Development and Validation of B rief Cognitive tool for ... · Adriana Hermida, MD NNDC...
32
Development and Validation of B rief Cognitive tool for Patients Receiving ECT ECT Task Group Adriana Hermida, MD Director, Geriatric Psychiatry Fellowship Department of Psychiatry and Behavioral Science Emory University School of Medicine
Transcript of Development and Validation of B rief Cognitive tool for ... · Adriana Hermida, MD NNDC...

Development and Validation of Brief Cognitive tool for Patients Receiving ECT
ECT Task Group
Adriana Hermida, MDDirector, Geriatric Psychiatry Fellowship
Department of Psychiatry and Behavioral ScienceEmory University School of Medicine

NNDC ECT Task Group
Task Group
Mustafa Husain, MD (Co-Chair)
Richard Weiner, MD, PhD (Co-Chair)
James Beeghly, MD
David Casey, MD
Andrew Francis, MD
Adriana Hermida, MD Sarah H. Lisanby, MD
Daniel Maixner, MD
Kevin Reeves, MD
Irving M. Reti, MD
Nelson Rodriguez, MD
Shirlene M. Sampson, MD
Stephen Seiner, MD
Salih Selek, MD
Neurocognitive sub-group:
Richard Weiner, MD, PhD
Mustafa Husain, MD
Irving Reti, MD
Daniel Maixner, MD
Shawn McClintock, PhD
Adriana Hermida, MD

Emory Group
Felicia Goldstein, PhD
David Loring, PhD
Limin Peng, PhD
Zixun Ye, MSPH
Susan Henderson, NP
Patricio Riva-Posse, MD William McDonald, MD
Adriana Hermida, MD
NNDC Collaborators
ECCA Group of Collaborators
Richard Weiner, MD, PhD
Mustafa Husain, MD
Irving Reti, MD
Daniel Maixner, MD
Shawn McClintock, PhD
International Collaborators
Aida de Arriba-Arnaú, MD
Mikel Urretavizcaya, MD, PhD
JM Mechón, MD
V. Soria MD

NNDC Task Group Response

• FDA considers ECT machine as Class III (high risk)• ECT devices were grandfathered (pre-market notification)
In 2009, the Government Accountability Office recommended that the FDA require that all such “grandfathered” devices be either reclassified into Class I or Class II (intermediate-risk) or undergo premarket approval
In Jan 2011, FDA Neurological Devices Advisory Panel met to discuss their assessment of the evidence regarding effectiveness and safety of ECT.
Weiner R, lisanby SH, Husain MM, Morales OG, Maixner DF, Hall SE, Beeghly J, Greeden JF; National Network of Depression Centers. Electroconvulsive therapy device classification: response to FDA advisory panel hearing and recommendations. J Clin Psychiatry. 2013 Jan;74(1):38-42.
FDA Classification
Effectiveness on acute beneficial response was supported but a major focus of the FDA was on memory
dysfunction.

Early detection of emerging cognitive side effects is extremely important.
Adjustment of treatment approach can be made in order to minimize severe long term memory problems.
Introduction

1 Personal Memory Questionnaire (PMQ)
7 CUAMI Columbia University Autobiographical Memory Inventory
7
2 Squire Subjective Memory Questionnaire (SSMQ)
3 Autobiographical Memory Inventory (AMI)
4 ECT Retrograde Amnesia and Perception Scale (ERAPS)
5 The Personal and Impersonal Memory Test (PIMT–P)
6 Goldberg-Barnett Remote Memory Questionnaire
Memory Tests in ECT

MoCA and MMSE
Nasreddine ZS, Phillips NA, Bedirian V, et al 2005. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 53:695–699Folstein MF, Folstein SE, McHugh PR. 1975. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 12:189–198.

Current Issues

Current Issues
The ECT field is in need of a short, easy to administer, stand-alone, sensitive tool.
Specific to the ECT cognitive domains.

Development of BriefCognitive Tool

12
ECCA Electroconvulsive Cognitive Assessment
Short tool specific for ECT.
Assessment of: subjective memory, autobiographical memory, attention, recall.
Quick and easy to administer (4 to 6 min).
To be done before the first ECT, prior to the 6th ECTs, at the end (1 to 3 weeks after finishing the acute course).
The goal is not to replace neuropsychological testing, but to be used instead of the MoCA and MMSE.
It could be done over the phone

13
Electroconvulsive Cognitive Assessment
Short test specific for ECT.
Assessment of: subjective memory, autobiographical memory, attention, recall.
Quick and easy to administer (4 to 6 min).
To be done prior to ECT, after 4 or 6 ECTs, at the end of the acute course and if possible, 1 to 3 weeks after finishing the acute course.
The goal is not to replace neuropsychological testing, but to be used instead of the MOCA and MMSE.

