Developing the Standard of Care for Post-Concussion...
15
© Copyright Cognitive FX 2016 1 Developing the Standard of Care for Post-Concussion Treatment: Neuroimaging-Guided Rehabilitation of Neurovascular Coupling Benjamin H. Wing 1,2 ; Braden J. Tucker 1,4 ; Alina K. Fong, PhD 1,3 ; E. Bruce McIff, MD 1,2 ; Mark D. Allen, PhD 1,2 1 Cognitive FX, Provo, UT 2 Notus Neuropsychological Imaging, Orem, UT 3 Utah Valley Regional Medical Center, Provo, UT 4 Case Western Reserve University School of Medicine, Cleveland, OH ABSTRACT Objective. Emerging research proposes the imbalance between microvascular supply and metabolic demand as a contributing factor in the pathophysiology of mild traumatic brain injury (mTBI). Prolonged effects on the dysregulation of neurovascular coupling (NVC) may explain persistent symptomatic models such as Post-Concussion Syndrome (PCS). Increased knowledge of what we refer to as Neurovascular Uncoupling (NVU) provides a template for establishing a new concussion treatment standard in the assessment and therapeutic guidance of concussion. Participants & Methods. The degree and localization of NVU was statistically contextualized against a normative-based atlas in 270 concussed patients using Functional NeuroCognitive Imaging TM (fNCI) to establish pre-treatment benchmarks and methodically guide neurotherapy. Conventional and fNCI-directed measures were used to evaluate post-rehabilitative outcomes. Results. fNCI was successful in identifying regions of NVU unique to each patient’s brain and concussion profile. Longitudinal objective outcome measures demonstrated timely and lasting improvement of NVC functioning in a significant majority of patients. Conclusions. We present practice-based evidence supporting the clinical administration of fNCI with particular efficacy in the neurorehabilitation of mTBI. We advocate the reliability of fNCI in assessing severity and localization of NVU, and promote its use in the therapeutic guidance and neurorehabilitation of mTBI. We further support the continual exploration of other potential pathophysiological involvement in this complex brain injury. KEYWORDS Mild traumatic brain injury (mTBI), concussion, post-concussion syndrome (PCS), regional cerebral blood flow (rCBF), neurovascular coupling (NVC), neurovascular uncoupling (NVU), enhanced performance in cognition TM (EPIC), functional magnetic resonance imaging (fMRI), clinical fMRI, blood oxygen level dependent (BOLD) signals, functional neurocognitive imaging TM (fNCI), severity index score (SIS), post-concussion symptom scale (PCSS), neurorehabilitation, treatment standards, accelerated improvement, longitudinal outcome
Transcript of Developing the Standard of Care for Post-Concussion...
©CopyrightCognitiveFX20161
DevelopingtheStandardofCareforPost-ConcussionTreatment:Neuroimaging-GuidedRehabilitationofNeurovascularCouplingBenjaminH.Wing1,2;BradenJ.Tucker1,4;AlinaK.Fong,PhD1,3;E.BruceMcIff,MD1,2;MarkD.Allen,PhD1,2
1CognitiveFX,Provo,UT2NotusNeuropsychologicalImaging,Orem,UT3UtahValleyRegionalMedicalCenter,Provo,UT4CaseWesternReserveUniversitySchoolofMedicine,Cleveland,OHABSTRACTObjective. Emerging research proposes the imbalance between microvascular supply andmetabolicdemandasacontributingfactorinthepathophysiologyofmildtraumaticbraininjury(mTBI). Prolonged effects on the dysregulation of neurovascular coupling (NVC)may explainpersistentsymptomaticmodelssuchasPost-ConcussionSyndrome(PCS).IncreasedknowledgeofwhatwerefertoasNeurovascularUncoupling(NVU)providesatemplateforestablishinganewconcussiontreatmentstandardintheassessmentandtherapeuticguidanceofconcussion.Participants&Methods. The degree and localization of NVUwas statistically contextualizedagainst a normative-based atlas in 270 concussed patients using Functional NeuroCognitiveImagingTM(fNCI)toestablishpre-treatmentbenchmarksandmethodicallyguideneurotherapy.ConventionalandfNCI-directedmeasureswereusedtoevaluatepost-rehabilitativeoutcomes.Results. fNCIwas successful in identifying regionsofNVUunique toeachpatient’sbrainandconcussionprofile.LongitudinalobjectiveoutcomemeasuresdemonstratedtimelyandlastingimprovementofNVCfunctioninginasignificantmajorityofpatients.Conclusions.Wepresentpractice-basedevidencesupportingtheclinicaladministrationoffNCIwithparticularefficacyintheneurorehabilitationofmTBI.WeadvocatethereliabilityoffNCIinassessingseverityandlocalizationofNVU,andpromoteitsuseinthetherapeuticguidanceandneurorehabilitationofmTBI.We further support the continual explorationof other potentialpathophysiologicalinvolvementinthiscomplexbraininjury.KEYWORDSMildtraumaticbraininjury(mTBI),concussion,post-concussionsyndrome(PCS),regionalcerebralblood flow (rCBF), neurovascular coupling (NVC), neurovascular uncoupling (NVU), enhancedperformanceincognitionTM(EPIC),functionalmagneticresonanceimaging(fMRI),clinicalfMRI,blood oxygen level dependent (BOLD) signals, functional neurocognitive imaging TM (fNCI),severityindexscore(SIS),post-concussionsymptomscale(PCSS),neurorehabilitation,treatmentstandards,acceleratedimprovement,longitudinaloutcome

©CopyrightCognitiveFX20162
