
Artificial Cells Containing Hepatocytes and/or Stem Cells ...
Upload
vivek-dixitCategory
view
213download
0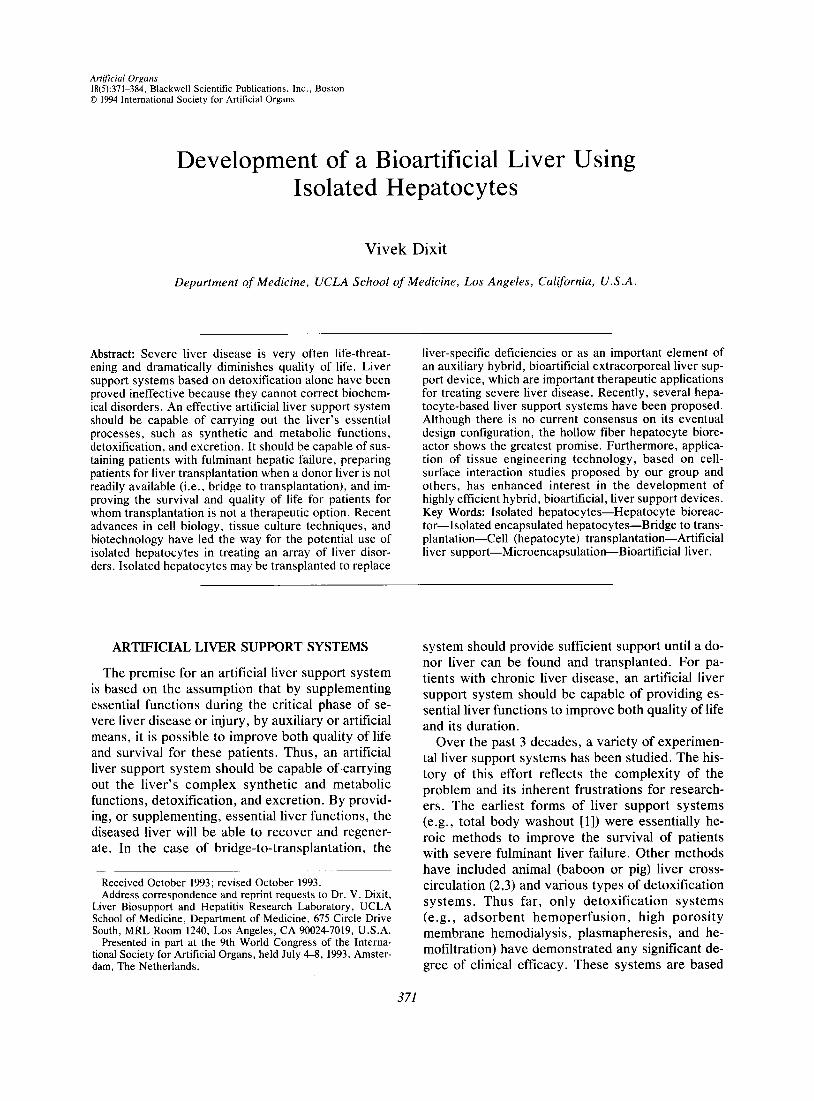
Artificial Organs 18(5):371-384, Blackwell Scientific Publications, Inc., Boston 0 1994 International Society for Artificial Organs
Development of a Bioartificial Liver Using Isolated Hepatocytes
Vivek Dixit
Department of Medicine, UCLA School of Medicine, Los Angeles, California, U.S .A.
Abstract: Severe liver disease is very often life-threat- ening and dramatically diminishes quality of life. Liver support systems based on detoxification alone have been proved ineffective because they cannot correct biochem- ical disorders. An effective artificial liver support system should be capable of carrying out the liver’s essential processes, such as synthetic and metabolic functions, detoxification, and excretion. It should be capable of sus- taining patients with fulminant hepatic failure, preparing patients for liver transplantation when a donor liver is not readily available (i.e., bridge to transplantation), and im- proving the survival and quality of life for patients for whom transplantation is not a therapeutic option. Recent advances in cell biology, tissue culture techniques, and biotechnology have led the way for the potential use of isolated hepatocytes in treating an array of liver disor- ders. Isolated hepatocytes may be transplanted to replace
liver-specific deficiencies or as an important element of an auxiliary hybrid, bioartificial extracorporeal liver sup- port device, which are important therapeutic applications for treating severe liver disease. Recently, several hepa- tocyte-based liver support systems have been proposed. Although there is no current consensus on its eventual design configuration, the hollow fiber hepatocyte biore- actor shows the greatest promise. Furthermore, applica- tion of tissue engineering technology, based on cell- surface interaction studies proposed by our group and others, has enhanced interest in the development of highly efficient hybrid, bioartifcial, liver support devices. Key Words: Isolated hepatocytes-Hepatocyte bioreac- tor-Isolated encapsulated hepatocytes-Bridge to trans- plantation-Cell (hepatocyte) transplantation-Artificial liver support-Microencapsulation-Bioartificial liver.
ARTIFICIAL LIVER SUPPORT SYSTEMS
The premise for an artificial liver support system is based on the assumption that by supplementing essential functions during the critical phase of se- vere liver disease or injury, by auxiliary or artificial means, it is possible to improve both quality of life and survival for these patients. Thus, an artificial liver support system should be capable of carrying out the liver’s complex synthetic and metabolic functions, detoxification, and excretion. By provid- ing, or supplementing, essential liver functions, the diseased liver will be able to recover and regener- ate. In the case of bridge-to-transplantation, the
Received October 1993; revised October 1993. Address correspondence and reprint requests to Dr. V . Dixit,
Liver Biosupport and Hepatitis Research Laboratory, UCLA School of Medicine, Department of Medicine, 675 Circle Drive South, MRL Room 1240, Los Angeles, CA 90024-7019, U.S.A.
Presented in part at the 9th World Congress of the Interna- tional Society for Artificial Organs, held July 4-8, 1993, Amster- dam, The Netherlands.
system should provide sufficient support until a do- nor liver can be found and transplanted. For pa- tients with chronic liver disease, an artificial liver support system should be capable of providing es- sential liver functions to improve both quality of life and its duration.
Over the past 3 decades, a variety of experimen- tal liver support systems has been studied. The his- tory of this effort reflects the complexity of the problem and its inherent frustrations for research- ers. The earliest forms of liver support systems (e.g., total body washout [I]) were essentially he- roic methods to improve the survival of patients with severe fulminant liver failure. Other methods have included animal (baboon or pig) liver cross- circulation (2,3) and various types of detoxification systems. Thus far, only detoxification systems (e.g., adsorbent hemoperfusion, high porosity membrane hemodialysis, plasmapheresis, and he- mofiltration) have demonstrated any significant de- gree of clinical efficacy. These systems are based
3 71

3 72 V. DIXIT
on the hypothesis that liver failure and its compli- cations can be reversed if the associated toxins are removed from the circulation. Indeed, detoxifica- tion systems have been reported to promote the re- covery of consciousness in patients in deep hepatic coma (4-6).
Currently, however, intensive critical care man- agement is the only therapy available to patients with severe life-threatening liver disease. Recently, orthotopic liver transplantation has become a suc- cessful alternative for such patients (7); however, this procedure is highly costly, complex, and lim- ited by a scarcity of donor livers (8) and by the limited time that donor livers can be preserved (9). A growing population of patients are likely to die waiting for a liver transplant either because of scar- city of organs available for transplantation or be- cause they are too sick to be transplanted. Thus, there is a growing and compelling need for an arti- ficial liver support system for sustaining patients with fulminant hepatic failure; preparing patients for liver transplantation when a donor liver is not readily available (i.e., bridge-to-transplanta- tion), or sustaining patients when a transplanted liver fails; and improving the survival and quality of life for patients for whom liver transplantation is not a therapeutic option.
It is now evident from experimental and clinical data that physical methods alone (i.e., detoxifica- tion) cannot sufficiently manage the complex bio- chemical disorders seen in severe liver disease. Re- cently, advances in biotechnology and tissue engineering have brought back into focus the im- portance of a biological component for a hybrid bio- artificial support system. Of the numerous ap- proaches being developed, the biological approach shows the greatest promise of being able to assume the full range of liver functions (10,ll). These ex- perimental endeavors are based on the hypothesis that hepatic assist for a failing or diseased liver can best be achieved with isolated liver cells (i.e., he- patocyte transplantation and the use of isolated he- patocytes in extracorporeal hepatocyte bioreac- tors).
HEPATOCYTE TRANSPLANTATION
Transplantation of isolated healthy hepatocytes to supplement failing or deficient liver function is an innovative technique that offers a variety of impor- tant applications. Treatment of liver disease by transplantation of healthy hepatocytes can also have significant implications for organ replacement therapy (12-14). Compared with whole organ trans-
plantation, it is a technically simple procedure that offers numerous advantages. For example, it may be possible in the future for relatives of patients to donate small samples of liver cells for transplanta- tion, or 1 intact liver could be used to treat many patients. Unlike whole organs, cells could also be cryopreserved for future use (14). During the last decade, various experimental approaches for trans- plantation of healthy isolated hepatocytes, with pre- viously limited success ( 1 9 , were investigated with very promising results. Hepatocyte transplantation showed considerable promise in being able to as- sume the full range of liver functions in several an- imal models of liver disease ranging from fulminant hepatic failure to congenital metabolic liver disease (10,11,1~18) .
Several hepatocyte transplantation sites have been reported in the literature. Among the first sites was the liver itself, which is the intuitively ideal site because it represents an optimal environment for the hepatocytes. However, this procedure led to hepatocyte aggregates in distal portal branches, si- nusoids, and central veins, resulting in extensive hepatic necrosis, severe portal hypertension, and pulmonary hypertension (19). Other sites have in- cluded subcutaneous tissue, intracapsular dorsal fat pads, muscle, peritoneum, renal capsule, lungs, and spleen (16,20). Among these sites, only the spleen (2 I ,22) and the peritoneal cavity (10,11,21,23-29) have shown any real measure of success. Between these 2 sites, the intraperitoneal route is by far the most advantageous. Intraperitoneal transplantation is a simple technique that causes negligible trauma to the recipient animal (1 1). The intraperitoneal route also allows several orders of magnitude greater quantities of hepatocytes to be transplanted as compared with the intrasplenic route (10,11,22).
