Developing JCIH Recommendations on Quality Infant Audiology Services (Q*IAS) National EHDI...
34
Developing JCIH Recommendations on Quality Infant Audiology Services (Q*IAS) National EHDI Conference February 18-21, 2004 Pat Brookhouser, M.D. Brandt Culpepper, Ph.D., CCC-A Judith Gravel, Ph.D., CCC-A
-
Upload
dwight-stephens -
Category
Documents
-
view
212 -
download
0
Transcript of Developing JCIH Recommendations on Quality Infant Audiology Services (Q*IAS) National EHDI...
Developing JCIH Recommendations on
Quality Infant Audiology Services (Q*IAS)
National EHDI Conference
February 18-21, 2004
Pat Brookhouser, M.D.Brandt Culpepper, Ph.D., CCC-AJudith Gravel, Ph.D., CCC-A

The Joint Committee on Infant Hearing (JCIH) is recognized both nationally and internationally for its role in shaping public health policy
with regard to early hearing detection and intervention (EHDI) programs.

First position statement in 1970 - JCIH advocated for early detection of hearing loss.
JCIH Year 2000 Position Statement - provided principles and guidelines for quality EHDI programs along with benchmarks and
quality indicators for newborn hearing screening, assessment and intervention.

JCIH 2000 offered broad suggestions regarding the
knowledge and skills needed by audiologists providing
services to infants and young children.
However, there has been no specific
direction offered by a nationally recognized professional group that
would assist state EHDI coordinators or primary care physicians in
identifying qualified providers of
infant audiology services

• Contract from Maternal and Child Health Bureau (MCHB/HRSA)
– Administered through BTNRH
• Deliverable: – Develop and ultimately publish strong and
comprehensive recommendations on Quality Infant Audiology Services (Q*IAS)

JCIH Q*IAS Recommendations
• Five project components: complete by August 31, 2004
1. Data collection;
2. Identification of existing models of service delivery;

1. Data Collection
• Survey of State EHDI system
• Web searches for additional resources
• Review of international and national policies, guidelines, and recommendations
Survey of State EHDI Systems
• One page survey sent to state EHDI coordinators (email and hardcopy)
• Follow-up email(s) to those not responding
• Phones call to state directors to those not responding to previous efforts

Copies Requested
• Audiology services survey (when and results)
• List of infant audiology service providers
• Assessment protocols
• Amplification protocols
• Web site(s), related information

Responses
• N= 56/56– 50 states, DC, AS, MP, GU, PR, VI– 43 - Returned by email/fax (2 mailings via
email and snail mail)– 13 responded to follow-up phone calls

U.S. Territories Responding

Has your state surveyed audiologists?
47
8 1
Yes No Pending N=56
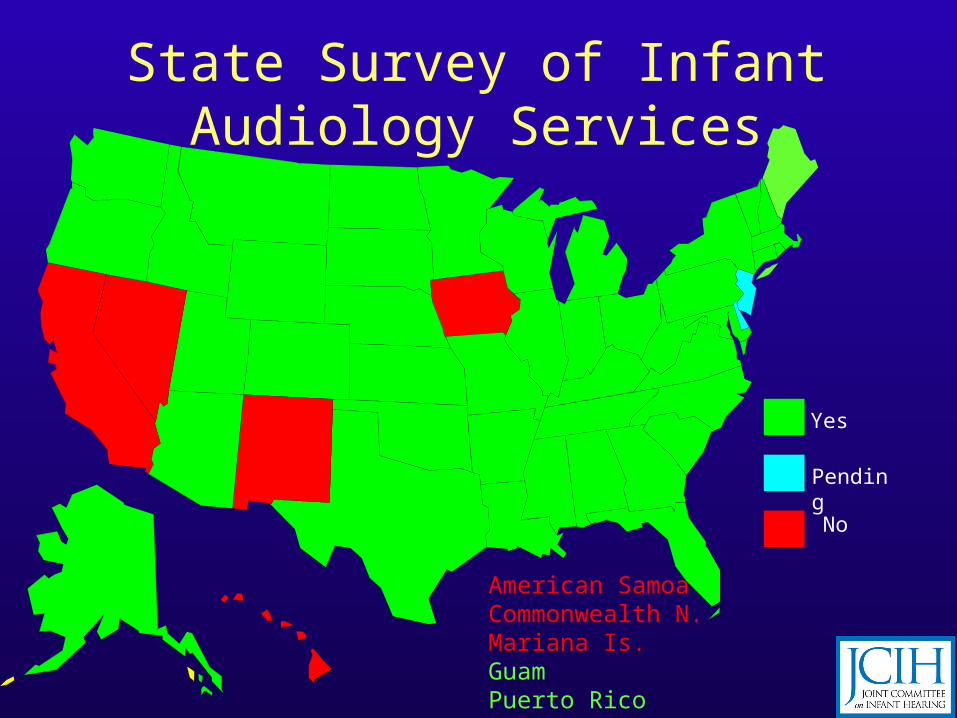
State Survey of Infant Audiology Services
Yes
Pending
No
American SamoaCommonwealth N. Mariana Is.GuamPuerto RicoVirgin Islands