1.INTRODUCTION1.1MILDTRAUMATICBRAININJURYRecent reports by the Center forDiseaseControl (CDC) indicate that traumaticbraininjury (TBI) has increased by 60% in thegeneral population from 2001-2010 withmild TBI (mTBI) composing approximately80% of those events (Management ofConcussion/mTBIWorkingGroup,2009).Likewise, Armed Services report nearly348,000traumaticbrain injuriessince2000with82.3%classifiedasmTBI(DefenseandVeterans Brain Injury Center, 2016). Thissignificant increase in mTBI diagnosis is aresult of improved awareness of itsepidemiology, etiology, presentation,sequela, and even trends toward moreaggressiveplayinsportsandotheractivities(Clayetal.,2013).Consequently, increasedhealth care demand has led to an urgentneed for valid guidelines for accuratelyassessinganddiagnosingthiscomplexinjury(Carney et al., 2014). Recently, extensiveeffortshavebeenmade tounderstand thediagnosis,prognosis,andtreatmentofmTBI,as well as the persistent underlyingphysiological changes that may occur inpost-concussion syndrome (PCS), such asneurovascularsignalingdisruptionsthattakeplace within cortical micro-structure.However, most current treatmentapproaches do not incorporate advancedscientificfindingsoftheunderlyingcausesofpersistent mTBI dysfunction intorehabilitative practice, but rather rely ontraditionalstrategiesthatarelargelyfocusedonreducingovertsymptoms.Currentguidelines for treatmentofacutemTBI center on limiting physical andcognitiveactivitywhilereducingexposuretosymptom-aggravating stimuli until it isdeemed that the patient has returned tonormalfunction(Clayetal.,2013).Inmany
cases,thetreatmentcoursemaylastweeks,months,andyears.For thesemorechronicsymptoms, the standing recommendationfortreatmentofpost-concussionconditionsis a symptoms-based approach(ManagementofConcussion/mTBI Working Group, 2009).In other words, clinicians address eachsymptom individually, as if they were anindependent condition, and often employpharmacologicalandmedicaltherapywhenrest itselfdoesnotmitigatethesymptoms.This approach can prove problematic formany mTBI patients because of theirincreased susceptibility to adverse sideeffects of the medication to treat theirsymptoms, often worsening overallsymptom presentation in many cases(Chapmanetal.,1999).Asalientexampleofthis problem is the common diagnosis andsubsequent psychopharmacologictreatment of psychiatric symptomsdiagnosedpost-mTBI.Often,thesideeffectsofthesemedicationsmimicandexacerbateongoing concussion symptoms (Warden etal.,2006).Additionally, the diagnosis of Axis Ipsychiatricconditionsishighlyquestionable,as many of these patients have nopremorbidhistoryofpsychiatricillness,anddeveloped these symptoms only afterstruggling with the sequelae for months(McAllister & Arciniegas, 2002; Warden etal., 1997). Although the current treatmentmethods promote patient recovery fromsome mTBI symptoms, this approach mayfail to address the underlying etiology andpathophysiologyofconcussionsthatresultsin longitudinal alterations in cognitive,occupational, emotional, andneuromuscular function (Warden et al.,2006).Consequently, a standard for care thataddresses and treats the underlying

B.H.Wing,B.J.Tucker,A.K.Fong,andM.D.Allen/StandardizationoffNCI-directedrehabilitation
©CopyrightCognitiveFX20163
pathologyisneededforeffectivetreatmentofpost-concussionsymptomsasopposedtomaskingtheconditionbytreatingindividualpresentations.1.2NEUROVASCULARCOUPLINGRecent scientific investigations on theeffects of concussion suggest thatdisruptionstoneuronally-triggeredregionalcerebralbloodflow(rCBF)mayaccountforasignificantportionofPCSsymptoms(Ellisetal.,2016;MacFarlane&Glenn,2015).Normal brain functioning relies on highlyresponsive mechanisms of blood flowregulation that are sensitive to theimmediateandshiftingdemandsforsteadyglucose metabolism throughout the brain(Giza & Hovda, 2001). Anything less thanprecise neurovascular coupling (NVC)betweenneuralactivityandbloodflowmayresult in obvious cognitive and physicaldeficits(Mikulis,2013).Althoughpermanentgross structural brain damage is notobservedinconcussion/mTBI(bydefinition),there is clear evidence for long-termdisruption of NVC, associated withmeasurableneurocognitivedysfunction (daCostaetal.,2016;Meieretal.,2015;Mutchetal.,2015;Wangetal.,2015;Bartnik-Olsonet al., 2014) and physical dysfunction(Kozlowski et al., 2013; Leddy et al., 2013)typical in PCS symptomology. We refer tothis phenomenon as NeurovascularUncoupling(NVU).GiventhekeyrolethatNVUislikelytoplayinPCS,effectivetreatmentshouldinclude1)an objective neuroimaging method fordetecting NVU in the brain, and 2) aninformed rehabilitation protocol withadvanced techniques for restoring normalNVC. We present here data from a largesample of mTBI patients assessing theeffectiveness of one specific treatmentprogram, Enhanced Performance in
CognitionTM (EPIC) treatment, whichemploysanovel,evidence-basedsystemofatypically aggressive NVC recoverytherapies.Functional magnetic resonance imaging(fMRI) has been used extensively over thelast twodecadesas thedominant researchtool for understanding human brainfunction. fMRI is often described as amethod that detects ‘brain activity.’However, a more accurate description offMRIwould be that it detects efficiency inNVC. Although fMRI does not directlymeasure neural activation, it hasnonetheless proven to be a highly reliabletool in brain function mapping, given theprecisecoupling thatnormallyexists in thehealthy brain between neural activity andthe blood oxygen level dependent (BOLD)signal that isdetectedby fMRI (Bandettini,2012). However, due to the very fact thatfMRI is a more direct measure of NVCefficiency than neural activity itself, it iscurrently the most ideal imaging tool tomeasure dissociations between NVC andwhat is otherwise normal brain cellfunctioning inunhealthybrains,specificallyasfoundinPCS.Given the special nature of fMRI withregard to mTBI dysfunction, many high-qualityresearchstudiesoverthelastdecadehave used fMRI to investigateneurocognitive effects of concussion(Keightley et al., 2014; McDonald et al.,2012; Slobounov et al., 2010; Chen et al.,2008), and, to a limited extent, treatmentoutcomes (Koski et al., 2015; Leddy et al.,2013). However, the fMRI method asstandardly employed in scientific researchlacksessentialfeaturesnecessaryforclinicalassessment: 1) a concurrently validated,reliable,andobjectivestandardizedprotocolappropriate for the scanning environment,and 2) a clinically acceptable normative-

©CopyrightCognitiveFX20164
based contextualization procedure forappropriate individualized patientassessment(Ellisetal.,2016).