Intrasplenic transplantation of hepatocytes Intrasplenic transplantation of hepatocytes is a
simple procedure that has been reported by several groups with varying degrees of success (21,30-33). This technique essentially involves injection of a small suspension of isolated hepatocytes into the splenic pulp. The hepatocytes then attach to and grow in the splenic red pulp to form hepatic cords and sinusoids. Splenic white pulp does not permit proliferation of implanted hepatocytes. Intrasplenic hepatocyte transplantation is not always reproduc- ible because transplanted hepatocytes often embo- lize to the liver or into the circulation, where they may die. Ebata et al. (30). demonstrated the forma- tion of a “hepatized” spleen (Fig. l) following in- trasplenic transplantation of syngeneic hepatocytes
Artif Organs, Vol. 18, No. 5 , 1994
DEVELOPMENT OF A BIOARTIFICIAL LIVER 3 73
FIG. 1. Cut surface of a hepatized spleen 27 months after transplantation. A suspension of freshly isolated syngeneic hepato- cytes was injected directly into the splenic pulp of the recipient animal. The transplanted hepatocytes proliferated in the splenic red pulp to occupy nearly two thirds of the splenic mass (Reprinted with permission) (32).
for the treatment of impaired liver function. One year after transplantation, the hepatocytes were functionally active and were reported to correct the inherited glucuronyltransferase deficiency in Gunn rats (3 1 ) . Despite such results, this interesting pro- cedure has many limitations. First, this technique requires long-term immunosuppressive therapy if other than syngeneic hepatocytes are transplanted. Furthermore, the hepatic tissue that can be accom- modated by the spleen (-3% of normal liver weight) is not sufficient to support an animal with severe liver failure. Finally, a very long time ( -1 year) is required to “hepatize” the spleen. Therefore, in- trasplenic hepatocyte transplantation does not ap- pear to be feasible.
Intraperitoneal transplantation of hepatocytes Pioneering studies of intraperitoneal transplanta-
tion of hepatocytes produced temporary but en- couraging results (15,23). It was not widely recog- nized that the peritoneal milieu did not offer suitable attachment sites for the anchorage-depen- dent hepatocytes, thus limiting their life span. In-
traperitoneal transplantation of hepatocytes did not advance further until recent developments in micro- carrier and microencapsulation technology, which can provide suitable attachment substrates. With microcarrier and microencapsulation techniques, intraperitoneally transplanted isolated hepatocytes have shown tremendous promise in being able to assume the full range of liver functions in several animal models of severe liver disease (10,11,14,17, 18,2 1).
HYBRID BIOARTIFICIAL LIVER SUPPORT SYSTEMS
Hybrid bioartificial forms of liver support couple biological and synthetic components. This process is best exemplified by intraperitoneal transplanta- tion of isolated hepatocytes using microcarrier and microencapsulation technology. Advances in tech- nology allowed a previously limited technique to demonstrate the greatest promise of being able to assume the full range of liver functions in several
Art$ Organs. Vol. 18, No. 5. 1994

374 V . DIXIT
animal models of severe liver disease (10,11,14,17, 18,21). Currently, hybrid liver support systems in- clude microcarrier-attached hepatocytes, microen- capsulated hepatocytes, and extrahepatic liver sup- port systems (hepatocyte bioreactors).
Microcarrier-attached hepatocytes Microcarriers have been available for use in tis-
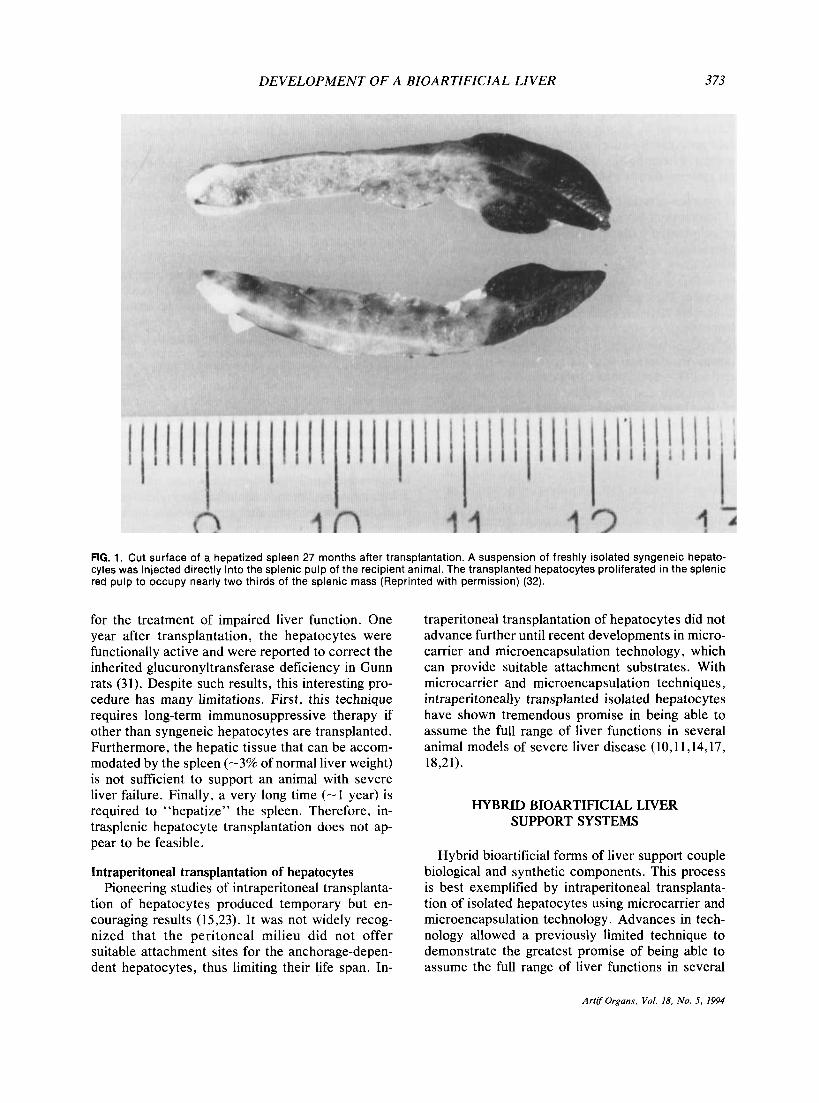
sue culture and biotechnology for more than 1 de- cade; however, their application in cell transplanta- tion studies is recent (10,21,24). Microcarriers provide essential attachment substratum for the he- patocytes. Their enormous surface area-to-volume relationship facilitates transplantation of huge quan- tities of hepatocytes in very small volumes of mi- crocarrier suspensions (Fig. 2). The first cell trans- plantation studies with microcarrier-attached hepatocytes were reported by Demetriou et al. (lo), who demonstrated the feasibility for restoration of deficient liver function in 2 animal models of con- genital metabolic liver defects: hyperbilirubinemia and analbuminemia. In these studies, microcarrier- attached hepatocytes were intraperitoneally trans- planted into hyperbilirubinemic Gunn rats and anal- buminemic Nagase rats, resulting in a significant decrease in hyperbilirubinemia and elevation in al- bumin levels in the respective animal models (Fig. 3). In cross-species experiments with isolated hu- man hepatocytes, this group demonstrated similar results in these animal models (25). They also showed that intraperitoneally transplanted micro- carrier-attached hepatocytes could significantly im- prove the survival of rats undergoing 90% partial hepatectomy (17), demonstrating that the trans- planted hepatocytes provided significant metabolic support while the hepatectomized animals’ livers regenerated (17).
Subsequently, other investigators demonstrat- ed significant reduction of serum LDL levels in
Microcarriers / I
FIG. 2. Microcarrier-attached hepatocytes. The enormous surface area-to-volume relationship of the microcarriers can facilitate transplantation of large quantities of hepatocytes in very small volumes of microcarrier suspensions.
congenitally hyperlipidemic Watanabe rabbits fol- lowing intraperitoneal transplantation of microcar- rier-attached hepatocytes (21). Intraperitoneal transplantation of microcarrier-attached hepato- cytes has also been shown to significantly improve the long-term survival of rats with galactosamine- induced fulminant hepatic failure (27). Recently, we developed biologically modified polyhydroxymeth- ylmethacrylate (Poly HEMA) microcarriers (Fig. 4) for high hepatocyte immobilization (>75% cover- age of the microcarriers as compared with approx- imately 25% coverage with collagen-coated dextran microcarriers) and function to provide optimal liver-specific metabolic function in experimental studies (34). Thus, the data from several centers strongly suggest that intraperitoneally transplanted, microcarrier-attached hepatocytes can provide sig- nificant metabolic support in animal models of both acute and chronic (congenital) metabolic liver dis- ease. However, without adequate immunosuppres- sion, hepatocyte rejection remained a significant problem in these trials (10,17,24).
