DEVELOPMENTAL PSYCHOLOGY AND ATTACHMENT...
62
DEVELOPMENTAL PSYCHOLOGY AND ATTACHMENT THEORIES Medical psychology seminar Tamás Dömötör SZALAI Semmelweis University, Institute of Behavioural Sciences [email protected] www.behsci.sote.hu
Transcript of DEVELOPMENTAL PSYCHOLOGY AND ATTACHMENT...

DEVELOPMENTAL PSYCHOLOGY AND ATTACHMENT THEORIES Medical psychology seminar Tamás Dömötör SZALAI Semmelweis University, Institute of Behavioural Sciences [email protected] www.behsci.sote.hu

Seminar schedule No seminars: 12th February, 2nd April Sleep lab: 19th February (Tömő st. 25-29. 3rd floor)

Requirements
Participation and absences:
one absence from the lectures and three absences from the seminars.
Evaluation:
Written final examination in the examination period.
Required literature:
Behavior & Medicine, 4th Edition, Danny Wedding, Hogrefe & Huber Publishers, Seattle, 2006.
Content of the lectures (slides)

Introduction of the course
1. Personal introduction
2. Thoughts, expectations
3. As a doctor
How can you utilize psychological knowledge?
What can you use a psychologist for?
4. How would you define medical psychology?

What is medical psychology?
Investigates phenomenons which influence our health and the development / flow of diseases through the central nervous system (CNS).
Internal and external factors, interpersonal relationships etc. (Kopp, 2005, 21. o)

2 main areas
1. Health psychology: psychological and physiological components of
health promotion and prevention 2. Psychosomatic / behavioural medicine: Understanding the role of psychological factors in
most diseases Psychotherapeutic methods in general medical
practice Psychology of suffering and healing Indispensable psychological concepts and
mechanisms of medication Doctor-patient relationship

Hungarians in medical psychology
Hans Selye – Stress theory, general daptation syndrome
Franz Alexander – the 7 most important psychosomatic diseases
Michael Bálint – Der Arzt, Ihr Patient und die Krankheit, the doctor as medicine
Ferenczi Sándor - conversions
Hermann Imre – the instinct of handhold

What is developmental psychology? Definition: a part of psychology which investigates the
physical, mental, emotional and social changes through the lifespan
Aim: to define, describe, and explain the role of certain developmental stages + comparison to others
Why is it important?
The understanding of
age-related changes, behaviour
and the picture of personality
is determining in efficient help

Historical Origins
During the 1900s three key figures have dominated the field of human development:
Jean Piaget (1896-1980),
Lev Vygotsky (1896-1934) and
John Bowlby (1907-1990).
Much of the current research continues to be influenced by these three theorists.

3 main theoretical approaches of developmental psychology
1. Psychoanalytic theories:
influenced by Sigmund Freud (unconscious mind, childhood experiences.)
Freud: development occurs through series of psychosexual stages.
Erik Erikson: expanded Freud's ideas by proposing a stage theory of psychosocial development. Conflicts arise at different stages of development throughout the lifespan.
2. Learning theories:
The environment’s impacts behavior (S-O-R)
Learning processes include classical conditioning, operant conditioning and social learning
behavior is shaped by the interaction between the individual and the environment.
3. Cognitive theories:
development of mental processes, skills, and abilities
Piaget's theory of cognitive development.

Interactions and development
Knowledge about ourselves is based on the interaction with others
Mirroring: a picture is reflected about ourselves -> this is understood and internalised
Self = the essence, conscious and sub-conscious representations about ourself
Self-awareness – self-image – body-image – me- not me
Every child plays an active role in the development of his/her personality: genetic influences, temper, selection of impulses, internalisation-projection etc.

