Development and Clinical Validation of Large Fusion Panel for ...
14
Development and Clinical Validation of Large Fusion Panel for Pediatric and Adult Cancers Fengqi Chang, Ph.D. Children’s Hospital of Philadelphia Perelman School of Medicine at the University of Pennsylvania 08-08-2016
Transcript of Development and Clinical Validation of Large Fusion Panel for ...

Development and Clinical Validation of Large Fusion Panel for Pediatric and Adult Cancers
Fengqi Chang, Ph.D.
Children’s Hospital of Philadelphia
Perelman School of Medicine at the University of Pennsylvania
08-08-2016

Rationales
• Gene fusion: one of the most common types of driver mutation in cancer
• Identification of oncogenic gene fusions: important for disease diagnosis, risk stratification and therapeutic decision making.
• FISH and RT-PCR: labor intensive, time consuming, and low throughput.
• Whole transcriptome sequencing (RNA-Seq): cost, sensitivity, efficiency, TAT, starting material; significant computational/bioinformatics resources.
Targeted, semi-quantitative RNA-sequencing methods emerge as an better solution to comprehensively sample known or novel fusions with high accuracy and sensitivity in clinical setting.

• The Fusion Panel includes 106 major fusion partner genes and can
detect 586 different known fusions and many more novel fusions in
both solid and liquid tumors in a single reaction.
• The panel uses Archer Anchored Multiplex PCR (AMP™) technology.
• The panel works on blood, BM, fresh/frozen tissues, and FFPE
tissues.
• CHOP FusionPanel also provides a reference of gene expression.
The CHOP FusionPanel

Nucleotide extractionRNA extraction:
RiboPureRneasy MiniAgencourt FormaPure
Library constructionArcherDX Universal RNA Kit
SequencingMiSeq/NextSeq
2X150bp
Analysis PipelineArcher Analysis Software
Fusion annotation & interpretationJbrowse: visualizationInternal database: common read- throughs
and false positivesDatabases:
Atlas of Genetics and Cytogenetics inOncology and Haematology
Mitelman database of Chromosome Aberrations and Gene Fusions in Cancer
TCGA fusion Gene DatabaseFusionCancerCOSMIC FusionsPubMedDr. Google
Fusion confirmationSanger sequencingReal-time quantitative PCRNested PCRFISH
Clinical report
QC check
QC check
QC checkQC check
Workflow and Analysis Pipeline
Sensitivity of CHOP FusionPanel
100% sensitivity:
Identified at least one causal fusion in all 30 positive cases
Detected NO fusion in 2 normal controls
• 32 validation samples from COG were tested blindly
Validation of Fusion Panel

Detection limit of CHOP FusionPanel
Strong evidence fusions:* >5 unique fusion supporting reads** >3 unique start sites
Validation of Fusion Panel - Cont’

• All 586 gene specific primers work properly in the multiplex PCR assay (reads ranging
from 9 to 16,000)
Validation of Fusion Panel - Cont’

Gene Expression Evaluation
* RNA Unique Molecular Bins: the RNA reads with unique molecular barcodes and random start site after deduplication.
der(Y)
XX
der(14)