Microencapsulated hepatocytes Microencapsulation techniques for hepatocyte
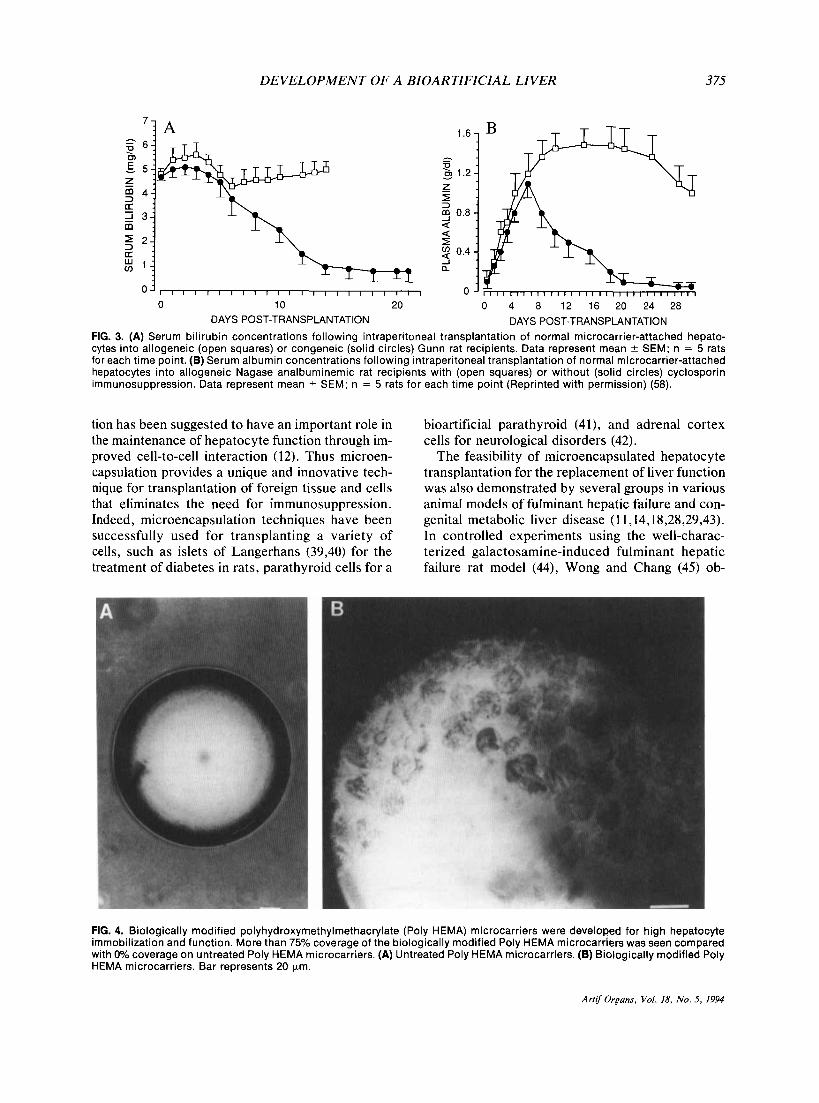
transplantation evolved after the successful exper- iments with microcarrier-attached hepatocytes de- scribed. Unlike microcarrier-attached hepatocytes, microencapsulating hepatocytes circumvent the need for immunosuppression. The technology for microencapsulation was derived from Chang’s pio- neering work (35) and the more recent application of this technique by Lim (36) and Sun et al. (37) for encapsulating islets of Langerhans. Microcapsules are synthetic, spherical, polymeric structures that are composed of ultrathin, semipermeable mem- branes of cellular dimensions (35). The microcap- sule membrane can be prepared from various poly- mers; its contents can consist of tissue or cells, enzymes, or other biologically active materials (38). The membrane prevents the contents of the micro- capsule from leaking out and causing immunologi- cal reactions, but still allows those contents to in- teract freely in biological reactions. In addition, this membrane keeps unwanted substances, such as cells and antibodies, from entering the microcap- sule (Fig. 5) .
In contrast to the microcarrier studies described, in which hepatocytes are cultured on the exterior surface of collagen-coated microcarriers (see Fig. 2), hepatocytes are microencapsulated within a three-dimensional collagen matrix separated from the external environment by a semipermeable mem- brane (see Fig. 5) . This three-dimensional orienta-
Art$ Organs, Vol. 18. No. 5 , 1994
DEVELOPMENT OF A BIOARTIFICIAL LIVER
1.6-
h .
P 0) 1.2-
z v
5 uj 0.8 - a a I
3 a "'"- 0 -
375
0 10 20 DAYS POST-TRANSPLANTATION
1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
0 4 8 12 16 20 24 28 DAYS POST-TRANSPLANTATION
FIG. 3. (A) Serum bilirubin concentrations following intraperitoneal transplantation of normal microcarrier-attached hepato- cytes into allogeneic (open squares) or congeneic (solid circles) Gunn rat recipients. Data represent mean ? SEM; n = 5 rats for each time point. (B) Serum albumin concentrations following intraperitoneal transplantation of normal microcarrier-attached hepatocytes into allogeneic Nagase analbuminemic rat recipients with (open squares) or without (solid circles) cyclosporin immunosuppression. Data represent mean ? SEM; n = 5 rats for each time point (Reprinted with permission) (58).
tion has been suggested to have an important role in the maintenance of hepatocyte function through im- proved cell-to-cell interaction (12). Thus microen- capsulation provides a unique and innovative tech- nique for transplantation of foreign tissue and cells that eliminates the need for immunosuppression. Indeed, microencapsulation techniques have been successfully used for transplanting a variety of cells, such as islets of Langerhans (39,40) for the treatment of diabetes in rats, parathyroid cells for a
bioartificial parathyroid (4 l ) , and adrenal cortex cells for neurological disorders (42).
The feasibility of microencapsulated hepatocyte transplantation for the replacement of liver function was also demonstrated by several groups in various animal models of fulminant hepatic failure and con- genital metabolic liver disease (1 1,14,18,28,29,43). In controlled experiments using the well-charac- terized galactosamine-induced fulminant hepatic failure rat model (44), Wong and Chang (45) ob-
FIG. 4. Biologically modified polyhydroxymethylmethacrylate (Poly HEMA) microcarriers were developed for high hepatocyte immobilization and function. More than 75% coverage of the biologically modified Poly HEMA microcarriers was seen compared with 0% coverage on untreated Poly HEMA microcarriers. (A) Untreated Poly HEMA microcarriers. (B) Biologically modified Poly HEMA microcarriers. Bar represents 20 pm.
Artif OrEans, Vol. 18, No. 5, 1994
3 76
175 - 150 - 125 -
100 - 75 - 50 -
25 - 0 -
V . DIXIT
IMPERMEABLE SUBSTANCES eg. Hepdtocytes, Lymphocytes, Antibodies, Bacteria, etc.
PERMEABLE SUBSTRATES ( S ) , PRODUCTS (P) eg. Ammonia, Phenols, Mercaptans, Fatty Acids, Bile Salts.
Albumin, Clotting Factors, etc. - FIG. 5. Microencapsulated hepatocytes. Microcapsules are synthetic, spherical, polymeric structures that are composed of ultrathin, semipermeable membranes of cellular dimen- sions. The membrane prevents the contents of the microcap- sule from leaking out and causing immunological reactions, but still allows those contents to interact freely in biological reactions. In addition, this membrane keeps unwanted sub- stances (e.g., cells and antibodies) from entering the micro- capsule.
served that the survival time of rats with liver fail- ure could be significantly increased if microencap- sulated hepatocytes were transplanted in late stages of hepatic coma. Furthermore, we reported (18) in the same animal model that if microencapsulated hepatocytes were transplanted in earlier stages of liver failure, a highly significant increase in the
h
[A cr: 3 0 z
overall survival rate of rats was achieved when compared with untreated control animals or control animals treated with empty microcapsules (Fig. 6). The animals in these studies received no immuno- suppression. Because fulminant hepatic failure es- sentially requires support only during the critical phase of liver injury, these studies demonstrated the effectiveness of microencapsulated hepatocyte transplantation for short-term liver support.