1. METHODOLOGY
2.1FUNCTIONALTASKBATTERYOur unique functional NeuroCognitiveImagingTM (fNCI) assessment protocolcombines the validity of conventionalneuropsychologictestingstandardswiththereliability and objectivity of informationaldata output provided by fMRI. The testingbatteryunderwent iterativepilot testing toensure concurrent validity, reliability,objectivity, and suitability for the scanningenvironment(Allen&Fongetal.,2010;Allen&Fong,2008a;Allen&Fong,2008b).The functional task battery, NotusNeuroCogsTM, is comprised of sixneuropsychologic test adaptations: thefunctionalMatrixReasoningTestTM(f-MRT),the functional Trail Making Test-BTM (f-TMTB),thefunctionalPictureNamingTestTM(f-PNT),thefunctionalFaceMemoryTestTM(f-FMT), the functional Verbal MemoryTestTM (f-VMT), and the functional VerbalFluencyTestTM(f-VFT).Eachofthesixtasksincludes eight Test Phases presented inalternating fashion with Rest Phases, inwhichthesubject isaskedtosilentlycountfrom 1 to 10. Compliance monitoring isperformed at intervals during each task.Operativedescriptionsareoutlinedbelow:The f-MRT tests non-verbal problemsolvingusinga3x3arrayofvisuallycomplexfigureswithonefiguremissing.Thesubjectis then instructed to select thebestmatchfor the missing figure from among four“candidate”figuresbypressingadesignatedbutton.The f-TMTBmeasures cognitive flexibilityby presenting a virtual connect-the-dotstasks using a button pad response system.
Randomlyarrangednumbersandlettersaredisplayedonascreenandthesubjectmustlocateandconnecteachseriesofnumbersand letters in ascending order whilealternatingbackandforthbetweenthetwocharactertypes.The f-PNT assesses semantic objectrecognition by displaying line drawings ofcommonobjectsforaperiodof1.5secondseach. Subjects are instructed to silentlyidentifyeachobjectuponpresentation.Thef-FMTinvestigateslong-termmemory.Subjectsareinstructedtomemorizecoloredphotographs of unfamiliar faces andinformed that they will be required toidentify some of the faces at a later time.Twenty faces are presented twice in 2random orders for three seconds eachduring scanning. Recognition accuracy isrecordedonapost-scantest.The f-VMT analyzes short-term verbalmemory.Foreachtestrun,thesubjectviewsa series of eight common words for onesecond each and is instructed to silentlymemorize the words as they appear.Subjects are given 12 additional secondsafterallwordshavebeenpresentedtorecallasmanyaspossible.Thef-VFTisaletter-basedfluencytest.Thesubject is instructed to silentlygenerateasmany unique words as possible (excludingpropernamesorvariantsofthesameword)withina20-secondtime limitusingagivenfirstletter.2.2NORMATIVEATLASInordertofurthersupportthereliabilityofour testing battery and employ its clinicalapplication, we utilized a group-summaryanalysisapproach,wheresingle-subjectNVCiscomparedagainstnormativedatasets.ThefNCIassessmentprotocolwasinitiallyperformedonapopulationcomprisedof59normativereferencevolunteers(27male,32

B.H.Wing,B.J.Tucker,A.K.Fong,andM.D.Allen/StandardizationoffNCI-directedrehabilitation
©CopyrightCognitiveFX20165
female)betweentheagesof19-57yearsold(Mean = 30.1, σ = 8.5). EdinburghHandedness Inventoryanalysis foundright-hand dominance in 91.5% of subjects.Majority of participants within thispopulationwereCaucasian(74.6%),withtheremaining being: Hispanic (11.8%), Asian(10.2%), and African American (3.4%).ReferencesubjectsallspokeEnglishastheirfirst languageandhadat leastoneyearofhighereducation(Mean=14.3,σ=2.9).Data analysis revealed 57 specificactivation regions found to be task-associatedwiththeNotusNeuroCogsTMtaskbattery. Additionally, these regions ofinterest were found to possess a normaldistribution of functional NVC efficiencyamongstreferencesubjects.Thisdistributiveproperty formulated a three-dimensionalactivation standard, or normative atlas,which was later used to statisticallycontextualizebothseverityand localizationofNVUin270concussedpatients.2.3CLINICALFUNCTIONALNEUROCOGNITIVEIMAGINGAlthough traditional uses of fMRI andother advanced neuroimaging methodshavebeenemployedprimarily forresearchpurposes or preoperative functionalmapping, we are rapidly approaching thestandardized integrationoftheseadvancedimaging techniques in clinical evaluation[Zhang et al., 2009; Matthews, Honey, &Bullmore,2006].Butseveralkeylimitationshavehinderedtheuniversalapplicationandestablishment of clinical fMRI practice. Forthescopeof thispaper,weaimtopresentthetwomostgeneral,yetmajor,limitationsand briefly discuss our standardizedapproachtoaddresstheirlimitingeffectsonfNCI-specific data retrieval,contextualization,andclinicalapplication.
