Dfid health seminar slides 270416 tk
18
The political economy of maternal health care in developing countries DFID, 27 April 2016 Tim Kelsall, ODI Frederick Golooba-Mutebi, ESID and Independent Sam Hickey, ESID/GDI, University of Manchester
-
Upload
global-development-institute -
Category
Healthcare
-
view
288 -
download
0
Transcript of Dfid health seminar slides 270416 tk

The political economy of maternal health care in developing countries
DFID, 27 April 2016Tim Kelsall, ODI
Frederick Golooba-Mutebi, ESID and IndependentSam Hickey, ESID/GDI, University of Manchester

Overview
1. Introduction to ESID2. Researching the Politics of Health Care3. Key findings from the case studies4. Policy implications5. Discussion
User
Have pulled this out as a separate point as it is not just related to pilotsbut coalition-building more generally - ok?

1. Introduction

ESIDwww.effective-states.org
Global Development Institute, University of Manchester
A DFID-funded research centre, 2011-2016 Sub-Saharan Africa, South Asia, Latin America
Key research question Under what political conditions do developmental
forms of state capacity and elite commitment emerge and become sustained?

Please add text here Please add text here Please add text here Please add text here Please add text here
Political settlement
Competitive clientelist
Dominant coalition
Country Ghana Bangladesh South Africa
Rwanda Uganda
Accumulat-ion
Growth/SBRs Growth/ SBRs
Growth/ SBRs
Growth/SBRs Growth/SBRs
Hydrocarbons/ Mining
Hydrocarbons
Redistribut-ion
EducationHealth
EducationHealth
Education EducationHealthSocial protection
EducationHealthSocial protection
Recognition GenderSpatial inequity
Gender Gender Gender GenderSpatial inequity
Global PEAPSR
PEAPSR
PSR PEAPSR

2. Researching the Politics of Health Care

The countries
Country PS Type Key features
Rwanda Dominant Long time-horizon, strong coordination capacity
Ghana Competitive Short-time horizon, weak coordination capacity
Uganda Dominant (interstitial) Short-time horizon, mixed coordination capacity
Bangladesh Competitive (interstitial) Short-time horizon, mixed coordination capacity

Our causal model

Our approach
• Political settlement mapping interviews/exercises at national and sectoral level
• Analytical narratives linking evolution in PS to health policy, implementation, and performance
• Comparison of better and worse performing districts (MMR) for additional insight
• Advice about how to work, developmentally, in different political contexts

3. Key findings from the case studies

Rwanda
• Dominant settlement facilitates sound policies and rigorous implementation– Top-down (performance contracts ) and diagonal
(league tables) accountability– Problem solving approach, eg TBAs>midwives;
SMS; antenatal wards– Joined up approach

Ghana, Uganda, Bangladesh• Competitive or intermediate settlements lead to
populist policy making and/or slipshod implementation– Ghana: NHIS bankrupting local health facilities; CHPS
compunds lack basic equipment and staff; 90% budget spent on salaries
– Uganda: Districtization leads to proliferation of local health depts w/o qualified or experienced staff
– Bangladesh: ‘Elite consensus’ around doctor absenteeism; mushrooming of CCs w/o proper facilities

However
• All three poorer performers have some pockets of effectiveness and successful multistakeholder initiatives– Ghana, Upper East: P of E around Regional MO– Uganda, Lyantonde: dominant local coalition
enforced performance and leveraged sons of the soil
– Bangladesh: vigorous NGO and private sector

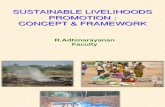
MMR trends in our case study countries
1990 1995 2000 2005 2010 20130
200
400
600
800
1000
1200
1400
1600
BangladeshGhanaRwandaUganda

4. Policy implications

Health system strengthening
• In dominant settlements like Rwanda, traditional health system strengthening approaches are likely to pay dividends
• In other types of settlement, there is insufficient national level political commitment for conventional approaches to work well. Maternal health policy needs to be more innovative, building out from pockets of effectiveness

‘Best fit’ strategies
Type of settlement Best ‘fit’ approach
Dominant developmental Government supporting
Competitive or intermediate Government connecting/brokering
Dominant predatory? Government substituting?

5. Discussion