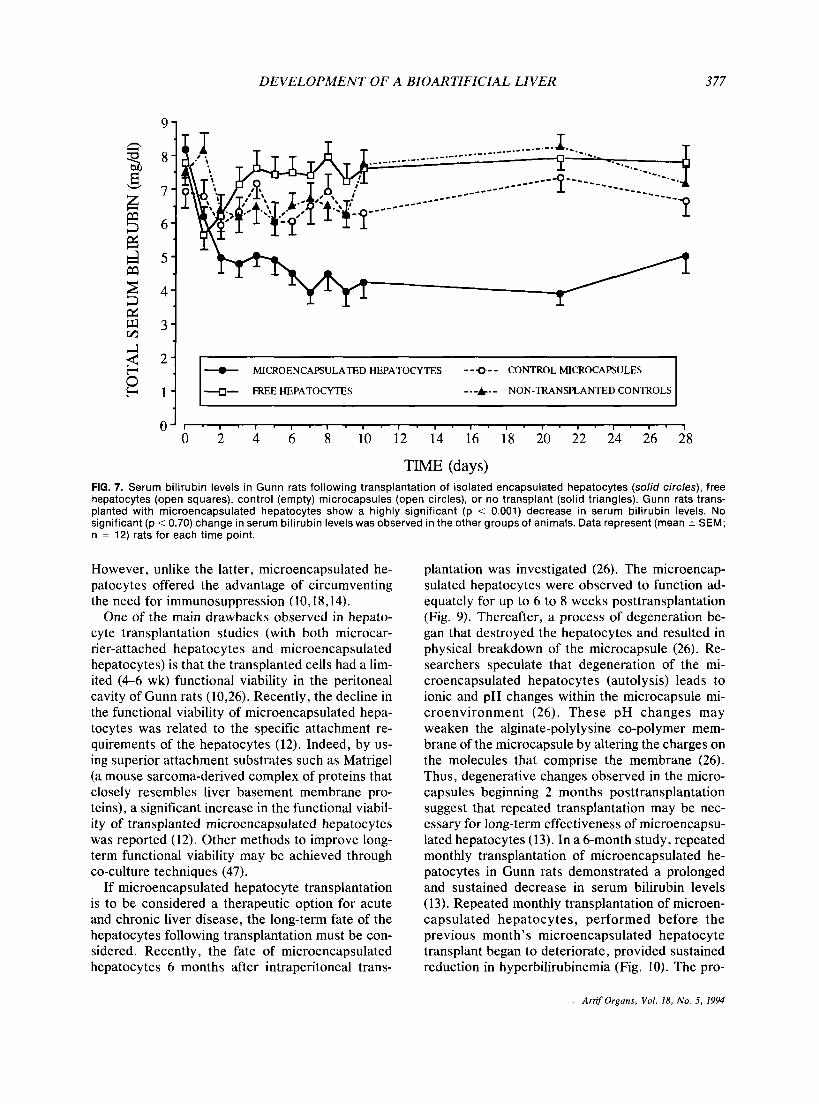
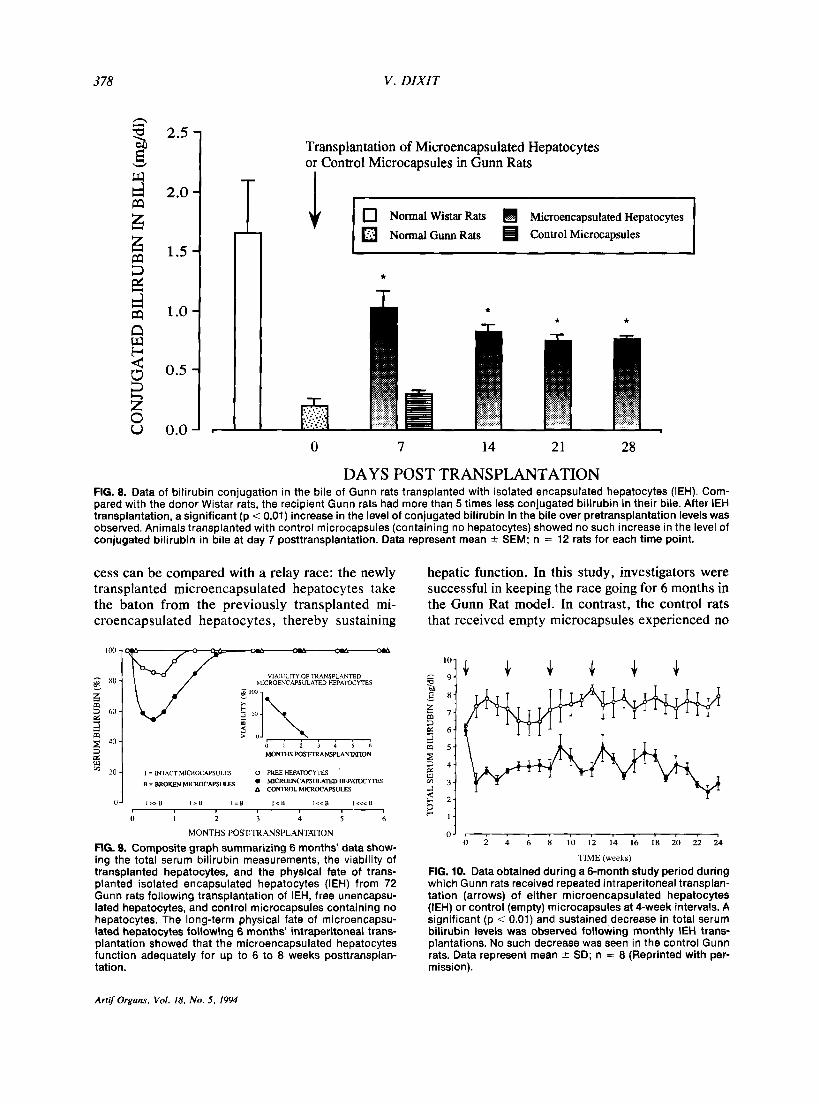
A major requirement of an acceptable artificial liver support system is that it must be effective for long-term supplementation of liver function. Sev- eral studies evaluated long-term effectiveness using the Gunn rat model. Gunn rats are congenitally de- ficient in the liver enzyme bilirubin-uridine diphos- phate glucuronyltransferase and are therefore un- able to conjugate bilirubin. This enzyme deficiency results in lifelong, nonhemolytic, unconjugated hy- perbilirubinemia in these animals (46). In long-term studies, the effectiveness of microencapsulated he- patocytes was evaluated for the replacement of a specific liver function in Gunn rats (1 1,14,29). These studies showed that transplanted microen- capsulated hepatocytes significantly lowered the level of hyperbilirubinemia (Fig. 7) in Gunn rats fol- lowing a single transplantation of microencapsu- lated hepatocytes (1 1,14). Also, concurrent with the decrease in serum bilirubin levels a significant in- crease in conjugated bilirubin in bile (Fig. 8) was also detected (12,14). These studies effectively demonstrated that transplanted microencapsulated hepatocytes were as competent as transplanted un- encapsulated, microcarrier-attached hepatocytes in providing liver function in Gunn rats (10,11,14).
B Grade I Coma
I U
- 50
5 M
- 25 v
- 0 CONTROL IEH NTx CONTROL IEH FHC
FIG. 6. Survival time and survival rate data following intraperitoneal transplantation of isolated encapsulated hepatocytes (IEH) in galactosamine-induced fulminant hepatic failure rats. A highly significant (p < 0.01) increase in survival time and rate was observed following IEH transplantation. (A) Animals treated in Grade II coma (mean * SEM, n = 14) (Reprinted with permission) (18). (B) Animals treated in Grade I coma (mean 2 SEM, n = 16) (Reprinted with permission) (18).
Artif Organs. Vol. 18. No, 5 , 1994
DEVELOPMENT OF A BIOARTIFICIAL LIVER
3 -
2 -
1-
377
+ MICROENCAPSULATED HEPATOCYTES --0 -- CONTROL MICROCAPSULES
4- FREE HEPATOCYTES ---).- NON-TRANSPLANTED CONTROLS
FIG. 7. Serum bilirubin levels in Gunn rats following transplantation of isolated encapsulated hepatocytes (solid circles), free hepatocytes (open squares), control (empty) microcapsules (open circles), or no transplant (solid triangles). Gunn rats trans- planted with microencapsulated hepatocytes show a highly significant (p < 0.001) decrease in serum bilirubin levels. No significant (p < 0.70) change in serum bilirubin levels was observed in the other groups of animals. Data represent (mean 2 SEM; n = 12) rats for each time point.
However, unlike the latter, microencapsulated he- patocytes offered the advantage of circumventing the need for immunosuppression (10,18,14).
One of the main drawbacks observed in hepato- cyte transplantation studies (with both microcar- rier-attached hepatocytes and microencapsulated hepatocytes) is that the transplanted cells had a lim- ited (4-6 wk) functional viability in the peritoneal cavity of Gunn rats (10,26). Recently, the decline in the functional viability of microencapsulated hepa- tocytes was related to the specific attachment re- quirements of the hepatocytes (12). Indeed, by us- ing superior attachment substrates such as Matrigel (a mouse sarcoma-derived complex of proteins that closely resembles liver basement membrane pro- teins), a significant increase in the functional viabil- ity of transplanted microencapsulated hepatocytes was reported (12). Other methods to improve long- term functional viability may be achieved through co-culture techniques (47).
If microencapsulated hepatocyte transplantation is to be considered a therapeutic option for acute and chronic liver disease, the long-term fate of the hepatocytes following transplantation must be con- sidered. Recently, the fate of microencapsulated hepatocytes 6 months after intraperitoneal trans-
plantation was investigated (26). The microencap- sulated hepatocytes were observed to function ad- equately for up to 6 to 8 weeks posttransplantation (Fig. 9). Thereafter, a process of degeneration be- gan that destroyed the hepatocytes and resulted in physical breakdown of the microcapsule (26). Re- searchers speculate that degeneration of the mi- croencapsulated hepatocytes (autolysis) leads to ionic and pH changes within the microcapsule mi- croenvironment (26). These pH changes may weaken the alginate-polylysine co-polymer mem- brane of the microcapsule by altering the charges on the molecules that comprise the membrane (26). Thus, degenerative changes observed in the micro- capsules beginning 2 months posttransplantation suggest that repeated transplantation may be nec- essary for long-term effectiveness of microencapsu- lated hepatocytes (13). In a 6-month study, repeated monthly transplantation of microencapsulated he- patocytes in Gunn rats demonstrated a prolonged and sustained decrease in serum bilirubin levels (13). Repeated monthly transplantation of microen- capsulated hepatocytes, performed before the previous month's microencapsulated hepatocyte transplant began to deteriorate, provided sustained reduction in hyperbilirubinemia (Fig. 10). The pro-
ArtifOrgans, Vol. 18, NO. 5 , 1994
378 V . DIXIT
2.5
2.0
1.5
1 .o
0.5
0.0
Transplantation of Microencapsulated Hepatocytes or Control Microcapsules in Gunn Rats
Normal Wistar Rats Microencapsulated Hepatocytes
Normal Gunn Rats Control Microcapsules
0 7 14 21 28
DAYS POST TRANSPLANTATION FIG. 8. Data of bilirubin conjugation in the bile of Gunn rats transplanted with isolated encapsulated hepatocytes (IEH). Com- pared with the donor Wistar rats, the recipient Gunn rats had more than 5 times less conjugated bilirubin in their bile. After IEH transplantation, a significant (p < 0.01) increase in the level of conjugated bilirubin in the bile over pretransplantation levels was observed. Animals transplanted with control microcapsules (containing no hepatocytes) showed no such increase in the level of conjugated bilirubin in bile at day 7 posttransplantation. Data represent mean & SEM; n = 12 rats for each time point.