In recent years, questions within thescientific community have been raisedregarding the clinical reliability of fMRIbecause of rising skepticism towards BOLDsignal stability. Skepticism revolves aroundthebeliefthatfMRIdataoutput(BOLDsignalactivation) is both unreliable andirreproducible(Plichtaetal.,2012;Bennett& Miller, 2010). To provide a betterframework that enforces BOLD signalstability, researchers have scientificallydiscovered a strong relationship betweenfMRIreliabilitycharacteristicsandparadigmstandardization (Ellis et al., 2016; Pichta etal., 2012). Through years of extensive pre-testing, Notus NeuroCogsTM has beenexaminedforconcurrentvalidity,reliability,objectivity, and suitability within thescanningenvironmentusingastandardizedadministration protocol (Allen et al., 2012;Allen,Wu,&Bigler,2011;Allenetal.,2011;Allen&Fong,2008a;Allen&Fong,2008b).Inaddition,ourstandardizedfunctionaltaskbatteryhasbeendirectlyassessedfor test-retest stability in a sample of 14 healthycontrols to date, yielding a correlationalaverage of r = 0.859 (StDev = 0.0904)amongst 57 task-associated regions (dataspecificsnotshown).The other well known, reoccurringargument made against clinical fMRIquestions the appropriateness andsufficiency of statistical corrections madeduring fMRI data analysis (Eklund et al.,2012). Notably, all fMRI analyses includecomplex chains of statistics, but there isnowhere in our statistical pipeline thatincludes the type of inferential process(es)that would be subject to the concern ofcorrectingforfalsepositives.Avoidingtheseclinical criticisms associated withexperimental methods of null hypothesistesting, our statistical contextualization
©CopyrightCognitiveFX20166
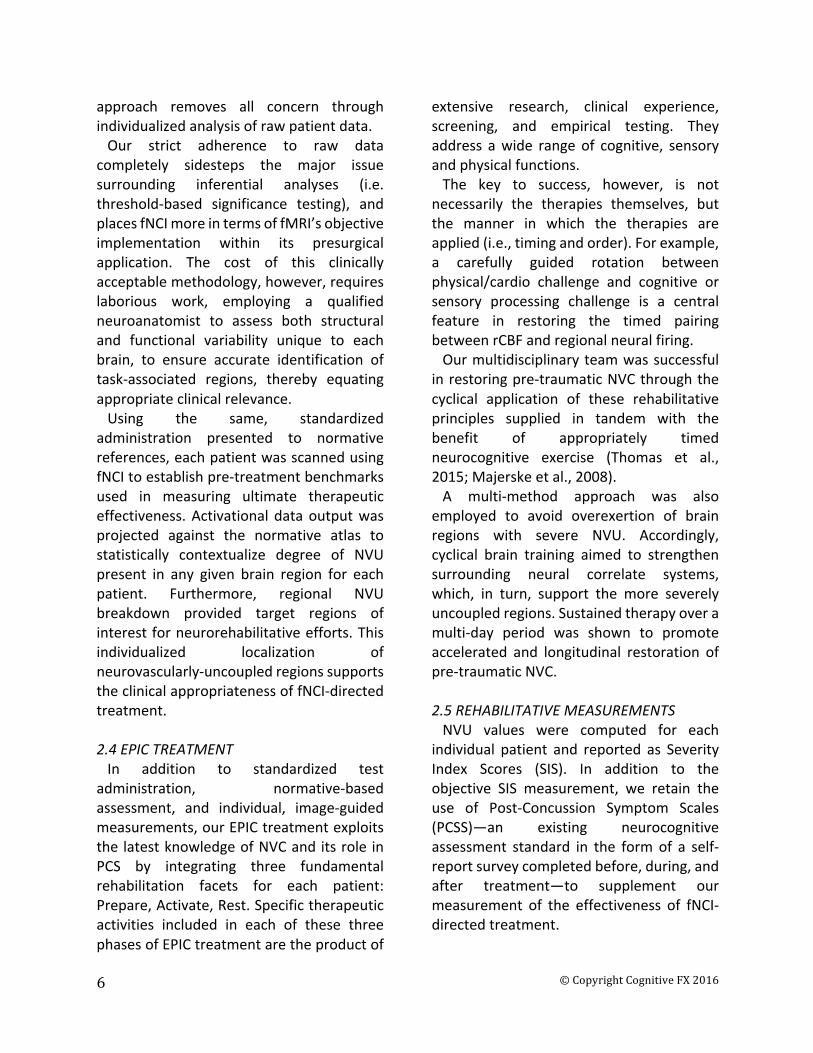
approach removes all concern throughindividualizedanalysisofrawpatientdata.Our strict adherence to raw datacompletely sidesteps the major issuesurrounding inferential analyses (i.e.threshold-based significance testing), andplacesfNCImoreintermsoffMRI’sobjectiveimplementation within its presurgicalapplication. The cost of this clinicallyacceptablemethodology,however,requireslaborious work, employing a qualifiedneuroanatomist to assess both structuraland functional variability unique to eachbrain, to ensure accurate identification oftask-associated regions, thereby equatingappropriateclinicalrelevance.Using the same, standardizedadministration presented to normativereferences,eachpatientwasscannedusingfNCItoestablishpre-treatmentbenchmarksused in measuring ultimate therapeuticeffectiveness.Activational dataoutputwasprojected against the normative atlas tostatistically contextualize degree of NVUpresent in any given brain region for eachpatient. Furthermore, regional NVUbreakdown provided target regions ofinterestforneurorehabilitativeefforts.Thisindividualized localization ofneurovascularly-uncoupledregionssupportstheclinicalappropriatenessoffNCI-directedtreatment.2.4EPICTREATMENTIn addition to standardized testadministration, normative-basedassessment, and individual, image-guidedmeasurements,ourEPICtreatmentexploitsthe latestknowledgeofNVCanditsrole inPCS by integrating three fundamentalrehabilitation facets for each patient:Prepare,Activate,Rest.Specifictherapeuticactivities included in each of these threephasesofEPICtreatmentaretheproductof
