 2017l
9340 T2DM patients3.8 yrs f/uCKD1 35%, CKD2 42%, CKD3 20%

17
K–Meier Analysis of Two Key Renal Outcomes.DPP4 inhibition and DKD: linagliptin
5466 T2D pt13 trialsSec EP: new onset A50% eGFR loss (CKD-EPI)S creat >250 umol/L
Prevention and treatment of DKD
American Diabetes Association recommendations 2017
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2018
Statins do not prevent GFR loss
CARDS study group, Am J Kidney Dis. 2009 Nov;54(5):810-9
Haynes R et al. JASN 2014, 25:1825-1833
Prevention and treatment of DKD
American Diabetes Association recommendations 2017
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2017

18
Cigarette smoking and DKD (T1D)
normo→micro mild→moder moder→ESRD
NC
EE
N
C
E
N
C
HR=2.39* for current smokers HR=ns* for current smokers HR=ns* for current smokers *Adjusted for duration of diabetes, HbA1c and hypertension
N=non-smokers, C= current smokers, E=Ex-smokers
Feodoroff et al Acta Diabetol 2016
Prevention and treatment of DKD
American Diabetes Association recommendations 2017
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 if high risk for CVD)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 mg/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2017
Multifactorial intervention in type 1 DM
Hovind, P, Diabetes Care, 26: 1258, 2003
600 patients20 years follow up
ACEi
SmokingA1CMAP

19
Multifactorial intervention in type 2 DM
Gaede, P, NEJM, 358: 580, 2008Diabetic Nephropathy Remission and Regression Team Triial (DNETT-Japan)
160 patients from Steno27.8 years tx + 5.5 yrs f/u
Primary end point: deathSec end point: ESRD
INTENSIVE:StatinASAACEi/ARBExercisediet
Prevention and treatment of DKD
American Diabetes Association recommendations 2018
Level of evidence A:control BP with appropriate agents (goal <140/90mmHg, <130/80 only for younger patients)control glycemia (A1C about 7%, personalized)control dyslipidemia (LDL goal <70-100 mg/dl)counsel about smoking cessationeducation
Level of evidence B:protein intake to 0.8 g/kg/day (more if dialysis)
ADA recommendations, Diabetes Care, January 2017
Dietary protein intake in DKD
Hansen HP et al, Kidney International, 62:220, 2002
Careful protein restriction in CKD 3 and above
Case
SmokerObeseBP150/90A1c 11%LDL 150High protein diet
Mr JD comes to you with GFR 50 cc/min/1.73m2
Non smokerExercise TIWBP130/80A1c 6.9%LDL 70Low protein diet
GFR loss 20 cc/min/year GFR loss 2 cc/min/year
ESRD in 2 year ESRD in 20 year
IT’’’’S UP TO MR JD AND TO YOU!

20
Objectives•Definition and screening for DKD
•2018 Treatment guidelines
•New approaches to patients risk stratification
Is hyperuricemia a predictor of outcome?
355 patients with DM and MABaseline uric acid determination6 years f/uEnd points: GFR Cystatin decline albuminuria
Ficociello et al, Diabetes Care. 2010 Jun;33(6):1337-43.
263 patients with type 1 diabetes, 18.1 years f/uUric acid measured 3 years after onset of diabetesAll patients NA at enrollment (23 with macroalbuminuria at f/u)
Hovind P et al, Diabetes, 2009 Jul;58(7):1668-71
Awaiting the results of the preventing early renal function loss
(PERL) allopurinol study
DKD: role of Vitamin D
168 consecutive patients in a CKD clinic (28% with DKD)6 years follow upBaseline Vitamin D adjusted for age, sex, smoking, CRP, albumin, ACE/ARB usage, eGFR
Ravani P et al, Kidney International (2009) 75, 88–95
TNF Receptors 1 and 2 in DKD
Cumulative risk for CKD>3 in patients with T1D during 12 years of follow-up according to quartile (Q1–Q4) of circulating TNFR2 at baseline.
Gohda T and Niewczas M et al, JASN, 23:516-524, 2012
(Caucasian Americans, 410 patients) Adapted from
Niewczas MA et al., JASN, 2012.(PIMA Native Americans, 193 patients) Adapted from
Pavkov ME et al. KI, 2014.
T1DM T2DM

21
Soluble Urokinase Receptor (suPAR)
Hayek SS et al. N Engl J Med 2015;373:1916-1925.
2292 patientsQ1: eGFR loss of 0.9 cc/minQ4: eGFR loss of 4.2 cc/min
suPAR levels in patients with T1D and DKD
(A)
0 2 4 6 82500
3000
3500
4000
4500
time (years)
suP
AR
(pg
/ml)
Normo-normo(n=10)
Normo-micro(n=10)
##
(B)
0 2 4 6 82500
5000
7500
10000
time (years)
suP
AR
(pg
/ml) Micro-micro
(n=10)
Micro-macro(n=10)
##
**
Normo Micro Macro
0
5000
10000
15000
suP
AR
(pg
/ml)
**
**
**
Normal GFR
(C)
Yoo T, Pedigo C.Fornoni et al., JASN, 2014
(D)
BA
SE
LIN
E
Role of dyslipidemia in DKD
Sacks F M et al. Circulation. 2014;129:999-1008 Anne J Overgaard et al, Proteome Sci. 2010; 8: 4
Plasma proteome analysis of patients with type 1 DM and DKD

22
Serum Amyloid A and DKD
Dieter BP et al, J Diabetes Complications. 2016 Nov - Dec;30(8):1467-1472
135 T2D patientsDKD stage 3a and severe albuminuria3.5 years of follow upOutcomes: death and ESRD
Plasma metabolomic analysis of patients with type 2 DM and DKD
Red circles: Common and stable metabolitesRed empty circles: Common metabolites that are not stableBlue: essential amino acids
Niewczas et al, Kidney International, 2014, 85:1214
DKD: next generation biomarkers DKD: system biology
Fornoni et al, Brenner Rector 11th Edition, In pressHeinzel et al,Frontiers in Cell and Developmental Biology, 2014

23
Acknowledgments
Nephrotic Syndrome Study Network
Questions?


