cess can be compared with a relay race: the newly transplanted microencapsulated hepatocytes take the baton from the previously transplanted mi- croencapsulated hepatocytes, thereby sustaining
VIABILITY OF TRANSPLANTED MICROENCAPSLLATED HEPATOCYTES
- 3 MONTHS FOSTTRANSPLANWION ' 2" 1 I = WTACT MICROCAPSULES 0 FREE HEPALYTES
= BROKEN MIcRoc~psuLEs 0 MICROENCAPSULATED HEPATOCYTES A CONTROL MICROCAPSULES
il 1 ; 3 i ; 4
MONTHS POST-TRANSPLANTAHON
FIG. 9. Composite graph summarizing 6 months' data show- ing the total serum bilirubin measurements, the viability of transplanted hepatocytes, and the physical fate of trans- planted isolated encapsulated hepatocytes (IEH) from 72 Gunn rats following transplantation of IEH, free unencapsu- lated hepatocytes, and control microcapsules containing no hepatocytes. The long-term physical fate of microencapsu- lated hepatocytes following 6 months' intraperitoneal trans- plantation showed that the microencapsulated hepatocytes function adequately for up to 6 to 8 weeks posttransplan- tation.
hepatic function. In this study, investigators were successful in keeping the race going for 6 months in the Gunn Rat model. In contrast, the control rats that received empty microcapsules experienced no
0 2 4 6 8 1 0 12 14 16 I8 20 22 24 0 J , , r , , , , , , , , , (
TIME (weeks)
FIG. 10. Data obtained during a 6-month study period during which Gunn rats received repeated intraperitoneal transplan- tation (arrows) of either microencapsulated hepatocytes (IEH) or control (empty) microcapsules at 4-week intervals. A significant (p < 0.01) and sustained decrease in total serum bilirubin levels was observed following monthly IEH trans- plantations. No such decrease was seen in the control Gunn rats. Data represent mean k SD; n = 8 (Reprinted with per- mission).
Artf Organs, Vol. 18, No. 5 , 1994

DEVELOPMENT OF A BIOARTIFICIAL LIVER 3 79
reduction in hyperbilirubinemia (see Fig. 10). The experimental animals tolerated the transplanted mi- crocapsules well, and there were no adverse side effects (e.g., inflammation, sepsis, irritation).
For microencapsulated hepatocyte transplanta- tion to provide a viable form of artificial liver sup- port (e.g., as a bridge-to-transplantation), or as an alternative to orthotopic liver transplantation, it must not only offer substantial therapeutic benefit to the recipient but also must be simple and conve- nient to use. Large quantities of healthy microen- capsulated hepatocytes must be readily available for transplantation when required. In concept, a fa- cility akin to a blood bank, in which microencapsu- lated hepatocytes could be stored and used as needed, would be ideal. Unfortunately, free hepa- tocytes in suspension are far more sensitive than other types of cells and are easily damaged by ca- sual handling. Furthermore, primary cultures of iso- lated hepatocytes do not store well because hepa- tocytes start to dedifferentiate within a few days (48). Although cryopreservation is a standard pro- cedure for preserving bone marrow as well as var- ious cell lines, it can inflict considerable injury to free suspensions of hepatocytes (48). Recently, we cryopreserved microencapsulated hepatocytes and showed that microencapsulation protects the hepa- tocytes from damage and allows them to be stored simply, conveniently, and inexpensively (14). Fur- thermore, cryopreserved, microencapsulated hepa- tocytes functioned as well as freshly prepared, non- frozen microencapsulated hepatocytes both in vitro and in vivo (14). Thus, transplantation of cryopre- served microencapsulated hepatocytes may provide a convenient therapeutic option for the manage- ment of fulminant hepatic failure, as well as of in- born errors of metabolism, without need for immu- nosuppression.
Isolated hepatocyte and extracorporeal hepatocyte bioreactors
Hepatocyte bioreactors are extracorporeal de- vices for auxiliary supplementation of liver function during disease. Such bioreactors usually consist of hepatic tissue cultivated as primary cultures of iso- lated hepatocytes or as a liver cell line (4%51). In the past, pieces of liver tissue and liver slices were also used with limited success (52,53). Although suspension cultures are the easiest to cultivate, they also are the most short-lived because hepatocytes are anchorage-dependent (48,54). Thus, hepatocyte cultures on membranes, microcarriers, and micro- capsules, which have a longer life span, are usually used. In conjunction with cryopreserved, microcar-
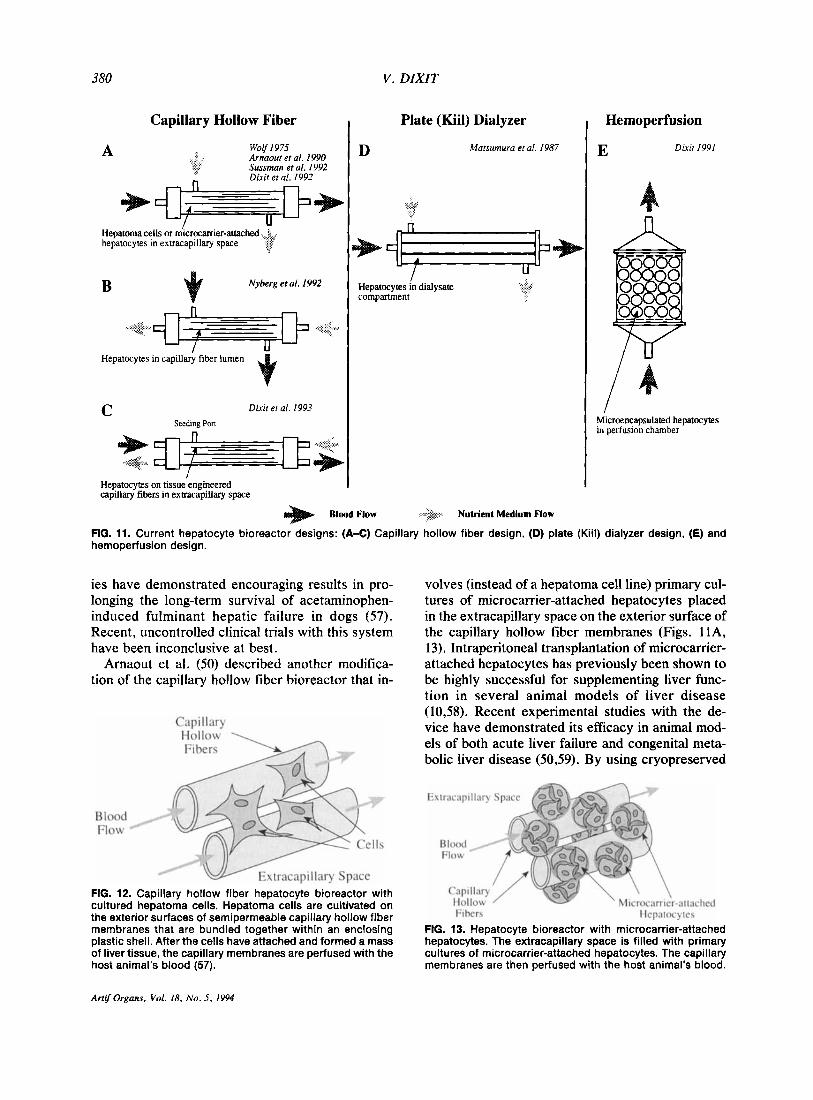
rier-attached hepatocytes and cryopreserved mi- croencapsulated hepatocytes, bioreactors have the distinct advantages of long-term storage; they can be prepared in advance and can be used off-the- shelf as needed (50,SS). The design characteristics of hepatocyte bioreactors have been based on the conventional renal hemodialysis system because of its physiological approach (i.e., counter-current blood flow design) to blood detoxification and its mass transfer characteristics (56). These designs are also advantageous because they are engineered for compactness and adaptability to high pressure op- eration in a form convenient for perfusion by blood. Thus far, 3 basic bioreactor design configurations have been proposed: capillary hollow fiber systems, plate dialyzer systems, and hemoperfusion systems (Fig. 11).
Capillary hollow fiber hepatocyte bioreactors The capillary hollow fiber hepatocyte bioreactor
design was first proposed by Wolf and Munkelt (49). This design involves cultivation of hepatoma cells (or primary hepatocytes) on the exterior sur- faces of semipermeable capillary hollow fiber mem- branes that are bundled together within an enclos- ing plastic shell (Figs. 1 IA, 12). Nutrient medium is circulated within the capillaries until the hepato- cytes attach and form a mass of liver tissue. The capillary membranes are then perfused with the host animal’s blood. In theory, the cells resting on the capillary membranes’ exterior surface and within the plastic shell should provide hepatic met- abolic function, and a symbiotic relationship should be established between the host and the cultured hepatocytes through the capillary membrane. In such a system, the cultured hepatocytes are pro- tected from the body’s immune system by the semi- permeable capillary membrane.
Recently, 4 prototype versions of capillary hol- low fiber membrane-based bioreactors were re- ported in the literature. Sussman et al. (57) de- scribed a system that is essentially the same as the pioneering design of Wolf and Munkelt (49) de- scribed (see Figs. 11A, 12); however, instead of the Reuber hepatoma cell line, this group used a new cell line known as C3A (57). The C3A cell line was described as a stable, well differentiated, clonaly- derived, hepatoma cell of human origin that grows to very high densities and is strongly contact- inhibited (57). The rationale for a hepatoma cell line is that it can provide a steady supply of large quan- tities of hepatocyte-like cells: It is not known whether hepatoma cells will cause any detrimental effects to the recipient. Limited experimental stud-
Artif Organs, Vol. 18. No. 5 , 1994
380 V . DZXZT
Capillary Hollow Fiber
Wolf I975 Arnaour er al. I990 Sussman et al. I992 Dixit et al. 1992
A
Hepatoma cells +J=P or rnrcrocamer-attached < hepatocytes in exaacaplllary space
Nyberg et al. I992 B
- Hepatocytes in capillary fiber lumen
Dixit er al. 1993 Seedina Pon
C
Hepatocytes on tissue engineered capillary fibers in exaacapillary space
Plate (Kiil) Dialyzer
Matsumura et al. 1987 D
Hepatocytes - in dialysate
compartment
Hemoper fusion
Dixit 1991 E
Microencapsulated hepatocytes in perfusion chamber
Blood Flow -3 Nutrient Medium Flow
FIG. 11. Current hepatocyte bioreactor designs: (A-C) Capillary hollow fiber design, (D) plate (Kiil) dialyter design, (E) and hemoperfusion design.
ies have demonstrated encouraging results in pro- longing the long-term survival of acetaminophen- induced fulminant hepatic failure in dogs (57). Recent, uncontrolled clinical trials with this system have been inconclusive at best.