extensive research, clinical experience,screening, and empirical testing. Theyaddress awide range of cognitive, sensoryandphysicalfunctions.The key to success, however, is notnecessarily the therapies themselves, butthe manner in which the therapies areapplied(i.e.,timingandorder).Forexample,a carefully guided rotation betweenphysical/cardio challenge and cognitive orsensory processing challenge is a centralfeature in restoring the timed pairingbetweenrCBFandregionalneuralfiring.Ourmultidisciplinaryteamwassuccessfulinrestoringpre-traumaticNVCthroughthecyclical application of these rehabilitativeprinciples supplied in tandem with thebenefit of appropriately timedneurocognitive exercise (Thomas et al.,2015;Majerskeetal.,2008).A multi-method approach was alsoemployed to avoid overexertion of brainregions with severe NVU. Accordingly,cyclical brain training aimed to strengthensurrounding neural correlate systems,which, in turn, support the more severelyuncoupledregions.Sustainedtherapyoveramulti-day period was shown to promoteaccelerated and longitudinal restoration ofpre-traumaticNVC.2.5REHABILITATIVEMEASUREMENTSNVU values were computed for eachindividual patient and reported as SeverityIndex Scores (SIS). In addition to theobjective SIS measurement, we retain theuse of Post-Concussion Symptom Scales(PCSS)—an existing neurocognitiveassessment standard in the formof a self-reportsurveycompletedbefore,during,andafter treatment—to supplement ourmeasurement of the effectiveness of fNCI-directedtreatment.

©CopyrightCognitiveFX20167
A B
Image1
SeverityIndexScores(A)andPost-ConcussionSymptomScales(B)aregraphicallyreportedasshownabove.A)Healthy,Borderline,Mild,Moderate,andSeverelevelsofneurovascularuncouplingcanbevisualized.B)VariouscategoricalsymptomscanbeindividuallyobservedinadditiontothePCSSTotalIndexScoreoverthesustained,multi-daytreatmentperiod.
2. RESULTS
3.1PATIENTOUTCOMESDatacollectionandanalysisconfirmedtheeffectiveness of fNCI-directed treatment inacceleratedconcussionrehabilitation.
Quantitativeimprovementwasobservedonboth objective fNCI measurements andsubjective symptom report measurementsafter an average of 4.1 days of EPICtreatment.Averagepre-andpost-treatmentmeasurementsarereportedforasampleof270concussedpatients.
A B
Image2
Averagepre-andpost-treatmentscoresreportedunderbothobjective(A)andsubjective(B)measurementsandarereportedtographicallyvisualizeaveragepatientoutcome.

©CopyrightCognitiveFX20168
3.2ASSESSMENTOFDEMOGRAPHICVARIABLESONOUTCOMESConsideringawidevarietyofconcussionprofileswithregardstoage,sex,modeof
injury,andtimesinceinjury,ourEPICtreatmenthasalsobeenshowntobeextremelyeffectiveunderbothobjectiveandsubjectivemeasures.
A B
C D
Image3
Concussionprofilesvarygreatlyamongstpatientsconsideringage(A),sex(B),mode-of-injury(C),timesinceinjury(D),andotherdemographicalcharacteristics.Patientoutcomesunderthesevaryingprofilesarereported.3.3.ImprovementOutcomesImprovement,inabroadsense,wasbeenobservedin99.6%and99.2%ofourpatientsunderobjectiveandsubjectmeasurements,respectively.Butthedegreeofimprovementvaried across a wide spectrum of percentdifferences(Range=3.24to157.0%).
Consequently, to address thiscomplication, we established incrementalimprovement thresholds and report thetotal percentageof our patients thatmeetand/or exceed such thresholds. Averageimprovementisalsographicallyvisualized

©CopyrightCognitiveFX20169
A
B
Image4
Formanypatients,thematterofsignificantimprovementvariesbased-uponthequality-of-life-impacttheirpersistentsymptomaticprofilemanifestspost-concussion.Assuch,ourpatientshavereporteda“significantimprovement”acrossaspectrumofpercentdifferences.Toadequatelyreportimprovementthresholds,aspectrumofimprovementpercentsaregraphicallypresentedagainstpercentsofourpatientpopulationwhohaveimprovedbysuchthresholdsorgreater.ImprovementthresholdsandtheirpercentagescanbeobservedforbothSISandPCSSmeasures.3.4.Short-TermOutcomeComparisonA random sample of 27 patients whounderwentEPICtreatmentwasgeneratedtovisuallycharacterizetheoriginalpoolof270patients.Thissamplewasreportedagainstagroup of 27 patients who, at the time ofinitialscanning,optedtodelayedtreatmentandwererescannedatalaterdate.