List of Infant Audiology Service Providers
40
14
2
Yes No Pending N=56

List of Infant Audiology Providers
Yes
Pending
No
American SamoaCommonwealth N. Mariana Is.GuamPuerto RicoVirgin Islands
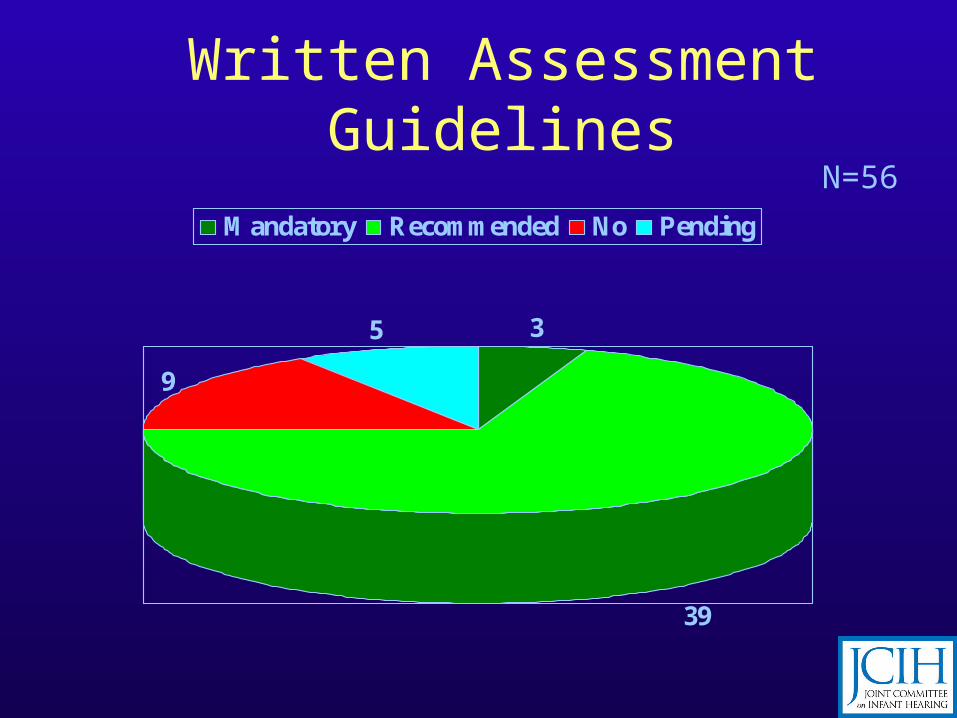
Written Assessment Guidelines
3
39
9
5
Mandatory Recommended No Pending
N=56