Arnaout et al. (50) described another modifica- tion of the capillary hollow fiber bioreactor that in-
Capillary Hollow
Blood Flow
FIG. 12. Capillary hollow fiber hepatocyte bioreactor with cultured hepatoma cells. Hepatoma cells are cultivated on the exterior surfaces of semipermeable capillary hollow fiber membranes that are bundled together within an enclosing plastic shell. After the cells have attached and formed a mass of liver tissue, the capillary membranes are perfused with the host animal's blood (57).
volves (instead of a hepatoma cell line) primary cul- tures of microcarrier-attached hepatocytes placed in the extracapillary space on the exterior surface of the capillary hollow fiber membranes (Figs. 11A, 13). Intraperitoneal transplantation of microcarrier- attached hepatocytes has previously been shown to be highly successful for supplementing liver func- tion in several animal models of liver disease (10,58). Recent experimental studies with the de- vice have demonstrated its efficacy in animal mod- els of both acute liver failure and congenital meta- bolic liver disease (5039). By using cryopreserved
Extracapillary Space
Fibers Hepatocytes
FIG. 13. Hepatocyte bioreactor. with microcarrier-attached hepatocytes. The extracapillary space is filled with primary cultures of microcarrier-attached hepatocytes. The capillary membranes are then perfused with the host animal's blood.
Artif Organs, Vol. 18, NO. 5 , 1994
DEVELOPMENT OF A BIOARTIFICIAL LIVER 381
Blood Flow
Hepatocytes Entrapped in Collagen Gel
Extracapillary Space
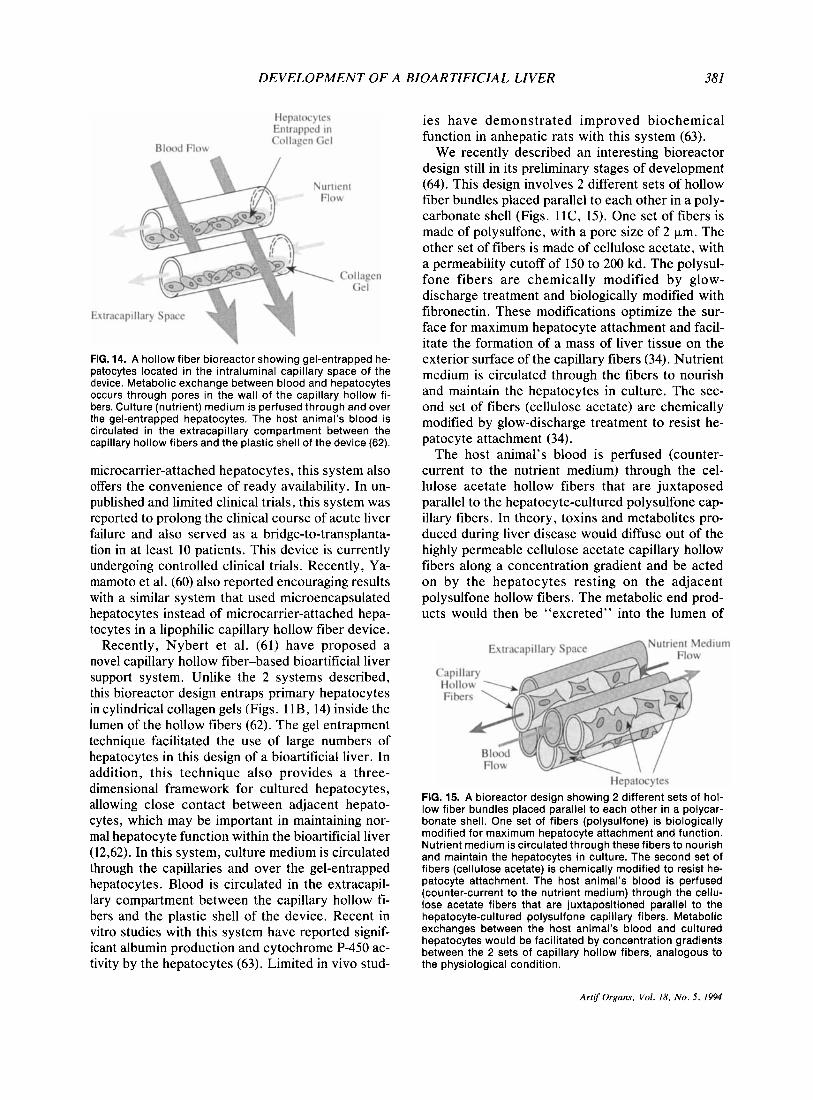
FIG. 14. A hollow fiber bioreactor showing gel-entrapped he- patocytes located in the intraluminal capillary space of the device. Metabolic exchange between blood and hepatocytes occurs through pores in the wall of the capillary hollow fi- bers. Culture (nutrient) medium is perfused through and over the gel-entrapped hepatocytes. The host animal’s blood is circulated in the extracapillary compartment between the capillary hollow fibers and the plastic shell of the device (62).
microcarrier-attached hepatocytes, this system also offers the convenience of ready availability. In un- published and limited clinical trials, this system was reported to prolong the clinical course of acute liver failure and also served as a bridge-to-transplanta- tion in at least 10 patients. This device is currently undergoing controlled clinical trials. Recently, Ya- mamoto et al. (60) also reported encouraging results with a similar system that used microencapsulated hepatocytes instead of microcarrier-attached hepa- tocytes in a lipophilic capillary hollow fiber device.
Recently, Nybert et al. (61) have proposed a novel capillary hollow fiber-based bioartificial liver support system. Unlike the 2 systems described, this bioreactor design entraps primary hepatocytes in cylindrical collagen gels (Figs. 1 lB, 14) inside the lumen of the hollow fibers (62). The gel entrapment technique facilitated the use of large numbers of hepatocytes in this design of a bioartificial liver. In addition, this technique also provides a three- dimensional framework for cultured hepatocytes, allowing close contact between adjacent hepato- cytes, which may be important in maintaining nor- mal hepatocyte function within the bioartificial liver (12,62). In this system, culture medium is circulated through the capillaries and over the gel-entrapped hepatocytes. Blood is circulated in the extracapil- lary compartment between the capillary hollow fi- bers and the plastic shell of the device. Recent in vitro studies with this system have reported signif- icant albumin production and cytochrome P-450 ac- tivity by the hepatocytes (63). Limited in vivo stud-
ies have demonstrated improved biochemical function in anhepatic rats with this system (63).
We recently described an interesting bioreactor design still in its preliminary stages of development (64). This design involves 2 different sets of hollow fiber bundles placed parallel to each other in a poly- carbonate shell (Figs. 11C, 15). One set of fibers is made of polysulfone, with a pore size of 2 pm. The other set of fibers is made of cellulose acetate, with a permeability cutoff of 150 to 200 kd. The polysul- fone fibers are chemically modified by glow- discharge treatment and biologically modified with fibronectin. These modifications optimize the sur- face for maximum hepatocyte attachment and facil- itate the formation of a mass of liver tissue on the exterior surface of the capillary fibers (34). Nutrient medium is circulated through the fibers to nourish and maintain the hepatocytes in culture. The sec- ond set of fibers (cellulose acetate) are chemically modified by glow-discharge treatment to resist he- patocyte attachment (34).
The host animal’s blood is perfused (counter- current to the nutrient medium) through the cel- lulose acetate hollow fibers that are juxtaposed parallel to the hepatocyte-cultured polysulfone cap- illary fibers. In theory, toxins and metabolites pro- duced during liver disease would diffuse out of the highly permeable cellulose acetate capillary hollow fibers along a concentration gradient and be acted on by the hepatocytes resting on the adjacent polysulfone hollow fibers. The metabolic end prod- ucts would then be “excreted” into the lumen of
Nutrient Medium
Hepatocytes FIG. 15. A bioreactor design showing 2 different sets of hol- low fiber bundles placed parallel to each other in a polycar- bonate shell. One set of fibers (polysulfone) is biologically modified for maximum hepatocyte attachment and function. Nutrient medium is circulated through these fibers to nourish and maintain the hepatocytes in culture. The second set of fibers (cellulose acetate) is chemically modified to resist he- patocyte attachment. The host animal’s blood is perfused (counter-current to the nutrient medium) through the cellu- lose acetate fibers that are juxtapositioned parallel to the hepatocyte-cultured polysulfone capillary fibers. Metabolic exchanges between the host animal’s blood and cultured hepatocytes would be facilitated by concentration gradients between the 2 sets of capillary hollow fibers, analogous to the physiological condition.
Artif Organs, Vol. 18, No, 5 , 1994
V . DIXIT
the polysulfone capillary fibers along a concentra- tion gradient and be removed by the circulating nu- trient medium. Concurrently, essential proteins and factors produced by the hepatocytes would diffuse along a concentration gradient and be taken up by the cellulose acetate capillary fibers lying alongside the hepatocytes. Thus, adequate liver function could be simulated, as in the physiological condi- tion. The semipermeable capillary hollow fiber membranes would protect the cultured hepatocytes from the body's immune system. Preliminary stud- ies show that tissue engineering techniques are ef- fective in creating highly specific hepatocyte attach- ment surfaces for optimal hepatocyte function in this bioreactor design. Current problems with this design relate mainly to fabrication of the bioreactor.