Additionally, it was comparativelyreported against a sample of 13 healthycontrolsthatwerescannedinordertoassesstest-retestreliabilityofthefNCImethod.Therandom sample accurately representsimprovement trends reported above (refertoImage4),observingimprovementin100%

©CopyrightCognitiveFX201610
of patients, with an average of ~70%improvement amongst the treated patientsample(73.1%ofwhichreturnedtowithin-normal-limits post-treatment. Incomparison,65.4%ofpatientswhodidnot
receive treatment saw spontaneousimprovement, averaging 18.4%improvement (only 3.8% of whichspontaneously returned to within-normal-limits
Image5Randomsamplingoftreatedpatients,non-treatedpatients,andhealthycontrolsaccuratelyrepresentstotalpatientoutcomes,andfurthersupportstheefficacyofpositiveshort-termresultsusingfNCI-directedtreatment.AllSISscoreswithinthedenotedrange(areashadedgreen)areconsideredwithinnormallimits.Note:Thehealthycontrolmean(SIS=0)elucidatesthepossibilityofnegativeSISvalues.Thesevaluesarestillconsideredtohavefallenwithinnormallimits.
3.5LONGITUDINALOUTCOMESRecoveryinacutemodelsofmTBIisoftenunpredictable. For those injuries thatprogress into persistent cases, researchfindings allude to the pathophysiologicalmisalignmentindefaultNVCefficiency.Accordingly,arehabilitativeapproachthatpromotes the restoration of default NVC
efficiency should, therefore, expectlongevity of positive outcomes in PCS. Asexpected, longitudinal outcomes for fNCI-directed treatment report sustainedrehabilitative outcomes in follow-up scansaveraging8.8monthspost-treatment.
Image6Sustainedrehabilitativeoutcomesareobservedinlongitudinal,follow-upscansaveraging8.8monthspost-treatment.AllSISscoreswithinthedenotedrange(areashadedgreen)areconsideredwithinnormallimits.

©CopyrightCognitiveFX201611
3. DISCUSSION&CONCLUSIONWe present practice-based evidence forthestandardizedapplicationof fNCI,whichis currently used in directingneurorehabilitation, with particularefficiency inmTBI.We indicate the clinicalappropriateness of this image-guidedapproach through iterative pilot testing,standardized administration, andindividualized, normative-basedcontextualization.We further demonstratetherehabilitativeguidancecapabilityoffNCIin establishing EPIC treatment standardsthat prioritize neurovascularly-uncoupledregions of interest unique to each patient,and support the targeted, multi-method,cyclical, and sustained approach employedbyourmultidisciplinaryteam.Positive patient outcomes—graphicallyrepresented using conventional and fNCI-directedmeasures—advocatefNCI’sefficacyin the accelerated and longitudinalneurorehabilitationofmTBIacrossavarietyofconcussionprofiles.
Longitudinaldatacollectionhasobservedamaintained SIS score within normal limits,signifyingtheprobablerestorationofpre-traumatic NVC and re-establishment ofdefault NVC efficiency. Continuedlongitudinaldatacollectionwilllikelyexplainthe mechanistic observation of thesepositiveoutcomes.Though our positive treatment outcomessupporttheroleofNVCinPCS,thecomplexinterconnectednessofvastneuralcorrelatesystemsfoundwithinthebrainadvocatetheetiologicalpotentialofmultiplemechanicalfailings (e.g. neuronal dysfunction,signaling/timing disruptions, and/orneurotransmitterdysregulation).Therefore, we support continualexploration of other advancedneurorehabilitative therapies and theirrelationshipstopersistentmodelsofmTBI.However, standardizedapplicationof thisevidence-based practice in generalneurocognitive assessment andrehabilitation may be key to establishingclinical fMRI practice standards specificallyinguidingneurorehabilitativeoutcomes.

©CopyrightCognitiveFX201612