Practice
Draw a „TIMELINE”
Most important life events (from birth until now)
What have influenced your personality, behaviour and motivations?
Draw for 10 minutes
Talk it over with a partner in 10-10 minutes
Biological basis of early personality development Development of sensations and perception:
The infant can not distinguish stimuluses from the mother and from the own body
First visceral sensation dominates
Development goes from internal to external
Bodily contact and tactile sensations (touches, warmth) are highly important for the dominance of exteroception
-> Early interactions are crucial to distinguish the self from the environment and for the development of the nervous system

Positive and negative experiences
Pribram (1984): sensations of warmth, pain or comfort can serve as the primary basis of good and bad experiences according to the intensity of the stimuluses
Determines the goodness of self or the world
Or whether the focus is localised on the own bodily sensations or on the external world
Nexus with early traumas, childhood diseases, separation and psychosomatic vulnerability
Object-constancy

The role of the endogene opiate system
Body contact increases the endogene opiate secretion, with sense of comfort and analgesic effects
Opiates increase the secretion of the growth hormone – psychosial dwarfism
The motivation to be in contact woth social others is maintained even in the case of pain and punishment, or it can even increases!
Seeking of contact in pain (analgesic bacgkround) vs. Social isolation increases the pain reaction
Social and physical pain has the same nervous system center

Effects of early interactions
Positive experiences based on early interactions are also cognitively represented
„everything’s fine / terrible”
Strict or enmashed border with the world
Trust in social others and exploration
Defence mechanisms
Influence on the personality development
Basic attiute to the world: „I am (not) OK you are (not) OK”
Eg. Punisher rather than being abused
Family features
What provides optimal environment and care for a child?
Practice – circles test:
Draw two circles twice:
(1) mother + you
(2) father and you
How would you change the position of the circles to makw it more comfortable?
The role of mothers
Optimal maternal care serves the basis of healthy self-development
Holding from the mother – smell – face – eyes and look
Handling and containg of emotions Unconditonal vs. Conditional acceptance Punishment with withdrawal of love Kohut: mirroring function of the mother and
empathic reactions for the childs inborn features Moternal reactions, care and self-esteem Mirror-neurons Mother-child interaction determines perceptions
of social support and trust in others
Margaret Mahler – differentiation from the mother
Normal autustic stage (0-1 month)
Symbiotic stage (2-4 month)
Differentiation of the body-schema
Detachment (separation and exploration)
Practicing stage
Re-approach to the mother
Stability of the self and the object
Most people have problem either with separation or cloeseness to others

Separation-individuation process
Symbiosis
Differentiation
Practice of own life
Re-approach
Also appears in friendships and romantic relationships
Practice
Mother-child drawing
Impressions, elaboration, special features, strength of the lines, discance of characters, using space, colours etc.
Change a few words about this topic with a partner

The role of fathers
Social reference, norms, socializing functions
Imitation, role-playing
„power for ego”
Oedipal stage and identification
Overidentification with the parents is almost as problemful as the complete lack of identification
Freud’s psychosexual developmental stages The libido (instinct-energy) occupies different body
parts:
1. Oral stage
2. Anal
3. Phallic - 3-6 – oedipal conflict
4. latency
5. Genital stage
Formation of the Superego
Identification with the same sex parent instead of the alliance with the opposite sex parent
Internalisation of the parents and their norms:
Instead of following the external rules - becuse of punishment and reward - the judgement becomes internal
Social roles, norms, moral vaues
Primar concepts about good and bad („wht should be done or mustn’t be done”)
Eg. later self-esteem, anxiety and compulsive states, sadistic superego

Winnicott’s developmental model
- A mother shall be „goog enough”
- Development of innate abilities towards the integration and independency
- Transient object
- When the mother is not good enough (too good/bad) one can build a false / fake self (constant role-play in order to hide or overcompensate)

Parenting styles
1. warm-restrictive -> there are borders, but
acceptance as well -> best way
2. warm-indulgent -> too much space -> impulsive, agressive child
3. cold-restrictive -> when we win, they are broken -> high compliance, low self-esteem, high anxiety
4. cold-indulgent
-> aggressive child with low self-esteem