PLATE DIAL.YZERS The plate, or Kiil, hemodialyzer hepatocyte
bioreactor system was first proposed by Matsumura et al. (65). A suspension, monolayers, or primary hepatocytes are cultured on multiple membranous plates in a configuration that allows blood to flow in a counter-current direction over the opposite side of the semipermeable membrane (Fig. 11D). Thus far, except for one case report on the dramatic improve- ment of a single fulminant hepatic failure patient, no experimental data with animal models have been published (65). Another Japanese group reported in- conclusive in vitro data with this system (66). Basic in vitro and in vivo studies are needed to evaluate the efficacy of this system.
HEPATOCYTE HEMOPERFUSION The hepatocyte hemoperfusion bioreactor design
essentially allows for the direct perfusion of blood over microencapsulated hepatocytes placed in an extracorporeal chamber. Because free hepatocytes can cause immunological reactions, we proposed that microencapsulated hepatocytes could be placed directly in a chamber through which the pa- tient's blood would be perfused (55). Because a spherical microcapsule membrane has the greatest surface area-to-volume relationship of any shape, maximum nutrient/product exchange across the mi- crocapsule membrane may be achieved by using mi- croencapsulated hepatocytes in a liver bioreactor (55) . Our group previously demonstrated the effi- cacy of transplanted microencapsulated hepato- cytes in providing significant metabolic support in animal models of severe liver disease. However, recent unpublished results showed that current mi- croencapsulation techniques do not consistently produce microcapsules that can withstand the high
shear stresses that would be expected in an extra- corporeal device with high blood flow velocities. Thus, until a more durable microcapsule membrane is developed, this system may not be effective in providing adequate hepatic function. Recently, groups in Japan have reported a similar system in which hepatocytes entrapped in calcium alginate hydrogels exhibited significant ammonia metabo- lism and urea synthesis (67). Also, recent in vivo perfusion experiments in cats with acute liver fail- ure indicated that such a system is able to provide liver function for up to 4 h (67).
FUTURE PERSPECTIVES The development of artificial liver support sys-
tems is still in its infancy. Several types of artificial liver support systems have been described. No one system has been proven as the ideal form of artifi- cial liver support, which is not surprising because the liver is a highly complex metabolic organ. It is increasingly evident that a multifactorial approach to liver support is necessary. For example, depend- ing on the type and severity of liver disease, detox- ification and biologically based liver support sys- tems may need to be combined to provide adequate liver support.
Recent cell culture and biotechnological ad- vances have brought bioartificial liver support sys- tems into a very exciting period of development. Many groups are actively developing bioreactors with an enthusiasm that has prompied some to limit animal testing and to forge ahead with clinical trials. Unfortunately, such trials do not permit the careful, controlled testing of devices that is warranted. Thus, to avoid the pitfalls of previous generations of artificial liver support research and to facilitate ob- jective comparison of the efficacy of various bioar- tificial liver support systems, we propose the fol- lowing guidelines. All liver biosupport systems should be tested in controlled animal experiments with well-characterized and reproducible animal models of liver diseases. The number of hepato- cytes, or mass of liver tissue, to be used in biore- actor devices should be standardized. Currently, different systems utilize widely divergent quantities of cells or liver tissue. Experimental studies should clearly define treatment end-points. Hepatocyte bioreactor treatment protocols should be standard- ized with regard to duration and frequency of treat- ment. Current protocols suggest treatment times ranging from 2 to 48 hours. Also, some protocols disagree as to whether treatment should be contin- uous or intermittent. Reliable assessment criteria should be established for evaluating hepatocyte
Artif Organs, Vol. 18, No, 5 , 1994
DEVELOPMENT OF A
bioreactors using transformed cell lines and primary hepatocyte cell cultures. Currently, there are some conflicting reports on whether transformed cell lines exhibit essential liver metabolic functions such as those involving P450 enzyme systems.
Other areas of future interest include the use of fetal liver tissue for both hepatocyte transplantation and extrahepatic liver assist systems. Fetal tissue offers significant advantages in that it may be trans- planted across the histocompatibility barrier, poten- tially eliminating the need for immunosuppression following transplantation. However, important eth- ical questions must be resolved before fetal tissue can be freely used. Finally, recent tissue engineer- ing studies suggest it may be possible, given the right polymer supports (scaffoldings) and hepato- cyte attachment substrates, to produce liver orga- noids. These organoids could be transplanted or used in extracorporeal hepatocyte bioreactor sys- tems (34,68-70). In the future, gene therapy tech- niques may enable a functional gene to be inserted into defective liver cells of patients. Autologous transplantation of such corrected cells would re- store a previously deficient liver function. The future of hepatocyte transplantation and its use in extra- corporeal bioreactor devices is promising. Carefully controlled animal trials are now necessary to bring this technology from the bench to the bedside.
1 .
2.
3.
4.
5 .
6.
7 .
8.
9.
10.
1 1 .
REFERENCES Klebanoff G, Hollander D, Cosimi AB, et al. Asanguineous hypothermic total body perfusion (TBF) in the treatment of stage IV hepatic coma. J Surg Res 1972;12:1. Hollander D, Klebanoff G, Osteen RT. Human-baboon cross circulation for treatment of hepatic coma. J Am Med Assoc 197 1 ;2 18:67. Tonnesen K. Cross-circulation in experimental hepatic fail- ure in the pig. Liver 1986;6262-7. Starzl TE, Chang TMS, Williams R, Nose Y. Liver support/ transplants and artificial organs: panel conference. Trans Am SOC Artif Intern Organs 1983;29:795-9. Chang TMS. Liver support systems. In: Bartlett R, White- house WM, Turcotte JG, eds. Life Support Systems in In- tensive Care. Year Book, 1984:461-85. Hughes RD, Nagaki M, Keane H, Sheron N, Williams R. Artificial liver support in acute liver failure: A review of studies at King’s. Artif Organs 1992;16:167-70. Martin P, Munoz SJ, Friedman LS. Liver transplantation for viral hepatitis: Current status. Am J Gastroenterol 1992;87: 409-18. Van Thiel DH, Makowka L, Starzl TE. Liver transplanta- tion: Where it’s been and where it’s going. CIin Gastroen- terol 1988; 17: 1-18. Blankensteijn JD, Terpstra OT. Liver preservation: The past and the future. Hepatology 1991;13:1235. Demetriou AA, Whiting JF, Feldman D, Levenson SM, Chowdhury NR, Moscioni AD, Kram M, Chowdhury JR. Replacement of liver function in rats by transplantation of microcarrier-attached hepatocytes. Science 1986;233: 119&2. Dixit V, Darvasi R, Arthur M, Brezina M, Lewin K, Gitnick G. Restoration of liver function in Gunn rats without immu-
BIOAR TIFICIAL LIVER 383
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
nosuppression using transplanted microencapsulated hepa- tocytes. Hepatology 1990;12:1342-9. Dixit V, Darvasi R, Arthur M, Lewin KJ, Gitnick G. Im- proved function of microencapsulated hepatocytes in a hy- brid bioartificial liver support system. Artif Organs 1992; 16: 3 3 6 4 1 . Dixit V, Arthur M, Gitnick G. Repeated transplantation of microencapsulated hepatocytes for sustained correction of hyperbilirubinemia in Gunn rats. Cell Transplant 1992;l:
Dixit V, Darvasi R, Arthur M, Lewin KJ, Gitnick G. Cryo- preserved microencapsulated hepatocytes: transplantation studies in Gunn rats. Transplantation 1993;55:61622. Matas AJ, Sutherland DE, Steffes MW, Mauer SM, Lowe A, Simmons RL, Najarian JS. Hepatocellular transplanta- tion for metabolic deficiencies: decrease of plasma bilirubin in Gunn rats. Science 1976;192:892-4. Fuller BJ. Transplantation of isolated hepatocytes. A review of current ideas. J Hepatol 1988;7:368-76. Demetriou AA, Reisner A, Sanchez J, Levenson SM, Mos- cioni AD, Chowdhury JR. Transplantation of microcamer- attached hepatocytes into 90% partial hepatectomized rats. Hepatology 1988;8: 1006-9. Dixit V, Gordon VP, Pappas SC, Fisher MM. Increased sur- vival in galactosamine induced fulminant hepatic failure in rats following intraperitoneal transplantation of isolated en- capsulated hepatocytes. In: Baquey C, Dupuy B, eds. Hy- brid Artificial Organs, vol 177. Paris, France: Colloque INSERM , 1 989: 257-64. Rivas P, Fabrega AJ, Schwartz D, Digiantis W, Pollak R. Preservation and transplantation of purified canine hepato- cytes. Transplant Proc 1992;24:2833-6. Sandbichler P, Then P, Vogel W, Erhart R, Dietze 0, Phil- adelphy H, Fridrich L, Kilima G, Margreiter R. Hepatocel- lular transplantation into the lung for temporary support of acute liver failure in the rat. Gastroenterology 1992;102:605-9. Weiderkehr JC, Kondos GT, Pollak R. Hepatocyte trans- plantation for the low-density lipoprotein receptor-deficient state. Transplantation 1990;50466-76. Selden C, Darby H, Hodgson HJF. Further observations on the survival, proliferation and function of ectopically im- planted syngeneic and allogeneic liver cells in rat spleen. Eur J Gastroenterol Hepatol 1991;3:607-1 I . Makowka L, Falk RE, Rotstein LE, Falk JA, Nossal N, Langer B, Blendis LM, Phillips MJ. Cellular transplantation in the treatment of experimental hepatic failure. Science 1980;210:901-3. Demetriou AA, Levenson SM, Novikoff PM, Novikoff AB, Chowdhury NR, Whiting JF, Reisner A, Chowdhury JR. Survival, organization, and function of microcarrier- attached hepatocytes transplanted in rats. Proc Natl Acad Sci USA 1986;83:7475-9. Moscioni AD, Chowdhury JR, Barbour R, Brown LL, Chowdhury NR, Competiello LS, Lahiri P, Demetriou AA. Human liver cell transplantation: prolonged function in athy- mic-Gunn and athymic-analbuminemic hybrid rats. Gastro- enterology 1989;96: 154651. Dixit V, Arthur M, Gitnick G . A morphological and func- tional evaluation of transplanted isolated encapsulated he- patocytes following long-term transplantation in Gunn rats. Biomater Artif Cells lmmob Biotechnol 1993;21:119-33. Nagaki M, Kano T, Muto Y, Yamada T, Ohnishi H, Mori- waki H. Effects of intraperitoneal transplantation of micro- carrier-attached hepatocytes in D-galactosamine induced acute liver failure rats. Gastroenrerol Jpn 1990;25:78-87.