Infant Assessment Guidelines
Recommended
Pending
Nonedeveloped
American SamoaCommonwealth N. Mariana Is.GuamPuerto RicoVirgin Islands
Mandatory
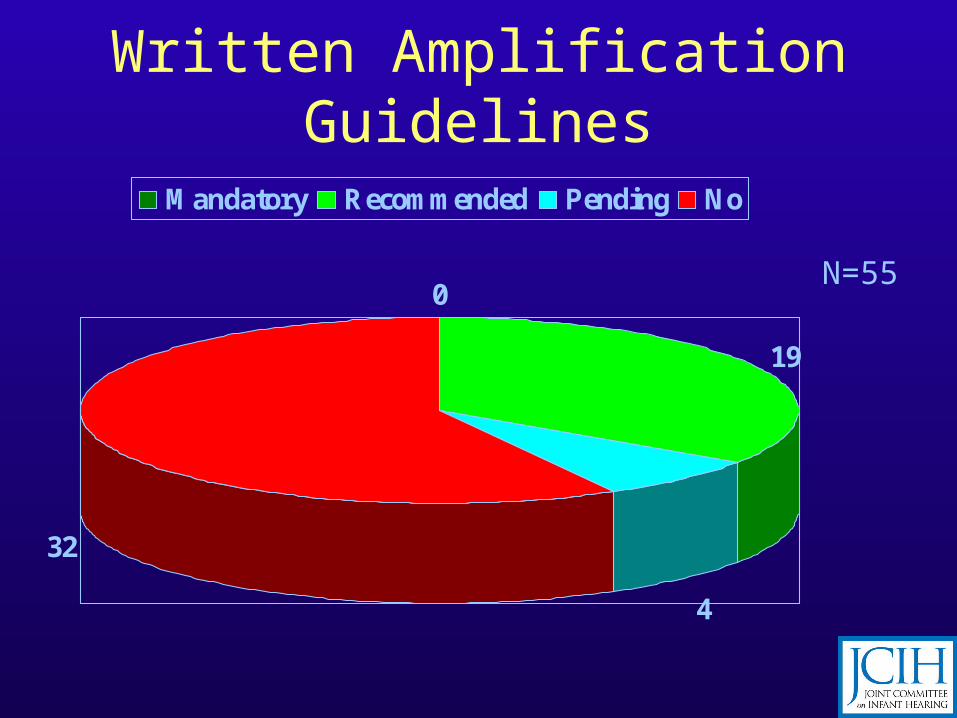
Written Amplification Guidelines
0
19
4
32
Mandatory Recommended Pending No
N=55

Infant Amplification Guidelines
Existing
Pending/Draft
No knowndocumentAmerican Samoa
Commonwealth N. Mariana Is.GuamPuerto RicoVirgin Islands
Mandatory

Credentials for Pediatric Audiology
Yes
Pending
NoAmerican SamoaCommonwealth N. Mariana Is.GuamPuerto RicoVirgin Islands
N=56
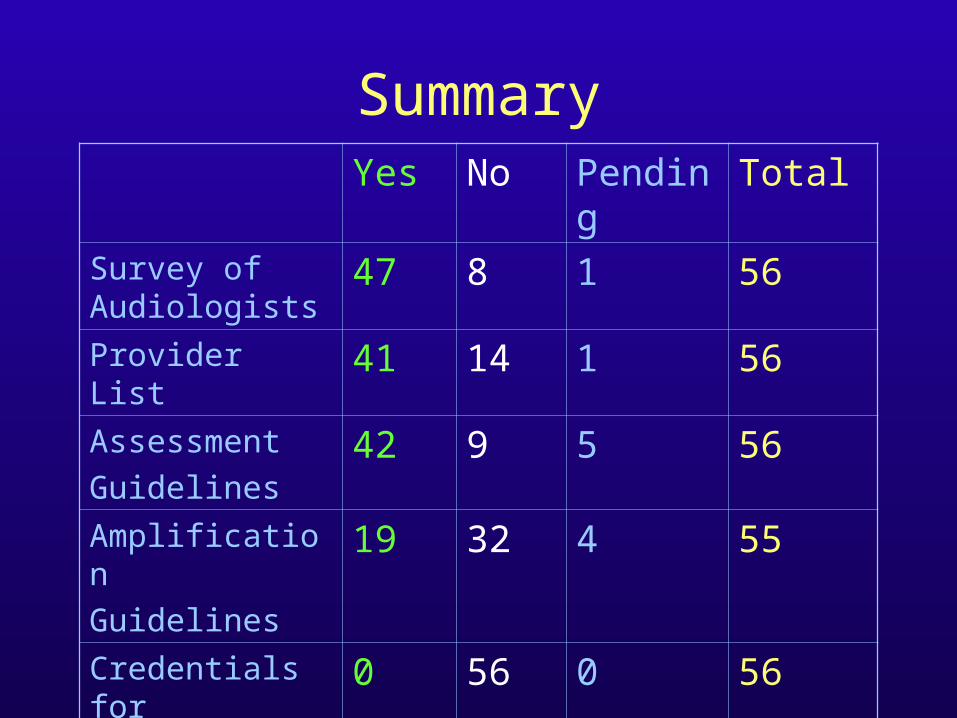
SummaryYes No Pending Total
Survey of Audiologists
47 8 1 56
Provider List 41 14 1 56
Assessment
Guidelines42 9 5 56
Amplification
Guidelines19 32 4 55
Credentials for
Pediatric Auds0 56 0 56
Summary of State-Developed Infant Assessment Documents
• 38/42 state assessment documents available for inclusion
• 5 states report documents exist, but not included in the tally