Enrolled
DepressedNo ECT
41 30.1%
Depressed with ECT
55 40.1%
Total
136 100%
NormalControl
40 29.4%

Analysis and Results

16


18

19
ECCA Domain Analysis

20

21

ECCA Spanish version preliminary data
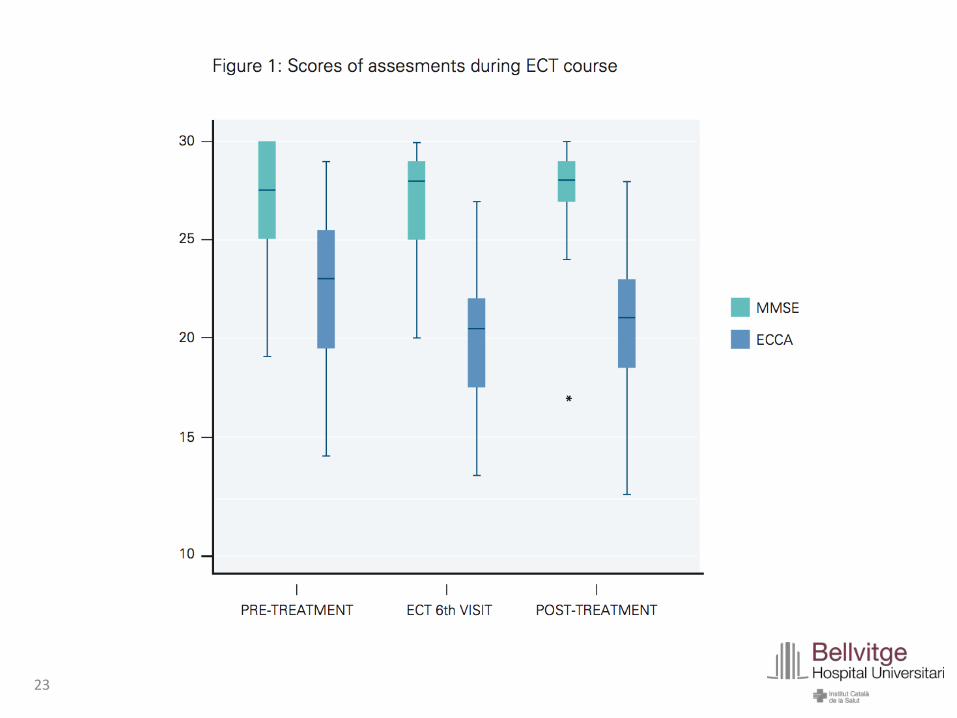
23

Multisite collaboration
Enrolled 14 depressed patients receiving ECTComparing ECCA with MMSE
Enrolled 9 subjects, comparing ECCA with neuropsych testing
Enrolled 25 - 3 groups
International collaboration

Small grant

ECT task Group – Impacting Patient Care
J Psychiatr Pract. 22(6):484-489, 2016.

ECT task Group – Exploring New Projects


Our data support that the ECCA may be a helpful tool to assess cognitive changes associated with ECT
ECCA could alert the clinician during the acute treatment course.
It is helpful to add collateral information when assessing the cognitive SE of ECT
Further research is warranted to determine the psychometric properties of the ECCA
Conclusions

30
WE CAN COLLABORATE !

Emory Group
Felicia Goldstein, PhD
David Loring, PhD
Limin Peng, PhD
Zixun Ye, MSPH
Susan Henderson, NP
Patricio Riva-Posse, MD William McDonald, MD
Adriana Hermida, MD
NNDC Collaborators
ECCA Group of Collaborators
Richard Weiner, MD, PhD
Mustafa Husain, MD
Irving Reti, MD
Daniel Maixner, MD
Shawn McClintock, PhD
International Collaborators
Aida de Arriba-Arnaú, MD
Mikel Urretavizcaya, MD, PhD
JM Mechón, MD
V. Soria MD

NNDC ECT Task Group
Task Group
Mustafa Husain, MD (Co-Chair)
Richard Weiner, MD, PhD (Co-Chair)
James Beeghly, MD
David Casey, MD
Andrew Francis, MD
Adriana Hermida, MD Sarah H. Lisanby, MD
Daniel Maixner, MD
Kevin Reeves, MD
Irving M. Reti, MD
Nelson Rodriguez, MD
Shirlene M. Sampson, MD
Stephen Seiner, MD
Salih Selek, MD