275-9.
28. Cai ZH, Shi ZQ, Sherman M, Sun AM. Development and evaluation of a system of microencapsulation of primary rat hepatocytes. Hepatology 1989; 1083540.
29. Bruni S, Chang TMS. Hepatocytes immobilized by microen- capsulation in artificial cells: effects on hyperbilirubinemia in Gunn rats. Biomater ArtfCells Artif Organs 1989;17:403-1 I .
A r t f o r g u n s , Vol. 18, NO. 5 , 1994
384 V . DIXIT
30. Ebata H, Kusano M, Onishi T, Saito T, Mito M. Liver re- generation utilizing isolated hepatocytes transplanted into the rat spleen. Surg Forum 1978;29:33840.
31. Mito M, Kusano M, Onishi T, Saito T, Sakamoto S. Mor- phology and function of isolated hepatocytes transplanted into rat spleen. Transplantation 1979;28:499-505.
32. Mito M, Kusano M. Hepatocyte transplantation in man. Cell Transplant 1993;2:65-74.
33. Nordlinger B, Bouma ME, Wang SR, Ballet F, Verthier N, Huguet C, Infante R. High-yield preparation of porcine he- patocytes for long survival after transplantation in the spleen. Eur Surg Res 1985;17:377-82.
34. Dixit V, Piskin E, Arthur M, Denizli A, Tuncel S. Denkbas E, Gitnick G. Hepatocyte immobilization on PHEMA mi- crocarriers and its biologically modified forms. Cell Trans- plant 1992;1:391-9.
35. Chang TMS. Semipermeable microcapsules. Science 1964; 1465265.
36. Lim F. Microencapsulation of living cells and tissues: The- ory and practice. In: Lim F, ed. Biomedical Applications of Microencapsulation. Boca Raton, FL: CRC Press, 1984: 137-54.
37. Sun AM, Cai ZH, Shi ZQ, Ma FZ, O’Shea GM, Gharapetian H. Microencapsulated hepatocytes as a bioartificial liver. Trans A m Soc Artiflntern Organs 1986;32:3941.
38. Chang TMS. Artificial cells in medicine and biotechnology. Appl Biochem Biotechnol 1984;10:5-24.
39. Sun AM, Lim F, Van Rooy H, O’Shea GM. Long-term stud- ies of microencapsulated islets of Langerhans: A bioartificial endocrine pancreas. Artif Organs 1981;5:784-6.
40. Lacy PE, Hegre OD, Gerasidimi-Vazeou A, Gentile FT, Di- onne KE. Maintenance of normoglycemia in diabetic mice by subcutaneous xenografts of encapsulated islets. Science 1991;254:17824.
41. Fu XW, Sun AM. Microencapsulated parathyroid cells as a bioartificial parathyroid. Transplantation 1989;47:432.
42. Aebischer P, Tresco PA, Winn SR, Green LA, Jaeger CB. Long-term cross-species brain transplantation of a polymer encapsulated dopamine-secreting cell line. Exp Neurol 1991 ; I 1 l:267.
43. Miura Y, Akimoto T, Kanazawa H, Yagi K. Synthesis and secretion of protein by hepatocytes entrapped within cal- cium alginate. Artif Organs 1986;10:460-5.
44. Dixit V, Chang TMS. Brain edema and the blood brain bar- rier in galactosamine-induced fulminant hepatic failure rats: an animal model for evaluation of liver support systems. ASAIO Trans 1990;36:21-7.
45. Wong H, Chang TMS. Bio-artificial liver: Implanted artifi- cial cells microencapsulated living hepatocytes increases survival of liver failure rats. Int J ArfifOrgans 1986;9:335-6.
46. Yeary RA, Grothaus RH. The Gunn rat as an animal model in comparative medicine. Lab Animal Sci 1971;21:362-6.
47. Guguen-Guillouzo C, Clement B, Baffet G, Beaumont C, Morel-Chaney E, Glaise D, Guillouzo A. Maintenance and reversibility of active albumin secretion by adult rat hepato- cytes co-cultured with another liver epithelial cell type. Exp Cell Res 1983;143:47-54.
48. Berry MN, Edwards AM, Bamtt GJ. Isolated hepatocytes preparation, properties and application. In: Burdon RH, van Knippenberg PH, eds. Laboratory Techniques in Biochem- istry and Molecular Biology. Amsterdam: Elsevier, 1991: 395.
49. Wolf CFW, Munkelt BE. Bilirubin conjugation by artificial liver composed of cultured cells and synthetic capillaries. Trans A m SOC Artiflntern Organs 1976;21: 16-27,
50. Arnaout WS, Moscioni AD, Barbour RL, Demetriou AA. Development of bioartificial liver: Bilirubin conjugation in Gunn rats. J Surg Res 1990;48:379-82.
51. Jauregui HO, Gann KL. Mammalian hepatocytes as a foun- dation for treatment in human liver failure. J Cell Biochem 1991 ;45:35945.
52. Kimura K , Gundermann KJ, Lie TS. Hemoperfusion over small l iver pieces for l iver support . Art i f Organs
53. Soyer T, Lempinen M, Walker JE, et al. Extracorporeal assist of anhepatic animals with liver slice perfusion. Am J Surg 1973 ; 126: 20-4.
54. Gerlach J , Kloppel K, Schauwecker HH, Tauber R, Miiller C, Biicherl ES. Use of hepatocytes in adhesion and suspen- sion cultures for liver support bioreactors. Int J Artif Organs 1989; 12:788-92.
55. Dixit V. Isolated hepatocytes and their potential use in the development of an artificial liver. Proceedings of the Third International Conference on the Use of Human Cells, Tis- sues and Organs in Research, NDRI, Washington, DC, USA, pp. 196-199, 1991.
56. Wolf CFW. Cells cultured on artificial capillaries and their use as a liver support device. Artif Organs 1980;4:279-84.
57. Sussman NL, Chong MG, Koussayer T, He D, Shang TA, Whisennand HH, Kelly JH. Reversal of fulminant hepatic failure using an extracorporeal liver assist device. Hepatol- ogy 1992; 16:6O-5.
58. Demetriou AA, Flecher A, Moscioni AD, Hepatocyte trans- plantation: a potential treatment for liver disease (confer- ence report). Dig Dis Sci 1991;36:1320-6.
59. Williams FR, Rozga J , Arnaout W, Moscioni AD, Wingard R, Hakim M, Demetriou AA. Bioartificial liver in the treat- ment of experimental liver failure. Hepatology 1990;12:838.
60. Yamamoto T, Kasai S, Kakisaka A, Ohe N, Mito M. New hepatocyte preparation for metabolic assist device on artifi- cial liver support. Artif Organs 1990;14:276-9.
61. Nyberg SL, Platt JL, Shirabe K, Payne WD, Hu WS, Cerra FB. Immunoprotection of xenocytes in a hollow fiber bioar- tificial liver (xenocyte bioartificial liver). ASAlO J 1992;38:
62. Nyberg SL, Shatford RA. Peshwa MV, White JG, Cerra FB, Hu WS. Evaluation of a hepatocyte entrapment hollow fiber bioreactor: A potential bioartificial liver. Biotech Bioeng 1993;41: 194-203.
63. Nyberg SL, Payne WD, Amiot B, Shirabe K, Remmel RP, Hu WS, Cerra FB. Demonstration of biochemical function by extracorporeal xenohepatocytes in an anhepatic animal model. Transplant Proc 1993;25:1944-5.
64. Dixit V, Piskin E, Denizli A, Kozluca A, Arthur M, Gitnick G . Preliminary studies on the design of an extracorporeal bioartificial liver support device with tissue engineering technology. Hepatology 1994 (in press).
65. Matsumura KN, Guevara GR, Huston H, Hamilton WL, Rikimaru M, Yamasaki G, Matsumura MS. Hybrid bioarti- ficial liver in hepatic failure: Preliminary clinical report. Sur- gery 1987; 101 :99-103.
66. Uchino J, Tsuburaya T, Kumagai F , Hase T, Hamada T, Komai T, Funatsu A, Hashimura E, Nakamura K, Kon T. A hybrid bioartificial liver composed of multiplated hepatocyte monolayers. ASAIO Trans 1988;34:972-7.
67. Yanagi K, Ookawa K, Mizuno S, Oshima N. Performance of a new artificial liver support system using hepatocytes en- trapped within a hydrogel. Trans A m Soc Artiflntern Or- gans 1989;35:570-2.
68. Anselme K, Bacques C, Charriere G, Hartmann DJ, Herb- age D, Garrone R. Tissue reaction to subcutaneous implan- tation of a collagen sponge. A histological, ultrastructural, and immunological study. J Biomed Muter Res 1990;24: 689-703.
69. Vacanti JP, Morse MA, Saltzman WM, Domb AJ, Perez- Atayde A, Langer R. Selective cell transplantation using absorbable artificial polymer matricies. J Pediatr Surg 1988;
70. Mooney D, Hansen L, Vacanti J , Langer R, Farmer S, Ingber D. Switching from differentiation to growth in hepa- tocytes: control by extracellular matrix. J Cell Physioll992;
1980;4:297-301.
M463-7.
23 3-9.
151 ~497-505.
ArtifOrgans, Vol. 18, No. 5 , 1994


