Videdos
Harlow studies and the need of contact
Self-recognition
Marshmallow test
Egocentrism
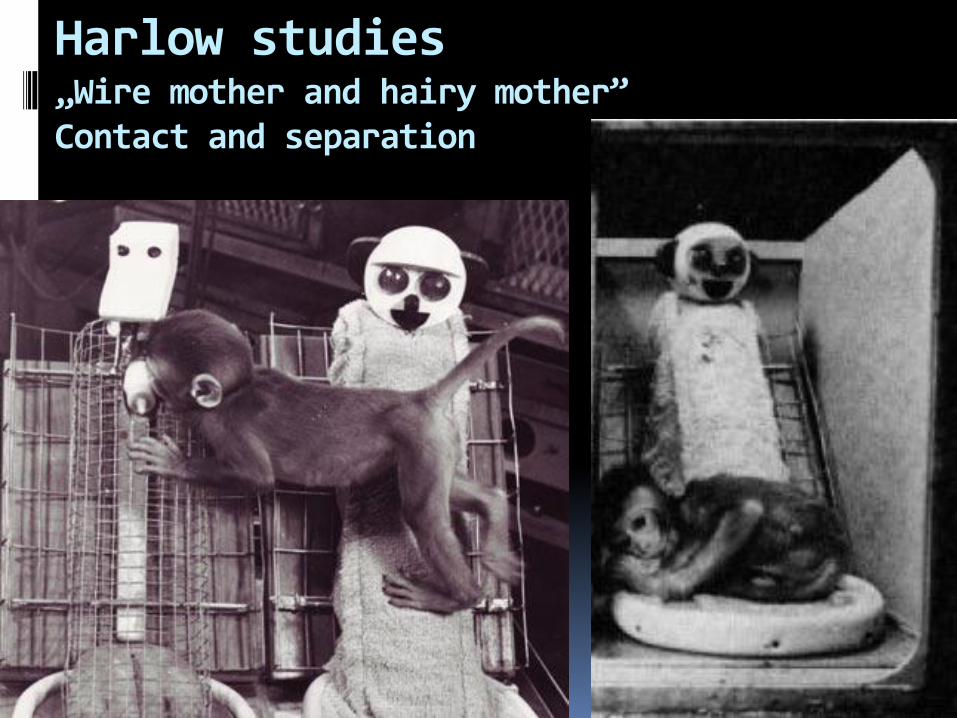
Harlow studies „Wire mother and hairy mother” Contact and separation

The „wire mother” monkeys’ life
No normal social interactions (withdrawal or aggression)
Inappropriate sexual reactions
Female monkeys became bad mothers: mishandling or neglecting their cubs
When contemporary interctions were present in the first 6 month, they became normal adult mokneys

The experience of separation (similar to hospitalization)
When the carer is not present, the infant experiences the lack of care
3 phases of reaction(Bowlby):
1. Protest: strong wish to see the other, who have left him/her. Crying, motoric and psychological agitatedness, problems with eating and sleeping
2. Despair and anger: no trust in reunion. Less crying, slower motor tempo, apathy
3. Acceptance: the child gives up the emotional bound with the attachment figure. Acceptance of the new carer. Somtimes dependent features, sticking to the partner remain present during the whole life.

Conclusions
A basic motivation is to live the closeness of others
In the same time: independency, autonomy, exploration
The child’s tendency to maintain physical safety and psychological comfort with seeking the company and regulating the closeness of social others
Harlow sudies show, that the contact comfort and the sensation of the carers presence is more important than food
The lack of carer causes serious psychological suffering and even physical vulnerability
Huge importance of relationships and attachment

Case Study Separation anxiety and its therapy
Key symptoms
Key intervention points of the treatment
How can you involve the parents?
What is attachment?
Evolutionary grounded, motivational-behavioural system and complex representation about self and significant others
„internal working model” almost determines emotions, expectations, perceptions and defences in interpersonal interactions
„Attachment is held to characterize human beings from the cradle to the grave” (Bowlby)

What are the charctersitics of attachment?
Four functions of attachment: 1. Maintaining of closeness with the attachment
figure 2. Safe refuge to seek comfort of safety 3. Separation anxiety when attachment figure is not
present 4. Safe base of exploration
When attachment in early years in unsuccessful, it can result to the inability for sufficient relationships in adulthood (Bowlby, 1973).
Practice
Strange situation VIDEO
Adult Attachment Scale
Fill out the questionnaire
Chose a partner and make a conversation about own attachment tendencies

Main types of attachment
Ainthwoth – strange situation
A, B, C, D attachment styles

Primary attachment and later relationships As a prototype of relationships, it can
determine our interpretations and reactions
Present feelings in relationships are often underlined by early representations
Determines our need of closeness or intimacy or independence
Strong correlation with the anxiety in all relationships
Trust in self and others

Adult Attachment


Why is attachment important?
Characteristics of childhood attachment infiltrate the personality and provide patterns for later social interactions
Serves as a prototype of relationship dynamics throughout the lifespan
It plays a crucial role also in everyday interactions, just as in psychological problems and psychiatric disorders