Assessment Information Reviewed
• Objective Components– Click ABR, frequency-specific ABR, middle ear
measures, EOAE, etc.
• Behavioral Components– BOA, VRA, COR, CPA, etc.
• Programmatic issues– Report to, minimal requirements
• Related components– Counseling, referrals, etc.
Summary of State-Developed Amplification Documents
• 18 * documents available for inclusion
• 4 states report documents developed
• 4 states said no, but have info to include
• 1 draft, but available
*2 center-based approach

Amplification Information Reviewed
• Candidacy
• Preselection considerations
• Selection
• Objective and Behavioral measures
• Instrumentation
Also available . . .
• Examining approaches in other countries:• Canada
– Ontario Infant Hearing Program (IHP)
• UK – Newborn Hearing Screening Programme
Workbook
• Australia

JCIH Q*IAS Recommendations• Five project components: complete by August 31,
2004
1. Data collection; 2. Identification of existing models of service
delivery; 3. Delineation of knowledge, skills, experience, and
instrumentation needed to provide quality infant audiology services;
4. Development of models for continuing education; and
5. Recommendations.
Panel Meeting Panel Meeting
Development of JCIH RecommendationsDevelopment of JCIH Recommendationson Quality Infant Audiology Services (Q*IAS)on Quality Infant Audiology Services (Q*IAS)
December 12-14, 2003December 12-14, 2003ASHA National Office
Supported by the Maternal & Child Health BureauContract #03-MCHB-057B-AB

PanelInvited Panel• Michael Gorga• Patricia Stelmachowicz• Barbara Cone-Wesson• Mary Pat Moeller• Richard Seewald• Brandt Culpepper
– Judy Widen– Anne Marie Tharpe
JCIH Panel Members• Yvonne Sininger• Christie Yoshinaga-
Itano• Jack Roush• Linda Pippins• Patrick Brookhouser• Judy Gravel
JCIH Q*IAS Recommendations will address:
• availability and use of current assessment technologies;
• timely and appropriate selection, evaluation and monitoring of acoustic amplification and, in some cases, candidacy for cochlear implantation;
• competency in counseling;
• awareness of all communication options open to a family of an infant with hearing loss or who is deaf; and,
• knowledge regarding public health and education laws including eligibility, accessibility and covered services.

Overriding aim - to influence decisions/referrals made by Early Intervention programs at the state and local levels; thereby,
• leading states to recognize quality providers of infant audiologic services;
• supporting the development of service delivery models that ensure infants and families receive appropriate services;
• facilitating the possible development of specialty recognition by professional audiology associations; and,
• providing guidance to pediatricians who must seek quality audiologic services as they coordinate care of an infant with hearing loss through the medical home.

JCIH will seek approval from the professional organizations represented by the Committee to publish and disseminate the document
• American Academy of Audiology, • American Academy of Pediatrics, • American Speech-Language-Hearing
Association,• American Academy of Otolaryngology – Head
and Neck Surgery, • Council on the Education of the Deaf • Directors of Speech and Hearing Programs in
State Health and Welfare Agencies

www.jcih.org