Clinical Application
Positive rate: 34.2% (39/114)
EWSR1 exon7 CREB1 exon6
EWSR1 exon11 HLF exon4
ETV6 exon5 RUNX1 exon4
NUP214 exon32 ABL1 exon3
ETV6 exon5 RUNX1 exon3
PAX7 exon7 FOXO1 exon2
EWSR1 exon7 FLI1 exon8
MTAP exon7 BRAF exon9
JAZF1 exon4 TAX1BP1 exon16
PAX3 exon6 FOXO1 exon2
ASPSCR1 exon7 TFE3 exon6
PAX5 exon8 SOX5 exon4
TCF3 exon16 PBX1 exon3
EWSR1 exon7 FLI1 exon6
BRAF exon9
BRAF exon9
NOTCH1 exon30 ROS1 exon34
KMT2A exon10 ARHGEF12 exon12
CIC exon20 DUX4 exon1
WFS1 exon1 PLAG1 exon3
IGH CRLF2
KIAA1549 exon16 BRAF exon9
C11orf95 exon3 RELA exon2
CRTC1 exon1 MAML2 exon2
COL1A1 exon25 PDGFB exon2
RBPMS exon5 NTRK3 exon14
KIAA1549 exon13
KIAA1549 exon15
KIAA1549 exon10 BRAF exon11
A case of B-ALL: treated as standard risk
NUP214-ABL1 fusion identified on day 7 - Ph-like ALL
Tyrosine kinase inhibitor added to the treatment
Protein domain architectures
KIAA1549 exon16 BRAF exon9
As of 8/5/2016, 114 FusionPanels tested
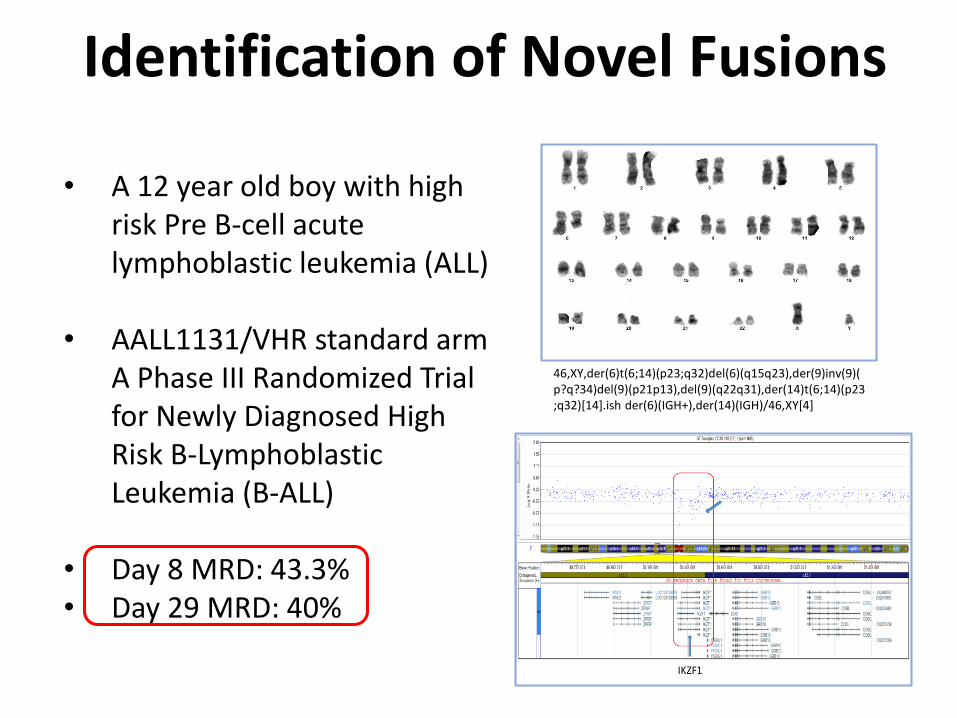
• A 12 year old boy with high risk Pre B-cell acute lymphoblastic leukemia (ALL)
• AALL1131/VHR standard arm A Phase III Randomized Trial for Newly Diagnosed High Risk B-Lymphoblastic Leukemia (B-ALL)
• Day 8 MRD: 43.3%• Day 29 MRD: 40%
Identification of Novel Fusions
46,XY,der(6)t(6;14)(p23;q32)del(6)(q15q23),der(9)inv(9)(p?q?34)del(9)(p21p13),del(9)(q22q31),der(14)t(6;14)(p23;q32)[14].ish der(6)(IGH+),der(14)(IGH)/46,XY[4]

1
0.61
0.02 0.011 0.00056610.00384160.00001740
0.2
0.4
0.6
0.8
1
1.2
M1 M2 M3 M4 M5 M6 M7
Real Time qPCR showed nearly two log
reduction after two months of ruxolitinib
treatment
Gel picture of RT-PCR3 forward primers which locatedat exon 8 (F3), exon 9 (F2) andexon 10 (F1) of GENE1 and 3reverse primers which located atexon 19 (R1), exon 20 (R2) andexon 22 (R3) of JAK2 weredesigned.
Identification of Novel Fusions
A personalized qPCR test

Conclusions
• We have developed a customized Fusion panel for pediatric and adult cancers
• Clinical validation showed 100% sensitivity and 1% detection limit
• CHOP FusionPanel is compatible with different sample types (FFPE samples)
• High detection yield (34.2%) in different types of cancers
• CHOP FusionPanel allows for the detection of actionable fusions that provide
accurate diagnosis, prognosis and new treatment options for cancer patients
• Enable the development of personalized test to monitor treatment response and
minimal residual diseases
DGD Cancer Genomic Diagnostics
Marilyn M. LiMinjie LuoFumin LinLuanne WainwrightDonna WilmothAdam GleasonTammy GrouGozde AkgumusDaniel J GalloMichele ThiessXiaonan ZhaoJunxia TangJorune BalciunieneDerek A Anderson
DGD Bioinformatics
Mahdi SarmadyKajia CaoChao Wu
CHOP Cancer CenterPathology Dept.
Steve HungerJohn MarisBruce PawelMariarita Santi-ViciniYael P. MosseAngela J. WaandersSarah TasianAnd others
Other DGD members