Attachment and psychopathology
„Attachment-based mental representations can mediate between the parental treatment and later psychopatological symptomes”
Insecure, anxious attachment may lead to increased stress, higher depression, emotional problems and social conflicts
It also increases the possibility of psychopatological symptoms.
Attchment and doctor-patient relationship
Often influences the doctor-patient relationship (wehen we feel vulnerable, we tend to seek help and care)
1. Preoccupied (self – others +)
higher level of dependence, compulsive seek for help, even intensifying the symptoms, control is at the doctor
-> Shorter visits more often, more reinforcement

Attchment and doctor-patient relationship
2. Avoidant / dismissive (self + others -)
Less emotions, mistrust about helping him/her, minimalization of need for help
Denying or reducing symptoms
keeps the distance and often avoid the controls, low compliance
-> Confirmation of appointments, trust and confidence is important
Attchment and doctor-patient relationship
3. Fearful attachment ( self – others -)
Double bind: asking for help, but in the same time rejecting it
Confused, unpredictable
-> Definition of borders, roles and responsibilities, setting real expectations
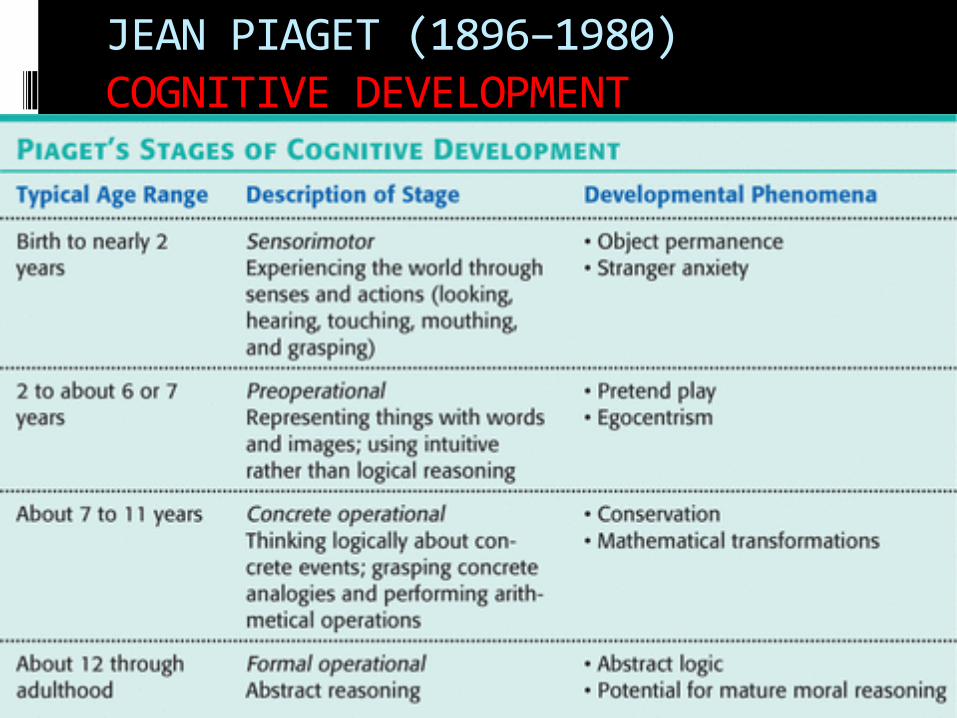
JEAN PIAGET (1896–1980) COGNITIVE DEVELOPMENT

ERIK ERIKSON: PSYCHOSOCIAL DEVELOPMENT


Practice
What stage are you in? What are your basic needs, porposes now?
Imagination of a simple flower