SUPPORTINGPUBLICATIONSAllen,M.D.,&Fong,A.K.(2008a).ClinicalapplicationofstandardizedcognitiveassessmentusingfMRI.I.Matrixreasoning.BehavNeurol,20(3),127-140.doi:10.3233/BEN-2008-0223Allen,M.D.,&Fong,A.K.(2008b).ClinicalapplicationofstandardizedcognitiveassessmentusingfMRI.II.Verbalfluency.BehavNeurol,20(3),141-152.doi:10.3233/BEN-2008-0224Allen,M.D.,Hedges,D.W.,Farrer,T.J.,&Larson,M.J.(2012).AssessmentofbrainactivityduringmemoryencodinginanarcolepsypatientonandoffmodafinilusingnormativefMRIdata.Neurocase,18(1),13-25.doi:10.1080/13554794.2010.547508Allen,M.D.,Owens,T.E.,Fong,A.K.,&Richards,D.R.(2011).AfunctionalneuroimaginganalysisoftheTrailMakingTest-B:implicationsforclinicalapplication.BehavNeurol,24(2),159-171.doi:10.3233/BEN-2011-0278Allen,M.D.,Wu,T.C.,&Bigler,E.D.(2011).TraumaticBrainInjuryAltersWordMemoryTestPerformancebySlowingResponseTimeandIncreasingCorticalActivation:AnfMRIStudyofaSymptomValidityTest.Psychol.Inj.andLaw,4:140.doi:10.1007/s12207-011-9105-4REFERENCESAllen,M.D.,&Fong,A.K.(2008a).ClinicalapplicationofstandardizedcognitiveassessmentusingfMRI.I.Matrixreasoning.BehavNeurol,20(3),127-140.doi:10.3233/BEN-2008-0223Allen,M.D.,&Fong,A.K.(2008b).ClinicalapplicationofstandardizedcognitiveassessmentusingfMRI.II.Verbalfluency.BehavNeurol,20(3),141-152.doi:10.3233/BEN-2008-0224Allen,M.D.,Hedges,D.W.,Farrer,T.J.,&Larson,M.J.(2012).AssessmentofbrainactivityduringmemoryencodinginanarcolepsypatientonandoffmodafinilusingnormativefMRIdata.Neurocase,18(1),13-25.doi:10.1080/13554794.2010.547508Allen,M.D.,Owens,T.E.,Fong,A.K.,&Richards,D.R.(2011).AfunctionalneuroimaginganalysisoftheTrailMakingTest-B:implicationsforclinicalapplication.BehavNeurol,24(2),159-171.doi:10.3233/BEN-2011-0278Allen,M.D.,Wu,T.C.,&Bigler,E.D.(2011).TraumaticBrainInjuryAltersWordMemoryTestPerformancebySlowingResponseTimeandIncreasingCorticalActivation:AnfMRIStudyofaSymptomValidityTest.Psychol.Inj.andLaw,4:140.doi:10.1007/s12207-011-9105-4Baker,J.G.,Freitas,M.S.,Leddy,J.J.,Kozlowski,K.F.,&Willer,B.S.(2012).Returntofullfunctioningaftergradedexerciseassessmentandprogressiveexercisetreatmentofpostconcussionsyndrome.RehabilResPract,2012,705309.doi:10.1155/2012/705309Bandettini,P.A.(2012).FunctionalMRI:Aconfluenceoffortunatecircumstances.Neuroimage.doi:10.1016/j.neuroimage.2012.01.130

B.H.Wing,B.J.Tucker,A.K.Fong,andM.D.Allen/StandardizationoffNCI-directedrehabilitation
©CopyrightCognitiveFX201613
Bartnik-Olson,B.L.,Holshouser,B.,Wang,H.,Grube,M.,Tong,K.,Wong,V.,&Ashwal,S.(2014).Impairedneurovascularunitfunctioncontributestopersistentsymptomsafterconcussion:apilotstudy.JNeurotrauma,31(17),1497-1506.doi:10.1089/neu.2013.3213Bennett,C.M.,&Miller,M.B.(2010).Howreliablearetheresultsfromfunctionalmagneticresonanceimaging?AnnNYAcadSci,1191,133-155.doi:10.1111/j.1749-6632.2010.05446.xCarney,N.,Ghajar,J.,Jagoda,A.,Bedrick,S.,Davis-OʼReilly,C.,duCoudray,H.,...Riggio,S.(2014).Concussionguidelinesstep1:systematicreviewofprevalentindicators.Neurosurgery,75Suppl1,S3-15.doi:10.1227/NEU.0000000000000433Chapman,E.H.,Weintraub,R.J.,Milburn,M.A.,Pirozzi,T.O.,&Woo,E.(1999).Homeopathictreatmentofmildtraumaticbraininjury:Arandomized,double-blind,placebo-controlledclinicaltrial.JHeadTraumaRehabil,14(6),521-542.Chen,J.K.,Johnston,K.M.,Petrides,M.,&Ptito,A.(2008).Recoveryfrommildheadinjuryinsports:evidencefromserialfunctionalmagneticresonanceimagingstudiesinmaleathletes.ClinicalJournalofSportMedicine,18(3),241-247.Clay,M.B.,Glover,K.L.,&Lowe,D.T.(2013).Epidemiologyofconcussioninsport:aliteraturereview.JChiroprMed,12(4),230-251.doi:10.1016/j.jcm.2012.11.005daCosta,L.,vanNiftrik,C.B.,Crane,D.,Fierstra,J.,&Bethune,A.(2016).TemporalProfileofCerebrovascularReactivityImpairment,GrayMatterVolumes,andPersistentSymptomsafterMildTraumaticHeadInjury.FrontNeurol,7,70.doi:10.3389/fneur.2016.00070DefenseandVeteransBrainInjuryCenter.(2016).DoDWorldwideNumbersforTBI[Datafile].Retrievedfromhttp://dvbic.dcoe.mil/files/tbi-numbers/DoD-TBI-Worldwide-Totals_2000-2016_Q1_May-16-2016_v1.0_2016-06-24.pdfEklund,A.,Andersson,M.,Josephson,C.,Johannesson,M.,&Knutsson,H.(2012).DoesparametricfMRIanalysiswithSPMyieldvalidresults?Anempiricalstudyof1484restdatasets.Neuroimage,61(3),565-578.doi:10.1016/j.neuroimage.2012.03.093Ellis,M.J.,Ryner,L.N.,Sobczyk,O.,Fierstra,J.,Mikulis,D.J.,Fisher,J.A.,...Mutch,W.A.(2016).NeuroimagingAssessmentofCerebrovascularReactivityinConcussion:CurrentConcepts,MethodologicalConsiderations,andReviewoftheLiterature.FrontNeurol,7,61.doi:10.3389/fneur.2016.00061Giza,C.C.,&Hovda,D.A.(2001).TheNeurometabolicCascadeofConcussion.JAthlTrain,36(3),228-235.