Identity
What is identity? Being identical with myself Acceptance of life-history, abilities, own body, parents, etc. Finding aims, values, partners Definition of myself is needed! Questions: Who / what I am? What sort of a person I
am? Self-esttem is highly important in it Differences of the actual – real – ideal – social self
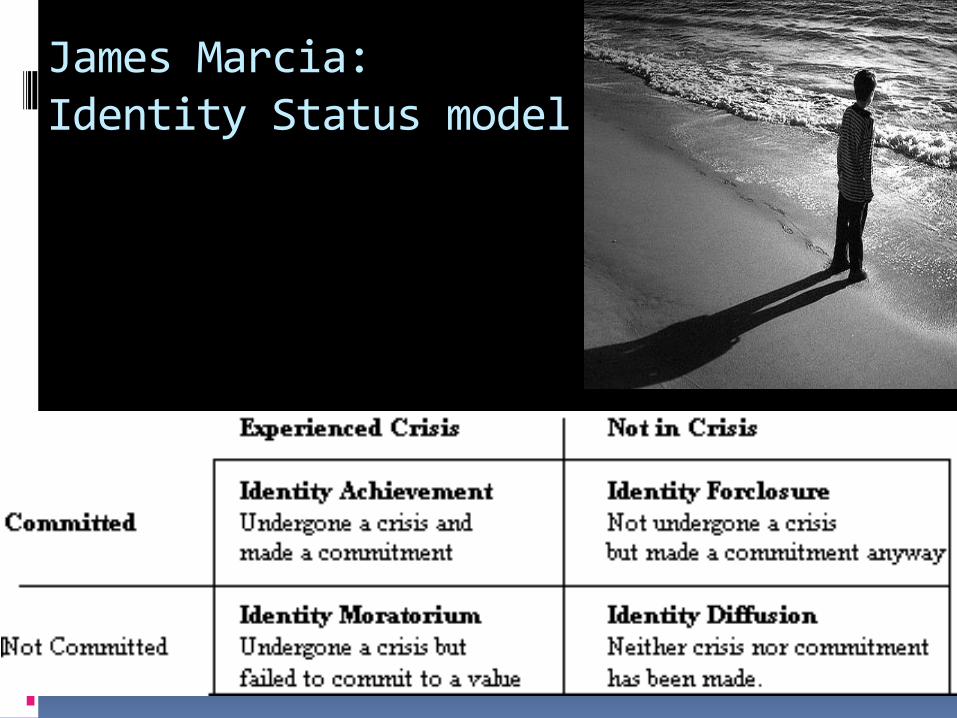
James Marcia: Identity Status model

Signs of the identity status
Practice
Draw a picture of an adolescent
How would you describe his/her state of mind?
What is the biggest problem and aim in their life?
What could be the most important, when communicating with them as a doctor?
Adolescene
Transitive developmental stage Periods (Clauss – Hiebsch): prepuberty 10 –13 years puberty 13 – 17 years adolescence 17-20-24 years Main characteristics: Biological changes, emotional independency, own
values and life-persective, definition of identity, influence of social others, exeptional role of firendships, constant fight with family, seeking ones for identification
Main aims of puberty / adolescence
3 developmental platforms: biological, psychological, sociological 3 main aims: 1. Emotional separation from parents 2. Internalisation of sexual role into the
personality 3. Finding a future role in the society

Frequent medical psychological problems in childhood and adolescence
Psychological factors may be involved in:
Anxiety disorders (separation anxiety, phobias, obsessive-compulsive disorders)
Obesity and emotional eating
Avoidant-restrictive food intake disorder
Impulse-control disorders
Abnormal defecation or urination
Learning or attention deficits (ADHD)
Posstraumatic stress disorders

Frequent medical psychological problems in adolescence
Childhood and adolescence depression Reasons: loosing a beloved person / courage / skill / self-
esteem, physical diseases, learned hopelesneess, constant mistreatment / bullying + meeting with own self is always crisis for the first time
Symptoms: dim / pale eyes, withdrawn lifestyle, problems with eating or sleeping, lack of energy, motivation, interests and courage, sometimes agitatedness, anger, hurting own body
Hidden depression: physical complaints dominate What helps? Human presence, understanding, normalizing
is needed + consultations are almost always required + confute negative automatic thoughts, increasing self-esteem, finding motivation, ressources and aims, social environment and support is a must


Frequent medical psychological problems in adolescence
Somatization
-> Double bind communication
-> Definition of roles
-> early diseases, injuries, traumas
-> Borders are defined and flexible in the family
-> acceptance of the bodily aspects of the self
-> Eds are very frequent!


Recommanded literature
Ainsworth, M.S. (1969). Object relations, dependency, and attachment: a theoretical review of the infant-mother relationship. Cild Development. 1969, 40, 969-1025.

Thak you for your kind attention!