©CopyrightCognitiveFX201614
Giza,C.C.,&Hovda,D.A.(2014).Thenewneurometaboliccascadeofconcussion.Neurosurgery,75Suppl4,S24-33.doi:10.1227/NEU.0000000000000505Group,M.o.C.m.W.(2009).VA/DoDClinicalPracticeGuidelineforManagementofConcussion/MildTraumaticBrainInjury.JRehabilResDev,46(6),CP1-68.Keightley,M.L.,SinghSaluja,R.,Chen,J.K.,Gagnon,I.,Leonard,G.,Petrides,M.,&Ptito,A.(2014).Afunctionalmagneticresonanceimagingstudyofworkingmemoryinyouthaftersports-relatedconcussion:isitstillworking?.Journalofneurotrauma,31(5),437-451.Koski,L.,Kolivakis,T.,Yu,C.,Chen,J.K.,Delaney,S.,&Ptito,A.(2015).Noninvasivebrainstimulationforpersistentpostconcussionsymptomsinmildtraumaticbraininjury.Journalofneurotrauma,32(1),38-44.Kozlowski,K.F.,Graham,J.,Leddy,J.J.,Devinney-Boymel,L.,&Willer,B.S.(2013).Exerciseintoleranceinindividualswithpostconcussionsyndrome.JAthlTrain,48(5),627-635.doi:10.4085/1062-6050-48.5.02Leddy,J.J.,Cox,J.L.,Baker,J.G.,Wack,D.S.,Pendergast,D.R.,Zivadinov,R.,&Willer,B.(2013).Exercisetreatmentforpostconcussionsyndrome:apilotstudyofchangesinfunctionalmagneticresonanceimagingactivation,physiology,andsymptoms.JHeadTraumaRehabil,28(4),241-249.doi:10.1097/HTR.0b013e31826da964Leddy,J.J.,Kozlowski,K.,Donnelly,J.P.,Pendergast,D.R.,Epstein,L.H.,&Willer,B.(2010).Apreliminarystudyofsubsymptomthresholdexercisetrainingforrefractorypost-concussionsyndrome.ClinJSportMed,20(1),21-27.doi:10.1097/JSM.0b013e3181c6c22cMacFarlane,M.P.,&Glenn,T.C.(2015).Neurochemicalcascadeofconcussion.BrainInj,29(2),139-153.doi:10.3109/02699052.2014.965208Majerske,C.W.,Mihalik,J.P.,Ren,D.,Collins,M.W.,Reddy,C.C.,Lovell,M.R.,&Wagner,A.K.(2008).Concussioninsports:postconcussiveactivitylevels,symptoms,andneurocognitiveperformance.JAthlTrain,43(3),265-274.doi:10.4085/1062-6050-43.3.265Matthews,P.M.,Honey,G.D.,&Bullmore,E.T.(2006).ApplicationsoffMRIintranslationalmedicineandclinicalpractice.NatRevNeurosci,7(9),732-744.doi:10.1038/nrn1929McAllister,T.W.,&Arciniegas,D.(2002).Evaluationandtreatmentofpostconcussivesymptoms.NeuroRehabilitation,17(4),265-283.McDonald,B.C.,Saykin,A.J.,&McAllister,T.W.,(2012).FunctionalMRIofmildtraumaticbraininjury(mTBI):progressandperspectivesfromthefirstdecadeofstudies.BrainImagingandBehavior.6(2),193-207.

B.H.Wing,B.J.Tucker,A.K.Fong,andM.D.Allen/StandardizationoffNCI-directedrehabilitation
©CopyrightCognitiveFX201615
Meier,T.B.,Bellgowan,P.S.,Singh,R.,Kuplicki,R.,Polanski,D.W.,&Mayer,A.R.(2015).Recoveryofcerebralbloodflowfollowingsports-relatedconcussion.JAMANeurol,72(5),530-538.doi:10.1001/jamaneurol.2014.4778Mikulis,D.J.(2013).Chronicneurovascularuncouplingsyndrome.Stroke,44(6Suppl1),S55-57.doi:10.1161/STROKEAHA.113.001081Mutch,W.A.,Ellis,M.J.,Ryner,L.N.,RuthGraham,M.,Dufault,B.,Gregson,B.,...Group,f.T.U.H.N.C.R.R.(2015).BrainmagneticresonanceimagingCO2stresstestinginadolescentpostconcussionsyndrome.JNeurosurg,1-13.doi:10.3171/2015.6.JNS15972Plichta,M.M.,Schwarz,A.J.,Grimm,O.,Morgen,K.,Mier,D.,Haddad,L.,...Meyer-Lindenberg,A.(2012).Test-retestreliabilityofevokedBOLDsignalsfromacognitive-emotivefMRItestbattery.Neuroimage,60(3),1746-1758.doi:10.1016/j.neuroimage.2012.01.129Slobounov,S.M.,Zhang,K.,Pennell,D.,Ray,W.,Johnson,B.,&Sebastianelli,W.(2010).Functionalabnormalitiesinnormallyappearingathletesfollowingmildtraumaticbraininjury:afunctionalMRIstudy.Experimentalbrainresearch,202(2),341-354.Thomas,D.G.,Apps,J.N.,Hoffmann,R.G.,McCrea,M.,&Hammeke,T.(2015).Benefitsofstrictrestafteracuteconcussion:arandomizedcontrolledtrial.Pediatrics,135(2),213-223.doi:10.1542/peds.2014-0966Wang,Y.,West,J.D.,Bailey,J.N.,Westfall,D.R.,Xiao,H.,Arnold,T.W.,...McDonald,B.C.(2015).DecreasedcerebralbloodflowinchronicpediatricmildTBI:anMRIperfusionstudy.DevNeuropsychol,40(1),40-44.doi:10.1080/87565641.2014.979927Warden,D.L.,Gordon,B.,McAllister,T.W.,Silver,J.M.,Barth,J.T.,Bruns,J.,...Group,N.G.W.(2006).Guidelinesforthepharmacologictreatmentofneurobehavioralsequelaeoftraumaticbraininjury.JNeurotrauma,23(10),1468-1501.doi:10.1089/neu.2006.23.1468Warden,D.L.,Labbate,L.A.,Salazar,A.M.,Nelson,R.,Sheley,E.,Staudenmeier,J.,&Martin,E.(1997).Posttraumaticstressdisorderinpatientswithtraumaticbraininjuryandamnesiafortheevent?JNeuropsychiatryClinNeurosci,9(1),18-22.doi:10.1176/jnp.9.1.18Zhang,D.,Johnston,J.M.,Fox,M.D.,Leuthardt,E.C.,Grubb,R.L.,Chicoine,M.R.,...Shimony,J.S.(2009).Preoperativesensorimotormappinginbraintumorpatientsusingspontaneousfluctuationsinneuronalactivityimagedwithfunctionalmagneticresonanceimaging:initialexperience.Neurosurgery,65(6Suppl),226-236.doi:10.1227/01.NEU.0000350868.95634.CA